Embed Size (px)
Citation preview

Abstract:Acute injuries to the lower extremityare among the most commonaffecting young athletes and arefrequently evaluated in theemergency department. Accuratediagnosis is essential to guideappropriate management to improveoutcome, shorten time to recoveryand return to sport/activity, andprevent complications. This articlewill describe the evaluation andmanagement of acute, sports-related, lower extremity injuries,including review of frequently injuredanatomical structures, physicalexamination techniques, indicationsfor imaging, initial treatment, andguidelines for follow-up and returnto sport.
Keywords:young athlete; lower extremity;emergency department; injury
Divisions of Emergency Medicine andOrthopedics and Sports Medicine, Ann &Robert H. Lurie Children's Hospital ofChicago, Chicago, IL.Reprint requests and correspondence:Divisions of Emergency Medicine andOrthopedics and Sports Medicine, Ann &Robert H. Lurie Children's Hospital ofChicago, 225 E Chicago Ave, Box #62,Chicago, IL [email protected].
1522-8401/$ - see front matter© 2013 Elsevier Inc. All rights reserved.
304 VOL. 14, NO. 4 • ACUTE SPORTS-RELATED LOW
Acute Sports-Related Lower
ExtremityInjuries
ER EXTREMITY INJURIES / HANG
Brian Hang, MD, MS
ecause there is a push for increased youth participationin physical activity and exercise, unfortunately, there Bwill be a similar increase in injuries. Acute injuries to thelower extremity are among the most common affectingyoung athletes and are frequently evaluated in the emergencydepartment (ED). Accurate diagnosis is essential to guideappropriate management to improve outcome, shorten time torecovery and return to sport/activity, and prevent complications.In high school athletes with lower extremity injuries, the leadingdiagnosis were sprains (50%), strains (17%), contusions (12%), andfractures (5%).1 The ankle (40%) and knee (25%) were the mostcommonbodyparts injured.1 This articlewill describe the evaluationand management of acute, sports-related, lower extremity injuries,including review of frequently injured anatomical structures,physical examination techniques, indications for imaging, initialtreatment, and guidelines for follow-up and return to sport.
ANKLE
AnatomyFor purpose of evaluation, the ankle can be divided into 4
compartments: lateral, medial, posterior, and anterior. The lateralcompartment comprises the fibula/lateral malleolus, lateralligamentous complex (anterior talofibular ligament [ATFL],calcaneofibular ligament [CFL], and posterior talofibular ligament[PTFL]), and the muscle tendons of the lateral compartment ofthe leg (peroneal longus and brevis). The medial compartmentcomprises the tibia/medial malleolus, medial ligamentous com-plex (deltoid ligament), and the deep posterior muscle compart-ment of the leg (tibialis posterior, flexor digitorum longus, and

ACUTE SPORTS-RELATED LOWER EXTREMITY INJURIES / HANG • VOL. 14, NO. 4 305
flexor hallucis longus). The Achilles tendon and itsattachment to the calcaneus are the main structuresin the posterior compartment. The tendons formuscles of the anterior compartment of the leg(tibialis anterior, extensor digitorum longus, andextensor hallucis longus) are located in the anteriorcompartment of the ankle, as are the syndesmosisand talus.
Examination
Inspection and PalpationEvaluate for an effusion (Figure 1), location of any
bruising or swelling, and any deformities. Focaltenderness of any of the superficial ankle structuresand landmarks can narrow the diagnosis anddetermine whether radiographs are necessary.
RadiographsThe Ottawa Ankle Rules2 may be used to deter-
mine if radiographs are necessary and are applicableto children older than 6 years.3 These guidelines,which are designed to rule out fractures of themalleoli and the midfoot, suggest that ankle radio-graphs (anteroposterior [AP], lateral, and mortiseviews) (Figure 2A) should be obtained if the patient has
Figure 1. Lateral ankle effusion.
• an inability to bear weight 4 steps on theinjured ankle (immediately after the injury orin the ED), or
• point tenderness over the posterior edge ofthe distal 6 cm of either malleolus, or
• point tenderness over the base of the fifthmetatarsal or navicular (including foot radio-graphs—AP, lateral, and oblique views).
If suspicious, the examiner should obtain radio-graphs to rule out fractures (Figure 2B) beforeproceeding with range of motion (ROM) and specialankle testing. The ankle has 3 articulations: thetibiotalar, subtalar, and tibiofibular joints. Anklefractures (such as plafond, triplane, Maissoneuve,talar, and calcaneal fractures–discussed below)typically require urgent orthopedic consultation orat least an orthopedist to review the radiographsbefore discharge from the ED. Avulsion fractures ofthe base of the fifth metatarsal (Figure 3) can betreated with a hard soled shoe, walker boot, orcrutches to support pain-free weight bearing.
Range of MotionComparing active ROM to the uninjured ankle is the
best way to evaluate ROM deficits. Range of motion isoften limited after acute injury and thus does notnecessarily help to narrow the diagnosis; however, full-active ROM in the acute setting suggests a less severeinjury. The normal ROM of the ankle is as follows:
Plantarflexion: 45°Dorsiflexion: 15-30°Inversion: 5°Eversion: 5°
Special TestingThe anterior drawer test (Figure 4) can determine
the degree of injury to the ATFL. It is performedwith the patient seated, knee flexed to 90°, and theankle slightly plantar flexed. The examiner stabi-lizes the distal tibia with one hand, whereas theother hand cups the heel and pulls it briskly forward,assessing the degree of laxity in comparison with theuninjured ankle.
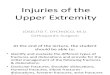
The talar tilt test (Figure 5) evaluates for laxity inthe CFL and is performed with the examiner's handsin the same position as for the anterior drawer test.The examiner briskly inverts the ankle, assessing forthe degree of laxity in comparison with the unin-jured ankle.
For either test, if there is pain but no laxitycompared with the uninjured ankle, this is indicativeof a grade 1 sprain or stretch injury to the ligament.Mild laxity, but with an end point, indicates a partial

Figure 3. Apophysis (double arrow) and avulsion fracture (singlearrow) of the base of the fifth metatarsal.
AP Mortise LateralA
B
Figure 2. A, Standard ankle radiographs. B, Fracture of distal fibula.
Figure 4. Anterior drawer test. Positive if more translation vsuninjured ankle.
