Embed Size (px)
DESCRIPTION
Amniocentese and Chorionic in prenatal diagnosis
Citation preview

Pergamon J Clin Epidamiol Vol. 47, No. 11, pp. 121S-1228, 1994
Copyright 0 1994 Elsevier Science Ltd Printed in Great Britain. All rights reserved
0895-4356/94 $7.00 + 0.00
PREFERENCES OF PREGNANT WOMEN FOR AMNIOCENTESIS OR CHORIONIC VILLUS SAMPLING
FOR PRENATAL TESTING: COMPARISON OF PATIENTS’ CHOICES AND THOSE OF A DECISION-ANALYTIC
MODEL
PAUL S. HECKERLING, ‘* MARION S. VERP~ and TERESA A. HADRO~ ‘Department of Medicine, University of Illinois, Chicago, IL, and 2,3Department of Obstetrics and
Gynecology, University of Chicago, Chicago, IL, U.S.A.
(Received in revised form 17 May 1994)
Abstract-Decision analytic models have suggested that the choice of amniocentesis or chorionic villus sampling for prenatal genetic testing is a utility-driven decision. We compared preferences for prenatal testing among 1.56 pregnant women who had chosen either amniocentesis (n = 82) or chorionic villus sampling (n = 74) for the indication of maternal age. We also compared their choices with those of a decision-analytic model based on their preferences, and age-specific rates of spontaneous abortion and chromo- somal abnormalities. Preferences were assessed using written scenarios describing potential outcomes of prenatal testing, and were recorded on linear rating scales. The differences in preference ratings for first- vs second-trimester prenatal diagnosis of a normal child (4.2 vs - 1.6, p = 0.0004), and for first- vs second-trimester abortion of an abnormal fetus (4.4 vs - 1.6, p = O.Ol), were significantly greater among women choosing chorionic villus sampling than among women choosing amniocentesis. There were no significant differences between chorionic villus sampling and amniocentesis patients in their preference ratings for test-related miscarriage, disconfirmed results at pregnancy termination, or maternal morbidity from therapeutic abortion. After adjusting for demographic and obstetric factors, the difference in preferences for early vs late prenatal diagnosis was an independent predictor of the choice of chorionic villus sampling in a multivariate model. Among women whose decision analyses selected amniocentesis, 56.8% had chosen amniocentesis, and among women whose analyses selected chorionic villus sampling, 63.2% had chosen chorionic villus sampling (p = 0.05). We conclude that the preferences of pregnant women for the outcomes of prenatal testing were associated with their choice of amniocentesis or chorionic villus sampling. In addition, the choice of prenatal test made by the majority of women was concordant with that of a decision-analytic model that incorporated their preferences. Nevertheless, because many women made choices that were discordant with their decision-analytic results, further research into the bases for their choices is warranted.
Prenatal testing Amniocentesis Chorionic villus sampling Utilities Decision analysis
*Reprint requests should be addressed to: Paul S. Heckerling, M.D., Department of Medicine, University of Illinois, Box 6998 M/C 787, Chicago, IL 60680, U.S.A.
1215

1216 PAUL S. HECKERLING et al.
INTRODUCTION
Amniocentesis and chorionic villus sampling are tests used for prenatal diagnosis of chromoso- ma1 abnormalities. Each test has advantages and disadvantages when compared to the other. Amniocentesis has a lower risk of procedure- related spontaneous abortion [l-6], lower false-positive [3,4,7-201 and indeterminacy [4, 13-l 5, 16-l 8,2 1,221 rates, and possibly a lower risk of induced malformations [23,24], compared to chorionic villus sampling. How- ever, because results are usually not available before the 20th gestational week, pregnancy termination after an abnormal amniocentesis requires a second-trimester abortion, with at- tendant risk of maternal morbidity [25]. In addition, delay in genetic diagnosis may result in increased maternal anxiety [26,27] and di- minished maternal-fetal bonding [28]. Chori- onic villus sampling provides genetic diagnosis in the first trimester, thereby decreasing ma- ternal anxiety [26,27] while providing the op- tion of a safer [29], less traumatic, first-trimester therapeutic abortion if the results are abnormal.
In our previous work [30], using a decision- analytic model, we showed that the choice of amniocentesis or chronic villus sampling for maternal age was driven by two factors: the difference in the decision maker’s utilities (val- ues) for first- and second-trimester therapeutic abortion; and the anxiety cost of awaiting sec- ond-trimester genetic diagnosis. These results remained true over a wide range of plausible values for the rates of spontaneous abortion after amniocentesis and chorionic villus sampling, abnormal and indeterminate chori- onic villus sampling results, false-positive and false-negative test results, and maternal morbid- ity after first- and second-trimester therapeutic abortion. This suggested that for pregnant women with differing values for first- vs second- trimester therapeutic abortion, and for early vs late genetic diagnosis, the optimal choice of prenatal test might differ. However, studies comparing these values, and values for other outcomes of prenatal testing, among women choosing amniocentesis and chorionic villus sampling have not been performed. In addition, how the choices of prenatal test made by preg- nant women compare with those prescribed by decision analytic models incorporating their values is not known.
To answer these questions, we studied prefer- ences for the outcomes of prenatal genetic test- ing among women choosing amniocentesis or
chorionic villus sampling for the indication of maternal age. We compared preferences of women choosing each test, and compared their choices with those of a decision-analytic model based on their preferences, and age-specific rates of spontaneous abortion and chromosomal abnormalities. We also examined demographic factors, obstetric factors, and factors related to locus of decision making (patient vs physician), to determine their effect on test choice.
METHODS
Study population
We studied 156 patients who were referred to the obstetrical genetic clinics of the University of Chicago Hospitals for prenatal testing because of maternal age. Patients presenting because of an abnormal fetus or child in a previous pregnancy, a family history of genetic disease, or an abnormal maternal serum alpha fetoprotein, were excluded. These 156 patients were referred by 73 different physicians, of whom 21 (28.8%) were university-based prac- titioners, and 52 (71.2%) were private prac- titioners from the local community and surrounding suburbs. Study patients were enrolled over a 10 month period, from mid- February to mid-December 1991. The enroll- ment period preceded local media publicity concerning the possible association of chorionic villus sampling and limb reduction defects by several months. Thus the preferences of study participants, and their choice of prenatal test, were not influenced by this factor. All eligible patients agreed to participate in the study.
The obstetrical genetic clinics consist of an amniocentesis clinic and a chorionic villus sampling clinic. In the chorionic villus sampling clinic, patients present at 10-l 1 weeks gestation for counseling and chorionic villus sampling. In the amniocentesis clinic, patients present at 15-16 weeks gestation for counseling and amniocentesis. Patients presenting to the clinics typically have already decided to have the respective procedure performed. The decision to have chorionic villus sampling or amniocentesis will have been made in some cases by the patient (and her partner), and in others by the referring physician.
Demographic and obstetric data
Prior to counseling and testing, patients com- pleted a questionnaire containing demographic and obstetric data. Demographic data included age, ethnic background, level of education,

Amniocentesis or Chorionic Villus Sampling for Prenatal Testing 1217
occupation, marital status, annual income, and type of medical insurance. Obstetric data in- cluded the number of prior amniocenteses, chorionic villus samplings, spontaneous abor- tions, stillbirths, elective abortions, and living children.
