Embed Size (px)
Citation preview
AopATU
ItApacm
Mtplci
Raw(i0dhp3
Cittc
PHJU
Iltso
Mttodwpy
op
Rltpecsfow
Ts
LLN
*
Cpre
TbpSMMSR
Iic(lp
Muci
Rafopbt
S107Vol. 211, No. 3S, September 2010 Surgical Forum Abstracts
n acuity adaptable patient care improves surgicalutcomes in patients undergoing major thoracicroceduresnai Kothari, Mark Hennon MD, Alejandro Munoz-del-Rio PhD,raci Bretl RN, Tracey Weigel MD, FACS, FACCPniversity of Wisconsin, Madison, WI
NTRODUCTION: Several academic and community medical cen-ers have replaced traditional intensive/general care units with Acuitydaptable Care Units (AACU). Few studies have measured the im-act of an AACU on surgical outcomes. We examined the effects ofdopting an AACU and compared it to our former intensive/generalare model with respect to surgical outcomes for patients undergoingajor thoracic surgeries.
ETHODS: We reviewed data from an IRB-approved, prospec-ively maintained thoracic surgery database during the three yeareriods pre- and post-adoption of an AACU model. We compared
ength of stay, 30 day mortality, and incidence of post-operativeomplications in patients undergoing major thoracic procedures dur-ng these two time periods.
ESULTS: There were 1393 (53.2%) patients in the pre-AACU erand 1223 (46.8%) in the post-AACU era. The 30 day mortality ratesere 1.9% and 1.8% in the pre- and post-AACU eras, respectively
p � 0.885). The in-hospital mortality rates were lower for patientsn the AACU (1.9%) compared to the pre-AACU era (2.9%; p �.002). Both length of stay (4 days, IQR 2-8 days post-AACU vs. 8ays, IQR 4-19 days pre-AACU; p � 0.001) and number of in-ospital complications were reduced in the post-AACU era com-ared to the pre-AACU era (27.7% post-AACU vs. pre-AACU6.8%; p�0.001).
ONCLUSIONS: An Acuity Adaptable Care Unit appears to be anmprovement in post-operative care for patients undergoing majorhoracic procedures. Our results demonstrate the model may con-ribute to improved surgical outcomes. Future study will focus on theost impact of the AACU model on patient care.
ost-discharge thromboprophylaxis after trauma.ow much would it cost?
ennifer C. Roberts MD, Ciaran Bradley MD, Karen Brasel MDniversity of Wisconsin, Madison, WI
NTRODUCTION: The optimal duration of venous thromboembo-ism prophylaxis in trauma patients is unknown. For high risk pa-ients, post-discharge prophylaxis is suggested. The purpose of thistudy is to estimate the cost-effectiveness of three different strategiesf post-discharge thromboprophylaxis in trauma patients.
ETHODS: A cost-effectiveness model was constructed comparinghree strategies of post-discharge thromboprophylaxis in trauma pa-ients: (1) No prophylaxis, (2) low molecular weight heparin (LMWH)nce daily, (3) low-dose unfractionated heparin (LDUH) three timesaily. Probabilities and costs were estimated using published literature,holesale drug price, and Medicare reimbursement. The primary end-oint was cost of prophylaxis per patient without VTE. Sensitivity anal-
ses were conducted to test the robustness of the results. The perspective ff the healthcare system was taken. Both patient compliance and com-lications from anticoagulation were considered.
