Embed Size (px)
Citation preview
RAYMOND WONG, MDHong Kong
• Consultant of the Department of Medicine & Therapeutics, Prince of Wales Hospital
• Dr. Wong received his medical degree from the Chinese University of Hong Kong and received his training in Haematology, Internal Medicine as well as Clinical Pharmacology and Therapeutics at the Prince of Wales Hospital, Hong Kong. He also obtained his Doctor of Medicine from the Chinese University of Hong Kong. He joined the Prince of Wales Hospital Poison Treatment Centre since its establishment in 2005 which is a tertiary referral centre for the management of patients with poisoning. Dr. Wong has published over 70 articles in peer-reviewed journals including Blood, Circulation, JAMA and the New England Journal of Medicine in various areas of haematology and therapeutics.

Acute Lymphocytic Leukemia: Best of 2014
Advances in Induction in ALL
Dr. Raymond Wong
Department of Medicine & Therapeutics
The Chinese University of Hong Kong
BTG 2015
Induction for ALL
• Cytotoxic chemotherapy regimens are currently the standard of care in the induction phase of treatment for adult ALL
• Several regimens are in use but none has been proven more efficacious than the others in clinical trials
• Regardless of the induction regimen employed, achieving CR prior to post-remission maintenance therapy is highly predictive of OS