Preference and decision -making data
Patients were also asked to indicate on the questionnaire their preference ratings for each of the potential outcomes of prenatal testing. Potential outcomes considered were first- and second-trimester diagnosis (by chorionic villus sampling and amniocentesis, respectively) of a normal child; spontaneous abortion after amniocentesis, chorionic villus sampling, and without prenatal testing (with genetic status of the abortus unknown); first- and second trimester therapeutic abortion after an abnor- mal test result, with abortus confirmed as abnormal, and with disconfirmed results (abor- tus normal); and maternal morbidity after therapeutic abortion (i.e. infection requiring hospitalization or bleeding requiring trans- fusion). In a subset of 142 patients, the prefer- ence ratings for spontaneous abortion after an abnormal amniocentesis and chorionic villus sampling were also determined. All preferences were recorded prior to counseling and testing. Neither assessed preference ratings, nor ex- pected values derived from the decision-analytic model (see below), were used to counsel patients concerning the test they had chosen. Counseling sessions focused on the likelihood of an abnor- mal pregnancy, the accuracy of prenatal testing, and the risk of spontaneous abortion or fetal injury from prenatal testing. The likelihood of maternal morbidity after therapeutic abortion of an abnormal pregnancy was not discussed unless the patient raised the issue.
Each preference rating was assessed using a written vignette describing a hypothetical situation in which the patient experienced the outcome in question. For example, the prefer- ence for first-trimester therapeutic abortion was assessed by a vignette that asked the patient to assume that she had a chorionic villus sampling; that the result was abnormal and she elected to have a therapeutic abortion; that the abortion was performed before she was visibly pregnant or had experienced fetal movement, and did not involve the induction of labor; and that the abortus was found to be chromosomally abnor- mal, as predicted. The preference for second- trimester therapeutic abortion was assessed by a
similar vignette, except that the patient was asked to assume that she had an amniocentesis; and that therapeutic abortion was performed in the second trimester, after she was visibly preg- nant and had experienced fetal movement, and involved the induction of labor. (Although abortion by dilatation and evacuation is avail- able for some second-trimester terminations at many centers, including ours, abortion by in- duction is more commonly used to terminate abnormal pregnancies following genetic amnio- centesis.) Other vignettes from the preference assessment instrument are shown in Appendix A. To control for the effects of vignette order on patients’ preferences, patients were randomized to receive questionnaires presenting amniocen- tesis-related or chorionic villus sampling-related vignettes first.
Patients’ preferences were recorded on linear rating scales [31] anchored at 100 units (the best possible outcome) and 0 units (the worse poss- ible outcome). Patients indicated their prefer- ences for each outcome by placing an “x” on the appropriate place on the scale. The distance from the “0” mark to the “x”, as measured by a ruler, was used to calculate each preference [i.e. preference = (distance from “0” to “x”/length of rating scale line] x 100). On this scale, preferences that differed by x3.75 units (3/16 in. on the rating scale line) were difficult to distinguish reproducibly by linear measurement. Therefore, when preference differences between paired amniocentesis- and chorionic villus sampling-related outcomes differed by c 3.75 units, they were assigned identical preferences (the mean of the two values), under the assump- tion that in these cases, the patient had intended the outcomes to be valued equivalently. This conservative assumption was designed to avoid assigning preference differences for amnio- centesis and chorionic villus sampling when none existed. This approximation procedure has not, to our knowledge, been tested in studies using rating scales, and its validity remains uncertain. Of the 156 study participants, 150 (96.2%) completed the rating scale part of the preference questionnaire.
Patients were also asked whether the decision to have an amniocentesis or chorionic villus sampling was made principally by themselves, by their physicians, or was shared equally between them. Responses were recorded on a five-point Likert-type scale, with a spectrum ranging from “decision entirely mine” to “de- cision entirely physician’s”.

1218 PAUL S. HECKERLINC er al.
Data analysis
From each patient’s recorded preferences, we derived four preference differences (costs): (1) the difference in preferences between first- and second-trimester diagnosis of a normal child. This represents a cost of waiting for prenatal testing results (cost of waiting); (2) the difference in preferences between spontaneous abortion without prenatal testing and spontaneous abor- tion after amniocentesis or chorionic villus sampling. This represents a cost imputed to the possibility that the testing procedure caused the abortion (cost of test-related miscarriage). To calculate this cost, we used preferences for spon- taneous abortion after testing of a fetus of unknown genetic status, because in the absence of testing, the status of an aborted fetus would generally not be known; (3) the difference in preferences between first- and second-trimester therapeutic abortion of an abnormal fetus. This represents a cost of therapeutic abortion per- formed after, rather than before, a woman is visibly pregnant and has experienced fetal movement, and that involves the induction of labor (cost of late therapeutic abortion); and (4) the difference in preferences of therapeutic abortion without vs with attendant maternal morbidity (cost of maternal morbidity).
Comparisons of demographic variables, obstetric variables, preferences, and derived costs between patients choosing amniocentesis and chorionic villus sampling were made using x2 with Yates’ correction for continuity for categorical data, and Student’s t for continuous data. Based on the variances in preference rat- ings, our study had 99.9 and 98.9% power to detect 5-unit differences between the amniocen- tesis and chorionic villus sampling groups in the preference costs of waiting for genetic diagnosis and late therapeutic abortion, respectively. Our study also had 99.4 and 95.3% power to detect IO-unit differences in the preference costs of test-related spontaneous abortion and maternal morbidity, respectively. These differences can determine the choice of amniocentesis or chori- onic villus sampling in decision models [30], and therefore are clinically important to detect.
To compare prenatal testing choices made by patients and those prescribed by formal decision analytic models, we used our previously published decision tree [30]. The tree models the choice of amniocentesis, chorionic villus sampling, and no prenatal testing, and includes probability and utility data important in making
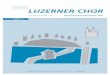
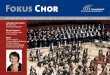
that choice. Because all patients in this study had prenatal testing performed, we restricted our analysis to the amniocentesis and chorionic villus sampling branches of the tree (Figs 1 and 2). For each patient, we used age-adjusted prevalences of chromosomal abnormalities [32-341 and spon- taneous abortion rates [35,36] (Appendix B), and the patient’s rating scale preferences, to evaluate the decision tree. Expected values for amniocentesis and chorionic villus sampling were calculated by folding back the decision tree [37], and the test with the higher expected value was considered the decision-analytic choice for that patient. We also calculated the difference in expected values between the amniocentesis and chorionic villus sampling strategies to determine how much better one strategy was than the other. Comparisons of decision-analytic based choices, and the test choices actually made by patients, were made using x2. Stepwise logistic regression [38] was used to determine the independent contributions of demographic factors, obstetric factors, preference ratings, expected values, and decision-maker status, to the choice of prenatal test. Odds ratios and 95% confidence limits were calculated from the logistic coefficients and their SEs. A two-tailed a level of 0.05 was considered significant.
RESULTS
Demographic and obstetric data for the 156 women in the study populations are shown in Table 1. The mean age was 37.5 years; 149 women (95.5%) were 35 years of age or older. Seven women <35 years of age (five at age 34;
I Abortion
Abnormal
Morbidity Abortus
(0 Positive: Second ‘Z 2 Trimester Normal B__(, Therapeutic :: Abortion
Abortus
‘2
2 Abnormal
No Morbidity r Abortus
Continue Normal Abortus
I Abnormal
Negative
[ Normal Child
Fig. I. The amniocentesis branch of the decision tree.

