Embed Size (px)
Citation preview
Acute Myocardial
InfarctionWillis E. Godin D.O., FACC
Acute Myocardial Infarction
Definition: Decreased delivery of oxygen and nutrients to
the myocardium Myocardial tissue necrosis causing irreparable
tissue/cell death
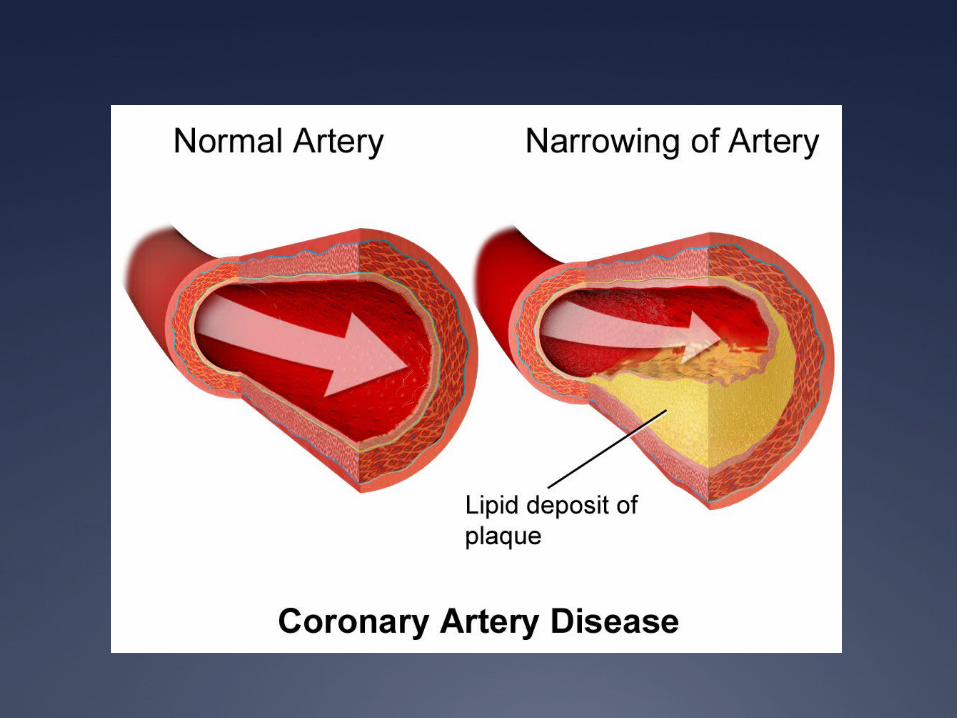
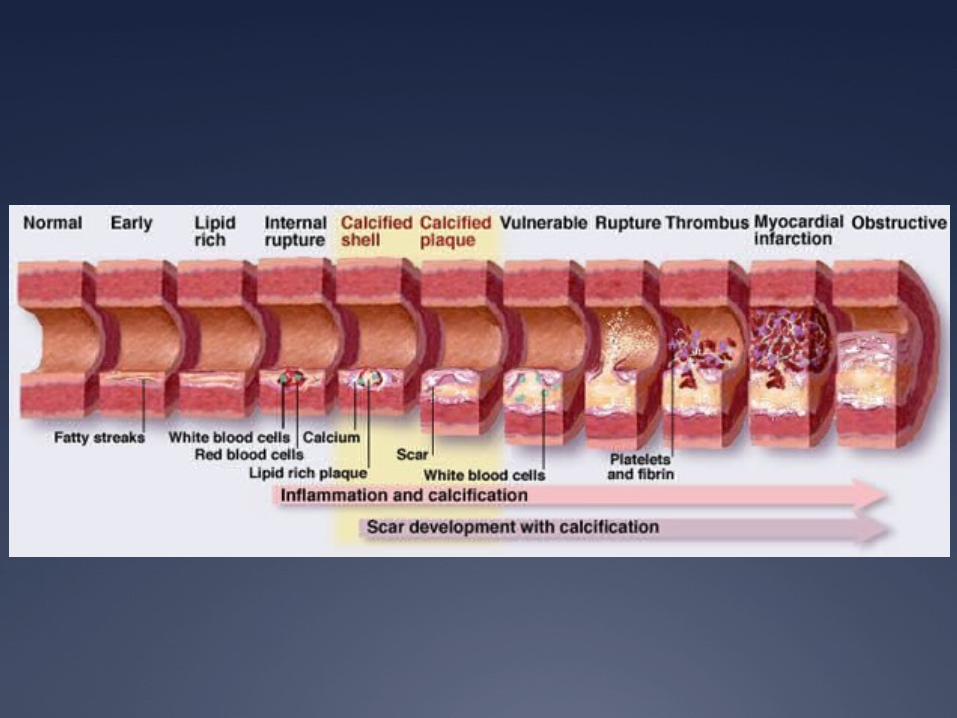
Pathophysiology
The most frequent cause of an acute MI is a disruption in the vascular endothelium that is associated with myocardial plaque
Plaque occurs over a period of years to decades
This combination causes the development of an intra-coronary thrombus, which causes the coronary artery to occlude
Within 20-40 minutes of an occlusion, irreversible myocardial cell damage/death occurs
Pathophysiology
2 primary characteristics of plaque development are 1) a fibromuscular cap and 2) an underlying lipid rich core.
