Embed Size (px)
Citation preview
An Analysis of Breast Cancer Surgery afterFree Transverse Rectus Abdominis
Myocutaneous (TRAM) Flap ReconstructionAlison C. Ross, MD, Montreal, Quebec, Conrad H. Rusnak, MD, Mark K. Hill, MD, J. David Naysmith, MD,
Sandra L.Taylor, MD, William E. Dunlop, MD, Allan H. Hayashi, MD, Victoria, British Columbia
BACKGROUND: Breast reconstruction is currentlyoffered on a more routine basis to patients aftermastectomy for breast cancer. This paper ana-lyzes the outcomes of breast cancer surgery,and the results and effects of breast reconstruc-tion using free TRAM flaps.
METHODS: A retrospective review of 75 consecu-tive patients who had free transverse rectus ab-dominis myocutaneous (TRAM) flap breast re-construction after breast cancer surgery wasperformed. A total of 92 free TRAM flaps wereperformed on 75 patients in Victoria, British Co-lumbia, from January 1992 to May 1999. Thirty-three patients (44%) underwent primary breastcancer surgery and an immediate reconstruction(7 bilateral and 27 unilateral) and 42 patients(56%) had delayed reconstruction (10 bilateraland 32 unilateral).
RESULTS: Twenty- one patients (28%) had stage 0disease, 20 (26.7%) had stage I disease, 17(22.7%) had stage IIA disease, 12 (15%) hadstage IIB disease, and 4 (5.3%) had stage IIIAdisease. In 1 patient the stage of disease wasunknown. The mean patient age was 49.4 years(range 33 to 73). Of the patients undergoing im-mediate reconstruction 3 had postoperative che-motherapy and 1 had postoperative radiotherapy.Three patients had combined chemoradiother-apy. In none of these cases was the adjuvanttherapy delayed by the reconstructive surgery.Overall mean follow-up time from cancer diagno-sis was 56.8 months and from the time of TRAMflap reconstruction, 36.7 months. To date, 5 re-currences have been detected (6.6%). Mean timebetween reconstruction and detection of recur-rence was 22.8 months. Detection of recurrence
was achieved clinically and was not impaired inany of the cases by the presence of the free flap.Patient satisfaction was assessed via a tele-phone survey, with 93% of patients pleased withthe cosmetic results of their surgery.
CONCLUSIONS: For those patients with breast can-cer requiring mastectomy, free TRAM flap recon-struction is a safe, cosmetically acceptable sur-gical alternative that impairs neither effectivebreast cancer surgery nor detection of recurrentdisease. Am J Surg. 2000;179:412–416. © 2000by Excerpta Medica, Inc.
Although the trend in the treatment of breast canceris toward breast conservation surgery followed byradiotherapy, mastectomy remains the treatment
of choice for many women. Breast reconstruction is cur-rently offered on a more consistent basis to patients requir-ing mastectomy for breast cancer. In those patients requir-ing mastectomy, reconstruction enables the patient toundergo restoration, or preservation, of body form andimage depending on whether the reconstruction is delayedor immediate.1 The literature is replete with reports doc-umenting the psychological benefits of breast reconstruc-tion, particularly that done immediately.2–6
Historically, there was concern raised that immediatebreast reconstruction may compromise not only the effec-tiveness of the cancer surgery, but also that it may impairdetection of local recurrences. However, those concernswere unfounded in patients reconstructed with im-plants.2,7,8 As reconstruction evolved with techniques suchas autologous tissue flaps and skin-sparing mastectomy, thechallenge to ensure continued safety and efficacy has beenaddressed by several groups. Slavin et al1 found that im-mediate breast reconstruction with myocutaneous flaps didnot effect the detection and treatment of local recurrencesof breast cancer. In addition, Kroll et al9,10 and Single-tary11 reported no increased risk of local recurrence inthose early breast cancer patients treated with skin sparingmastectomy and immediate breast reconstruction.
The technique of using autologous tissue in the form of atransverse rectus abdominis myocutaneous (TRAM) flapwas first described in 1981 by Scheflan and Hartrampf.12
The TRAM flap has since become the most commonsource of autogenous tissue for breast reconstruction.13,14
The flap can be performed either as a free tissue transfer oras a pedicled flap. This technique has become more widelyaccepted by patients, surgeons, and oncologists given therecent literature regarding its oncologic safety1,10 as well asits esthetic benefits.1,4,5 The TRAM flap provides tissue
From the Department of General Surgery (ACR), McGill Univer-sity, Montreal, Quebec, Canada, and the Department of SurgicalServices (CHR, MKH, JDN, SLT, WED, AHH), Capital HealthRegion, Victoria, British Columbia, Canada.
