Embed Size (px)
DESCRIPTION
Adeno Plus Testing System
Citation preview

7/15/2019 AdenoPlus Brochure US-1
http://slidepdf.com/reader/full/adenoplus-brochure-us-1 1/5RAPID RESULTS FOR A CONFIDENT DIAGNOSIS
New AdenoPlus™ aids in the
rapid dierential diagnosisof acute conjunctivitis, allowingfor appropriate managementbased on diagnostic evidence
DECODE THE RED EYE

7/15/2019 AdenoPlus Brochure US-1
http://slidepdf.com/reader/full/adenoplus-brochure-us-1 2/5
Overlap in clinical signs and symptoms of acute conjunctivitis5,9,10
Viral, bacterial, or allergic—the signs and symptomso acute conjunctivitis can be indistinguishable
• It has been estimated that at least 6 million cases o acute conjunctivitis are diagnosedin the U.S. each year1
• Viral, bacterial, and allergic are the most common types and present similarly2-4
• Diferential diagnosis using only signs and symptoms can be challenging5-8
“Treatment of conjunctivitis is ideally directed at the root cause. Indiscriminate use
of topical antibiotics or corticosteroids should be avoided, because antibiotics can induce toxicity and corticosteroids can potentially prolong adenoviral infections…”18
— American Academy of Ophthalmology (AAO), Preferred Practice Pattern®
, 2011
Redness
81%
83%
38%
Itching
38%
33%
86%
Irritation/foreign
body sensation
19%
17%
52%Watery
discharge/tearing
50%
39%
48%
Follicles
47%
42%
8%
ucoid
scharge
19%
17%
18%
Purulent
discharge
25%
28%
N/A
Viral
Bacterial
Allergic
Early, accurate diagnosis o acute conjunctivitismay prevent serious consequences
• Adenovirus causes approximately 1 out o every 4 acute conjunctivitis casesseen by eye care proessionals and is ot en misdiagnosed2-5,11,12
• Adenovirus is associated with signicant morbidity, including11,13-15
— Decreased visual acuity— Light sensitivity— Chronic excessive tear production— Visual loss— Presence o subepithelial inltrates
Contagion with adenovirus is fast and widespread
• Inected patients are contagious or up to 3 weeks16
• Between close contacts the inection rate is up to 50%16
• Adenovirus can live on inanimate suraces or up to 28 days17,18
Studies indicate that eye care professionals make an accurate dierentdiagnosis for acute conjunctivitis approximately 50% of the time2-4
• The majority o acute conjunctivitis cases result in a prescription or antibiotics,even when they are unnecessary19
• Unnecessary antibiotic use may increase adverse efects and promote resistance11
“While some cases of acute conjunctivitis are more obviously associated
with one etiology or another, the majority of cases have similar presentation, making the differential diagnosis challenging.”
— Kelly Nichols, OD, MPH, PhD, FAAO

7/15/2019 AdenoPlus Brochure US-1
http://slidepdf.com/reader/full/adenoplus-brochure-us-1 3/5
RAPID RESULTS FOR A CONFIDENT DIAGDECODE THE RED EYE
Introducing AdenoPlus™—the rst in-oceimmunoassay that aids in the rapid diferentialdiagnosis o acute conjunctivitis
Fast
• ≤ 2 minutes to complete test; results in just 10 minutes
Accurate
• Identies adenovirus (which accounts or 90% o all viralconjunctivitis2,20,21) with 90% sensitivity and 96% specicity
Easy
• Completed in the oce in 4 simple steps
An objective diagnosis may enhance the patient experience2
• Patients know i their red eye is adenovirus beore leaving the clinician’s oce
• They know whether or not they can return to work
• They may avoid paying or unnecessary treatments such as antibiotics
“With AdenoPlus
™
, practices benefit from a laboratory-quality diagnosis at the point of care.”
— Paul Karpecki, OD, FAAO
AdenoPlus™ eatures proprietary technology utilizing direct samplemicroltration with a lateral ow assay strip, enabling a small sample
o ocular uid to aid in a rapid diferential diagnosis in the oce.
