Embed Size (px)
Citation preview
Cardiovascular malformations are present in up to45% of patients with Turner’s syndrome.1 Whileaortic coarctation and bicuspid aortic valve are
the most frequent abnormalities, aortic dissection or rup-ture represents the most serious complication in thesepatients. We report the unusual case of a 36-year-oldwoman with Turner’s syndrome who died followingaortic intramural haemorrhage (IMH) complicated bydissection and rupture, with no evidence of aortic inti-mal tear.
Case Report
The patient had undergone successful corrective surgeryfor coarctation of the aorta at the age of 6 years. She wason long-term oestrogen replacement therapy but took noother medication. Regular cardiology reviews during the12 years before the patient’s death found her to be con-sistently normotensive, with no clinical evidence ofresidual coarctation of the aorta. Serial trans-thoracicechocardiograms were limited by very poor echocardio-graphic windows, but Doppler velocities of 2.0–3.0 m/s(pressure gradient up to 36 mmHg) in the region of thecoarctation repair suggested only minor residual nar-rowing. The patient also had a known congenital bicus-pid aortic valve with a mean gradient of 15 mmHg,consistent with mild stenosis. Left ventricular systolicfunction was normal, but the aortic root and ascendingaorta dimensions could not be adequately assessed by
Case Report
An Unusual Case of Aortic Dissection inTurner’s Syndrome
Philip M. Mottram, MB BS (Hons), FRACP,1 Shelley D. Robertson, MB BS, FRCPA2 andRichard W. Harper, FRACP, FACC1
1Department of Cardiology, Monash Medical Centre and 2Victorian Institute of Forensic Medicine, Melbourne, Victoria, Australia
Cardiovascular malformations are common in patients with Turner’s syndrome. Aorticcoarctation and bicuspid aortic valve are the most frequently occurring abnormalities, and areassociated with cystic medial necrosis of the aortic wall. Aortic dissection is an uncommon butcatastrophic complication of the ‘aortopathy’ of Turner’s syndrome. We report the unusual caseof a Turner’s syndrome patient (with a bicuspid aortic valve and previous coarctation repair)who died following an intramural haemorrhage of the aortic root that was complicated bydissection and rupture, with no evidence of aortic intimal tear. The role of intramuralhaemorrhage in the pathogenesis of acute aortic syndromes in Turner’s syndrome patients isunclear. The condition may be associated with atypical clinical presentations, it can be difficultto confirm with imaging techniques, and it carries a high risk of progression to classical aorticdissection and death. This case therefore highlights the need for a high index of suspicion whenassessing Turner’s syndrome patients presenting with chest pain syndromes. Furthermore, theeffective management of Turner’s syndrome patients with cardiovascular abnormalities requiresthe development of evidence-based preventive (such as echocardiographic surveillance of aorticdilatation) and interventional strategies. (Heart, Lung and Circulation 2001; 10: 158–160)
Key words: aortic dissection, cardiovascular malformation, Turner’s syndrome.
Correspondence: Philip Mottram, University Department ofMedicine, Princess Alexandra Hospital, Ipswich Road,Woolloongabba, Queensland 4102, Australia.Email: [email protected]
Heart, Lung and Circulation 2001; 10 P. M. Mottram et al.Aortic dissection in Turner’s syndrome
159
trans-thoracic imaging. A trans-oesophageal study wasconsidered but was not expected to alter management,and the patient had declined to have the procedure. Theelectrocardiogram consistently showed an intraventric-ular conduction delay and widespread non-specific STand T wave changes.
Eighteen days before her death, the patient presentedto the Emergency Department at the Monash MedicalCentre with sharp retrosternal chest pain that was worseon inspiration. On examination, blood pressure was120/70 and all pulses were palpable, equal and normal.Apart from an ejection systolic murmur consistent withher aortic valve disease, there were no abnormal cardio-vascular findings. The electrocardiogram (ECG) wasunchanged from previous recordings. Serial cardiacenzyme levels were normal. The chest X-ray radiographwas also normal, with no abnormality of the mediastinalcontour. The patient’s chest pain resolved over severalhours and after a further period of observation she wasdischarged. Over subsequent days the patient presentedto her general practitioner with symptoms of lethargyand a severe cough. A diagnosis of viral infection wasmade and the symptoms gradually improved over thefollowing fortnight. She was then unexpectedly founddeceased at her home by family members who hadfound her to be well several hours earlier.