306 VOL. 14, NO. 4 • ACUTE SPORTS-RELATED LOWER EXTREMITY INJURIES / HANG
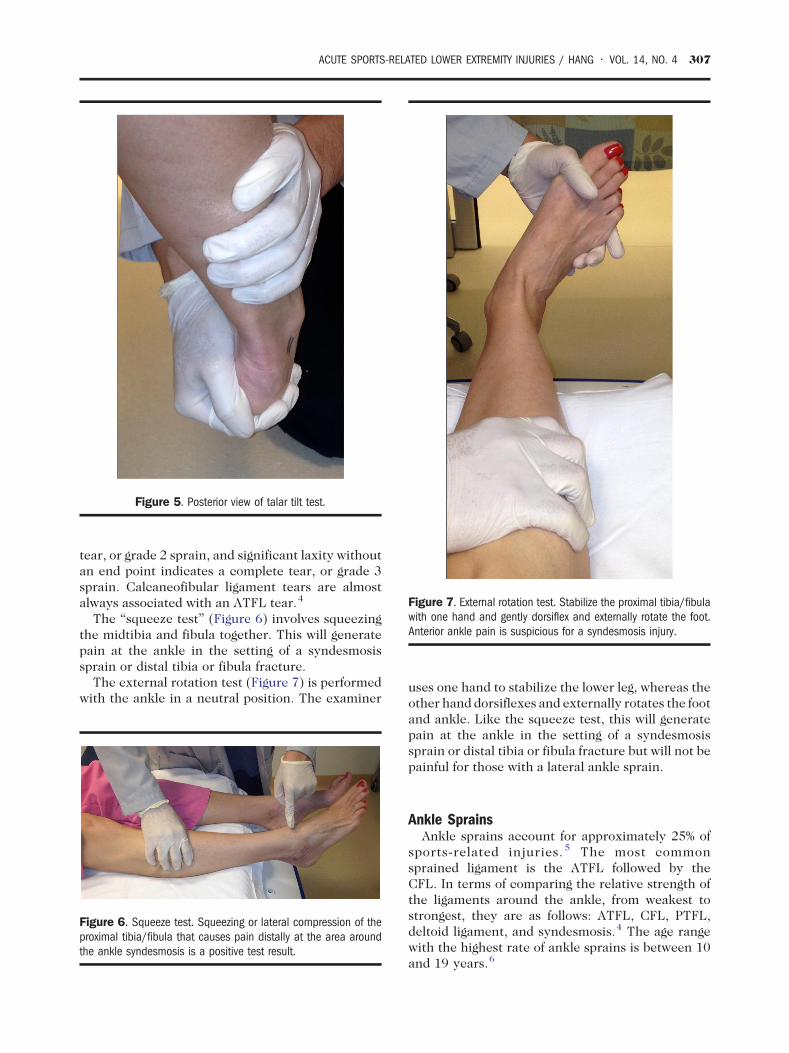
Figure 5. Posterior view of talar tilt test.
Figure 7. External rotation test. Stabilize the proximal tibia/fibulawith one hand and gently dorsiflex and externally rotate the foot.Anterior ankle pain is suspicious for a syndesmosis injury.
ACUTE SPORTS-RELATED LOWER EXTREMITY INJURIES / HANG • VOL. 14, NO. 4 307
tear, or grade 2 sprain, and significant laxity withoutan end point indicates a complete tear, or grade 3sprain. Calcaneofibular ligament tears are almostalways associated with an ATFL tear.4
The “squeeze test” (Figure 6) involves squeezingthe midtibia and fibula together. This will generatepain at the ankle in the setting of a syndesmosissprain or distal tibia or fibula fracture.
The external rotation test (Figure 7) is performedwith the ankle in a neutral position. The examiner
Figure 6. Squeeze test. Squeezing or lateral compression of theproximal tibia/fibula that causes pain distally at the area aroundthe ankle syndesmosis is a positive test result.
uses one hand to stabilize the lower leg, whereas theother hand dorsiflexes and externally rotates the footand ankle. Like the squeeze test, this will generatepain at the ankle in the setting of a syndesmosissprain or distal tibia or fibula fracture but will not bepainful for those with a lateral ankle sprain.
Ankle SprainsAnkle sprains account for approximately 25% of
sports-related injuries. 5 The most commonsprained ligament is the ATFL followed by theCFL. In terms of comparing the relative strength ofthe ligaments around the ankle, from weakest tostrongest, they are as follows: ATFL, CFL, PTFL,deltoid ligament, and syndesmosis.4 The age rangewith the highest rate of ankle sprains is between 10and 19 years.6
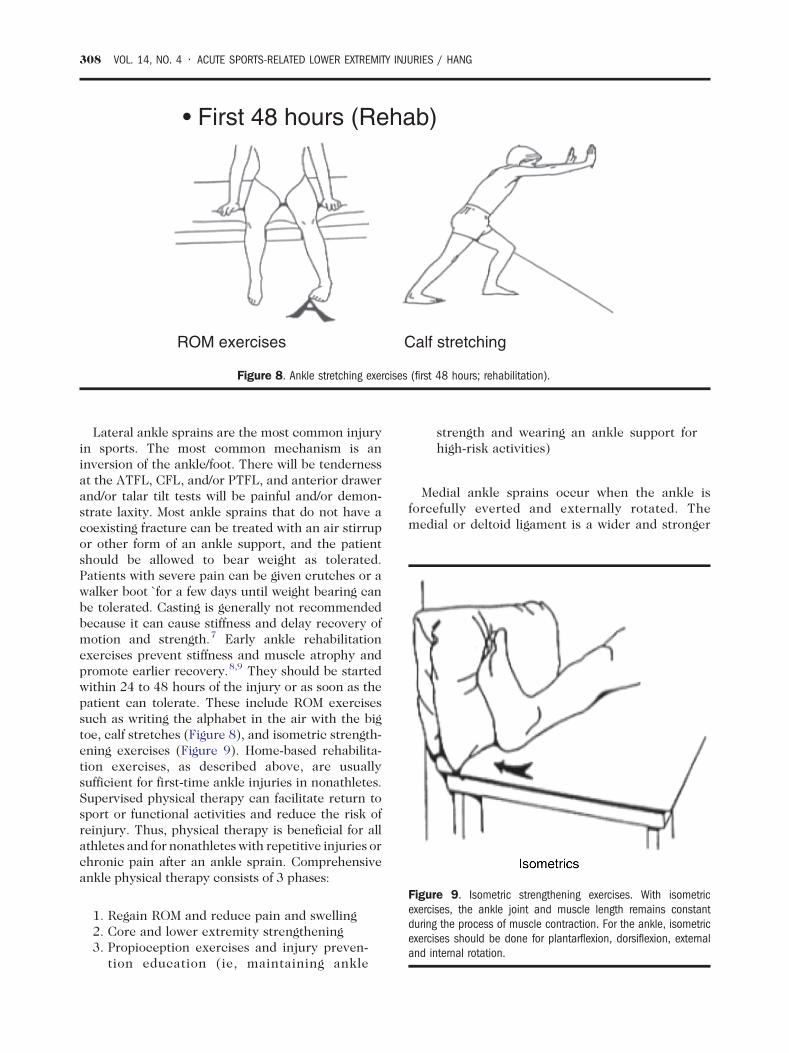
ROM exercises Calf stretching
• First 48 hours (Rehab)
Figure 8. Ankle stretching exercises (first 48 hours; rehabilitation).