AdenoPlus™ in practice—aiding in makingan accurate diagnosis or better patient care
With AdenoPlus™, eye care proessionals can:
• Quickly obtain accurate evidence or a diferential diagnosis22
• Comply with AAO guidelines by counseling contagious patients to minimizeor prevent spread o the disease in the community18
• Signicantly reduce cost to the U.S. healthcare system12
— A published cost-efectiveness study ound that incorporating AdenoPlus™ as aroutine, point-o-care test or the red eye could save more than $400 million annually
• More efectively and eciently manage their patients with red eye2,11,22
Providing accurate results in 4 simple steps
1. Use a “dab and drag”motion in 6 to 8 locationson the palpebralconjunctiva (lower eyelid)to collect a tear sample.
2. Snap the sample collectorinto the test cassette andpress rmly where indicated.
3. Dip the test cassetteinto the provided bufervial or 20 seconds.Replace the cap.
4. Read the results: 2 line(1 red, 1 blue) = positiv1 line (blue) = negative
“ [AdenoPlus™
] helps reduce the number of misdiagnoses and leads to better patient management and treatment.”2
— Terrence P. O’Brien, MD
7/15/2019 AdenoPlus Brochure US-1
http://slidepdf.com/reader/full/adenoplus-brochure-us-1 4/5
RAPID RESULTS FOR A CONFIDENT DIAGDECODE THE RED EYE
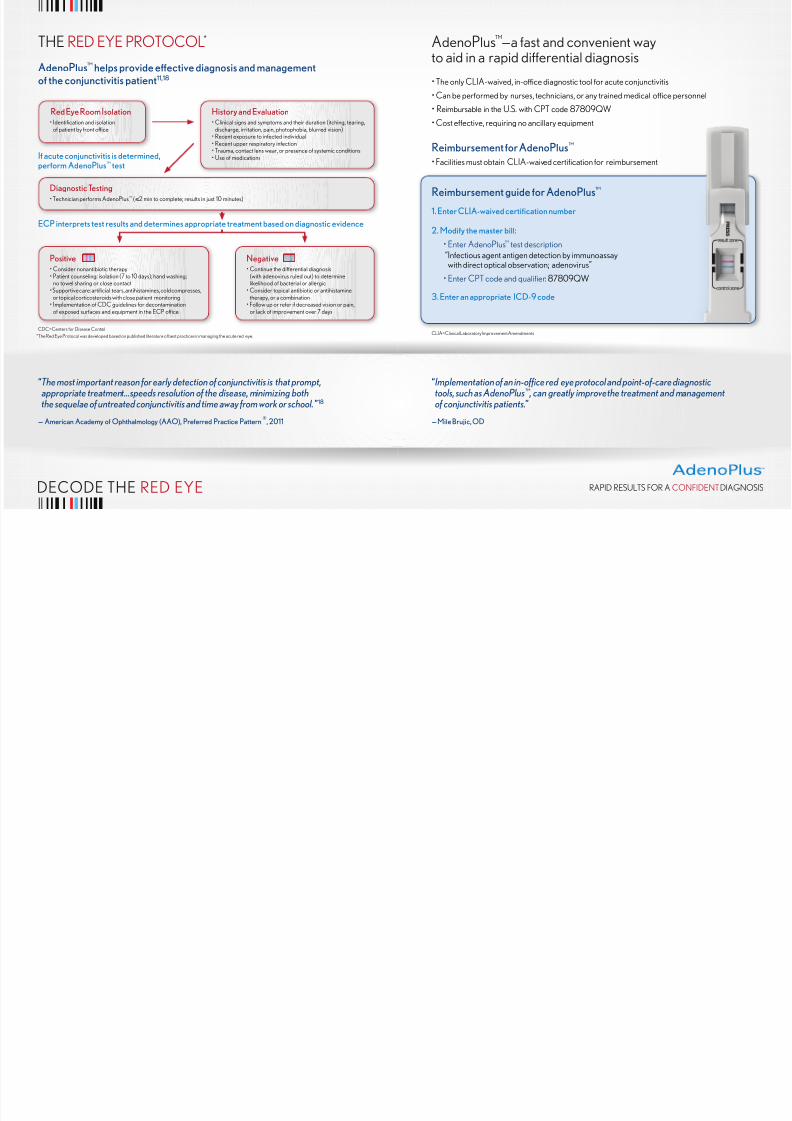
THE RED EYE PROTOCOL*
AdenoPlus™ helps provide eective diagnosis and managementof the conjunctivitis patient11,18
AdenoPlus™—a ast and convenient wayto aid in a rapid diferential diagnosis
• The only CLIA-waived, in-oce diagnostic tool or acute conjunctivitis
• Can be perormed by nurses, technicians, or any trained medical oce personnel
• Reimbursable in the U.S. with CPT code 87809QW
• Cost efective, requiring no ancillary equipment
Reimbursement for AdenoPlus™
• Facilities must obtain CLIA-waived certication or reimbursement
“The most important reason for early detection of conjunctivitis is that prompt,
appropriate treatment…speeds resolution of the disease, minimizing boththe sequelae of untreated conjunctivitis and time away from work or school.”18
— American Academy of Ophthalmology (AAO), Preferred Practice Pattern®
, 2011
Red Eye Room Isolation• Identication and isolation
o patient by ront oce
History and Evaluation• Clinical signs and symptoms and their duration (itching, tearing,
