Embed Size (px)
Citation preview
Listen to this manuscript’s
audio summary by
JACC Editor-in-Chief
Dr. Valentin Fuster.
J O U R N A L O F T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 6 7 , N O . 2 2 , 2 0 1 6
ª 2 0 1 6 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 6 . 0 3 . 5 5 5
THE PRESENT AND FUTURE
STATE-OF-THE-ART REVIEW
Acute Ischemic Stroke Intervention
Priyank Khandelwal, MD,a Dileep R. Yavagal, MD, MBBS,b,c Ralph L. Sacco, MD, MSbABSTRACT
Fro
Ne
Mi
tria
da
res
Ing
Dr
Ma
Acute ischemic stroke (AIS) is the leading cause of disability worldwide and among the leading causes of mortality.
Although intravenous tissue plasminogen activator (IV-rtPA) was approved nearly 2 decades ago for treatment of AIS,
only a minority of patients receive it due to a narrow time window for administration and several contraindications to its
use. Endovascular approaches to recanalization in AIS developed in the 1980s, and recently, 5 major randomized trials
showed an overwhelming superior benefit of combining endovascular mechanical thrombectomy with IV-rtPA over
IV-rtPA alone. In this paper, we discuss the evolution of catheter-based treatment from first-generation thrombectomy
devices to the game-changing stent retrievers, results from recent trials, and the evolving stroke systems of care to
provide timely access to acute stroke intervention to patients in the United States. (J Am Coll Cardiol 2016;67:2631–44)
© 2016 by the American College of Cardiology Foundation.
A cute ischemic stroke (AIS) occurs when thereis a sudden occlusion of the arterial bloodsupply to part of the brain, and is most
commonly manifested by focal neurological deficits.More than 750,000 stroke cases occur every year inthe United States, making it the fifth leading causeof death and the leading cause of disability. Strokescost more than $70 billion annually, and have adevastating effect on the quality of life of a significantproportion of patients and their caregivers (1).
The mechanisms of ischemic stroke can be dividedinto embolic (artery to artery or cardioembolic), lip-ohyalinotic occlusion of small arteries, or in situthrombosis over an atherostenotic plaque (athero-thrombosis). Thrombolysis to recanalize the occlusionand reperfuse the brain, through either pharmacolog-ical or mechanical means, is the mainstay of treatmentoptions for patients with AIS. Until recently, intrave-nous recombinant tissue plasminogen activator(IV-rtPA) was the only approved therapy for patientswith AIS presenting within 0 to 4.5 h (2). Although
m the aDepartment of Interventional Neuroradiology, Brigham andWome
urology, University of Miami Miller School of Medicine, Miami, Florida; a
ami Miller School of Medicine, Miami, Florida. Dr. Yavagal serves as a stee
l and the RECOVER-Stroke trial; serves as a consultant to Medtronic/Covid
ta and safety monitoring board member of the ESCAPE trial, for which he
earch funding from the National Institute of Neurological Disorders and
elheim. Dr. Khandelwal has reported that he has no relationships re
s. Khandelwal and Yavagal contributed equally to this work.
nuscript received November 18, 2015; revised manuscript received March
approval of IV-rtPA was a landmark step towardtreatment of AIS, more than 50% of patients receivingIV-rtPA were still either severely disabled or dead(3,4). The absolute reduction in chance of pooroutcome in patients treated with IV-rtPA within 3 h is10%, which amounts to a number needed to treat(NNT) of 10. In a 3- to 4.5-h time window, the effectis reduced further, to 7% (NNT of 14) (5,6). Delays inachieving reperfusion, inadequately complete recan-alization, and hemorrhagic transformation weresome of the limitations of intravenous thrombolysis.To overcome these limitations, minimally invasiveendovascular approaches were developed over thelast 2 decades. After initial disappointing results fromtrials using the first generation of mechanical throm-bectomy devices, in 2015, endovascular mechanicalthrombectomy with a retrievable stent (commonlycalled a stent retriever), along with IV-rtPA wasestablished as the new standard of care for AIS due tolarge vessel occlusion (LVO) (7). In this paper, we shallreview the evolution of endovascular catheter-based
n’s Hospital, Boston, Massachusetts; bDepartment of
nd the cDepartment of Neurosurgery, University of
ring committee member of the SWIFT Prime clinical
ien Neurovascular and Aldagen/Cytomedix; and is a
has received travel support. Dr. Sacco has received
Stroke, American Heart Association, and Boehringer
levant to the contents of this paper to disclose.
14, 2016, accepted March 16, 2016.

TABLE
1. Onset
2. Signifi
3. Any h
4. Acute>1.7,
5. Arteria
6. Recenwithi
7. Curreninhib
8. Histormalfo
9. CT sharter
*Criteria fono prior hagent.
AIS ¼ alitus; GI ¼venous reNIHSS ¼ N
ABBR EV I A T I ON S
AND ACRONYMS
AIS = acute ischemic stroke
ASPECTS = Alberta Stroke
Program Early CT score
CT = computed tomography
CTA = computed tomography
angiography
FIO = functionally independent
outcome
IV-rtPA = intravenous
recombinant tissue
plasminogen activator
LVO = large vessel occlusion
mRS = modified Rankin Score
MT = mechanical
thrombectomy
NIHSS = National Institutes of
Health Stroke Scale
Khandelwal et al. J A C C V O L . 6 7 , N O . 2 2 , 2 0 1 6
Acute Ischemic Stroke Intervention J U N E 7 , 2 0 1 6 : 2 6 3 1 – 4 4
2632
treatment of stroke, the reasoning behindthe overwhelming success of recent endo-vascular clinical trials in AIS, and their effecton acute stroke care.
EVOLUTION OF AIS TREATMENT
INTRAVENOUS THROMBOLYSIS. IV-rtPAtreatment was shown to benefit patients withAIS in the 1995 NINDS (National Institute ofNeurological Disorders and Stroke) study.IV-rtPA was a major milestone in stroketreatment, as the first disease-modifyingtherapy for AIS (3). On the basis of theNINDS study results, in 1996, the Food andDrug Administration (FDA) approved the useof IV-rtPA for patients with AIS presentingwithin 3 h of symptom onset. Subsequently,in 2008, ECASS (European Cooperative AcuteStroke Study) III showed benefit of IV-rtPA
over placebo among those treated within 3 to 4.5 hof symptom onset (6,8). These studies establishedIV-rtPA as a standard therapy for patients with AISwithin 4.5 h of symptom onset. Although the FDA didnot modify the original indication for use of IV-rtPAbeyond 3 h, recent stroke guidelines from the Amer-ican Heart Association (AHA) recommended using itup to 4.5 h from onset of symptoms in eligible pa-tients (2). Despite this recommendation, the use ofIV-rtPA is estimated to occur in <3% of patients pre-senting with AIS (9). The narrow therapeutic timewindow of 4.5 h is the most common reason thatpatients do not receive IV-rtPA, along with a fewothers (Table 1). Also IV-rtPA has major therapeutic
1 Contraindications for IV-rtPA in AIS
of symptoms more than 4.5 h.*
cant head trauma or prior stroke in previous 3 months.
istory of previous intracranial hemorrhage.
bleeding diathesis, including platelet count <100,000, INRor PT >17 s.
l puncture at noncompressible site in previous 7 days.
t major surgery within 14 days and recent GI tract hemorrhagen 21 days.
t use of direct thrombin inhibitors or direct factor Xaitors.
y of previous intracranial neoplasm, arteriovenousrmation, or aneurysm.
owing early ischemic changes in more than one-third of MCAy distribution.
r IV-rtPA between 3 to 4.5 h: patient <80 years of age, NIHSS <25 andistory of DM and AIS (both), and not taking any oral anticoagulation
cute ischemic stroke; CT ¼ computed tomography; DM ¼ diabetes mel-gastrointestinal; INR ¼ international normalized ratio; IV-rTPA ¼ intra-
combinant tissue plasminogen activator; MCA ¼ middle cerebral artery;ational Institute of Health Stroke Scale; PT ¼ prothrombin time.
limitations, including unresponsiveness of largethrombi to enzymatic digestion, resulting in a lowrecanalization rate (13% to 50%) in LVO stroke and alow rate of benefit in the patients having the mostdisabling strokes (10,11). To overcome these majorlimitations of IV-rtPA, endovascular approaches havebeen developed over the last 2 decades using cathe-ters that are delivered intra-arterially to the site of theintracranial clot to recanalize the occluded vessel.
INTRA-ARTERIAL THROMBOLYSIS. PROACT (Prolysein Acute Cerebral Thromboembolism Trial) was thefirst prospective randomized controlled trial (RCT) toinvestigate the safety and efficacy of intra-arterialrecombinant prourokinase (IA-proUK) and heparincompared with intra-arterial heparin alone, appliedwithin 6 h of stroke symptom onset in patients withmiddle cerebral artery occlusion (12). This phase IIstudy, which randomized 46 patients, showed asignificantly higher recanalization rate with IA-proUKalong with a nonsignificant, but higher symptomatichemorrhage rate. PROACT II, a phase III study of 180patients, soon followed and showed the clear supe-riority of IA-proUK in achieving the primary outcomeof no or slight disability, defined as a modified RankinScale (mRS) of 0 to 2 at 90 days, functionally inde-pendent outcome (FIO) in 60% versus 18% (p < 0.001)of patients, as well as a greater recanalization rate of40% versus 25% (p < 0.04) compared withintra-arterial (IA) heparin alone. The improved clin-ical outcome occurred despite a higher symptomatichemorrhage rate of 10% in the treatment armcompared with 2% in control subjects. Despite thesuccess of PROACT II, the FDA did not approveIA-proUK, and soon afterward, this pharmacologicalagent was no longer commercially available (13). TheAHA 2005 and 2013 guidelines recommended IAthrombolysis in carefully selected patients withmiddle cerebral artery (MCA) occlusions within 6 hwho were not candidates for IV-rtPA (Class I, Level ofEvidence: B), but it was not enough to make it astandard of care (14,15).