Figure 9. Isometric strengthening exercises. With isometricexercises, the ankle joint and muscle length remains constantduring the process of muscle contraction. For the ankle, isometricexercises should be done for plantarflexion, dorsiflexion, externaland internal rotation.
308 VOL. 14, NO. 4 • ACUTE SPORTS-RELATED LOWER EXTREMITY INJURIES / HANG
Lateral ankle sprains are the most common injuryin sports. The most common mechanism is aninversion of the ankle/foot. There will be tendernessat the ATFL, CFL, and/or PTFL, and anterior drawerand/or talar tilt tests will be painful and/or demon-strate laxity. Most ankle sprains that do not have acoexisting fracture can be treated with an air stirrupor other form of an ankle support, and the patientshould be allowed to bear weight as tolerated.Patients with severe pain can be given crutches or awalker boot `for a few days until weight bearing canbe tolerated. Casting is generally not recommendedbecause it can cause stiffness and delay recovery ofmotion and strength.7 Early ankle rehabilitationexercises prevent stiffness and muscle atrophy andpromote earlier recovery.8,9 They should be startedwithin 24 to 48 hours of the injury or as soon as thepatient can tolerate. These include ROM exercisessuch as writing the alphabet in the air with the bigtoe, calf stretches (Figure 8), and isometric strength-ening exercises (Figure 9). Home-based rehabilita-tion exercises, as described above, are usuallysufficient for first-time ankle injuries in nonathletes.Supervised physical therapy can facilitate return tosport or functional activities and reduce the risk ofreinjury. Thus, physical therapy is beneficial for allathletes and for nonathletes with repetitive injuries orchronic pain after an ankle sprain. Comprehensiveankle physical therapy consists of 3 phases:
1. Regain ROM and reduce pain and swelling2. Core and lower extremity strengthening3. Propioception exercises and injury preven-
tion education (ie, maintaining ankle
strength and wearing an ankle support forhigh-risk activities)
Medial ankle sprains occur when the ankle isforcefully everted and externally rotated. Themedial or deltoid ligament is a wider and stronger
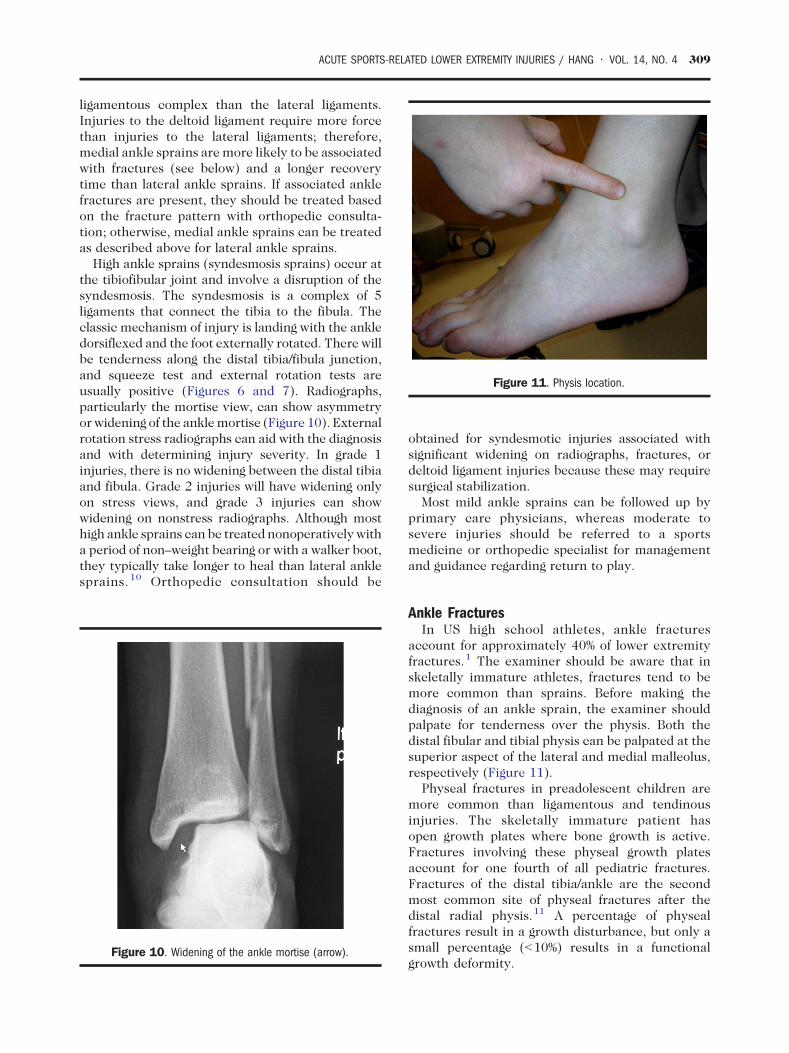
Figure 11. Physis location.
ACUTE SPORTS-RELATED LOWER EXTREMITY INJURIES / HANG • VOL. 14, NO. 4 309
ligamentous complex than the lateral ligaments.Injuries to the deltoid ligament require more forcethan injuries to the lateral ligaments; therefore,medial ankle sprains are more likely to be associatedwith fractures (see below) and a longer recoverytime than lateral ankle sprains. If associated anklefractures are present, they should be treated basedon the fracture pattern with orthopedic consulta-tion; otherwise, medial ankle sprains can be treatedas described above for lateral ankle sprains.
High ankle sprains (syndesmosis sprains) occur atthe tibiofibular joint and involve a disruption of thesyndesmosis. The syndesmosis is a complex of 5ligaments that connect the tibia to the fibula. Theclassic mechanism of injury is landing with the ankledorsiflexed and the foot externally rotated. There willbe tenderness along the distal tibia/fibula junction,and squeeze test and external rotation tests areusually positive (Figures 6 and 7). Radiographs,particularly the mortise view, can show asymmetryor widening of the anklemortise (Figure 10). Externalrotation stress radiographs can aid with the diagnosisand with determining injury severity. In grade 1injuries, there is no widening between the distal tibiaand fibula. Grade 2 injuries will have widening onlyon stress views, and grade 3 injuries can showwidening on nonstress radiographs. Although mosthigh ankle sprains can be treated nonoperatively witha period of non–weight bearing or with a walker boot,they typically take longer to heal than lateral anklesprains. 10 Orthopedic consultation should be
Figure 10. Widening of the ankle mortise (arrow).
obtained for syndesmotic injuries associated withsignificant widening on radiographs, fractures, ordeltoid ligament injuries because these may requiresurgical stabilization.
Most mild ankle sprains can be followed up byprimary care physicians, whereas moderate tosevere injuries should be referred to a sportsmedicine or orthopedic specialist for managementand guidance regarding return to play.
