Embed Size (px)
Citation preview
Amiodarone in Pediatric Patients
MACDONALD DICK II, M.D., and WILLIAM A. SCOTX M.D.From the Division of Pediatric Cardiology, C.S, Mott Children's Hospital, and the Department of Pediatrics,
University of Michigan Medical School, Ann Arbor, Michigan
DICK M, II, and SCQTT WA; Amiodarone in pediatric patients. The reported world clinical experienceof amiodarone in children is revieioed; the known age-dependent electrophysiological and pharmacokineticcharacteristics of amiodarone are examined; and guidelines for the use of amiodarone in children are suggested.(Clin. Prog. Electrophysiol. Pacing, Vol. 4, 1986)
pharmacokinetics, side effects, supraventricular tachycardia, ventricular fibrillation, ventricular tachycardia.
Recent interest in cardiac arrhythmias in chil-dren has been motivated by a growing aware-ness and understanding of primai}^ rhythm dis-orders in the young as well as by an increasingemergence of cardiac arrhythmias followingsurgical repair of many congenital heart de-fects. An increased understanding and use ofboth conventional and investigational antiar-rhythmic medications in children has, by neces-sity, accompanied this clinical development. Ofparticular interest is the emergence of amio-darone hydrochloride, an iodinated benzofuranderivative, in the treatment of arrhythmias. Thisarticle focuses on the electophysiology, pharma-cology, experience, side effects, dosages, andindications for amiodarone especially relevantto the pediatric patient.
Electrophysiology and Pharmocology
The electrophysiological effects and pharma-cology of amiodarone are reviewed elsewherein this issue. Among the observed electrophys-iological changes induced by amiodarone area slowing of the spontaneous sinus node dis-charge rate, slowing of atrioventricular conduc-tion, and prolongation of atrial and ventricular
Address for reprint: Macdonald Dick U, M.D., F1123, Box0204.C-S. Motl Children's Hospital, University of MichiganMedical Center, 1500 E. Medical Center Drive, Ann Arbor, MI48109-0204.
effective refractory periods.- Both acute intra-venous and chronic oral amiodarone prolongadult human and canine ventricular repolariza-tion (type III effects)^ and exhibit rate-relatedprolongation of the ventricular action potentialas well as QRS duration (type I effects)"* Re-cent work by Yabek and associates suggestsimportant age-dependent effects of amio-darone.^ Acute data from the neonatal canineventricle have demonstrated no change in ven-tricular repolarization, suggesting a decreasedsensitivity to amiodarone in the young mam-malian myocardium. Further, amiodarone pro-duces a greater concentration-dependent short-ening of the action potential and effective re-fractory period of neonatal canine Purkinjefibers when compared to the effects on the adultcanine Purkinje fiber. In contrast, rate-relateddecreases in the action potential amplitude and^max ^^ both neonatal and adult tissues aresimilar, and thus are not age-dependent. Thesefindings suggest that, when compared to theadult myocardium, type III effects may be lessoperative in the immature myocardium inwhich dispersion of refractoriness is minimal.Furthermore, the rate-related type I antiar-rhythmic action of amiodarone may be of par-ticular significance in the young in whom boththe baseline and tachycardia heart rate tend tobe higher.-
The pharmacokinetics of orally administeredamiodarone are significantly different between
522 Clinical Progress in Electrophysiology and Pacing Vol 4, No. 6, 1986
AMIODARONE IN PEDIATRIC PATIENTS
the adult and child. The time of onset of thera-peutic effect is four to five days in the pediatricpopulation compared to nine to ten days in theadult population.^^ Although the eliminationof the drug by both groups is biexponential withan initial rapid phase followed by a more pro-longed second phase due to clearance from tis-sue stores, the half-life of this elimination is twoto three weeks in children compared to two tofour months in the adult, perhaps due to amore rapid equilibration of the drug betweenplasma and tissue in the young.^^ In bothchildren and adults, amiodarone is metabolizedin part by the liver to the nonactive desethylam-iodarone; this metabolite and the parent drugare then cleared by the liver. Therapeuticplasma concentrations, considered to be be-tween 1.0 and 2.5 / g/ml, correlate only fairlywith either beneficial effect or side effects. - "On the other hand, correlation has been shownbetween therapeutic antiarrhythmic effect andprolongation of the QT interval in adults receiv-ing 400-600 mg of amiodarone per day."
