Embed Size (px)
DESCRIPTION
description about Acute Lymphocytic Leukemia
Citation preview
ACUTE Leukemia
What Is Leukemia?• Cancer of the white blood cells• Acute or Chronic• Affects ability to produce normal blood cells• Bone marrow makes abnormally large number of immature white
blood cells called blasts
History• Means “white blood” in Greek• Discovered by Dr. Alfred Velpeau in France, 1827• Named by pathologist Rudolf Virchow in Germany, 1845
Main Types• Acute Lymphocytic Leukemia (ALL)• Acute Mylogenous Leukemia (AML)• Chronic Lymphocytic Leukemia (CLL)• Chronic Mylogenous Leukemia (CML)
28/04/2023 5
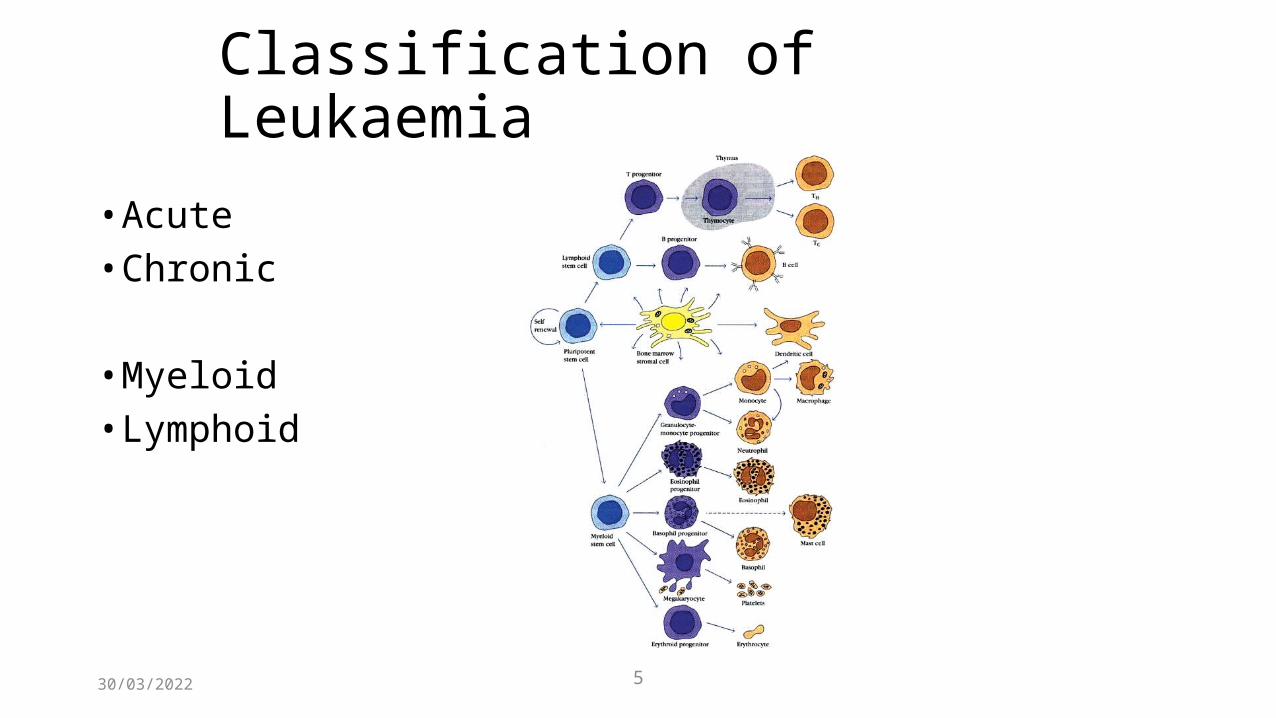
Classification of Leukaemia• Acute• Chronic
• Myeloid• Lymphoid
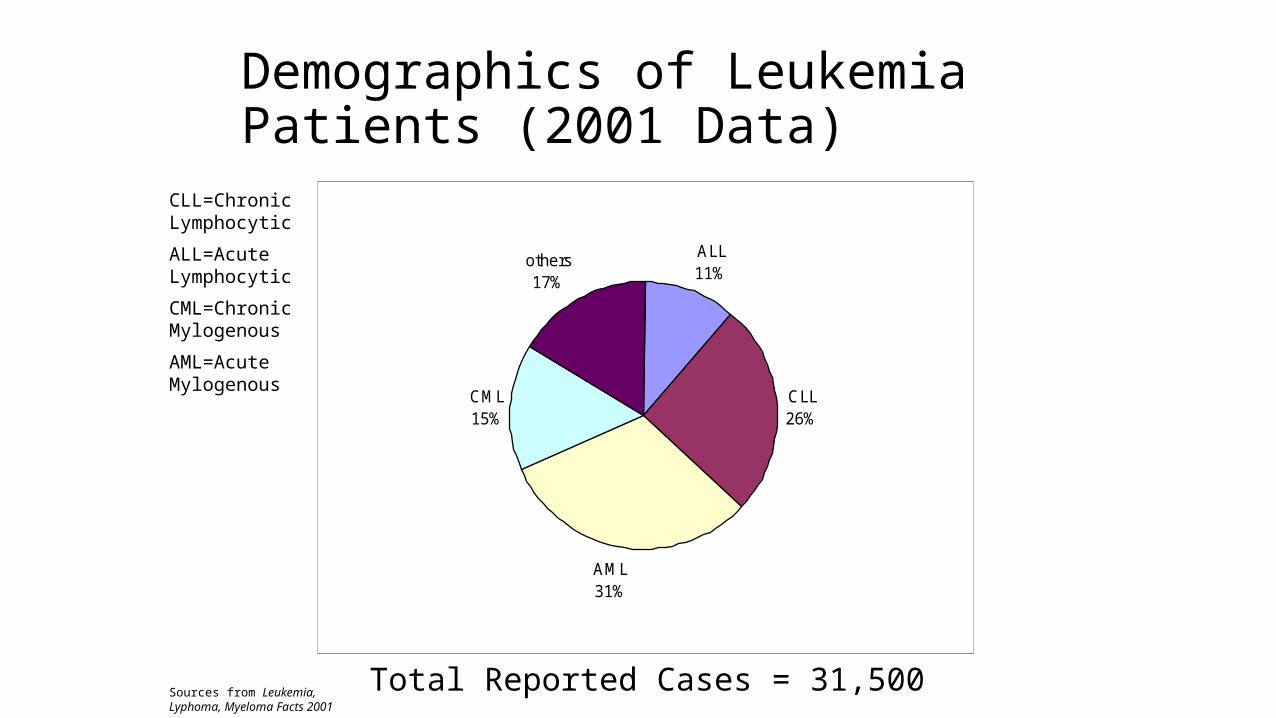
Demographics of Leukemia Patients (2001 Data)
ALL11%
CLL26%
AML31%
CML15%
others17%
Total Reported Cases = 31,500Sources from Leukemia, Lyphoma, Myeloma Facts 2001