Requests for reprints should be addressed to Conrad H. Rus-nak, MD, Division of General Surgery, 302-2020 Richmond Ave-nue, Victoria, British Columbia V8R 6R5, Canada.
Manuscript submitted January 20, 2000, and accepted in re-vised form March 10, 2000.
Presented at the 86th Annual Meeting of the North PacificSurgical Association, Vancouver, British Columbia, Canada, No-vember 12–13, 1999.
412 © 2000 by Excerpta Medica, Inc. 0002-9610/00/$–see front matterAll rights reserved. PII S0002-9610(00)00357-3

bulk that is similar in consistency to breast parenchyma,giving a more normal-appearing breast mound and con-tour. Advantages of the free TRAM technique include amore limited disruption of the rectus muscle, which mayminimize postoperative abdominal wall weakness and spar-ing of the inframammary crease by avoiding the tunnelingrequired in a pedicled flap.15 Another major advantage ofTRAM flaps is their use in patients who have failed breast-conserving surgery with radiotherapy. These patients willrequire salvage mastectomy in a previously irradiated re-gion, and autologous free tissue based on the larger deepinferior epigastric vessels provides a better blood supply tothe region.1
This study was done in order to analyze the results ofbreast cancer surgery in those patients who underwentbreast reconstruction using free TRAM flaps, as well as theresults of the reconstruction itself.
METHODSFrom January 1992 to May 1999, 75 patients with carci-
noma of the breast underwent free TRAM flap reconstruc-tion in Victoria, British Columbia. These patients werereviewed retrospectively. Thirty-three patients (44%) un-derwent primary breast cancer surgery with immediate re-construction (7 bilateral and 26 unilateral) and 42 patients(56%) had delayed reconstruction (11 bilateral and 31unilateral). Eight patients underwent salvage mastectomyfollowing biopsy proven failure of breast conserving sur-gery. All patients were reconstructed using a two-teamapproach.
The type of mastectomy performed is determined bymany factors, including previous biopsy results, invasion,multicentricity, size of tumor, family history, and patientpreference. An appropriate mastectomy (and axillary nodedissection if required) is performed using a skin-sparing, orperiareolar technique, where possible. The general andplastic surgeons discuss the planned incisions prior to thecase. At no time is the adequacy of cancer surgery com-promised for cosmetic benefit. A skin-sparing techniqueinvolves a circumareolar incision, which is extended later-ally. Where present, the majority of biopsy sites are re-moved with an appropriate ellipse of skin.
While the mastectomy is being performed, a second teambegins the flap harvest which starts with an elliptical inci-sion of the abdominal wall. The deep inferior epigastricvessels are identified and dissected distally to their pene-tration on the deep surface of the rectus abdominis. Afterthis, a window of rectus muscle is resected that includes theaccompanying blood supply. This technique allows forboth a medial and a lateral column of muscle to be leftrelatively undisturbed, which may improve the patient’sabdominal wall strength postoperatively. The deep inferiorepigastric vessels are then dissected proximally to theirjunction with the external iliac vessels, in order to createthe longest possible pedicle.
In all cases a two-team approach is employed, with sep-arate instruments and nursing staff. In those cases recon-structed in a delayed fashion, the initial time is used toopen the axilla and dissect out the recipient thoracodorsalvessels.
Once the axilla or chest wall and donor flap are ade-quately prepared, the flap is moved up to the chest wall;
and the anastomosis of the deep inferior epigastric vesselsto the thoracodorsal vessels is performed with either a 9-0prolene suture or a 3M microanastomotic device of appro-priate caliber.
Further moulding and contouring of the new breastmound follows, with care to achieve a symmetric andesthetic result. The abdominal wall closure is performedsimultaneously by reapproximating the fascia and then theskin with repositioning of the umbilicus. In cases wherethere is significant tension on the abdominal wall, a mer-silene mesh is used for reinforcement. Nipple-areolar re-construction can be performed either at the time of recon-struction or in a delayed fashion.
