Embed Size (px)
Citation preview
Australian Journal of Ophthalmology. (198 I) , 9. pp. 255-261
Council Lecture
AN AUSTRALIAN CHOROIDAL MELANOMA SURVEY Factors affecting Survival following enucleation
c H GREER" FRACO FRCPA FRCP Pafhology Department, Royal Victorian €ye and Ear Hospital, Melbourne
c ~UCKLEY+ FRACO FRCS Pathology Department, Royal Victorian €ye and Ear Hospital, Melbourne.
J BUCKLEY" Ph.D BSc MBBS Department of Social & Community Medicine, University of Oxford
R RAMSAY' FRACO FRACS Pathology Department, Royal Victorian Eye and Ear Hospital, Melbourne.
J LA NAUZE' FRACO FRACS Pathology Department, Royal Victorian €ye and Ear Hospital, Melbourne
Abstract This study is based on a computer-assisted analysis of 484 enucleated malignant melanomas of the choroid from The Royal Victorian €ye & Ear Hospital, Melbourne. The following factors which might influence survival were analysed; the sex and age of the patient, the interval between presentation for medical opinion and enucleation, the size of the melanoma and its position in the eye, the cell type of the melanoma and the presence of extraocular extension.
From this analysis it was found that: 1) The overall 15-year relative survival rate following enucleation was 75%. 2) the survivat curve flattened out at six years after enucleation indicating relatively few melanoma-related deaths for the remainder of the 15-year period. 3) there was no increase in death rate at 2 years after enucleation. 4) considering only melanoma-related deaths, increasing age is a strongly depressing influence on survival after enucleation, the 15-year relative survival being 80% for those less than age 40 and only 30% for patients aged 70 and over. 5) submacular melanomas had a very good prognosis for patient survival due in part to their small size and benign cytology. 6) extension into a scleral emissary appeared to exert an unexpectedly depressing effect on prognosis. 7) as in other published series, small melanomas tended to have a good prognosis, and survival rates diminished with increasing size. 8) there was a possibility, to be fuffher explored, that ciliary body melanomas may over all have a worse prognosis than melanomas of the choroid.
Key terms. Choroidal melanoma; survival; enucleation
Firstly I would Lke to thank the Council of the College for inviting me to give the Council lecture
for 1980. This is a great honour of which I am deeply appreciative.
~~~~ ~
* Pathologist + Ophthalmologist * Epidemiologist Delivered by Dr C. H. Greer at the 12th Annual Scientific Congress of the Royal Australian College of Ophthalmologists, Christchurch, New Zealand, 30th October, 1980. Reprint requests: Dr C. Buckley, 8 I Collins Street, Melbourne. 3000
AN AUSTRALIAN CHOROIDAL MELANOMA SURVEY 255
Figiire I
TIWE WErJIsl
Figure 3
TIME IEbASI
Figure 4
---7
,om- I --
TI*E IVEAIUI
Figure 6
256 AUSTRALIAN JOURNAL OF OPHTHALMOLOGY
I i-1-
, ' I , -
CHOROIDAL MELANCMA - RELATIVE SURVIVAL RELATEO ro CELL TYPE
_ - _ IANXS. __ Y\*_ I
YI.ro I(cm,c -. . . ...
~~ rs / l *EL laD
TIME WEARS1
Figure 7
The subject of my lecture is "An Australian Choroidal Melanoma Survey" and in case anyone should think that we in Victoria are being presumptuous in choosing this title, I will explain how we came to do so.
In 1977 three registrars at The Royal Victorian Eye and Ear Hospital in Melbourne conceived the idea of a survey and follow-up of alI the cases of malignant melanoma of the uveal tract recorded in the files of the Department of Pathology at the Hospital from 1952 to 1977.
The three former registrars, now all Fellows of the College, are Christopher Buckley, Robert Ramsay and James La Nauze. I became involved because I had made the original histopathological examinations of 95% of the enucleated eyes.