Induction for ALL
• During the past 20 years, development of risk-stratified, multi-agent, multi-phase treatment regimens for pediatric ALL patients has resulted in >95% patients achieving CR, and 5-year EFS >80%
• Therapeutic regimens for adults with ALL has been less effective, achieving OS of < 50%
• In the past decade, studies have shown that older adolescents and young adults (aged 16-21 years) treated with pediatric ALL regimens achieved improved outcomes
• A multicenter, phase 2 trial to assess the feasibility of treating newly diagnosed ALL with the Dana-Farber Cancer Institute (DFCI) Pediatric ALL Consortium regimen
• Between 2002 and 2008, 92 eligible patients aged 18–50 years were enrolled at 13 participating centers
DeAngelo DJ, et al. Leukemia 2014
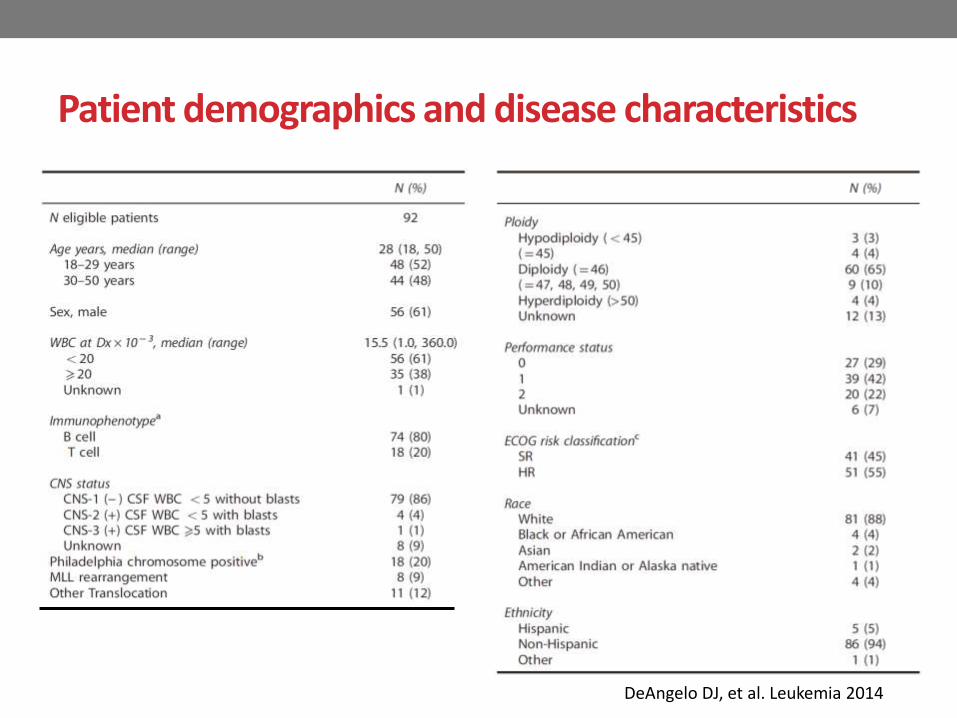
Patient demographics and disease characteristics
DeAngelo DJ, et al. Leukemia 2014
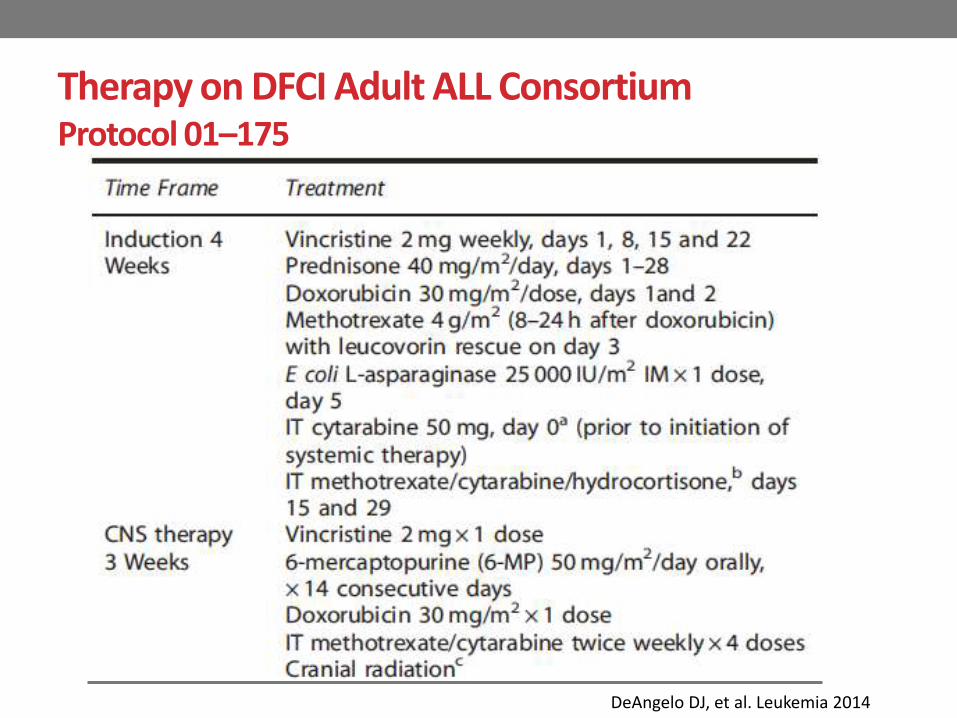
Therapy on DFCI Adult ALL Consortium Protocol 01–175
DeAngelo DJ, et al. Leukemia 2014
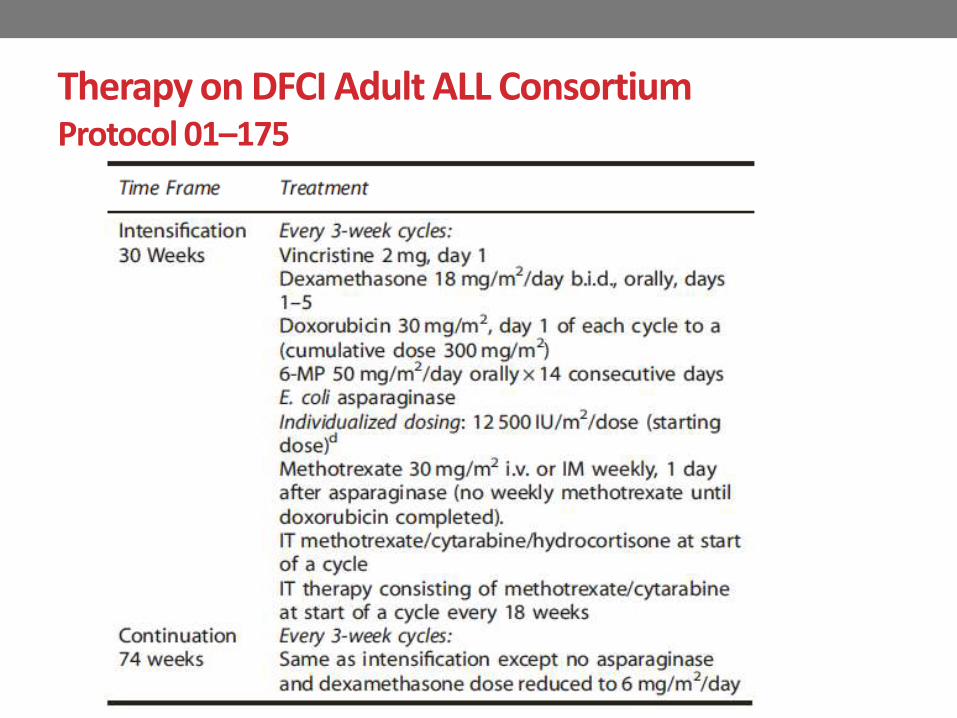
Therapy on DFCI Adult ALL Consortium Protocol 01–175

