Embed Size (px)
Citation preview
MEDICAL EDUCATION
An Investigation Into Medical Students’Approaches to Anatomy Learning in aSystems-Based Prosection Course
CLAIRE FRANCE SMITH1* AND HAYDN MATHIAS2
1Centre for Learning Anatomical Sciences, School of Medicine, University of Southampton,Boldrewood Campus, Southampton, Hampshire, United Kingdom
2School of Education, University of Southampton, Highfield Campus, Southampton, Hampshire,United Kingdom
Students’ approaches to learning anatomy are driven by many factors andperceptions, e.g., the curriculum, assessment, previous educational experi-ence, and the influence of staff and fellow students. However, there has beenremarkably little research into characterizing how students approach theiranatomy learning. What is known, based on a sample of 243 students, is thatstudents studying medicine at the University of Southampton adopt primarilya ‘‘deep’’ approach to learning. Medical students at Southampton learn anat-omy in a systems-based curriculum through prosections. Analysis of data froman Approaches to Study Inventory (ASSIST) revealed that students preferredusing a deep approach over a strategic or surface approach (P < 0.001 andP < 0.001, respectively). They also adopted an increasingly strategic approachas they moved through the medical curriculum. There was a relationshipbetween anatomy examination results and approach to learning. Students whoadopted a strategic approach performed better (R ¼ 0.266, P < 0.001). It isargued that curriculum design, including the form of assessment, is the key topromote effective anatomy education and the goal of deep and meaningfullearning in preparation for professional practice. Clin. Anat. 20:843–848,2007. VVC 2007 Wiley-Liss, Inc.
Key words: anatomical education; approaches to learning; assessment; medi-cal curriculum
INTRODUCTION
Surprisingly little is known about how students actuallylearn anatomy. A considerable amount of research anddebate has focused on the pros and cons of dissection (Skid-more, 1995; Utting and Willan, 1995; Nnodim et al., 1996;Yeager, 1996; Dinsmore et al., 1999; Ellis, 2001; Granger,2004; Pawlina and Lachman, 2004; Topp, 2004) and curric-ular issues, e.g., decrease in time allotted to anatomy (Jones,1997; McKeown et al., 2003; Prince et al., 2005). Theseissues have all been important in placing anatomy educationwhere is it today. Some research has investigated themechanics of learning anatomy in terms of spatial aware-ness (Rochford, 1985; Marks, 2000; Miller, 2000; Garget al., 2001; Moss, 2001), but there has been a distinct lackof research on the student experience of learning anatomy.
The research reported here is mainly the quantitativeelement of a wider quantitative–qualitative exploratorystudy, investigating how students perceive and approachlearning anatomy in the context of medical education in asystems-based prosection course in the United Kingdom.
*Correspondence to: C.F. Smith, Centre for Learning AnatomicalSciences, School of Medicine, University of Southampton, Biologi-cal Sciences Building, Bassett Crescent East, Southampton,Hampshire SO16 7PX, United Kingdom.E-mail: [email protected]
Received 28 December 2006; Revised 28 June 2007; Accepted13 July 2007
Published online 20 August 2007 in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/ca.20530
VVC 2007 Wiley-Liss, Inc.
Clinical Anatomy 20:843–848 (2007)
The qualitative element used interviews and focus groupsto gain a deeper understanding of the student experi-ence and to provide evidence to help make sense of thequantitative results. The research used the Approaches andStudy Skills Inventory for Students (ASSIST) Inventory(Entwistle, 2006) to determine students’ approaches toanatomy learning. Taking into consideration the literature,which comments that students have a lamentable anatomi-cal knowledge resulting in increased litigation (Ellis, 2002),we hoped that our study would elucidate such concerns byexamining how students approached the learning of anat-omy (e.g., whether they took a superficial or ‘‘surface’’approach) and what might be influencing the approachesthey adopted.