Ankle FracturesIn US high school athletes, ankle fractures
account for approximately 40% of lower extremityfractures.1 The examiner should be aware that inskeletally immature athletes, fractures tend to bemore common than sprains. Before making thediagnosis of an ankle sprain, the examiner shouldpalpate for tenderness over the physis. Both thedistal fibular and tibial physis can be palpated at thesuperior aspect of the lateral and medial malleolus,respectively (Figure 11).
Physeal fractures in preadolescent children aremore common than ligamentous and tendinousinjuries. The skeletally immature patient hasopen growth plates where bone growth is active.Fractures involving these physeal growth platesaccount for one fourth of all pediatric fractures.Fractures of the distal tibia/ankle are the secondmost common site of physeal fractures after thedistal radial physis.11 A percentage of physealfractures result in a growth disturbance, but only asmall percentage (b10%) results in a functionalgrowth deformity.
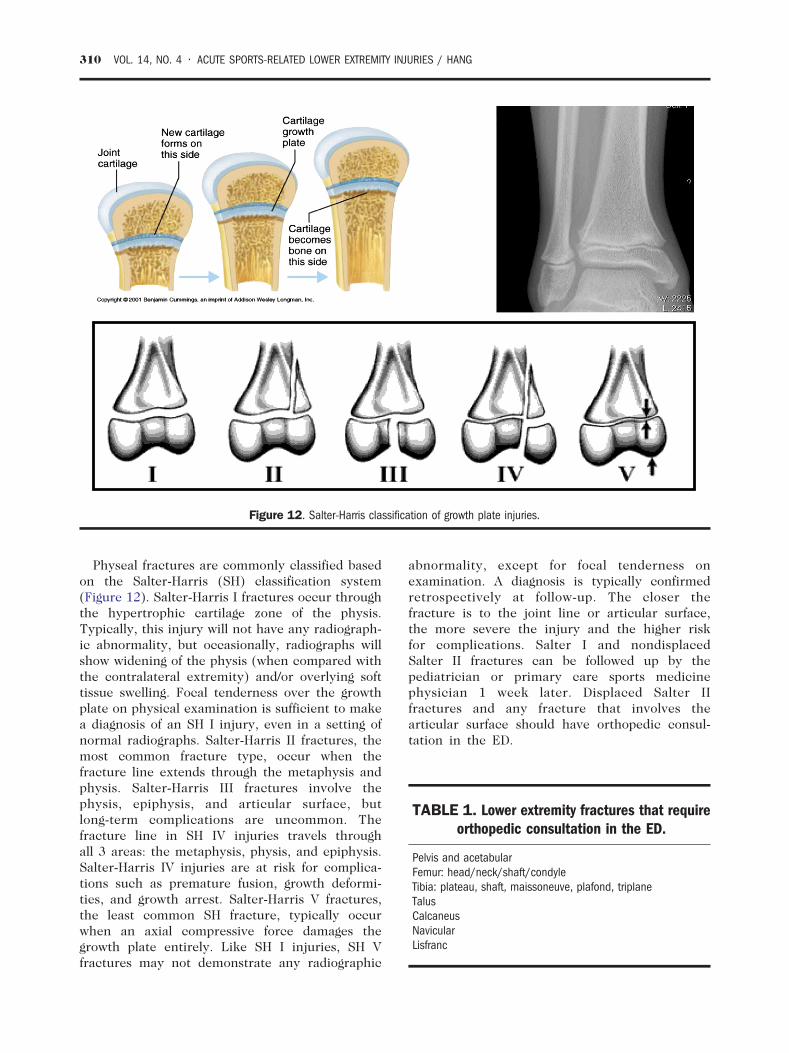
TABLE 1. Lower extremity fractures that requireorthopedic consultation in the ED.
Pelvis and acetabularFemur: head/neck/shaft/condyleTibia: plateau, shaft, maissoneuve, plafond, triplaneTalusCalcaneusNavicularLisfranc
Figure 12. Salter-Harris classification of growth plate injuries.
310 VOL. 14, NO. 4 • ACUTE SPORTS-RELATED LOWER EXTREMITY INJURIES / HANG
Physeal fractures are commonly classified basedon the Salter-Harris (SH) classification system(Figure 12). Salter-Harris I fractures occur throughthe hypertrophic cartilage zone of the physis.Typically, this injury will not have any radiograph-ic abnormality, but occasionally, radiographs willshow widening of the physis (when compared withthe contralateral extremity) and/or overlying softtissue swelling. Focal tenderness over the growthplate on physical examination is sufficient to makea diagnosis of an SH I injury, even in a setting ofnormal radiographs. Salter-Harris II fractures, themost common fracture type, occur when thefracture line extends through the metaphysis andphysis. Salter-Harris III fractures involve thephysis, epiphysis, and articular surface, butlong-term complications are uncommon. Thefracture line in SH IV injuries travels throughall 3 areas: the metaphysis, physis, and epiphysis.Salter-Harris IV injuries are at risk for complica-tions such as premature fusion, growth deformi-ties, and growth arrest. Salter-Harris V fractures,the least common SH fracture, typically occurwhen an axial compressive force damages thegrowth plate entirely. Like SH I injuries, SH Vfractures may not demonstrate any radiographic
abnormality, except for focal tenderness onexamination. A diagnosis is typically confirmedretrospectively at follow-up. The closer thefracture is to the joint line or articular surface,the more severe the injury and the higher riskfor complications. Salter I and nondisplacedSalter II fractures can be followed up by thepediatrician or primary care sports medicinephysician 1 week later. Displaced Salter IIfractures and any fracture that involves thearticular surface should have orthopedic consul-tation in the ED.

Left knee effusion
Figure 13. Knee effusion.
Figure 14. Palpating collateral knee ligaments, patient in figurefour position.
ACUTE SPORTS-RELATED LOWER EXTREMITY INJURIES / HANG • VOL. 14, NO. 4 311
Although open physes are weaker than surround-ing structures and are more prone to injury, there isgreater remodeling potential at the physes due torapid growth and cellular changes. As a result,physeal injuries, if properly identified and treated,often heal uneventfully.
The ankle fractures that follow (Table 1) shouldbe managed with orthopedic consultation in EDbecause of inherent instability or significant artic-ular surface involvement and high likelihood ofrequiring surgery.
Plafond/Pilon fracture: a comminuted fracture ofthe distal tibia just above the ankle (tibiotalar) joint,involving the articular cartilage of the ankle joint.These result from high-energy vertical axial loading(eg, fall from a significant height) and thus are oftenassociated with distal fibula fractures and significantsoft tissue injuries.