All the clinical and pathological information about these cases, painstakingly gathered during the past three years mainly by Dr Ramsay has
{ TlUE IYEARSI
Figure 8
AN AUSTRALIAN CHOROIDAL MELANOMA SURVEY
TAHLE I
MELANOMAS OF CHOROID
DISTRIBUTION BY STATES
VICTOR I A 300
N S W 42
QU EENSLAND 86
SOUTH AUSTRALIA 14
WESTERN AUSTRALIA 12
TASMANIA 25
NORTHERN TERRITORY 1
NEWZEALAND 4
been subjected to a computer-assisted analysis of survival rates conducted by the 5th member of the group, Dr Jonathan Buckley, an epidemiologist in the Department of Social and Community Medicine at the University of Oxford. This survey has, therefore, been very much a team effort and I am privileged indeed to have this opportunity of reporting, on behalf of the group, some of the results which have emerged.
This report is confined to a consideration of choroidal melanomas. An analysis of ciliary body melanomas will form the subject of a subsequent
TABLE 2
DISTRIBUTION OF CASES BY CELL TYPE
Australian
Choroid
Spindle A Spindle B 35 Mixed 50 Epithelioid 6.5 Necrotic 5.5
'aul et al 1962
Choroid + CB
% 5
39 45
3 7
- Australian
Survey 1980
Ciliary Body
%
19 66 15
-
-
257
Position Number of Cases
Submacular 62 Ant. or Post. 159
Ant. and Post. 106
communication. With regard to iris melanomas, follow-up has been so unsatisfactory that they have been eliminated from consideration for the time being.
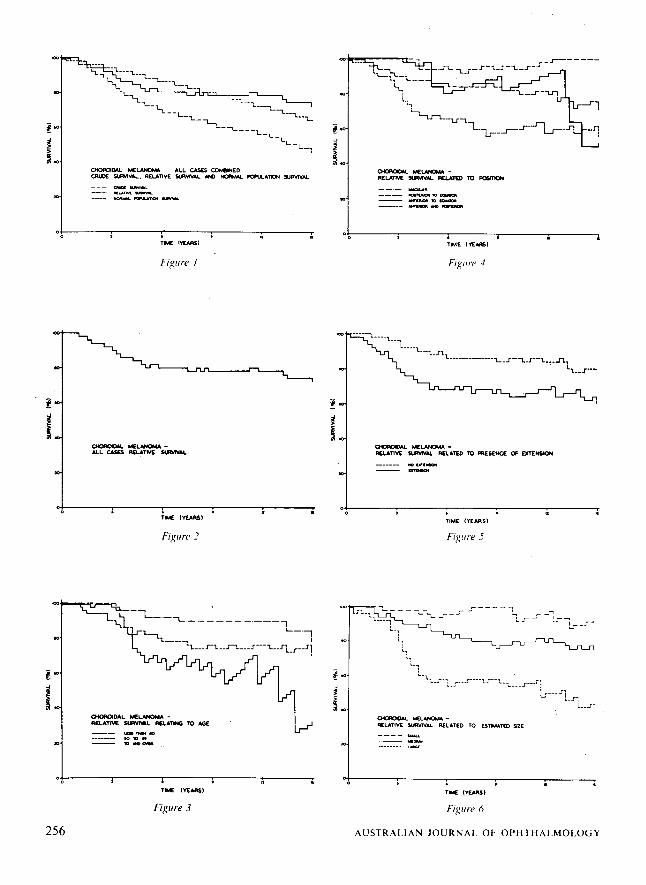
Data Collection Records of 484 malignant melanomas of the choroid were found in the files of my department for the years from 1952 - 1977. This total comprised not only cases from our Hospital but also enucleated eyes sent to me from ophthalmologists and pathologists in all the Australian states together with a small number from New Zealand (table 1).
This is the largest series of choroidal melanomas reported from Australia up to the present time.