Autopsy examination revealed dilatation of theascending aorta with IMH and dissection originating inthe region of the ostium of the right coronary artery. Thedissection had ruptured externally through the aorticadventitia, resulting in pericardial tamponade (withapproximately 500 mL of partially clotted blood in the
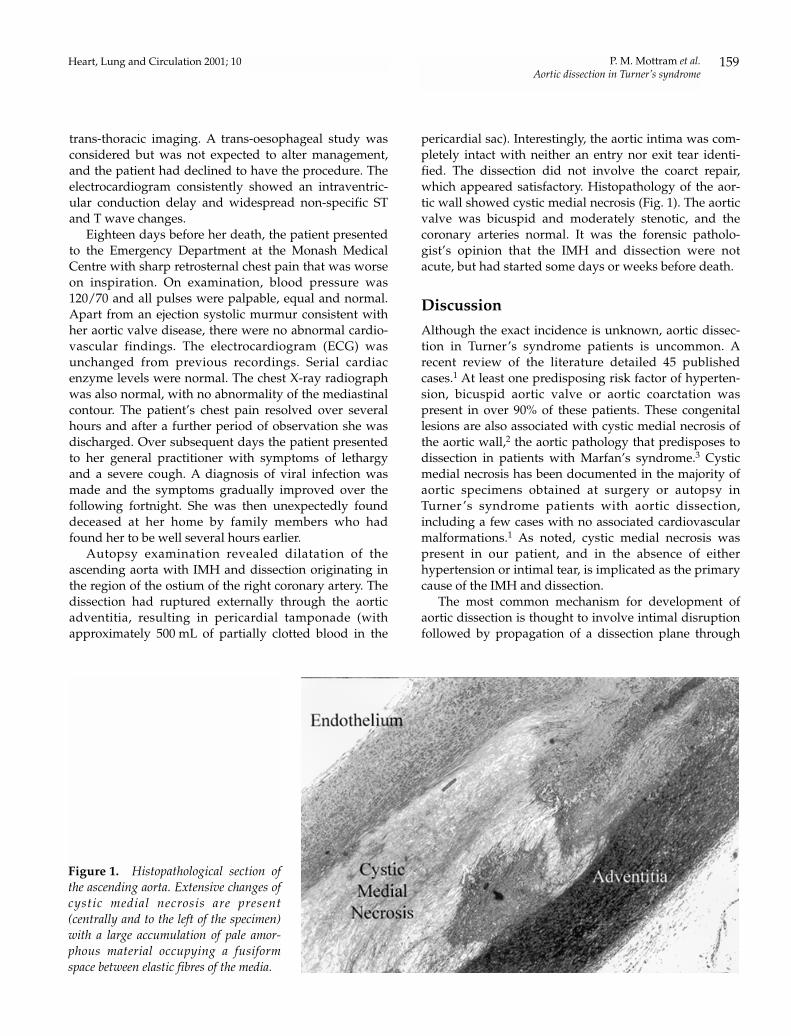
pericardial sac). Interestingly, the aortic intima was com-pletely intact with neither an entry nor exit tear identi-fied. The dissection did not involve the coarct repair,which appeared satisfactory. Histopathology of the aor-tic wall showed cystic medial necrosis (Fig. 1). The aorticvalve was bicuspid and moderately stenotic, and thecoronary arteries normal. It was the forensic patholo-gist’s opinion that the IMH and dissection were notacute, but had started some days or weeks before death.
Discussion
Although the exact incidence is unknown, aortic dissec-tion in Turner’s syndrome patients is uncommon. Arecent review of the literature detailed 45 publishedcases.1 At least one predisposing risk factor of hyperten-sion, bicuspid aortic valve or aortic coarctation waspresent in over 90% of these patients. These congenitallesions are also associated with cystic medial necrosis ofthe aortic wall,2 the aortic pathology that predisposes todissection in patients with Marfan’s syndrome.3 Cysticmedial necrosis has been documented in the majority ofaortic specimens obtained at surgery or autopsy inTurner ’s syndrome patients with aortic dissection,including a few cases with no associated cardiovascularmalformations.1 As noted, cystic medial necrosis waspresent in our patient, and in the absence of eitherhypertension or intimal tear, is implicated as the primarycause of the IMH and dissection.
