Embed Size (px)
Citation preview
American Journal of Transplantation 2009; 9: 1957–1960Wiley Periodicals Inc.
C© 2009 The AuthorsJournal compilation C© 2009 The American Society of
Transplantation and the American Society of Transplant Surgeons
doi: 10.1111/j.1600-6143.2009.02714.xCase Report
Acute Humoral Rejection in an ABO CompatibleCombined Liver–Kidney Transplant—The KidneyIs Not Always Protected
T. W. Reichmana,*, S. R. Marinob, J. Milnera,†,
R. C. Harlanda, A. Cochranec, J. M. Millisa
and G. Testaa
aDepartment of Surgery, bDepartment of Pathology andcDepartment of Pharmacology, University of ChicagoMedical Center, Chicago, IL*Corresponding author: Trevor W. Reichman,[email protected]†Current address: Loyola University Medical Center,Maywood, IL
Combined liver–kidney transplantation has become acommon practice for the treatment of patients withconcurrent end-stage renal disease and end-stage liverdisease. Liver transplantation in the setting of multi-organ transplantation is thought to have a protectiveeffect against humoral rejection even when a positivecrossmatch is obtained prior to surgery. In most cen-ters, a pre liver–kidney transplant crossmatch is rarelyperformed because of the known immunoprotectiveeffect of the liver allograft. In this report, a case of acutehumoral rejection in the kidney allograft after a com-bined liver–kidney transplant is described. Althoughhumoral rejection was treated using plasmapheresis,intravenous immunoglobulin and rituximab, the kid-ney required 3 months to recover function and finallyprogressed to chronic allograft nephropathy. A height-ened index of suspicion for acute humoral rejectionof the renal allograft is necessary when performingcombined liver–kidney transplants to highly sensitizedpatients due to previous organ transplants.
Key words: Humoral allograft rejection, kidney allo-graft, kidney graft survival, liver transplantation, sen-sitised transplant recipient
Received 04 January 2009, revised 16 April 2009 andaccepted for publication 21 April 2009
Introduction
It is widely appreciated that the liver is resistant toantibody-mediated injury and that it has a protective ef-fect on other allografts (1). Experimental and clinical expe-rience have shown that the liver is capable of absorbingantibodies from the circulation, which may account for the
protection it affords other organs in combined transplantsettings (2,3). Although the liver may be subject to someforms of antibody-mediated rejection over time, as seemsto be the case with ABO-incompatible grafts, there areonly a few reports of acute rejection of the liver in humans(4,5). To the best of our knowledge, we present the firstcase of isolated acute humoral rejection of a renal allograftin an ABO compatible combined liver–kidney transplantrecipient.
Case History
A 52-year-old dialysis-dependent CMV negative African–American man, blood group A positive, was referred in2006 with a diagnosis of hepatitis C cirrhosis secondaryto blood transfusions and end-stage renal disease (ESRD)secondary to hypertension for a combined liver–kidneytransplant procedure. His past medical history was signifi-cant for a living related kidney transplant (from his mother)in 1979 (Table 1). The graft failed and was removed after 4weeks due to acute cellular rejection. The patient remainedon hemodialysis until a complement-dependent cytotoxic-ity (CDC) crossmatch-negative deceased-donor kidney be-came available to him in 1989 (Table 1). Prior to his secondtransplant, HLA class I percent panel reactive antibodies(PRA) by CDC assay was 95%. Six months following thetransplant, he was diagnosed with acute cellular and vas-cular rejection and was treated with OKT3 and radiation.The graft eventually failed and was removed in 1997 foracute cellular on chronic rejection.
Following referral, he was transplanted with a liver and akidney from a 43-year-old blood group A positive, CMV neg-ative, deceased donor. The recipient MELD at the time oftransplant was 33. His class I and class II PRA prior to trans-plantation were 100% and 86%, respectively (Table 2). TheHLA-A1, B13, B60, DR4 and DQ3 (DQ7, DQ8, DQ9) anti-bodies were donor specific (Table 2). No peritransplant con-ditioning was performed because of the assumed immuno-protective effect of the liver. Induction immunosuppressionwas thymoglobulin (2.5 mg/kg ideal body weight adminis-tered every other day for three doses total) and a 5-daysteroid taper with conversion to maintenance tacrolimus(goal serum level 10–15 ng/ml) and mycophenolate mofetil(1000 mg twice daily). The steroid-free regimen was used
1957

Reichman et al.