MECHANICAL THROMBECTOMY
The era of mechanical thrombectomy (MT) beganwith development of the “mechanical embolusremoval in cerebral ischemia” (MERCI) device. Thedevice is made of a corkscrew-shaped nitinol wirethat is deployed into the thrombus in the occludedintracranial artery. Both the device and corkscrew areremoved as one unit to recanalize the artery acutely.This device was tested for safety and early efficacy inthe MERCI trial, a single-arm, multicenter trial ofthrombectomy in patients with LVO treated within

J A C C V O L . 6 7 , N O . 2 2 , 2 0 1 6 Khandelwal et al.J U N E 7 , 2 0 1 6 : 2 6 3 1 – 4 4 Acute Ischemic Stroke Intervention
2633
8 h of symptom onset. Successful recanalization wasdefined as achieving Thrombolysis In MyocardialInfarction (TIMI) grade 2 or 3 flow in the target artery.The device achieved a recanalization rate of 46%,against a recanalization rate of 18% (p < 0.001) seenin historical control subjects in PROACT. A goodneurological outcome was achieved in 27.7% of pa-tients, a relatively low rate compared with the 60%rate seen in the PROACT II trial. This led to FDAapproval of the MERCI device in August 2004, thefirst mechanical thrombectomy device approved fortreatment of occluded intracranial arteries. The MultiMERCI trial ensued with the second-generation de-vice and expanded on the MERCI trial results,demonstrating a recanalization rate of 57% with MTonly and 69% if used in conjunction with IA-rtPA. Therate of FIO was 36%, a slight improvement over theMERCI trial result. The rate of symptomatic intracra-nial hemorrhage (sICH) was 7.8% in MERCI and 9.8%in Multi MERCI subjects, respectively (16,17). Apooled analysis of both studies concluded that finalrecanalization status represents the strongest pre-dictor of independent clinical outcome at 90 days inpatients undergoing thrombectomy (18).
Another mechanical thrombectomy device forstroke that works by thromboaspiration in occludedintracranial vessels was also developed. The Penum-bra stroke trial was a single-arm, multicenter, phase IIstudy. The trial enrolled 125 patients with NationalInstitutes of Health Stroke Scale (NIHSS) scores of 8or more, presenting within 8 h of symptom onset andwith angiographic occlusion (TIMI 0 to 1) of a treat-able LVO. The study demonstrated successful recan-alization (TIMI grade 2 or 3) in 81.6% of target vessels.This led to FDA approval of the Penumbra Strokesystem in January 2008. Again, the rate of FIO waslow (25%) in this study, and the rate of sICH was11.2% (19).
The MERCI and Penumbra devices were break-throughs in the field of mechanical thrombectomy,with recanalization rates higher than those seen inthe PROACT trials for IA thrombolysis and withacceptable safety. However, the clinical results ofthese trials demonstrated relatively low rates of goodneurological outcomes.
RANDOMIZED TRIALS WITH
FIRST-GENERATION DEVICES
To demonstrate functional benefit of MT/IA-rtPA plusstandard medical management over standard medicalmanagement alone, several RCTs were conducted,including the MR RESCUE (Mechanical Retrieval andRecanalization of Stroke Clots Using Embolectomy),
the IMS (Interventional Management of Stroke) III,and the SYNTHESIS EXP (Intra-arterial vs. SystemicThrombolysis for Acute Ischemic Stroke) trials. TheIMS III trial was an international RCT comparingstandard-dose IV-rtPA with a combination of low-dose IV- and IA-rtPA or mechanical thrombectomy(20). Patients presenting with AIS within 3 h wererandomized to receive either a full dose of IV-rtPA orto stop IV-rtPA after 40 min and proceed to endo-vascular treatment. No pre-procedure vascular imag-ing was required before enrolling patients for thestudy, which led to 89 (21%) patients enrolled in theendovascular arm without LVO. The first-generationMERCI device was the only FDA-approved device atthe time of the study, and was used in the majority ofpatients. Although the Solitaire stent retrieverbecame available at a later phase of the study, it wasused in a minority of patients. In 2012, the study wasstopped due to futility after enrolling 656 patientsover 6 years and showing no significant difference inlong-term functional outcome between groups: FIO at90 days was 40.8% for mechanical thrombectomywith IV-rtPA versus 38.7% for IV-rtPA alone; absolutedifference, 1.5% (95% confidence interval [CI]: 6.1% to9.1%) (20).
Similar neutral results were seen in the SYNTHESISEXP trial, conducted in Europe. SYNTHESIS EXPrandomized patients into IV-rtPA or endovasculararms (MT with or without IA thrombolysis) (21).Vascular imaging was not mandatory to randomizepatients in the endovascular arm, similar to IMS III.Second-generation devices were used in only 13% ofpatients undergoing endovascular treatment. Nofunctional benefit of endovascular therapy wasobserved in this trial (30.4% for endovascular therapyvs. 34.8% for IV-rtPA therapy; p ¼ 0.37) (20,21).
The MR RESCUE trial was an RCT of first-generation device MT in the anterior circulation inpatients randomized by magnetic resonance imaging(MRI) perfusion imaging, in addition to randomiza-tion of embolectomy versus medical therapy (22).Among 118 patients enrolled with moderately severestroke up to 5.5 h from onset, there were no signifi-cant differences between the MT and medical therapygroups (FIO at 90 days, 18.75% vs. 20%), regardless ofrecanalization status. There was also no significantbenefit with MT seen in either of the subgroups withpenumbral versus nonpenumbral patterns. Similar toIMS-III and SYNTHESIS EXP, sICH rates were low, at4% and 3% in the endovascular and medical therapyarms, respectively.
Thus, the 3 trials using mainly first-generation MTdevices and done within acute stroke systems of carebetween 2004 and 2012 did not show functional

FIGURE 1 Mechani
(A) Clot engagemen
(clot extraction) from
from Medtronic, Irvin
(B) Solitaire FR stent
Image from Medtron
with closed-cell sten
Mountain View, Calif
Khandelwal et al. J A C C V O L . 6 7 , N O . 2 2 , 2 0 1 6
Acute Ischemic Stroke Intervention J U N E 7 , 2 0 1 6 : 2 6 3 1 – 4 4
2634
benefit in treatment of moderate to severe AIS. All ofthe trials discussed in the preceding text were pub-lished in 2013 and raised serious concerns about theefficacy of acute endovascular reperfusion in LVO.However, there were 2 reasons to continue with newstudies of MT: 1) in 2012, 2 phase 2b studies of 2second-generation devices, thrombus retrievers witha stent design, called stent retrievers, showed sig-nificant superiority over first-generation devices inachieving recanalization as well as improved func-tional outcomes (23,24); and 2) a post hoc analysisfrom IMS-3 showed significant functional benefit inthe subgroup of patients with proven LVO whencomputed tomography angiography (CTA) was per-formed prior to endovascular therapy compared withIV-rtPA alone (25).
MAJOR PROGRESS WITH STENT RETRIEVERS
MECHANISM OF THE STENT RETRIEVERS. Stentretrievers were formerly designed for purpose ofstent-assisted coiling and for retracting errant coilsdislodged during endovascular procedures (26). Soon,it was realized that these devices are also very effective
sm of Thrombectomy With Stent Retrievers and Device Design
t and retrieval with stent retriever. Mechanical thrombectomy
large intracranial vessel, with help of Solitaire stent retriever. Image
g California, with permission. (B and C) Design of stent retrievers.
retriever device, with parametric overlapping design for clot removal.
ic, Irving, California, with permission. (C) Trevo stent retriever,
t-like design for clot retrieval. Image from Stryker Neurovascular,
ornia, with permission.
in capturing naturally occurring thrombus and couldhave a major effect on early vessel recanalization. Themost recent generation of these devices is a novel formof clot retrievers, commonly known as stent retrievers.These are self-expanding stents that are deliveredacross the thrombus with the help of a microcatheter.Their design, with multiple crisscrossing struts, en-sures capture of the thrombus within the stent wall,followed by withdrawal of the then-unfolded stentinto the guide catheter under constant aspiration. Af-ter the clot is removed from the vessel, flow in thevessel is immediately restored (Figure 1A).