Information regarding the fetal pharmacologyof amiodarone is incomplete. A 27-week gesta-tion fetus with atrial flutter (260 bpm) wastreated by oral administration of amiodarone(in conjunction with verapamil) to the mother.The fetal ventricular rate slowed with resolutionof fetal heart failure. The fetus progressed toterm without adverse outcome; direct currentcardioverison to sinus rhythm was achieved at24 hours of age.^ In two other women whowere undergoing treatment for arrhythmia inthe third trimester, the fetal-to-maternal plasmaconcentration ratio was 0.2 and 0.25 withoutadverse side effects. In another report, themother was treated with amiodarone (200 mgper day maintenance dose) for supraventriculartachycardia beginning at the 16th week. Deliv-ery at 39 weeks of a normal newborn was un-eventful. Nine hours after the last maternaldose, the cord blood amiodarone concentrationwas 0.08 ^g/ml, the placenta serum concentra-tion, 0.23 /ig/ml, and the placental tissue con-centration, 7.2 Mg/g ' similar to reported hearttissue concentrations after chronic therapy.^The mother's amiodarone serum level was0.8 /ig/ml. Maternal and infant thyroid studies
were normal. At two weeks of age the child'samiodarone serum was 0.06 figlrrd. The infant'sQTc was 0.49 seconds at 24 hours of age, and0.39 seconds at 7 weeks of age.^ Thus thefetal-to-matemal serum concentration ratio inthis infant at delivery was approximately 0.1,demonstrating transplacental passage but noadverse fetal effects aiter continuous exposureto amiodarone beginning early in the sec-ond trimester. This small experience suggeststhat amiodarone may be safe in the second andthird trimester. On the other hand, since thereare no reports of first-trimester use, and becauseof the widespread tissue distribution as well asthe multiple organ toxicity in the adult, the pos-sibility of teratogenesis during the first trimes-ter may be great; thus, we suggest that the drugshould not be used in early pregnancy, andperhaps only sparingly in later pregnancy.
Clinical Experience
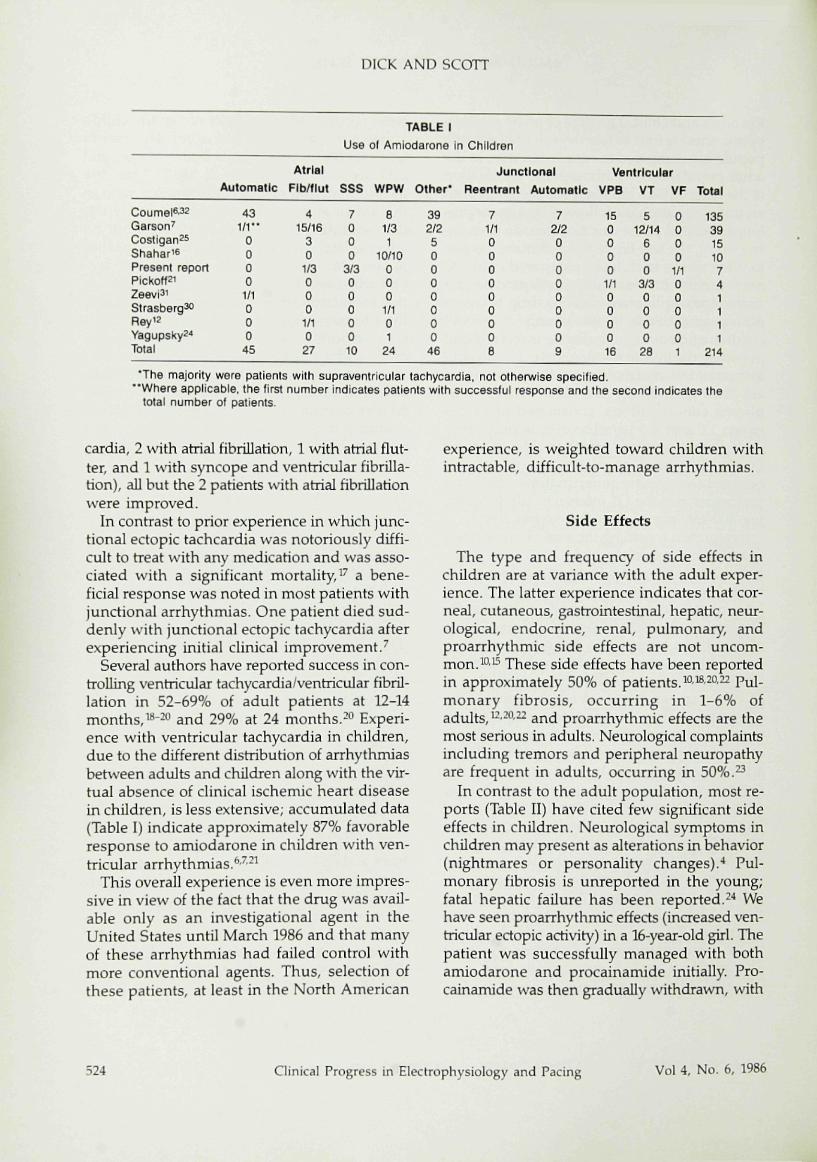
