Embed Size (px)
Citation preview

Medical and Pediatric Oncology 14:166-172 (1986)
Age at Diagnosis in Childhood Acute Lymphoblastic Leukemia Harland N. Sather, PhD
Age at initial diagnosis in ALL has been identified in numerous studies to be an im- portant prognostic factor. Data were exam- ined from a large series of patients entered on ALL clinical trials of the Childrens Cancer Study Group during the period 1972-1983. These data confirm the importance of age as a prognostic factor and show that even after adjustment for other factors by multivariate analysis, age remains a highly significant pre- dictor of outcome. The data suggest that there are three main age groups with different
prognoses: infants ( < I year at diagnosis), the 1-9 age group, and those 10 or greater. The best prognosis is found in the intermediate age range and the worst in the infant group. While age is presumably a surrogate factor reflecting the effect of factors with more di- rect and explainable relationships to the dis- ease process, analysis of data in this review and from other recent studies do not yet ad- equately explain the age effect in terms of other prognostic factors.
I Key words: age, leukemia, childhood, prognosis, ALL
INTRODUCTION
The age at diagnosis of a child with acute lymphoblas- tic leukemia (ALL) has long been recognized as having interesting relationships to the incidence of the disease and the eventual outcome [l-101. Data from the popula- tion-based registries that participate in the United States National Cancer Institute’s SEER program [Il l show that the yearly incidence rate is at a peak in the first 5 years of life with 4.4 cases/100,000 population/year. This rate gradually decreases over the next 15 years of the child- hood range, as shown in Table I.
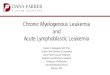
The following data come from a series of clinical trials of childhood ALL conducted by the Children’s Cancer Study Group (CCSG) of the United States. These studies enrolled over 5,000 patients during the period 1972 to 1983. Figure 1 shows a graph of the proportional inci- dence of the disease in the birth to 20 years of age range. One observes the usual peak incidence at about 3 years of age. Since many of the hospitals in this network are pediatric institutions and often have age limitations for admission, the category of patients 16 years of age and older is somewhat under-represented relative to the true incidence rate in that group. Table I1 shows that the with this exception, however, the CCSG incidence data are very similar to population-based figures. This is not sur- prising, since the hospitals in the network are widely distributed across the United States and currently treat a large proportion of all the newly diagnosed cases seen in the U . S . (about one-third) .
earlier eras, when therapy was relatively ineffective and almost all children with this malignancy died. For exam- ple, in 1971 Zippin reported a large series of over a thousand cases [l] that were originally diagnosed in the period 1955 to 1964 before central nervous system (CNS) prophylaxis was being routinely used and before systemic chemotherapy for the disease was very effective. This group of patients had a median survival of only 7% months with a 3-year survival of about 5%. Neverthe- less, there were strikmg differences among the age groups. The infants (less than 1 year of age at diagnosis) had a median survival of less than 2 months, while the children in the age range of 1 to 9 years had about a 10- month median, and those in the adolescent ages had a median of approximately 6 months.
Results have changed dramatically since that time and we now can expect to cure approximately 60% of chil- dren with ALL. Nevertheless, the relative effect of age has remained very similar in our more recent era. Figure 2 shows the estimated 5-year disease-free survival (DFS) rate according to age at diagnosis for all children who achieved a remission in the studies conducted by CCSG. Visually, we can see two possible breakpoints in the distribution. One is for the infant group as contrasted with those who are greater than 1 year of age. Here the difference in 5-year DFS rate is 40%. Another impres- sive change in outcome, but of a lesser magnitude, occurs at approximately 10 years. We see that for children 9
THE EFFECT OF AGE ON OUTCOME
Age at diagnosis has been well-established as a useful prognostic indicator of outcome for children with acute lymphoblastic leukemia. This was recognized even in
From the Children’s Cancer Study Group, University of Southern California, Pasadena.
Address reprint requests to Harland N. Sather, Children’s Cancer Study Group, University o f Southern California, 199 North Lake Avenue, 3rd Floor, Pasadena, CA 91101.
@ 1986 Alan R. Liss. Inc.