Amniocentesis or Chorionic Villus Sampling for Prenatal Testing 1219
Chorionic Villus sampling
L
Spontaneous Abortion
Continue
Positive: First Trimester
Abnormal
Morbidity Abortus 0
Normal
Abortus
Indeterminate Amniocentesis
Abnormal
Vegative
Fig. 2. The chorionic villus sampling branch of the decision tree.
one at age 33; one at age 32) received prenatal testing solely because of maternal age, and were therefore included. Eight-two women (52.6%) chose amniocentesis for prenatal testing, and 74 women (47.4%) chose chorionic villus sampling. In 79 cases (52.7%) the choice of prenatal test was made entirely or mostly by the patient, in 45 cases (30.0%) the choice was shared equally between patient and physician, and in 26 cases (17.4%) the choice was made entirely or mostly by the physician.
Table 2 compares demographic and obstetric factors between women choosing amniocentesis and women choosing chorionic villus sampling. Women choosing chorionic villus sampling were more frequently college educated, professionally employed, and covered by commercial in- surance, than women choosing amniocentesis, but the differences were not significant. In addition, women choosing chorionic villus sampling showed a trend toward more fre- quently having had a prior amniocentesis or chorionic villus sampling. There were no sig- nificant differences in the frequencies of spon- taneous abortion, elective abortion, or living children, among women choosing amniocentesis or chorionic villus sampling. Among women choosing amniocentesis, the choice of prenatal test was made by the patient in 51.9% of cases, by the physician in 20.3%, and shared between patient and physician in 27.8%; among women choosing chorionic villus sampling, the choice
was made by the patient in 54.3% of cases, by the physician in 14.3%, and shared between patient and physician in 31.4% (p = 0.62).
Table 3 compares rating scale preferences and derived costs (preference differences) between women choosing amniocentesis and chorionic villus sampling. The cost of waiting for genetic diagnosis (the difference in preferences for first- and second-trimester diagnosis of a normal child), and the cost of late therapeutic abortion (the difference in preferences for first- and sec- ond-trimester therapeutic abortion of an abnor- mal fetus), were significantly greater among women choosing chorionic villus sampling than among women choosing amniocentesis. There were no significant differences in the costs of test-related spontaneous abortion or maternal morbidity between the two groups. Stepwise logistic regression identified the cost of waiting for genetic diagnosis as a significant indepen- dent predictor of choosing chorionic villus sampling (odds ratio for a l-unit change in utility cost, 1.16; 95% confidence limits, 1.01-1.33; odds ratio for a 5-unit change, 2.06; 95% confidence limits, 1.03-4.11).
Table 3 also compares expected values of amniocentesis and chorionic villus sampling, determined by decision analysis, among women choosing each test. The expected value of chori- onic villus sampling, and the difference in ex- pected values between chorionic villus sampling and amniocentesis, were significantly greater

1220 PAUL S. HECKERLING et al.
among women choosing chorionic villus sampling. There was no difference in the ex- pected value of amniocentesis between the two groups. When expected values were included as candidate variables for the logistic model, the difference in expected values between chorionic villus sampling and amniocentesis (odds ratio for a l-unit change, 1.21; 95% confidence limits, 1.02-1.43), and having had a prior amnio- centesis (odds ratio 8.98; 95% confidence limits, 1.03-78.6), were significant independent predic- tors of choosing chorionic villus sampling for prenatal testing.
Table 4 stratifies the comparisons of prefer- ences, costs, and expected values between the amniocentesis and chorionic villus sampling groups by locus of decision making. Among women who either made or shared in the choice of test, the cost of waiting for genetic diagnosis, the cost of late therapeutic abortion, and the difference in expected values between chorionic villus sampling and amniocentesis, were signifi- cantly greater among those choosing chorionic villus sampling. Among women whose phys- icians made the choice of test, there were no
Table 1. Demographic and obstetric data for the study population
Demographic Age W 31.5 * 2.5’
Ethnicity White non-Hispanic 103 (66.0)? Hispanic 9 (5.8) Black 38 (24.4) Other 6 (3.8)
Occupation Housewife 31 (20.0)? Non-professional 78 (50.3) Professional 46 (29.7)
Education < 16 yr 85 (54.5)t > 16 yr 71 (45.5)
Marital Not married 29 (18.7)t Married 126 (81.3)
Income (thousands of dollars) 61.5 _+ 39.2’
Insurance Commercial 141 (91.6)t Public aid 13 (8.4)
Obstetric Amniocenteses 0 147 (93.6)t
21 10 (6.4)
Chorionic villus samplings 0 I53 (97.5)? 31 4 (2.5)
Spontaneous abortions 0 98 (62.4)t >l 59 (37.6)
Elective abortions 0 123 (78.3)t 21 34 (21.7)
Children 0 51 (32.5)-l 31 106 (67.5)
*Mean f SD. tNumber (%).
significant differences in preferences, costs, or expected values between the two groups.
Based on patients’ preference ratings, decision analysis showed amniocentesis to be the choice in 74.7% of cases, and chorionic villus sampling to be the choice in 25.3% of cases. The test choices made by women and prescribed by their decision analyses agreed in 58.4% of cases, and disagreed in 41.6% of cases. Among women whose decision analyses selected an amniocentesis strategy, 56.8% had chosen amniocentesis, and 43.2% had chosen chorionic villus sampling; among women whose decision analyses selected a chorionic villus sampling strategy, 36.8% had chosen am- niocentesis, and 63.2% had chosen chorionic villus sampling (p = 0.05). Among women who either made or shared in the choice of test, 54.4% of those whose decision analyses selected amniocentesis chose amniocentesis, and 63.6% of those whose decision analyses selected chori- onic villus sampling chose chorionic villus sampling (p = 0.11). Among women whose physicians made the choice of test, 60% of those whose decision analyses selected amniocentesis chose amniocentesis, and 50% of those whose decision analyses selected chorionic villus sampling chose chorionic villus sampling (p = 0.68).