Triplane fracture: a fracture of the distal tibia ina skeletally immature adolescent patient. Thename, triplane, describes the multiplanar fracturepattern. A triplane fracture extends in thetransverse plane through the physis, in the sagittalplane through the epiphysis, and in the coronalplane through the metaphysis. Triplane fracturesappear as an SH type III on AP radiographs andSH type II on a lateral radiographs. Computedtomography is helpful in assessing the degree ofarticular involvement.
Maissoneuve fracture: a rotational injury can occurthrough the ankle where the traumatic force istransmitted from the medial ankle, causing a medialmalleolar fracture or deltoid ligament injury (seeabove), through the syndesmosis and interosseousmembrane and proximally to the fibula causing aproximal fibular fracture. Thus, the proximal fibulashould be palpated in all patients with medial anklefractures or sprains.
KNEE/TIBIA
AnatomyThe knee can be divided into 4 compartments:
medial, lateral, anterior, and posterior. Themedial compartment comprises the medial menis-cus, medial collateral ligament (MCL), and pesanserinus (attachment of the sartorius, gracilus,and semitendinosus muscles). The lateral com-partment comprises the lateral meniscus andlateral collateral ligament (LCL). The anteriorknee comprises the tibial tuberosity, patella, andpatella tendon. The posterior knee includes theneurovascular bundle, and the hamstring andgastrocnemius tendons. When there is intra-
articular swelling, it may be evident in theposterior compartment as a popliteal cyst orBaker cyst. The anterior and posterior cruciateligaments (ACL and PCL, respectively) are deeperstructures within the knee that cannot be placedinto 1 of these 4 compartments.
Examination
Inspection/PalpationInspect for an effusion (Figure 13) and any
deformities. Location of any tenderness guides the

312 VOL. 14, NO. 4 • ACUTE SPORTS-RELATED LOWER EXTREMITY INJURIES / HANG
diagnosis. It may be helpful to place the patient in afigure 4 position (Figure 14) to palpate the jointlines, MCL, and LCL.
RadiographsRadiographs should be obtained to rule out
fractures before proceeding with ROM and ligamen-tous testing, particularly in skeletally immaturepatients. Similar to the Ottawa Ankle Rules, theOttawa Knee Rules have also been validated inchildren (ages 2-16 years).12 Per the Ottawa criteria,indications to obtain radiographs of the knee include:
• an inability to bear weight 4 steps on theinjured extremity (immediately after theinjury or in the ED), or
• point tenderness over the head of the fibula,or
• point tenderness over the patella, or• inability to flex the knee to 900.
Distal femur, patella, and tibial plateau fracturesrequire immediate orthopedic consultation. Avulsionfractures of the tibial spine are important to identifybecause they often present with signs and symptomssimilar to ACL sprains, but treatment is distinctlydifferent (see below). A Segond fracture (avulsionfracture of the joint capsule from the lateral tibialcondyle of the knee) is pathognomic for anACL injury.
Range of MotionRange of motion is best evaluated by comparing
with the uninjured knee. Range of motion may belimited because of pain, effusion, and/or fracture orloose body. Typical knee ROM is from 0° (extension)to 140° (flexion).
Figure 15. Lac
Special Knee Testing—ACL InjuryThe Lachman test (Figure 15) is the most sensitive
test (87-98%) for evaluating ACL injury.13 With thepatient supine, the knee is slightly flexed to 15° to 30°to relax the hamstrings. The examiner places onehand firmly around the distal thigh to stabilize it,while the other hand grasps the proximal tibia anduses a brisk motion to pull it anteriorly, assessing foramount of translation and presence of an endpoint compared with the uninjured knee. It is usefulto examine the uninjured knee first. Laxity is gradedas 1+ for 0 to 5 mm of displacement, 2+ for 5 to10 mm of displacement, and 3+ for greater than10 mm displacment.
The anterior drawer test (Figure 16) also evalu-ates for ACL injury but is not as sensitive andspecific as the Lachman. With the patient supineand the knee at 90° of flexion and hip at 45° offlexion, the examiner can partially sit on the top ofpatient's foot to provide stability and countertrac-tion. The examiner then places both hands aroundthe proximal tibia with the thumbs at the tibialplateau and pulls it anteriorly, evaluating foramount of translation of the tibia in relation to thefemur compared with the uninjured knee. Laxity isgraded as above.
The most reliable factor in the patient history thatis suggestive of an ACL tear is a report of an audiblepop, reported in approximately 40% of cases.14
Unlike ankle injuries, sex plays a significant factorbecause the incidence of ACL tears occur muchhigher in female than in male athletes.15,16
Special Knee Testing—PCL InjuryThe posterior drawer test evaluates the integrity
of the PCL. Positioning of the patient is the same as
hman test.

Figure 16. Position for anterior and posterior drawer test.
ACUTE SPORTS-RELATED LOWER EXTREMITY INJURIES / HANG • VOL. 14, NO. 4 313
for the anterior drawer test (Figure 16), except thatthe examiner applies a posterior force to theproximal tibia, assessing the degree of posteriortranslation of the tibia in relation to the femurcompared with the uninjured knee. The sensitivityand specificity of the posterior drawer test areapproximately 90% and 99%, respectively.17
The sag test may also be used to evaluate the PCL.The patient is placed in a supine position, and thehips are flexed to 45° and knees at near 90°, with thepatient's foot held by the examiner's hand andthe patien'ts leg is gently lifted up towards theceiling. The examiner observes for posterior dis-placement, or sag, of the tibia in relation to the femurcompared with the uninjured knee (Figure 17).
The quadriceps extension test may also be used toevaluate the PCL. The patient's position is the same asfor theanterior andposterior drawer tests. Thepatient
Figure 17.
is asked to extend theknee. In thePCL-deficient knee,the tibial tuberosity will rise from a sagged position.
Special Tests for Meniscus InjuryApproximately one third of meniscal injuries are
associated with ACL injuries.18 Reported symptomssuch as popping, catching, locking, buckling, and/orjoint line tenderness are suggestive of meniscalinjuries. Joint line tenderness itself is 74% sensitiveand has a 50% positive predictive value.19
McMurray test: with the patient supine, theexaminer places his/her palm over the patella withthe thumb and index or middle finger over each jointline while the other hand cups the heel. Theexaminer then flexes the knee while rotating thetibia (Figure 18). The sensitivity and specificity ofthis test are 100% and 15%, respectively.19 Painfulpopping over the joint line suggests a meniscal injury.
Sag test.