The overall loss of structural stability of the plaque usually occurs at the junction between the fibromuscular cap and the vessel wall (shoulder region)
Thrombus develops (due to the platelet-mediated activation of the coagulation cascade) and partial or complete occlusion occurs causing an acute myocardial infarction.
Pathophysiology
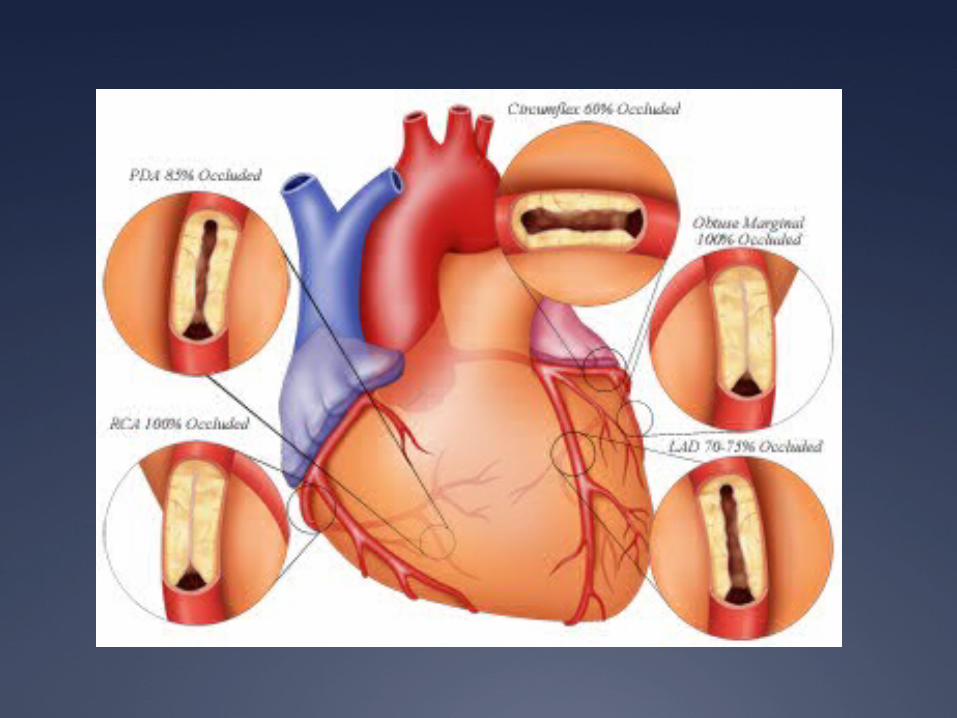
The severity of an MI depends on three factors 1) The level of the occlusion in the coronary
artery Generally, the more proximal the coronary
occlusion, the more extensive the amount of myocardium that will be at risk of necrosis