Approaches to Learning: Deep/Surface/Strategic
Over the last 30 years there has been an increasing em-phasis on research into the student learning experience. Theseminal work of Marton and Saljo (1976) and later of Rams-den (2003) investigated how students tackled various learn-ing tasks and identified qualitatively different approaches tolearning characterized by the students’ conceptions of learn-ing, their perceptions of the learning context, the influence oftheir previous learning experiences, their intentions forlearning, and their learning preferences. The main app-roaches to learning identified were termed ‘‘deep’’ and‘‘surface.’’ Related and subsequent work by researchersEntwistle and Biggs (Biggs, 2003) led to the identification ofa further distinct approach of ‘‘strategic’’ (or ‘‘achieving’’).Various inventories were developed to measure approachesto learning, e.g., the Approaches to Studying Inventory (ASI)developed by Entwistle and McCune (Entwistle, 2006).
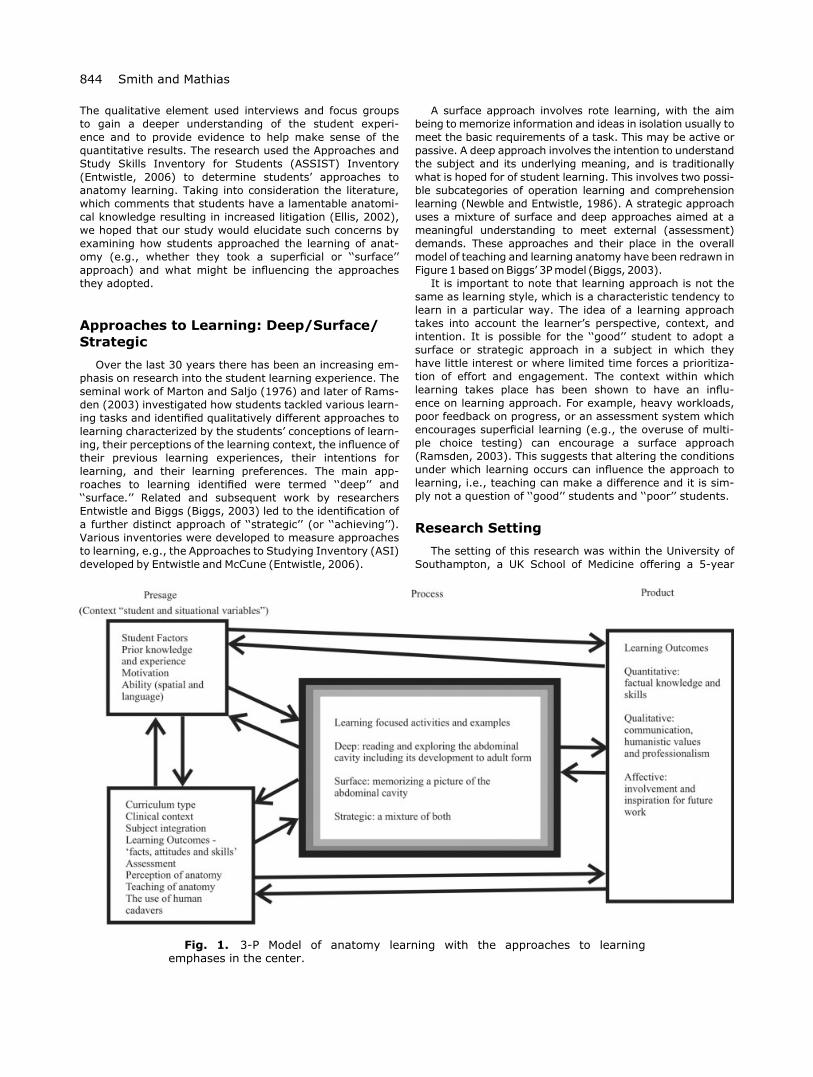
A surface approach involves rote learning, with the aimbeing to memorize information and ideas in isolation usually tomeet the basic requirements of a task. This may be active orpassive. A deep approach involves the intention to understandthe subject and its underlying meaning, and is traditionallywhat is hoped for of student learning. This involves two possi-ble subcategories of operation learning and comprehensionlearning (Newble and Entwistle, 1986). A strategic approachuses a mixture of surface and deep approaches aimed at ameaningful understanding to meet external (assessment)demands. These approaches and their place in the overallmodel of teaching and learning anatomy have been redrawn inFigure 1 based onBiggs’ 3Pmodel (Biggs, 2003).
