Embed Size (px)
Citation preview
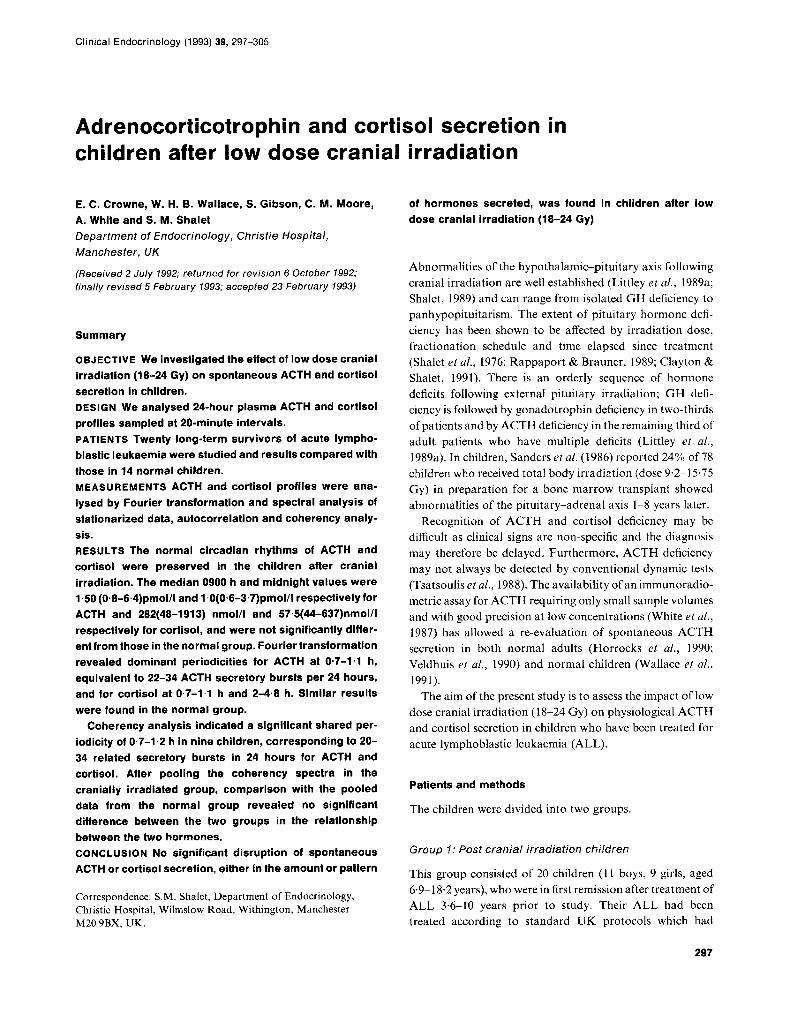
Clinical Endocrinology (1993) 39, 297-305
Adrenocorticotrophin and cortisol secretion in children after low dose cranial irradiation
E. C. Crowne, W. H. B. Wallace, S. Gibson, C. M. Moore, A. White and S. M. Shalet Department of Endocrinology, Christie Hospital, Manchester, UK
(Received 2 July 1992; returned for revision 6 Ocfober 1992; finally revised 5 February 1993; accepted 23 February 1993)
Summary
OBJECTIVE We investigated the effect of low dose cranial irradiation (18-24 Gy) on spontaneous ACTH and cortisol secretion in children. DESIGN We analysed 24-hour plasma ACTH and cortisol profiles sampled at 20-minute intervals. PATIENTS Twenty long-term survivors of acute lympho- blastic leukaemia were studied and results compared with those in 14 normal children. MEASUREMENTS ACTH and cortisol profiles were ana- lysed by Fourier transformation and spectral analysis of stationarired data, autocorrelation and coherency analy- sis. RESULTS The normal circadian rhythms of ACTH and cortisol were preserved in the children after cranial irradiation. The median 0900 h and midnight values were 1.50 (0.8-6.4)pmolll and 1 ~O(0~6-3~7)pmolll respectively for ACTH and 282(48-1913) nmol/l and 575(44-637)nmol/l respectively for cortisol, and were not significantly differ- entfrom those in the normal group. Fourier transformation revealed dominant periodicities for ACTH at 0.7-1.1 h, equivalent to 22-34 ACTH secretory bursts per 24 hours, and for cortisol at 0.7-1.1 h and 2-4.8 h. Similar results were found in the normal group.
Coherency analysis indicated a significant shared per- iodicity of 0.7-1.2 h in nine children, corresponding to 20- 34 related secretory bursts in 24 hours for ACTH and cortisol. After pooling the coherency spectra in the cranially irradiated group, comparison with the pooled data from the normal group revealed no significant difference between the two groups in the relationship between the two hormones. CONCLUSION No significant disruption of spontaneous ACTH or cortisol secretion, either in the amount or pattern
Correspondence: S.M. Shalct, Department of Endocrinology, Christie Hospital, Wilmslow Road, Withington, Manchester M20 9BX. UK.
of hormones secreted, was found in children after low dose cranial irradiation (18-24 Gy)
Abnormalities of the hypothalamic-pituitary axis following cranial irradiation are well established (Littley et a/., 1989a; Shalet, 1989) and can range from isolated G H deficiency to panhypopituitarism. The extent of pituitary hormone defi- ciency has been shown to be affected by irradiation dose, fractionation schedule and time elapsed since treatment (Shalct et ul., 1976; Rappaport & Brauner, 1989; Clayton & Shalet, 1991). There is an orderly sequence of hormone deficits following external pituitary irradiation; G H defi- ciency is followed by gonadotrophin deficiency in two-thirds of patients and by ACTH deficiency in the remaining third of adult patients who havc multiple deficits (Littley er a/., 1989a). In children, Sanders et al. (1 986) reported 24% of 78 children who received total body irradiation (dose 9.2- 15.75 Gy) in preparation for a bone marrow transplant showed abnormalities of the pituitary-adrenal axis 1-8 years later.
