Embed Size (px)
Citation preview
Allergic Rhinitis and Allergic Rhinitis and AsthmaAsthma
Dean TeyPaediatric Allergist & Immunologist
FRACP Lecture Monday 17th May 2010FRACP Lecture Monday 17th May 2010
Talk OverviewTalk Overview
1. Background1. Background2. Allergic rhinitis3 Asthma3. Asthma
Talk OverviewTalk Overview
1. Background1. Background2. Allergic rhinitis3 Asthma3. Asthma

Bi d l?Big deal?
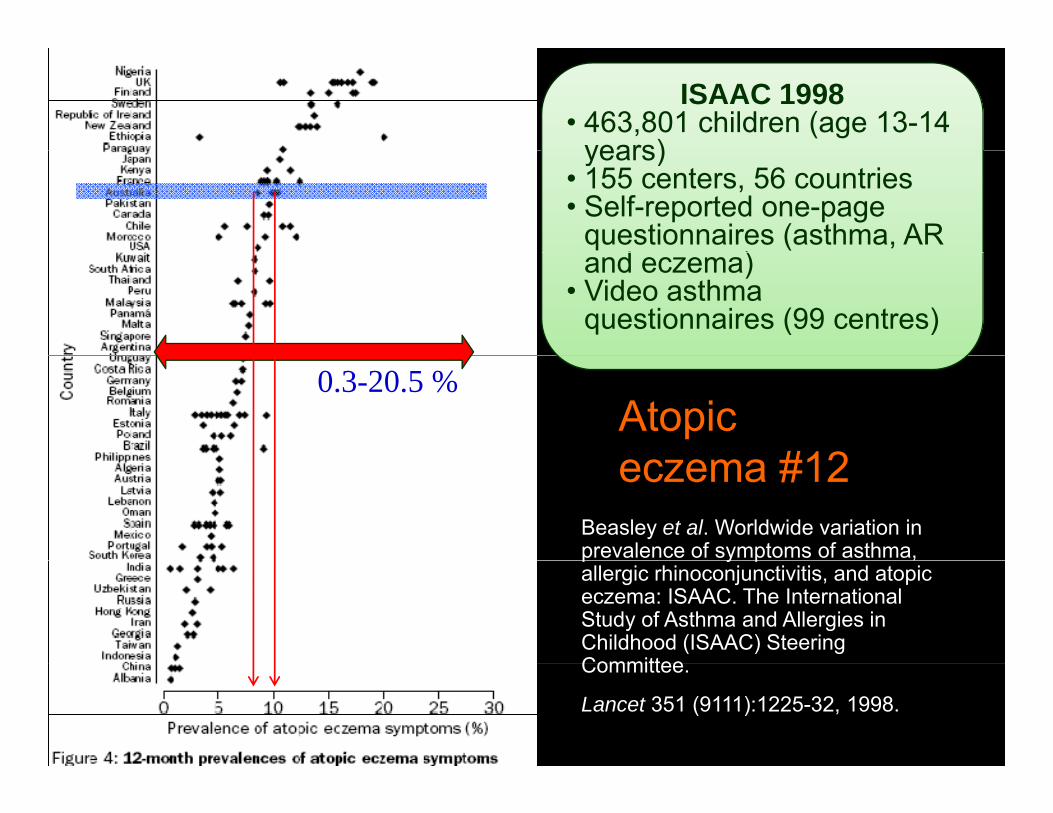
ISAAC 1998• 463,801 children (age 13-14
years)years)• 155 centers, 56 countries• Self-reported one-page
questionnaires (asthma, AR d )and eczema)
• Video asthma questionnaires (99 centres)
Atopic #12
0.3-20.5 %
Beasley et al. Worldwide variation in prevalence of symptoms of asthma,
eczema #12
p y p ,allergic rhinoconjunctivitis, and atopic eczema: ISAAC. The International Study of Asthma and Allergies in Childhood (ISAAC) Steering CommitteeCommittee.
Lancet 351 (9111):1225-32, 1998.
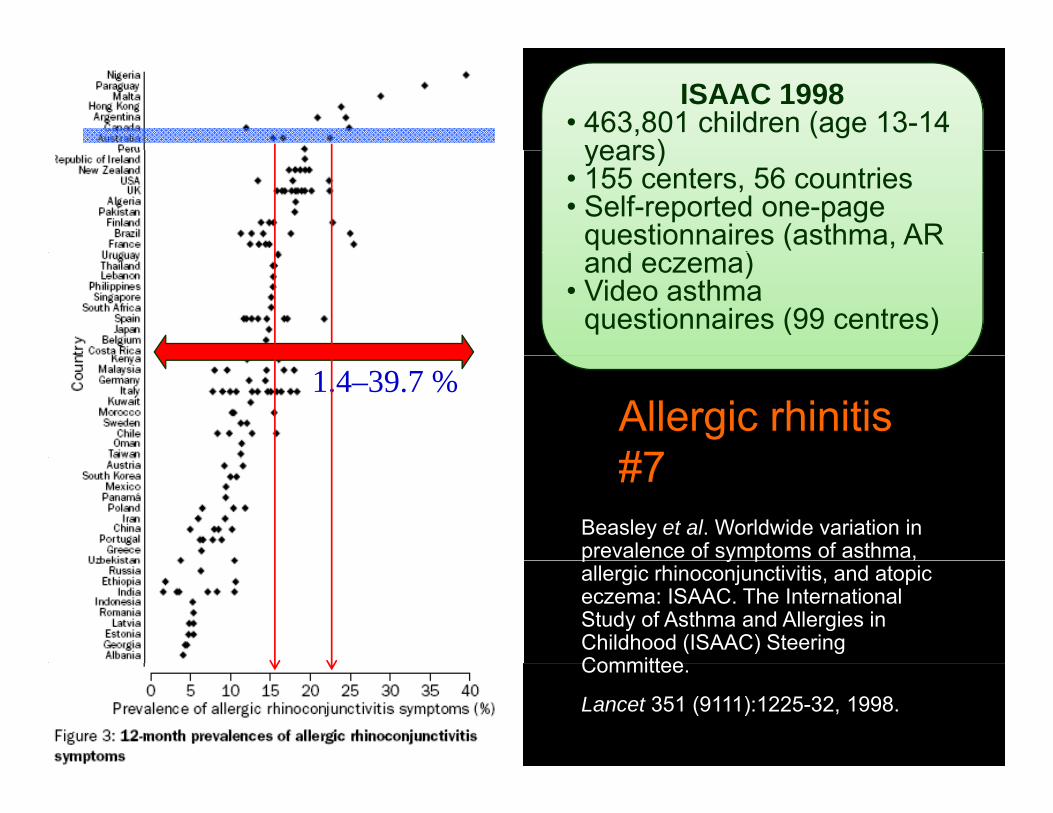
ISAAC 1998• 463,801 children (age 13-14
years)years)• 155 centers, 56 countries• Self-reported one-page
questionnaires (asthma, AR d )and eczema)
• Video asthma questionnaires (99 centres)
1.4–39.7 %Allergic rhinitis #7
Beasley et al. Worldwide variation in prevalence of symptoms of asthma,
#7
p y p ,allergic rhinoconjunctivitis, and atopic eczema: ISAAC. The International Study of Asthma and Allergies in Childhood (ISAAC) Steering CommitteeCommittee.
Lancet 351 (9111):1225-32, 1998.