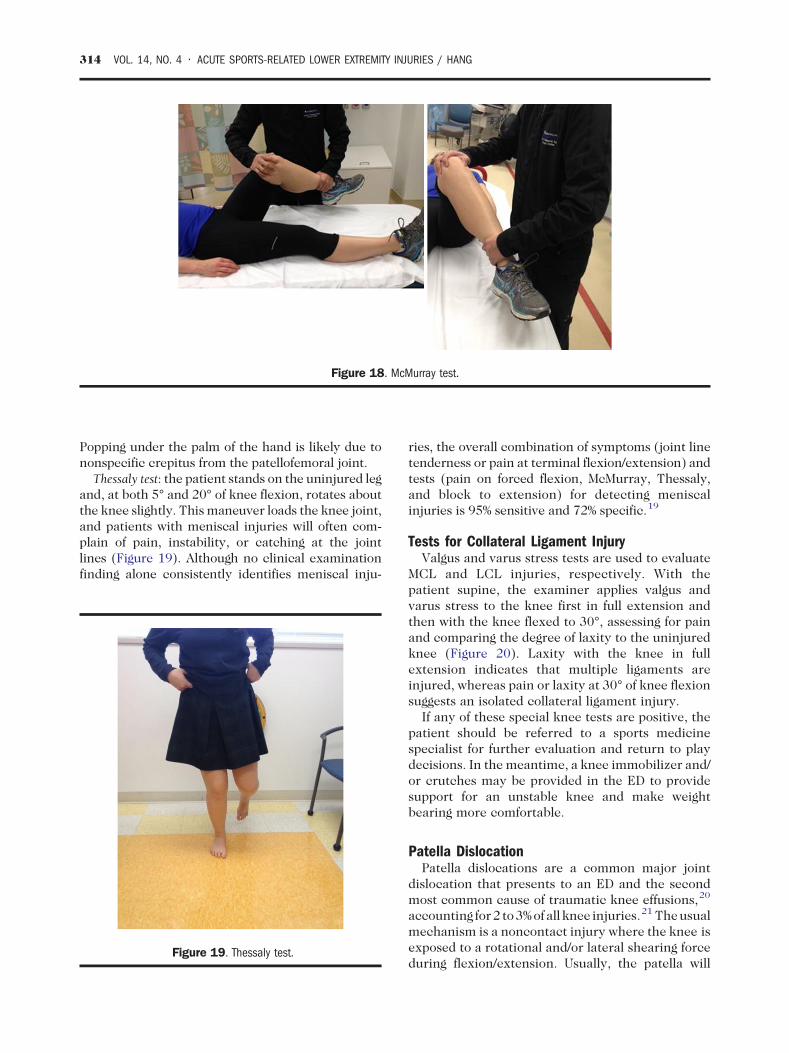
Figure 18. McMurray test.
314 VOL. 14, NO. 4 • ACUTE SPORTS-RELATED LOWER EXTREMITY INJURIES / HANG
Popping under the palm of the hand is likely due tononspecific crepitus from the patellofemoral joint.
Thessaly test: the patient stands on the uninjured legand, at both 5° and 20° of knee flexion, rotates aboutthe knee slightly. This maneuver loads the knee joint,and patients with meniscal injuries will often com-plain of pain, instability, or catching at the jointlines (Figure 19). Although no clinical examinationfinding alone consistently identifies meniscal inju-
Figure 19. Thessaly test.
ries, the overall combination of symptoms (joint linetenderness or pain at terminal flexion/extension) andtests (pain on forced flexion, McMurray, Thessaly,and block to extension) for detecting meniscalinjuries is 95% sensitive and 72% specific.19
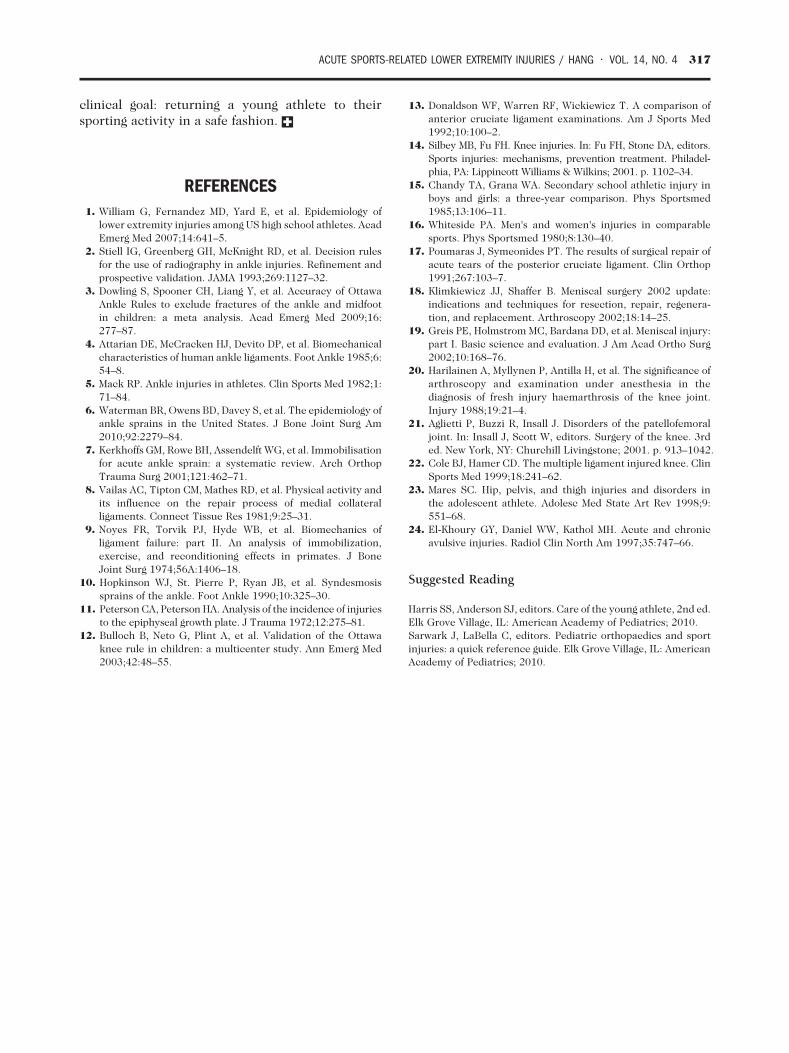
Tests for Collateral Ligament InjuryValgus and varus stress tests are used to evaluate
MCL and LCL injuries, respectively. With thepatient supine, the examiner applies valgus andvarus stress to the knee first in full extension andthen with the knee flexed to 30°, assessing for painand comparing the degree of laxity to the uninjuredknee (Figure 20). Laxity with the knee in fullextension indicates that multiple ligaments areinjured, whereas pain or laxity at 30° of knee flexionsuggests an isolated collateral ligament injury.
If any of these special knee tests are positive, thepatient should be referred to a sports medicinespecialist for further evaluation and return to playdecisions. In the meantime, a knee immobilizer and/or crutches may be provided in the ED to providesupport for an unstable knee and make weightbearing more comfortable.