Results
• 78 patients (85%) achieved a CR after 1 month of intensive induction therapy
DeAngelo DJ, et al. Leukemia 2014
Results
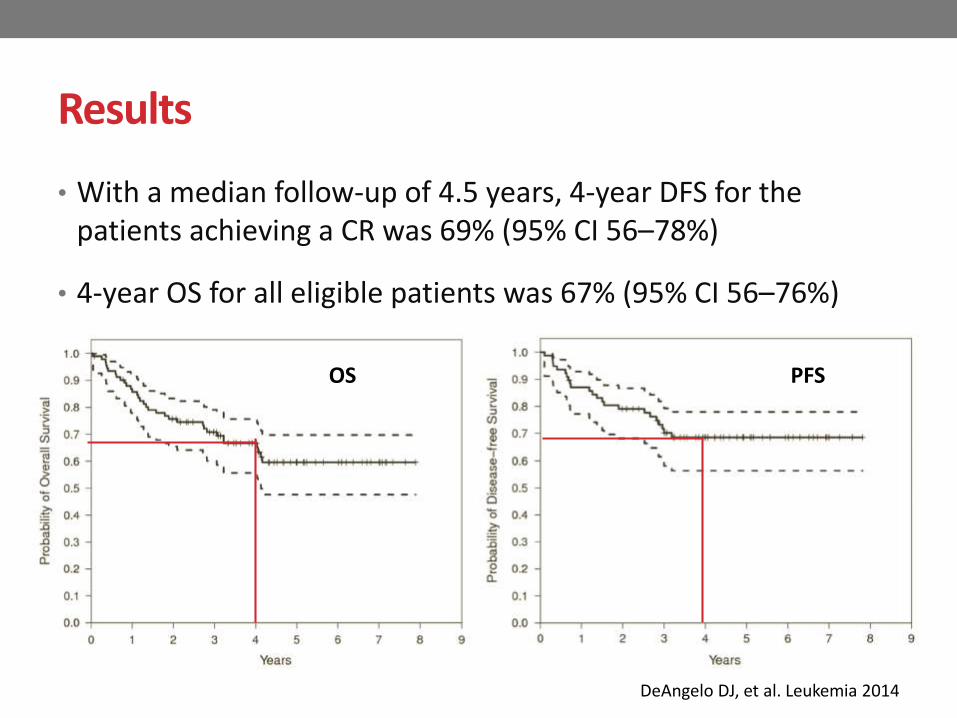
• With a median follow-up of 4.5 years, 4-year DFS for the patients achieving a CR was 69% (95% CI 56–78%)
• 4-year OS for all eligible patients was 67% (95% CI 56–76%)
DeAngelo DJ, et al. Leukemia 2014
OS PFS

Results
• The 4-year DFS for the 64 patients who achieved a CR and were Ph−ve was 71% (95% CI, 58–81%)
• For all 74 Ph−ve patients the 4-year OS was 70% (95% CI 58–79%)
DeAngelo DJ, et al. Leukemia 2014
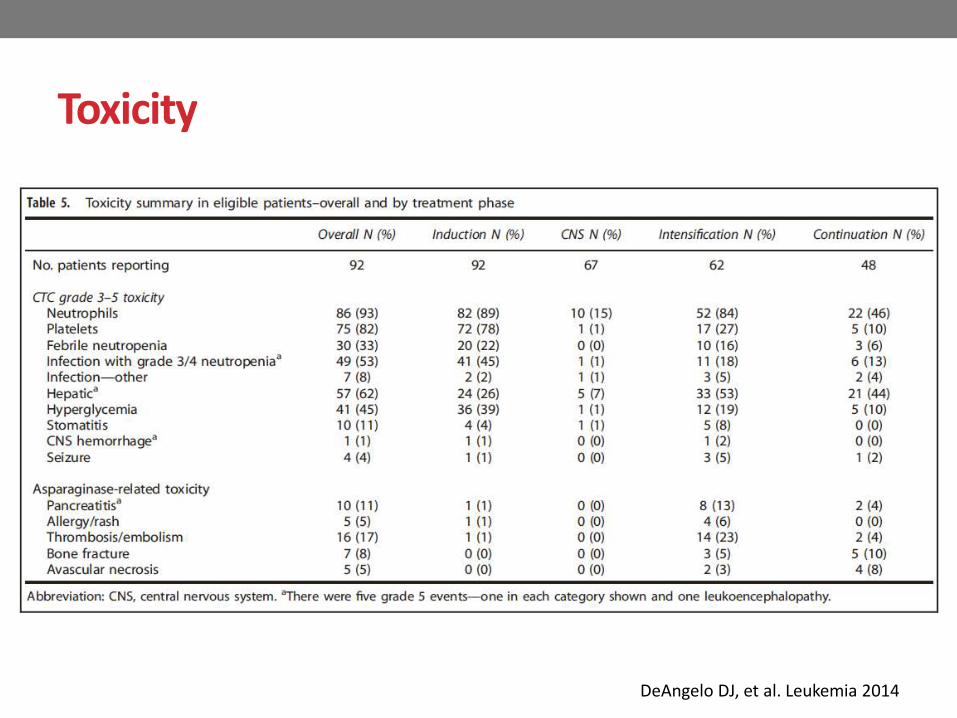
Toxicity
DeAngelo DJ, et al. Leukemia 2014

Asparaginase Dosing Regimen

Toxicity
DeAngelo DJ, et al. Leukemia 2014
• 72% of the patients who initiated the 30-week asparaginasecourse were able to receive ≥ 26 doses (87% of targeted therapy), similar to, although slightly lower than the proportion of pediatric patients.
• The incidence of major asparaginase-related toxicities, such as pancreatitis, and thrombosis was also similar to that reported in older children