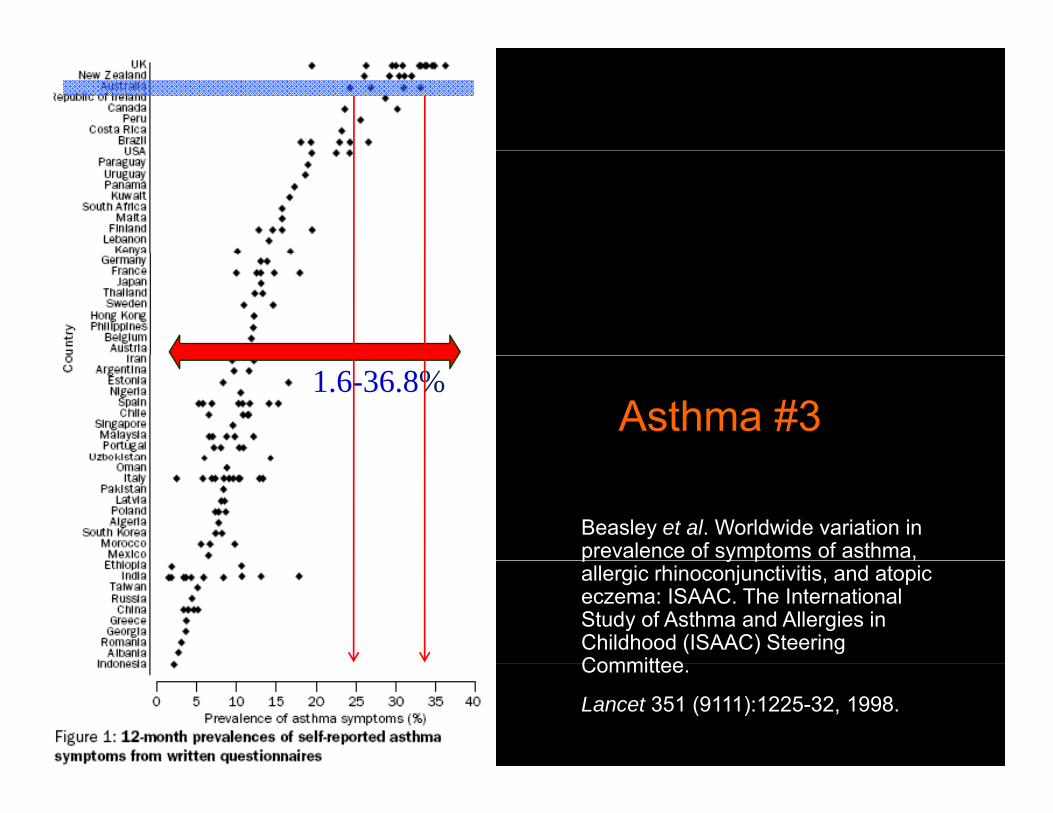
1.6-36.8%Asthma #3
Beasley et al. Worldwide variation in prevalence of symptoms of asthma, p y p ,allergic rhinoconjunctivitis, and atopic eczema: ISAAC. The International Study of Asthma and Allergies in Childhood (ISAAC) Steering CommitteeCommittee.
Lancet 351 (9111):1225-32, 1998.
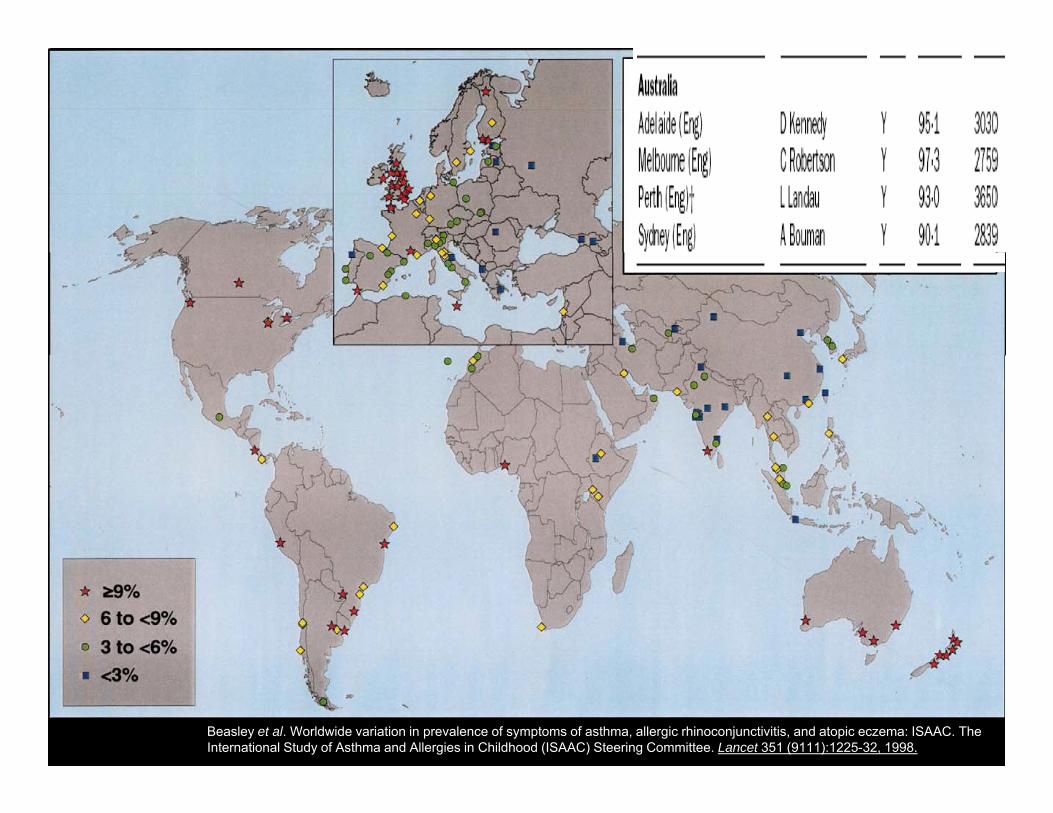
Beasley et al. Worldwide variation in prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and atopic eczema: ISAAC. The International Study of Asthma and Allergies in Childhood (ISAAC) Steering Committee. Lancet 351 (9111):1225-32, 1998.
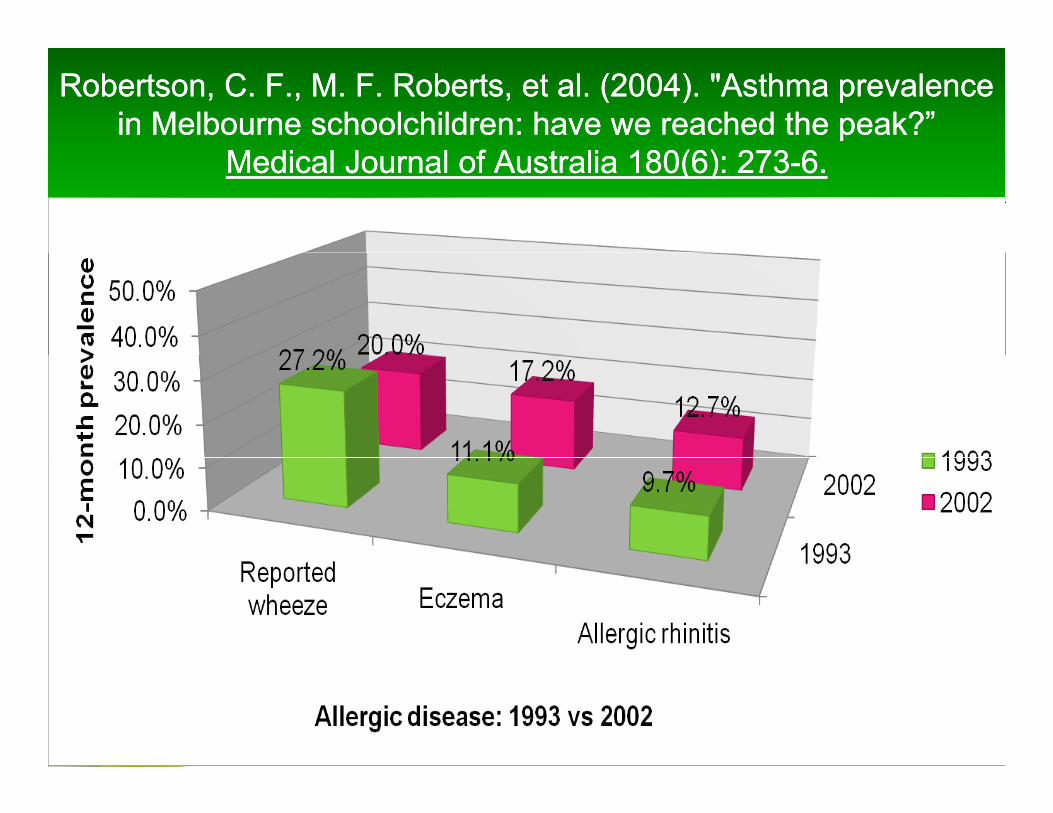
Robertson, C. F., M. F. Roberts, et al. (2004). "Asthma prevalence Robertson, C. F., M. F. Roberts, et al. (2004). "Asthma prevalence in Melbourne schoolchildren: have we reached the peak?”in Melbourne schoolchildren: have we reached the peak?”
M di l J l f A li 180(6) 273M di l J l f A li 180(6) 273 66Medical Journal of Australia 180(6): 273Medical Journal of Australia 180(6): 273--6.6.