Table 1: History of previous transplants
Transplant date Rejection type Transplant type HLA type
Recipient – – A30, A74; B39, BR53; Bw4, Bw6;Cw4, -DR17 (DR3), DR7; DQ2, -;DR52, DR53
1979 Acute cellular Living related kidney transplant(mother)
Unknown but presumed haplotypematched
11/08/1989 Acute cellular on chronic Deceased donor kidney transplant A31, A32; B8, B65; Bw6; Cw7, Cw8DR3, DR7; DR52, DR53; DQ2, -
08/14/2006 Acute humoral Deceased donor liver-kidneytransplant
A1, A31; B13, B60; Bw4, Bw6; Cw6,Cw10 DR4, DR7; DR53; DQ2, DQ3
secondary to the believed immunoprotective effect of theliver and the increased risk of recurrence of hepatitis Cin patients treated with steroids. An orthotopic piggybacktechnique was used to perform the liver transplant. Stan-dard anatomy was observed. A separate left-lower quad-rant incision was used for the renal transplant. The coldischemic time for the liver and kidney were approximately9 and 16 h, respectively. Rewarming times were 40- and30 min, respectively.
Initially postoperatively, adequate function was observedin both allografts. On postoperative day 9, the urine outputdecreased and the serum creatinine started to rise afterreaching a nadir of 2.7 mg/dL. A renal ultrasound was ob-tained which was normal. The patient was returned to theoperating room for exploration of the renal allograft andopen kidney biopsy. A temporary mesh was necessaryto facilitate a tension free closure in the setting of tissue
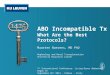
edema. A renal biopsy demonstrated the presence of focalacute tubular necrosis and diffuse peritubular capillary C4ddeposition consistent with humoral rejection (Figure 1).Postsurgery sera was sent for flow cytometric crossmatchand both T-cell and B-cell crossmatch were positive. An-tirejection therapy consisted of 75 g IVIG (1g/kg IBW)prior to plasmapheresis followed by replacement IVIG (200mg/kg IBW) given after each plasmapheresis. After the ini-tial plasmapheresis on postoperative day 11, one dose ofrituximab 375 mg/m2 was administered. The next treat-ment of plasmapheresis occurred approximately 48 h afteradmission of rituximab, and the patient received one finaldose of IVIG (2g/kg IBW) at the end the course of plasma-pheresis. Plasmapheresis treatments were performed sixtimes over the course of 12 days. Basic induction plasma-pheresis schedule was opted for and administered subjectto the patient’s clinical condition with the goal of affect-ing a negative continuous dynamic donor-specific serum
Table 2: Recipient sensitization history and clinical course
Sample date Clinical history % PRA1 class I % PRA1 class II HLA antibodies1
04/30/2002 86 – A1, A2, A3, A11, A23, A24, A26,A29, A36, A66, B8
08/29/2005 NA2 31 DQ7, DQ8, DQ907/24/2006 21 days pre-LKT 100 86 A13, A2, A3, A11, A23, A24, A25,
A26, A29, A30, A32, A34, A36,A43, A66, A68, A69, A80 B7, B8,B13, B18, B27, B2708, B37,B4005, B41, B42, B44, B45, B46,B47, B48, B49, B50, B54, B55,B56, B57, B58, B59, B60, B61,B62, B63, B64, B65, B67, B72,B73, B76, B77, B81, B82 DR1,DR4, DR9 DQ4, DQ5, DQ6,DQ74, DQ8, DQ9 DP4
07/27/2007 ∼11 months post-LKT, off dialysis,Cr 1.5
45 37 A2, A25 B8, B57, B58, B73, B76DQ7, DQ8, DQ9
06/03/2008 ∼22 mo post- LKT, declining kidneyand liver function, dialysisrestarted 2 months later
76 71 A1, A2, A11, A23, A24, A25, A26,A66 B8, B13, B27, B44, B45, B51,B57, B58, B62, B63, B76 DR1,DR4, DR11, DR13, DR15, DR16,DR51 DQ,6, DQ7, DQ8, DQ9
1Tests performed using solid-phase assays.2NA = not available.3Donor-specific antibodies are underlined.4Donor typing is DQ3. The DQ7, DQ8 and DQ9 serological specificities are splits of DQ3.