CLL=Chronic Lymphocytic
ALL=Acute Lymphocytic
CML=Chronic Mylogenous
AML=Acute Mylogenous
Symptoms• When there are excessive white blood cells --> Infections• When there are few red blood cells: Paleness --> Anemia• When there are few platelets --> Excessive bleeding
Tests For Diagnosis• Finger prick• Blood sample• Blood dye• Bone marrow sample• Spinal Tap/Lumbar Puncture
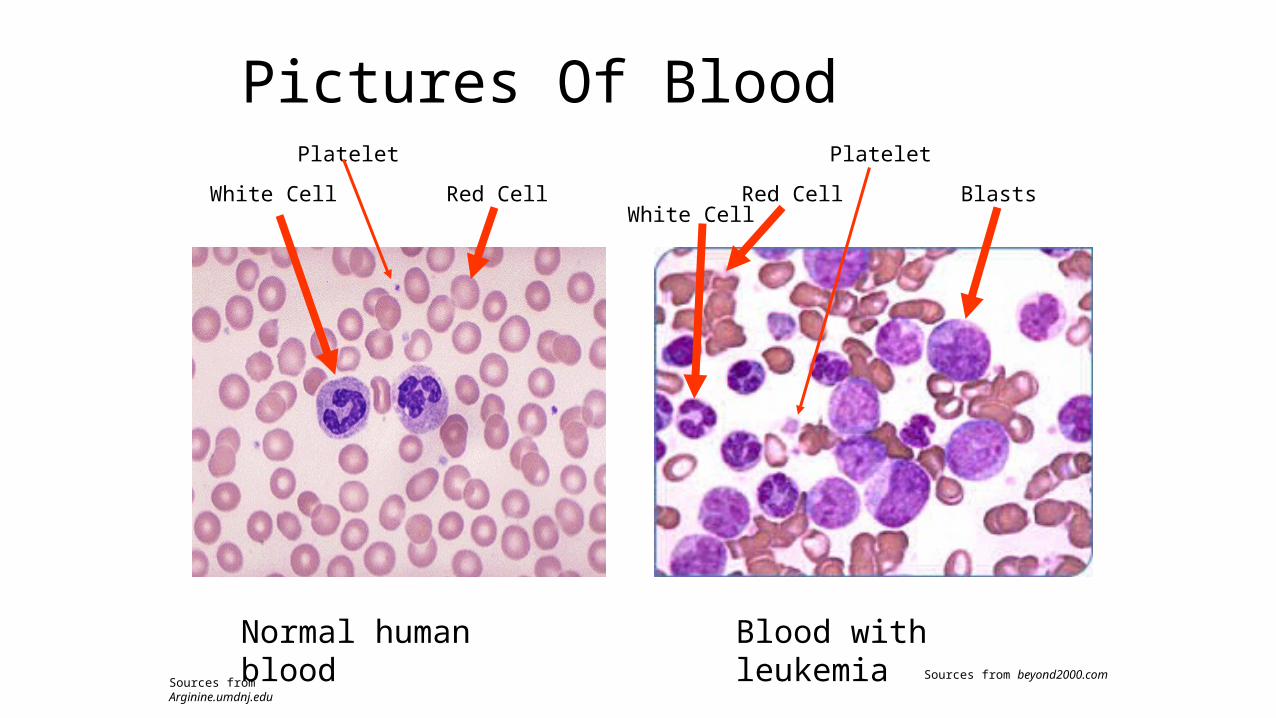
Pictures Of Blood
Normal human blood
White Cell Red Cell
Platelet
Blood with leukemia
BlastsRed Cell
Platelet
White Cell
Sources from Arginine.umdnj.eduSources from beyond2000.com
Effects On the Body• Attacks the immune system• Infections• Anemia• Weakness• No more regular white blood cells, red blood cells, and
platelets• Blasts clog blood stream and bone marrow
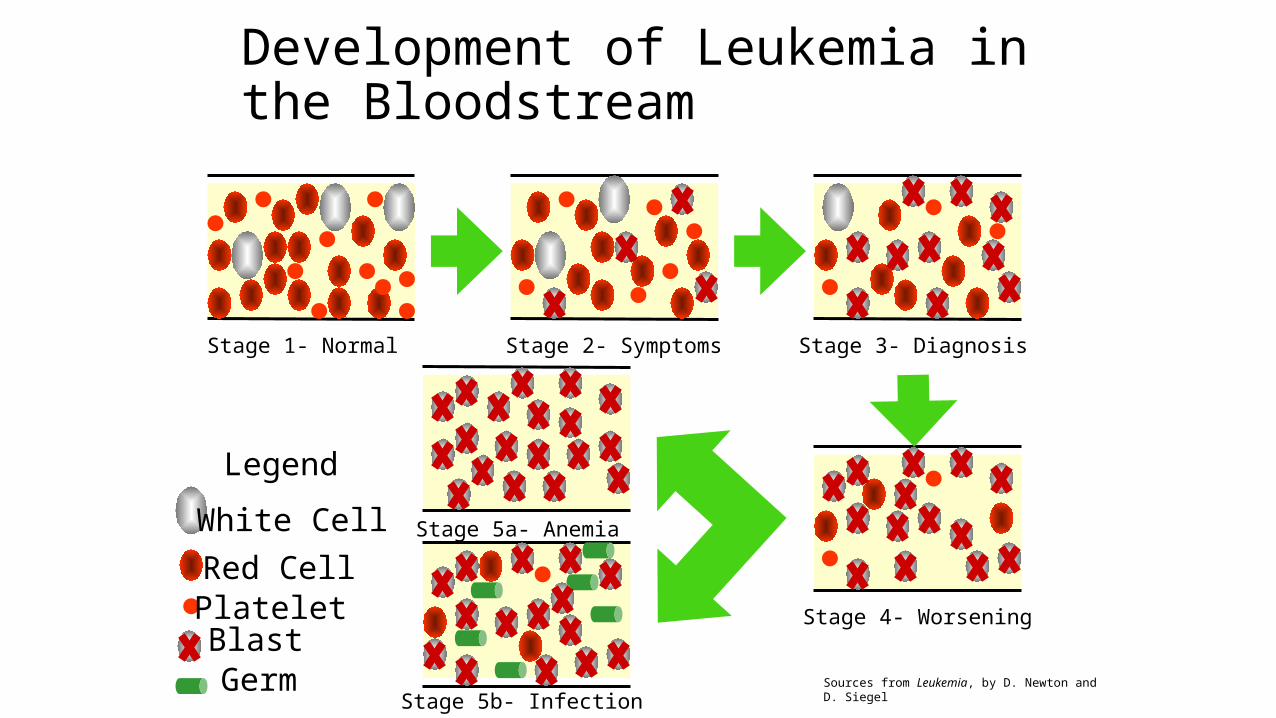
Development of Leukemia in the Bloodstream