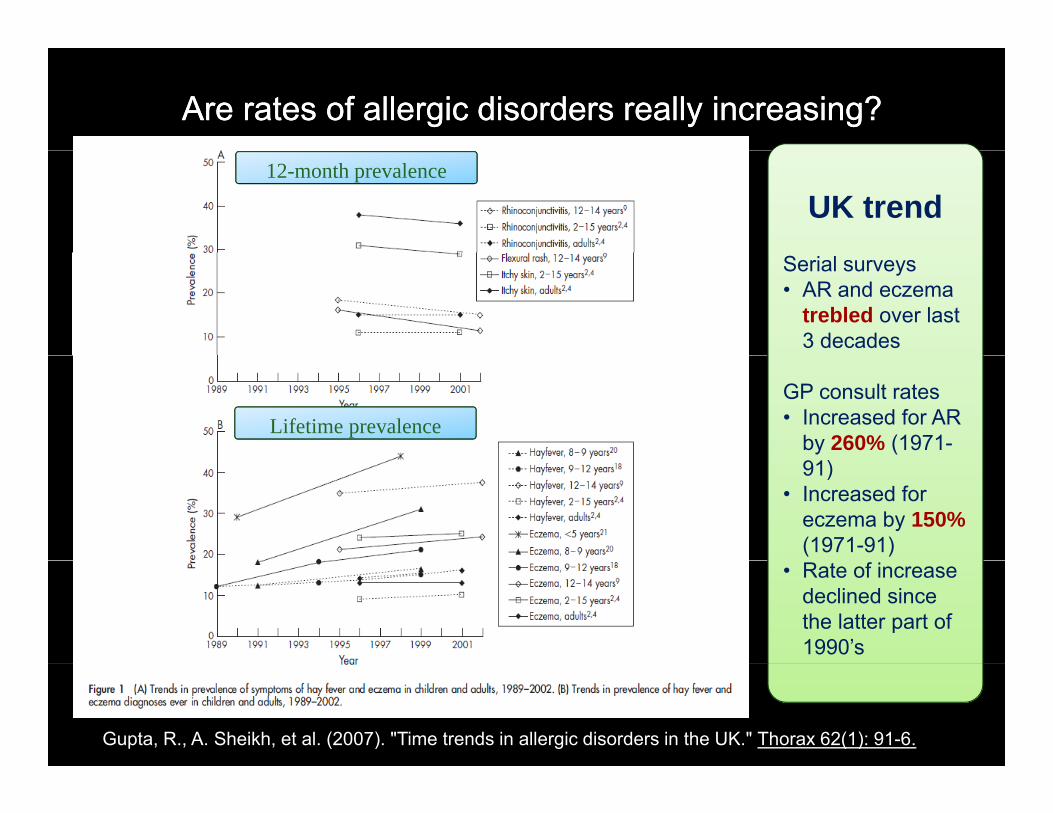
Are rates of allergic disorders really increasing?Are rates of allergic disorders really increasing?
UK trend12-month prevalence
Serial surveys• AR and eczema
trebled over last 3 decades
GP consult rates• Increased for AR
by 260% (1971-Lifetime prevalence
91)• Increased for
eczema by 150% (1971-91)
• Rate of increase declined since the latter part of 1990’s
Gupta, R., A. Sheikh, et al. (2007). "Time trends in allergic disorders in the UK." Thorax 62(1): 91-6.
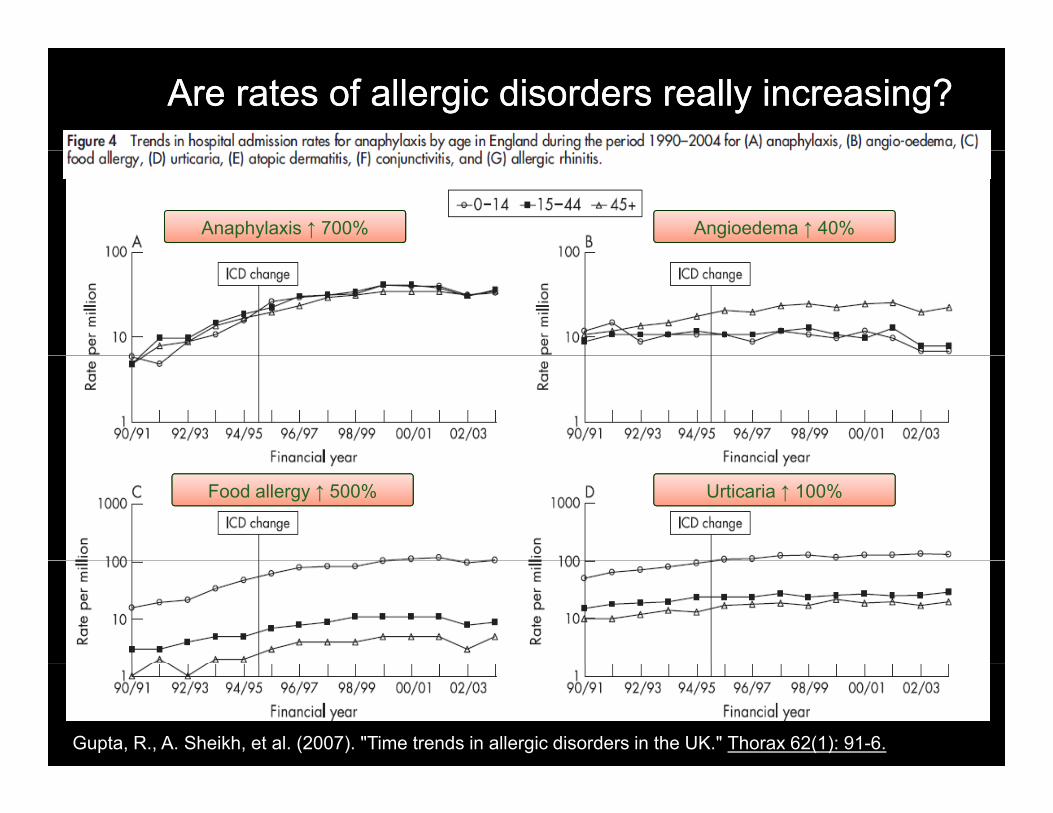
Are rates of allergic disorders really increasing?Are rates of allergic disorders really increasing?
Anaphylaxis ↑ 700% Angioedema ↑ 40%
Food allergy ↑ 500% Urticaria ↑ 100%
Gupta, R., A. Sheikh, et al. (2007). "Time trends in allergic disorders in the UK." Thorax 62(1): 91-6.
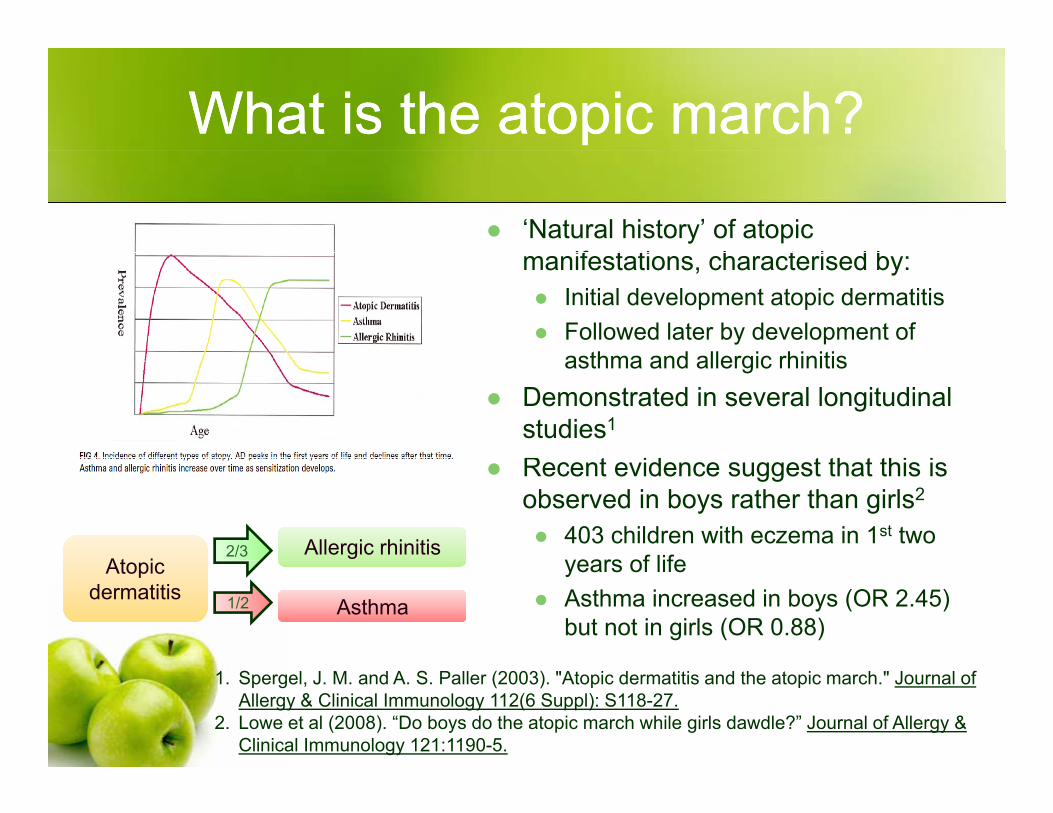
What is the atopic march?What is the atopic march?