STENT RETRIEVER PHASE 2 TRIALS. The SWIFT(Solitaire Flow Restoration Device Versus the MerciRetriever in Patients With Acute Ischemic Stroke) andTREVO 2 (Trevo Versus Merci Retrievers for Throm-bectomy Revascularization of LVO in Acute IschemicStroke) phase 2 studies showed stent retrievers(Figure 1B and C) to have better reperfusion and goodneurological outcomes at 90 days compared with thefirst-generation Merci Retrieval System (23,24). TheSWIFT study enrolled eligible patients to undergoMT either by stent retriever (n ¼ 58) or MERCI device(n ¼ 55). The primary outcome of a TIMI score of 2 or 3was greater among the Solitaire group compared withthe MERCI group (61% vs. 24%; p < 0.0001). Good FIOwas also seen more frequently in the Solitaire groupthan in the MERCI group (58% vs. 33%; p < 0.0001).Similar results were found in the TREVO trial, whichenrolled patients to undergo MT, either by Trevodevice (stent retriever) or by MERCI device. The pri-mary outcome was defined as a TICI (Thrombolysisin Cerebral Infarction) score (explained later in thesection “Comparison of Past and Present Trials:Key Factors That Made the Difference”) of $2,and was seen in 76 (86%) patients in the Trevogroup compared with 54 (60%) in the Merci group(p < 0.0001). Compared with the Merci group, morepatients in the Trevo group had good long-term FIO(40% vs. 22%; p < 0.013). Incidence of the primarysafety endpoint (sICH or other complications) didnot differ between groups (23,24).
STENT RETRIEVER PHASE 3 TRIALS. In late 2014 andearly 2015, the results of 5 RCTs were published inquick succession, all showing clear superiority of MTdone with second-generation devices in combinationwith IV-rtPA (a minority of patients received only MT)compared with IV-rtPA alone. Figure 2 demonstratescomplete restoration of blood flow after MT using astent retriever in a young patient with MCA occlusion.
MR CLEAN (Multicenter Randomized Clinical Trialof Endovascular Treatment for Acute Ischemic Strokein the Netherlands) randomized acute stroke patients

FIGURE 2 Acute Ischemic Stroke Patient With Large Vessel Occlusion Undergoing Mechanical Thrombectomy
(A) Digital subtraction angiograms (DSAs) showing no opacification of the right middle cerebral artery (MCA) due to clot in the M1 segment of
the artery in the anterior posterior (AP) plane. (B) Unsubstracted AP image showing stent retriever placement in the occluded portion of the
artery through the microcatheter. (C and D) DSA showing complete opacification of the right MCA artery in AP and lateral planes after removal
of the clot. (Thrombolysis in Cerebral Infarction score 3).
J A C C V O L . 6 7 , N O . 2 2 , 2 0 1 6 Khandelwal et al.J U N E 7 , 2 0 1 6 : 2 6 3 1 – 4 4 Acute Ischemic Stroke Intervention
2635
presenting within 6 h of stroke onset to standardmedical management alone (n ¼ 267) or standardmedical management followed by MT (n ¼ 233) (27).Noninvasive vascular imaging before enrolling a pa-tient into MT was mandatory, and as long as therewas clear vessel occlusion, a wide range of NIHSS(0 to 42, where higher numbers indicate severeneurological deficit) was allowed. Patients with AISwho were older than 18 years of age and with anteriorcirculation LVO confirmed on noninvasive vascularimaging were eligible to be enrolled in the trial.Contrary to first- and second-generation trials, whichdid not include patients over 80 years of age, MRCLEAN had no cutoff on the upper age limit. Theauthors did report the rate of FIO in relation to theAlberta Stroke Program Early CT score (ASPECTS);
however, ASPECTS was not used for randomization ofpatients. To avoid selection bias, insurers in theNetherlands did not reimburse the procedure outsideof the study, a truly remarkable step not seen inprevious endovascular trials. Stent retrievers wereused in 190 of the 233 patients (81.5%) assigned to IAtreatment. Although the reperfusion rates (TICI 2b or3) were lower than expected (only 59%), good FIO wassuperior among those treated with the combination ofMT and standard medical management (32.6% vs.19.1%; odds ratio: 1.67 [95% CI: 1.21 to 2.30]). Therewere no significant differences in mortality or occur-rence of sICH (27).
In light of the MR CLEAN results, the ESCAPE(Endovascular Treatment for Small Core and AnteriorCirculation Proximal Occlusion With Emphasis on

Khandelwal et al. J A C C V O L . 6 7 , N O . 2 2 , 2 0 1 6
Acute Ischemic Stroke Intervention J U N E 7 , 2 0 1 6 : 2 6 3 1 – 4 4
2636
Minimizing CT to Recanalization Times) trial wasstopped early for the first interim analysis. TheESCAPE trial had several unique protocol features. Itencouraged the use of CTA (preferably multiphaseCTA for better estimation of collateral blood supply)and discouraged use of MRI. ESCAPE focused onimproving workflow in enrolling hospitals and setambitious goals of door-to-puncture times <60 minand door-to-recanalization times <90 min. The firstinterim analysis, with 315 patients enrolled, showed arate of FIO in 53% of the MT patients versus 29% withstandard therapy (p < 0.001). Good reperfusion (TICI2b or 3) was achieved in 72% of patients. Interventionwas associated with reduction in mortality of 10%(MT) versus 19% in the control group, and rates ofsICH were similar in both groups (3.6% MT vs. 2.7%control) (28).
SWIFT PRIME (Solitaire with the Intention forThrombectomy as Primary Endovascular Treatment)was the next trial stopped by the data safety moni-toring board after interim analysis (29). The trialenrolled 196 patients between 2012 and 2014. Thisstudy randomized patients who were between 18 and80 years of age, had NIHSS scores between 8 and 30,and had pre-stroke mRS <1 into intervention andcontrol groups. Noninvasive vascular imaging toidentify LVO was mandatory before randomization.Enrolling centers were encouraged to use RAPID, anoperator-independent image post-processing systemsoftware for target-mismatch penumbral profile(Figure 3); however, it was not mandatory for patientrandomization. A desirable rate of reperfusion (TICI2b or 3) was achieved in 73 of 83 (88%) patients. Therate of FIO at 90 days was higher in the MT group thanin the control group (60% vs. 35%; p < 0.001). Theefficacy of MT was better than in the MR CLEAN trial(60% vs. 32%) and comparable to the ESCAPE trial(60% vs. 53%). There were no significant between-group differences in 90-day mortality (9% vs. 12%;p ¼ 0.50) or sICH (0% vs. 3%; p ¼ 0.12) (29).
EXTEND-IA (Extending the Time for Thrombolysisin Emergency Neurological Deficits—Intra-Arterial)was an Australian trial that required mandatorycomputed tomography (CT) perfusion imaging withpost-processing by standardized software (RAPID) torandomize patients with a favorable penumbralmismatch pattern to IV-rtPA alone versus IV-rtPAplus MT (30). This trial had some unique inclusioncriteria. For example, there were no restrictions onage or clinical severity, as assessed by the NIHSSscore; however, like SWIFT PRIME, it requiredIV-rtPA to be given to patients within 4.5 h and MT tobe started within 6 h of symptom onset. Similar to allthe new trials, noninvasive vascular imaging to
identify LVO in the anterior circulation was manda-tory. A pre-treatment mRS score of 0 to 2 wasrequired to be eligible for randomization. The trialwas stopped after enrolling 35 patients in each group.It showed vastly superior functional outcomes in theMT plus IV-rtPA arm of 70% versus 40% in the controlgroup (p ¼ 0.001). No significant difference was notedin the rates of sICH or mortality between the 2 groups(30). Figure 4 demonstrates the result from meta-analysis of all trials of endovascular therapy versusstandard therapy for the outcome of proportionaltreatment benefit (31).
REVASCAT (Randomized Trial of Revascularizationwith Solitaire FR Device versus Best Medical Therapyin the Treatment of Acute Stroke Due to AnteriorCirculation LVO Presenting within Eight Hours ofSymptom Onset) was conducted primarily in Spainand enrolled patients within 8 h after symptom onset(32). REVASCAT randomly assigned 206 patients in a1:1 ratio to receive either medical therapy (includingIV-rtPA when eligible) and MT treatment with theSolitaire stent retriever or medical therapy alone.Eligible patients were between 18 and 80 years of age,had an occlusion in the anterior circulation confirmedby noninvasive vascular imaging, had an NIHSS >6,and had a pre-treatment mRS score #1. The mainexclusion criteria were ASPECTS <7 on CT scan or <6on diffusion-weighted imaging on MRI. Afterenrolling 160 patients, study inclusion criteria weremodified to restrict age to <85 years and ASPECTS to>8 on CT scan. The primary outcome of functionalindependence at 3 months was more frequent in theintervention group (43.7% vs. 28.2%; odds ratio: 2.1;95% CI: 1.1 to 4.0). The rates of sICH were similar(1.9%) in both groups, and rates of mortality were18.4% and 15.5%, respectively (p ¼ 0.06) (32). Table 2summarizes the results of these most recent RCTs.