Amiodarone has been remarkably effective inreducing the rate and frequency of either auto-matic or reentrant supraventricular and ventric-ular arrhythmias in children. We were able tofind detailed documentation of approximately200 children reported in the literature (Table I),the vast majority reported by Coumel." Amio-darone was effective in controlling most atrialarrhythmias. Because of its effect of prolongingthe refractory period of the accessory pathwayconnection as well as decreasing the conductionvelocity of the circus movement in differentparts of the circuit, " amiodarone is especiallyuseful for control of arrhythmias in patientswith the Wolff-Parkinson-White syndrome,^including children. ' Coumel^ reports fair togood (normal sinus rhythm or a marked de-crease in frequency and rate of the tachycardia)in 92% (86 of 93) of children with atrial arrhyth-mias and 85% of children with ventricular ar-rhythmias. Garson^ reported complete or par-tial effectiveness of amiodarone in 96% of chil-dren with atrial flutter, 86% of children withventricular tachcardia, and 78% of patients withsupraventricular tachycardia (overall success87%). Among our 7 patients who have receivedamiodarone (3 with supraventricular tachy-
Vol 4, No. 6, 1986 Clinical Progress in Electrophysiology and Pacing 523
DICK AND SCOTT
Coume|6.32Garson'Costigan25ShatiariePresent reportPickotf2'2eevi3iStrasberg30Rey'2Yagupsky2'*Total
Automatic
431/1"
00001/1000
45
Atrial
FIb/ilut
415/16
30
1/3000
1/1027
Use
sss
7000
3/30000010
1rABLE 1
of Amiodarone In
WPW
81/31
10/100001/101
24
Other*
392/250000000
46
Children
Junctlonal
Reentrant ,
71/100000c008
VentricularAutomatic VPB
72/2000000009
150000
1/1000016
VT
512/14
600
3/30000
28
VF
0000
1/1000001
ToUl
135391510741111
214
*The majority were patients with supraventricular tachycardia, not otherwise specified."Where applicable, the first number indicates patients with successlul response and Ihe second indicates the
total number of patients.
cardia, 2 with atrial fibrillation, 1 with atrial flut-ter, and 1 with syncope and ventricular fibrilla-tion), all but the 2 patients with atrial fibrillationwere improved.