Age at Diagnosis in Childhood ALL 167
Program (1973-1977)
Age range (years) per 100,Wiyear 5
2.2 n
Incidence rate 80
W
W
rn LL
6 0 - 0-4 4.4 5-9
10-14 1.3 0 4 0 -
15-19 1 .O 0 W L
-
66
W 2ok TABLE 11. Prowrtional Incidence Rate of CCSG Studies AGE e l 1 2 3 Cornoared to 6.3 SEER Data
Proportional incidence for ages of less than 20 at diagnosis (%)
Age (years) CCSG SEER
0-4 52.5 49.4 5-9 27.3 24.7
10-14 15.4 14.6 15-19 4.7 11.2
5 16 c
<1 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16-3n
M 11 12 13 14 I 16+
n 112 3 7 8 7 3 0 7 5 2 6 1 5 4 2 6 338 2 3 1 1 8 9 168 1 7 6 1 4 0 1 4 4 1 4 2 130 110 117
Fig. 2. Life table estimates of disease-free survival (DFS) percentage at 5 years after successful remission induction by age at diagnosis. (CCSG studies: 1972-1983.)
~ 1.00 a I > U
0.75 w W
2 $! 0.50 a 5
fi 0.25
w
l- a 5 w o + 0)
.____, ...... I ......... ~
i ........................................
40 80 120 160 . - _ _
AGE AT DIAGNOSIS n 1 2 7 401 7 7 4 796 6 4 8 448 355 248 199 1 7 9 190 151 158 15s 147 121 127
Fig. 1. Proportional “incidence” of acute lvrnphoblastic leukemia by age in CCSG studies 1972-1983 (n = 5,228). at-diagnosis groups (CCSG studies: 1972-1983.)
TIME IN MONTHS AFTER REMISSION INDUCTION
Fig. 3. Disease-free survival following remission induction by age-
years of age the DFS rate is 60% while for those 10 years of age it is reduced to 45 % . There is a suggestion of a possible further valley in prognosis in the older age range occurring at 13 years (38%) and a slightly improved outcome in those 16 to 20 years of age (49%). These latter observations are very tenuous, however, and would need to be examined in other large ALL data sets to see if such possible relationships are also apparent. On the other hand, prognostic breakpoints at about 1 and at 10 years are very solid statistical results and have been observed by numerous researchers [1,4,6,7,9,10,12].
Figure 3 shows a life table curve of DFS for the three prognostic groups by age. The long-term DFS rates for
the infant, 1-9, and 10+ groups are 20, 61, and 41%, respectively. While it is interesting to note these prognos- tic differences, the natural question that arises is what types of other characteristics related to prognostic out- come and associated with age might be responsible for these differences. In particular, are there some character- tistics related to the basic biology of the disease that can account for these age differences?
In attempting to look at those issues, one notes that this pattern of outcome by age is indeed modified in various ways when we examine it closer. For example, if we examine the infant group closer, there is evidence of further heterogeneity of outcome. A recent study by

168 Sather
TABLE 111. 5-Year Disease-Free Survival Rate by Age at Diagnosis and Sex Group
Age at Dx Males Females (F-M)
< I 19.2 20.8 1.6 1 52.7 68.8 16.1 2 55.6 74.8 19.2 3 60.7 73.7 13.0 4 60.0 73.7 13.7 5 54.2 69.3 15.1 6 51.1 64.7 13.6 7 53.1 79.8 26.7 8 51.9 68.8 16.9 9 45.0 74. I 29.1
10 36.8 58.3 21.5 11 39.6 50.1 10.5 12 33.6 56.3 22.7 13 30.8 48.4 17.6 14 37.1 59.1 18.0 15 41.4 48.3 6.9 16+ 44.8 56.5 11.7
Difference
Reaman et a1 [lo] of the CCSG examined approximately the same group of infants shown in the previous age at diagnosis/outcome graph. Their analysis showed that the children less than 3 months of age have the worst prog- nosis, those 4 to 6 months a slightly better outcome, and those 6 to 11 months the best prognosis among the infant group.