Recognition of ACTH and cortisol deficiency may be difficult as clinical signs are non-specific and the diagnosis may therefore be delayed. Furthermore, ACTH deficiency may not always be detected by conventional dynamic tests (Tsatsoulis et ul., 1988). The availability of a n immunoradio- metric assay for ACTH requiring only small sample volumes and with good precision at low concentrations (White et al., 1987) has allowed a re-evaluation of spontaneous ACTH secretion in both normal adults (Horrocks et al., 1990; Veldhuis et a/., 1990) and normal children (Wallace et al., 1991).
The aim of the present study is to assess the impact of low dose cranial irradiation (18-24 Gy) on physiological ACTH and cortisol secretion in children who have been treated for acute lymphoblastic leukaemia (ALL).
Patients and methods
The children were divided into two groups.
Group I: Post cranial irradiation children
This group consisted of 20 children ( 1 1 boys, 9 girls; aged 6.9-18.2 years), who were in first remission after treatment of ALL 3.6-10 years prior to study. Their ALL had been treated according t o standard UK protocols which had
297

298 €. C. Crowne et a / . Clinical Endocrinology (1993) 39
included prophylactic cranial irradiation (18 Gy in 10 fractions over 14 days, n = 17; 24 Gy in 12 fractions over 21 days, I I = 3).
Group 2: Normal children
Details of these 14 children (9 boys, 5 girls; aged 3.0-15.5 years) have previously been reported (Wallace et a/ . , 1991). In brief, eight were normal siblings of Group 1 and six were children with familial short stature but normal growth velocities and normal G H responses to standard provocation tests. They were undergoing hormone investigations as part of on-going studies of G H secretion.
The children were admitted the night before sampling to acclimatize to the hospital. None of the children showed any cvidcncc of chronic disease or wcrc taking any medication. Pubertal staging was performed according to Tanner (1 962).
Samples were taken every 20 minutes for 24 hours (0900- 0900 h). Thc children rcmained ambulant and ate meals a t appropriate times. Extension tubing was attached at night to avoid disturbance of sleep. Samples were collected into heparinized containers, centrifuged and separated every hour, and then stored at -70°C until assayed. Care was taken to ensure that the total volume of blood taken was always less than 8% of the subject's estimated blood volume.
The study was approved by the local ethical committee and written informed consent given by a parent for cach child.
Assays
All samples from one individual were measured in duplicate in the same assay. ACTH was measured in unextracted plasma using a two-site immunoradiometric assay (White et a/., 1987) which detects intact ACTH but not ACTH fragments (detection limit 1 pmol/l). Two monoclonal antibodies were employed; radiolabelled antibody IA12 binds to ACTH 10-18, and antibody 2A3 coupled to Sephacryl for the solid phase of the assay binds to ACTH 24- 39.
Cortisol was measured in unextracted plasma at low pH to eliminate binding by corticosteroid binding proteins. Corti- sol antiserum was preincubated with donkey anti-sheep antiserum and normal sheep serum (Scottish Antibody Production Unit) diluted in 0.13 M sodium chloride/phos- phate buffer, pH 4.0. This was then incubated with cortisol- 3-carbo~ymethyloxime~~~1 histamine and either standard or sample for 90 rninutcs at 37"C, centrifuged, separated and the supernatant counted in a multigamma counter.
Anafysis
The regularly sampled ACTH and cortisol profiles each form classical time series and are therefore amenable to spectral analysis. The profiles wcre examined to look at the impact of cranial irradiation on both the underlying patterns of secretion of ACTH and cortisol considcred separately, and the shared pulsatile features of the paired hormones. These techniques of hormone profile analysis have bccn uscd previously by Follenius et ul. (1987) for ACTH and cortisol, Veldhuis and Johnson (1988) for prolactin and LH, and Wallace et a/. (1991) also for ACTH and cortisol. The basic approach is an extension of cross-spectral analysis into coherency, where It is the shared spectral propcrtics that are of primary interest. The coherency spectrum has some advantages over the cross spectrum itself. Spectral analysis and coherency are discussed in the appendix.
Statistics
The areas under the curve (AUC) were calculated by the Gill-Miller Quadrature method (Gill & Millcr, 1972). Diffcr- ences between groups of individual factors were analysed using the Mann-Whitney U-test initially. In addition, allow- ance for possible interactions between the three factors, namely treatment group, sex and pubertal status, were investigated using a rcgression approach to the analysis of unbalanced data. The hormone data were clearly not normally distributed on thc original scale of measurement and suitablc lransformations were required, namely the square root of the ACTH data and logarithmic transforma- tion of the cortisol data. The necessary assumptions for the analysis were satisfied with the transformed scales. Results are expressed as median(range).
Results
A normal circadian rhythm of ACTH and cortisol secretion was preserved in the children who had received cranial irradiation. The median 0900 h and midnight ACTH values were 1.5 (0.8-6.4)pmol/l and 1 .O (0.6-3.7)pmol/l respect- ively. The midnight value was below the level of detection of the ACTH assay in nine subjects. For cortisol the 0900 h and midnight values were 282 (48-1913)nmol/l and 57.5 (44- 637)nmo1/1 respectively.