All patients are transferred to a specialized unit postop-eratively, for monitoring and 1-to-1 nursing care. Standardmonitoring techniques include routine fluorescene injec-tions followed by vascular flow determination for a periodof 5 days. Laser dopplers are also used periodically to assessvascular patency within the flap vessels and anastomosis.The flaps are routinely assessed for color and temperaturein order to detect vascular insufficiency. Patients are mo-bilized on the second postoperative day. Standard medica-tions include chlorpromazine, 10 mg, QID for 5 days; dex-tran 40, 100 mg bolus followed by an infusion of 25 cc/hourfor 5 days; and ASA 325 mg QD for 3 months.
After discharge, patients are followed up routinely byboth the general surgeon and the plastic surgeon, as well asby the oncology department at the British Columbia Can-cer Agency.
Suspicious lesions were detected by the above physiciansby physical examination and mammography, and wereroutinely biopsied by the general surgeon. Further treat-ment for locoregional recurrences and/or distant metastaseswas multidisciplinary with surgical resection, chemother-apy and radiotherapy all being employed.
RESULTSThe mean patient age was 49.4 years, with a range from
33 to 73 years. Tumor histopathology showed the followingdistribution: ductal carcinoma 83%, lobular carcinoma 9%,mixed 5%, and 3% unknown. There were no patients withinflammatory carcinoma. Analysis of the pathologic stage,using the American Joint Committee on Cancer TNMstaging system, is shown in Table I. Of the patients withstage I disease, 20 (27%) were T1N0. The patients withstage IIA disease consisted of 10 (13%) with T2N0 and 7(9%) with T1N1. Of the patients with stage IIB disease, 12
TABLE IStage of Disease
Stage*No. of
Patients
0 21 (28%)I 20 (27%)IIA 17 (23%)IIB 12 (16%)IIIA 4 (5.0%)Unknown 1 (1.0%)
* American Joint Committee on Cancer staging.
ANALYSIS OF BREAST CANCER SURGERY AFTER TRAM RECONSTRUCTION/ROSS ET AL
THE AMERICAN JOURNAL OF SURGERY® VOLUME 179 MAY 2000 413
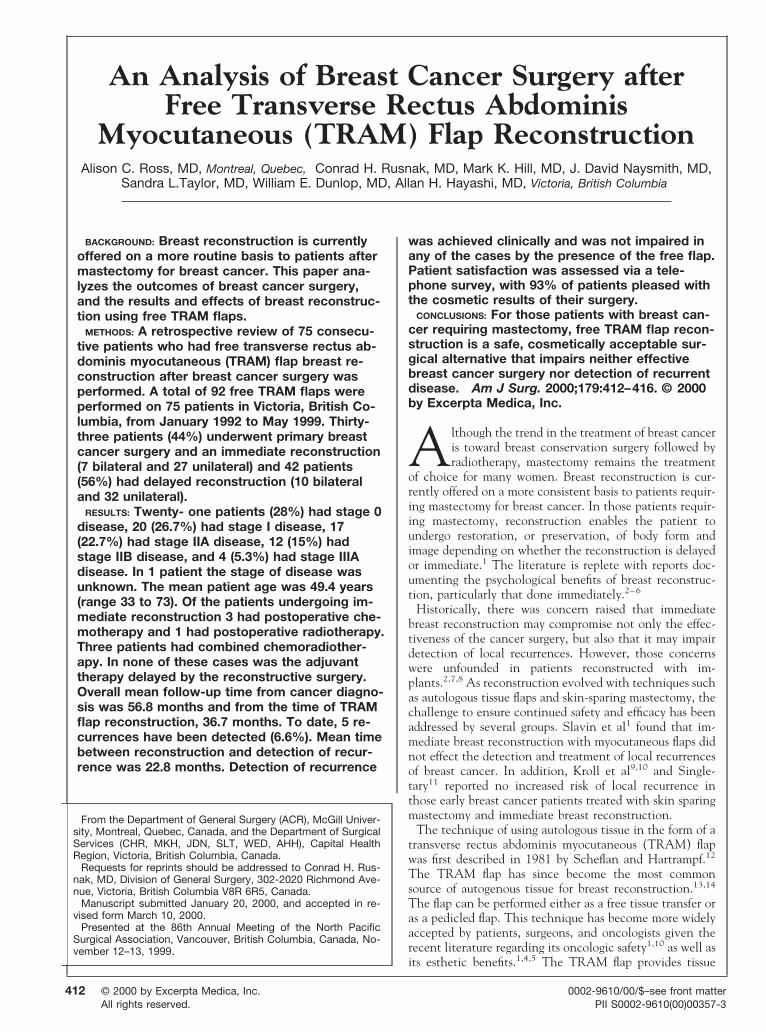
(16%) were T2N1. Of the patients with stage IIIA disease,4 (5%) were T3N1. The types of mastectomy performedare shown in the Figure. The majority of patients under-went modified radical mastectomy (MRM). The patientwith the subcutaneous mastectomy had moderate atypicalhyperplasia and a positive family history. The patient listedas “other” had an unknown type of mastectomy.