If we look at the age effect within sex group, there are also some interesting patterns. Table I1 gives the 5-year DFS rates by sex group. One notes that in infants the results are nearly the same, but for all other ages there is a fairly marked benefit for females corresponding to the well-known prognostic advantage for females with ALL [8,13,14]. A slightly different pattern emerges for long- term survival, however. Table IV shows the life-table- estimated rates for survival at 7 years from diagnosis. Seven years was chosen for this table because that time point occurs at a time long after the cessation of therapy in almost all the patients in these data, most of whom were treated for 2 or 3 years. Moreover, there are suffi- cient patients with follow-up in excess of 7 years to make that estimate very reliable statistically and probably a good approximation of the true cure rates. In this table, we see that while the female prognostic advantage is readily apparent, it is of a much smaller magnitude in the peak incidence range of 1 to 6 years of age than might have been anticipated from the previous table of 5-year DFS data. In the older age ranges of childhood, there is generally a very large difference favoring females at each age value, which is consistent with the DFS data, how- ever. If one looks at these data further, it appears that the ability to retreat patients successfully who suffer an initial relapse varies both with the age of the patient and with the sex group.
TABLE IV. 7-Year Survival Rate By Age at Diagnosis and Sex Group
Difference Age at Dx Males Females (F -M)
<1 27.0 27.8 0.8 I 63.6 71.2 7.6 2 69.4 76.6 7.2 3 72.3 73.1 0.8 4 72.6 76.9 4.3
6 63.3 71.0 7.7
8 58.0 80.1 22.1
10 47.7 59.5 11.8
5 66.8 68.2 1.4
7 62.5 79.0 16.5
9 51.2 71.7 20.5
11 43.9 57.3 13.4 12 38.0 57.1 19.1 13 37.1 51.3 14.2 14 38.2 48.0 9.8 15 41.6 55.8 14.2 1 6 f 44.1 67.0 22.9
RELATIONSHIP TO OTHER FACTORS
In order to examine the age effect in a more systematic way, its association with many potentially important pa- tient characteristics at diagnosis was examined. Table V shows the interrelationships of age with a number of other front-end patient characteristics. White blood count (WBC) obviously has a very strong correlation with age. One notes that in the infant group 64% have initial WBC over 50,000 as compared to only 13% in the favorable 1-9 age range. There is also a significant excess of high WBC values in the 10+ age range compared to the 1-9 group, but to a lesser degree than the infant group. The sex ratio varies in an interesting manner, with roughly equal sex ratio in the infant group and progressively showing a higher male-to-female age ratio with increas- ing age. Presence of a mediastinal mass was also signifi- cantly different due to the higher incidence in children above 10 years of age.
No important age differences were observed for the proportion with marked adenopathy, but highly signifi- cant differences existed for both marked splenomegaly and hepatomegaly . The splenomegaly association is due totally to the very high incidence in infants. While the infant group is primarily responsible for the significant difference of hepatomegaly, the 1-9 group also had a statistically significant difference as compared with the 10+ group, which actually had a lower incidence of liver enlargement than the favorable age range.
CNS disease at diagnosis was distributed differently, but this was again due solely to the infant group, which had an exceedingly high incidence of this problem. Plate- let count distribution was also significant, with the big- gest difference related to the much lower levels in infants.

Age at Diagnosis in Childhood ALL 169
Hemoglobin levels were very different, but these data are not corrected for the gradual increase occurring in this age range. Nevertheless, it is unlikely that this would account totally for the magnitude of the difference among these groups. E-rosette results seem to show a clear correlation, indicating that the positivity rate increases with increasing age.
FAB morphology has a significantly different distri- bution largely due to the less favorable distribution of the 10+ group when contrasted with the 1-9 age range. There was no evidence of any significant difference in racial distribution among the age categories. Serum im- munoglobulins do seem to be distributed quite differ- ently. These data are corrected for the natural change in normal immunoglobulin levels over this range, and nevertheless fairly major differences exist. One observa- tion from these data is that the infant group generally presents with a higher proportion of depressed levels compared to the 1-9 age group. It also appears that the 10+ group has a much larger proportion of individuals with depressed levels of IgA and IgM when compared to the favorable age range.
