Embed Size (px)
Citation preview

Pediatric Hematology and Oncology, 22:499–505, 2005Copyright C© Taylor and Francis Inc.ISSN: 0888-0018 print / 1521-0669 onlineDOI: 10.1080/08880010591002332
AN UNUSUAL ASSOCIATION OF TAR SYNDROME WITH
ESOPHAGEAL ATRESIA: A Variant?
Erdal Eren, MD � Department of Pediatrics, Suleyman Demirel University Facultyof Medicine, Isparta, Turkey
B. Ilker Buyukyavus, MD, and I. Faruk Ozguner � Department of PediatricSurgery, Suleyman Demirel University Faculty of Medicine, Isparta, Turkey
Bahattin Tunc, MD � Department of Pediatric Hematology, Suleyman DemirelUniversity Faculty of Medicine, Isparta, Turkey
M. Cagri Savas, MD � Department of Pediatric Surgery, Suleyman Demirel UniversityFaculty of Medicine, Isparta, Turkey
� Thrombocytopenia and absent radii (TAR) syndrome is a rare disorder. It may be associated with,for example, as cardiovascular, genitourinary, gastrointestinal, skeletal, neurological, ophthalmic,and facial anomalies. Esophageal atresia is also a rare anomaly associated with genitourinary,skeletal, and cardiovascular anomalies, among others. Here, the authors present a child with TARsyndrome and esophageal atresia with tracheoesophageal fistula. This association has been reportedin only one other case in literature.
Keywords esophageal atresia thrombocytopenia absent radii syndrome
Incidence of esophageal atresia (EA) is 2–3 per 10,000 births [1]. Con-genital anomalies associated EA have been reported to be between 50 and70%. Most common anomalies include cardiovascular, genitourinary, gas-trointestinal, and skeletal. Furthermore, different anomalies, such as neu-rological, ophthalmic, and facial, have been reported. EA is also found inconjunction with VACTERL and CHARGE [1]. EA without fistula is veryrare. The syndrome of thrombocytopenia with absent radii (TAR) is a rarecongenital hematological disease. This syndrome is characterized by skeletaland hematological abnormalities. Fanconi aplastic anemia (FA) is also associ-ated with esophageal atresia, especially with VACTERL association [2]. TARsyndrome and esophageal atresia with tracheoesophageal fistula has been
Received 20 October 2004; accepted 28 April 2005.Address correspondence to M. Cagri Savas, MD, Associate Professor of Pediatric Surgery, Suleyman
Demirel University Medical Faculty, Posta Kutusu 76, 32000 Isparta, Turkey. E-mail: [email protected]
499
Pedi
atr
Hem
atol
Onc
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
he U
nive
rsity
of
Man
ches
ter
on 1
1/06
/14
For
pers
onal
use
onl
y.

500 E. Eren et al.
reported in only one case in literature [3]. We present the second case withEA + bilaterally TAR syndrome in the literature.
CASE REPORT
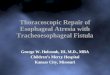
An 8-day-old female newborn was referred to our hospital with the suspi-cion of esophageal atresia due to a swallowing problem and increased oralsecretion. The patient was born to a 28-year-old gravida 2 para 2 mother bycaesarean section at full term and her weight was 2600 g. The pregnancyhad been uncomplicated and there was no history of polyhydroamnios ortaking drugs or alcohol. There was a family history of consanguinity anda congenitally malformed child who died at 10 days old because of hydro-cephalous and other congenital problems. Physical examination revealedthat the length, weight, and head circumference of the patient were all innormal percentages. There were no hematological signs like petechiae, ec-chymosis, hepatomegaly, and splenomegaly. All systems except limbs werenormal on physical examination. Bilaterally absent radii and thumbs werefound and confirmed by roentgenograms (Figures 1–3) but there was novertebral anomaly.
On admission, complete blood count (CBC) showed hemoglobin of18.4 g/dL, white blood cell count of 10.3 × 109/L, and platelet count of10 × 109/L. Blood chemistry and urinalysis were normal. We have seen
FIGURE 1 Baby with TAR syndrome showing shortened forearms with radial deviation of the hands.
Pedi
atr
Hem
atol
Onc
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
he U
nive
rsity
of
Man
ches
ter
on 1
1/06
/14
For
pers
onal
use
onl
y.