A pediatric-like treatment strategy for young adults with de novo ALL is feasible, associated with tolerable toxicity, and results in improved outcomes compared with historical regimens in young adult patients with ALL
DeAngelo DJ, et al. Leukemia 2014
Intensified Chemotherapy for Older Patients with ALLA phase II study from the DFCI ALL Consortium
• To determine the efficacy in patients 51-75 years old with newly diagnosed ALL or lymphoblastic lymphoma
• Based on the DFCI ALL Consortium pediatric regimen:
• incorporation of clofarabine in consolidation
• adjustment to dose and scheduling of PEG asparaginase and steroids • prednisolone x 21 days for patients < 60 years old
• prednisolone x 7 days for patients ≥ 60 years old
• inclusion of stem cell transplant (SCT) for eligible patients after induction and 1st consolidation
Fathi A T et al. Blood 2014;124:3714
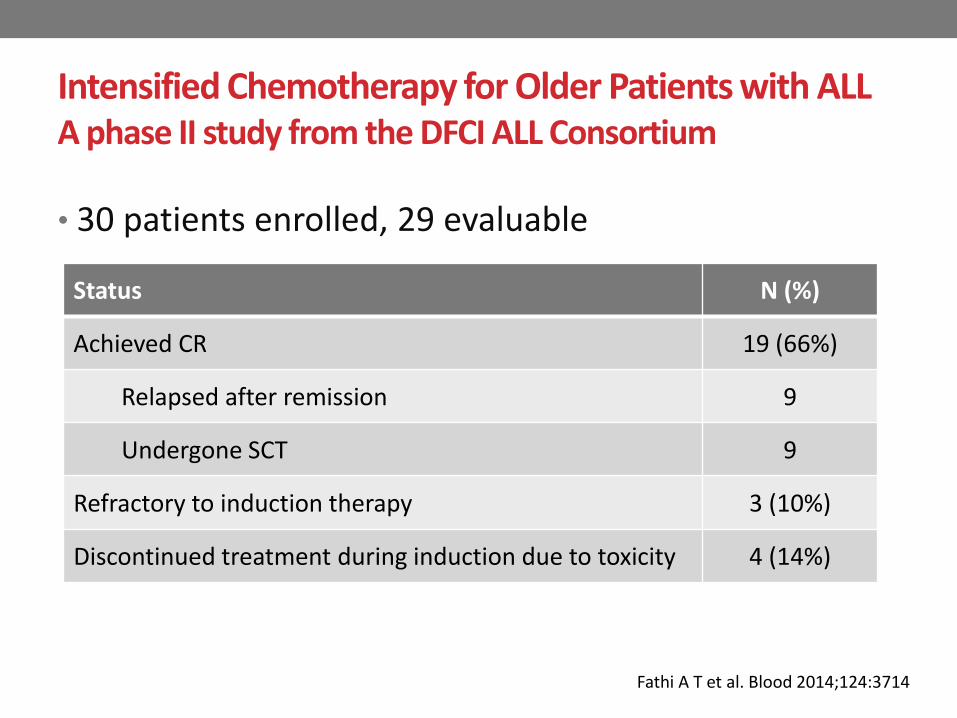
Intensified Chemotherapy for Older Patients with ALLA phase II study from the DFCI ALL Consortium
• 30 patients enrolled, 29 evaluable
Status N (%)
Achieved CR 19 (66%)
Relapsed after remission 9
Undergone SCT 9
Refractory to induction therapy 3 (10%)
Discontinued treatment during induction due to toxicity 4 (14%)
Fathi A T et al. Blood 2014;124:3714

Fathi A T et al. Blood 2014;124:3714
Intensified Chemotherapy for Older Patients with ALLA phase II study from the DFCI ALL Consortium
• OS (by Kaplan-Meier) at 1 year = 62% (95% CI, 41-77%)
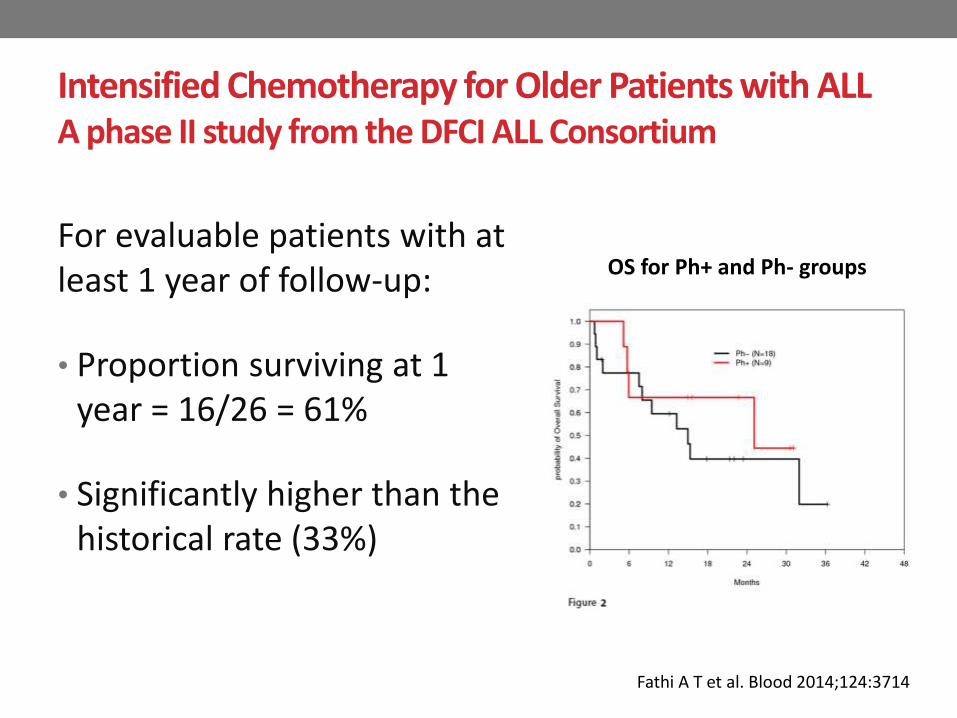
For evaluable patients with at least 1 year of follow-up:
• Proportion surviving at 1 year = 16/26 = 61%
• Significantly higher than the historical rate (33%)
Intensified Chemotherapy for Older Patients with ALLA phase II study from the DFCI ALL Consortium
OS for Ph+ and Ph- groups
Fathi A T et al. Blood 2014;124:3714