Preference ratings for spontaneous abortion of a fetus of unknown genetic status were generally low, and were less than preference ratings for therapeutic abortion of an abnormal fetus (Tables 3 and 4). This probably reflects a belief by our patients that most such spon- taneously aborted fetuses would be normal. Preference ratings for spontaneous abortion of an abnormal fetus were higher (Tables 3 and 4). When we reanalyzed the decision trees using these preference ratings for spontaneous abor- tion, 57.1% of women whose decision analyses selected amniocentesis chose amniocentesis, and 56.8% of those whose decision analyses selected chorionic villus sampling chose chorionic villus sampling (p = 0.18). Among women who made or shared in the choice of test, 54.8% of those whose decision analyses selected amniocentesis chose amniocentesis, and 60.5% of those whose decision analyses selected chorionic villus sampling chose chorionic villus sampling (p = 0.18). Among women whose physicians made the choice of test, 61.9% of those whose decision analyses selected amniocentesis chose amniocentesis, and 28.6% of those whose de- cision analyses selected chorionic villus

Amniocentesis or Chorionic Villus Sampling for Prenatal Testing
Table 2. Comparison of demographic and obstetric variables among women choosing amniocentesis (AMN) and chorionic villus sampling (CVS)
1221
Variable AMN cvs p value
Demographic Age (yr) 37.5
Ethnicitv White non-Hisnanic 63.4% Hispanic * Black Other
Occupation Non-professional Professional
Education c 16 yr 3 16 yr
Marital Not married Married
Income (thousands of dollars)
Insurance Commercial Public aid
Obstetric Amniocenteses
Chorionic villus samplings
Spontaneous abortions
Elective abortions
Children
6.1% 26.8%
3.7%
76.5% 23.5%
60.5% 39.5%
22.5% 11.5%
60.9
87.5% 12.5%
37.6
69.9% 5.5%
20.5% 4.1%
63.0% 37.0%
47.3% 52.1%
14.9% 85.1%
61.9
95.9% 4.1%
0 91.6% 89.2% ,l 2.4% 10.8%
0 100% 94.6% ,l 0% 5.4%
0 64.6% 60.8% ,l 35.4% 39.2%
0 82.9% 74.3% ,l 17.1% 25.1%
0 34.1% 31.1% ,l 65.9% 68.9%
0.71
0.82
0.067
0.14
0.32
0.89
0.12
0.07
0.10
0.74
0.26
0.81
sampling chose chorionic villus sampling (p = 0.65).
There were no significant differences in demo- graphic or obstetric factors between women who did and did not choose the test prescribed by their decision-analytic model. Women whose decision analyses prescribed amniocentesis but who chose chorionic villus sampling had had a prior amniocentesis somewhat more frequently (10.4% vs 1.6%, p = 0.11) than women who chose amniocentesis. Women whose decision analyses prescribed chorionic villus sampling but who chose amniocentesis assigned signifi- cantly lower costs to waiting (2.3 vs 12.5, p < 0.03), and to late therapeutic abortion (2.7 vs 12.7, p < 0.05), compared with women who chose chorionic villus sampling. Among women whose decision analyses prescribed amnio- centesis, there were no significant differences in preference costs between those choosing amnio- centesis or chorionic villus sampling. Among women who chose the test prescribed by their decision analysis, the choice had been theirs in 57.0%, shared with their physicians in 23.3%, and made by their physicians in 19.8% of cases. Among women who did not choose the test
prescribed by their decision analysis, the choice had been theirs in 44.8%, shared with their physicians in 39.7%, and made by their physicians in 15.5% of cases (p = 0.11).
DISCUSSION
We found that the preferences of pregnant women for the outcomes of prenatal genetic testing were associated with their choice of amniocentesis or chorionic villus sampling. The cost of waiting for genetic diagnosis (the differ- ence in preferences for first- and second- trimester diagnosis of a normal child), and the cost of late therapeutic abortion (the difference in preferences for first- and second-trimester abortion of an abnormal fetus), were signifi- cantly higher among women choosing chorionic villus sampling than among women choosing amniocentesis. In addition, the cost of waiting for diagnosis was an independent predictor of the choice of chorionic villus sampling in a multivariate model. In the majority of cases, women’s choices of prenatal test agreed with the choices of decision analytic models that incorporated their preferences. Nevertheless, in

1222 PAUL S. HECKERLING et al.
41.6% of cases, the choices of women and their the cost of maternal morbidity between the decision models differed. groups.
Greater utility increments for early vs late genetic diagnosis, and first- vs second-trimester therapeutic abortion, led to a choice of chori- onic villus sampling in a decision analytic model [30], and in our patients. Other studies that did not use formal preference assessment methods have also shown that testing during the first trimester [39-411, shorter waiting period for results [39,40], and type of abortion available for abnormals [39,40], were the most import- ant factors in the choice of chorionic villus sampling over amniocentesis. Although risk of spontaneous abortion was the most import- ant factor in the choice of amniocentesis in some studies [39,40], we found no difference in the cost of test-related abortion between women choosing amniocentesis or chorionic villus sampling. In addition, although women choosing amniocentesis are at greater risk for maternal morbidity from therapeutic abortion [25,29], we found no difference in
Demographic and obstetric factors may also affect the choice of prenatal genetic test. Some studies have shown a higher proportion of minority patients among women choosing amniocentesis [42], and a higher level of edu- cation among women choosing chorionic villus sampling [42,43], although other studies have not confirmed these associations [39,44,45]. We found that women choosing chorionic villus sampling were somewhat more frequently col- lege educated, professionally employed, and covered by commercial insurance, compared with women choosing amniocentesis, but the differences were not significant. In one study of women seeking prenatal diagnosis for advanced maternal age, 36% of those preferring amnio- centesis compared with 22% of those preferring chorionic villus sampling had experienced a spontaneous abortion in a prior pregnancy [40]. In another study, 25% of women choosing chorionic villus sampling compared with none
Table 3. Comparison of rating scale preferences, costs, and expected values among women choosing amniocentesis (AMN) and chorionic
villus sampling (CVS)
Variable AMN cvs p value
Preference ratings Normal child after AMN Normal child after CVS Spontaneous abortion Spontaneous abortion after AMN Spontaneous abortion after CVS Spontaneous abortion after AMN
(abortus abnormal) Spontaneous abortion after CVS
(abortus abnormal) Therapeutic abortion after AMN
(abortus abnormal) Therapeutic abortion after CVS
(abortus abnormal) Therapeutic abortion after AMN
with maternal morbidity Therapeutic abortion after CVS
with maternal morbidity Therapeutic abortion after AMN
(abortus normal) Theraneutic abortion after AMN
(abortus normal) Therapeutic abortion after CVS
(abortus normal)
Costs Cost of waiting Cost of test-related miscarriage Cost of late therapeutic abortion Cost of maternal morbidity
Expected values Expected value of AMN Expected value of CVS A Expected value (AMN - CVS)
94.1 93.7 0.64 93.1 97.1 0.02 28.4 32.6 0.31 21.9 32.2 0.34 21.3 33.7 0.13
64.9
65.9
63.7
62.1
38.8
39.4
15.9
15.9
15.7
61.5 0.51
61.5 0.39
58.3 0.32
62.1 0.92
36.1 0.66
37.0 0.62
15.3 0.89
15.3 0.89
17.5 0.68
- 1.6 4.1 0.0004 0.83 0.41 0.93
- 1.6 4.4 0.01 23.8 23.7 0.98
91.34 90.31 0.62 89.80 93.96 0.031
1.54 - 3.64 0.0006

Amniocentesis or Chorionic Villus Sampling for Prenatal Testing
Table 4. Comparison of rating scale preferences, costs, and expected values among women choosing amniocentesis (AMN) and chorionic villus sampling (CVS), stratified by decision maker
1223
Variable
Patient/shared Physician
AMN cvs p value AMN cvs p value
Preference ratings Normal child after AMN Normal child after CVS Spontaneous abortion Spontaneous abortion after AMN Spontaneous abortion after CVS Spontaneous abortion after AMN
(abortus abnormal) Spontaneous abortion after CVS
(abortus abnormal) Therapeutic abortion after AMN
(abortus abnormal) Therapeutic abortion after CVS
(abortus abnormal) Therapeutic abortion after AMN
with maternal morbidity Therapeutic abortion after CVS
with maternal morbidity Therapeutic abortion after AMN
(abortus normal) Therapeutic abortion after CVS
(abortus normal)
costs Cost of waiting Cost of test-related miscarriage Cost of late therapeutic abortion Cost of maternal morbidity
Expected values Expected value of AMN Expected value of CVS
94.5 93.8 93.3 97.7 28.7 33.1 29.7 31.5 29.3 33.4
64.7
65.9
65.3
63.4
39.7
40.8
15.2
14.9
60.9
61.3
56.1
60.9
37.2
37.5
13.3
15.7
- 1.2 4.2 - 0.75 1.58 - 1.9 4.8 24.1 21.2
91.16 90.20
90.27 94.02
- 3.75 A Expected value (AMN - CVS) 0.96
0.77 95.8 0.04 93.3 0.32 29.4 0.71 23.2 0.38 22.0
0.49 65.5
0.42 65.5
0.12 57.9
0.67 57.6
0.63 36.8
0.52 35.1
0.66 16.6
0.86 16.8
0.0008 - 2.6 0.65 6.7 0.02 - 0.3 0.62 21.8
0.71 92.31 0.07 89.26 0.002 3.05
93.3 0.51 95.8 0.56 36.8 0.47 39.6 0.14 36.7 0.15
64.4 0.94
57.3 0.53
66.3 0.54
64.5 0.62
30.6 0.62
30.6 0.70
24.6 0.49
24.6 0.50
::: - 1.8 34.8
0.25 0.29 0.68 0.32
89.97 0.54 91.76 0.60
- 1.79 0.26
of those choosing amniocentesis, had previously had an elective abortion (p = 0.014) [42]. These results suggested that the lower abortion rate following amniocentesis may have been particu- larly important to women who had experienced spontaneous abortion, and that the earlier diag- nosis of chorionic villus sampling may have been important to women who had undergone elective abortion. However, we, as others [43], found no differences in spontaneous or elective abortions among women choosing amnio- centesis or chorionic villus sampling.