The median AUC for ACTH and cortisol for Groups 1 and 2 sub-divided according to pubertal status are shown in Table 1. There was no significant difTerence within Group 1 between the prepubertal and pubertal children, or thc males and females, for either ACTH or cortisol AUC, mean 0900 or midnight value. Analysis of variance was used to look for any interactions of irradiation, pubertal status or sex on the
Clinical Endocrinology (1993) 39
Table 1 Comparison of ACTH and cortisol profiles (median (range)) in children after low dose cranial irradiation (Group 1) with those in normal children (Group 2)
Table 2 Fourier transform of autocovariance data for ACTH and cortisol in children after cranial irradiation
ACTH and cortisol secretion after cranial irradiation 299
Group 1
ACTH (AUC) Cortisol (AUC) n (pmol/l h) (nmolil h) n
Total 20 32 (3-90) 4931 (3154-7242) 14 Prepubertal 7 25 (8-54) 4512 (3154-5842) 9 Pubertal 13 36 (3-90) 4936 (3778-7242) 5
Group 2
ACTH (AUC) Cortisol (AUC) (pmoI/l h) (nmol/l h)
30 (9-54) 5114 (3562-8631) 29 (9-54) 5223 (4627-863 I ) 30 (12-47) 4290 (3562-4833)
~~ ~ ~~
ACTH dominant
Subject frequencies
Prepubertal I 0.8' 2 0.8* 0.9* 1.5 3 0.7* 0.9* 4 0.9* 1.0 2.0t 5 0.9* 1.3 6 0,8* 1.0 7 I.1*
8 0.8* 2.4 9 0.8*
10 0.7* 11 0.7* 0.9* 12 0.7* 13 0.7* 14 0.9* 15 0,7* 1.4t 3.0 16 0,8* 17 1.0* 18 0.9* 1.1' 19 NIL 20 0.7*
Pubertal
Cortisol dominant
frequencies
Coherency significantly shared
periodicities
0.8* 1.2 3.7 0.8* 0.9* 1.7 0.7* 0.9* 3.7 0,8* 2.17 I . l * 1.8 3.7 0.7* 1.3 2.7 1.0* 1,2* 2.0
0.8* 1.3 3.2 0.7* 1.4 2.3 4.4 0.7* 0.8* 2.5 0,7* 0.9* 1.6 2.3 1.6 0.8* 1.2 2.3 0.7* 0,9* 1.8 0.7* 0.9* 4.8 0.8* 1.4t 2.5 0.8* 1.2 4.8/1 0.7 0.9* 1.5 0,8* 1.1* 2.5 1.0 1.2 2.5 0.8* 1.2 2.3
0.7* 0.9' 1.3 0,7* 0.9* 1.7 3.4 0.8* 1.9t 2.7 5.3 0.7 4.0 1.4 2.2 0.8 0.9* 2-1
2.7 Nil Nil (near 1.0) (Near 1.0) 3.4 Nil 0.7* 0,8* 3.2 I.O* 2.3 0.8* 1.9 2.7 5.3 1.2* 1.5 2.3 I.O* 2.5 Nil (near 1.1) 0.9* 2.5
Values are in hours. *and 7, Related periodicities.
amount (i.e. AUC or mean level) of hormone secreted. There was no significant effect of these factors on ACTH secretion. Cortisol secretion did not show any effect of sex, either alone or combined with the other factors. Analysis of variance did however show a significant interaction of pubertal status and treatment group on cortisol secretion (P=0.01). It can be seen in Table 1 that cortisol AUC is lower in the pubertal normal group when compared with the prepubertal group. There is no significant difference in the irradiated group and the trend is in the opposite direction.
The dominant periodicities revealed by Fourier transfor- mation of the autocovariance data of both ACTH and cortisol in Group 1 are shown in Table 2. Univariate spectra
(the first two columns) show individual characteristic perio- dicities but say nothing about how closely related are ACTH and cortisol. The coherency data in the third column identify what is effectively the square of the linear correlation between ACTH and cortisol at each periodicity. The closer the coherency to unity, the more closely related are ACTH and cortisol secretory processes during a given period.
The results arc very similar to those found in the normal children (Wallace et al., 1991). Cortisol shows two significant periodicies, at 0.7-1 ' 1 h and 2-4.8 h (cf.O.7-1.0 h and 2-3.2 h in Group 2). ACTH has dominant periodicities at 0.7-1.1 h, equivalent to 22-34 ACTH secretory bursts per 24 hours (cf. 0.7-1.0 h in Group 2).
300 E. C. Crowne e ta / . Clinical Endocrinology (1993) 39
2 1.0 V
0.6
0 . 2
1.0
0.6
0 - 2
4.8 1.6 0.96 0-68 4.8 1-6 0.960.68 4.8 1.6 0.96 0.68 4.8 1.6 0-46 0.68 4.8 1.6 0.96 0.66
Periodicity ( h )
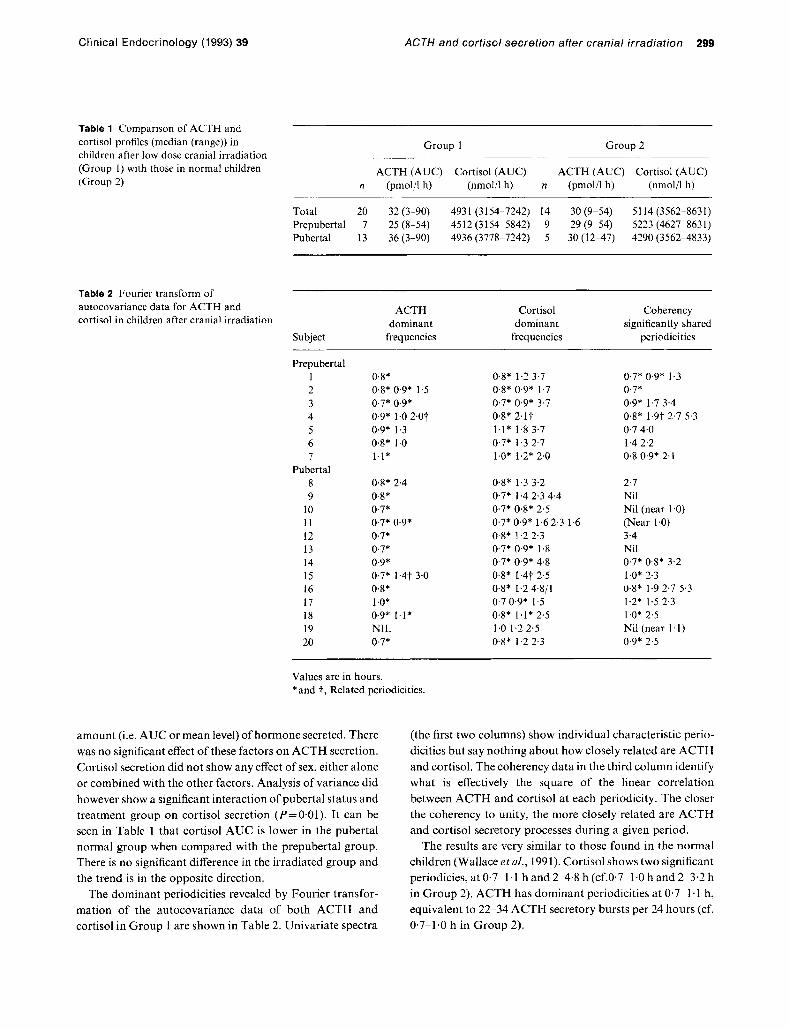
Table 2 also shows the significant shared periodicities between ACTH and cortisol (i.e. those that have achieved a 9S'X confidence levcl) for Group 1 . The coherency spectrum for each child in Group 1 is shown in Fig. 1. There is a significant shared periodicity of 0.7-1.2 h in nine childrcn, corresponding lo 20-34 related secretory bursts in 24 hours for ACTH and cortisol. I t is interesting to note in the pubertal group, although there are significant periodicities for both ACTH and cortisol a t 0.8 1.0 h in most of the individual profiles, Lhese do not achieve significance in the coherency data because the longer periodicities of 1.6-3.4 h are the more dominant for cortisol.