It is important to note that learning approach is not thesame as learning style, which is a characteristic tendency tolearn in a particular way. The idea of a learning approachtakes into account the learner’s perspective, context, andintention. It is possible for the ‘‘good’’ student to adopt asurface or strategic approach in a subject in which theyhave little interest or where limited time forces a prioritiza-tion of effort and engagement. The context within whichlearning takes place has been shown to have an influ-ence on learning approach. For example, heavy workloads,poor feedback on progress, or an assessment system whichencourages superficial learning (e.g., the overuse of multi-ple choice testing) can encourage a surface approach(Ramsden, 2003). This suggests that altering the conditionsunder which learning occurs can influence the approach tolearning, i.e., teaching can make a difference and it is sim-ply not a question of ‘‘good’’ students and ‘‘poor’’ students.
Research Setting
The setting of this research was within the University ofSouthampton, a UK School of Medicine offering a 5-year
Fig. 1. 3-P Model of anatomy learning with the approaches to learningemphases in the center.
844 Smith and Mathias

systems-based undergraduate course. Students experienceanatomy through the study of prosected cadaveric materialin conjunction with lectures and tutorials in the early yearsand later in clinical situations and tutorials. Third year stu-dents have the opportunity to take a 10-week human dis-section module. Students are assessed using a variety ofwritten modes and semester-based ‘‘spotters’’ (practicalexaminations on specimens). All cohort years were includedin the study to allow for comparisons.
MATERIALS AND METHODS
In line with Central Office for Research Ethics Commit-tees Approval (05/Q1704/147), the 2005/06 cohort ofmedical students (all years) were all invited (n ¼ 996) toparticipate in an online questionnaire containing the ASSISTInventory that identified students’ approaches to learning.
The online inventory was written in Questionmark Per-ception (Version 4) and hosted by university servers. Theservers required students to log in with their universityidentity and password in order to prevent multiple entries.Students received e-mail and written mail inviting them totake part in the study by following the link at the end of thee-mail/letter. The invitations contained consent forms andparticipant information sheets. The inventory was accessi-ble to students for 1 month, and during that time theyreceived one reminder and a notice of closure. Data wereextracted from the servers and stored in accordance withthe Data Protection Act 1998.
The inventory took ~20 min for students to complete. Asan incentive, participants were entered into three prizedraws for book tokens. All students were also offered feed-back on the analysis of their individual scores; 10%responded and received a personal e-mail of their scoresand specific suggested study tips.
ASSIST Inventory
Consent was granted from the Enhancing Teaching andLearning Projects, University of Edinburgh, to use the in-ventory and the word ‘‘anatomy’’ was inserted as appropri-ate. The ASSIST Inventory (Entwistle, 2006) comprises 52statements (Table 1) to which the students respond byselecting the option with which they most agree on the Lik-ert Scale (5 ¼ agree, 4 ¼ agree somewhat, 3 ¼ unsure, 2 ¼disagree somewhat, 1 ¼ disagree). Responses were loggedand saved by the server.
RESULTS
The results were imported into the Statistical Packagefor the Social Sciences (SPSS, Version 14). The data werereviewed to remove incomplete inventory entries, resultingin a final sample of 243 (25% response) students. Itincluded 94 (38.7%) males and 149 (61.3%) females. Thiswas representative of the school’s gender ratio during2005/06 of 39% male and 61% female students. In com-paring the cohorts of the course, a good spread of partici-pants responded: Year 1 ¼ 60 (25%), Year 2 ¼ 50 (21%),Year 3 ¼ 48 (20%), Year 4 ¼ 57 (23%), and Year 5 ¼ 28(11%).
Following the analysis procedures accompanying theASSIST Inventory, subscores from the Likert Scale were
calculated for each student to give a score for each approach(deep, surface, strategic). The highest score reflected thedominant preference. Frequency testing showed that a deepapproach was preferred by 113 (46.5%) students closely fol-lowed by the strategic preference by 94 students (38.7%;Table 2).