‘Natural history’ of atopic if t ti h t i d bmanifestations, characterised by:
Initial development atopic dermatitisFollowed later by development of
th d ll i hi itiasthma and allergic rhinitisDemonstrated in several longitudinal studies1
R t id t th t thi iRecent evidence suggest that this is observed in boys rather than girls2
403 children with eczema in 1st two years of lifeAt i
Allergic rhinitis2/3 years of lifeAsthma increased in boys (OR 2.45) but not in girls (OR 0.88)
Atopic dermatitis
Asthma1/2
1. Spergel, J. M. and A. S. Paller (2003). "Atopic dermatitis and the atopic march." Journal of Allergy & Clinical Immunology 112(6 Suppl): S118-27.
2. Lowe et al (2008). “Do boys do the atopic march while girls dawdle?” Journal of Allergy & Clinical Immunology 121:1190-5.

The economic impact of allergic disease in Australia: The economic impact of allergic disease in Australia: not to be sneezed at. not to be sneezed at.
Access Economics for ASCIA, 2007.Access Economics for ASCIA, 2007.
In 2007, the financial cost of allergies wasIn 2007, the financial cost of allergies was $7.8 billionCompare this to:Compare this to:
Schizophrenia $1.8 billionBipolar affective disorder $1 6 billionBipolar affective disorder $1.6 billion

The economic impact of allergic disease in Australia: not The economic impact of allergic disease in Australia: not to be sneezed at. to be sneezed at.
Access Economics for ASCIA, 2007.Access Economics for ASCIA, 2007.
Breakdown of $7.8 billion costBreakdown of $7.8 billion cost$5.6 billion (72%): loss of productivity
$4.2 billion = ‘Presenteeism’$1.1 billion = Lower employment rates$196 million = Absenteeism$84 million = Premature death
$1.2 billion (15%): direct health system expenditure$262 million (3%): indirect costs$783 million (10%): deadweight loss
Talk OverviewTalk Overview
1. Background1. Background2. Allergic rhinitis3 Asthma3. Asthma
Allergic rhinitisAllergic rhinitis
1. Causes of rhinitis1. Causes of rhinitis2. Pathophysiology3 Classification3. Classification4. Clinical assessment5. Investigations6. Managementa age e
Allergic rhinitisAllergic rhinitis
1. Causes of rhinitis1. Causes of rhinitis2. Pathophysiology3 Classification3. Classification4. Clinical assessment5. Investigations6. Managementa age e
Causes of RhinitisCauses of Rhinitis
Allergic rhinitis (50-70%)Symptomatic inflammatory disorder of the nose mediated by IgE antibody in the membrane lining the nose after allergen exposureReversible spontaneously or with treatment
All i & ll iAllergic & non-allergicOccupational
Chemicals/irritants e.g. manufacturing plants, hair & nail salonsAllergens e.g. lab animals (rats, mice, guinea pigs),
Non-allergic rhinitis1. Infectious – viral, bacterial, other1. Infectious viral, bacterial, other2. Drug-induced
Aspirin-exacerbated respiratory diseaseRhinitis medicamentosaRhinitis medicamentosa
1. Wallace et al. JACI 2008; 122: S1-84.2. Bousquet et al. ARIA 2008. Allergy 2008; 63 (Sup 86): 8-1603. Kemp et al. Australian Family Physician 2008; 37 (4): 214-220
Causes of RhinitisCauses of Rhinitis
Non-allergic rhinitis (cont)g ( )4. Idiopathic/vasomotor
● Triggered by tobacco smoke, strong odours, changes in temperature and humidity, exercise, undeterminedp y, ,
5. Non-allergic rhinitis with eosinophillia syndrome (NARES)?Subgroup of idiopathic rhinitisPerennial nasal symptoms particularly nasal congestionPerennial nasal symptoms, particularly nasal congestionNasal smears demonstrate > 20% eosinophils. Usually middle-aged adults (rare in childhood < 2%)
6 Other6. OtherHormonal, emotional, atrophic, food
1. Wallace et al. JACI 2008; 122: S1-84.2. Bousquet et al. ARIA 2008. Allergy 2008: 63 (Sup 86): 8-1603. Kemp et al. Australian Family Physician 2008; 37 (4): 214-220
Differential DiagnosisDifferential Diagnosis
1. Nasal polyps2. Structural/mechanical factors
1. Deviated septum/septal wall defects2. Adenoidal hypertrophyyp p y3. Trauma4. Foreign body5. Nasal tumors6. Choanal atresia7. Cleft palate8. Pharyngonasal reflux9 Acromegaly (excess growth hormone)9. Acromegaly (excess growth hormone)
3. Cerebospinal fluid rhinorrhoea4. Ciliary dyskinesia syndromey y y