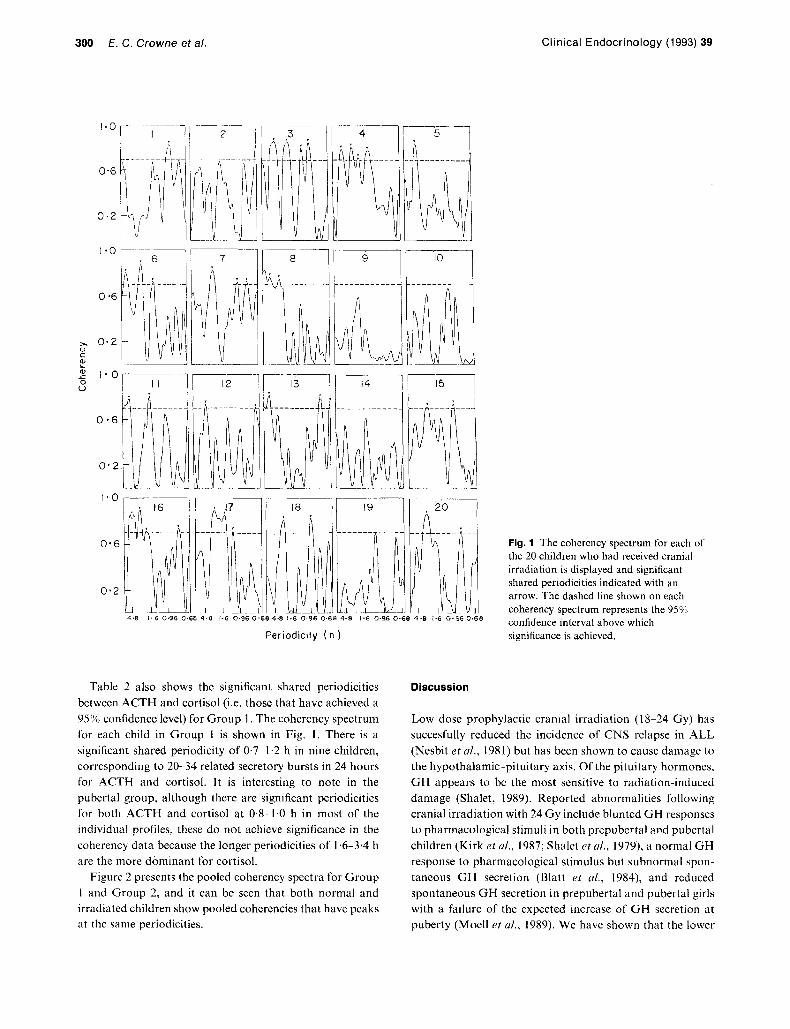
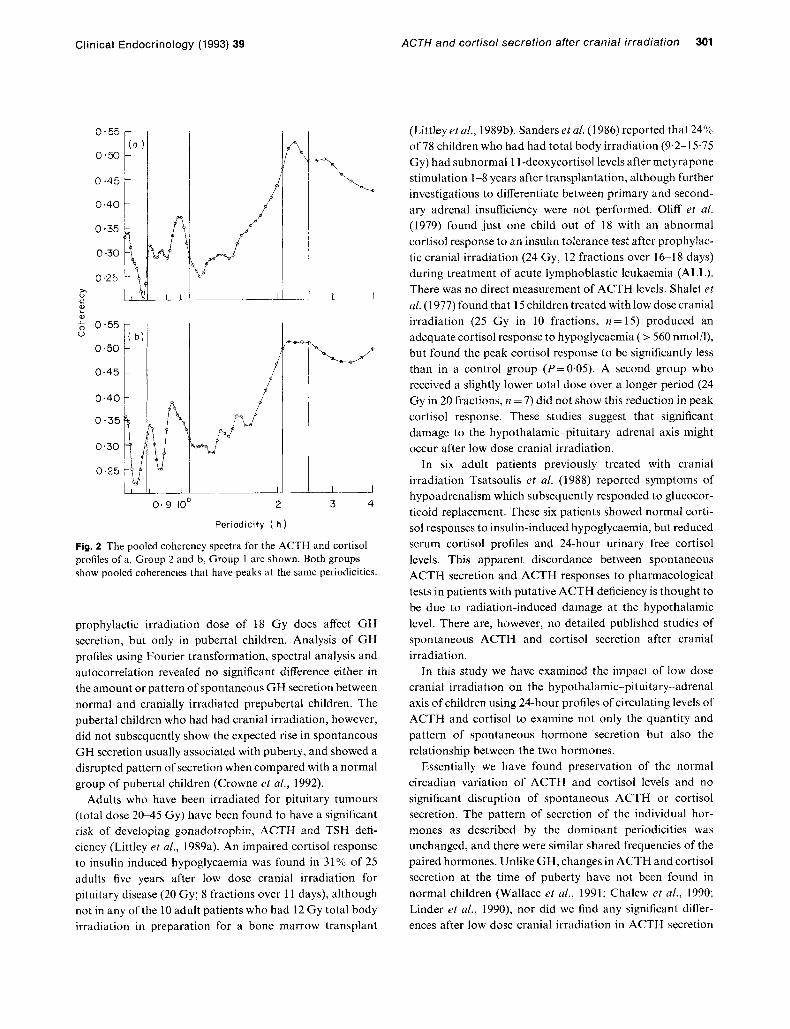
Figure 2 presents the pooled coherency spectra for Group 1 and Group 2, and it can be seen that both normal and irradiated children show pooled cohcrcncics that have peaks at the same periodicities.