The most common mechanism for development ofaortic dissection is thought to involve intimal disruptionfollowed by propagation of a dissection plane through
Figure 1. Histopathological section ofthe ascending aorta. Extensive changes ofcystic medial necrosis are present(centrally and to the left of the specimen)with a large accumulation of pale amor-phous material occupying a fusiformspace between elastic fibres of the media.

Heart, Lung and Circulation 2001; 10P. M. Mottram et al.Aortic dissection in Turner’s syndrome
160
the media under the driving force of systemic bloodpressure. Primary IMH with an intact intima, as docu-mented in our case, represents an unusual variant ofaortic dissection (5–10% of cases) with the postulatedpathogenesis involving rupture of the vasa vasorum intoa weakened media.4 While IMH has been implicated inapproximately 10% of Marfan’s syndrome-related aorticdissections,5 its role in Turner’s syndrome patients isunknown. In the case described, it is likely that thepatient’s chest pain 18 days before the aortic rupture rep-resented the onset of the IMH. The natural history of thiscondition remains unclear: cases of complete healing ofan IMH have been described in non-Turner patients, ashas progression to aortic dissection and rupture.4 Onecould postulate that severe coughing may have con-tributed to the latter outcome in this case, as a result oftransient marked increases in intrathoracic pressure.Management of IMH is controversial, but as progressionto either classic dissection or rupture has been docu-mented in up to 60% of cases, an aggressive approach isgenerally recommended as per classic aortic dissection.
This unusual case of aortic IMH in Turner’s syn-drome emphasises the need for a high index of suspicionwhen these patients present with chest pain syndromes,particularly if they have accompanying hypertension orcardiovascular malformations. Furthermore, in exclud-ing aortic complications in the acute setting, one shouldconsider imaging techniques that can accurately detectIMH in the absence of an intimal tear or classic dissec-tion, such as transoesophageal echocardiography,4 com-puted tomography or magnetic resonance imaging.6
With regards to prevention, it is known that Turner’ssyndrome patients with or without cardiovascular mal-formations have an increased incidence of aortic dilata-tion (as was present in our case), with more severedilatation correlating with the presence of a bicuspidaortic valve.7 The natural history of aortic dilatationin Turner’s syndrome and its relationship to the risk ofaortic dissection and rupture (as has been shown in
Marfan’s syndrome8) is currently unknown. Further-more, there are no data examining the effects of inter-ventions such as beta blockade or prophylactic aorticsurgery in this patient group. Accordingly, while peri-odic echocardiographic monitoring of aortic root sizemay identify those at increased risk of aortic complica-tions, prospective studies are required to develop effec-tive guidelines for managing Turner’s syndrome patientswith cardiovascular abnormalities.
Acknowledgements
The authors wish to thank the Victorian Institute ofForensic Medicine photographer, Karen Byrne, for pro-viding the histopathological photograph.
References
1. Sybert VP. Cardiovascular malformations and complications inTurner syndrome. Pediatrics 1998; 101: e11.
2. Isner JM, Donaldson RF, Fulton D, Bhan I, Payne DD, ClevelandRJ. Cystic medial necrosis in coarctation of the aorta. Circulation1987; 75: 689–95.
3. Pyeritz RE, McKusick VA. The Marfan syndrome: Diagnosisand management. N. Eng. J. Med. 1979; 300: 772–7.
4. Mohr-Kahaly S, Erbel R, Kearney P, Puth M, Meyer J. Aorticintramural haemorrhage visualized by transesophagealechocardiography: findings and prognostic implications. J. Am.Coll. Cardiol. 1994; 23: 658–64.
5. von Kodolitsch Y, Spielmann RP, Nienaber CA. Acute andchronic aortic diseases in Marfan syndrome and arterialhypertension – a comparison of anatomy, clinical aspects andprognosis. Z. Cardiol. 1995; 84: 542–52.
6. Stanson AW, Welch TJ, Ehman RL, Sheedy PF II. A variantof aortic dissection: computed tomography and magneticresonance findings. Cardiovasc. Imaging 1989; 1: 55–9.
7. Allen DB, Hendricks SA, Levy JM. Aortic dilation in Turnersyndrome. J. Pediatr. 1986; 109: 302–5.
8. Roman MJ, Rosen SE, Kramer-Fox R, Devereux RB. Prognosticsignificance of the pattern of aortic root dilation in the Marfansyndrome. J. Am. Coll. Cardiol. 1993; 22: 1470–6.