Students’ preferences for approach to learning werethen compared. A paired t-test revealed that students pre-ferred using a deep approach over a strategic approach (P< 0.001) and a strategic approach over a surface approach(P < 0.001). When comparing deep and surface their pre-ferred approach was deep (P < 0.001)
One-way analysis of variance indicated that studentswere adopting an increasingly strategic approach to learninganatomy as they moved through their medical curriculum.There were three positive significant differences between thefollowing years: 1st and 3rd (P ¼ 0.038), 3rd and 4th (P ¼0.011), and 4th and 5th (P ¼ 0.036). In comparing gender, aKruskal Wallis test showed significant differences in the stra-tegic approach with females favoring it (P ¼ 0.021) and inthe deep approach with males favoring it. This result sup-ports earlier findings by Mattick et al. (2004).
Is There a Relationship BetweenApproach and Assessment Success?
Students’ anatomy examination results from their firstyear were compared with their individual approaches tolearning anatomy scores. Using Pearson product-momenttwo-tailed correlation coefficients, there was a significantresult with students who adopted a strategic approach per-forming better in examination (R ¼ 0.266 and P ¼ 0.001).As no significant correlations were found for students whoperformed poorly or failed, the researchers explored eachapproach in more detail. In students who adopted a surfaceapproach 8.6% failed compared to 2.9% and 6.6% of thosethat adopted strategic and deep approaches, respectively.
DISCUSSION
This was an exploratory study in an important areawhich has been relatively under-researched. The overallresponse rate of 25% appears relatively low (but, arguably,reasonable for this kind of study which relies on voluntaryparticipation), and it is accepted that the data may havebeen biased by those students choosing to participate.However, the response rates for each year were similar(except for year 5) and the statistical relationships foundwere quite strong to give us confidence that the resultswere reasonably indicative of the population as a whole.The tendency for students to adopt an increasingly strategicapproach to learning as they moved through the curriculumwas not unexpected, as they learned how to cope with theheavy course demands. It is also important to add thatthe study reported here forms one part of a wider study ofthe student experience and the views of stakeholders. Wehope to report on this broader study at a later date so thatthe results of the approaches to learning inventory can beplaced in a more meaningful context.
Anatomy learning is complex and multifaceted. Medicalcurricula have experienced considerable reductions in fac-tual content following the GMC recommendations (GeneralMedical Council, 2003), but in medicine, including anatomi-cal sciences, there is still a copious volume of subject mat-
845Students’ Approaches to Anatomy Learning
TABLE 1. Statements in the ASSIST Inventory Grouped According to the Approach (Entwistle, 2006)
Deep approachSeeking meaning4. I usually set out to understand for myself the meaning of what we have to learn in anatomy.17. When I’m reading an anatomy article or book, I try to find out for myself exactly what the author means.30. When I am reading I stop from time to time to reflect on what I am trying to learn from it.43. Before tackling a problem or assignment, I first try to work out what lies behind it.Relating ideas11. I try to relate anatomy ideas I come across to those in other topics or other courses whenever possible.21. When I’m working on a new topic, I try to see in my own mind how all the ideas fit together.33 Ideas in anatomy course books or articles often set me off on long chains of thought of my own.46. I like to play around with ideas of my own even if they do not get me very far.Use of evidence9 I look at the evidence carefully and try to reach my own conclusion about what I am studying.23. Often I find myself questioning things I hear in lectures or read in books.36. When I read, I examine the details carefully to see how they fit in with whatsis being said.49. It is important for me to be able to follow the argument, or to see the reason behind things.Interest in ideas (Related subscale)13. Regularly I find myself thinking about ideas from anatomy lectures when I am doing other things.26. I find that studying anatomy topics can be quite exciting at times.39. Some of the ideas I come across on the course I find really gripping.52. I sometimes get ‘‘hooked’’ on academic topics and feel I would like to keep on studying them.Strategic approachOrganized studying1. I manage to find conditions for studying which allow me to get on with my work