Embed Size (px)
Citation preview

Acute Kidney
Injury
Ajay Dhaygude


Admitting specialty

Inadequate risk assessment

Missed complications


AKI vs ACS
• Cardiac muscle
Vs
Pre, intra and post
AKI
• Rapidity & symptoms
• Biomarker[s]


Relationship between GFR and Serum creatinine


Epidemiology
• UK data 172 to 630 pmp/yr
• AKI requiring dialysis: 200 pmp/year
• ICU national audit: 4.9% patients have AKI and 10% bed days are accounted for AKI
• Mortality: uncomplicated- 10%
with MOF: 50%
With RRT: 80%
• Financial implications- £ 450-600 million/yr (more than Skin, breast and lung cancer treatment together)

Definition and stages
• Serum creatinine rises by ≥ 26.5 μmol/L within 48 hours or
• Serum creatinine rises ≥ 1.5 fold from the reference value,
which is known or presumed to have occurred within one
week or
• urine output is < 0.5ml/kg/hr for >6 consecutive hours
• Stage 1: 1.5 to 1.9 times raised S Cr.
• Stage 2: 2 to 2.9 times raised S Cr.
• Stage 3: S Cr more than 3 times high or absolute increase
by 353 mmol/lr OR need to start dialysis

Selby et al PLoS One. 2012; 7(11): e48580.

Risk factors

Case-1 • JW-83 Yrs old, back ground, CKD, IHD
• Admitted with Cl diff diarrhoea.
• Inspite of oral vancomycin + rehydration
developed AKI
• Ref by ITU cons at CDH:
• Decreased UOP (?). BP 110 systolic, apyrexial
• Urea- 24.9, K- 4.6, Creat 423, (CRP improving)
• pH 7.2, base excess -11, bicarb 15
• Pt has received 6 litres fluid in last 48 hours now
RR 18, basal crackles, gases okay

Results


• How do you treat him?
• ?diuretics
• Urgent dialysis
• Anything else




Diuretics in AKI, Bagshaw et al
• 67% clinicians use diuretics in AKI
• 86% patients had pulmonary oedema
• IV Furosemide was most commonly used drug
• Most clinicians were aware of toxicity, effect on
renal recovery.
• Most were willing to take part in RCT

Diuretics in AKI
• Use if:
– Fluid overloaded
– Not hypotensive (?)
• Use single large dose [up to 250 mg iv over 4
hours]
• If no response then abandon further use
• Monitor electrolytes/ fluid balance
• Can enhance gentamicin toxicity
• Diuretics does not cure AKI !!!

Case-2
• LH- 53 years young previously fit and well female
patient is admitted with sudden onset severe
abdominal pain.
• On admission found to be confused, hypotensive
• Rapid deterioration requiring ventilation and
inotropic suport.

How will you investigate her?
• CT abd excluded ischaemic bowel.

Biochemistry

Transferring patients with AKI
• Death during transfer should be avoided at
any cost
• Get your critical care team involved if your
patients has-
– Severe acidosis,
– refractory hyperkalemia,
– haemodynamically unstable patients and
severe pulmonary oedema

Cause of death in AKI, Selby et al

Early Goal-Directed Therapy in the Treatment
of Severe Sepsis and Septic Shock
Emanuel Rivers, M.D., M.P.H., Bryant Nguyen, M.D., Suzanne Havstad,
M.A., Julie Ressler, B.S., Alexandria Muzzin, B.S., Bernhard Knoblich,
M.D., Edward Peterson, Ph.D., Michael Tomlanovich, M.D., for the Early
Goal-Directed Therapy Collaborative Group
Volume 345: 1368-1377 November 8, 2001
Sepsis and the critically ill

Protocol group


Treatment given 0-6 hours 7-72 hours 0-72 hours
Fluids (ml)
EGDT 4991 8625 13443
Standard 3499 10602 13358
P value <0.001 0.01 0.73
RBC transfusion
(%)
EGDT 64.1 11.1 68.4
Standard 18.5 32.8 44.5
P value <0.001 <0.001 <0.001
Vasopressor use
(%)
EGDT 27.4 29.1 36.8
Standard 30.3 42.9 51.3
P value 0.62 0.03 0.02
Dobutamine use
(%)
EGDT 13.7 14.5 15.4
Standard 0.8 8.4 9.2
P value <0.001 0.14 0.15
Mechanical
ventilation (%)
EGDT 53.0 2.6 55.6
Standard 53.8 16.8 70.6
P value 0.90 <0.01 0.02