In contrast to prior experience in which junc-tional ectopic tachcardia was notoriously diffi-cult to treat with any medication and was asso-ciated with a significant mortality, ^ a bene-ficial response was noted in most patients withfunctional arrhythmias. One patient died sud-denly with junctional ectopic tachycardia afterexperiencing initial clinical improvement/
Several authors have reported success in con-trolling ventricular tachycardia/ventricular fibril-lation in 52-69% of adult patients at 12-14months,i* --* * and 29% at 24 months.-'^ Experi-ence with ventricular tachycardia in children,due to the different distribution of arrhythmiasbetween adults and children along with the vir-tual absence of clinical ischemic heart diseasein children, is less extensive; accumulated data(Table I) indicate approximately 87% favorableresponse to amiodarone in children with ven-tricular arrhythmias.^'"^
This overall experience is even more impres-sive in view of the fact that the drug was avail-able only as an investigational agent in theUnited States until March 1986 and that manyof these arrhythmias had failed control withmore conventional agents. Thus, selection ofthese patients, at least in the North American
experience, is weighted toward children withintractable, difficult-to-manage arrhythmias.
Side Effects
The type and frequency of side effects inchildren are at variance with the adult exper-ience. The latter experience indicates that cor-neal, cutaneous, gastrointestinal, hepatic, neur-ological, endocrine, renal, pulmonary, andproarrhythmic side effects are not uncom-jT Qj lo.L These side effects have been reportedin approximately 50% of patients.^ ' -^ ' Pul-monary fibrosis, occurring in 1-6% ofadults,' •-' •" and proarrhythmic effects are themost serious in adults. Neurological complaintsincluding tremors and peripheral neuropathyare frequent in adults, occurring in 50%.^
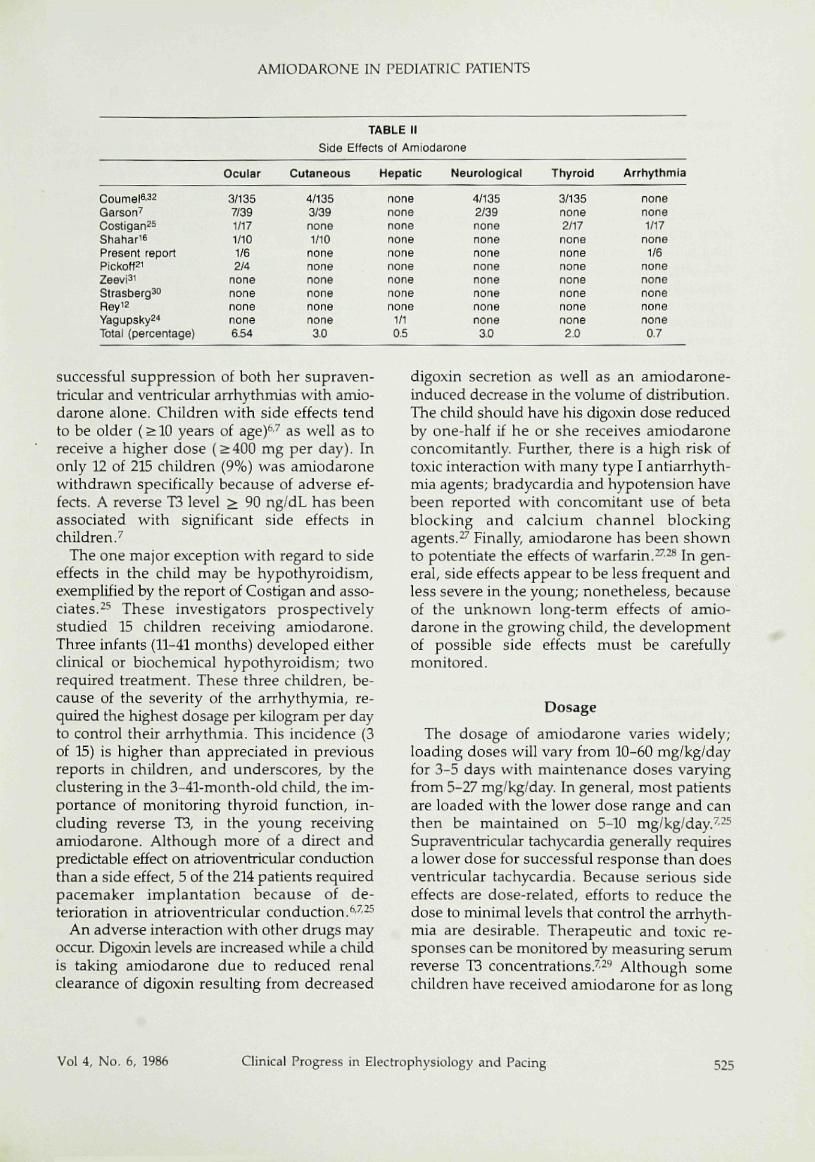
In contrast to the adult population, most re-ports (Table II) have cited few significant sideeffects in children. Neurological symptoms inchildren may present as alterations in behavior(nightmares or personality changes).•• Pul-monary fibrosis is unreported in the young;fatal hepatic failure has been reported.' '* Wehave seen proarrhythmic effects (increased ven-tricular ectopic activity) in a 16-year-old girl. Thepatient was successfully managed with bothamiodarone and procainamide initially. Pro-cainamide was then gradually withdrawn, uith
524 Clinical Progress in Electrophysiology and Pacing Vol 4, No. 6, 1986
AMIODARONE IN PEDIATRIC PATIENTS
Coumel '32Garson^Costigan^sShahariePresent reportPickoff2iZeevi^iStrasberg30Reyi2YagupskyS"*Total (percentage)