• Most common grade 3/4 toxicities:• transaminitis
• hyperbilirubinemia
• cytopenias
• hypophosphatemia
• hyperglycemia
• neutropenic fever
• liver injury reduction of PEG-asparaginase dosage
• The data suggest that intensive multi-agent chemotherapy is tolerable in older patients with ALL and can result in improved outcomes when compared to historical data
Intensified Chemotherapy for Older Patients with ALLA phase II study from the DFCI ALL Consortium
Fathi A T et al. Blood 2014;124:3714

Asparaginase in ALL
• An enzyme that deamidases serum asparagine, depleting it from ALL lymphoblasts
• Several large randomized pediatric ALL trials reported that higher cumulative doses of asparaginase result in significantly improved outcomes
• In contrast, large adult ALL clinical trials generally involve no asparaginase or use it in only one to two post-remission cycles, considering its potential higher toxicity

• To study a pegaspargase dosing strategy based on its pharmacokinetic characteristics in adults aged 18 to 57 years with newly diagnosed ALL treated with the adult ALL BFM protocol and included 6 doses of IV pegaspargase at 2,000 IU/m2 per dose
• Intervals between doses were longer than 4 weeks and rationally synchronized with other chemotherapy drugs to prevent overlapping toxicities
Douver D, et al. JCO 2014

Patient Demographic and Clinical Characteristics
Douver D, et al. JCO 2014


Results
Minimal enzymatic activity of 0.2 IU/mL for complete asparagine deamidation
Douver D, et al. JCO 2014

Results
• 49/51 patients (96%) achieved CR, 2 had resistant disease
• CR was achieved in 48 patients (98%) after induction phase 1 (at 4 weeks)
• Among the 40 Ph-negative patients, 39 (98%) achieved CR, all by 4 weeks
All patients (N=51) Ph-ve ALL (N = 40)
7-year OS 51% 58%
7-year DFS 58% 58%
Douver D, et al. JCO 2014

Asparaginase-Related Toxicity
• 23 patients (45%) received all 6 pegaspargase doses
• 31 patients (61%) received ≥3 doses
• 10 patients (20%) discontinued pegaspargase after prohibitive toxicity • pancreatitis
• severe allergy
Douver D, et al. JCO 2014

Ph+ ALL
• Until recently, Ph+ ALL was associated with a poor prognosis (5-year OS, 10%–20%), with the greatest hope for success via allogeneic HSCT
• Combination of cytotoxic chemotherapy with TKIs is effective in the treatment of Ph+ ALL
• Imatinib and dasatinib have been approved for use in Ph+ ALL

Phase II Study of Combination of Hyper-CVAD + Ponatinib in Frontline Therapy of Ph+ ALL
• Patients with newly diagnosed Ph+ ALL received 8 cycles of hyper-CVAD alternating with high dose MTX and cytarabine every 21 days
• Ponatinib was given at 45mg daily po for days 1-14 of cycle 1 then continuously for cycle 2-8
• Patients in CR received maintenance with ponatinib45mg daily, vincristine and prednisolone monthly for 2 years followed by ponatinib indefinitely
Jabbour E, et al. Blood 2014;124:2289

• 34 patients with untreated Ph+ ALL and 3 patients treated with 1 previous course received a median of 6 cycles (range 2-8)
• 10 patients are receiving maintenance in CR
• 3 patents have completed maintenance and are receiving TKI alone
Phase II Study of Combination of Hyper-CVAD + Ponatinib in Frontline Therapy of Ph+ ALL
Jabbour E, et al. Blood 2014;124:2289