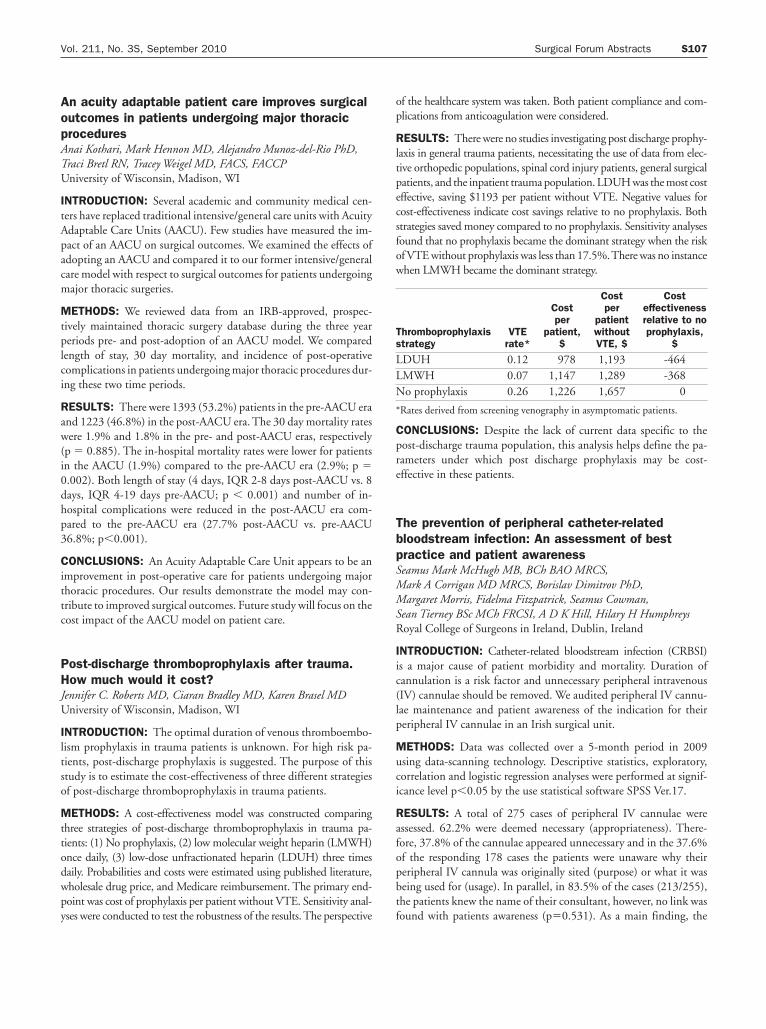
ESULTS: There were no studies investigating post discharge prophy-axis in general trauma patients, necessitating the use of data from elec-ive orthopedic populations, spinal cord injury patients, general surgicalatients, and the inpatient trauma population. LDUH was the most costffective, saving $1193 per patient without VTE. Negative values forost-effectiveness indicate cost savings relative to no prophylaxis. Bothtrategies saved money compared to no prophylaxis. Sensitivity analysesound that no prophylaxis became the dominant strategy when the riskf VTE without prophylaxis was less than 17.5%.There was no instancehen LMWH became the dominant strategy.
hromboprophylaxistrategy
VTErate*
Costper
patient,$
Costper
patientwithoutVTE, $
Costeffectivenessrelative to noprophylaxis,
$
DUH 0.12 978 1,193 -464MWH 0.07 1,147 1,289 -368o prophylaxis 0.26 1,226 1,657 0
Rates derived from screening venography in asymptomatic patients.
ONCLUSIONS: Despite the lack of current data specific to theost-discharge trauma population, this analysis helps define the pa-ameters under which post discharge prophylaxis may be cost-ffective in these patients.
he prevention of peripheral catheter-relatedloodstream infection: An assessment of bestractice and patient awarenesseamus Mark McHugh MB, BCh BAO MRCS,ark A Corrigan MD MRCS, Borislav Dimitrov PhD,argaret Morris, Fidelma Fitzpatrick, Seamus Cowman,
ean Tierney BSc MCh FRCSI, A D K Hill, Hilary H Humphreysoyal College of Surgeons in Ireland, Dublin, Ireland
NTRODUCTION: Catheter-related bloodstream infection (CRBSI)s a major cause of patient morbidity and mortality. Duration ofannulation is a risk factor and unnecessary peripheral intravenousIV) cannulae should be removed. We audited peripheral IV cannu-ae maintenance and patient awareness of the indication for theireripheral IV cannulae in an Irish surgical unit.
ETHODS: Data was collected over a 5-month period in 2009sing data-scanning technology. Descriptive statistics, exploratory,orrelation and logistic regression analyses were performed at signif-cance level p�0.05 by the use statistical software SPSS Ver.17.
ESULTS: A total of 275 cases of peripheral IV cannulae weressessed. 62.2% were deemed necessary (appropriateness). There-ore, 37.8% of the cannulae appeared unnecessary and in the 37.6%f the responding 178 cases the patients were unaware why theireripheral IV cannula was originally sited (purpose) or what it waseing used for (usage). In parallel, in 83.5% of the cases (213/255),he patients knew the name of their consultant, however, no link was
ound with patients awareness (p�0.531). As a main finding, the