COMPARISON OF FIRST GENERATION
AND CURRENT ENDOVASCULAR TRIALS:
KEY FACTORS THAT MADE THE DIFFERENCE
CT NEUROIMAGING IN PATIENT SELECTION. A non-contrast brain CT scan is often the initial imagingperformed to exclude patients presenting with intra-cranial hemorrhages. In addition to detecting hem-orrhage, CT scans can be useful to detect earlyischemic changes. ASPECTS is a 10-point scoringsystem that reliably predicts the extent of earlyischemic changes from CT scans (33). Multiple studieshave shown that patients with pre-treatmentASPECTS of 7 or more have better outcomes (34,35).Earlier RCTs using first-generation devices did notadequately assess the extent of early ischemic
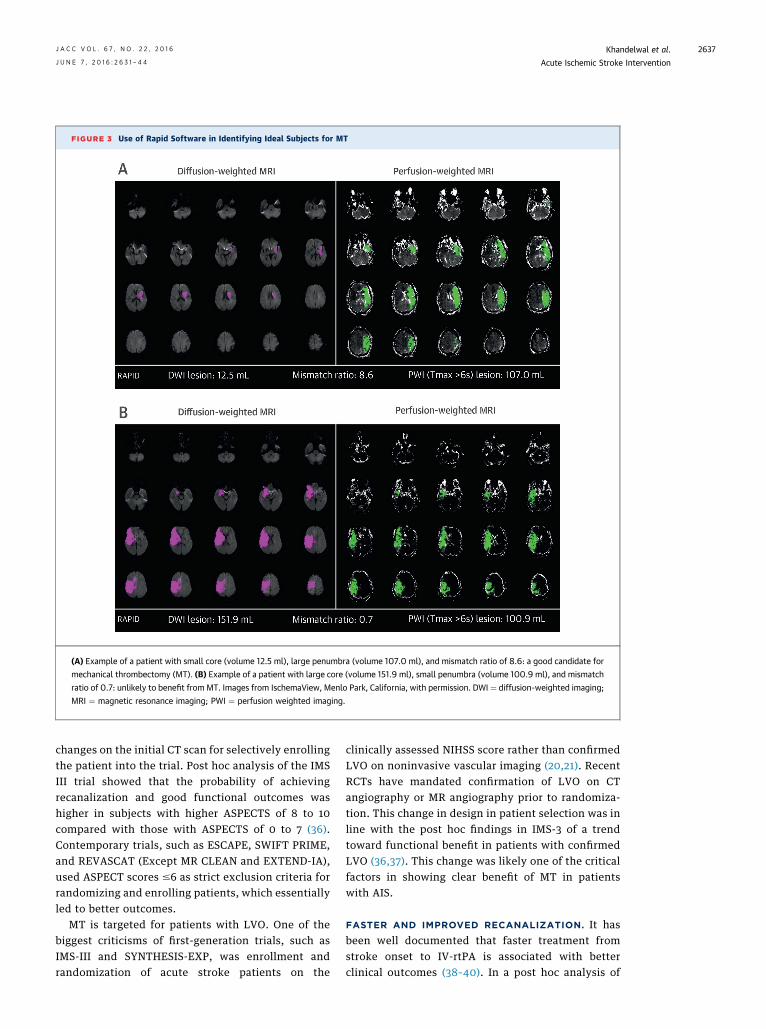
FIGURE 3 Use of Rapid Software in Identifying Ideal Subjects for MT
(A) Example of a patient with small core (volume 12.5 ml), large penumbra (volume 107.0 ml), and mismatch ratio of 8.6: a good candidate for
mechanical thrombectomy (MT). (B) Example of a patient with large core (volume 151.9 ml), small penumbra (volume 100.9 ml), and mismatch
ratio of 0.7: unlikely to benefit from MT. Images from IschemaView, Menlo Park, California, with permission. DWI ¼ diffusion-weighted imaging;
MRI ¼ magnetic resonance imaging; PWI ¼ perfusion weighted imaging.
J A C C V O L . 6 7 , N O . 2 2 , 2 0 1 6 Khandelwal et al.J U N E 7 , 2 0 1 6 : 2 6 3 1 – 4 4 Acute Ischemic Stroke Intervention
2637
changes on the initial CT scan for selectively enrollingthe patient into the trial. Post hoc analysis of the IMSIII trial showed that the probability of achievingrecanalization and good functional outcomes washigher in subjects with higher ASPECTS of 8 to 10compared with those with ASPECTS of 0 to 7 (36).Contemporary trials, such as ESCAPE, SWIFT PRIME,and REVASCAT (Except MR CLEAN and EXTEND-IA),used ASPECT scores #6 as strict exclusion criteria forrandomizing and enrolling patients, which essentiallyled to better outcomes.
MT is targeted for patients with LVO. One of thebiggest criticisms of first-generation trials, such asIMS-III and SYNTHESIS-EXP, was enrollment andrandomization of acute stroke patients on the
clinically assessed NIHSS score rather than confirmedLVO on noninvasive vascular imaging (20,21). RecentRCTs have mandated confirmation of LVO on CTangiography or MR angiography prior to randomiza-tion. This change in design in patient selection was inline with the post hoc findings in IMS-3 of a trendtoward functional benefit in patients with confirmedLVO (36,37). This change was likely one of the criticalfactors in showing clear benefit of MT in patientswith AIS.
FASTER AND IMPROVED RECANALIZATION. It hasbeen well documented that faster treatment fromstroke onset to IV-rtPA is associated with betterclinical outcomes (38–40). In a post hoc analysis of

FIGURE 4 Forest Plot Assessment of Pre-Defined Subgroups From the 4 Recent Major
Endovascular Trials
Controln=386
191192328
55
191193
15515076
16314986
206195
21218932774
Age<70y≥70y<80y≥80y
2.45 (1.68, 3.56) 0.393.16 (2.05, 4.86)2.57 (1.90, 3.50) 0.173.46 (1.58, 7.60)
2.56 (1.76, 3.72) 0.912.80 (1.91, 4.11)
2.84 (1.85, 4.38) 0.723.05 (1.97, 4.73)3.25 (1.66, 6.35)
5.23 (2.60, 10.53) 0.182.41 (1.77, 3.28)1.77 (0.55, 5.65)
4.38 (1.82, 10.52) 0.482.53 (1.91, 3.36)
0.86 (0.23, 3.18) 0.072.53 (1.65, 3.86)3.07 (2.12, 4.47)
2.50 (1.87, 3.35) 0.683.30 (1.65, 6.63)
2.76 (2.05, 3.72) 0.472.00 (1.04, 3.84)
SexFemaleMale
NIHSS0-1516-20>20
ICAM1 MCAM2 MCA
66287
23
41345
31152197
32759
30875
32675
.1 1Favorscontrol
FavorsIntervention
2 10
32378
22161
205
43358
73285
33
n=401 (95% CI) P-value Intervention Odds Ratio Interaction
Site of Vessel Occlusion
Tandem Occlusion
ASPECTS
IV Thrombolysis
Onset to Randomization Time
TandemNo Tendem
0-56-89-10
AlteplaseNo Alteplase
<5h>5h
Treatment effect in pre-defined subgroups from the 4 recent endovascular trials
(SWIFT PRIME [Solitaire with the Intention for Thrombectomy as Primary Endovascular
Treatment], ESCAPE [Endovascular Treatment for Small Core and Anterior Circulation
Proximal Occlusion With Emphasis on Minimizing CT to Recanalization Times], EXTEND-IA
[Extending the Time for Thrombolysis in Emergency Neurological Deficits—Intra-Arterial],
REVASCAT [Randomized Trial of Revascularization with Solitaire FR Device versus Best
Medical Therapy in the Treatment of Acute Stroke Due to Anterior Circulation LVO
Presenting within Eight Hours of Symptom Onset]), adjusted for age, sex, baseline stroke
severity, site of occlusion, intravenous alteplase treatment, carotid occlusion, Alberta
Stroke Program CT Score, and time from onset to treatment to randomization. Reprinted
with permission from Campbell et al. (31). ASPECTS ¼ Alberta Stroke Program Early CT
Score; CI ¼ confidence interval; ICA ¼ internal carotid artery; MCA ¼ middle cerebral
artery; NIHSS ¼ National Institute of Health Stroke Scale.
Khandelwal et al. J A C C V O L . 6 7 , N O . 2 2 , 2 0 1 6
Acute Ischemic Stroke Intervention J U N E 7 , 2 0 1 6 : 2 6 3 1 – 4 4
2638
the pooled IMS pilot trials, the relative probability ofa good outcome declined by 12% to 15% for every30-min delay in recanalization (41,42). Moreover,post hoc analysis of the STAR (Solitaire FR Throm-bectomy for Acute Revascularization) trial showedthat faster recanalization results in better outcomes
(43). The mean time from symptom onset to IA in theMR-RESCUE study was 381 min. In SYNTHESIS EXPand IMS III, the median times from symptom onset tostart of endovascular treatment were 225 and 240min, respectively, indicating significant time delays.Learning from the time delays in previous trials,the recent endovascular trials all emphasized theimportance of faster door-to-recanalization times.Of all recent trials, ESCAPE stands out for itsrapid workflow design. The ESCAPE trial achievedremarkably short door-to-puncture times of <60 min,which eventually led to better outcomes (FIO of 52%patients in the intervention arm vs. 29% in theIV-rtPA arm). In comparison, MR CLEAN reported atime of 114 min to randomize patients after receivingIV-rtPA, resulting in a lower FIO of 32% amongpatients in the intervention arm. A comparison ofNNTs between the 5 trials and the IMS-III trial isshown in Table 3.