2) The length of time of the occlusion The longer the period of vessel occlusion, the
greater the chances of irreversible myocardial damage distal to the occlusion
3) The presence or absence of collateral circulation
Pathophysiology
STEMI “complete” blockage of a coronary artery
NSTEMI “near-complete” blockage of a coronary artery
Pathophysiology
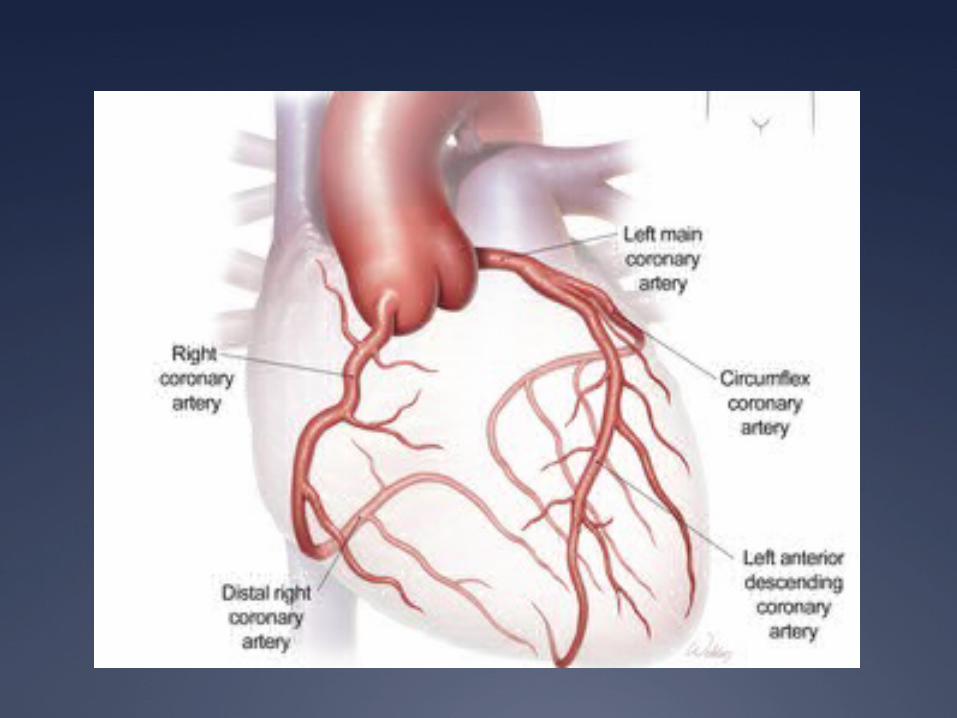
Left Coronary Artery Left Anterior Descending Artery (LAD)
“widow maker” Anterior MI Lateral MI
Left Circumflex Artery (LCx) Lateral MI Posterior MI
Right Coronary Artery Inferior MI RV MI
Prevalence
Myocardial Infarction is the leading cause of death in the United States