Operative time was assessed. Overall mean operative timefor a unilateral free TRAM was 5 hour and 15 minutes andthat for a bilateral free TRAM was 8 hours and 27 minutes.However, there has been a considerable reduction in thetime required for unilateral flaps likely due to the learningcurve as well as to technical advances with the 3M anas-tomotic device. The mean time required for the last 10unilateral cases has been 4 hours and 28 minutes.
Mean length of hospital stay was 9.1 days with a range of7 to 16 days. The patients were followed up postoperativelyfor a period ranging from 2 to 89 months. The mean timeof follow-up was 36.7 months.
Locoregional recurrence or metastatic disease was identi-fied postoperatively in 5 of 75 patients (6.7%). The averagetime to diagnosis of any recurrence was 22.8 months. Ofthose patients who had locoregional recurrence only, av-erage time to diagnosis of recurrence was 24 months.
Four of the 5 patients with recurrences were treated withsalvage mastectomy. All recurrences were detected clini-cally and confirmed by biopsy and appropriate imagingtechniques. All local recurrences in this series presented asa nodularity or thickening of the scar between the nativeskin and the flap skin, and were easily detected by clinicalexamination.
Of the 5 patients with recurrences, 3 are currently alive.Two patients died of progressive metastatic disease at 17and 72 months postoperatively. One patient is currentlyalive, 75 months postoperatively, but is receiving palliativetreatment for progressive metastatic disease. Two patientsare alive at 36 months postoperatively; 1 is well and 1 hasrecently been found to have metastatic disease to the liver.
There were no full flap losses. There were 2 abdominalwall hernias, which were subsequently repaired. Partial flaploss and donor site infection occurred in 1 patient each. Fatnecrosis occurred in 2 patients, 1 of whom had a pulmonaryembolus. Superficial skin necrosis of the mastectomy flapoccurred in 5 patients. Only 3 of these patients requiredtherapy for the skin necrosis in the form of a split thicknessskin graft. One patient had a mucus plug requiring reintu-bation, and 1 patient had a pressure sore on the forehead.Overall complication rate was 17%; however, only 13%
required additional treatment that either prolonged hospi-tal stay or required an additional hospital admission.
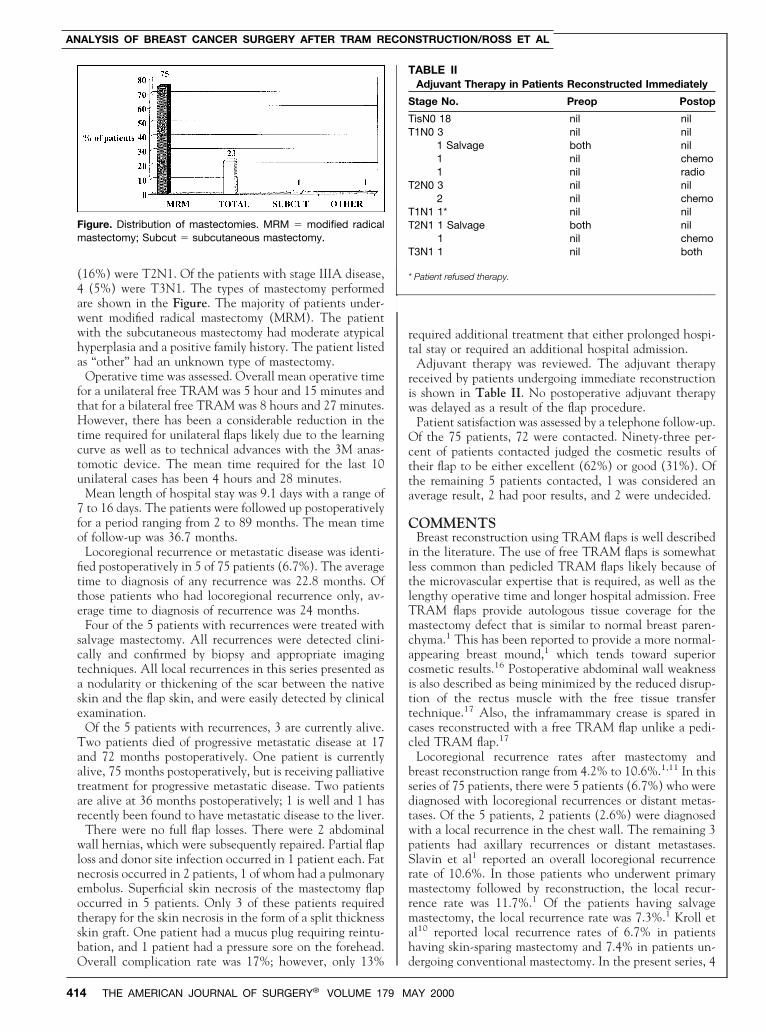
Adjuvant therapy was reviewed. The adjuvant therapyreceived by patients undergoing immediate reconstructionis shown in Table II. No postoperative adjuvant therapywas delayed as a result of the flap procedure.