1958 American Journal of Transplantation 2009; 9: 1957–1960
AHR in LK Transplant
Figure 1: C4d immunofluorescence of a kidney biopsy. Slideshows diffuse peritubular capillary C4d deposition indicative ofhumoral rejection of kidney.
antibody titer. We did not measure these variables in thiscase as the C4d stain demonstrated allograft evidence ofrejection. It has been our experience that donor-specific an-tibody and crossmatch may be negative in the presence ofa humoraly rejecting organ due to dynamic serum antibodydepletion secondary to reaction in the allograft. Hemodialy-sis was resumed 3 days a week for volume and electrolytemanagement.
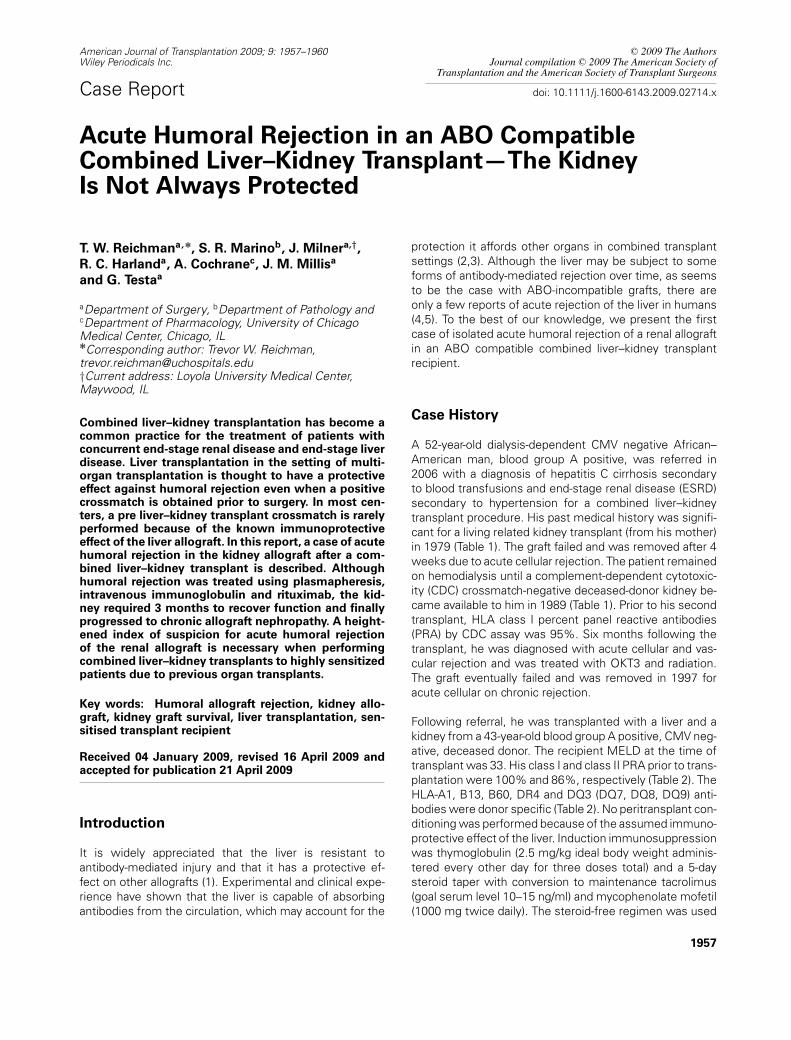
On postoperative day 15, the temporary mesh was re-moved and a second renal biopsy was obtained. The biopsyshowed worsening acute tubular necrosis and a similaramount of C4d deposition. A liver biopsy was performed,which demonstrated mild preservation injury and no mor-phologic evidence of humoral rejection on H&E stain butC4d hepatic arterial endothelial reactivity and sinusoidalendothelial cell reactivity in the periportal regions on im-munostain (Figure 2). His total bilirubin was 1.3 mg/dL,alkaline phosphatase 152 U/L, SGOT 37 U/L and SGPT 36U/L. Maintenance tacrolimus and mycophenolate mofetilwas continued during treatment for humoral rejection, withmycophenolate mofetil being reduced to 500 mg threetimes a day secondary to leukopenia.