In our study, women who chose chorionic villus showed a trend toward having had prior amniocentesis more frequently than women choosing amniocentesis (p = 0.07). In addition, prior amniocentesis emerged as a predictor of the choice of chorionic villus sampling in a multivariate model that controlled for patients’ preferences. These results suggest that indepen- dent of their values for the outcomes of prenatal testing, some women choose chorionic villus sampling because of negative experiences with amniocentesis from a prior pregnancy. How-
ever, others have found that the frequency of prior amniocentesis was similar among women choosing amniocentesis and chorionic villus sampling [42].
Decision analysis is a method for explicitly defining choices and outcomes under conditions of uncertainty [37,46]. Decision analysis incorporates probabilities and utilities for each uncertain outcome into a structured tree, and selects the best choice according to the theory of maximum expected utility. It therefore allows the decision maker to trade-off the risks and benefits that are normally involved in a decision. Our results show that decision-analytic results were predictive of women’s choices of prenatal test. The difference in expected values between chorionic villus sampling and amniocentesis from each woman’s decision model was the most important predictor of choice of test in a multivariate model that considered each of their preferences and preference costs separately. Thus some women in our study appeared to be able to consider all relevant preferences in making their choice of prenatal test. Among

1224 PAUL S. HECKERLING et al.
women whose decision analyses selected amnio- centesis, 56.8% had chosen amniocentesis, and among women whose decision analyses selected chorionic villus sampling, 63.2% had chosen chorionic villus sampling, a difference that was significant (p = 0.05). Thus the majority of women’s choices of prenatal test were concordant with those of decision models that incorporated their preferences. Others have suc- cessfully used decision analysis to guide the choices of pregnant women for amniocentesis or no prenatal testing [47,48].
Nevertheless, almost 42% of the women in our study did not choose the prenatal test prescribed by their decision-analytic model. There are several reasons why this may have occurred. One possibility is that these women considered all relevant outcome values but weighted them improperly due to inaccurate estimates of their likelihood of occurrence. The choice of amniocentesis or chorionic villus sampling in our decision analytic model was relatively insensitive to a wide range of outcome probabilities [30]. Therefore, inaccurate esti- mates of probabilities are unlikely to entirely explain the difference between women and de- cision models. Nevertheless, we cannot exclude the possibility that women’s probability esti- mates were poorly calibrated, or were confounded with their preferences.
Another possibility is that despite lack of agreement with an expected value model, these women made choices consistent with their preferences. In this regard, it is notable that women whose decision analysis prescribed chorionic villus sampling but who chose amnio- centesis had significantly lower preference costs for waiting for genetic diagnosis, and for late therapeutic abortion, than women who chose chorionic villus sampling. Indeed, their prefer- ence costs for these outcomes were not different from those of women whose choice of amnio- centesis matched that of their decision models (data not shown). These results suggest that despite their decision-analytic outcomes, these women made a choice that was in some sense consonant with their preferences. However, there were no differences in preference costs for patients who decision analysis prescribed am- niocentesis and who did and did not choose this test. Thus the decision making of the latter group of women cannot be explained on this basis.
A third possibility is that in cases where test choice and decision analysis did not agree, the
preferences used to select the test were the physicians’ rather than the patients’. Because we did not assess physicians’ preferences for the outcomes of prenatal testing, we cannot address this possibility directly. However, it is notable that in these cases, physicians either made, or shared in, the choice of test somewhat more frequently (p = 0.11) than in the cases where test choice and decision analysis agreed. Thus it is possible that it was the physicians’, rather than the patients’, preferences that weighed more heavily in the cases where patients and decision analyses differed. Studies have shown that patients’ and physicians’ utilities for vari- ous patient outcomes may differ considerably [49, 501. It is also possible that our patients’ partners’ preferences determined the choice of test, but we have no data to support or refute this possibility.
Finally, it is possible that factors not captured by decision-analytic models determined our patients’ choices of test. Studies have shown that patients [51] and physicians [52,53] often make choices that differ from those of decision- analytic models based on their utilities. Reasons for discrepancies between decision making and expected utility models are probably multi- factorial, and include the overweighting of small probabilities [54], considerations of regret [52,55, 561, perceptions of short- vs long-term expectation [57], as well as other factors.
There are several limitations to our study. First, and most important, women provided preferences for prenatal testing after they had decided which test to have. Thus it is possible that their preferences were confounded by stage of decision making, and served as a post hoc justification of their choice. The fact that some women choosing amniocentesis assigned higher preference ratings to second- as compared to first-trimester diagnosis of a normal child, and to second- as compared to first-trimester thera- peutic abortion of an abnormal fetus, supports this possibility. In addition, women presenting for testing when their pregnancy is too advanced for chorionic villus sampling may favor amnio- centesis because it is their only viable option. Others have found that up to 71% of women choosing amniocentesis do so because their pregnancy has progressed too far for chorionic villus sampling to be performed [45].
Second, we assessed preferences using linear rating scales rather than standard reference gambles, to improve comprehension of the task [58]. Rating scales have shown intra-rater

Amniocentesis or Chorionic Villus Sampling for Prenatal Testing 1225
[59-611 and test-retest [62] reliabilities compar- able to those of standard gambles [62,63], and have demonstrated acceptable inter-rater re- liability [59]. Moderately high correlations between rating scale preferences and standard gamble utilities have been found in some studies [64], although not in others [63]. Although standard gambles, derived from the axioms of utility theory [37,65], are the reference method for measuring health outcomes, and are most appropriate for use in decision trees, they may demonstrate internal inconsistencies depending on the outcomes of the gamble [66].