Patella DislocationPatella dislocations are a common major joint
dislocation that presents to an ED and the secondmost common cause of traumatic knee effusions,20
accounting for2 to3%of all knee injuries.21 Theusualmechanism is a noncontact injury where the knee isexposed to a rotational and/or lateral shearing forceduring flexion/extension. Usually, the patella will
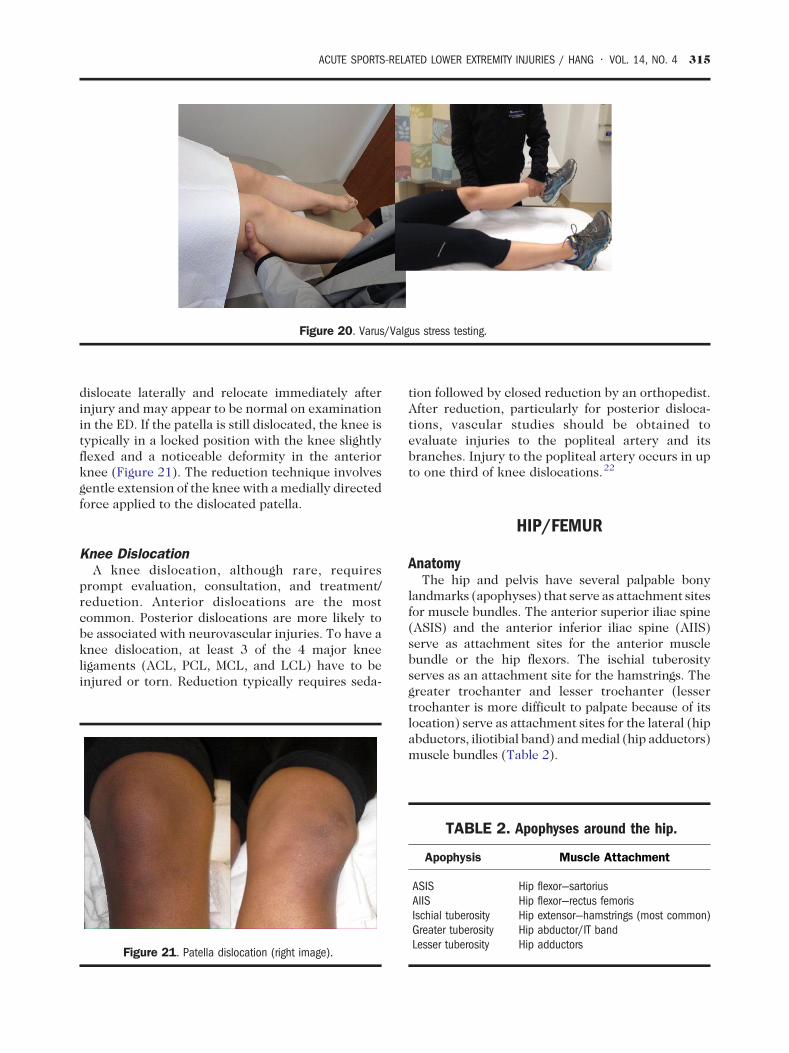
Figure 20. Varus/Valgus stress testing.
ACUTE SPORTS-RELATED LOWER EXTREMITY INJURIES / HANG • VOL. 14, NO. 4 315
dislocate laterally and relocate immediately afterinjury and may appear to be normal on examinationin the ED. If the patella is still dislocated, the knee istypically in a locked position with the knee slightlyflexed and a noticeable deformity in the anteriorknee (Figure 21). The reduction technique involvesgentle extension of the knee with amedially directedforce applied to the dislocated patella.
Knee DislocationA knee dislocation, although rare, requires
prompt evaluation, consultation, and treatment/reduction. Anterior dislocations are the mostcommon. Posterior dislocations are more likely tobe associated with neurovascular injuries. To have aknee dislocation, at least 3 of the 4 major kneeligaments (ACL, PCL, MCL, and LCL) have to beinjured or torn. Reduction typically requires seda-
Figure 21. Patella dislocation (right image).
tion followed by closed reduction by an orthopedist.After reduction, particularly for posterior disloca-tions, vascular studies should be obtained toevaluate injuries to the popliteal artery and itsbranches. Injury to the popliteal artery occurs in upto one third of knee dislocations.22
HIP/FEMUR
AnatomyThe hip and pelvis have several palpable bony
landmarks (apophyses) that serve as attachment sitesfor muscle bundles. The anterior superior iliac spine(ASIS) and the anterior inferior iliac spine (AIIS)serve as attachment sites for the anterior musclebundle or the hip flexors. The ischial tuberosityserves as an attachment site for the hamstrings. Thegreater trochanter and lesser trochanter (lessertrochanter is more difficult to palpate because of itslocation) serve as attachment sites for the lateral (hipabductors, iliotibial band) andmedial (hip adductors)muscle bundles (Table 2).
TABLE 2. Apophyses around the hip.
Apophysis Muscle Attachment
ASIS Hip flexor—sartoriusAIIS Hip flexor—rectus femorisIschial tuberosity Hip extensor—hamstrings (most common)Greater tuberosity Hip abductor/IT bandLesser tuberosity Hip adductors

316 VOL. 14, NO. 4 • ACUTE SPORTS-RELATED LOWER EXTREMITY INJURIES / HANG
Examination
Inspection/PalpationIt can be difficult to inspect for asymmetry around
the hip and pelvis, especially if the patient is not ableto bear weight. Bony landmarks should be palpatedfor tenderness, especially the apophyses (Table 2).Pelvic stability is assessed with gentle anterior-posterior and lateral pelvic compression, noting ifthis elicits any pain or movement.
RadiographsIf a patient has focal tenderness at one of the
apophyses after an acute injury or a strong muscularcontraction (such as kicking a ball or sprinting fromstarting blocks) followed by severe pain or a poppingsensation, one should be suspicious of an apophy-seal avulsion fracture, and standard radiographs ofthe hip and pelvis should be obtained. Otherfindings suspicious for a pelvic or femur fracturethat warrant radiographs are as follows: a painful legwith an obvious deformity, the affected leg appear-ing shortened and or internally or externally rotatedcompared with the contralateral leg, or pain with afulcrum test (the examiner places a finger from eachhand under the middle of the femur and gently liftsthe thigh). Treatment of pelvic and femur fracturesvaries by age from spica casting for femoral shaftfractures in smaller children to surgical fixation forpelvic and femoral shaft fractures to resting for mostavulsion fractures.
Range of MotionAfter fractures have been ruled out with radio-
graphs, the examiner can continue with ROMtesting. For the hip, the reference range is as follows:
Internal rotation
30-45° External rotation 45-60° Flexion 120-135° Extension 15-30° Abduction 45-60° Adduction 15-30°Motor Function TestingFor motor strength testing, the examiner can test
the specific muscle bundles for the 4 compart-ments (anterior, medial, lateral, and posterior) ofthe hip joint.