Electrolyte contents of some common fluids

Case-3
• IW- 70 Year old pt with H/O NHL is admitted with
generalised oedema, and feeling unwell.
• Finished chemotherapy 5 months ago, in remission.
• O/E Gross oedema, hypotensive and tachypnoeic
• CXR- Pulmonary oedema.
• What investigations are needed?
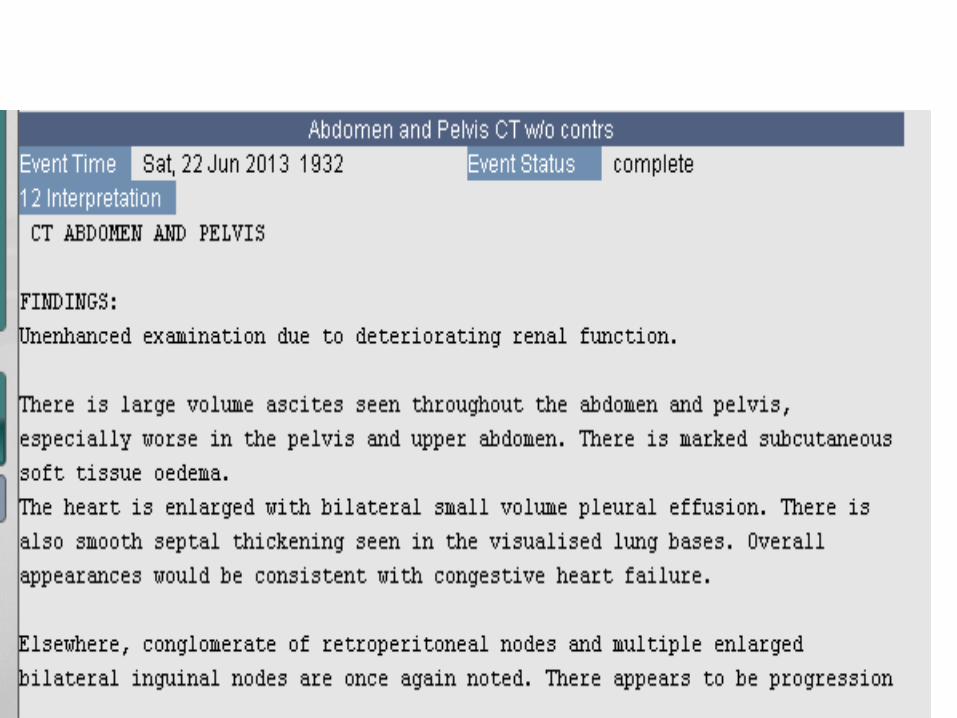

Biochemistry

She is known to have severe biventricular failure due
to valvular heart disease.

Management of cardio-renal syndrome
• Diuretics Optimisation Strategies Evaluation trial:
308 pts low or high dose furosemide given as 12
hourly boli or continuous infusion.
• No difference in infusion or bolus regime
• High dose was associated with better response but
higher likelyhood of renal impairment [23% vs 14%]
• CARRESS-HF trial: compared haemofiltration
versus stepped pharmacologic therapy. Later
approach was superior.

Case-4
• AD, 79 yrs old male presented with haematuria and
during hospital stay developed AKI

How would you investigate?


Missed investigations -NCEPOD

Case-5
• GB, 65 yr old pt with known CKD III was admitted with PR
bleed. Sigmoidoscopy was normal but was found to have
weight loss and was hospitalised.
• Developed progressive AKI in hospital. Referred to medics
• Also has purpuric rash, haematuria and haemoptysis.
• CT chest- widespread nodular shadow, bronchoscopy-
pulmonary haemorrhage.
• Became anuric and was transferred to HDU for
haemofiltration