Approximately 450,000 people in the US die from coronary disease per year
50% of all acute MI’s in the US occur in people under the age of 65
No longer considered a “disease of the elderly”
Risk Factors
Dyslipidemia
Diabetes Mellitus
Hypertension
Tobacco use
Family History
Male gender
Diagnosis
Symptoms (gained by an accurate history)
Electrocardiogram (ECG)
Laboratory Tests CK CK-MB Troponin
Echocardiogram
Symptoms
Chest pain described as a pressure sensation, fullness, or squeezing in the midportion of the thorax
Radiation of chest pain into the jaw or teeth, shoulder, arm, and/or back
Associated dyspnea or shortness of breath
Associated epigastric discomfort with or without nausea and vomiting
Associated diaphoresis or sweating
Syncope or near syncope without other cause
Impairment of cognitive function without other cause
Electrocardiogram
ST elevation myocardial infarction (STEMI) > 1mm ST elevations in contiguous leads
Non-ST elevation myocardial infarction (NSTEMI) ST depression T wave inversions No obvious ECG changes
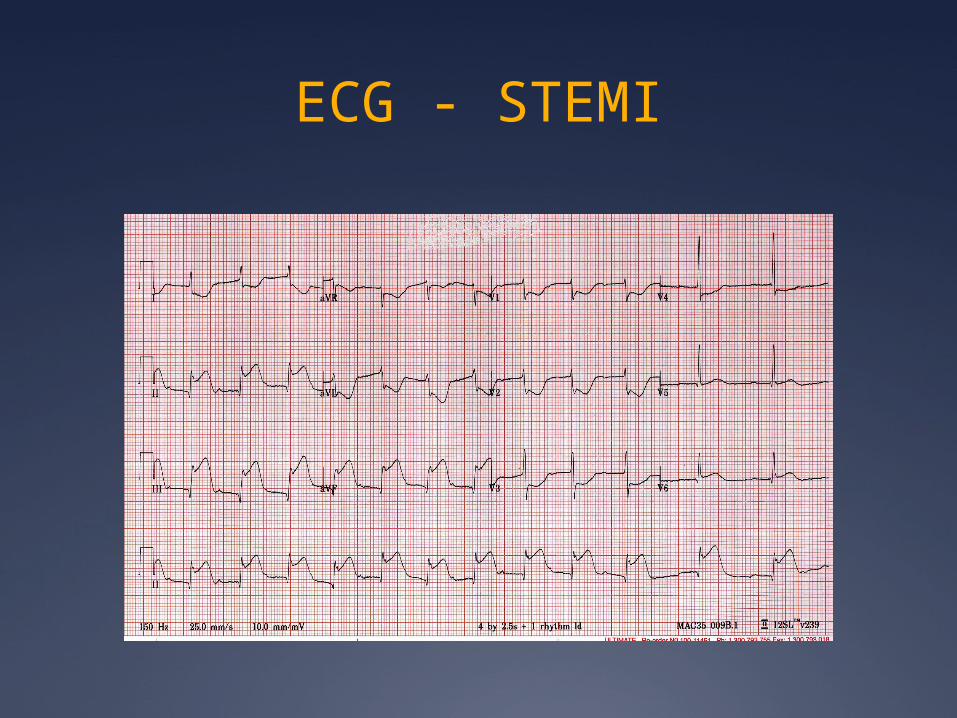
ECG - STEMI
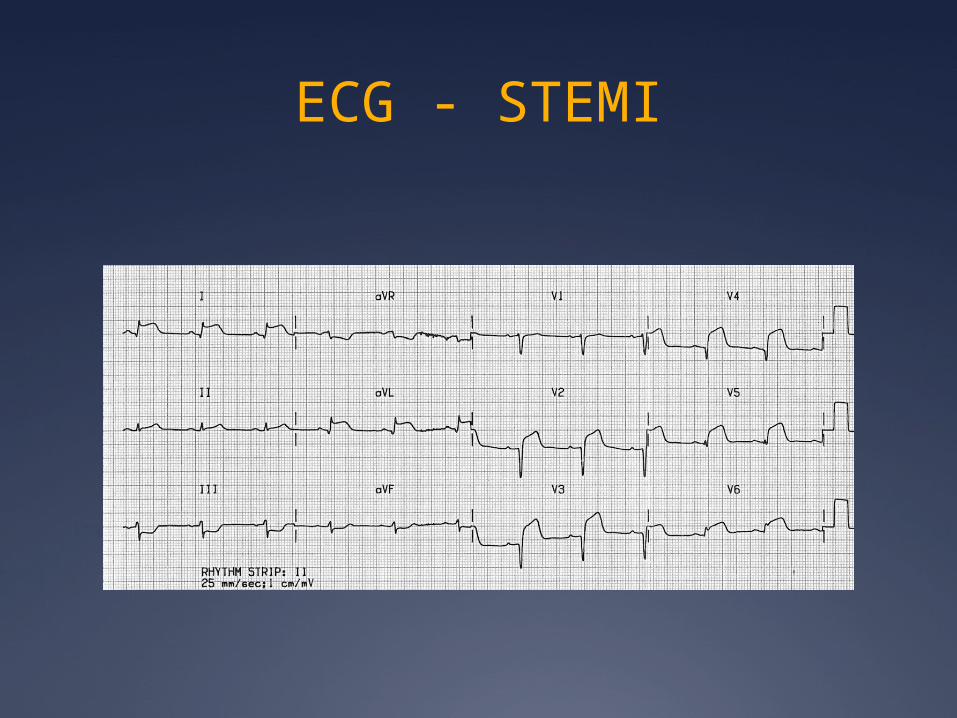
ECG - STEMI
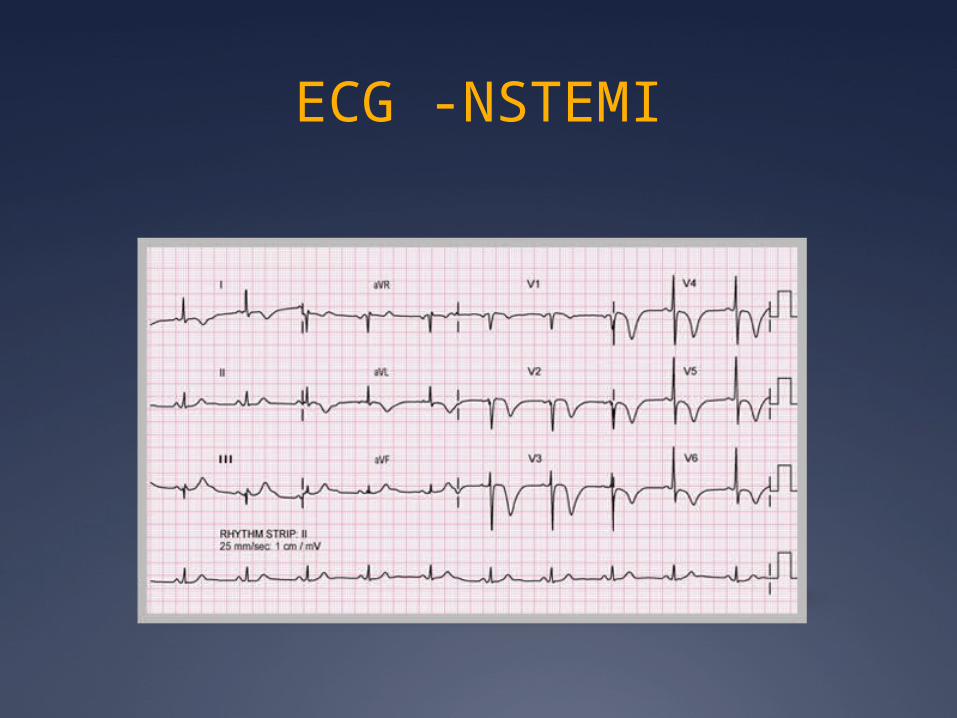
ECG -NSTEMI
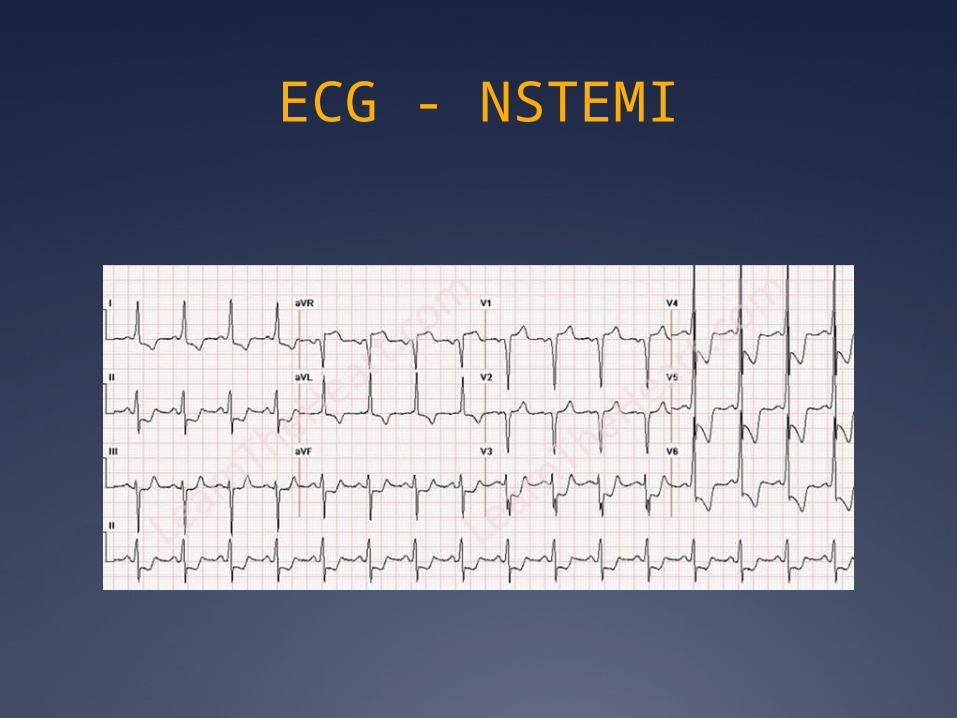
ECG - NSTEMI
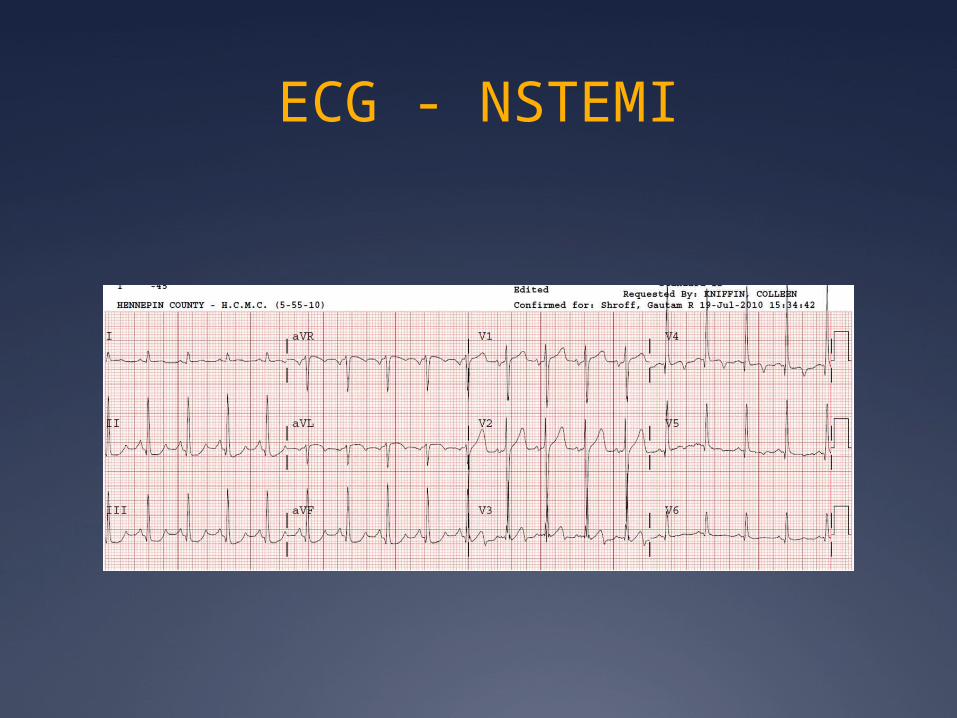