The last entry in the table shows the final response to induction therapy according to age group. It is very clear that the infants have a relatively poor response to therapy, with a threefold higher rate of induction failure than the 1-9 group. The 10+ group also has induction response results that are not as good as the 1-9 group, showing approximately a twofold higher failure rate.
TABLE V. Relationship of Age at Diagnosis to Other Patient Characteristics
Age at diagnosis group (years) percentage of
< 1 1-9 10-15 16f P
WBC <10K 10-50 K 50-100 K >100K
Sex M F
Yes No
Yes No
Yes No
Yes No
Yes No
Platelets <SO K
> 150 K Hemoglobin
< 8 gm 8- 10 11+
E-Rosettes +
Mediastinal mass
Lymphadenopathy
Splenomegaly
Hepatomegal y
CNS @ Dx
50-150 K
Morphology L1 LUL2 L2
Race White Black Other
Depressed Non-depressed
Depressed Non-depressed
Depressed Non-depressed
Induction response MI or M2 M3
IgG
IgA
IgM
15 21 15 49
51 49
5 95
9 91
38 62
38 62
14 86
62 28 10
70 20 10
4 96
77 18 5
82 6
13
36 64
26 74
38 62
88 3
Death 9
54 33 6 7
54 46
5 95
7 93
15 85
16 84
2 98
49 32 19
61 29 10
7 93
83 14 3
84 6
10
19 81
11 89
19 81
96 1 3
49 27 9
14
58 42
11 89
7 93
16 84
13 87
4 96
39 37 24
40 39 22
12 88
72 22 6
84 6
10
22 78
24 76
25 75
93 3 4
49 28
8 14
69 31
6 94
7 93
9 91
3 97
2 98
46 31 23
42 37 21
15 85
79 16 5
77 9
14
21 79
24 76
33 67
92 4 4
< .001
.01
< .001
NS
< .001
< .001
< ,001
< .001
< .001
< ,001
< .001
NS
.004
< .001
< ,001
< ,001
MULTIVARIATE ANALYSIS OF AGE A N D OTHER FACTORS
The previous data make it clear that if we are properly to assess the prognostic effect of age and its interrelation- ship with other factors in ALL, then some type of multi- variate analysis will be needed since age is so tightly linked to numerous other characteristics. Consequently, the significance of age was assessed on the recent CCSG ALL series of patient entry during 1978 to 1983 using all the preceding factors plus a measure of rapidity of mar- row remission, the day-I4 bone marrow result. The anal- ysis used only those patients who had achieved an initial remission and examined DFS as the outcome index with the Cox regression model [ 151.
All of the factors mentioned previously except serum IgG and IgA showed significant univariate effect on prognosis in this large data set of approximately 1,500 patients with ALL. The ranking of age was relatively high on the scale of simple unadjusted univariate signifi- cance, ranking fifth after WBC, mediastinal mass, sex, and splenomegaly, respectively. The univariate analysis provided an estimate of the excess risk for each of the poor-risk age categories as contrasted with the favorable 1-9 range. Infants are estimated to have 4.08 times higher

170 Sather
TABLE Vl. Significant Prognostic Factors For CCSG ALL Studies 1978-1983
Final x2 Order of importance value p-value Relative risk
1. White blood count 39.3 <.OOO1 >20K:<20K = 1.70 2. Sex 37.4 <.OOO1 M:F = 1.78 3. Mediastinal mass 21.6 < .OOO1 Yes:No = 1.93 4. Rapidity of remission 36Sa <.OOO1 M3:Ml = 2.43
M2:Ml = 1.63
<1:1-9 = 1.52 5. Age 28.4a <.OO01 10+:1-9 = 1.66
6. Platelet count 13.1 .OOO3 < 5 0 K : > 5 0 K = 1.27 7. FAB morphology 15Sa .oO04 L2:Ll = 2.10
LI/L2:LI = 1.35 8. Hepatomegaly 11.7 .OOO6 Mark:Norm+Mod = 1.46
“Based on two degree of freedom x2; all other categories based on single degree of freedom x2.
risk of relapse or death interrupting the initial remission than the 1-9 group, while the rate is 1.95 times higher in the 10+ group as compared to the 1-9 range.