In order to augment the often rather meagre clinical records, a questionnaire was devised and sent to all those from whom accessions had originated. The following information was sought concerning each case: 1) The time interval between presentation for
Position Small Medium Large
Su bmacular
Ant. or Post.
12-Y ear Relative
% Survival
98 86 *All figures in percentages. P < 0.0002 58
medical opinion and enucleation of the eye. 2) The nature of any investigations camed out
before the eye was enucleated e.g. fluorescein angiography or P32 uptake.
3) Most importantly, the present status of the patient in question; whether alive and well, or alive with metastases, or dead and, if so, was death known to be due to melanoma or to some other cause. I should like to take this opportunity of thanking
all those who took the trouble to answer our questionnaire and provide the information asked for. In those instances where it was not possible to obtain satisfactory replies by the above means, recourse was had to the State Cancer Registry or local medical practitioners. In very exceptional cases an inquuy was addressed to the patients themselves, or their relatives. Altogether it has been possible to follow up 78% of the 484 patients.
From the histopathological reports the following factors were extracted for each melanoma: (1) Position in the eye.
Extension Number Of Cases
Absent 200
Present 125
-~ Diameter in mm x Elevation in mm 12-Year Position
Relative % Survival
85 Submacular
66
TII~I I- 7
Cell Type
Spindle A Spindle B Mixed & Necrotic
Epithelioid
CORRELATION BETWEEN POSITION &CELL TYPE
Position
Submacular Anterior Posterior AntlPost
5(50%) 1 3 1 32125%) 10 54 31
29(15%) 20 74 74
1(4.5%) 2 7 11
CellType
Spindle A Spindle B Mixed & Necrotic
Epithelioid
TAIII.I 8
9 2 0 21 -40 41 - 6 0 61 -80 > 100
8 2 0 0 0 37 34 15 38 17
21 48 47 65 69
1 4 5 10 10
~
CORRELATION BETWEEN CELL TYPE A N D MEASURED SIZE
SURVIVAL
Unknown Known
Information Incomplete
~~ ~
ESTIMATED SIZE
SMALL MEDIUM LARGE
17 40 26 18 41 27
16 42 25
'
TAIII.': 9
Whether anterior or posterior to the equator of the globe or both. Among the posteriorly located growths. submacular melanomas were classified separately.
This was given special attention. Both the diameter and the elevation of each growth were measured on sections through the melanoma where it was at its maximum size.
(3) The presence or absence of tumour extension. Extension outside the globe was charted separately from extension which appeared to be confined to an underlying scleral emissary.
The melanomas were typed according to the Callender classification which, despite its many shortcomings, still has its uses. The distribution of cell types in the present series is seen in table 2.
You will see that I have retained the category of spindle A cell melanoma for a small number of tumours in this series. This is worth mentioning because in 1978 McLean, Zimmerman and Evans' in reviewing 105 spindle A cell melanomas in the files of the Armed Forces Institute of Pathology reclassified all of them either as uveal naevi or as melanomas of spindle B or mixed cell type. One might, therefore, gain the impression that spindle A cell melanomas no longer exist, but this has not been my experience. The spindle A cell melanomas in our series are neither choroidal naevi, as I understand the term. nor do they belong in any other category.
The percentages of each type of melanoma in our series show a fair degree of correspondence with those in the mammoth series of 2652 melanomas of the choroid and ciliary body reported from the Armed Forces Institute of Pathology by Paul, Parnell and Franker,' except that we have relatively twice as many epithelioid melanomas.
I would direct attention to the third column of the table which shows that the incidence of more malignant cell types is much higher in our ciliary body melanomas than in our choroidal melanomas. This, and the fact that ciliary body melanomas tend to be large. suggest that they may have a worse prognosis than choroidal melanomas.
259
(2) The size of the melanoma.
(4) Cell type.

For this reason we decided that they should be studied separately.