Finally, we studied women who presented for prenatal testing for the indication of maternal age. Our results therefore cannot be generalized to women who seek testing because of a prior genetic abnormality. Because of their greater likelihood of requiring therapeutic abortion, these women often choose chorionic villus sampling [28,67], as decision-analytic models suggest that they should [30].
In conclusion, the preferences of pregnant women for the outcomes of prenatal testing were associated with their choice of amnio- centesis or chorionic villus sampling. The choices of prenatal test made by the majority of women were concordant with those of a de- cision analytic model that incorporated their preferences. Therefore, most pregnant women were able to convert their preferences for delayed diagnosis, therapeutic abortion, test-re- lated spontaneous abortion, and maternal mor- bidity, into an appropriate choice of prenatal test. These results suggest that women’s prefer- ences for prenatal testing may be useful for genetic counseling [47,48], and for quality- adjusting outcomes of clinical trials [68]. How- ever, because many women made choices that were discordant with their decision-analytic results, further research into the bases for their choices is warranted.
Acknowledgement-This project was supported by grant No. H.506945Ol Al from the Agency for Health Care Policy and Research.
REFERENCES
NICHD National Registry for Amniocentesis Study Group. Midtrimester amniocentesis for prenatal diag- nosis: safety and accuracy. JAMA 1976; 236: 1471-1476. Crandall BF, Howard J, Lebherz TB, Rubinstein L, Sample WF, Sarti D. Follow-up of 2000 second- trimester amniocenteses. Obstet Gynecol 1980; 56: 625-628. Tabor A, Philip J, Madsen M, Bang J, Obel EB,
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
IS.
16.
17.
18.
19.
20.
21.
22.
Norgaard-Pedersen B. Randomized controlled trial of genetic amniocentesis in 4606 low-risk women. Laneet 1986; 1: 1287-1293. Crane JP, Beaver HA, Cheung SW. First trimester chorionic villus sampling versus mid-trimester genetic amniocentesis: preliminary results of a controlled prospective trial. Prenat Diag 1988; 8: 355-366. Rhoads GG, Jackson LG, Schlesselman SE et al. The safety and efficacy of chorionic villus sampling for early prenatal diagnosis. N Engl J Med 1989; 320: 609-617. Canadian Collaborative CVS-Amniocentesis Clinical Trial Group. Multicentre randomized clinical trial of chorionic villus sampling and amniocentesis. Laneet 1989; 1: 1-6. Golbus MS, Loughman WD, Epstein CJ, Halbasch G, Stephens JD, Hall BD. Prenatal genetic diagnosis in 3000 amniocenteses. N Engl J Mad 1979; 300: 157-163. Polani PE, Alberman E, Alexander BJ er al. Sixteen years’ experience in counseling, diagnosis, and prenatal detection in one genetic centre: progress, results, and problems. J MedCenet 1979; 16: 166-175. Sauire JA. Nauth L. Ridler MAC. Sutton S. Timber- lake C. Prenatal diagnosis and o&ome of pregnancy in 2036 women investigated by amniocentesis. Hum Genet 1982; 61: 215-222. Young SR, Wade RV, Watt GW, Hixson ET, Dennis EJ. The results of one thousand consecutive prenatal diagnoses. Am J Obstet Gynecol 1983; 147: 181-188. Dacus JV, Wilroy RS, Summitt RL et al. Genetic amniocentesis: a twelve years’ experience. Am J Med Genet 1985; 20: 443-452. Benn PA, Hsu LYF, Carlson A, Tannenbaum HL. The centralized prenatal genetics screening program of New York City. III. The first 7000 cases. Am J Med Genet 1985; 20: 369-384. Hogge WA, Schonberg SA, Golbus MS. Chorionic vill;s sampling: experience in the first 1000 cases. Am J Obstet Gvnecol 1986: 154: 1249-1252. Sachs ES, jahoda MGJ, Kleijer WJ, Pijpers L, Gal- jaard H. Impact of first-trimester chromosome, DNA, and metabolic studies on pregnancies at high genetic risk: experience with 1000 cases. Am J Med Genet 1988; 29: 293-303. Jackson L. Prenatal genetic diagnosis by chorionic villus sampling (CVS). Bern Perinat 1985; 9: 209-218. Martin AO, Simpson JL, Rosinsky BJ, Elias S. Chori- onic villus sampling in continuing pregnancies. II. Cvtoaenetic reliabilitv. Am J Obstet Cvnecol 1986: 154: ljS3~1362. - Therkelsen AJ, Jensen PKA, Hertz JM, Smidt-Jensen S, Hahnemann N. Prenatal cytogenetic diagnosis after transabdominal chorionic villus sampling in the first trimester. Prenat Diag 1988; 8: 19-3i. _ NICHD CVS Studv Grouo. Diagnostic accuracv in chorionic villus saipling (CVS): iiitial findings from the U.S. Collaborative Study. Am J Hum Gmet 1988; 43: A242. Metaxotou C, Antsaklis A, Panagiotopoulou P, Mavrou A, Aravantinos D, Matsaniotis N. Prenatal diagnosis from chorionic biopsy samples. Clin Genet 1985; 28: 450. Simoni G, Fraccaro M, Gimelli G, Maggi F, Dagna Bricarelli F. False-positive and false-negative findings on chorionic villus sampling. Prenat Diag 1987; 7: _ _ 671-672. Leschot NJ, Wolf H, Verjaal M et al. Chorionic villi sampling: cytogenetic and clinical findings in 500 preg- na&es.-Br- Med J 1987; 295: 407-410.- Green JE. Dorfmann A, Jones SL. Bender S, Patton L, Schulman JD. Chorionic villus sampling: experience with an initial 940 cases. Obstet Gynecol 1988; 71: 208-2 12.

1226 PAUL S. HECKERLING ef al.
23.
24.
25.
26.
21.
28.
29.
30.
31.
32.
33.
34.
35.
36.
31.
38.
39.
40.
41.
42.