The multivariate regression analysis used a stepwise entry and deletion procedure that permitted the assess- ment of effects on the significance of all other factors as certain factors were selected as having prognostic impor- tance. The results of the analysis showed that only two factors had much importance in explaining the prognostic significance of age. First, the WBC does explain statisti- cally part of the reason for the significance of age as a prognostic factor. This is most prominent with respect to the infant group, which, as we noted earlier, generally does have very high WBC levels, although the entry of WBC into the regression equation also reduces the signif- icance of the prognostic effect in the older age group. Nevertheless, substantial prognostic effect remains after accounting for the interrelationship of age and WBC. The other factor that had an attenuating influence on the prognostic significance of age on DFS was the rapidity of initial remission, the day 14-marrow result. This has an explanatory effect principally for the infant group, many of whom achieve their remission at a very slow rate, and consequently there is a large proportion with substantial blast percentages after 2 weeks of treatment.
Table VI shows the final set of significant prognostic factors after accounting for the interrelationships among the factors. One sees that even after adjustment for its relationship with other factors, age at diagnosis still had a major prognostic influence in this large data set. The estimate of the relative risk of failure to maintain a remission is 1.66 times greater in the older age range when compared with the favorable age range. The risk for the infant group is 1.52 times greater than that of the favorable age group, which is a fairly impressive reduc- tion from the original unadjusted risk ratio of 4.08. How- ever, it should be pointed out that much of this reduction is due to the explanatory influence of rapidity of marrow remission, which is not a true front-end patient character-
istic, but one that is determined during the process of initial induction treatment. Had the remission rapidity factor not been included in this analysis of DFS, then the risk ratio for the infant group as compared to the favor- able age group would be much larger. Since in the group of patients who achieve a remission the rapidity of remis- sion plays such an important prognostic role in predicting the DFS duration, it was considered appropriate to in- clude that variable with the other true front-end charac- teristics in these analyses.
What about children in a very poor risk category? How important is age as a prognostic factor in such a group? This was looked at by considering just the subset of patients with initial WBC above 50,000/mrn3. A mul- tivariate analysis on this subset was again done with the Cox regression procedure. Interestingly, age now ranked second on the scale of prognostic importance with ad-just- ment for the other variables (Table VII). This prognostic significance was due almost exclusively to the poorer outcome in the older age range, which could not be explained by that group’s associations with other factors. The results indicated that the adjusted relative risk of the infant group was similar to the good age range and, hence, the infants’ poor prognosis explained statistically by the higher frequency of other bad risk factors in that group. Nevertheless, the major reason for the reduced significance of the infant group was again its association with the day-14 marrow result, which was the single most significant predictor of DFS in this poor prognosis subset.
THE ROLE OF IMMUNOPHENOTYPE
The question to be asked at this stage is whether, in lieu of any totally satisfactory explanation for the prog- nostic effect of age among the factors thus far described, other factors not studied in these analyses could be re- sponsible for the effect. One important candidate might be ALL immunophenotypes. The studies just described

Age at Diagnosis in Childhood ALL 171
100
80
v)
W
I= 50 a
TABLE VII. Significant Prognostic Factors for High WBC Patients (> 50,W/mm3)
Order of importance value p-value Relative risk
1. Rapidity of remission 9.4F .009 M3:Ml = 1.96 M2:Ml = 1.62
Final x2
2. Age 7.70a .02 10+:1-9 = 1.61 <1:1-9 = 1.02
3. Hepatomegaly 4.32 .04 Mark:Norm+Mod = 1 . 4 4 4. Mediastinal mass 3.94 .05 Yes:No = 1.47 5. Sex 3.15 .08 M:F = 1.36 6. log WBC 2.88 .09 > 100 K:50-1OO K = 1.29
aBased on two degree of freedom x2; all other categories based on single degree of freedom x 2 .
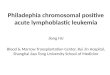
0 CALL A N-ALL 0 1 - A L L
Fig. 4. Relative proportions of ALL subtypes as a function of age. From ref. 16.
only had assessment by E-rosetting and did not use the more modern technology currently available to identify such subtypes.