• All patients (N = 37) achieved CR after cycle 1
• 32 patients with cytogenetic analysis at baseline
• 30 (94%) achieved CCyR after 1 cycle
• 1 had mCyR
• 1 had no CG analysis at CR
• 35 patients (95%) achieved MMR and 26 (70%) CMR
• Median time to MMR and CMR were 3 and 10 week
• MRD is negative in 35/36 evaluable patients (97%)
• 9 (24%) received allo-BMT after a median of 4 cycles
Phase II Study of Combination of Hyper-CVAD + Ponatinib in Frontline Therapy of Ph+ ALL
Jabbour E, et al. Blood 2014;124:2289
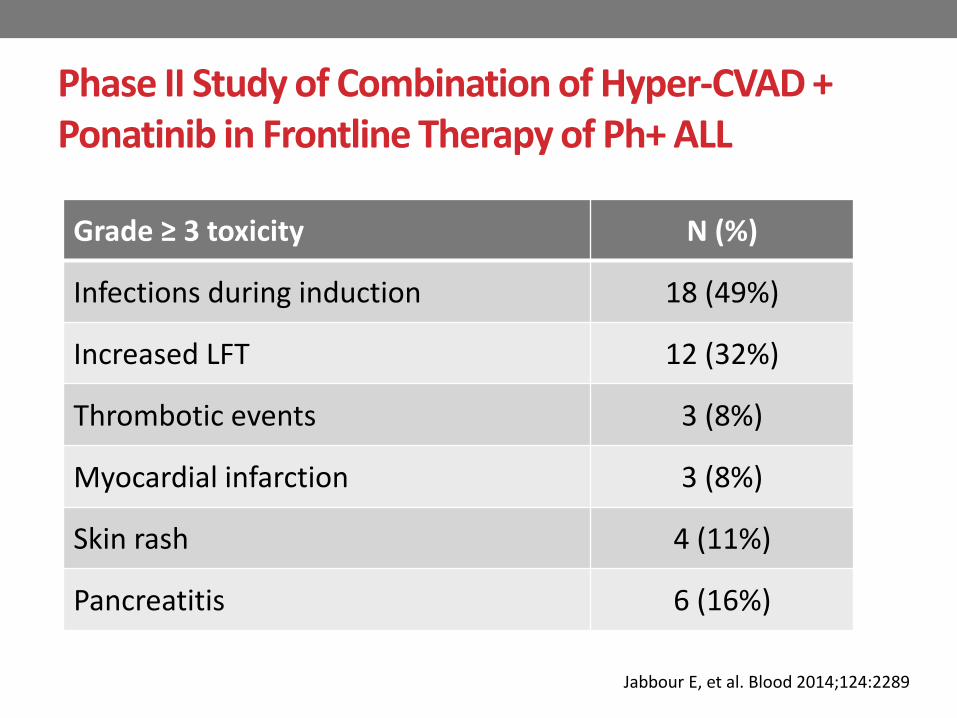
Grade ≥ 3 toxicity N (%)
Infections during induction 18 (49%)
Increased LFT 12 (32%)
Thrombotic events 3 (8%)
Myocardial infarction 3 (8%)
Skin rash 4 (11%)
Pancreatitis 6 (16%)
Phase II Study of Combination of Hyper-CVAD + Ponatinib in Frontline Therapy of Ph+ ALL
Jabbour E, et al. Blood 2014;124:2289

• With a median FU of 18 months (9 - 31), 31 patients are alive
• Causes of death:
• unrelated cardiac event after off therapy and was on imatinib
• multi-organ failure (C2D13)
• NSTEMI (CsD41)
• potential MI (C4D42)
• head injury sustained after a fall (C4D13)
• sepsis post allo-BMT
Phase II Study of Combination of Hyper-CVAD + Ponatinib in Frontline Therapy of Ph+ ALL
Jabbour E, et al. Blood 2014;124:2289
• At the last follow-up,
• 8 patients (19%) are alive post allo-BMT
• 14 patients on ponatinib 15mg daily
• 1 patient on ponatinib 30mg daily
• 7 patients were switched to dasatinib
• 2 patient were switched to imatinib/nilotinib (1 each)
• 1 year PFS and OS were 96% and 86% respectively
• The combination of hyperCVAD with ponatinib is highly effective in patients with Ph+ ALL
Phase II Study of Combination of Hyper-CVAD + Ponatinib in Frontline Therapy of Ph+ ALL
Jabbou E, et al. Blood 2014;124:2289
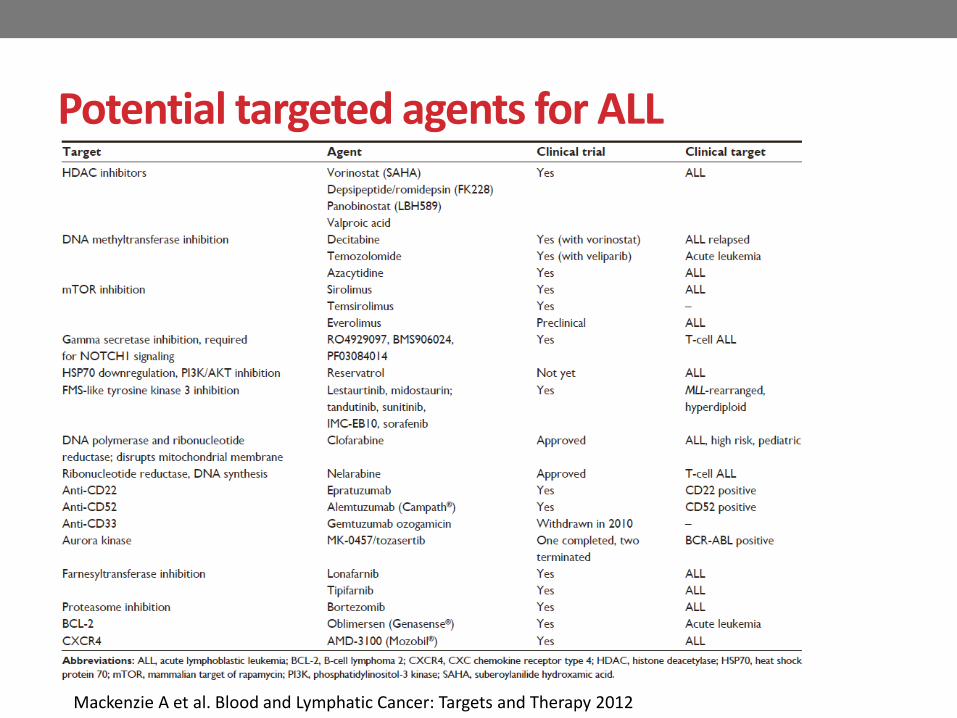
Potential targeted agents for ALL
Mackenzie A et al. Blood and Lymphatic Cancer: Targets and Therapy 2012