Another significant difference in the recent trialswas the tremendously improved rate of substantialrecanalization, primarily through the use of stentretriever devices. Angiographic recanalization ismeasured by the TICI scale, which ranges from 0 (noperfusion) to 2a (<50% reperfusion of target vessel),2b (>50% reperfusion of target vessel), and 3 (fullperfusion of target vessel), which is a modification ofa previously simplified version of the TICI 0 or 1, 2,3, scoring system (adapted from the cardiologyTIMI scoring system) (44). The rates of substantialrecanalization (TICI 2b or above) of individual ves-sels noted in IMS III were 38% for an occlusion inthe internal carotid artery, 44% for an occlusion inM1, and 44% for an occlusion in M2. A furtheranalysis of IMS III reported the proportion of pa-tients with mRS scores 0 to 2 at 90 days was: 12.7%with TICI 0; 27.6% with TICI 1; 34.3% with TICI 2a;47.9% with TICI 2b; and 71.4% with TICI 3; thesescores clearly indicate the role of recanalizationin improving outcomes (42). MR RESCUE reportedsubstantial recanalization in only 27% of subjects,whereas the rate of recanalization was not reportedby SYNTHESIS-EXP. In comparison, the rates of sub-stantial recanalization noted in recent studies were:MR CLEAN 58%, ESCAPE 72%, SWIFT PRIME 88%,EXTEND IA 94%, and REVASCAT 66%, showingremarkable improvement over previous studies.Figure 5 shows comparison among workflow times,rates of substantial reperfusion, and co-relation toNNT in recent trials.
ROLE OF PERFUSION-WEIGHTED IMAGING. Theischemic penumbra is an area of the brain withreversible ischemia, whereas the core represents
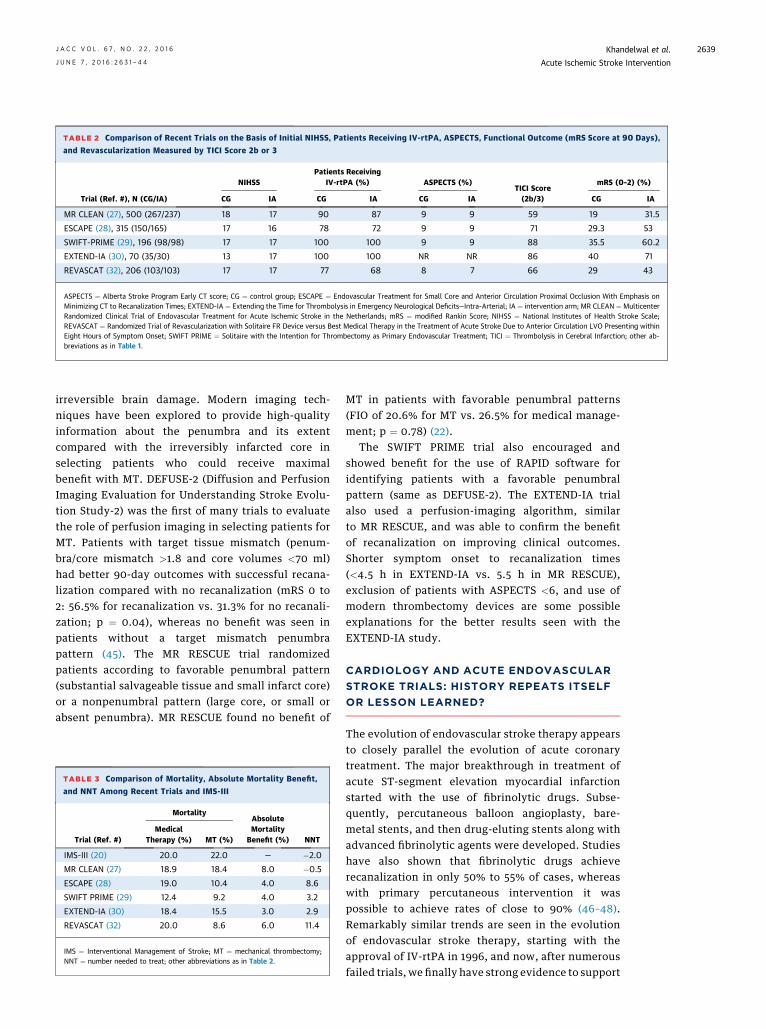
TABLE 2 Comparison of Recent Trials on the Basis of Initial NIHSS, Patients Receiving IV-rtPA, ASPECTS, Functional Outcome (mRS Score at 90 Days),
and Revascularization Measured by TICI Score 2b or 3
Trial (Ref. #), N (CG/IA)
NIHSSPatients Receiving
IV-rtPA (%) ASPECTS (%)TICI Score(2b/3)
mRS (0–2) (%)
CG IA CG IA CG IA CG IA
MR CLEAN (27), 500 (267/237) 18 17 90 87 9 9 59 19 31.5
ESCAPE (28), 315 (150/165) 17 16 78 72 9 9 71 29.3 53
SWIFT-PRIME (29), 196 (98/98) 17 17 100 100 9 9 88 35.5 60.2
EXTEND-IA (30), 70 (35/30) 13 17 100 100 NR NR 86 40 71
REVASCAT (32), 206 (103/103) 17 17 77 68 8 7 66 29 43
ASPECTS ¼ Alberta Stroke Program Early CT score; CG ¼ control group; ESCAPE ¼ Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion With Emphasis onMinimizing CT to Recanalization Times; EXTEND-IA ¼ Extending the Time for Thrombolysis in Emergency Neurological Deficits—Intra-Arterial; IA ¼ intervention arm; MR CLEAN ¼ MulticenterRandomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands; mRS ¼ modified Rankin Score; NIHSS ¼ National Institutes of Health Stroke Scale;REVASCAT ¼ Randomized Trial of Revascularization with Solitaire FR Device versus Best Medical Therapy in the Treatment of Acute Stroke Due to Anterior Circulation LVO Presenting withinEight Hours of Symptom Onset; SWIFT PRIME ¼ Solitaire with the Intention for Thrombectomy as Primary Endovascular Treatment; TICI ¼ Thrombolysis in Cerebral Infarction; other ab-breviations as in Table 1.
J A C C V O L . 6 7 , N O . 2 2 , 2 0 1 6 Khandelwal et al.J U N E 7 , 2 0 1 6 : 2 6 3 1 – 4 4 Acute Ischemic Stroke Intervention
2639
irreversible brain damage. Modern imaging tech-niques have been explored to provide high-qualityinformation about the penumbra and its extentcompared with the irreversibly infarcted core inselecting patients who could receive maximalbenefit with MT. DEFUSE-2 (Diffusion and PerfusionImaging Evaluation for Understanding Stroke Evolu-tion Study-2) was the first of many trials to evaluatethe role of perfusion imaging in selecting patients forMT. Patients with target tissue mismatch (penum-bra/core mismatch >1.8 and core volumes <70 ml)had better 90-day outcomes with successful recana-lization compared with no recanalization (mRS 0 to2: 56.5% for recanalization vs. 31.3% for no recanali-zation; p ¼ 0.04), whereas no benefit was seen inpatients without a target mismatch penumbrapattern (45). The MR RESCUE trial randomizedpatients according to favorable penumbral pattern(substantial salvageable tissue and small infarct core)or a nonpenumbral pattern (large core, or small orabsent penumbra). MR RESCUE found no benefit of
TABLE 3 Comparison of Mortality, Absolute Mortality Benefit,
and NNT Among Recent Trials and IMS-III
Trial (Ref. #)
MortalityAbsoluteMortality
Benefit (%) NNTMedical
Therapy (%) MT (%)
IMS-III (20) 20.0 22.0 — �2.0
MR CLEAN (27) 18.9 18.4 8.0 �0.5
ESCAPE (28) 19.0 10.4 4.0 8.6
SWIFT PRIME (29) 12.4 9.2 4.0 3.2
EXTEND-IA (30) 18.4 15.5 3.0 2.9
REVASCAT (32) 20.0 8.6 6.0 11.4
IMS ¼ Interventional Management of Stroke; MT ¼ mechanical thrombectomy;NNT ¼ number needed to treat; other abbreviations as in Table 2.
MT in patients with favorable penumbral patterns(FIO of 20.6% for MT vs. 26.5% for medical manage-ment; p ¼ 0.78) (22).
The SWIFT PRIME trial also encouraged andshowed benefit for the use of RAPID software foridentifying patients with a favorable penumbralpattern (same as DEFUSE-2). The EXTEND-IA trialalso used a perfusion-imaging algorithm, similarto MR RESCUE, and was able to confirm the benefitof recanalization on improving clinical outcomes.Shorter symptom onset to recanalization times(<4.5 h in EXTEND-IA vs. 5.5 h in MR RESCUE),exclusion of patients with ASPECTS <6, and use ofmodern thrombectomy devices are some possibleexplanations for the better results seen with theEXTEND-IA study.
CARDIOLOGY AND ACUTE ENDOVASCULAR
STROKE TRIALS: HISTORY REPEATS ITSELF
OR LESSON LEARNED?