easily.14. I think I am quite systematic and organized when it comes to revising for anatomy exams.27. I am good at following up some of the reading suggested by lecturers or tutors.40. I usually plan out my week’s work in advance, either on paper or in my head.Time management5. I organize my study time carefully to make the best use of it.18. I am pretty good at getting down to work whenever I need to.31. I work steadily through the term or semester, rather than leave it all until the last minute.44. I generally make good use of my time during the day.Alertness to assessment demands2. When working on an assignment, I am keeping in mind how best to impress the marker.15. I look carefully at tutors’ comments on course work to see how to get higher marks next time.28. I keep in mind who is going to mark an assignment and what they are likely to be looking for.41. I keep an eye open for what lecturers seem to think is important and concentrate on that.Achieving (Related subscale)10. It is important to me to feel that I am doing as well as I really can on the anatomy courses here.24. I feel that I am getting on well, and this helps me put more effort into the work.37. I put a lot of effort into studying because I am determined to do well.50. I do not find it at all difficult to motivate myself.Monitoring effectiveness (Related subscale)7. I go over the work I have done carefully to check the reasoning and that it makes sense.20 I think about what I want to get out of this anatomy course to keep my studying well focused.34. Before starting work on an anatomy assignment or exam question, I think first how best to tackle it.47. When I have finished a piece of work, I check it through to see if it really meets the requirements.Surface apathetic approachLack of purpose3. Often I find myself wondering whether the work I am doing in anatomy is really worthwhile.16. There is not much of the work in anatomy that I find interesting or relevant.29. When I look back, I sometimes wonder why I ever decided to come here.42. I am not really interested in this course, but I have to take it for other reasons.Unrelated memorizing6. I find I have to concentrate on just memorizing a good deal of what I have to learn.19. Much of what I am studying makes little sense: it is like unrelated bits and pieces.32. I am not really sure what is important in anatomy lectures, so I try to get down all I can.45. I often have trouble in making sense of the things I have to remember.Syllabus-boundness12. I tend to read very little beyond what is actually required to pass.25. I concentrate on learning just those bits of information I have to know to pass.38. I gear my studying closely to just what seems to be required for assignments and exams.51. I like to be told precisely what to do in essays or other assignments.Fear of failure (Related subscale)8. Often I feel I am drowning in the sheer amount of material we are having to cope with.22. I often worry about whether I will ever be able to cope with the work properly.35. I often seem to panic if I get behind with my work.48. Often I lie awake worrying about work I think I would not be able to do.
846 Smith and Mathias

ter to understand. Assessment is often at regular intervalsin the curriculum and calendar year. These factors influencestudents’ learning and the approaches they take. High loadsand certain forms of assessment may push students from adeep approach toward a strategic or surface approach. Thissuggests, as indicated in the literature, that context influen-ces approaches to learning and that our key challenge is tocreate conditions within the curriculum which counteractthese effects and encourage a deep approach to learning.
Anatomy is often perceived as the introduction to ‘‘real’’medicine and an important component in the initial processof socialization into professional practice. However, it is alsoperceived as involving the learning of a challenging rangeof knowledge, concepts, skills, and attitudes as part of theprofessional rite of passage which has to be reproduced forassessment. Arguably, the context of learning is one whichcould easily push students toward adopting a surfaceapproach. What has been encouraging from the results ofour research is that the majority of students have preferreda deep or strategic approach to their learning of anatomy,with the minority adopting a surface approach and who per-formed less well in assessments. This reflects positively onthe curriculum and the conditions it has created for inhibi-ting surface approaches, for example, the integrated natureof the courses and how they apply to clinical practicethrough components on Medicine in Practice in years 1 and2 and the Scientific Basis of Medicine in the later years.