Renal function improved and hemodialysis was success-fully discontinued at 3 months. His baseline creatinine atthis time was 1.7 mg/dL. A follow-up liver biopsy performedapproximately two and half months posttransplant for el-evated liver function tests showed no evidence of acuterejection and features consistent with early recurrent HCV.The patient continued to maintain his kidney function de-spite a repeat biopsy at 11 months depicting glomerularand peritubular capillaritis and C4d staining consistent withacute humoral rejection. His serum creatinine at the timewas 1.5 mg/dL. Repeat solid-phase antibody testing as-say performed around the same time showed absence
Figure 2: Low-power magnification (100 ×) of C4d immunos-
taining of a liver biopsy. Slide depicts positive staining for C4daround the portal vein and hepatic artery (arrow) but is negativearound the central vein.
of donor-specific antibodies except for DQ3 (DQ7, DQ8,DQ9) antibodies (Table 2). Kidney biopsy at 21 months wasconsistent with chronic humoral rejection. The degree ofcapillaritis had decreased significantly. The patient’s kidneycontinued to function well until the patient’s liver ultimatelyfailed secondary to recurrent hepatitis C approximately2 years later. Solid-phase antibody testing of a serum sam-ple 2 years after transplant had the HLA-A1, B13, DR4 andDQ3 (DQ7, DQ8, DQ9) donor-specific antibodies. The pa-tient died shortly thereafter.
Discussion
Combined liver–kidney transplantation has become com-monplace, and is standard of care for patients with bothend-stage liver disease and ESRD (6). However, the use ofcrossmatches in the liver pretransplant setting is controver-sial secondary to the believed immunoprotective effect ofthe liver. The exact mechanism for this immunoprotectiveeffect is not well known but several potential mechanismshave been hypothesized. It has been speculated that thiseffect is secondary to the secretion of soluble HLA anti-gens by the liver (7) and to phagocytosis of these reactiveantibodies by Kupffer cells (8). This immunoprotective ef-fect has allowed the successful transplantation of liversand combined liver–kidney transplants in the setting of apositive crossmatch and ABO incompatibility (1,3,9–11).The complete removal of HLA antibodies by the liver allo-graft converting a crossmatch from positive to negative dur-ing combined a liver–kidney transplant has been reported(12). However, the long-term beneficial effect of the liver incombined liver–kidney transplants has been debated (13).Although the liver is thought to protect against antibody-mediated rejection, acute humoral rejection of the liver has
American Journal of Transplantation 2009; 9: 1957–1960 1959

Reichman et al.
been described in the literature (4,5,14). In most cases,these rejections appear to be salvageable.
Several strategies have been described to thwart rejec-tion in the setting of a positive crossmatch. One strat-egy is the use of pretransplantation plasmapheresis toreduce reactive antibodies, prior to transplantation in pa-tients who have a known positive crossmatch (10). Othercenters have described staggered transplantation of or-gans allowing time for the liver to absorb the antibod-ies prior to implantation of the renal allograft (15). Inone case series, 15% acute rejection was observed withno reported hyperacute rejection (15). The use of bothstrategies resulted in successful combined liver–kidneytransplantation.
Review of the recipient’s sensitization history revealed thepresence of donor-specific antibodies prior to transplan-tation. At the time of the transplantation, the antibodyburden was likely too overwhelming for the liver to effec-tively clear to prevent humoral rejection. With the help ofplasmapharesis and antirejection therapy, we hypothesizethat the antibody load was lowered enough to allow theliver to recover and temper the humoral rejection. The livereventually was able to control the antiallograft antibodiesas 1 year posttransplant, A1, B13, B60 and DR4 donor-specific antibodies were no longer observed. However, asthe liver function started to deteriorate secondary to the re-currence of HCV, the liver likely began to gradually lose itsability to effectively clear reactive antibodies and there wasa reemergence of some donor-specific antibodies. Interest-ingly, the B60 donor-specific antibody present in the pre-transplant serum was not present in the last serum tested22 months after transplant, representing one of the anti-bodies continued to be absorbed by the liver (Table 2). Asthe patient’s liver rapidly deteriorated secondary to wors-ening fibrosis, the kidney failed and the patient was placedback on hemodialysis. The ultimate demise of the kidneywas likely multifactorial and involved both increasing anti-body burden, deposition of HCV-related immunocomplexand hepatorenal syndrome.