In summary, therefore, the following factors which might have relevance to survival were analysed: 1. Sex and age of the patient. 2. The interval between presentation for medical
opinion and enucleation of the eye. 3. Position of the melanoma in the eye. 4. Size of the melanoma. 5. The presence of intrascleral and/or extrascleral
6. The cell type of the melanoma. extension.
Statistical analysis A detailed exposition of the theoretical basis of the statistical method used in this survey is beyond the scope of this lecture. However, some explanation of the analytical procedure is necessary. The basic implements of our survey were relative survival cures3 and the reason we used these was to ensure with a high degree of certainty that only deaths due to melanoma were being considered.
(1) First, actuarial crude survival curves for our melanoma patients were plotted using the method of Cutler and Ederer.4 These were based on deaths among the melanoma patients from any cause whatsoever. These crude survival curves by themselves were of little value and had to be adjusted to take account of deaths unrelated to melanoma.
(2) In order to do this, the crude survival curves were adjusted for expected survival in the normal Australian population. The figures necessary for these adjustments were obtained from the Year Book of Australia for 1978.’ In this adjustment our melanoma patients were exactly matched for sex, age and calendar year with persons in the normal population.
(3) The end result of this statistical method was relative survival curves for our melanoma patients. These curves are purged, as it were, of the influence of deaths due to causes other than melanoma. The use of relative survival curves thus ensured with a high degree of certainty that deaths which we were analysing among our melanoma patients were in fact due to melanoma. Survival curves were compared by the logrank method.6
260
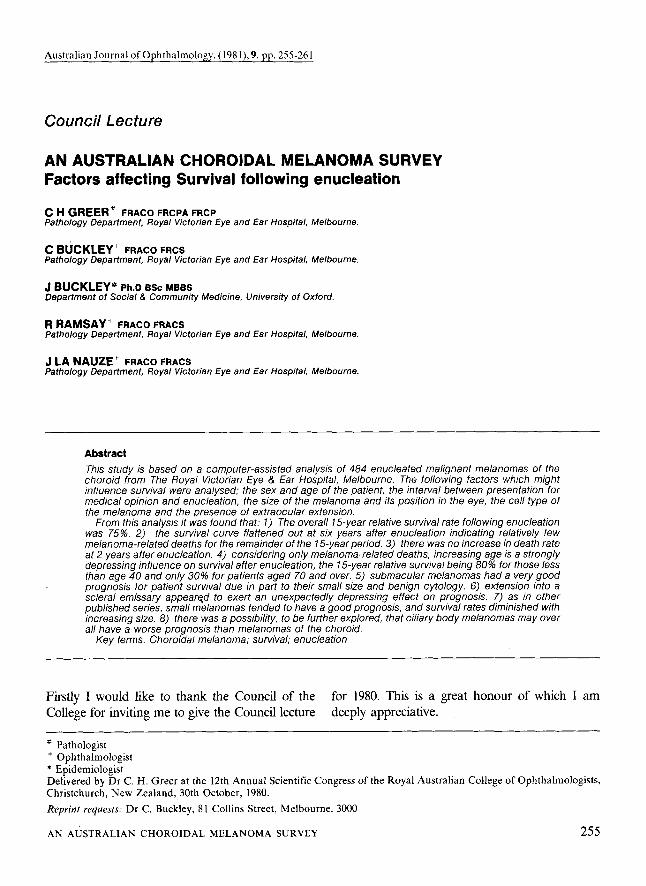
(4) Unlike actuarial survival curves, which when plotted, decline steadily with the passage of time, relative survival curves may fluctuate. This is because the points on the curve represent the difference between the crude survival and expected survival curves. When the latter two converge, the relative survival curve rises and. conversely, when they diverge the relative survival curve falls. In the event that the two basic curves run parallel (i.e. constant difference) the relative survival curve levels off as is seen in Figure 1.
Results The overall relative survival rate for all the choroidal melanomas in this series irrespective of size, position, extrascleral extension, cell type or any other factor is 75%. (Figure 2).