• Phase 1 study with 2 parts: decitabine alone or in combination with Hyper-CVAD
• Decitabine was given IV at doses of 10–120 mg/m2 per day for 5 days
Benton CB, et al. BJH 2014

Decitabine +/- Hyper-CVADBenton CB, et al. BJH 2014

Decitabine +/- Hyper-CVAD
Benton CB, et al. BJH 2014

Benton CB, et al. BJH 2014
Decitabine +/- Hyper-CVAD
• Decitabine was tolerated at all doses administered
• Grade 3 or 4 toxic effects included non-life-threatening hepatotoxicity and hyperglycemia.
• Induction of DNA hypomethylation was observed at doses of decitabine up to 80 mg/m2
• Decitabine +/- Hyper-CVAD is safe and has clinical activity in patients with advanced ALL
Decitabine +/- Hyper-CVAD
Benton CB, et al. BJH 2014

• To investigate the tolerability and efficacy of decitabine and vorinostat plus chemotherapy in relapse/refractory ALL
Burke MJ, et al. 2014
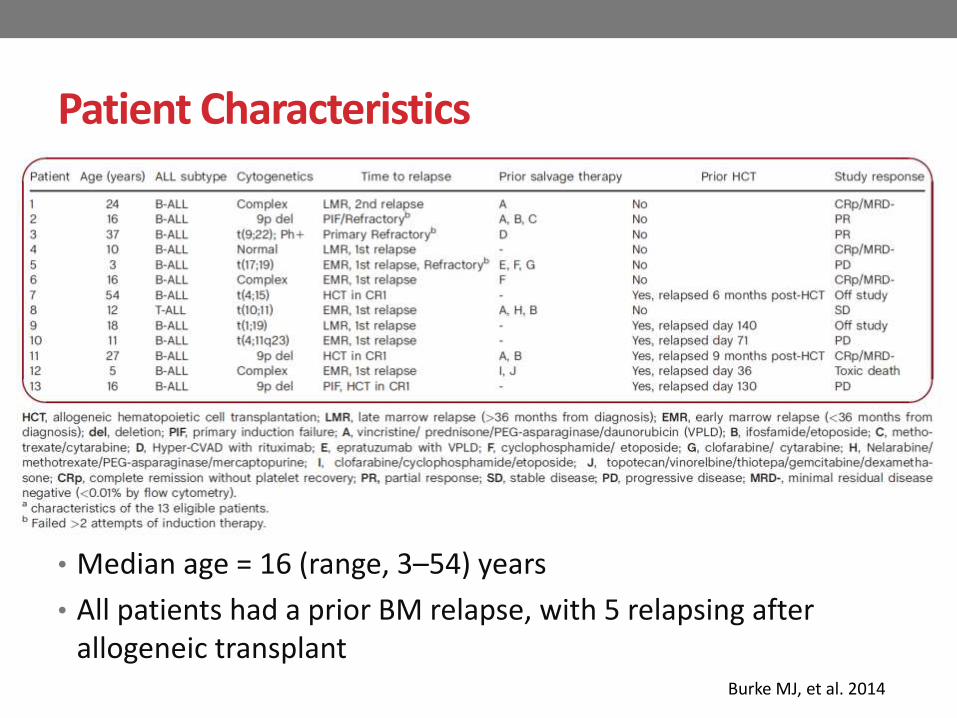
Patient Characteristics
• Median age = 16 (range, 3–54) years
• All patients had a prior BM relapse, with 5 relapsing after allogeneic transplant
Burke MJ, et al. 2014