discharge, irritation, pain, photophobia, blurred vision)• Recent exposure to inected individual• Recent upper respiratory inection• Trauma, contact lens wear, or presence o systemic conditions• Use o medicationsIf acute conjunctivitis is determined,
perform AdenoPlus™ test
Diagnostic Testing• Technician perorms AdenoPlus™ (≤ 2 min to complete; results in just 10 minutes)
Positive• Consider nonantibiotic therapy• Patient counseling: isolation (7 to 10 days); hand washing;
no towel sharing or close contact• Supportive care: articial tears, antihistamines, cold compresses,
or topical corticosteroids with close patient monitoring• Implementation o CDC guidelines or decontamination
o exposed suraces and equipment in the ECP oce
Negative• Continue the diferential diagnosis
(with adenovirus ruled out) to determinelikelihood o bacterial or allergic
• Consider topical antibiotic or antihistaminetherapy, or a combination
• Follow up or reer i decreased vision or pain,or lack o improvement over 7 days
ECP interprets test results and determines appropriate treatment based on diagnostic evidence
“Implementation of an in-office red eye protocol and point-of-care diagnostic
tools, such as AdenoPlus™ , can greatly improve the treatment and management of conjunctivitis patients.”
— Mile Brujic, OD
CDC=Centers or Disease Control
*The Red Eye Protocol was developed based on published literature o best practices in managing the acute red eye.CLIA=Clinical Laboratory Improvement Amendments
Reimbursement guide for AdenoPlus™
1. Enter CLIA-waived certication number
2. Modify the master bill:
• Enter AdenoPlus™ test description “Inectious agent antigen detection by immunoassaywith direct optical observation; adenovirus”
• Enter CPT code and qualier: 87809QW
3. Enter an appropriate ICD-9 code

7/15/2019 AdenoPlus Brochure US-1
http://slidepdf.com/reader/full/adenoplus-brochure-us-1 5/5
Introducing AdenoPlus™—rapid resultsor a condent diagnosis
• Fast: Results in just 10 minutes
• Accurate: 90% sensitivity and 96% specicity• Easy: Complete in the oce in 4 simple steps
• RED EYE PROTOCOL: Helps provideefective diagnosis and management
References: 1. Data on fle, Nicox Ophthalmic Diagnostics. 2. O’Brien TP, Jeng BH, McDonald M, et al. Acute conjunctivitis: truth and misconceptions. Curr Med Res Opin . 2009;25(8):1953-1961.