The evolution of endovascular stroke therapy appearsto closely parallel the evolution of acute coronarytreatment. The major breakthrough in treatment ofacute ST-segment elevation myocardial infarctionstarted with the use of fibrinolytic drugs. Subse-quently, percutaneous balloon angioplasty, bare-metal stents, and then drug-eluting stents along withadvanced fibrinolytic agents were developed. Studieshave also shown that fibrinolytic drugs achieverecanalization in only 50% to 55% of cases, whereaswith primary percutaneous intervention it waspossible to achieve rates of close to 90% (46–48).Remarkably similar trends are seen in the evolutionof endovascular stroke therapy, starting with theapproval of IV-rtPA in 1996, and now, after numerousfailed trials, we finally have strong evidence to support

FIGURE 5 Time to Intervention, TICI 2b/3 Rate, and NNT
7.0
6.0
5.0
4.0
3.0
2.0
1.0
0.0
IMS-3
MR Rescue
REVASCAT
ESCAPE
MR CLEAN
EXTEND IA
SWIFT-PIM
S-3
MR Rescue
MR CLEAN
ESCAPE
EXTEND IA
SWIFT-P
REVASCAT
IMS-3
MR Rescue
REVASCAT
ESCAPE
MR CLEAN
EXTEND IASWIFT
IMS-3
MR Rescue
MR CLEAN
ESCAPE
EXTEND IA
SWIFT-P
REVASCAT
1009080706050403020100
987654321
0
987654321
0
Onset to IA
Onet to Reperfusion
NNT
TICI 2b/3
NNT
A B
(A) Relationship between onset to intra-arterial therapy/reperfusion and NNT in patients undergoing EVT among second- and third-generation
endovascular trials. The NNT to have good outcome decreases with rapid treatment times. (B) Relationship between good reperfusion (TICI 2b)
score and NNT among second- and third-generation trials. IA ¼ intra-arterial; IMS ¼ Interventional Management of Stroke; MR CLEAN ¼Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands; MR RESCUE ¼ Mechanical
Retrieval and Recanalization of Stroke Clots Using Embolectomy; NNT ¼ number needed to treat; TICI ¼ Thrombolysis In Cerebral Infarction;
other abbreviations as in Figure 4.
TABLE 4 Summary of Updated (June 2015) AHA Guidelines for Patients Undergoing MT
Indication Recommendation Level of Evidence
Eligible patients should receive IV-rtPA, even if IAT is considered. Class I A
Patient presenting within 0–6 h of symptom onset, mRS 0–1, age >18 years, NIHSS >6, ASPECTS >6, with provenocclusion of internal carotid artery or proximal middle cerebral artery (M1), should receive IAT with stent retriever.
Class I A
Aim of the revascularization procedure should be to receive a TICI 2b/3 score as early as possible. Class I B
In selected patients with anterior circulation stroke who have contraindication to IV-rtPA, it is reasonable to performIAT with stent retrievers. IAT with stent retrievers may be useful for certain patients with occlusion of M2, M3,(distal MCA), anterior cerebral artery, or vertebral artery, if treatment can be initiated within 6 h.
Class II C
Observing patients after IV-rtPA to assess for clinical response before pursuing IAT is not required to achievebeneficial outcomes and is not recommended.
Class III B
Emergent imaging of brain, preferably CT scan, should be obtained before beginning any specific treatment for AIS. Class I A
If IAT is considered, then nonvascular imaging (CTA or MRA) should be performed to confirm vascular obstruction;however, IV-rtPA administration should not be delayed.
Class I A
Benefit of additional imaging beyond CT, CTA, or MRA, such as perfusion imaging with CT or MRI, is unknown. Class IIb C
Patient should be transferred to the nearest certified primary stroke or comprehensive stroke center. Class I A
A regional system of stroke care, including health care facilities to provide initial emergent treatment, a primarystroke center, and comprehensive centers capable of performing IAT, should be developed.
Class I A
Data from Powers et al. (7).
AHA ¼ American Heart Association; CTA ¼ computed tomography angiography; IAT ¼ intra-arterial thrombolysis; MRA ¼ magnetic resonance angiography; MRI ¼ magnetic resonanceimaging; other abbreviations as in Tables 1 to 3.
Khandelwal et al. J A C C V O L . 6 7 , N O . 2 2 , 2 0 1 6
Acute Ischemic Stroke Intervention J U N E 7 , 2 0 1 6 : 2 6 3 1 – 4 4
2640

CENTRAL ILLUSTRATION New Standard-of-Care in AcuteIschemic Stroke Intervention: Mechanical Thrombectomy WithIV-rtPA for LVO Ischemic Stroke
NY
NY
NY
Acute stroke
Large vessel occlusion(LVO) 20%
IV-tPA
Intensive care unit/stroke unitwith standard medical treatment
Mechanicalthrombectomy
Non-LVO80%
Hemorrhagic15%
Ischemic85%
Symptom onset0-3/4.5 hours?
Contraindicationsto tissue
plasminogenactivator (IV-tPA)
LVO?
Symptom onset 0–6 hoursAspect score >6
National institute of healthstroke scale > 6
on non invasive imaging
Khandelwal, P. et al. J Am Coll Cardiol. 2016;67(22):2631–44.
The algorithm shows the application of mechanical thrombectomy in addition to IV-rtPA
as the new standard-of-care treatment approach to patients with acute ischemic stroke
who have a large cerebral artery occlusion within 6 h of symptom onset with a favorable
imaging on brain computed tomography. LVO ¼ large vessel occlusion; NIHSS ¼ National
Institutes of Health Stroke Scale; Non LVO ¼ no large vessel occlusion.
J A C C V O L . 6 7 , N O . 2 2 , 2 0 1 6 Khandelwal et al.J U N E 7 , 2 0 1 6 : 2 6 3 1 – 4 4 Acute Ischemic Stroke Intervention
2641
the superiority of endovascular therapy comparedwith fibrinolytic therapy alone. Moreover, the field ofacute coronary intervention has evolved tremen-dously. In addition to the development of new drugsand percutaneous coronary intervention techniques, itwas soon acknowledged that faster door-to-perfusiontimes led to better outcomes, leading to initiativessuch as door-to-balloon time (49). A study reviewedthe effect of these initiatives and noted that door-to-balloon times have decreased nationally from a me-dian of 96 min in 2005 to 64 min in 2010 (50). Theimpressive results in shortening the time tomyocardialreperfusion for acute MI obtained through such ini-tiatives provided the inspiration for launching projectslike Target Stroke. Target Stroke is a national initiativeorganized by the AHA/American Stroke Association inpartnership with other organizations, and aims toassist hospitals in increasing the proportion of IV-rtPA–treated patients in whom guideline-recommendeddoor-to-needle times are achieved. The initial goalis to achieve a door-to-needle time of no more than60 min for at least 50% of patients with AIS (51). Morerecently, the new Target Stroke goal has been revisedto achieve a door-to-needle time of 45 min. We nowhave the evidence needed to support MT; however,the implementation of endovascular stroke practicehas yet to achieve the level of refinement seen in thetreatment of acute coronary syndrome.
LIMITATIONS OF CURRENT
ENDOVASCULAR TRIALS
The 5 recent randomized trials prove the consistentbenefit of endovascular therapy plus IV-rtPA overstandard medical management alone; however, therecent trials are not without limitations. For examplethe EXTEND-IA screen to enrollment ratio was 100:1(70 patients were enrolled after screening 7,000 pa-tients), and ESCAPE recruited only 1.44 patients/month/center. Hence, the primary message, whichreverberates across all trials, is that limited numbersof patients will benefit from intervention, and clini-cians must be selective when choosing patients forendovascular therapy. Moreover, centers partici-pating in the trials were high-volume centers withvery experienced neurointerventionalists. Thesecenters also had streamlined workflow protocols forrapid triage of the stroke patients (ESCAPE and SWIFTPRIME, in particular), hasty transfer of patients fromthe primary center to tertiary centers, along withincredibly fast door-to-treatment times. This, how-ever, needs to be translated into all centers across thecountry, which may have less volume and lessexperienced house staff than the centers chosen for
the studies. Additionally, these trials differed in theeffect size of intervention, from 13% to 31%. As aresult, there has been some speculation that the 4 of5 trials that were stopped early (except MR CLEAN,the only completed study) may have overestimatedthe treatment effect. An additional prospective

Khandelwal et al. J A C C V O L . 6 7 , N O . 2 2 , 2 0 1 6
Acute Ischemic Stroke Intervention J U N E 7 , 2 0 1 6 : 2 6 3 1 – 4 4
2642
registry should be able to answer this questioneffectively.
CURRENT RECOMMENDATIONS AND
FUTURE DIRECTIONS
Due to consistent findings across multiple endo-vascular trials, in the recent (June 2015) revisionof guidelines from the AHA/American Stroke Associ-ation, Class I recommendations were made (Level ofEvidence: A) for the use of MT along with IV-rtPAtreatment for AIS for eligible patients. The guide-lines endorsed the use of IV-rtPA in combination withMT in patients with AIS of <6 h duration who had LVOconfirmed with vascular imaging, were >18 years ofage, had NIHSS score >6, and had ASPECTS >6. Theevidence for MT is less clear for patients presenting>6 h after symptom onset. The evidence for MT isalso not clear for patients with posterior circulationstrokes, as the majority of present and past trials haveexcluded these patients. Evidence of the benefit ofMT in posterior circulation stroke is from prospectiveand retrospective patient cohorts, rather than RCTs.In the future, trials focusing on posterior circulationstroke are needed to establish effective windows andtechniques for this group of patients. The guidelinesalso recommend use of stent retrievers as the first-line device; however, other devices may be useful incertain situations. Other recommendations includefaster door-to-recanalization time, the angiographicgoal of TICI 2b/3 for better clinical outcomes, anddevelopment of comprehensive stroke centerscapable of performing MT. Table 4 summarizes thecurrent updated guidelines for MT (7).