Fig. 1 The coherency spectrum for each of the 20 children who had received cranial irradiation is displayed and significant shared periodicities indicated with an arrow. The dashed line shown on each coherency spectrum represents the 95% confidence interval above which significance is achieved
Discussion
Low dose prophylactic cranial irradiation (18-24 Gy) has succesfully reduced the incidence of CNS relapse in ALL (Nesbit et al., 1981) but has been shown to cause damage to the hypothalamic-pituitary axis. Of the pituitary hormones, G H appears to bc the most sensitive to radiahn-induced damage (Shalet, 1989). Reported abnormalities following cranial irradiation with 24 Gy include blunted G H responses to pharmacological stimuli in both prepubertal and pubertal children (Kirk et al., 1987; Shalet et al., 1979), a normal G H response to pharmacological stimulus but subnormal spon- tancous GH secretion (Blatt et al., 1984), and reduced spontaneous GH secretion in prepubertal and pubertal girls with a failurc of the expected increase of GH secretion at puberty (Moell et ul., 1989). We havc shown that the lower
Clinical Endocrinology (1993) 39
0.45
0.40
I / d
L a
0 5 0.55
0.45
0.40
0.35 I 1
0.30
0.25
P i
0.9 loo 2
Periodicity ( h )
I
I_-/ 3 4
Fig. 2 The pooled coherency spectra for the ACTH and cortisol profiles of a, Group 2 and b, Group 1 are shown. Both groups show pooled coherencies that have peaks at the same periodicities.
prophylactic irradiation dose of 18 Gy does affect G H secretion, but only in pubertal children. Analysis of GH profiles using Fourier transformation, spectral analysis and autocorrelation revealed no significant difference either in the amount or pattern of spontaneous G H secretion between normal and cranially irradiated prepubertal children. The pubertal children who had had cranial irradiation, however, did not subsequently show the expected rise in spontaneous G H secretion usually associated with puberty, and showed a disrupted pattcrn of secretion when compared with a normal group of pubertal children (Crowne et a[., 1992).
Adults who have been irradiated for pituitary tumours (total dose 20-45 Gy) have been found to have a significant risk of developing gonadotrophin, ACTH and TSH defi- ciency (Littley et a[., 1989a). An impaired cortisol response to insulin induced hypoglycaemia was found in 31% of 25 adults five years after low dose Cranial irradiation for pituitary disease (20 Gy; 8 fractions over 11 days), although not in any of the 10 adult patients who had 12 Gy total body irradiation in preparation for a bone marrow transplant
ACTH and cortisol secretion after cranial irradiation 301
(Littleyetul., 1989b). SandersetaL(1986)reported that24% of 78 children who had had total body irradiation (9.2-1 5.75 Gy) had subnormal 1 I-deoxycortisol levels after metyrapone stimulation 1-8 years after transplantation, although further investigations to differentiate between primary and second- ary adrenal insufficiency were not performed. Oliff et al. (1979) found just one child out of 18 with an abnormal cortisol response to an insulin tolerance test after prophylac- tic cranial irradiation (24 Gy, 12 fractions over 16-1 8 days) during treatment of acute lymphoblastic leukaemia (ALL). There was no direct measurement of ACTH levels. Shalet et a[. (1 977) found that 15 children treated with low dose cranial irradiation (25 Gy in 10 fractions, n = 15) produced an adequate cortisol response to hypoglycaemia ( > 560 nmol/l), but found the peak cortisol response to be significantly less than in a control group (P=O.O5). A second group who received a slightly lower total dose over a longer period (24 Gy in 20 fractions, n = 7) did not show this reduction in peak cortisol response. These studies suggest that significant damage to the hypothalamic-pituitary-adrenal axis might occur after low dose cranial irradiation.
In six adult patients previously treated with cranial irradiation Tsatsoulis et al. (1988) reported symptoms of hypoadrenalism which subsequently rcsponded to glucocor- ticoid replacement. These six patients showed normal corti- sol responses to insulin-induced hypoglycaemia, but reduced serum cortisol profiles and 24-hour urinary free cortisol levels. This apparent discordance between spontaneous ACTH secretion and ACTH responses to pharmacological tests in patients with putative ACTH deficiency is thought to be due to radiation-induced damage at the hypothalamic level. There are, however, no detailed published studies of spontaneous ACTH and cortisol secretion after cranial irradiation.
In this study we have examined the impact of low dose cranial irradiation on the hypothalamic-pituitary-adrenal axis of children using 24-hour profiles of circulating levels of ACTH and cortisol to examine not only the quantity and pattern of spontaneous hormone secretion but also the relationship between the two hormones.