3. Leibowitz HM, Pratt MV, Flagstad IJ, et al. Human conjunctivitis. Arch Ophthalmol . 1976;94:1747-1749. 4. Stenson S, Newman R, Fedukowicz H. Laboratory studies in acute conjunctivitis. Arch
Ophthalmol . 1982;100:1275-1277. 5. Fitch CP, Rapoza PA, Owens S, et al. Epidemiology and diagnosis o acute conjunctivitis at an inner-city hospital. Ophthalmology . 1989;96:1215-1220.
6. Rietveld RP, ter Riet G, Bindels PJE, et al. Predicting bacterial cause in inectious conjunctivitis: cohort study on inormativeness o combinations o signs and symptoms. BMJ . 2004;329:206.
7. Rietveld RP, vanWeert CPM, ter Riet G, et al. Diagnostic impact o signs and symptoms in acute inectious conjunctivitis: systematic literature search. BMJ . 2003;327:789. 8. Gigliotti F, Williams
WT, Hayden FG, et al. Etiology o acute conjunctivitis in children. J Pediatrics . 1981;98(4):531-536. 9. Solomon AS. Symptoms o allergic conjunctivitis. Arch Ophthalmol. 1985;103(7):891.
10. Kosrirukvongs P, Visitsunthorn N, Vichyanond P, et al. Allergic conjunctivitis. Asian Pac J Allergy . 2001;19:237-244. 11. Sambursky R, Tauber S, Schirra F, et al. The RPS Adeno Detector
or diagnosing adenoviral conjunctivitis. Ophthalmology . 2006;113:1758-1764. 12. Udeh BL, Schneider JE, Ohseldt RL. Cost eectiveness o a point-o-care test or adenoviral conjunctivitis.
Am J Med Sci . 2008;336(3):254-264. 13. Butt AL, Chodosh J. Adenoviral keratoconjunctivitis in a tertiary care eye clinic. Cornea . 2006;25(2):199-202. 14. Hyde KJ, Berger ST. Epidemic
keratoconjunctivitis and lacrimal excretory system obstruction. Ophthalmology . 1988;95(10):1447-1449. 15. Hammer LH, Perry HD, Donneneld ED, et al. Symblepharon ormation in epidemic
keratoconjunctivitis. Cornea . 1990;9(4):338-340. 16. Kauman HE. Adenovirus advances: new diagnostic and therapeutic options. Curr Opin Ophthalmol . 2011;22:290-293. 17. Gordon YJ,
Gordon RY, Romanowski E, et al. Prolonged recovery o desiccated adenoviral serotypes 5, 8, and 19 rom plastic and metal suraces in vitro. Ophthalmology . 1993;100(12):1835-1840.
18. American Academy o Ophthalmology Cornea/External Disease Panel. Preerred Practice Patt ern®
Guidelines. Conjunctivitis–Limited Revision. San Francisco, CA: American Academy
o Ophthalmology; 2011. Available at: www.aao.org/ppp. 19. Everitt H, Little P. How do GPs diagnose and manage acute inective conjunctivitis? A GP survey. Fam Pract . 2002;19(6):658-660.
20. Matsui K, Shimizu H, Yoshida A, et al. Monitoring o adenovirus rom conjunctival scrapings in Japan during 2005–2006. J Med Virol . 2008;80:997-1003. 21. Woodland RM, Darougar S,
Thaker U, et al. Causes o conjunctivitis and keratoconjunctivitis in Karachi, Pakistan. Royal Soc Tropical Medicine Hygiene . 1992;86(3):317-320. 22. Sambursky RP, Fram N, Cohen EJ.
The prevalence o adenoviral conjunctivitis at the Wills Eye Hospital emergency room. Optometry . 2007;78:236-239.
AdenoPlus is a trademark of Rapid Pathogen Screening, Inc.
© 2012 Nicox, Inc. All rights reserved. www.Nicox.com
RAPID RESULTS FOR A CONFIDENT DIAGNOSIS
For more inormation or to order AdenoPlus™, contact your local
Ophthalmic Account Manager or call 1.855.MY.NICOX (1.855.696.4269).