Figure 4 shows data from a large series of ALL cases in England that were studied by Greaves [ 161. This figure shows the relative proportions of common ALL, null ALL, and T-ALL from his series. Obviously a very different pattern of relative frequencies for these subtypes occurs in the pediatric age range. Greaves found a large proportion of infants with null ALL, but this subtype was rare among children in the favorable age range, although there was a suggestion of an increased proportion again in the 10+ age group. Correspondingly, the favorable age range was largely composed of the common ALL
TABLE VIII. ALL Subtype Distribution for Recent CCSG Studies by Age at Diagnosis Group
Age group (percentage) < I 1 4 5-9 10-15 16-20
Common ALL 25.0 76.1 73.9 60.4 53.0 T cell ALL 12.5 14.1 17.1 23.1 23.5 Null cell ALL 62.5 9.8 9.0 16.5 23.5 No. of patients 8 142 134 91 17
subtype, while T-ALL is rare at young ages but seemed to have a gradually greater representation with increasing age until young adulthood when it began to decrease again. Also, Greaves and others have shown that the prognostic ordering of these subtypes is such that com- mon ALL has a better outcome than null ALL, which may in turn be somewhat better than T-ALL.
Data from the current generation of CCSG ALL stud- ies were examined to see if a similar pattern with age existed for the phenotypes described by Greaves. This group of CCSG studies was started in 1983 and at present they have rather short follow-up. Although the phenotyp- ing data are quite extensive on these studies, what has been examined at this stage is still very preliminary. Table VIII shows the percentages by age group with common, null, and T-ALL among a group of 392 pa- tients with complete phenotyping data. These data show a pattern very similar to that described by Greaves. Since the follow-up is relatively short in this group, it was not yet feasible statistically to assess the effect of age after adjustment for phenotype. That type of analysis would be a useful strategy to see if the predictive information from age is related to a more biologically based factor.
However, there is some evidence from other research- ers that such an analysis still may fail to account ade- quately for the effects of age. Kalwinsky et al of St. Jude’s reported a multivariate analysis of their data that showed that WBC, age, and race were still important prognostic variables even after accounting for many other

172 Sather variables including immunophenotype and cytogenetics [17]. An analysis by Crist of data from the Pediatric Oncology Group [ 121 demonstrated an important prog- nostic effect for immunophenotype in a multivariate anal- ysis of 272 children with non-T, non-B ALL. Nevertheless, they found that age was still a highly im- portant prognostic variable, second only to the white blood count in order of significance.
DISC U SSlO N
It appears that the important prognostic effects of age possibly cannot be explained in any totally satisfactory manner by the menu of clinical and biologic characteris- tics that have been well-studied at present in ALL. None- theless, many interesting correlations of age with these factors have been noted and presumably our understand- ing of age and other prognostic factors in ALL will improve, especially with the more refined ways in which we can categorize the disease by such procedures as cytogenetics, the use of monoclonal antibodies , and dif- ferences in drug metabolism.
In conclusion, while we continue to pursue some of these new avenues to ascertain basic biologic information about their effect on prognosis and any relationship to age that they might have, we may also wish to explore some other types of rudimentary factors that could play a role in the unexplained phenomena we currentIy ob- serve. I would like to suggest just one such factor. An interesting issue, but one that is admittedly difficult to study easily, is the patient’s compliance with therapy. In ALL therapy for a number of years, oral methotrexate and 6-mercaptopurine have been the backbone for most of the maintenance therapy regimens we give. Doctors often report patients whom they suspect or eventually find out do not adhere rigorously to the protocol’s speci- fied dosage and schedule for the oral medications to be taken at home. The magnitude of this noncompliance with oral medications is really not accurately known, although a few people have studied it with some success [18,19]. An observation that at present does not have established scientific validity, but is nevertheless interest- ing, is the following. The problem of noncompliance with therapy for pediatric and adolescent patients is gen- erally believed to be most prevalent in the 10 to 16 age range. For age at diagnosis, that is a range that has a very strong prognostic effect that is not satisfactorily explained by the correlation with other known prognostic factors. Thus, while we investigate more basic biologic factors that we hope will better explain our current ques- tions about ALL, we may also find that some simple yet presently unrecognized phenomena play a role in the prognosis of the disease.