TAR Syndrome with Esophageal Atresia 501
FIGURE 2 Baby with TAR syndrome showing shortened forearms with radial deviation of the hands.
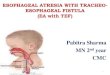
nonaggregated seldom thrombocyte cells in the peripheral blood smear ex-amination. Then we performed bone marrow aspiration and found rare smallmegacaryocyte cells. Diagnosis of TAR syndrome was made by the physicalexamination and other diagnostic techniques mentioned above, like CBC,bone marrow aspiration, and peripheral blood smear findings. Diagnosisof esophageal atresia with tracheoesophageal fistula was made by barium-contrast study of the upper pouch of the esophagus (Figure 4). Double gas-trostomy was performed first due to a long gap between upper and loweresophageal endings. During the operation, there was no bleeding and onlythree units platelets were given to the patients. The upper esophagus wasforced to advance by bougienage, and after 4 weeks primary anastomosisand ligation of fistula was performed. Postoperative period was uneventfuland the esophageal passage had been established by esophagography. Butthe patient died of septicemia on postoperative day 12. The patient did notdevelop neutropenia.
DISCUSSION
TAR syndrome was first noted by Greenwald and Sherman in 1929 but cer-tain definition of the syndrome was done by Hall et al. [4, 5]. TAR syndromeis a rare autosomal disorder and includes various system abnormalities, suchas hematological, skeletal, cardiac, and gastrointestinal. TAR syndrome may
Pedi
atr
Hem
atol
Onc
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
he U
nive
rsity
of
Man
ches
ter
on 1
1/06
/14
For
pers
onal
use
onl
y.

502 E. Eren et al.
FIGURE 3 Roentgenogram showing absent radii and thumb.
be associated with skeletal defects of upper and lower extremities, such asulnar, humeral, and femoral hypoplasia, and congenital hip dislocation, syn-dactyly, talipes equinovarus, and genu varum. Cardiac and renal defects likehorseshoe kidney may be found in cases with TAR syndrome [6]. TAR syn-drome commonly needs to be differentiated from Fanconi aplastic anemia(FA), trisomy 18, and Holt-Oram syndrome. Aplasia of thumbs is not seen inHolt-Oram syndrome and blood cell counts are normal in contrast to those
Pedi
atr
Hem
atol
Onc
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
he U
nive
rsity
of
Man
ches
ter
on 1
1/06
/14
For
pers
onal
use
onl
y.

TAR Syndrome with Esophageal Atresia 503
FIGURE 4 Barium roentgenogram showing upper pouch of esophagus (esophageal atresia).
of TAR syndrome. FA has aplasia of the thumbs, chromosome fragility, pan-cytopenia, and rare onset of thrombocytopenia before 1 years of age. FA iscommonly seen at the mean age of 8.5 years old, unlike in our case, andour case never presented with pancytopenia. Unfortunately, chromosomalfragility (DEB) testing was not done because we could not perform the testin our hospital. Thumbs are always present in TAR, but were absent in ourcase [2].
Pedi
atr
Hem
atol
Onc
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
he U
nive
rsity
of
Man
ches
ter
on 1
1/06
/14
For
pers
onal
use
onl
y.