We were hoping to determine whether or not leaving melanomas untreated for long periods of time greatly influenced survival rates. We found that there was no statistically significant relationship between survival and the time interval between presentation and enucleation. Neither was there any significant relationship between the sex of the patient and survival.
Age and relative survival As would be expected, crude survival of melanoma patients decreases steadily with increasing age of the patient at the time of enucleation. If one removes the obvious influence of age-related deaths due to other causes, there persists a strong trend towards shortened survival with increasing age, and this due solely to the melanoma. (Figure 3). The relative survival curve shows that the 15 years survival is 30% for patients 70 years of age or more at the time of enucleation, and 80% for patients aged less than 40 years.
Position and relative survival Relative survival related to the position of the
melanoma in the globe is shown. in Figure 4, from which we see that the prognosis for submacular melanomas is extremely good and considerably better than that for melanomas located elsewhere in the eye. As will presently appear, small size and benign cell type are among factors responsible for this favourable outcome. The correlation between
AUSTRALIAN J O U R N A L OF OPHTHALMOLOGY
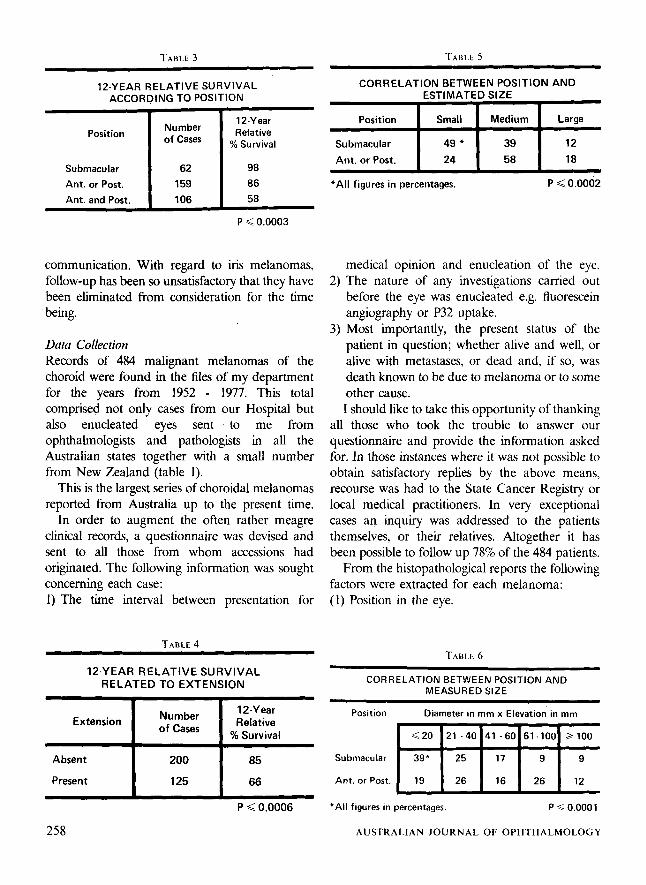
position and 12-year relative survival is presented in table 3.
Extension and relative survival As might be expected when extension was plotted against no extension, extension was seen to influence survival unfavourably (Figure 5) . Extension here included not only extrascleral extension but also intrascleral extension into an underlying scleral emissary. Correlation between extension and relative survival is shown in table 4. The following points of interest have emerged.
(1'). The relative survival curve for extrascleral extension alone (not shown) was found to be almost identical to the curve shown in Figure 5 for extrascleral and intrascleral extension combined. This suggests that intrascleral extension by itself has an unexpectedly depressing influence on survival.
(2) Even when extension had occurred there were very few tumour-related deaths later than six years after enucleation.
Estimated size and relative survival Estimated size is the size of the melanoma as judged by naked eye inspection of the opened enucleated globe. The relationship between estimated size and relative survival is shown in Figure 6.