Wallace et al. JACI 2008; 122: S1-84.
Allergic rhinitisAllergic rhinitis
1. Causes of rhinitis1. Causes of rhinitis2. Pathophysiology3 Classification3. Classification4. Clinical assessment5. Investigations6. Managementa age e

IgE Pathophysiology
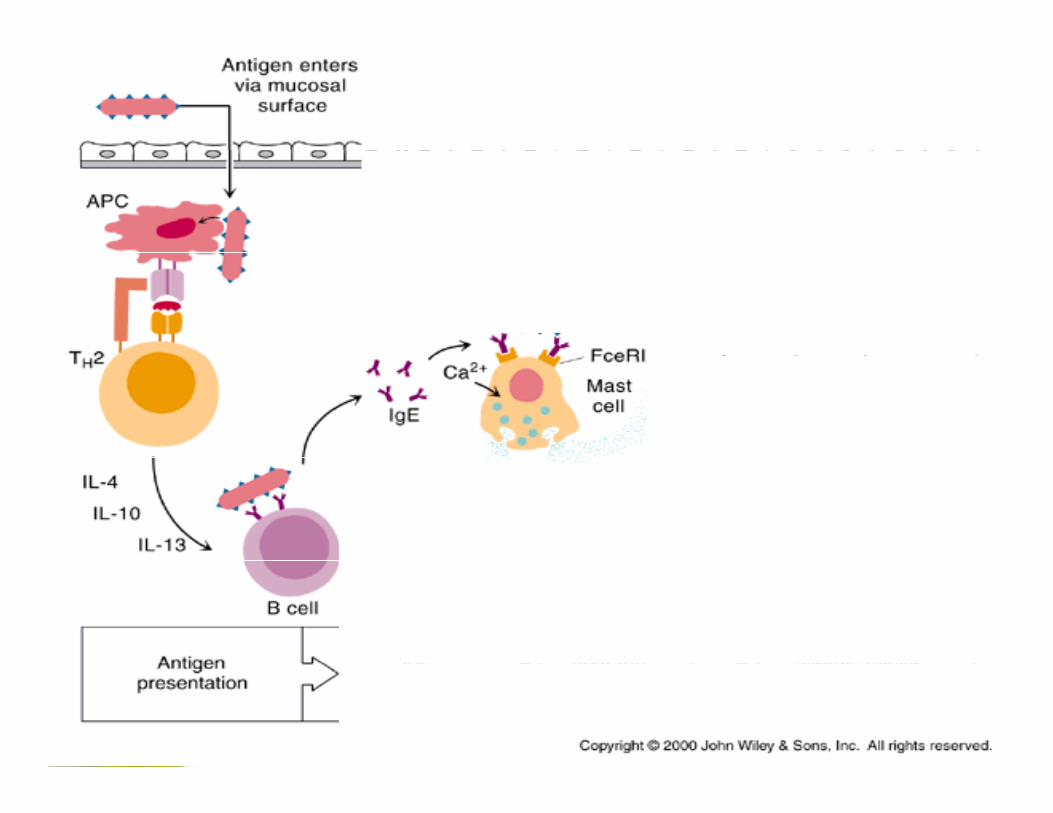
IgE Pathophysiology
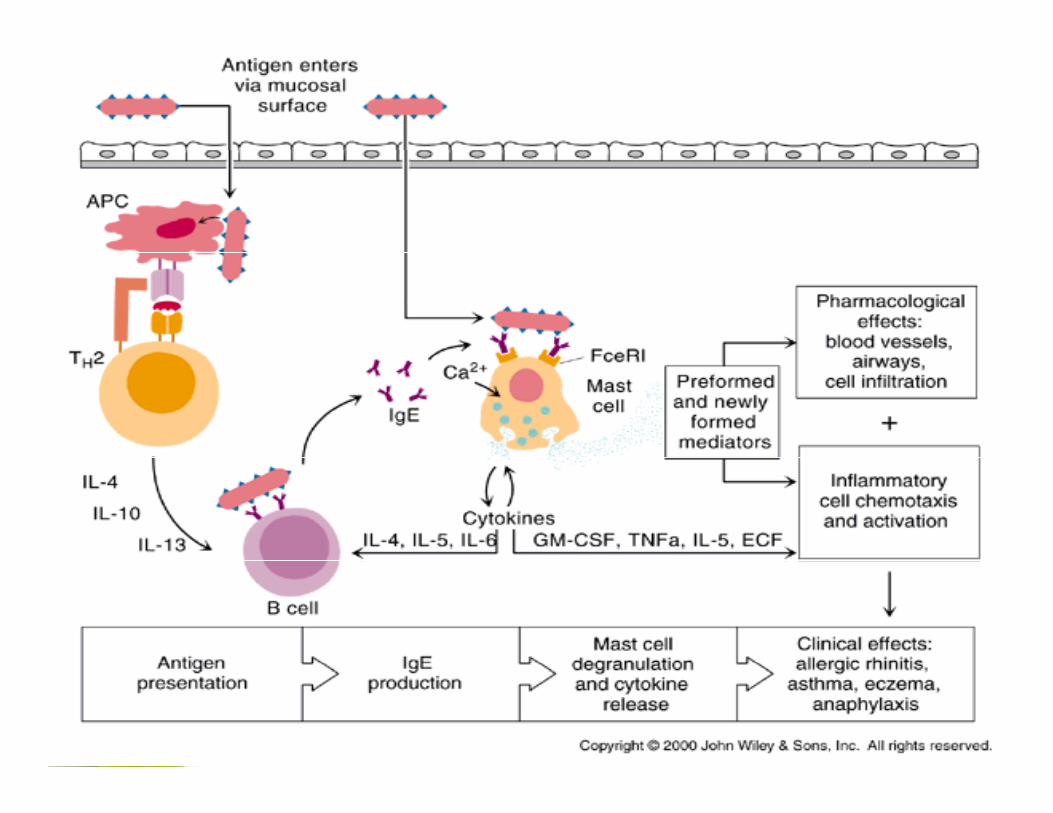
IgE Pathophysiology
PathophysiologyPathophysiology of ARof AR
Immediate response to allergenImmediate response to allergenDue to mediators of mast cell degranulationSymptoms – sneezing watery nose itchSymptoms sneezing, watery nose, itch
Delayed response to allergenDelayed response to allergenDue to invasion of inflammatory cells (eosinophils etc)(eosinophils etc)Symptoms – as above plus nasal congestion
Allergic rhinitisAllergic rhinitis
1. Causes of rhinitis1. Causes of rhinitis2. Pathophysiology3 Classification3. Classification4. Clinical assessment5. Investigations6. Managementa age e
Old classification system:Old classification system:Ti fTi fTime of exposureTime of exposure
1 Seasonal (outdoor allergens)1. Seasonal (outdoor allergens)Tree pollens: Late winter/early springGrass pollens:
N th t l J /F b/MNorthern coastal areas: Jan/Feb/MarSouthern coastal areas: Oct/Nov/Dec
Weed pollens: August to May
2. Perennial (indoor allergens) Dust mite, pet dander, moulds, cockroach
O ti l3. Occupational
1. Australasian Society of Clinical Immunology and Allergy (ASCIA). www.allergy.org.au2. Bousquet et al. ARIA 2008. Allergy 2008: 63 (Sup 86): 8-160
Old classification system:Old classification system:Time of exposureTime of exposureTime of exposureTime of exposure
Problem with this classification1. Pollen seasons
Vary year-to-year with climate change In some areas, pollens and moulds are perennial, p pSome patients with monosensitation to a single pollen species have perennial symptoms
2. HDM allergygySome patients with HDM allergy have only intermittent symptoms (esp Mediterranean area where HDM levels are low in summer)
M j i f i l i i d3. Majority of patients are polysensitizedThus they are exposed to different allergens throughout the yearN ifi i it t ( i ll ti ) tNon-specific irritants (e.g. air pollution) may aggravate symptoms
1. Bousquet et al. ARIA 2008. Allergy 2008: 63 (Sup 86): 8-160
New classification system:New classification system:Frequency of symptomsFrequency of symptomsFrequency of symptomsFrequency of symptoms
ARIA GUIDELINES
I t itt t Persistent
ARIA GUIDELINES
Intermittent<4 days a week
Persistent>4 days a weeky
OR <4 consecutive weeks a year
yAND
>4 consecutive weeks a year
1. Bousquet et al. ARIA 2008. Allergy 2008: 63 (Sup 86): 8-160
Classification of severityClassification of severity
ARIA GUIDELINES1. Sleep disturbance2 I i t f d il ti iti l i d/
ARIA GUIDELINES
2. Impairment of daily activities, leisure and/or sport
3. Impairment of school or work4. Troublesome symptoms
None of the aboveMild
One or more of the aboveModerate or severe
1. Bousquet et al. ARIA 2008. Allergy 2008: 63 (Sup 86): 8-160
Allergic rhinitisAllergic rhinitis
1. Causes of rhinitis1. Causes of rhinitis2. Pathophysiology3 Classification3. Classification4. Clinical assessment5. Investigations6. Managementa age e
AR AR –– HistoryHistory
SymptomsSymptomsNasal
Sneezing itchy nose & rhinorrhoeaSneezing, itchy nose & rhinorrhoeaNasal blockage (may be only symptom)
Mouth breathing and snoringMouth breathing and snoringSleep apnoea – daytime somnolence, headaches
Non-nasalItchy & watery eyes
Wallace et al. JACI 2008; 122: S1-84.
AR AR –– HistoryHistory
Oth t th t i ht t AROther symptoms that might suggest ARRecurrent URTIFrequent sore throatsFrequent sore throatsHoarse voiceHalitosisHalitosisCoughingRecurrent serous OMRecurrent serous OMLoss of smell
AR AR –– HistoryHistory
Other important aspectsOther important aspectsChronicityFrequency of symptomsFrequency of symptomsSeasonality: perennial versus seasonalTriggers e g petsTriggers e.g. pets
Functional impact on QOLFatigue sleep disturbance learning andFatigue, sleep disturbance, learning and attention problems, absenteeism, presenteeism
Wallace et al. JACI 2008; 122: S1-84.