Ocular
3/1357/391/171/101/62/4
nonenonenonenone6.54
TABLE IISide Effects of Amiodarone
Cutaneous
4/1353/39none1/10
nonenonenonenonenonenone3.0
Hepatic
nonenonenonenonenonenonenonenonenone
1/10.5
Neurological
4/1352/39nonenonenonenonenonenonenonenone3.0
Thyroid
3/135none2rt7nonenonenonenonenonenonenone2.0
Arrhythmia
nonenone1/17
none1/6
nonenonenonenonenone0.7
successful suppression of both her supraven-tricular and ventrictilar arrhythrruas with amio-darone alone. Children with side effects tendto be older (> 10 years of age)" '' as well as toreceive a higher dose {>400 mg per day). Inonly 12 of 215 children (9%) was amiodaronewithdrawn specifically because of adverse ef-fects. A reverse T3 level > 90 ng/dL has beenassociated with significant side effects inchildren/
The one major exception with regard to sideeffects in the child may be hypothyroidism,exemplified by the report of Costigan and asso-ciates.-^ These investigators prospectivelystudied 15 children receiving amiodarone.Three infants {11-41 months) developed eitherclinical or biochemical hypothyroidism; tworequired treatment. These three children, be-cause of the severity of the arrhythymia, re-quired the highest dosage per kilogram per dayto control their arrhythmia. This incidence {3of 15) is higher than appreciated in previousreports in children, and underscores, by theclustering in the 3-41-month-old child, the im-portance of monitoring thyroid function, in-cluding reverse T3, in the young receivingamiodarone. Although more of a direct andpredictable effect on atrioventricular conductionthan a side effect, 5 of the 214 patients requiredpacemaker implantation because of de-terioration in atrioventricular conduction. ' - ^
An adverse interaction with other drugs mayoccur. Digoxin levels are increased while a childis taking amiodarone due to reduced renalclearance of digoxin resulting from decreased
digoxin secretion as well as an amiodarone-induced decrease in the volume of distribution.The child should have his digoxin dose reducedby one-half if he or she receives amiodaroneconcomitantly. Further, there is a high risk oftoxic interaction with many type I antiarrhyth-mia agents; bradycardia and hypotension havebeen reported with concomitant use of betablocking and calcium channel blockingagents.-'' Finally, amiodarone has been shownto potentiate the effects of warfarin.^-^ In gen-eral, side effects appear to be less frequent andless severe in the young; nonetheless, becauseof the unknown long-term effects of amio-darone in the growing child, the developmentof possible side effects must be carefullymonitored.