Relative survival percentages at 15 years after enucleation for the three categories of melanomas are -
Small 97% Medium 70% Large 42%
It seems probable that an equally valid and prognostically significant estimate of size could be made ophthalmoscopically. The correlation between position and estimated size as set out in table 5 shows that almost half the submacular melanomas are small, while very few are large. On the other hand for melanomas located either anterior or posterior to the equator of the globe more than half are of medium size while only one quarter are small.
Measured size and relutive survival In order to make more precise the foregoing
correlation between size and survival, measured size was substituted for estimated size and the result is seen in Figure 7. Measured size in this context is the product of maximum diameter in mm times maximum elevation in mm. This of course is not a measurement of either volume or area, but is a useful, if somewhat artificial, index of size. The curves in Figure 7 show that melanomas with an index less than 20 have a 97% relative survival at 15 years, while those with an index over 100 have a 15 year survival of 53%. The hatched area, representing melanomas with an index between 21 and 100, have an average survival rate intermediate in value at 74%.
Correlation between position and measured b e is shown in table 6 from which it will be seen that 39% of submacular melanomas are less than 20 on this scale of measurement, while only 18% gave an index of more than 60. This contrasts with melanomas located either anteriorly or posteriorly in the globe which show a strong tendency to be larger since only 19% have an index of less than 20. Size, therefore, appears to be an important factor in the good prognosis of submacular melanomas.
Cell. type and relative survival The outcome according to cell type in our series (Figure 8) is in fair agreement with that derived from actuarial survival curves, except that our patients with mixed cell melanomas show a considerably better 12-year and 15-year survival.
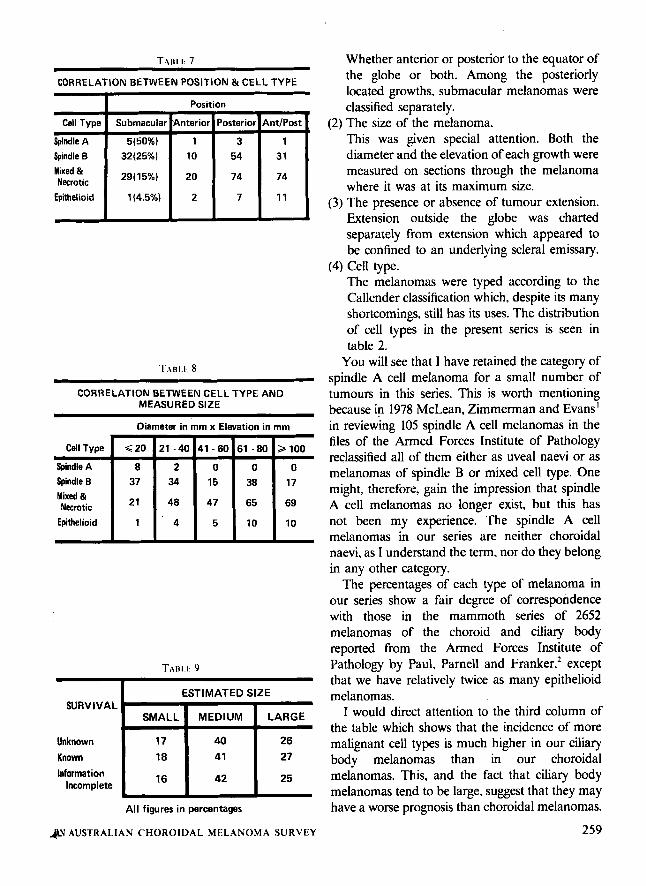
Correlation between cell type and position in the eye is shown in table 7, which reveals another possible factor in the good prognosis of submacular melanomas, in that 75% of them are of the less malignant spindle cell types. Table 8 which shows the correlation between cell type and the measured size as previously defined, reveals that all spindle A cell melanomas in this series are small while most epithelioid cell melanomas are large. In the case of spindle B cell melanomas, more are small than large while in the mixed cell and necrotic groups, more are large than small.