These trials certainly are landmark studies, andundoubtedly have advanced a new era in the field ofacute stroke intervention. However, we still havelong way to go. Use of MT for AIS has remained low inthe United States, ranging from 0.6% to 2% of allpatients with AIS (52,53). A recently published studyreported that only 1.6% of patients with ischemicstroke received MT, including 1.1% of patientsreceiving MT alone and 0.5% receiving both MT andIV-rtPA. By comparison, 8.0% of patients withischemic stroke in these hospitals received IV-rtPAalone, without endovascular therapy (53). Delay inarrival to the hospital is the most common reasonseen in exclusion of patients with AIS for intravenousthrombolysis, along with other contraindicationsmentioned earlier (Table 1). In contrast, exclusioncriteria for MT are less stringent, and patients aregenerally considered good candidates for MT as longas they present within 6 h from symptom onset, haveLVO on noninvasive imaging, have an NIHSS score
>5, and ASPECTS >6. Unfortunately, there are stilltoo many patients with acute stroke who do notrecognize the warning signs of stroke, call 911, andarrive quickly enough to be eligible for these thera-pies. Ongoing education of the general populationabout early recognition of stroke signs and symptomsand the need for rapid treatment is of paramountimportance. In addition, greater emphasis onimproving pre-hospital systems, rapid transport ofpatients from primary stroke centers to comprehen-sive centers, or bypass of primary stroke centerswhen there is a suspicion of a LVO should be prior-ities. There are still areas in which further research isneeded to evaluate the expanded indications for MT,including the role of MT in wake-up stroke; the use ofMT in selected patients treated beyond 6 h, particu-larly with image selection criteria; and the use ofadjunctive pharmacological therapies, such as hypo-thermia and neuroprotection.
ACCESS TO ACUTE STROKE INTERVENTION
FOR LVOs IN THE UNITED STATES
There are not yet any focused epidemiological studiesof LVO ischemic stroke qualifying for mechanicalthrombectomy. However, in 2012, Zaidat et al. (54)estimated that 4% to 14% of the total of 675,000ischemic strokes in the United States could have LVO,yielding a range of 27,000 to 97,000 patients annuallyfor whom mechanical thrombectomy would be indi-cated. Their estimate was derived by averaging thenumbers of LVOs from previous studies of strokesubtypes in the population, endovascular strokeclinical trial recruitment numbers, and local andregional registries. Of note, in their analysis, if onlythe proportion of LVO from population and epide-miology studies were used for this estimate, LVOswould be approximately 9% to 27% of the total,yielding numbers as high as 60,750 to 182,250 totalLVO patients per year in the United States.
Access to acute stroke intervention for LVO pa-tients in the United States has been evolving in thelast decade. A study estimated, using 2011 data, that56% of the U.S. population had access within 60 minby ground to endovascular stroke treatment-capablehospitals (55). Comprehensive stroke centers (CSCs)are certified stroke centers that have the resourcesand meet criteria for achieving good outcomeswith endovascular treatment of stroke (56). Recentmodeling data, with an assumption of addition of20 optimally located CSCs per state, estimate that63% of the U.S. population would have 60-minground access and 83% would have 60-min ground/air access to a CSC (57). Thus, AHA guidelines

J A C C V O L . 6 7 , N O . 2 2 , 2 0 1 6 Khandelwal et al.J U N E 7 , 2 0 1 6 : 2 6 3 1 – 4 4 Acute Ischemic Stroke Intervention
2643
recommend the current tiered system of acute strokecare with acute stroke-ready hospitals, primarystroke centers, and CSCs to ensure starting IV-rtPAwith the least possible delay after symptom onset,and rapid transfer to CSCs for mechanical thrombec-tomy for LVO patients (7). In terms of the availableworkforce for MT, using the mean estimate ofthe number of LVO cases provided previously, and1,000 fellowship-trained neurointerventionalists,there would be a wide range from 27 to 97 MT cases/year per practitioner (54). Thus, it is clear thatworkforce demand-supply for MT is in a rapid state ofevolution and more data are needed for accuratedeterminations.
CONCLUSIONS
Recent endovascular acute stroke trials have com-pellingly demonstrated the superiority of combined
treatment with MT (with stent retriever) and IV-rtPAover medical therapy alone for patients with LVOwho present within 6 h. This is a revolutionaryadvance in our ability to combat the massive disabilitythat results from stroke. The Central Illustration out-lines the overall approach to implementing this newstandard of care in clinical practice. The challengenow is to increase access to MT for acute strokepatients in the shortest time possible by building upthe stroke systems of care in the United States andworldwide.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.Dileep R. Yavagal OR Dr. Ralph L. Sacco, Departmentof Neurology, University of Miami Miller School ofMedicine, 1140 Northwest 14th Street, Miami,Florida 33136. E-mail: [email protected] [email protected].
RE F E RENCE S
1. Lloyd-Jones D, Adams RJ, Brown TM, et al., forthe American Heart Association Stroke Council.Heart disease and stroke statistics—2010 update: areport from the American Heart Association. Cir-culation 2010;121:e46–215.
2. Del Zoppo GJ, Saver JL, Jauch EC, et al., for theAmerican Heart Association Statistics Committeeand Stroke Statistics Subcommittee. Expansion ofthe time window for treatment of acute ischemicstroke with intravenous tissue plasminogen acti-vator: a science advisory from the American HeartAssociation/American Stroke Association. Stroke2009;40:2945–8.
3. National Institute of Neurological Disordersand Stroke rt-PA Stroke Study Group. Tissueplasminogen activator for acute ischemic stroke.N Engl J Med 1995;333:1581–7.
4. Albers GW, Bates VE, Clark WM, et al. Intrave-nous tissue-type plasminogen activator for treat-ment of acute stroke: the Standard Treatmentwith Alteplase to Reverse Stroke (STARS) study.JAMA 2000;283:1145–50.
5. Wardlaw JM, Zoppo G, Yamaguchi T, et al.Thrombolysis for acute ischaemic stroke. CochraneDatabase Syst Rev 2003:CD000213.
6. Hacke W, Kaste M, Bluhmki E, et al., for theECASS Investigators. Thrombolysis with alteplase3 to 4.5 hours after acute ischemic stroke. N Engl JMed 2008;359:1317–29.
7. Powers WJ, Derdeyn CP, Biller J, et al., for theAmerican Heart Association Stroke Council. 2015AHA/ASA focused update of the 2013 Guidelinesfor the Early Management of Patients With AcuteIschemic Stroke Regarding Endovascular Treat-ment: a guideline for healthcare professionalsfrom the American Heart Association/AmericanStroke Association. Stroke 2015;46:3020–35.
8. Bluhmki E, Chamorro A, Davalos A, et al.Stroke treatment with alteplase given 3.0-4.5 hafter onset of acute ischaemic stroke (ECASS III):
additional outcomes and subgroup analysis of arandomised controlled trial. Lancet Neurol 2009;8:1095–102.
9. Albers GW, Olivot JM. Intravenous alteplase forischaemic stroke. Lancet 2007;369:249–50.
10. Saqqur M, Uchino K, Demchuk AM, et al., forthe CLOTBUST Investigators. Site of arterial oc-clusion identified by transcranial Doppler predictsthe response to intravenous thrombolysis forstroke. Stroke 2007;38:948–54.
11. Paciaroni M, Balucani C, Agnelli G, et al. Sys-temic thrombolysis in patients with acute ischemicstroke and Internal Carotid ARtery Occlusion: theICARO study. Stroke 2012;43:125–30.
12. del Zoppo GJ, Higashida RT, Furlan AJ, et al.PROACT: a phase II randomized trial of recombi-nant pro-urokinase by direct arterial delivery inacute middle cerebral artery stroke. Stroke 1998;29:4–11.
13. Furlan A, Higashida R, Wechsler L, et al., forthe PROACT Investigators. Intra-arterial prour-okinase for acute ischemic stroke. The PROACT IIstudy: a randomized controlled trial. JAMA 1999;282:2003–11.
14. Adams H, Adams R, Del Zoppo G, et al.Guidelines for the early management of patientswith ischemic stroke: 2005 guidelines update ascientific statement from the Stroke Council of theAmerican Heart Association/American Stroke As-sociation. Stroke 2005;36:916–23.
15. Jauch EC, Saver JL, Adams HP Jr., et al., for theAmerican Heart Association Stroke Council,Council on Cardiovascular Nursing, Council onPeripheral Vascular Disease, and Council on Clin-ical Cardiology. Guidelines for the early manage-ment of patients with acute ischemic stroke: aguideline for healthcare professionals from theAmerican Heart Association/American Stroke As-sociation. Stroke 2013;44:870–947.
16. Smith WS, Sung G, Starkman S, et al., for theMERCI Trial Investigators. Safety and efficacy ofmechanical embolectomy in acute ischemic stroke:results of the MERCI trial. Stroke 2005;36:1432–8.
17. Smith WS, Sung G, Saver J, et al., for the MultiMERCI Investigators. Mechanical thrombectomyfor acute ischemic stroke: final results of the MultiMERCI trial. Stroke 2008;39:1205–12.
18. Nogueira RG, Liebeskind DS, Sung G, et al., forMERCI, and the Multi MERCI Writing Committee.Predictors of good clinical outcomes, mortality,and successful revascularization in patients withacute ischemic stroke undergoing thrombectomy:pooled analysis of the Mechanical EmbolusRemoval in Cerebral Ischemia (MERCI) and MultiMERCI. Trials. Stroke 2009;40:3777–83.
19. Penumbra Pivotal Stroke Trial Investigators.The Penumbra Pivotal Stroke Trial: safety andeffectiveness of a new generation of mechanicaldevices for clot removal in intracranial large vesselocclusive disease. Stroke 2009;40:2761–8.