ECG - NSTEMI
Cardiac Enzymes
Serial blood draws
Every 4 hours x 4 sets
Myoglobin peaks first (detectable in 1-4 hrs)
Troponin peaks last (detectable in 3-12 hrs) most specific remains detectable in serum the longest
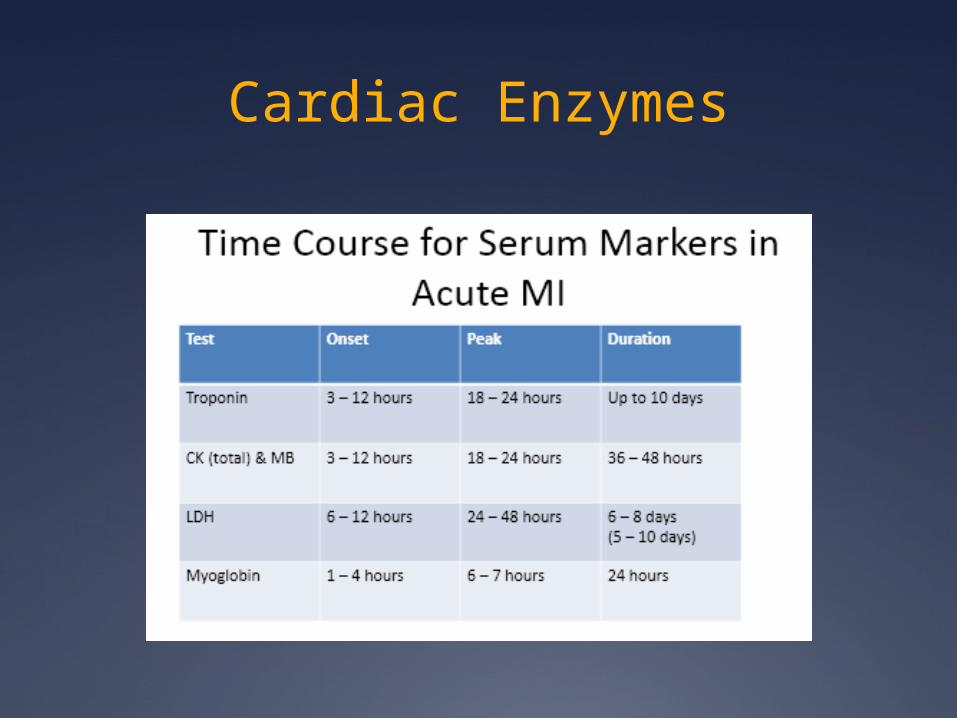
Cardiac Enzymes
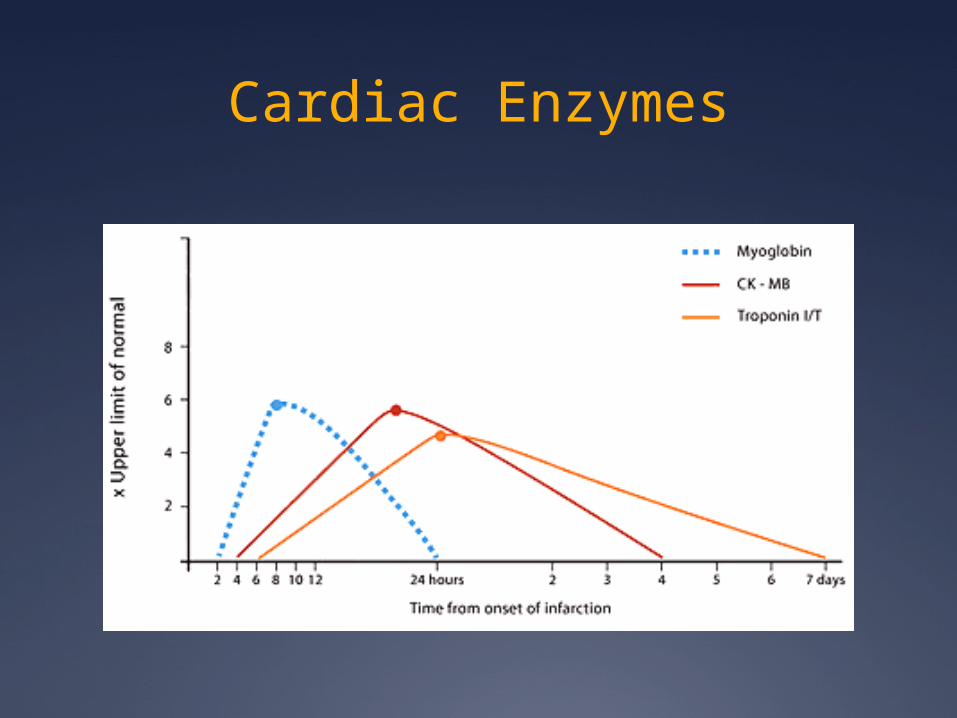
Cardiac Enzymes
Imaging (Echocardiography)
An echocardiogram can be performed to assess areas of the left ventricle that are not contracting normally as compared to areas that are contracting normally
After normal blood flow is interrupted, the area of the myocardium affected by the occluded artery will not function normally.