Stage 1- Normal Stage 2- Symptoms Stage 3- Diagnosis
Stage 4- Worsening
Stage 5a- Anemia
Stage 5b- Infection
Legend
White Cell Red Cell Platelet Blast Germ Sources from Leukemia, by D. Newton and D. Siegel
Causes• High level radiation/toxin exposure• Viruses• Genes• Chemicals• Mostly unknown
Treatment• Chemotherapy• Immunotherapy• Radiation• Bone marrow transplant

ACUTE LEUKAEMIA
28/04/2023 15
• Rapidly progressive• Proliferation of primitive “blast” cells• Acute myeloblastic (myeloid) leukaemia
• “Acute non-lymphoblastic leukaemia”
• Acute lymphoblastic leukaemia
CLINICAL PRESENTATION
Symptoms of acute leukaemia are largely the result of interference with normal haematopoiesis.
Generally it is not possible on clinical presentation to differentiate lymphoid from myeloid leukaemia.
Causes of Acute Leukemias• Idiopathic (most)• underlying hematologic disorders• chemicals, drugs• ionizing radiation• viruses (Human T Lymphotropic Virus I)• hereditary/genetic conditions• Preceding bone marrow disorders• Chemotherapy – especially alkylating agents, epipodophyllotoxins and
anthracyclines

CLINICAL SIGNSpallorlymphadenopathyhepatosplenomegalysternal tendernesspurpura / petechiaeretinal haemorrhagesmouth ulcersgum hypertrophy (monocytic type)
LABORATORY FINDINGS
Hb is invariably low (30-80 g/L)
WBC is usually high (especially lymphoblastics and monocytics). Can be normal or low.
Plts usually dangerously low
Generally it is not possible to differentiate myeloblasts from lymphoblasts by morphology alone.
MANAGEMENT
Cytotoxic chemotherapy, radiotherapy and bone marrow transplantation. The goal is to eradicate the leukaemic cell mass while giving supportive care. In children with ALL postremission therapy includes central nervous system (CNS) prophylaxis.