504 E. Eren et al.
Characteristic hematological findings in TAR syndrome are hy-pomegakaryocytic thrombocytopenia, periodic leukemoid reactions, andeosinophilia. Three cases with TAR syndrome who developed leukemia havealso been reported [7]. The risk of life-threatening hemorrhage from throm-bocytopenia, especially in the first year of life, is an important and fatal com-plication of TAR syndrome. An increase susceptibility to infections is alsoobserved. Forty percent of affected patients die during early infancy [8].After the first year of life, the thrombocytopenia usually improves and attimes spontaneously resolves. The pathophysiology of thrombocytopenia inthis syndrome is not clear. TAR syndrome may be diagnosed prenatally byfinding of thrombocytopenia at the time of cordosentesis and sonographicfeatures. Prenatal detection of the disease can be useful because of more ap-propriate management including intrauterine platelet transfusion to preventfetal hemorrhage in labor, and a planned atraumatic delivery or terminationof pregnancy [9].
EA is characterized by incomplete formation of the esophagus. One-halfof EA is associated with congenital anomalies. Various systems such as mus-culoskeletal, gastrointestinal, cardiac, and genitourinary may be affected.Sometimes EA may be a part of VATER (vertebral defect, anorectal malfor-mation, tracheoesophageal fistula, and renal) anomaly or VACTERL asso-ciation (vertebral defect, anorectal malformation, cardiac defect, tracheoe-sophageal fistula, renal anomaly, limb defects). Up to 10% of infants with EAhave associated VATER syndrome [10]. Esophageal abnormalities have beendescribed in only one case with TAR syndrome. The case presented with uni-laterally absent radius with esophageal atresia. Our case had bilateral absentradius with thumbs and esophageal atresia with tracheoesophageal fistula(type III), which differed from the usual TAR association of esophageal atre-sia with the aspect of thumb absence, which is unusual in TAR syndrome [2].This case may be an unusual presentation of TAR syndrome with esophagealatresia. We believe that TAR syndrome did not affect the prognosis of thepatient but it may have been acting on the immune system of the case andhelped develop sepsis.
REFERENCES
[1] Harmon CM, Coran AG. Congenital anomalies of the esophagus. In: O’Neil JA, Rowe MI, GrosfeldJL, Fonkalsrud EW, Coran AG, eds. Pediatric Surgery, ed 5. St. Louis: Mosby Year Book; 1998:941–967.
[2] Alter BP, Young NS. The bone marrow failure syndromes. In: Nathan DG, Orkin SH, eds. Hematologyof Infancy and Childhood, ed 5. Philadelphia: WB Saunders; 1998: 259–309.
[3] Bajaj R, Jain M, Kasat L, et al. Tar syndrome with unilateral absent radius and associated esophagealatresia: a variant? Indian J Pediatr. 1999;66:460–463.
[4] Greenwald HM, Sherman I. Congenital essential thrombocytopenia. Am J Dis Child. 1929;38:1245–1251.
[5] Hall JG, Levin J, Kuhn JP, et al. VA. Thrombocytopenia with absent radius (TAR). Medicine.1969;48:411–39.
Pedi
atr
Hem
atol
Onc
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
he U
nive
rsity
of
Man
ches
ter
on 1
1/06
/14
For
pers
onal
use
onl
y.

TAR Syndrome with Esophageal Atresia 505
[6] Bradshaw A, Donnelly LF, Foreman JW. Thrombocytopenia and absent radii (TAR) syndrome as-sociated with horseshoe kidney. Pediatr Nephrol. 2000;14:29–31.
[7] Fadoo Z, Naqvi SM. Acute myeloid leukemia in a patient with thrombocytopenia with absent radiisyndrome. J Pediatr Hematol Oncol. 2002;24:134–135.
[8] Hedberg VA, Lipton JM. Thrombocytopenia with absent radii: a review of 100 cases. Am J PediatrHematol Oncol. 1988;10:51–64.
[9] Tongsong T, Sirichotiyakul S, Chanprapaph P. Prenatal diagnosis of thrombocytopenia-absent-radius (TAR) syndrome. Ultrasound Obstet Gynecol. 2000;15:256–258.
[10] Clark DC. Esophageal atresia and tracheoesophageal fistula. Am Fam Physician. 1999;59:910–916.
Pedi
atr
Hem
atol
Onc
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
he U
nive
rsity
of
Man
ches
ter
on 1
1/06
/14
For
pers
onal
use
onl
y.