Completeness Finally, can we say anything about the survival of patients in this series who, for one 'reason or another, we have been unable to follow up or
A N AUSTRALIAN CHOROIDAL MELANOMA SURVEY 26 1

whose follow up data is incomplete? Do the foregoing conclusions, based on patients adequately followed up, apply to those whose fate is not known with certainty? Were these latter cases atypical in some way related to survival? It is important to know this because if they were, our relative survival curves and the conclusions based on them may be biased.
As a check on this possibility we have compared cases in which survival rates are known with those in which survival rates are either unknown or the data is incomplete. Table 9, relating these three patient categories to estimated tuniour size, will make the position clear.
From this table we see that cases with incomplete or unknown survival information, occur in almost identical proportions to those cases whose survival is known. Similar tabulations have been made for other prognostic factors such as the patient’s age, the presence of intrascleral and extrascleral extension and the cellular constitution of the melanomas. Close concordance has been found between the three patient categories relative to all the prognostic factors studied. We have therefore felt justified in concluding that patients without adequate follow up would have shown the same survival tendencies as those demonstrated by patients with complete follow up information.
ACKNOWLEDGEMENTS We wish especially to thank Mrs D. Marshall who acted throughout as co-ordinating secretary to the project. We are also much indebted to Miss M. Cox and her staff in the Medical Records Department at The Royal Victorian Eye and Ear Hospital and Miss A. Dodds and her staff a the Melbourne Cancer Registry. Our thanks are also due to Mrs J. Buckley for skdled assistance in drawing up our graphs, to the Medical Illustration Department of The Royal Victorian Eye and Ear Hospital for preparing the figures and tables for publication and to Mrs. E. Hendrie and Miss F. Ritchie for typing the manuscript. The work was supported by a Royal Victorian Eye and Ear Hospital Grant No. 32.
References I . McLean IW, Zimmerman LE, Evans RM. Reappraisal
of Callender’s Suindle A t w e of malignant melanoma of‘ Choroid and diliary bob;. Am J 5phthalmol 1978: 86:557.
2. Paul EV, Parnell BL, Fraker M. Prognosis of malignant melanomas of the Choroid and Ciliary body. Int Ophthalmol Clin. Boston, Little Brown & Co 1961:387
3 . Berkson J, Gage RP. Calculation of survival rates for cancer. Proc Staff Meetings Mayo Clinic 1950; 25:270.
4. Cutler SJ, Ederer BS. Maximum utilization of life table method in analysing survival. J Chron Dis 1958; 8:699.
5. Year Book Australia. Australian Bureau of Statistics. Canberra. 1978.
6 . Peto R, Peto J. Asymptotically efficient rank invariant test procedures. J R Statist SOC A 1972; 135:185.
262 AUSTRALIAN JOURNAL OF OPHTHALMOLOGY











![Successful carbon-ion radiotherapy for choroidal melanoma ... › pdf › NFO-3-158.pdf · Choroidal melanoma is a rare but life-threatening intraocular malignant tumor [1]. Local](https://img.dokumen.tips/doc/110x75/5ed9830c1b54311e7967b2a8/successful-carbon-ion-radiotherapy-for-choroidal-melanoma-a-pdf-a-nfo-3-158pdf.jpg)
![OPEN ACCESS Case Report Congenital Choroidal Nevus in a ...choroidal nevus) [10]; likewise, the nevus is characterized by having a high internal reflectivity, unlike the melanoma that](https://img.dokumen.tips/doc/110x75/5ea21f6a6c088018070115eb/open-access-case-report-congenital-choroidal-nevus-in-a-choroidal-nevus-10.jpg)

![Ophthalmology Update - Cleveland Clinicchoroidal nevi prevalence and choroidal melanoma incidence. The results, published in Ophthalmol-ogy [Singh AD, et al. Ophthalmology 2005;112:1784-89],](https://img.dokumen.tips/doc/110x75/5ed991a01b54311e7967ce4b/ophthalmology-update-cleveland-clinic-choroidal-nevi-prevalence-and-choroidal.jpg)