Essentially we have found preservation of the normal circadian variation of ACTH and cortisol levels and no significant disruption of spontaneous ACTH or cortisol secretion. The pattern of secretion of the individual hor- mones as described by the dominant periodicities was unchanged, and thcre were similar shared frequencies of the paired hormones. Unlike GH, changes in ACTH and cortisol secretion at the time of puberty have not been found in normal children (Wallace et ul., 1991; Chalew et a/., 1990; Linder et al., 1990), nor did we find any significant differ- ences after low dose cranial irradiation in ACTH secretion

302 E. C . Crowne et a/ . Clinical Endocrinology (1993) 39
between the prepubertal and pubertal groups. There did appear to bc a significant interaction between pubertal status and treatment group and thc amount of cortisol secreted. This is probably caused by the decrease in cortisol levels between the normal prepubertal and pubertal groups (5223 us 4290 iimol/lh). In view of the small numbers in the normal pubertal group (n=5) and the fact that this has not been found by other workers, the physiological significance of this result remains unknown.
We have not subjected our patients to the stress of insulin- induced hypoglycaemia but at some time during the 24-hour profile 17 of our 20 patients showed a cortisol level in excess of 500 nmol/l, and the remainder had values bctween 450 and 500 nmol/l. Values of this order if obtained during an insulin tolerance test would be interpreted as reflecting an intact hypothalamic-pituitary-adrenal axis.
In conclusion, despite the existing literature indicating significant potential for irradiation damage to the hypothala- mic-pituitary-adrenal axis, identified using pharmacologi- cal stimulation tests, we have found no significant disruption of spontaneous ACTH and cortisol secretion after low dose cranial irradiation (18-24 Gy over 14-21 days) in prcpuber- tal and pubertal children.
Acknowledgements
We would like to thank Dr P. H. Morris-Jones and Dr D. A. Price for permission to study patients under their care, and I). Ryder for statistical advice.
This study was supported by a grant from the Leukaemia Research Fund. S. Gibson was funded by the Cancer Research Campaign.
References
Blatt, J., Bercu, B.B., Gillin, J.C., Mendelson, W.B. & Poplack, D.G. (1984) Reduced pulsatile growth hormone secretion in children after therapy for acute lymphoblastic leukaemia. Journal of Paediatrics, 104, 182-186.
Chalew, S.A., Zadik, Z., McCarter, R. & Kowarski, A.A. (1990) Hypocortisolemia in children undergoing evaluation for growth hormone deficiency. Journal of Clinical Endocrinology and Metah- o h m , 71, 952-957.
Clayton, P.E. & Shalet, S.M. (1991) Dose dependency of time of onset of radiation-induced growth hormone deficiency. Journal nf Paediatrics, 118, 226-228.
Crowne, E.C., Moore, C., Wallace, W.H.B., Ogilvy-Stuart, A.L., Addison, G.M., Morris-Jones, P.H. & Shalet, S.M. (1992) A novel variant of growth hormone (GH) insufficiency following low dose cranial irradiation. Clinical Endocrinology, 36, 59-68.
Follenius, M., Simon, C., Brandenberger, G. & Lenzi, P. (1987)
Ultradian plasma corticotrophin and cortisol rhythms: time series analyses. Journal of Endocrinological Invrstigation, 10, 261 266.
Gill, P.E. & Miller, G.F. (1972) An algorithm for the integration of unequally spaced data. Computing Journal, 15, 80-83.
Horrocks, P.M., Jones, A.F., Ratcliffe, W.A., Holder, G., White, A., Holder, R., Ratcliffe, J.G. & London, D.R. (1990) Patterns of ACTH and cortisol pulsatility over 24 hours in normal males and females. Clinical Endorrinolugy, 32, 127-1 34.
Kirk, J.A., Raghupathy, P., Stevens, M.M., Cowell, C.T., Menser, M.A., Bergin, M., Tink, A., Vines. R.H. & Silink, M. (1987) Growth failure and growth hormone deficiency after treatment for acute lymphoblastic leukaemia. I m c e t , i, 190-193.
Linder, B.L., Esteban, N.V., Yergey, A.L., Winterer, J.C., Loriaux, D.L. & Cassoria, F. (1990) Cortisol production rate in childhood and adolescence. Jnurnal of Pediatrics, 117, 892-896.
Littley, M.D., Shalet, S.M., Beardwell, C.G., Ahmed, S.R., Apple- gate, G. & Sutton, M.L. (1989a) Hypopituitarism following external radiotherapy for pituitary tumours in adults. Quarterly Journal ($Medicine, 262, 145-160.
Littley, M.D., Shalet, S.M., Beardwell, C.G., Robinson, E.L. & Sutton, M.L. (1989b) Radiation-induced hypopituitarism is dose- dependent. Clinical Endocrinology, 31, 363-373.
Ljung, G.M. & Box, G.E.P. (1978) On a measure of lack of fit in time series models. Biornetrica, 65, 297-303.
Lynn, P.A. (1973) An Introduction to the Analysis and Proctwing oj’ Signals. Macmillan.
M o d , C., Garwicz, S., Westgren, U., Wiebe, T. & Albertsson- Wiklund, K. (1989) Suppressed spontaneous secretion of growth hormone in girls after treatment for acute lymphoblastic leukae- mia. Archive of Disease in Childhood, 64, 252-258.
Nesbit, M.E., Sather, H.N., Robinson, L.L., Ortega, J., Littman, P.S., D’Angio, G.J. & Denman Hammond, G. (1981) Presympto- matic central nervous system therapy in previously untreated childhood acute lymphoblastic leukaemia: comparison of 1800 and 2400 rdd. Lancet, i, 461-466.