Patient satisfaction was assessed by a telephone follow-up.Of the 75 patients, 72 were contacted. Ninety-three per-cent of patients contacted judged the cosmetic results oftheir flap to be either excellent (62%) or good (31%). Ofthe remaining 5 patients contacted, 1 was considered anaverage result, 2 had poor results, and 2 were undecided.
COMMENTSBreast reconstruction using TRAM flaps is well described
in the literature. The use of free TRAM flaps is somewhatless common than pedicled TRAM flaps likely because ofthe microvascular expertise that is required, as well as thelengthy operative time and longer hospital admission. FreeTRAM flaps provide autologous tissue coverage for themastectomy defect that is similar to normal breast paren-chyma.1 This has been reported to provide a more normal-appearing breast mound,1 which tends toward superiorcosmetic results.16 Postoperative abdominal wall weaknessis also described as being minimized by the reduced disrup-tion of the rectus muscle with the free tissue transfertechnique.17 Also, the inframammary crease is spared incases reconstructed with a free TRAM flap unlike a pedi-cled TRAM flap.17
Locoregional recurrence rates after mastectomy andbreast reconstruction range from 4.2% to 10.6%.1,11 In thisseries of 75 patients, there were 5 patients (6.7%) who werediagnosed with locoregional recurrences or distant metas-tases. Of the 5 patients, 2 patients (2.6%) were diagnosedwith a local recurrence in the chest wall. The remaining 3patients had axillary recurrences or distant metastases.Slavin et al1 reported an overall locoregional recurrencerate of 10.6%. In those patients who underwent primarymastectomy followed by reconstruction, the local recur-rence rate was 11.7%.1 Of the patients having salvagemastectomy, the local recurrence rate was 7.3%.1 Kroll etal10 reported local recurrence rates of 6.7% in patientshaving skin-sparing mastectomy and 7.4% in patients un-dergoing conventional mastectomy. In the present series, 4
Figure. Distribution of mastectomies. MRM 5 modified radicalmastectomy; Subcut 5 subcutaneous mastectomy.
TABLE IIAdjuvant Therapy in Patients Reconstructed Immediately
Stage No. Preop Postop
TisN0 18 nil nilT1N0 3 nil nil
1 Salvage both nil1 nil chemo1 nil radio
T2N0 3 nil nil2 nil chemo
T1N1 1* nil nilT2N1 1 Salvage both nil
1 nil chemoT3N1 1 nil both
* Patient refused therapy.
ANALYSIS OF BREAST CANCER SURGERY AFTER TRAM RECONSTRUCTION/ROSS ET AL
414 THE AMERICAN JOURNAL OF SURGERY® VOLUME 179 MAY 2000

of the 5 patients who were diagnosed with recurrences hadundergone salvage mastectomy. In this series, 8 patientsunderwent salvage mastecomy. Of those, 4 were diagnosedwith either a locoregional recurrence or distant metastases.Two patients with salvage mastectomy had local recur-rence in the chest wall. Of the remaining 67 patients whohad primary mastectomy, only 1 was diagnosed with arecurrence. Because the number of patients in this series issmall, statistical significance is impossible to attain; how-ever, certainly there is a trend toward a higher recurrencerate in patients undergoing salvage mastectomy.