20. Broderick JP, Palesch YY, Demchuk AM, et al.,for the Interventional Management of Stroke(IMS) III Investigators. Endovascular therapy afterintravenous t-PA versus t-PA alone for stroke.N Engl J Med 2013;368:893–903.
21. Ciccone A, Valvassori L, Nichelatti M, et al., forthe SYNTHESIS Expansion Investigators. Endo-vascular treatment for acute ischemic stroke.N Engl J Med 2013;368:904–13.
22. Kidwell CS, Jahan R, Gornbein J, et al., for theMR RESCUE Investigators. A trial of imaging se-lection and endovascular treatment for ischemicstroke. N Engl J Med 2013;368:914–23.
23. Nogueira RG, Lutsep HL, Gupta R, et al., forthe TREVO 2 Trialists. Trevo versus Merci re-trievers for thrombectomy revascularisation oflarge vessel occlusions in acute ischaemic stroke(TREVO 2): a randomised trial. Lancet 2012;380:1231–40.

Khandelwal et al. J A C C V O L . 6 7 , N O . 2 2 , 2 0 1 6
Acute Ischemic Stroke Intervention J U N E 7 , 2 0 1 6 : 2 6 3 1 – 4 4
2644
24. Saver JL, Jahan R, Levy EI, et al., for the SWIFTTrialists. Solitaire flow restoration device versusthe Merci Retriever in patients with acute ischae-mic stroke (SWIFT): a randomised, parallel-group,non-inferiority trial. Lancet 2012;380:1241–9.
25. Demchuk AM, Goyal M, Yeatts SD, et al., forthe IMS III Investigators. Recanalization and clin-ical outcome of occlusion sites at baseline CTangiography in the Interventional Management ofStroke III trial. Radiology 2014;273:202–10.
26. Wakhloo AK, Gounis MJ. Retrievable closedcell intracranial stent for foreign body and clotremoval. Neurosurgery 2008;62:ONS390–3, dis-cussion ONS393–4.
27. Berkhemer OA, Fransen PS, Beumer D, et al.,for the MR CLEAN Investigators. A randomizedtrial of intraarterial treatment for acute ischemicstroke. N Engl J Med 2015;372:11–20.
28. Goyal M, Demchuk AM, Menon BK, et al., forthe ESCAPE Trial Investigators. Randomizedassessment of rapid endovascular treatment ofischemic stroke. N Engl J Med 2015;372:1019–30.
29. Saver JL, Goyal M, Bonafe A, et al., for theSWIFT PRIME Investigators. Stent-retrieverthrombectomy after intravenous t-PA vs. t-PAalone in stroke. N Engl J Med 2015;372:2285–95.
30. Campbell BC, Mitchell PJ, Kleinig TJ, et al., forthe EXTEND-IA Investigators. Endovascular ther-apy for ischemic stroke with perfusion-imagingselection. N Engl J Med 2015;372:1009–18.
31. Campbell BC, Hill MD, Rubiera M, et al. Safetyand efficacy of solitaire stent thrombectomy: in-dividual patient data meta-analysis of randomizedtrials. Stroke 2016;47:798–806.
32. Jovin TG, Chamorro A, Cobo E, et al., for theREVASCAT Trial Investigators. Thrombectomywithin 8 hours after symptom onset in ischemicstroke. N Engl J Med 2015;372:2296–306.
33. Barber PA, Demchuk AM, Zhang J, et al., forthe ASPECTS Study Group. Validity and reliabilityof a quantitative computed tomography score inpredicting outcome of hyperacute stroke beforethrombolytic therapy. Lancet 2000;355:1670–4.
34. Wahlgren N, Ahmed N, Eriksson N, et al., forthe SITS-MOST Investigators. Multivariable anal-ysis of outcome predictors and adjustment of mainoutcome results to baseline data profile in ran-domized controlled trials: Safe Implementation ofThrombolysis in Stroke-MOnitoring STudy (SITS-MOST). Stroke 2008;39:3316–22.
35. Pexman JH, Barber PA, Hill MD, et al. Use ofthe Alberta Stroke Program Early CT Score (AS-PECTS) for assessing CT scans in patients withacute stroke. AJNR Am J Neuroradiol 2001;22:1534–42.
36. Hill MD, Demchuk AM, Goyal M, et al., for theIMS3 Investigators. Alberta Stroke Program early
computed tomography score to select patients forendovascular treatment: Interventional Manage-ment of Stroke (IMS)-III Trial. Stroke 2014;45:444–9.
37. Menon BK, O’Brien B, Bivard A, et al.Assessment of leptomeningeal collaterals usingdynamic CT angiography in patients with acuteischemic stroke. J Cereb Blood Flow Metab 2013;33:365–71.
38. Lees KR, Bluhmki E, von Kummer R, et al., forthe ECASS, ATLANTIS, NINDS and EPITHET rt-PAStudy Group Investigators. Time to treatmentwith intravenous alteplase and outcome in stroke:an updated pooled analysis of ECASS, ATLANTIS,NINDS, and EPITHET trials. Lancet 2010;375:1695–703.
39. ATLANTIS, ECASS, and NINDS rt-PA StudyGroup Investigators. Association of outcome withearly stroke treatment: pooled analysis ofATLANTIS, ECASS, and NINDS rt-PA stroke trials.Lancet 2004;363:768–74.
40. Marler JR, Tilley BC, Lu M, et al. Early stroketreatment associated with better outcome: theNINDS rt-PA stroke study. Neurology 2000;55:1649–55.
41. Khatri P, Abruzzo T, Yeatts SD, et al., forthe IMS I and II Investigators. Good clinicaloutcome after ischemic stroke with successfulrevascularization is time-dependent. Neurology2009;73:1066–72.
42. Khatri P, Yeatts SD, Mazighi M, et al., for theIMS III Trialists. Time to angiographic reperfusionand clinical outcome after acute ischaemic stroke:an analysis of data from the Interventional Man-agement of Stroke (IMS III) phase 3 trial. LancetNeurol 2014;13:567–74.
43. Menon BK, Almekhlafi MA, Pereira VM, et al.,for the STAR Study Investigators. Optimal work-flow and process-based performance measures forendovascular therapy in acute ischemic stroke:analysis of the Solitaire FR Thrombectomy forAcute Revascularization study. Stroke 2014;45:2024–9.
44. Tomsick T. TIMI, TIBI, TICI: I came, I saw, I gotconfused. AJNR Am J Neuroradiol 2007;28:382–4.
45. Lansberg MG, Straka M, Kemp S, et al., for theDEFUSE 2 Study Investigators. MRI profile andresponse to endovascular reperfusion after stroke(DEFUSE 2): a prospective cohort study. LancetNeurol 2012;11:860–7.
46. GUSTOAngiographic Investigators. The effectsof tissue plasminogen activator, streptokinase, orboth on coronary-artery patency, ventricularfunction, and survival after acute myocardialinfarction. N Engl J Med 1993;329:1615–22.
47. Stone GW, Grines CL, Cox DA, et al., for theControlled Abciximab and Device Investigation to
Lower Late Angioplasty Complications (CADILLAC)Investigators. Comparison of angioplasty withstenting, with or without abciximab, in acutemyocardial infarction. N Engl J Med 2002;346:957–66.
48. Mehta RH, Harjai KJ, Cox D, et al., for thePrimary Angioplasty in Myocardial Infarction(PAMI) Investigators. Clinical and angiographiccorrelates and outcomes of suboptimal coronaryflow inpatients with acute myocardial in-farction undergoing primary percutaneous coro-nary intervention. J Am Coll Cardiol 2003;42:1739–46.
49. Krumholz HM, Bradley EH, Nallamothu BK,et al. A campaign to improve the timeliness ofprimary percutaneous coronary intervention:Door-to-Balloon: An Alliance for Quality. J AmColl Cardiol Intv 2008;1:97–104.
50. Krumholz HM, Herrin J, Miller LE, et al.Improvements in door-to-balloon time in theUnited States, 2005 to 2010. Circulation 2011;124:1038–45.
51. Fonarow GC, Zhao X, Smith EE, et al.Door-to-needle times for tissue plasminogenactivator administration and clinical outcomesin acute ischemic stroke before and after aquality improvement initiative. JAMA 2014;311:1632–40.
52. Menon BK, Saver JL, Goyal M, et al. Trends inendovascular therapy and clinical outcomes withinthe nationwide Get With The Guidelines-Strokeregistry. Stroke 2015;46:989–95.
53. Hassan AE, Chaudhry SA, Grigoryan M, et al.National trends in utilization and outcomes ofendovascular treatment of acute ischemic strokepatients in the mechanical thrombectomy era.Stroke 2012;43:3012–7.
54. Zaidat OO, Lazzaro M, McGinley E, et al.Demand-supply of neurointerventionalists forendovascular ischemic stroke therapy. Neurology2012;79:S35–41.
55. Adeoye O, Albright KC, Carr BG, et al.Geographic access to acute stroke care in theUnited States. Stroke 2014;45:3019–24.
56. Alberts MJ, Latchaw RE, Selman WR, et al., forthe Brain Attack Coalition. Recommendations forcomprehensive stroke centers: a consensus state-ment from the Brain Attack Coalition. Stroke2005;36:1597–616.
57. Mullen MT, Branas CC, Kasner SE, et al. Opti-mization modeling to maximize population accessto comprehensive stroke centers. Neurology 2015;84:1196–205.
KEY WORDS large vessel occlusion,mechanical thrombectomy, stent retrievers,stroke systems