AR AR -- ExaminationExamination
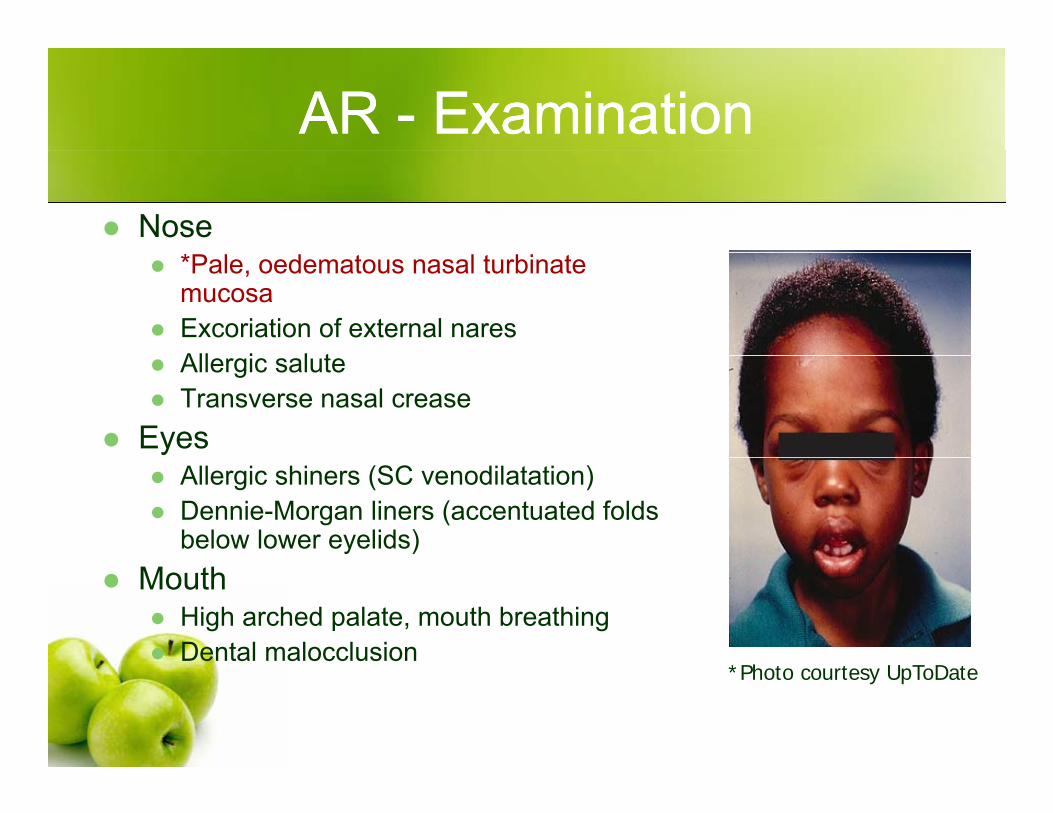
Nose*Pale, oedematous nasal turbinate mucosaExcoriation of external naresAll i l tAllergic salute Transverse nasal crease
EyesAllergic shiners (SC venodilatation)Dennie-Morgan liners (accentuated folds below lower eyelids)
MouthHigh arched palate, mouth breathingDental malocclusion
*Photo courtesy UpToDate
Allergic rhinitisAllergic rhinitis
1. Causes of rhinitis1. Causes of rhinitis2. Pathophysiology3 Classification3. Classification4. Clinical assessment5. Investigations6. Managementa age e
AR - Investigations
TestsSkin prick testsSerum allergen-specific IgE
Basic principlesAlways correlate with clinical symptomsPositive history + positive test = confirmatory evidence of specific allergyPositive test can occur in the absence of clinicalPositive test can occur in the absence of clinical disease not useful as a screening tool
1. Bousquet et al. ARIA 2008. Allergy 2008: 63 (Sup 86): 8-160
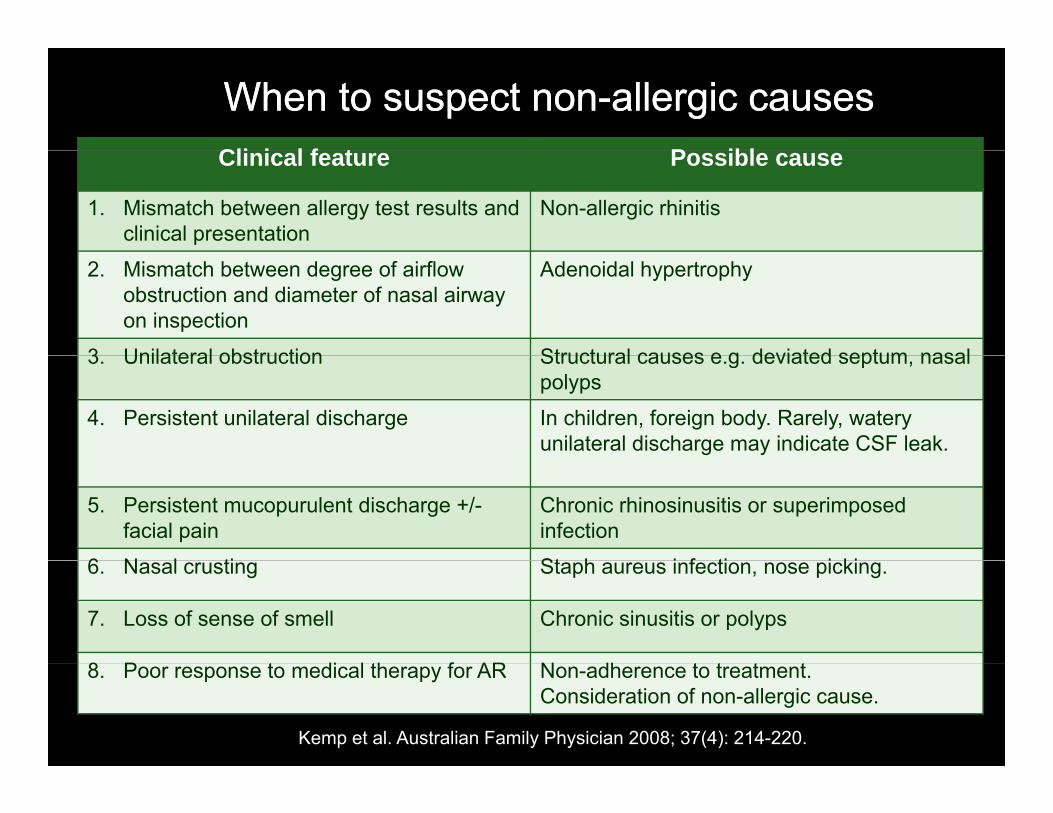
When to suspect nonWhen to suspect non--allergic causesallergic causesCli i l f t P iblClinical feature Possible cause
1. Mismatch between allergy test results and clinical presentation
Non-allergic rhinitis
2. Mismatch between degree of airflow obstruction and diameter of nasal airway on inspection
Adenoidal hypertrophy
3 Unilateral obstruction Structural causes e g deviated septum nasal3. Unilateral obstruction Structural causes e.g. deviated septum, nasal polyps
4. Persistent unilateral discharge In children, foreign body. Rarely, watery unilateral discharge may indicate CSF leak.
5. Persistent mucopurulent discharge +/-facial pain
Chronic rhinosinusitis or superimposed infection
6 N l ti St h i f ti i ki6. Nasal crusting Staph aureus infection, nose picking.
7. Loss of sense of smell Chronic sinusitis or polyps
8 P t di l th f AR N dh t t t t8. Poor response to medical therapy for AR Non-adherence to treatment.Consideration of non-allergic cause.
Kemp et al. Australian Family Physician 2008; 37(4): 214-220.
Allergic rhinitisAllergic rhinitis
1. Causes of rhinitis1. Causes of rhinitis2. Pathophysiology3 Classification3. Classification4. Clinical assessment5. Investigations6. Managementa age e
AR AR -- ManagementManagement
1. Allergen avoidance1. Allergen avoidance2. Pharmacotherapy
AntihistaminesAntihistaminesIntranasal corticosteroids (INCS)Other medicationsOther medications
3. Immunotherapy
AR AR -- ManagementManagement
1. Allergen avoidance1. Allergen avoidance2. Pharmacotherapy
AntihistaminesAntihistaminesIntranasal corticosteroids (INCS)Other medicationsOther medications
3. Immunotherapy
1. Allergen Avoidance1. Allergen Avoidance
A 1 House dust miteA. 1. House dust mite B. 2. PollensC. 3. Pet allergens
1. Allergen Avoidance1. Allergen Avoidance
A 1 House dust miteA. 1. House dust mite B. 2. PollensC. 3. Pet allergens
1A. House dust mite avoidance1A. House dust mite avoidance
HDM feed on skin flakes contained within dustAllergen is contained within faecal particles and body parts of HDMRelatively large allergen particle 10-30umRemain airborne for short period (20-30 min)Mites infest fabrics (bedding)G t t ll i lGreatest exposure usually in sleep
1A. House dust mite avoidance1A. House dust mite avoidance
Most important species arep pDermatophagoides pteronyssinus (Der p)Dermatophagoides farinae (Der f)p g ( )Euroglyphus maynei (Eur m)Lepidoglyphus destructor (Lep d)Blomia tropicalis (Blo t)
1. Bousquet et al. ARIA 2008. Allergy 2008: 63 (Sup 86): 8-160
1A. House dust mite avoidance1A. House dust mite avoidanceCurrent RCH adviceCurrent RCH advice
1. HDM encasements – pillow, mattress & doona
Current RCH adviceCurrent RCH advice
2. Remove sheepskin or woollen underlay3. Remove reservoirs (toys, clothing, furnishings)4. Remove drapes5. Every week
Wash all bed linen in hot water (>55oC kills HDM)Vacuum carpetDamp dustDamp dust
?Acaricide sprays*Ineffective: dehumidifiers & air-filter devicesIneffective: dehumidifiers & air filter devices
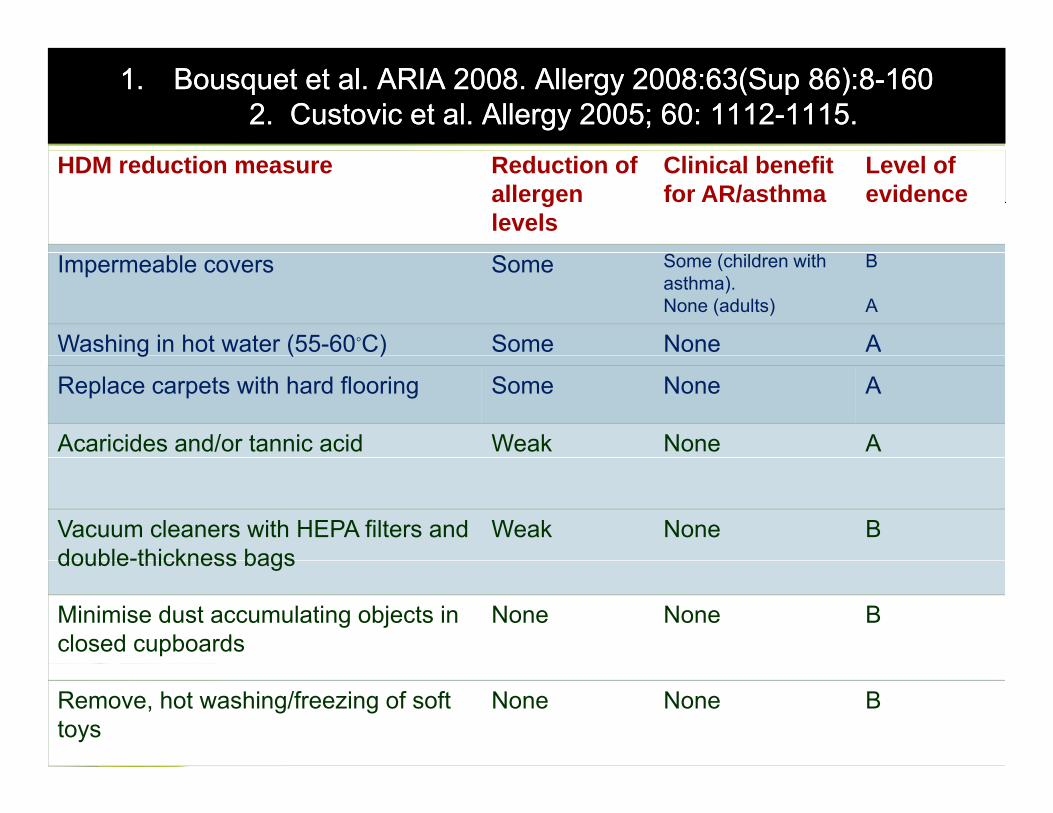
1.1. Bousquet et al. ARIA 2008. Allergy 2008:63(Sup 86):8Bousquet et al. ARIA 2008. Allergy 2008:63(Sup 86):8--1601602. Custovic et al. Allergy 2005; 60: 11122. Custovic et al. Allergy 2005; 60: 1112--1115.1115.