Patients who undergo salvage mastectomy have failedconservative surgical treatment. Recurrences such as thishistorically have indicated more aggressive disease.18,19
The ability of a tumor to recur locally is more a function ofthe histopathology of the tumor and stage at diagnosis thanit is a function of the type of surgery or reconstructionperformed.7,11 The majority of patients who recur locallyafter mastectomy will go on to develop metastatic dis-ease.19 Thirty percent to 60% of patients with a localrecurrence will be found to have synchronous metastaticdisease.20 The overall prognosis of patients who have alocal recurrence is poor.19
The majority of local recurrences occur within 24 monthsof the diagnosis.1 In the series by Sandelin et al,21 a localrecurrence rate of 8% was reported with a median time todiagnosis of 7.8 months (range 1 to 23). Noone et al2
reported a 31-month interval to local recurrences. In ourseries, the mean interval to recurrence was 22.8 months,falling well within the reported time frame for recurrence.
Local recurrences following breast reconstruction aremost often identified as nodular regions in the native skinflap or subcutaneous tissue, which is adjacent to the mas-tectomy site.22 The 2 patients in this series who recurredlocally presented with nodularity in the region of theprevious incision. In neither case did the presence of theflap impair the physicians’ ability to detect the recurrence.
The complications associated with this type of recon-struction include total and partial flap loss, fat necrosis,skin flap necrosis, and hernia. The reported rates of totaland partial flap loss range from 0% to 8% (average 5.3%).Skin flap necrosis ranges from 3% to 6%, and abdominalwall hernias occur in 0% to 7% (average 3.7%) of pa-tients.11,13,23–25 In the present series, 10 patients (13.3%)had complications that required additional treatment, re-quiring either prolonged hospital stay or an additionalhospital admission. Overall, the complications in this serieswere less frequent than reported in the literature, indicat-ing that in this center, free flap reconstruction is a safesurgical option.
Patient satisfaction is an important issue to address whenmanaging breast reconstruction. The psychological benefitsof restoring or preserving body form are well described.2–6
However, in order to derive the maximum psychologicalbenefits, patients themselves must be satisfied with thecosmetic results of their reconstruction. If the patient feelsthat the reconstructed breast is inferior cosmetically, thenthe benefits derived are less. In this series, 72 of the 75patients (96%) were contacted by telephone and ques-tioned about their perception of the cosmetic appearanceof the TRAM flap. Sixty-seven patients (93% of patients
contacted) judged the results to be either excellent orgood. This indicates that the majority of patients whounderwent reconstruction in this series were pleased withthe cosmetic results of their flap. Presumably, this satisfac-tion will contribute to the maximal psychological benefitderived by these patients.
CONCLUSIONSIn patients requiring primary mastectomy for breast can-
cer therapy, reconstruction with free TRAM flaps is anoncologically safe and cosmetically appealing surgical al-ternative. Despite the higher local recurrence rate in thosepatients undergoing salvage mastectomy, these patientsderive similar positive psychological benefits as thosewomen undergoing primary mastectomy. The risk of localrecurrence is ultimately determined by the histology of thetumor and the stage of disease at diagnosis, not the pres-ence of a reconstructed breast. Perhaps the improved qual-ity of time remaining for these patients is more importantthan the potentially limited quantity of time. Thesewomen should not be denied reconstruction based only ontheir salvage mastectomy status.
Breast reconstruction is not for every patient. It is a safeand satisfactory surgical option that should be consideredfor all patients, however, regardless of disease stage orsalvage mastectomy status.