Oliff, A,, Bode, U., Bercu, B.B., Di Chiro, G., Graves, V. & Poplack, D.G. ( I 979) Hypothalamic-pituitary dysfunction following CNS prophylaxis in acute lymphocytic leukaemia: correlation with CT scan abnormalities. Medical and Pediatric Oncology, 7, 141-151.
Priestley, M.B. (1981) Specrral Analysis and Time Series. Volumes 1 and 2. Academic Press.
Rappaport, R . & Brauner, R. (1989) Growth and endocrine disorders secondary to cranial irradiation. Pediatric Research, 25, 561-567.
Sanders, J.E., Pritchard, S., Mahoney. P., Amos, D., Buckner, C.D., Witherspoon, R.P., Deeg, H.J., Doney, K.C., Sullivan, K.M., Appelbaum, F.R., Storb, R. &Thomas, E.D. (1986) Growth and development following marrow transplantation for leukaemia.
Shalet, S.M. (1989) Endocrine consequences of treatment of malig- nant disease. Archives of Disease in Childhood, 64, 1635-1641.
Shalet, S.M., Beardwell, C.G., Morris-Jones, P.H. 8.1 Pearson, D. (1976) Growth hormone deficiency after treatment of acute lymphoblastic leukaemia in children. Archives of’ Disease in Childhood, 51,489-493.
Shalet, S.M., Beardwell, C.G., Twomey, J.A., Morris Jones, P.H. & Pearson, D. (1977) Endocrine function following the treatment of acute leukaemia in childhood. Journal of Pediatrics, 90, 920 923.
Shalet, S.M., Price, D.A., Beardwell, C.G., Morris-Jones, P.€I. & Pearson, D. (1979) Normal growth despite abnormalities of
Blood, 68, 1129-1 135.

Clinical Endocrinology (1993) 39
growth hormone secretion in children treated for acute leukaemia. Journal of Pediatrics, 94, 719-722.
Tanner, J.M. (1962) Growth at Adolescence. Blackwell Scientific Publications, Oxford.
Tsatsoulis, A, , Shalet, S.M., Harrison, J.M., Ratcliffe, W.A., Beardwcll, C.G. & Robinson, E.L. ( I 988) Adrenocorticotrophin (ACTH) deficiency undetected by standard dynamic tests of the hypothalamic ~ pituitary-adrenal axis. Clinical Endocrinology, 28,
Veldhuis, J.D. &Johnson, M. (1988) Operating characteristics of the hypothalamo-pituitary-gonadal axis in men: circadian, ultradian and pulsatile release of prolactin and its temporal coupling with luteinizing hormone. Journal of’ Clinical Endocrinology and Melubolism, 61, 116-123.
Veldhuis, J.D., Iranmanesh, A., Johnson, M.L. & Lizdrrdlde, G. (1990) Amplitude, but not frequency, modulation of adrenocorti- cotropin secretory bursts gives rise to the nyctohemeral rhythm of the corticotropic axis in man. Journal qf Clinical Endocrinology and Metuholism, 11,452-463.
Wallace, W.H.B., Crowne, E.C., Shalet, S.M., Moore, C., Gibson, S., Littley, M.D. &White, A. (1991) Episodic ACTH and cortisol secretion in normal children. Clinical Endocrinology, 34,215 -221.
White, A, , Smith, H., Hoadley, M., Dobson, S.H. & Ratcliffe, J.G. (1987) Clinical evaluation of a two site immunoradiometric assay for adrenocorticotrophin in unextractcd human plasma using monoclonal antibodies. Clinical Endocrinology, 26, 41-52.
225-232.
Appendix: Spectral Analysis
Frequency domain analysis
Both ACTH and cortisol were regularly sampled for 24 hours in each patient, hencc the available data form classic time series. Such series are amenable to both temporal and frequency domain analysis. The fundamental basis of fre- quency domain analysis is that any complex waveform may be represented as the summation of a number of more basic waveforms of a single category. The best known approach is that due to Fourier, where summed basic waveforms are sinusoidal with appropriate amplitudes, periodicities and relativc phases. The Fourier series and the Fourier transform are central to periodic and aperiodic analysis respectively (Lynn, 1973).
Periodic data analysis: Fourier series
When frequency domain analysis is to be applied to a truly periodic data waveform of repetitive pulses then it is appropriate to use the well known Fourier series approach. The description supplied by the Fourier series is accurate for all time, since the periodic data waveform is represented by a summation of sinusoidal functions which are themselves periodic. A graphical plot of the sinusoidal functions and
ACTH and cortisol secretion after cranial irradiation 303
their amplitudes is termed the frequency line spectrum. The line spectrum emphasizes the use of discrete frequency components in Fourier series descriptions.
Aperiodic data analysis: Fourier transforms
The extension of frequency domain analysis to encompass aperiodic data waveforms requires the less well understood Fourier transform. The Fourier transform permits the frequency domain description of data waveforms that are not truly periodic and which d o not exist for all time. Such waveforms can range from noise adulterated pulse sequences to single pulses.
The key to understanding the difference between the Fourier series and the Fourier transform is to focus on the duration and separation of pulses in a waveform. Simple periodic waveforms are composed of pulse trains with identical duration and constant separation. However, an aperiodic data waveform can be constructed from this by allowing pulse separation to increase whilst pulse duration remains constant.
In the limit, a single pulse is left since neighbouring pulses have moved infinitely distant on either side. Since by definition there is a n inverse relationship between time and frequency, the fundamental frequency describing pulse sepa- ration must then tend to zero and the frequency components in the corresponding spectrum must become so closely spaced that the spectrum is continuous. The Fourier trans- form formally embodies these concepts.