Firth HV, Body PA, Chamberlain P, MacKenzie IZ, Lindenbaum, RH, Huson SM. Severe limb abnormal- ities after chorion villus sampling at 56-66 days’ gestation. Lancet 1991; 337: 762-763. Schloo R, Miny P, Holzgreve W, Horst J, Lenz W. Distal limb deficiency following chorionic villus sampling? Am J Med Genet 1992; 42: 402-413. Peterson WF, Berry FN, Grace MR, Gulbranson CL. Second-trimester abortion by dilatation and evacua- tion: an analysis of 11,747 cases. Ohstet Gynecol 1983; 62: 1855190. Robinson GE, Garner DM, Olmsted MA, Shime J, Hutton EM, Crawford BM. Anxiety reduction after chorionic villus sampling and genetic amniocentesis. Am J Obstet Gynecol 1988; 159: 953-956. Spencer JW, Cox DN. Emotional responses of preg- nant women to chorionic villi sampling or amniocente- sis. Am J Obatet Gyneeol 1987; 157: 1155-l 160. Spencer JW, Cox DN. A comparison of chorionic villi sampling and amniocentesis: acceptability of pro- cedure and maternal attachment to pregnancy. Obstet Gynecol 1988; 72: 714-718. Burnhill MS. Reducing the morbidity of vacuum aspi- ration abortion. In: Zatuchni GI, Sciarra JJ, Speidel JJ, Eds Pregnancy Termination: Procedures, Safety, and New Developments. Hagerstown: Harper & Row; 1979: 136-148. Heckerling PS, Verp MS. Amniocentesis or chorionic villus sampling for prenatal genetic testing: a decision analvsis. J Clin Enidemiol 1991: 44: 6577670. Torrance GW. -Utility approach to measuring health-related quality of life. J Chron Dis 1987; 40: 593600. Hook EB, Cross PK, Schreinemachers DM. Chromo- somal abnormality rates at amniocentesis and in live born infants. JAMA 1983; 249: 2034-2038. Hook EB, Cross PK, Jackson L, Pergament E, Bram- bati B. Maternal age-specific rates of 47, f21 and other cytogenetic abnormalities diagnosed in the first trimester of pregnancy in chorionic villus biopsy spec- imens: comparison with rates expected from obser- vation at amniocentesis. Am J Hum Genet 1988; 42: 797-807. Hook EB. Evaluation and projection of rates of chromosome abnormalities in chorionic villus studies (CVS). Am J Hum Cenet 1988; 43: A108. Wilson RD, Kedrick V, Wittman BK, McGillivray B. Spontaneous abortion and pregnancy outcome after normal first-trimester ultrasound examination. Obstet Gynecol 1986; 67: 352-355. Gilmore DH, McNay MB. Spontaneous fetal loss in early pregnancy. Lancet 1985; 1: 107. Weinstein MC, Fineberg HV, Elstein AS, Frazier H’S, Neuhauser D, Neutra RR, McNeil BJ. Clinical De- cision Analysis. Philadelphia, PA: (W. B.) Saunders; 1980. Engelman L. Stepwise logistic regression. In: Dixon WJ, Engelman L, Hill MA, Jennrich MI, Eds BMDP Statistical Software Manual. Berkeley, CA: University of California Press: 1988: 941-969. McGovern MM, Goldberg JD, Desnick RJ. Accept- ability of chorionic villi sampling for prenatal diagno- sis. Am J Obstet Gynecol 1986; 155: 25-29. Lippman A, Perry TB, Mandel S, Cartier L. Chorionic villi sampling: women’s attitudes. Am J Med Genet 1985; 22: 395-401. Abramsky L, Rodeck CH. Women’s choices for fetal chromosome analysis. Prenat Diag 1991; I I: 23-28. Tunis SL, Golbus MS, Copeland KL, Fine BA, Rosinsky BJ, Seely L. Patterns of mood states in pregnant women undergoing chorionic villus sampling or amniocentesis. Am J Med Genet 1990; 37: 191-199.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
Sjogren B, Uddenberg N. Prenatal diagnosis and psychological distress: amniocentesis or chorionic vil- lus biopsy? Prenat Diag 1989; 9: 477-487. Caccia N, Johnson JM, Robinson GE, Barna T. Impact of prenatal testing on maternal-fetal bonding: chorionic villus sampling versus amniocentesis. Am J Obstet Gynecol 1991; 165: 1122-I 125. Brandenburg H, Van Der Zwan L, Jahoda MGJ, Stijnen T, Wladimiroff JW. Prenatal diagnosis in advanced maternal age. Amniocentesis or CVS, a patient’s choice or lack of information? Prenat Diag 1991; 11: 6855690. Pauker SG, Kassirer JP. Decision analysis. N Engl J Med 1987; 316: 250-258. Pauker SP, Pauker SG. Prenatal diagnosis: a directive approach to genetic counseling using decision analysis. Yale J Biol Med 1977; 50: 2755289. Pauker SP, Pauker SG. The amniocentesis decision: ten years of decision analytic experience. In: Eveers- Kiebooms G, Cassiman J-J, Van den Berghe H, d’Ydewalle G. Eds Genetic Risk, Risk Perception, and Decision Making. Birth Defects: Original Article Series 23. New York: Alan R. Liss; 1987: 151-169. Holmes MM, Rovner DR, Rothert ML, Elstein AS, Holzman GB, Hoppe RB, Metheny WP, Ravitch MM. Women’s and physicians’ utilities for health outcomes in estrogen replacement therapy. J Gen Intern Med 1987; 2: 1788182. Boyd NF, Sutherland HJ, Heasman KZ, Tritchler DL, Cummings BJ. Whose utilities for decision analysis? Med Decis Making 1990; IO: 58867. Pauker SP, Pauker-SG. The amniocentesis decision: an explicit guide for parents. In: Eustein CJ. Currv CJR. Packman S, Sherman S, Hall SD, Eds Risk, Commnni- cation, and Decision Making in Genetic Counseling. Birth Defects: Original Article Series XV(SC). New York: Alan R. Liss; 1979; 289-324. Elstein AS, Holzman GB, Ravitch MM, Metheny WA, Holmes MM, Hoppe RB, Rothert ML, Rovner DR. Comparison of physicians’ decisions regarding estro- gen replacement therapy for menopausal women and decisions derived from a decision analytic model. Am J Med 1986; 80: 246-258. Clancy CM, Cebul RD, Williams SV. Guiding individ- ual decisions: a randomized controlled trial of decision analysis. Am J Med 1988; 84: 2833288. Tversky A, Kahneman D. The framing of decisions and the psychology of choice. Science 1981; 211: 453-458. Bell DE. Regret in decision making under uncertainty. Operations Res 1982; 30: 961-981. Feinstein AR. The “chagrin factor” and qualitative decision analysis. Arch Intern Med 1985; 145: 125771259. Lopes LL. Decision making in the short run. J Exp Psycho1 (Human Learn Mem) 1981; 7: 3777385. d’Ydewalle G, Evers-Kiebooms G. Experiments on genetic risk perception and decision making: explora- tive studies. In: Evers-Kiebooms G, Cassiman J-J, Van den Berghe H, d’Ydewalle G, Eds Genetic Risk, Risk Perception, and Decision Making. Birth Defects: Orig- inal Article Series 23. New York: Alan R. Liss; 1987; 209-225. Patrick DL, Bush JW, Chen MM. Methods for measuring levels of well-being for a health status index. Health Serv Res 1973; 8: 228-245. Cadman D, Goldsmith C. Construction of social value or utility-based health indices: the usefulness of factorial experimental design plans. J Chron Dis 1986; 39: 643-651. Torrance GW. Preferences for health states: a review of measurement methods. Mead Johnson Symp Perinat Develop Med 1982; 20: 37-45.

Amniocentesis or Chorionic Villus Sampling for Prenatal Testing 1227
62.
63.
64.
65.
66.
67.
68.
O’Connor AM, Boyd NF, Till JE. Influence of elici- tation technique, position order and test-retest error on preferences for alternative cancer drug therapy. Nnrshsa Reseueh: Science for Oualitv of Care: Proc Tenth lhhmi Nursing Reaearch~Confknce. Toronto: University of Toronto; 1985. Torrance GW. Social preference for health states: an empirical evaluation of three measurement techniques. Socioecon Planning Sci 1976; 10: 129-136. Read JL, Quinn RJ, Berwick DM, Fineberg HV, Weinstein MC. Preferences for health outcomes: com- parison of assessment methods. Med Decis Making 1984; 4: 315-329. Keeny RL, Raiffa H. Decisiolls with Multiple Objec- tives: Preferences and Value Tradeoffs. New York: Wiley, 1976. Llewellyn-Thomas H, Sutherland HJ, Tibshirani R, Ciampi A, Till JE, Boyd NF. The measurement of uatients’ values in medicine. Med Decis Maklne 1982: 2: 449-462.