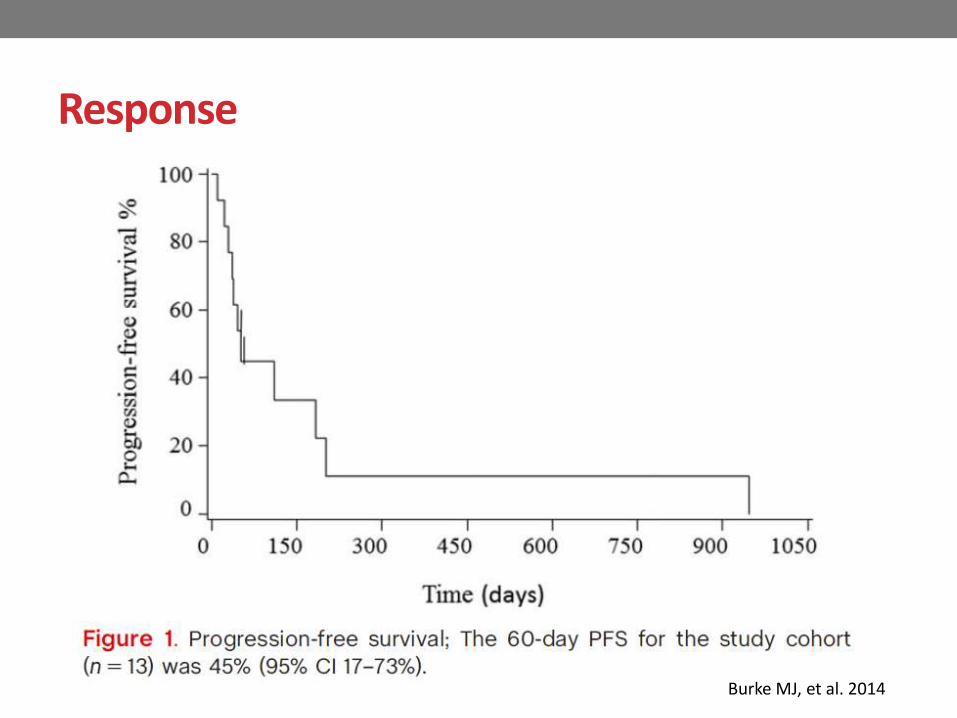
Response
• Of the 13 eligible patients
• 4 (31%) achieved CR without platelet recovery (CRp)
• 2 (15%) partial response (PR)
• 1 (8%) stable disease (SD)
• 1 (8%) progressive disease (PD)
• 2 (15%) deaths on study
• 3 (23%) did not have end of therapy evaluations
• Overall response rate = 46.2% (CRp + PR)
Burke MJ, et al. 2014
Response
Burke MJ, et al. 2014

Burke MJ, et al. 2014
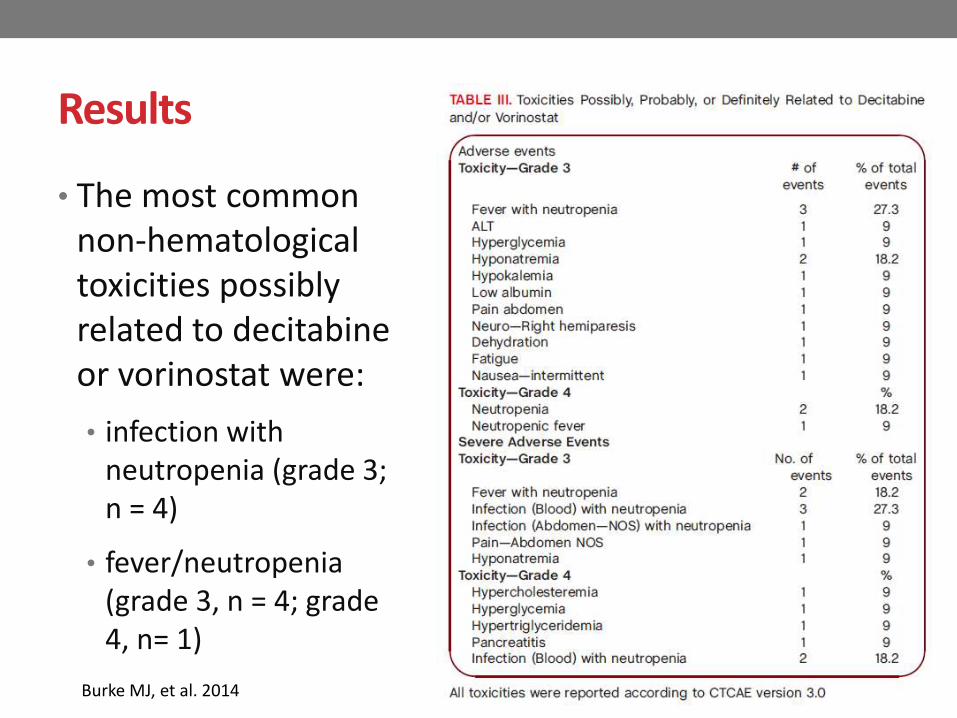
Results
• The most common non-hematological toxicities possibly related to decitabineor vorinostat were:
• infection with neutropenia (grade 3; n = 4)
• fever/neutropenia (grade 3, n = 4; grade 4, n= 1)
Burke MJ, et al. 2014

• Decitabine and vorinostat followed by re-induction chemotherapy was tolerable and demonstrated clinical benefit in relapsed patients with ALL
• Methylation differences were identified between responders and non-responders indicating inter-patient variation, which could impact clinical outcome
Burke MJ, et al. 2014

Summary
• New approaches are needed to improve the cure rate for adult patients with ALL
• Pediatric-inspired regimens have been shown to be feasible with promising results in older patients but more clinical trials are needed to confirm their benefits and toxicities
• Improved understanding of the molecular pathways, development of more precisely targeted agents and incorporation of these novel agents into frontline induction therapy may further improve the outcomes

The End
Thank you