Real data analysis: Fourier transforms
The majority of interesting data waveforms are simply not repetitions of similar pulses, and so must be described by Fourier transform analysis. The more complex the data waveform the more statistical information is actually car- ried. Of course, it is the meaning of such statistical informa- tion that is actually sought, since in the extrcme the most complex waveforms may be totally random and of little intrinsic value. The random and the periodic Waveforms represent extremes of data behaviour. Fourier transform analysis can also provide descriptions of random data waveforms, a feature that can be exploited when attempting to glean evidence of non-random behaviour in erratic data. The wide range of data waveforms to which Fourier transform analysis can be applied has ensured its widespread usc in scientific data analysis (Priestley, 1981).
Univariate and bivariate spectral analysis
The ACTH and cortisol time series examined in this and a previous paper (Wallace et al., 1991) individually exhibit some form of regulated pulsatile behaviour. Hence trans-

304 E . C. Crowne et a/ . Clinical Endocrinology (1993) 39
form techniques can provide corresponding frequency spec- tra that, quite expectedly, contain distinct peaks centred about particular frequencies or periodicities. Such analysis is termed univariate. The most widely used approach is to generate a power spectral estimate by Fourier transforming the autocorrelation/covariance function of the stationarized waveform data. Autocorrelation/covariance and power spectral representations are complementary ways of analys- ing waveform data, though power spectra are often more easily interpreted, since by definition they directly portray periodicity.
In this paper the shared periodic features between ACTH and cortisol are of primary interest, rather than features peculiar to cortisol or ACTH individually. To identify shared features requires a bivariate spectral analysis. Just as autocorrelation and the power spectrum are transform related in univariate analysis, so too are cross correlation and cross spectral density in the bivariate case. However, the cross spectral density can exhibit large peaks at given periodicities simply because the particular periodic compo- ncnts arc powerful in only one of the two data waveforms.
Coherency
To identify genuinely shared periodic components a form of modified cross spectrum is required; this IS the coherency spectrum. Coherency is a measure of the interdependence of two data waveforms. Consider the ACTH and cortisol data as the input of interest to bivariate spectral analysis. If to represents periodicity, then the squared coherency is related to the smoothed estimate of the cross-spectrum,fcu(wj, for a cortisol ACTH assay pair, and to the smoothed univariate spectral estimates, fc(wj, fa(wj for cortisol and ACTH respectively. Both fc(w) and fu(wj spectra are computed using the corresponding covariance data. The squarcd coherency, C(UJ), at frequency (11 IS between zero and one and is given by;
Hence the coherency is normalized byfc(ru) andfk(cuj so that periodic components which are very powerful in one hor- mone waveform only, do not give rise to high coherency values as they might in the cross spectrum fca(w).
Coherency and cross spectral analysis are reported by Veldhuis et al. (1988) and Follenius el al. (1987) for prolactin/luteinizing hormone and ACTH/cortisol relation- ships respectively.
Computing coherency
Scientific software libraries incorporate the necessary mathe- matical subroutines required to generate coherency spectra.
The results shown here were obtained using the Numerical Algorithms Group Fortran library section G13. This is available on the Christie Hospital and Paterson Institute’s DEC VAX computer LAN, forming part of the Manchcstcr University Network. The analytical steps for our particular form of time series analysis involved stationarization of data and autoregressive modelling prior to actual computation of coherency results. The computational steps are outlined below. More detailed guidance for this type of analysis can be found in Priestley’s text, Volume 2, chapter 9 on bivariate spectral analysis (Priestley, 1981 j.
Stationarization of cortisol and ACTH data by differencing
Stationarity requires that the probabilistic structure of a time series be unaffected by a shift in the time origin, that is, the series should look similar at whatever point in time observa- tions begin. Raw ACTH and cortisol assay data are clearly not stationary and so require numerical processing, usually by differencing.
Inspection of the functional form of the assay plots indicates the degree of differencing required. For example, where there are only linear trends in the data, first-order differencing will normally sufice. If quadratic behaviour is discernible, then second-order processing can be applied.
Autoregressive-integrated moving average (ARIMA) modelling of both cortisol and ACTH assays
This is an iterative procedure, where the minimum number of model parameters is required for a satisfactory fit to assay data. Test criteria often operate by computing the residuals between the data and the model itself, followed by generation of a statistic measuring remnant correlation in the residuals. A good model fit leaves little correlation in the residuals. The NAG libraries provide for Box--Ljung testing of model adequacy (Ljung & Box, 1978).
Prewhitening of ACTH cortisol data
Consider two time series that are thought to be causally related so that a n input-output relationship can be de- scribed. Then for an uncorrelated input series, also uncorre- lated with other inputs, the cross correlation function describes the interdependence of the two series. Such an input series is described as white noise. In reality, the data forming an input timc series will be correlated and so will require numerical processing to remove correlation. The residuals left from ARIMA modelling of the input data form white noise. If the same ARIMA model is used to filter or

Clinical Endocrinology (1993) 39
‘whiten’ the output data into another set of residuals, then the relationship between the input and output time series is preserved in the corresponding residual series. This pro- cedure is termed prewhitening.
It may be appropriate to align the two modified series by shifting or lagging. The need for this can be determined by inspection of the cross correlations. If any alignment is required then an ARIMA model for the output time series finds use in predicting any necessary additional data values.
Computation of smoothed cross and auto spectra from modified data
The determination of these spectra is necessarily performed using the same computational parameters. Consideration must be given to the form of smoothing window utilized. For this study the Parzen window was chosen. In addition the
ACTH and cortisol secretion after cranial irradiation 305
window cut-off lag is important. Once again the cut-off lag is best determined by inspecting results produced by varying the window size. In this case a lag of40 was chosen, where the maximum window available was 72.
Computation of coherency spectrum and confidence limits
Estimates of the squared coherency have values between 0 and 1 . In the NAG implementation, the hypothesis that the cortisol and ACTH assays are unrelated, at any frequency w, may be rejected at the 5% level if the squared coherency is greater than a returned level of coherency. For a cut-off lag of 40 this is 0.7. Confidence limits can be generated across the entire coherency spectrum; however, these limits strictly apply only where a coherency peak has already been established as significant.