HDM reduction measure Reduction of allergen levels
Clinical benefitfor AR/asthma
Level of evidence
Impermeable covers Some Some (children with asthma).None (adults)
B
A
Washing in hot water (55-60◦C) Some None Ag ( )
Replace carpets with hard flooring Some None A
Acaricides and/or tannic acid Weak None A
Vacuum cleaners with HEPA filters and double-thickness bags
Weak None Bdouble-thickness bags
Minimise dust accumulating objects in closed cupboards
None None B
Remove, hot washing/freezing of soft toys
None None B
Sheikh A, Hurwitz B, Sheikh A, Hurwitz B, ShehataShehata Y. House dust mite avoidance Y. House dust mite avoidance measures for perennial allergic rhinitis. measures for perennial allergic rhinitis. Cochrane Database Cochrane Database
f S t ti R i 2007f S t ti R i 2007
Evaluated 7 randomised controlled trials
of Systematic Reviews 2007.of Systematic Reviews 2007.
Acaricide sprays – 2 trialsHigh-efficiency particulate air (HEPA) filters –g y ( )2 trialsHDM impermeable bedding – 3 trials
Reduction in HDM load6 of 7 trials showed intervention resulted in i ifi t d ti f HDM l d hsignificant reduction of HDM load when
compared to control
Sheikh A, Hurwitz B, Sheikh A, Hurwitz B, ShehataShehata Y. House dust mite avoidance Y. House dust mite avoidance measures for perennial allergic rhinitis. measures for perennial allergic rhinitis. Cochrane Database Cochrane Database
f S t ti R i 2007f S t ti R i 2007
Only 2 of 7 trials were of good quality (investigated
of Systematic Reviews 2007.of Systematic Reviews 2007.
mite impermeable bedding)Terreehorst 2003: No significant difference on visual analogue scales, nasal allergen-provocation testing or g g p gdaily symptom score in 279 patients.Ghazala 2004: Statistically significant decrease in subjective rhinitis and ocular symptom scores in all 26 j y ppatients receiving either placebo or active treatements.
ConclusionAcaricide sprays and extensive bedroom basedAcaricide sprays and extensive bedroom based environmental control programmes may be of some benefit in reducing rhinitis symptomsHDM impermeable bedding used in isolation is unlikely toHDM impermeable bedding used in isolation is unlikely to be beneficial
1. Terreehorst et al. NEJM 2003; 349(3):237-46.2. Ghazala et al. Allergologie 2004;27:26-34.

1. Allergen Avoidance1. Allergen Avoidance
A 1 House dust miteA. 1. House dust mite B. 2. PollensC. 3. Pet allergens

1B. Pollen avoidance1B. Pollen avoidance
Pollens• In Latin, means ‘fine flour’• Can be
• Anemophilous - carried by wind • Entomophilous - carried by insects
• Pollens nature and numbers vary by• Pollens nature and numbers vary by• Vegetation, geography, temperature, climate, region
• Size• Varies from 10 to 100 µm – explains deposition in nostrils and
eyes.• However pollens can be borne on submicronic particles and p p
induce ‘thunderstorm asthma’
Bousquet et al. ARIA 2008. Allergy 2008: 63 (Sup 86): 8-160
1B. Pollen avoidance1B. Pollen avoidance
• Grass pollens • Universally distributed• Bermuda (Cynodon dactylon) and Bahia (Paspalum notatum) do
not usually cross-react with other grasses• Usually pollinate end of spring and beginning of summer
• WeedsMugwort (Artemisia)• Mugwort (Artemisia)
• Ragweed (Ambrosia): end of summer & beginning of autumn• Parietaria: pollinates over long periods (Mar-Nov) and can result
i i l tin perennial symptoms• Trees
• Birch (Betula), Cypress (Cupressus).( ) y ( )• Pollinate end of winter and beginning of spring, but varies year-to-
year.Bousquet et al. ARIA 2008. Allergy 2008: 63 (Sup 86): 8-160
1B. Pollen avoidance1B. Pollen avoidance
1. Avoid going outdoors before midday (if possible). g g y ( )2. Avoid going out on windy days or after
thunderstorms.3. Wear sun glasses.4. Avoid activities with high exposure to pollens, such
i th l ( t i i id h it ias mowing the lawn (or staying inside when it is being mown). If mowing is unavoidable, wear a mask.
5 Keep windows closed both at home and in the car5. Keep windows closed both at home and in the car. Where possible, use recirculating air-conditioning in the car.
Australasian Society of Clinical Immunology and Allergy (ASCIA). www.allergy.org.au
1B. Pollen avoidance1B. Pollen avoidance
6. Avoid picnics in parks or in the country during the y gpollen season.
7. Try to plan holidays out of the pollen season or h lid t th idholiday at the seaside.
8. Remove weeds or trees outside the bedroom if particular sensitivities are knownparticular sensitivities are known.
9. Shower after arriving home and irrigate eyes with wet washer.washer.
Australasian Society of Clinical Immunology and Allergy (ASCIA). www.allergy.org.au
1. Allergen Avoidance1. Allergen Avoidance
A 1 House dust miteA. 1. House dust mite B. 2. PollensC. 3. Pet allergens
1C. Pet avoidance1C. Pet avoidance
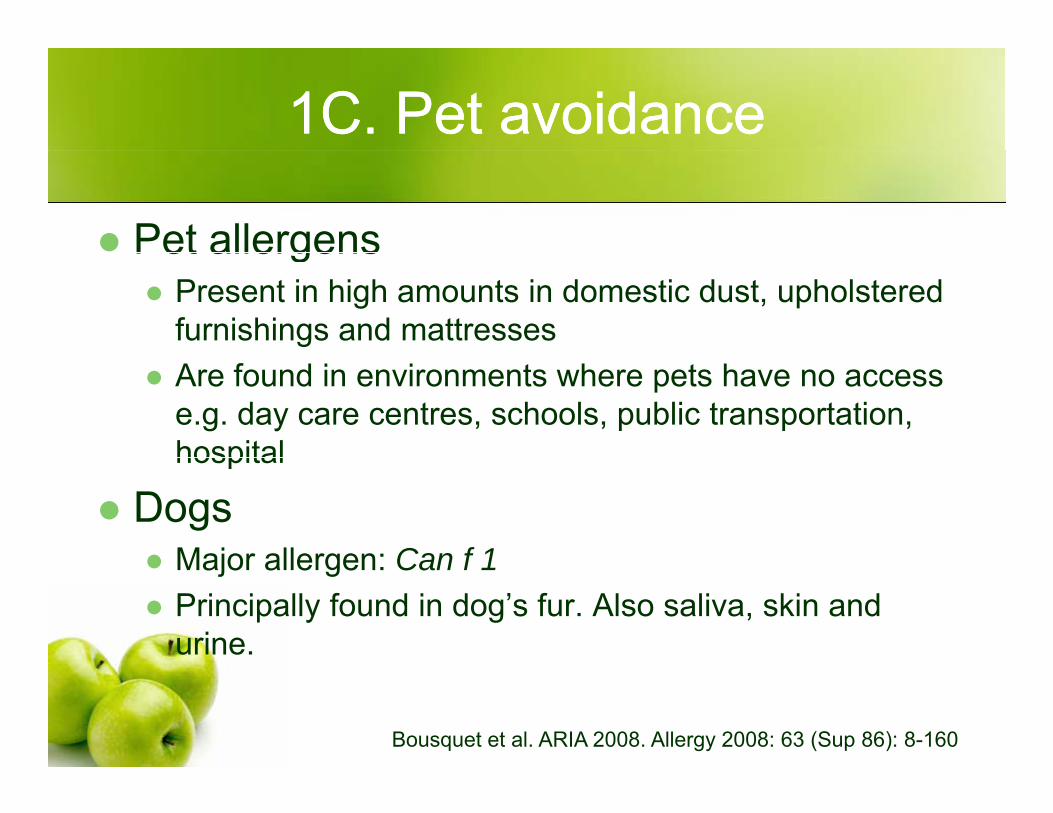
Pet allergensPet allergensPresent in high amounts in domestic dust, upholstered furnishings and mattresses Are found in environments where pets have no access e.g. day care centres, schools, public transportation, hospitalhospital
DogsMajor allergen: Can f 1Major allergen: Can f 1Principally found in dog’s fur. Also saliva, skin and urine.