This abnormal wall motion can be detected by echocardiography
Treatment Antiplatelets
Supplemental oxygen
Nitrates
Pain control
Beta Blockers
Statin Therapy
Heparin (unfractionated / low-molecular-weight heparin)
Fibrinolytics
Angiotensin-Converting Enyme Inhibitors / Angiotensin Receptor Blockers
Glycoprotein Iib/IIIa Antagonists
Aldosterone Antagonists
Other Treatment Options
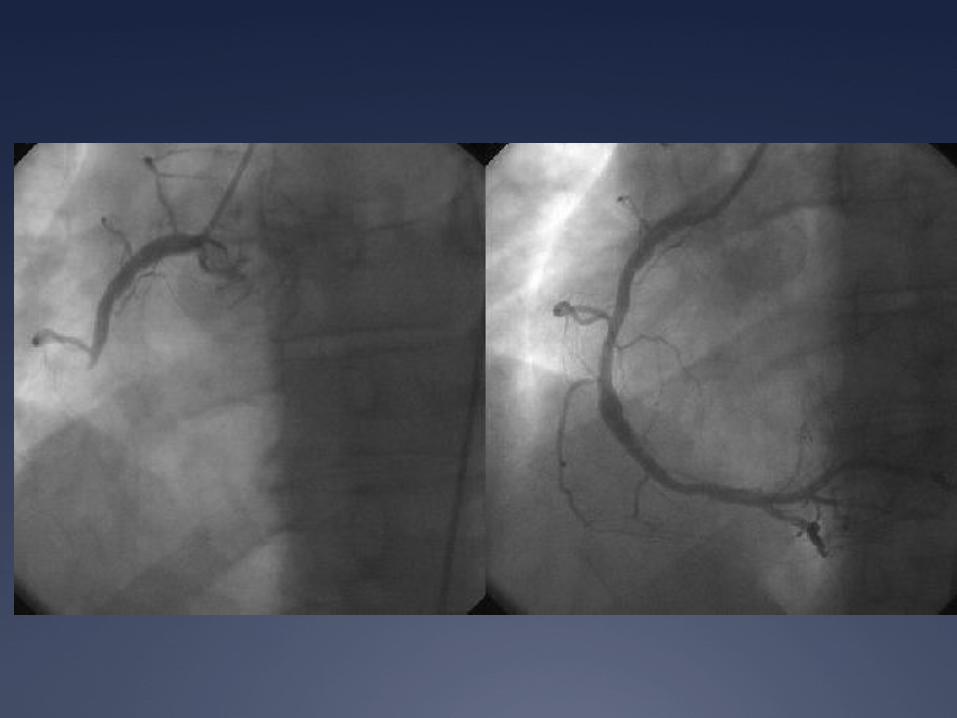
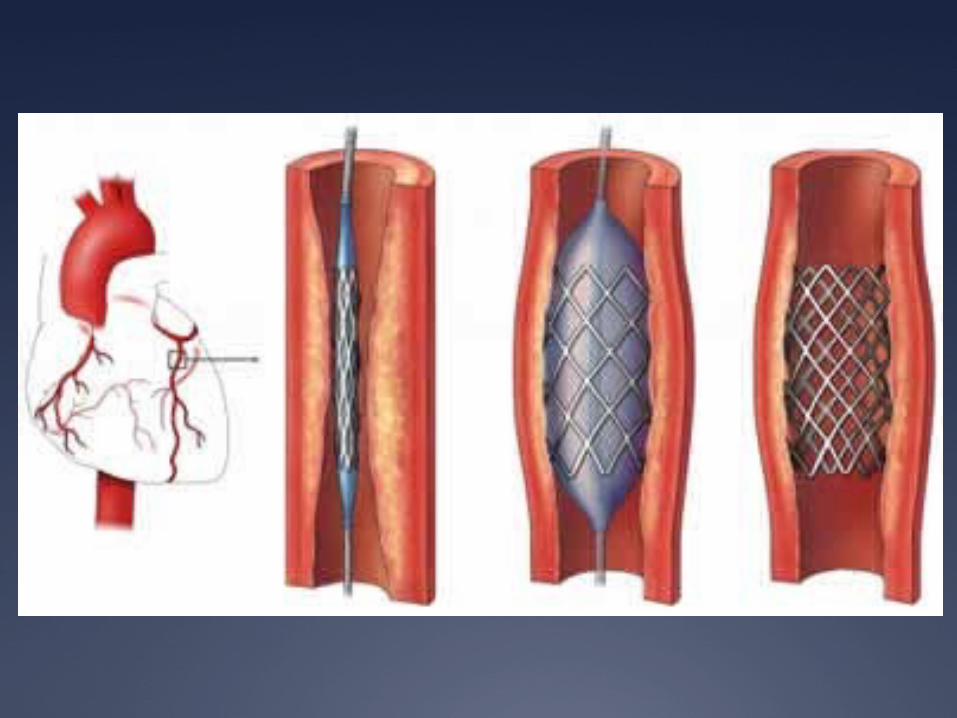
Percutaneous Coronary Intervention PCI / coronary stenting
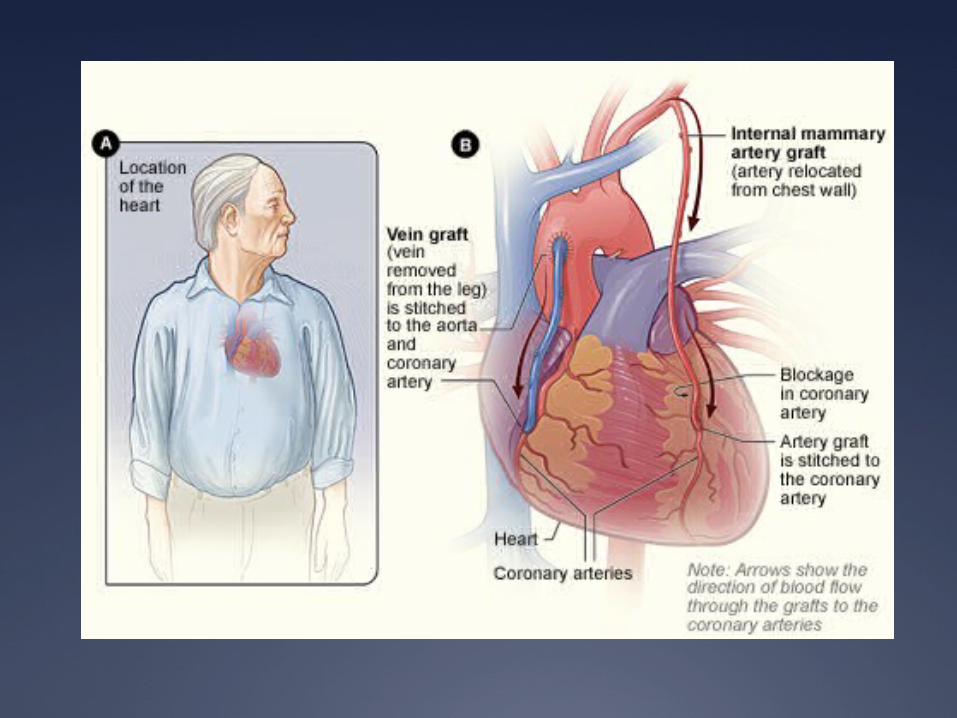
Surgical Revascularization CABG
Implantable Cardiac Defibrillators AICD
Treatment Outcomes
Long-term medications
Smoking cessation
Cardiac Rehabilitation
Long-Term Medications
Most oral medications instituted in the hospital at the time of acute MI will be continued long term
Aspirin, beta blockade, and statin therapy is continued indefinitely in all patients
ACE inhibitors are continued indefinitely in patients with CHF, left ventricular dysfunction, hypertension, or diabetes
Diet modification, regular exercise
Smoking Cessation
Smoking is a major risk factor for coronary artery disease and MI
For patients who have undergone an MI, smoking cessation is essential to recovery, long-term health, and prevention of re-infarction
In one study, the risk of recurrent MI decreased by 50% after 1 year of smoking cessation
Smoking Cessation