If we look beyond the surface layer of knowledge andfacts often associated with anatomy, we can discern at leastfour important aspects of anatomy learning in the contextof medical education. The first is the learning and use of anew specialist language. The second is the conceptualiza-tion of what may be described as a five-dimensional experi-ence: the three-dimensional map of the human form(including variation) with the fourth and fifth dimensionsbeing growth/development and aging. The third factor isthe unique experience of human cadavers, and the effectsof this have been reported by many (Tschernig et al., 2000;Francis and Lewis, 2001; McGarvey et al., 2001; O’Carrollet al., 2002). The final factor is the integration and applica-tion of the knowledge as part of professional practice.These four aspects need to be strongly reflected in theanatomy curriculum if students are to see beyond the sim-ple acquisition of facts.
Students tend to view the curriculum in terms of assess-ment (Biggs, 2003), and assessment has a strong influenceon how they approach their learning. From her experienceof some 6 years of teaching and assessing students in anat-omy, one of the authors (Smith) has observed how thestrategic student uses anatomy activities to achieve. Whenthese students experience an anatomy task, they acutelyevaluate what they need to do. For example, the brachialplexus (a clinically important area in which the detail isassimilated in stages) involves students learning new termsmaybe with the aid of a mnemonic. Just this activity would
constitute a surface approach but, when adding a basic dia-gram and understanding the composition of the nerves andthe muscle groups they supply, a deep approach may beinvolved. The strategic learner will use a mix of the factsmentioned earlier, dependent on their perception of thegoal at that time. The strategic learner will be able at timesto identify information that is just detail and informationthat is essential for clinical use and understanding. In com-parison, the surface learner would have a limited under-standing (i.e., rely on memorization, for example, by study-ing atlas pictures) and would not be able to discriminatekey points essential to understanding. The deep learnerwould understand the theory and apply it to clinical prac-tice, forming a map of the body in their own mind. Theywould have a good and grounded understanding on whichthey can always draw. The deep approach in particular mayinvolve a few key aspects specific to anatomy learning onhuman cadavers. These features include how the studentsuse their spatial ability and touch-mediated perception toexplore specimens and form understanding.
The results of this study give us confidence that the ma-jority of students are not adopting surface approaches inanatomy which may in the future result in a lack of knowl-edge and an increase in litigation cases (Ellis, 2002). Pre-dominantly students are using a deep approach and holisti-cally experiencing the discipline and its application. Whetherthis is a feature of the particular curriculum under study or amore widespread finding has to be left to future research. Itseems clear, however, that curriculum design plays a crucialrole in creating the appropriate conditions for facilitating thekind of learning we wish to foster in our students. If studentsare adopting surface approaches, we should be asking whatis driving them toward this behavior rather than simply label-ing them as poor students. Inventories such as ASSIST canbe used as diagnostic tools to identify and monitor students’approaches to learning, and to understand the factors under-lying their approaches. We would argue that, more oftenthan not, surface approaches are encouraged by features ofthe curriculum design and the assessment regime ratherthan by the quality of the students. The curriculum is morethan a syllabus but rather a design for learning. This sug-gests that the future of anatomy education and the quality ofthe learning we wish to promote in our students is very muchin the hands of teachers and course designers.
ACKNOWLEDGMENTS
The authors thank Mrs J. Gray for her help in producingFigure 1.
REFERENCES
Biggs J. 2003. Teaching for Quality Learning at University. Bucking-ham: Open University Press.
Dinsmore CE, Daugherty S, Zeitz HJ. 1999. Teaching and learninggross anatomy: Dissection, prosection, or ‘‘both of the above?’’.Clin Anat 12:110–114.
Ellis H. 2001. Teaching in the dissecting room. Clin Anat 14:149–151.Ellis H. 2002. Medico-legal litigation and its links with surgical anat-
omy. Surgery 20;8:i–ii.Entwistle NJ. 2006. Approaches to study skills inventory for stu-
dents. Enhancing teaching and learning project. URL: http://www.ed.ac.uk/etl/publications.html#measurement [accessedOctober 2006].
TABLE 2. Learning Approach Preferences
Approach Frequency Percent
Deep 113 46.5Strategic 94 38.7Surface 34 14.0No preference 2 0.8Total 243 100.0
847Students’ Approaches to Anatomy Learning

Francis NR, Lewis W. 2001. What price dissection? Dissection liter-ally dissected. J Med Humanit 27:2–9.