PROGNOSIS
Young patients do better than old. Patients presenting with low white counts do better. Must achieve complete remission (no signs of leukaemia and return of normal haematology parameters) to prolong survival.
28/04/2023 21
Acute Lymphoblastic Leukaemia• WHO classification:
• Precursor B cell ALL• Precursor T cell ALL• Burkitt’s mature B lymphoblastic leukaemia/lymphoma• Bi-phenotypic leukaemia
• FAB• L1, L2, L3
28/04/2023 22
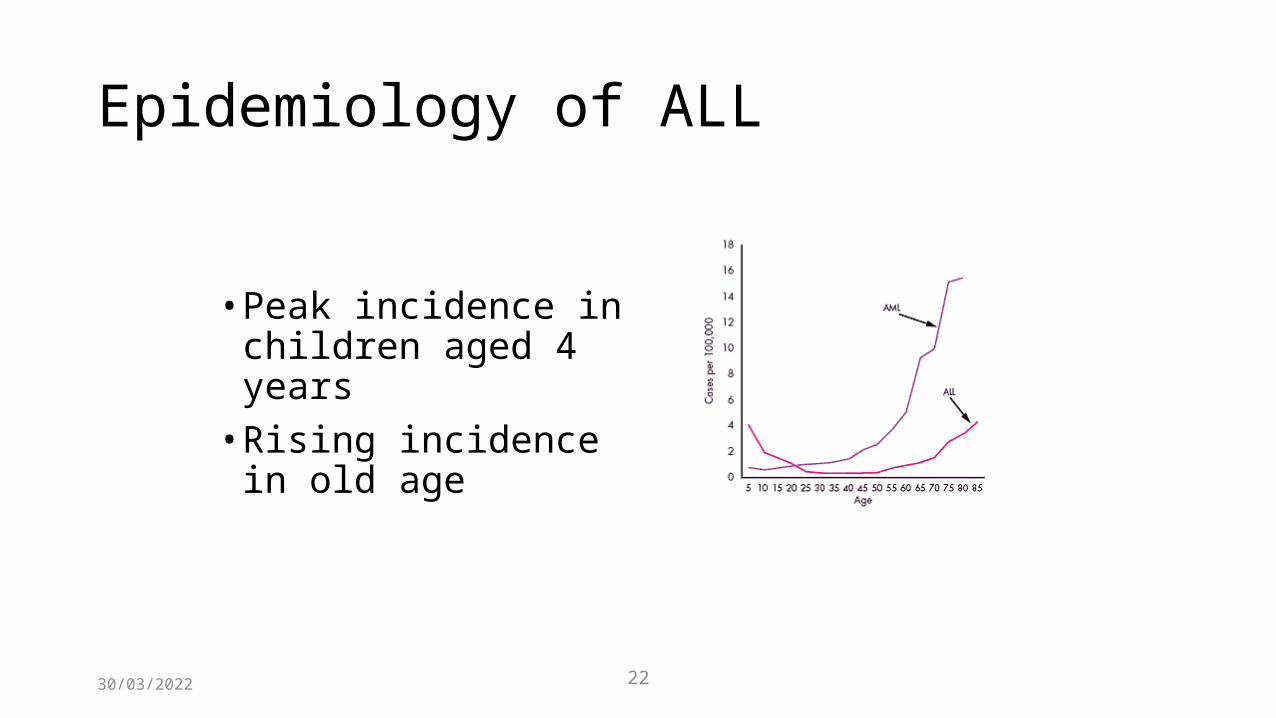
Epidemiology of ALL
• Peak incidence in children aged 4 years
• Rising incidence in old age
28/04/2023 23
Prognostic factors in ALL• Sex: female > male• Ethnicity: caucasian > non-caucasian• Age: <10 and >1 year old• WBC < 50 x 109/l• CNS involvement is bad• Initial response to treatment (day 14 BM)• Morphological and genetic sub-types
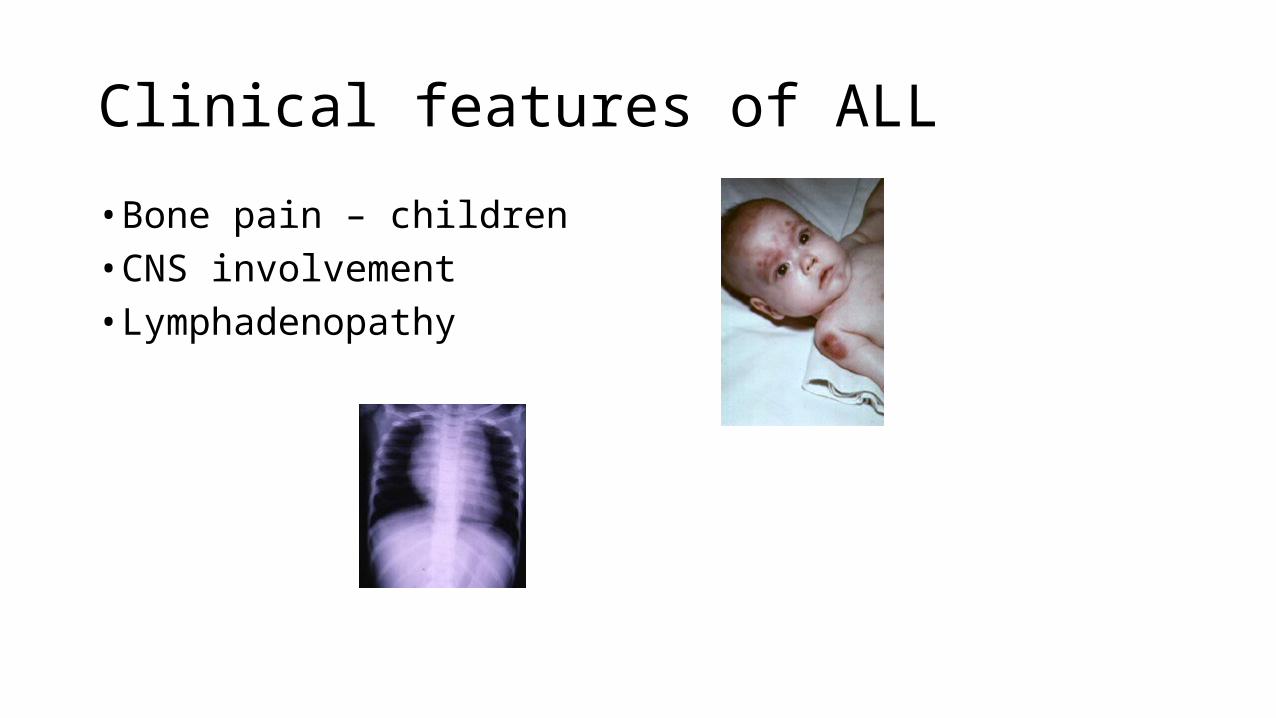
Clinical features of ALL• Bone pain – children• CNS involvement• Lymphadenopathy
Continue…• Involvement of other tissue such as spleen, liver, lymph node, and
meninges are common• Involvment of CNS may give rise to headach, vomiting and irritable
behaviour.
Principles of Treatment• combination chemotherapy
• first goal is complete remission• further Rx to prevent relapse
• supportive medical care• transfusions, antibiotics, nutrition,
metabolic /electrolyte abnormalities• psychosocial support
• patient and family
Therapeutic Concepts in ALL• Induce a complete remission and restore normal
hematopoiesis avoiding excessive toxicity• Reduce inapparent leukemia with short-term, high-
dosage cytocidal therapy early in remission when the child is well and drug sensitivity is greatest
• Prevent CNS leukemia• Use prolonged combination chemotherapy to
eradicate residual disease when there is no evidence of leukemia

Basic Therapy in Childhood ALL
• Induction Treatment 4-8 wk• Consolidation treatment (intensification) 2-10 wk• Continuation treatment (maintenance) 2-3 y• Reinduction therapy (delayed intensification) 2-7 wk• CNS-directed therapy (intrathecal injection of methotrexate
and cranial radiation) 3 wk