How do you investigate further?
• How do you manage this patient?
• Urgent renal referral please.
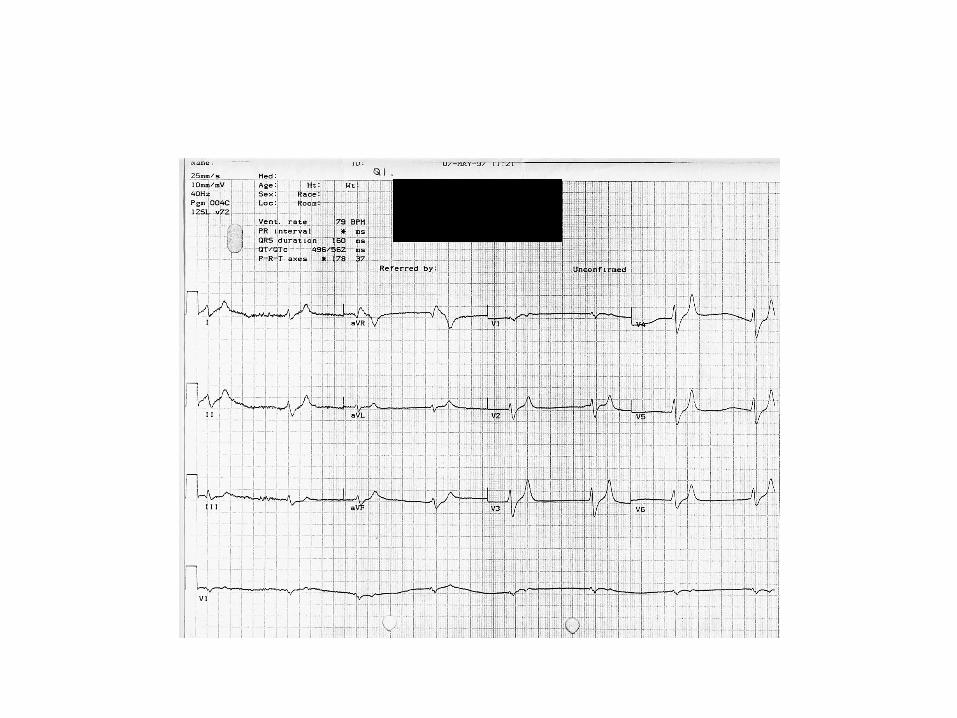
Hyperkalaemia

Hyperkalaemia
• Do an ECG + attach to cardiac monitor
• 10ml 10% Calcium Gluconate; repeat until ECG normalizes
• Nebulised Salbutamol (5-10mg)
• 50ml 50% Dextrose + 10 unit Insulin
• iv Sodium Bicarbonate (50-100ml 8.4% NaHCO3 via central line)
• Calcium Resonium (30g rectally)

Fluid overload
Pulmonary Oedema
• Furosemide 500mg iv over 1 hour
• Oxygen
• Opiates
• Nitrate iv
Dialysis if refractory to above
Pericarditis
• Pericarditis
• More common in chronic renal failure than ARF
• Risk of progression to tamponade
Acidosis Severe Acidosis
• eg if pH <7.1
Symptomatic uraemia
Symptomatic Uraemia
• Confusion, coma, asterixis

Do I put in a central line?
Do I test the urine?
Do I use diuretic?
Do I use Dopamine?
Do I give any other drugs?
Do I ask for urgent dialysis?
Only if uncertain of volume status
Of course
Only for fluid overload
No
No
If hyperkalaemia, fluid overload,
pericarditis, acidosis
Do’s and Don’ts

The take-home message
• AKI is associated with significant mortality and has
financial implications.
• Elderly patients are at increased risk
• Small rise in Creatinine suggests big drop n GFR
• Sepsis is commonest cause of death
• Remember acidosis!

Indications for Dialysis
Persistent hyperkalaemia
Fluid overload
Pericarditis
Acidosis
Symptomatic uraemia


AKI= FLUIDS
• F fluid balance
• L low BP
• U urine dipstics
• I imaging
• D drugs
• S sepsis

Case -6
65Yr M. Admitted to BVH ITU with Creat 1100
H/o travel to Tenerife and developed some D&V
PMH- Known single kidney (Creat 180- 3 months ago)
USS ?Obstruction- nephrostomy- no Urine
CT Pelvis- no cause for obstruction found
Transferred to RPH- Immunology negative
Kidney biopsy: crescentic GN+ Ischaemic changes + CPN
Renal angio- RAS- Stented, antibiotics
Remained on dialysis. Died after 6 months (line sepsis)






