REFERENCES
1.
2.
3.
4.
5
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
Zippin C, Cutler S, Reeves W, Lum D: Variation in survival among patients with acute lymphocytic leukemia. Blood 37:59- 72, 1971. Pierce M, Borges W, Heyn R, Wolff J, Gilbert E: Epidemiolog- ical factors and survival experience in 1770 children with acute leukemia. Cancer 23: 1296-1304, 1969. Hardisty R, Till M: Acute leukaemia 1959-64: Factors affecting prognosis. Arch Dis Child 43:107-115, 1968. George S, Fernbach D, Vietti T, Sullivan M, Lane D, Haggard M, Berry D, Lonsdale D, Komp D: Factors influencing survival in pediatric acute leukemia. Cancer 32: 1542-1553, 1973. Robison L, Sather H, Coccia P, Nesbit M, Hammond D: Assess- ment of the interrelationship of prognostic factors in childhood acute lymphoblastic leukemia. Am J Pediatr Hematol Oncol2:5- 13, 1980. Miller D, Leikin S, Albo V, Sather H, Karon M, Hammond D: Prognostic factors and therapy in acute lymphoblastic leukemia of childhood. Cancer 51: 104-1049, 1983. Simone J, Versoza M, Rudy J: Initial features and prognosis in 363 children with acute lymphoblastic leukemia. Cancer 36:2099- 2108, 1975. Gustafsson G, Kreuger A: Sex and other prognostic factors in acute lymphoblastic leukemia in childhood. Am J Pediatr Hema- to1 Oncol5:243-250, 1983. Kardos G, Revesz T, Koos R, Petroczky A, Schuler D: Infant leukemia in Hungary. Med Pediatr Onocol 10:201-207, 1982. Reaman G, Zelter P, Bleyer A, Amendola B, Level C, Sather H, Hammond D: Acute lymphoblastic leukemia in infants less than one year of age. J Clin Onocol 3:1513-1521, 1985. National Cancer Institute: “Surveillance, Epidemiology and End Results: Incidence and Mortality Data, 1973-77. ” NCI Mono- graph 57, Washington, DC: U.S. Government Printing Office, 1981. Crist W, Boyett J, Roper M, Pullen J, Metzgar R, Van Eys J, Ragab A, Starling K, Vietti T, Cooper M: Pre-B cell leukemia responds poorly to treatment. Blood 63:407-414, 1984. Sather H, Miller D, Nesbit M, Heyn R, Hammond D: Differ- ences in prognosis for boys and girls with acute lymphoblastic leukaemia. Lancet 1:739-743, 1981. Baumer J, Mott M: Sex and prognosis in childhood acute lym- phoblastic leukemia. Lancet 2: 128-129, 1978. Cox D: Regression models and life tables J R Stat Soc (B)
Greaves M: Subtypes of acute lymphoblastic leukemia: Implica- tion for the pathogenesis and epidemiology of leukemia. In Ma- grath I, O’Conor G , Ramot B (eds): “Pathogenesis of Leukemias and Lymphomas: Environmental Influences.” Vol27 of Progress in Cancer Research and Therapy. New York: Raven Press, pp
Kalwinsky D, Roberson P, Dahl G, Harber J, Rivera G, Bowman P, Pui C, Ochs J, Abromowitch M, Costlow M, Melvin S, Stass S, Williams D, Murphy S: Clinical relevance of lymphoblast biologic features in children with acute Iymphoblastic leukemia. J Clin Oncol 3:477-484, 1985. Smith S, Rosen D, Trueworthy R, Lowman J: A reliable method for evaluating drug compliance in children with cancer. Cancer
Smith S, Trueworthy R, Vats T, Klopvich P, Kisker S: Pediatric clinical pharmacology of 6-mercaptopurine: Lack of compliance as a factor in leukemia relapse. Proc Am SOC Clin Oncol 3:204, 1984.
341187-220, 1972.
129-139, 1984.
43:169-173, 1979.