Hip flexors (anterior): patient is seated or supine,and strength can be tested with leg raise off the tableagainst resistance.
Adductors (medial): patient is seated or lying onthe side, and strength can be tested with the
patient pushing legs together toward the midlineagainst resistance.
Abductors (lateral): patient is seated or lying on theside, and strength can be tested with the patientpushing the legs away from midline.
External rotators (lateral): patient is lying on theside, with the lower leg straight and the upper leg thatis being tested is in a position with the knee bent.Strength is tested with resisted external rotation.
Hamstrings (posterior): patient is lying prone, andstrength can be tested with the patient raising theirleg off table against resistance.
Pelvic Avulsion FracturesAvulsion fractures typically occur in skeletally
immature athletes. Mechanism of injury typicallyincludes a sudden forceful contraction of the musclegroup, such as taking off from the starting blocks forsprinters or getting ready to kick a ball for soccerplayers. Patients will report feeling a painful pop andmay have difficulty bearing weight. There istenderness at the affected apophysis and pain withresisted motor testing of the attached muscle group.An anteroposterior radiograph of the pelvis willidentify most apophyseal avulsions. The mostcommon sites are the ASIS, AIIS, and ischialtuberosity. Management plans for these injuriesvary by type of avulsion fracture, displacement offragment, and age of patient. Treatment optionsrange from rest and/or immobilization to surgicalfixation for significantly displaced fragments. Al-though there is no consensus on what is considered“wide” displacement of fragments, athletes canexpect symptom resolution within 2 months ofinjury. Athletes experiencing symptoms after2 months may also be considered for surgicalfixation.23,24
SUMMARYThis article has covered the most common lower
extremity injuries that occur in young athletes thatare likely to present to an ED. Detailed knowledge ofthe anatomy in the lower extremity will help inmaking an accurate diagnosis. Proper technique anduse of lower extremity special examinations will aidin diagnosis. If there is a concern for fracture,radiographs should be obtained before full-ROMtesting of an injured extremity. It is generally safe toimmobilize injured extremities and limit weightbearing until subspecialty evaluation can beobtained, ideally within the week. Timely andcorrect diagnosis will help achieve the ultimate
ACUTE SPORTS-RELATED LOWER EXTREMITY INJURIES / HANG • VOL. 14, NO. 4 317
clinical goal: returning a young athlete to theirsporting activity in a safe fashion.
REFERENCES1. William G, Fernandez MD, Yard E, et al. Epidemiology of
lower extremity injuries among US high school athletes. AcadEmerg Med 2007;14:641–5.
2. Stiell IG, Greenberg GH, McKnight RD, et al. Decision rulesfor the use of radiography in ankle injuries. Refinement andprospective validation. JAMA 1993;269:1127–32.
3. Dowling S, Spooner CH, Liang Y, et al. Accuracy of OttawaAnkle Rules to exclude fractures of the ankle and midfootin children: a meta analysis. Acad Emerg Med 2009;16:277–87.
4. Attarian DE, McCracken HJ, Devito DP, et al. Biomechanicalcharacteristics of human ankle ligaments. Foot Ankle 1985;6:54–8.
5. Mack RP. Ankle injuries in athletes. Clin Sports Med 1982;1:71–84.
6. Waterman BR, Owens BD, Davey S, et al. The epidemiology ofankle sprains in the United States. J Bone Joint Surg Am2010;92:2279–84.
7. Kerkhoffs GM, Rowe BH, Assendelft WG, et al. Immobilisationfor acute ankle sprain: a systematic review. Arch OrthopTrauma Surg 2001;121:462–71.
8. Vailas AC, Tipton CM, Mathes RD, et al. Physical activity andits influence on the repair process of medial collateralligaments. Connect Tissue Res 1981;9:25–31.
9. Noyes FR, Torvik PJ, Hyde WB, et al. Biomechanics ofligament failure: part II. An analysis of immobilization,exercise, and reconditioning effects in primates. J BoneJoint Surg 1974;56A:1406–18.
10. Hopkinson WJ, St. Pierre P, Ryan JB, et al. Syndesmosissprains of the ankle. Foot Ankle 1990;10:325–30.
11. Peterson CA, Peterson HA. Analysis of the incidence of injuriesto the epiphyseal growth plate. J Trauma 1972;12:275–81.
12. Bulloch B, Neto G, Plint A, et al. Validation of the Ottawaknee rule in children: a multicenter study. Ann Emerg Med2003;42:48–55.
13. Donaldson WF, Warren RF, Wickiewicz T. A comparison ofanterior cruciate ligament examinations. Am J Sports Med1992;10:100–2.
14. Silbey MB, Fu FH. Knee injuries. In: Fu FH, Stone DA, editors.Sports injuries: mechanisms, prevention treatment. Philadel-phia, PA: Lippincott Williams & Wilkins; 2001. p. 1102–34.
15. Chandy TA, Grana WA. Secondary school athletic injury inboys and girls: a three-year comparison. Phys Sportsmed1985;13:106–11.
16. Whiteside PA. Men's and women's injuries in comparablesports. Phys Sportsmed 1980;8:130–40.
17. Poumaras J, Symeonides PT. The results of surgical repair ofacute tears of the posterior cruciate ligament. Clin Orthop1991;267:103–7.
18. Klimkiewicz JJ, Shaffer B. Meniscal surgery 2002 update:indications and techniques for resection, repair, regenera-tion, and replacement. Arthroscopy 2002;18:14–25.
19. Greis PE, Holmstrom MC, Bardana DD, et al. Meniscal injury:part I. Basic science and evaluation. J Am Acad Ortho Surg2002;10:168–76.
20. Harilainen A, Myllynen P, Antilla H, et al. The significance ofarthroscopy and examination under anesthesia in thediagnosis of fresh injury haemarthrosis of the knee joint.Injury 1988;19:21–4.
21. Aglietti P, Buzzi R, Insall J. Disorders of the patellofemoraljoint. In: Insall J, Scott W, editors. Surgery of the knee. 3rded. New York, NY: Churchill Livingstone; 2001. p. 913–1042.
22. Cole BJ, Hamer CD. The multiple ligament injured knee. ClinSports Med 1999;18:241–62.
23. Mares SC. Hip, pelvis, and thigh injuries and disorders inthe adolescent athlete. Adolesc Med State Art Rev 1998;9:551–68.
24. El-Khoury GY, Daniel WW, Kathol MH. Acute and chronicavulsive injuries. Radiol Clin North Am 1997;35:747–66.
Suggested Reading
Harris SS, Anderson SJ, editors. Care of the young athlete, 2nd ed.Elk Grove Village, IL: American Academy of Pediatrics; 2010.Sarwark J, LaBella C, editors. Pediatric orthopaedics and sportinjuries: a quick reference guide. Elk Grove Village, IL: AmericanAcademy of Pediatrics; 2010.