Bousquet et al. ARIA 2008. Allergy 2008: 63 (Sup 86): 8-160
1C. Pet avoidance1C. Pet avoidance
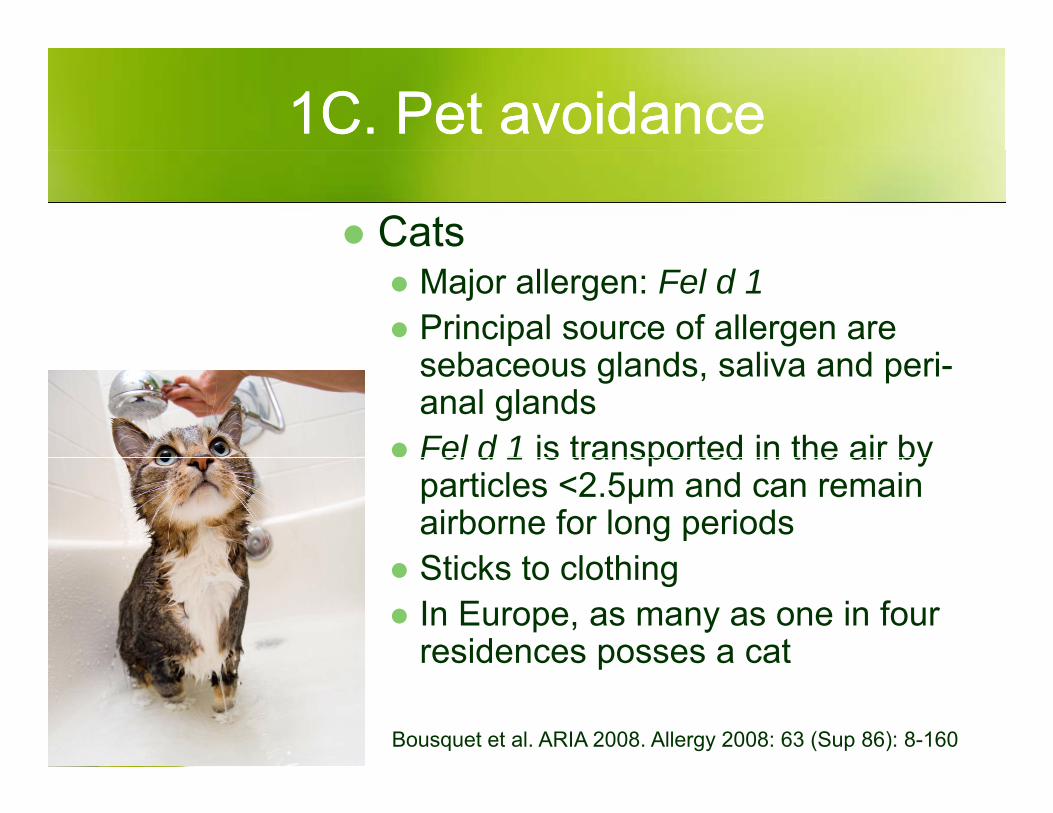
CatsMajor allergen: Fel d 1Principal source of allergen are
b l d li d isebaceous glands, saliva and peri-anal glandsFel d 1 is transported in the air byFel d 1 is transported in the air by particles <2.5μm and can remain airborne for long periodsSti k t l thiSticks to clothing In Europe, as many as one in four residences posses a cates de ces posses a ca
Bousquet et al. ARIA 2008. Allergy 2008: 63 (Sup 86): 8-160

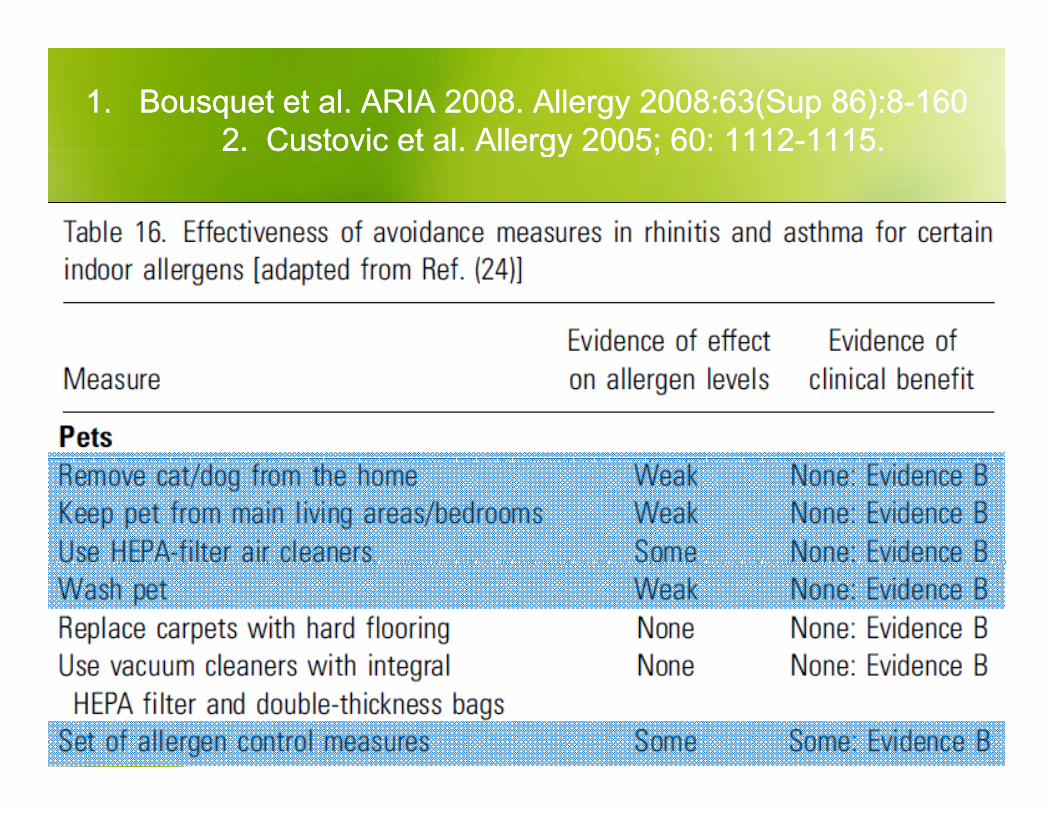
1.1. Bousquet et al. ARIA 2008. Allergy 2008:63(Sup 86):8Bousquet et al. ARIA 2008. Allergy 2008:63(Sup 86):8--1601602. Custovic et al. Allergy 2005; 60: 11122. Custovic et al. Allergy 2005; 60: 1112--1115.1115.2. Custovic et al. Allergy 2005; 60: 11122. Custovic et al. Allergy 2005; 60: 1112 1115.1115.




![3. Allergic Rhinitis.ppt [Read-Only] - ocw.usu.ac.idocw.usu.ac.id/.../mk_aia_slide_allergic_rhinitis.pdf · Allergic rhinitis is clinically defined as a symptomatic disorder of the](https://img.dokumen.tips/doc/110x75/5d5608b088c99353208bdbb7/3-allergic-read-only-ocwusuacidocwusuacidmkaiaslideallergicrhinitispdf.jpg)