_
McCormack MJ, Rylance ME, MacKenzie WE, New- ton J. Patients’ attitudes following chorionic villus sampling. Prenat Wag 1990; 10: 253-255. Feeny DH, Torrance GW. Incorporating utility-based quality-of-life measures in clinical trials: Two examples. Med Care 1989; 27: Sl90-S204.
APPENDIX A
Preference Rating Questionnaire (iid This questionnaire is designed to determine your attitudes towards various possible outcomes of pregnancy related to prenatal genetic testing for chromosomal abnormalities.
Amniocentesis and chorionic villus sampling are tests to evaluate the possibility of a chromosomally-abnormal fetus.
Amniocentesis is performed during the 4th month of pregnancy, at a time when a woman is visibly pregnant and may have felt the fetus move. The results are available about 2 weeks after the test. An abortion performed because of an abnormal amniocentesis result would have to be per- formed after this time, and would possibly require inducing labor.
01)
(9 Chorionic villus sampling is performed at 25 months of
pregnancy, at a time when a woman is not yet visibly pregnant and has not felt the fetus move. The results are available about 1 week after the test. An abortion performed because of an abnormal chorionic villus sampling result could be performed before a woman was visibly pregnant or had felt the fetus move, and would not require inducing labor.
(3
We assume that for you the best outcome would be to give birth to a normal child, and that the worst outcome would be to give birth to a genetically abnormal child. If, on the visual scales shown below, the best outcome (a normal child) is worth 100 points, and the worst outcome (an abnormal child) is worth 0 points, please indicate the worth of each of the following outcomes by marking an “x” on the appropri- ate point on the scale:
04
(1)
(W
You decide to have an amniocentesis. As a result, for 4-5 months of your pregnancy, you don’t know whether your fetus is normal or abnormal. Two weeks after the test, the result is available, and shows a chromosomally normal fetus. At birth, the child is normal. l________________________l________________________ l 0 100 You decide to have a chorionic villus sampling. As a result, for 253 months of your pregnancy, you don’t know whether your fetus is normal or abnormal. One week after the test, the result is available, and shows a
(4
(4
(e)
0-J
chromosomally normal fetus. At birth, the child is normal. I________________________l________________________ 1 0 100 You decide not to have any prenatal genetic testing. Your pregnancy ends in a miscarriage. *______________________--I_________________________ 1 0 100 You decide to have an amniocentesis at 4 months. An amniocentesis can cause a miscarriage, although most miscarriages that occur after amniocentesis are due to other causes. Sometime after the test is performed, your pregnancy ends in a miscarriage. I________________________l________________~_______ 1 0 100 You decide to have a chorionic villus sampling at 2f months. A chorionic villus sampling can cause a mis- carriage, although most miscarriages that occur after chorionic villus sampling are due to other causes. Sometime after the test is performed, your pregnancy ends in a miscarriage. I________________________l_____-___________________ l 0 100 You decide to have an amniocentesis at 4 months. The result shows a chromosomally abnormal fetus. While you are deciding whether or not to have an abortion, the pregnancy ends in a miscarriage. The fetus is found to be abnormal, as predicted. *________________________I_________________________ l 0 100 You decide to have a chorionic villus sampling at 2; months. The result shows a chromosomally abnormal fetus. While you are deciding whether or not to have an abortion, the pregnancy ends in a miscarriage. The fetus is found to be abnormal, as predicted. I________________________I_________________________ * 0 100 You decide to have an amniocentesis at 4 months. The result shows a chromosomally abnormal fetus, and you decide to have an abortion. The aborted fetus is found to be abnormal, as predicted. I_____________________.__l________________________ 1 0 100 You decide to have a chorionic villus sampling at 2f months. The result shows a chromosomally abnormal fetus, and you decide to have an abortion. The aborted fetus is found to be abnormal, as predicted. l________________________l___-_____________________ 1 0 100 The same as question (h), but after the abortion you experience pain and vaginal bleeding, and require hos- pitalization and antibiotic therapy for infection. I________________________l____-____________________ * 0 100 The same as question (i), but after the abortion you experience pain and vaginal bleeding, and require hos- pitalization and antibiotic therapy for infection. *________________________I______________~__________ l 0 100 You decide to have an amniocentesis at 4 months. The test result shows a chromosomally abnormal fetus, and you decide to have an abortion. It turns out that the aborted fetus was normal, and that the test result was incorrect. l________________________I_________________________ 1 0 100
(m) You decide to have a chorionic villus sampling at 2; months. The test result shows a chromosomally abnor- mal fetus, and you decide to have an abortion. It turns out that the aborted fetus was normal, and that the test result was incorrect. l________________________I_____-____________________ * 0 100

228 PAUL S. HECKERLING et al.
APPENDIX B
Probabilities Used in the Decision Analyses
Probability AMN cvs
Spontaneous abortion* & Ages 30-34 0.028 Ages 35-39 0.039 Ages B 40 0.074
Chromosomal abnormalityt (excess over abnormal liveborn rate)$t Ages <35 0.007 1 (0.002 1)
36 0.0089 (0.0027) 37 0.0113 (0.0035) 38 0.0142 (0.0044) 39 0.0178 (0.0056) 40 0.0224 (0.0069) 41 0.0283 (0.0087) 42 0.0356 (0.0108) 43 0.0448 (0.0134) 44 0.0564 (0.0165)
245 0.0710 (0.0204)
Indeterminate test result 0
Chromosomal abnormality after an indeterminate test 0.08
False-negative test result 0.004
False-positive test result 0.0007
Morbidity after therapeutic abortion 0.014
0.033 0.044 0.079
0.0085 (0.0035) 0.0108 (0.0046) 0.0139 (0.0061) 0.0178 (0.0080) 0.0227 (0.0105) 0.0291 (0.0136) 0.0373 (0.0177) 0.0477 (0.0229) 0.0611 (0.0297) 0.0782 (0.0383) 0.1001 (0.0495)
0.011
-
0.004
0.001
0.006
*Assuming ultrasonic viability at 8-10 weeks gestation. With amniocentesis, 45% of spontaneous abortions were assumed to occur in the first trimester, and 55% were assumed to occur in the second and third trimesters. With chorionic villus sampling, 55% of spontaneous abortions were assumed to occur in the first trimester, and 45% were assumed to occur in the second and third trimesters.
tRepresents the rates of chromosomal abnormalities at the time of amniocentesis and chorionic villus sampling 132-341.
$The excess over abnormal liveborn rates represents abnormal fetuses that would have spontaneously aborted, but were instead terminated by therapeutic abortion because they were detected by prenatal testing. The probabilities of an abnormal child after a negative test result, and of a normal abortus after a positive test result, were calculated as Bayesian probability revisions using maternal age-adjusted abnormal liveborn rates, and the false-negative and false-positive rates of amniocen- tesis and chorionic villus sampling.