Although the liver is thought to be immunoprotective incombined organ transplantation, caution should be takenwhen transplanting highly sensitized patients. In this selectgroup of patients, pretransplant crossmatch might be ad-vantageous. Although a positive crossmatch may not pre-clude a transplant, the use of pretransplant plasmaphere-sis or delayed kidney transplant can be used successfullyto prevent acute humoral rejection. In the setting of com-bined liver–kidney transplantation, acute humoral rejectionoccurs and can have devastating consequences. Increasedvigilance should be used in selecting organs for highly sen-
sitized patients for combined liver–kidney transplants—thekidney is not always protected.
References
1. Flye MW, Duffy BF, Phelan DL, Ratner LE, Mohanakumar T. Pro-tective effects of liver transplantation on a simultaneously trans-planted kidney in a highly sensitized patient. Transplantation 1990;50: 1051–1054.
2. Margreiter R, Kornberger R, Koller J et al. Preliminary results withcombined hepatorenal transplantation. Transplant Proc 1987; 19:3552–3553.
3. Fung J, Makowka L, Tzakis A et al. Combined liver-kidneytransplantation: Analysis of patients with preformed lymphocy-totoxic antibodies. Transplant Proc 1988; 20(1 Suppl 1): 88–91.
4. Bird G, Friend P, Donaldson P et al. Hyperacute rejection in livertransplantation: A case report. Transplant Proc 1989; 21: 3742–3744.
5. Gordon RD, Iwatsuki S, Esquivel CO et al. Experience with primaryliver transplantation across ABO blood groups. Transplant Proc1987; 19: 4575–4579.
6. Ruiz R, Kunitake H, Wilkinson AH et al. Long-term analysis ofcombined liver and kidney transplantation at a single center. ArchSurg 2006; 141: 735–741.
7. McMillan RW, Gelder FB, Zibari GB, Aultman DF, Adamashvili I,McDonald JC. Soluble fraction of class I human histocompatibilityleukocyte antigens in the serum of liver transplant recipients. ClinTransplant 1997; 11: 98–103.
8. Starzl TE, Valdivia LA, Murase N et al. The biological basis of andstrategies for clinical xenotransplantation. Immunol Rev 1994; 141:213–244.
9. Gordon RD, Fung JJ, Markus B et al. The antibody crossmatch inliver transplantation. Surgery 1986; 100: 705–715.
10. Mjornstedt L, Friman S, Backman L, Rydberg L, Olausson M.Combined liver and kidney transplantation against a positive crossmatch in a patient with multispecific HLA-antibodies. TransplantProc 1997; 29: 3164–3165.
11. Saidman SL, Duquesnoy RJ, Demetris AJ et al. Combined liver-kidney transplantation and the effect of preformed lymphocyto-toxic antibodies. Transpl Immunol 1994; 2: 61–67.
12. Morrissey PE, Gordon F, Shaffer D et al. Combined liver-kidneytransplantation in patients with cirrhosis and renal failure: Effect ofa positive cross-match and benefits of combined transplantation.Liver Transpl Surg 1998; 4: 363–369.
13. Katznelson S, Cecka JM. The liver neither protects the kidney fromrejection nor improves kidney graft survival after combined liverand kidney transplantation from the same donor. Transplantation1996; 61: 1403–1405.
14. Rostron A, Carter V, Mutunga M et al. A case of acute humoral re-jection in liver transplantation: Successful treatment with plasma-pheresis and mycophenolate mofetil. Transpl Int 2005; 18: 1298–1301.
15. Faenza A, Fuga G, Nardo B et al. Combined liver-kidney transplan-tation: The experience of the University of Bologna and the caseof preoperative positive cross-match. Transplant Proc 2006; 38:1118–1121.
1960 American Journal of Transplantation 2009; 9: 1957–1960