All STEMI and NSTEMI patients with a history of smoking should be advised to quit and offered smoking cessation resources Nicotine replacement therapy Pharmacologic therapy Referral to behavioral counseling or support
groups
Smoking cessation counseling should begin in the hospital, at discharge, and during follow up

Cardiac Rehabilitation
Provides a venue for continued education, reinforcement of lifestyle modification, and adherence to a comprehensive prescription of therapies for recovery from MI including exercise training
Participation in cardiac rehabilitation programs after MI is associated with decreases in subsequent cardiac morbidity and mortality
Other benefits include improvements in quality of life, functional capacity, and social support
Summary
MI results from myocardial ischemia and cell death, most often because of an intra-arterial thrombus superimposed on an ulcerated or unstable atherosclerotic plaque
Despite advances in therapy, MI remains the leading cause of death in the United States.
MI risk factors include hyperlipidemia, diabetes, hypertension, male gender, and tobacco use.
Diagnosis is based on the clinical history, ECG, and blood test results, especially creatine phosphokinase (CK), CK-MB fraction, and troponin I and T levels.
Summary
Outcome following an MI is determined by the infarct size and location, and by timely medical intervention.
Aspirin, nitrates, and beta blockers are critically important early in the course of MI for all patients.
Post-discharge management requires ongoing pharmacotherapy and lifestyle modification.





