Dosage
The dosage of amiodarone varies widely;loading doses will vary from 10-60 mg/kg/dayfor 3-5 days with maintenance doses varyingfrom 5-27 mg/kg/day. In general, most patientsare loaded with the lower dose range and canthen be maintained on 5-10 mg/kg/day.'-^''Supraventricular tachycardia generally requiresa lower dose for successful response than doesventricular tachycardia. Because serious sideeffects are dose-related, efforts to reduce thedose to minimal levels that control the arrhyth-mia are desirable. Therapeutic and toxic re-sponses can be monitored by measuring serumreverse T3 concentrations/-'' Although somechildren have received amiodarone for as long
Vol 4, No. 6, 1986 Clinical Progress in Eiectrophysiology and Pacing 525
DICK AND SCOTT
as six years,*" more long-term (more than oneyear) experience in children is limited.
Indications and Conclusion
Amiodarone has many of the attributes of theideal universal antiarrhythmic agent. It has along half-life, can be administered once a day,and often less frequently, is highly effective,especially in supraventricular tachycardia, andappears to be well tolerated in children. None-theless, the toxicit}^ although considerably lessin terms of lethal dose by weight compared toother antiarrhythmic agents, involves virtuallyevery organ system. Its effects on the growingchild are unknown and should be consideredpotentially very serious. Thus, amiodaroneshould be reserved for the child with life-threat-ening and/or cardiac disabling arrhythmias onlyafter other forms of treatment have been ex-hausted. Although the drug has been releasedin the United States by the FDA, its use is con-fined to adults with life-threatening ventriculararrhythmias. Thus, its use in children shouldbe reserved for clearly life-threatening or intract-able disabling arrhythmias until further data re-garding its effect on human development areavailable.
References
1. Dick, M., and Campbell, R.M.: Advances in themanagement of cardiac arrhythmias in children.Pediatr. Clin. North Am., 31:1175, 1984.
2. Singh, B.N., and Vaughn Willianns, E.M,,; Theeffects of amiodarone, a new anti-anginal drug,on cardiac muscle. Br. }. Pharmacol. 39:657, 1970.
3. Tuna, I.C., Qi, A., Gomick, C , el al.: Kinetics ofelectTophysiologic changes during oral loading ofamiodarone and after withdrawal of amiodaronein the unsedated dog. Circulation, 72:1380, 1985.
4. Morady, R, DiCarlo, L.A., Krol, R.B., et al.; Acuteand chronic effects of amiodarone in ventricularrefractoriness, interventTicular conduction andventricular tachycardia induction. /. Am. Coll.Cardiol.. 7:148, 1986.
5. Yabek, S.M., Kato, R., and Singh, B.N.: Acuteeffects of amiodarone on the electrophysiologicproperties of isolated neonatal and adult cardiacfibers. /. ^ "1 . Coll. CardioL, 5:1109, 1985.
6, Coumel, P., and Fidelle, J.: Amiodarone in thetreatment of cardiac arrhythmias in children: Onehundred thirty-five cases. Am. Heart j . , 100:1063,1980.
7 Carson, Jr., A., Gillette, P.O., and McVey, R:Amiodarone treatment of critical arrhythmias inchildren and young adults. /. Atn. Coll. Cardiol.,4:749, 1984,
8. Latini, R, Tognoni, C , and Kates, R.E.; Clinicalpharmacokinetics of amiodarone. Clin.Phamiacokitietics. 9:136, 1984.
9, Rotmensch, H.H,, Belhassen, B., Swanson, B.N.,et al.: Steady-state serum amiodaroneconcentrations: Relationships with antiarrhythmicefficacy and toxicity. Ann. Intern. Med.. 10:462,1984.
10. Raeder, E.A., Podrid, P.J., and Lown, B.: Sideeffects and complications of amiodarone therapy.Am. Heart J.. 109:975, 1985.
11. Torres, V., Tepper, D., Flowers, D, et al.: QTprolongation and the antiarrhythmic efficacy ofamiodarone. /. Am. Coll. Cardiol., 7:142, 1986.
12. Rey, E. Duperron, L., Cauthier, R., et al.:Transplacental treatment of tachycardia-inducedfetal heart failure with verapamil and amiodarone:A case report. Am. J. Obstet. GynecoL, 153:311,1985.
13. Penn, I.M., Barrett, P.A., Pannikote, V, et al.:Amiodarone in pregnancy. Am. J. Cardiol., 56:196,1985.
14. Wellens, H.J.J., Lie, K.I., Bar, F.W., et al.: Effectof amiodarone in the Wolff-Parkinson-Whitesyndrome. Am. J. Cardiol., 38:189, 1976.