REFERENCES1. Slavin SA, Love SM, Goldwyn RM. Recurrent breast cancerfollowing immediate reconstruction with myocutaneous flaps. PlastReconstr Surg. 1994;93:1191.2. Noone RB, Murphy JB, Spear SL, et al. A 6-year experiencewith immediate reconstruction after mastectomy for cancer. PlastReconstr Surg. 1985;76:258.3. Dean C, Chetty U, Forrest APM. Effects of immediate breastreconstruction on psychosocial morbidity after mastectomy. Lancet.1983;1:459.4. Stevens LA, McGrath MH, Druss RG, et al. The psychologicalimpact of immediate breast reconstruction for women with earlybreast cancer. Plast Reconstr Surg. 1984;73:619.5. McGuire WL, Clark GM. Prognostic factors and treatmentdecisions in axillary node negative breast cancer. NEJM. 1992;326:1756.6. Morris T, Greer SH, White P. Psychological and social adjust-ment to mastectomy. Cancer. 1977;40:2381.7. Georgiade GS, Riefkohl R, Cox E, et al. Long-term clinicaloutcome of immediate reconstruction after mastectomy. Plast Re-constr Surg. 1985;76:415.8. Johnson CH, van Heerden JA, Donohue JH, et al. Oncologicaspects of immediate breast reconstruction following mastectomyfor malignancy. Arch Surg. 1989;124:819.9. Kroll SS, Ames F, Singletary SE, Schusterman MA. The onco-logic risks of skin preservation at mastectomy when combined withimmediate reconstruction of the breast. Surg Gynecol Obstet. 1991;172:17.10. Kroll SS, Schusterman MA Tadjalli HE, et al. Risk of recur-rence after treatment of early breast cancer with skin-sparing mas-tectomy. Ann Surg Oncol. 1997;4:193.11. Singletary SE. Skin-sparing mastectomy with immediate breastreconstruction: the MD Anderson Cancer Center experience. AnnSurg Oncol. 1996;3:411.12. Scheflan M, Hartrampf CR, Black PW. Breast reconstructionwith a transverse abdominal island flap. Plast Reconstr Surg. 1982;16:900.13. Wilkins EG, August DA, Kuzon WM, et al. Immediate trans-
ANALYSIS OF BREAST CANCER SURGERY AFTER TRAM RECONSTRUCTION/ROSS ET AL
THE AMERICAN JOURNAL OF SURGERY® VOLUME 179 MAY 2000 415

verse rectus abdominis musculocutaneous flap reconstruction aftermastectomy. J Am Coll Surg. 1995;180:177.14. Hartrampf, CR. Bennett GK. Autogenous tissue reconstructionin the mastectomy patient. Ann Surg. 1987;205:508.15. Grotting JC, Urist MM, Maddox WA, Vasconez LO. Conven-tional TRAM flap versus free microsurgical TRAM flap for imme-diate breast reconstruction. Plast Reconstr Surg. 1989;83:828.16. Kroll SS, Coffey JA, Rodger JW, Schusterman MA. A com-parison of factors affecting aesthetic outcomes of TRAM flap breastreconstruction. Plast Reconstr Surg. 1995;96:860.17. Kroll SS. Immediate breast reconstruction: a review. AnnalesChirurgiae et Gynaecologiae. 1997;86:5.18. Ames FC, Balch CM. Management of local and regional re-currence after breast-conserving treatment. Surg Clin North Am.1990;70:1115.19. Gilliland MD, Barton RM, Copeland EM. The implications oflocal recurrence of breast cancer as the first site of therapeuticfailure. Ann Surg. 1983;197:284.
20. Newman LA, Kuerer HM, Hunt KK, et al. Presentation, treat-ment and outcome of local recurrence after skin-sparing mastec-tomy and immediate breast reconstruction. Ann Surg Oncol. 1998;5:620.21. Sandelin K, Billgren A, Wickman M. Management, morbidityand oncologic aspects in 100 consecutive patients with immediatebreast reconstruction. Ann Surg Oncol. 1998;5:159.22. Donegan WL, Perez-Mesa CM, Watson FR. A biostatisticalstudy of locally recurrent breast carcinoma. Surg Gynecol Obstet.1966;122:529.23. Baldwin BJ, Schusterman MA, Miller MJ, et al. Bilateral breastreconstruction: conventional versus free TRAM. Plast ReconstrSurg. 1994;93:1410.24. Arnez ZM, Bajec J, Bardsley AF, et al. Experience with 50 freeTRAM breast reconstructions. Plast Reconstr Surg. 1991;87:470.25. Elliott LF, Eskenazi L, Beegle PH, et al. Immediate TRAM flapbreast reconstruction: 128 consecutive cases. Plast Reconstr Surg.1993;92:2,217.
ANALYSIS OF BREAST CANCER SURGERY AFTER TRAM RECONSTRUCTION/ROSS ET AL
416 THE AMERICAN JOURNAL OF SURGERY® VOLUME 179 MAY 2000





