Garg AX, Norman G, Sperotable L. 2001. How medical studentslearn spatial anatomy. Lancet 357:363–364.
General Medical Council. 2003. Tomorrow’s Doctors: Recommenda-tions on Undergraduate Medical Education. London: GeneralMedical Council Publications.
Granger NA. 2004. Dissection laboratory is vital to medical grossanatomy education. Anat Rec B New Anat 281:6–8.
Jones DG. 1997. Anatomy departments and anatomy education:Reflections and myths. Clin Anat 10:34–40.
Marks SC. 2000. The role of three-dimensional information in healthcare and medical education: The implications for anatomy anddissection. Clin Anat 13:448–452.
Marton F, Saljo R. 1976. On qualitative differences in learning: 1-Outcome and process. Brit J Education Psychol 46:4–11.
Mattick K, Dennis I, Bligh J. 2004. Approaches to learning andstudying in medical students: Validation of a revised inventoryand its relation to student characteristics and performance. MedEduc 38:535–543.
McGarvey MA, Farrell T, Conroy RM, Kandiah S, Monkhouse WS.2001. Dissection: A positive experience. Clin Anat 14:227–230.
McKeown PP, Heylings DJ, Stevenson M, McKelvey KJ, Nixon JR,McCluskey DR. 2003. The impact of curricular change on medicalstudents’ knowledge of anatomy. Med Educ 37:954–961.
Miller R. 2000. Approaches to learning spatial relationships in grossanatomy: Perspective from wider principles of learning. ClinAnat 13:439–443.
Moss K. 2001. Learner retention of anatomical information pre-sented in a digital two-dimensional format versus a digital three-dimensional format. J Biocommun 28:4–10.
Newble DI, Entwistle NJ. 1986. Learning styles and approaches:Implications for medical education. Med Educ 20:162–175.
Nnodim JO, Ohanaka EC, Osuji CU. 1996. A follow-up comparativestudy of two modes of learning human anatomy: By dissectionand from prosections. Clin Anat 9:258–262.
O’Carroll RE, Whiten S, Jackson D, Sinclair DW. 2002. Assessing theemotional impact of cadaver dissection on medical students.Med Educ 36:550–554.
Pawlina W, Lachman N. 2004. Dissection in learning and teachinggross anatomy: Rebuttal to McLachlan. Anat Rec B New Anat281:9–11.
Prince KJ, Scherpbier AJ, van Mameren H, Drukker J, van derVleuten CP. 2005. Do students have sufficient knowledge of clin-ical anatomy? Med Educ 39:326–332.
Ramsden P. 2003. Learning to Teach in Higher Education, 2nd Ed.London: Falmer Press.
Rochford K. 1985. Spatial learning disabilities and underachieve-ment among university anatomy students. Med Educ 19:13–26.
Skidmore JR. 1995. The case for prosection: Comment on R.L.MNewell’s paper. Clin Anat 8:128–130.
Topp KS. 2004. Prosection vs. dissection, the debate continues:Rebuttal to Granger. Anat Rec B New Anat 281:12–14.
Tschernig T, Schlaud M, Pabst R. 2000. Emotional reactions of med-ical students to dissecting human bodies: A conceptual approachand its evaluation. Anat Rec 261:11–13.
Utting M, Willan P. 1995. What future for dissection in courses ofhuman topographical anatomy in universities in the UK? ClinAnat 8:414–417.
Yeager VL. 1996. Learning gross anatomy: Dissection and prosec-tion. Clin Anat 9:57–59.
848 Smith and Mathias








![Apex: A Cadaveric Prosection...application. It has emerged as an appealing approach for the surgical treatment of basilar apex aneurysms [1, 10]. In a seminal cadaveric prosection](https://img.dokumen.tips/doc/110x75/5e670ade07ebf233ac00c510/apex-a-cadaveric-prosection-application-it-has-emerged-as-an-appealing-approach.jpg)