15. Rosenbaum, M.B., Chiale, PA., Halpern, M.S.,et al,: Clinical efficacy of amiodarone as anantiarrhythniic agent. Am. J. Cardioi. 58:934, 1976.
16. Shahar, E., Barzilay, Z., Frand, M., et al.:Amiodarone in control of sustainedtachyarrhythmias in children with Wolff-Parkinson-White syndrome. Pediatrics, 72:813,1983.
17. Garson, Jr., A., and Gillette P C : Junctionalectopic tachycardia in children:Electrocardiography, electrophysiology andpharmacologic response. Am. }. Cardiol.. 44:298,1979.
18. Morady, F., Sauve, M.J., Malone, P., et aL: Long-term efficacy and toxicity of high-dose amiodaronetherapy for ventricular tachycardia or ventricularfibrillation. Am. /. Cardiol., 52:975, 1983.
19. Heger, J.J., Prystowsky, E.N., Jackman, W.M., etal.: Amiodarone: Clinical efficacy andelectrophysiology during long-term therapy forrecurrent ventricular tachycardia or ventricular
526 Clinical Progress in Electrophysiology and Pacing Vol 4, No. 6, 1986
AMIODARONE IN PEDIATRIC PATIENTS
fibrillation. N. Efiy/. /. Med.. 305:539, 1981.20. Fogoros, R.N., Anderson, K.R, Winkle, R.A., et
al.; Amiodarone: Clinical efficacy and toxicity in96 patients with recurrent, drug-refractoryarrhythmias. Circulation, 68:88, 1983.
21. Pickoff, A.S., Singh, S., Flinn, C.)., et al.: Use ofcuniodarone in the therapy of primary ventriculararrhythmias in children. Dro. Phannncol. Ther.,6:73," 1983.
22. Smith, W.M., Lubbe, W.F., Whitlock, R.M., et al.:Long-term tolerance of amiodarone treatment forcardiac arrhythmias. -4m. /. Cardioi. 57:1288, 1986.
23. Charness, M.E., Morady, R, Scheinman, M.M.:Frequent neurologic toxicity associated withamiodarone therapy. Neurology. 669, 1984.
24. Yagupsky, P., Gonzala, E., Sofer, S., et al.: Fatalhepatic failure and encephalopathy associatedwith amiodarone. /. Pediatr.. 107:967, 1985.
25. Costigan, D.C., Holland, F.J., Daneman, D., et al.:Amiodarone therapy effects on childhood thyroidfunction. Pediatrics. 77:703, 1986.
26. Koren, G., Hesslein, P.S., and MacLeod, S.M.:
Digoxin toxicity associated wth amiodaronetherapy in children. /. Pediatr., 104:467, 1984.
27. Marcus, F.I.: Drug interactions with amiodarone.Am. Heart J., 106:924, 1983.
28. Hamer, A., Peter, T., Mandel, W.J., et al.: Thepotentiation of warfarin anticoagulation byamiodarone. Circulation. 65:1025, 1982.
29. Nademanee, K., Singh, B.N., Hendrickson, J.A.,et al.: Pharmacokinetic significance of serumreverse Tj levels during amiodarone treatment: Apotential method for monitoring chronic drugtherapy. Circulation. 66:202, 1982.
30. Strasberg, B., Davidson, E., and Berand, M.:Amiodarone-induced sinotrial block. Int. }.Cardioi, 8:214, 1985.
31. Zeevi, B., Berant, M., Sclarovsky, S., et al.:Treatment of multifocal atrial tachycardia withamiodarone in a child with congenital heartdisease. Am. J. Cardioi, 57:344, 1986.
32. Coumel, P., Lucet, V., and Ngoc, D D.: The useof amiodarone in children. PACE. 6:930, 1983.
Vol 4, No. 6, 1986 Clinical Progress in Electrophysiology and Pacing 527






























