Embed Size (px)
Citation preview

ACUPUNCTURE IN IVF
Acupuncture and herbal medicine in in vitro fertilisation: a review ofthe evidence for clinical practice
YING CHEONG1, LUCIANO G. NARDO2,3, TONY RUTHERFORD4, & WILLIAM LEDGER5
1Division of Developmental Origins of Adult Diseases, University of Southampton School of Medicine (DOHaD), Level F,
Princess Anne Hospital, Southampton, UK, 2Department of Reproductive Medicine, St. Mary’s Hospital, Manchester, UK,3North West Fertility, IVF Unit, UK, 4Reproductive Medicine Unit, Leeds General Infirmary, Leeds, UK, and 5Academic
Unit of Reproductive and Developmental Medicine, University of Sheffield, Sheffield, UK
AbstractThe objectives of this systematic review were to determine the effectiveness of (a) acupuncture and (b) Chinese herbalmedicine on the treatment of male and female subfertility by assisted reproductive technologies (ART). All reports fromRCTs of acupuncture and/or Chinese herbal medicine in ART were obtained via searches through The CochraneMenstrual Disorders and Sub-fertility Group’s Specialised Register of controlled trials, and other major databases. Theoutcome measures were determined prior to starting the search, and comprised: live birth rate, ongoing pregnancy rate,clinical pregnancy rate, the incidence of ovarian hyperstimulation syndrome and multiple pregnancy, miscarriage rateand adverse effects arising from treatment. Overall, 14 trials (a total of 2670 subjects) were included in the meta-analysis. The results provided no evidence of benefit in the use of acupuncture during assisted conception. Furtherstudies should attempt to explore the potential placebo, as well as treatment, effects of this complimentary therapy.Essential elements for a quality RCT will be the size of the trial, the use of a standardised acupuncture method and ofplacebo needles.
Keywords: Acupuncture, herbal medicne, assisted conception, IVF, pregnancy, RCT
Introduction
One in seven couples in Western countries suffer
from sub-fertility (Schmidt et al., 1995; Boivin et al.,
2007) and many will seek medical help in the form of
assisted reproductive technologies (ART), including
controlled ovarian stimulation with or without
intrauterine insemination (IUI) and in vitro fertilisa-
tion (IVF) treatment. More than 10,000 children are
born each year in the United Kingdom following
IVF. Traditional Chinese medicine (TCM), espe-
cially in the form of acupuncture and herbal
medicine, is widely used to treat many common
conditions and has been explored in ART. However,
its role and efficacy in reproductive medicine is still a
matter of much debate.
In its original form, the use of acupuncture and
Chinese herbal remedies was based on the princi-
ples of TCM, which is a 3000-year old holistic
system. TCM combines medicinal herbs, acupunc-
ture, food therapy, massage and therapeutic ex-
ercise for the treatment and the prevention of
disease. TCM drug treatment typically consists of
complex prescriptions of a combination of several
components. The combination is based on the
Chinese diagnostic patterns (i.e. inspection, listen-
ing, smelling, inquiry and palpation) and follows a
completely different rationale than many conven-
tional treatments. Herbal medicine is the most
important part of TCM. Acupuncture ‘involves the
insertion of fine needles into the skin along the
meridians and provides a means of altering the flow of
energy through the body’ (Vickers & Zollman, 1999).
In a typical treatment, between 4 and 10 points are
needled for 10–30 min. Needles can be stimulated by
manual twirling or with a small electric current
(electro-acupuncture, EA). Some acupuncturists
attempt to produce a sensation called ‘de Qi’ – a
sense of heaviness, soreness or numbness at the point
of needling. This is regarded as a sign of stimulating
the acupuncture point correctly. To date, there have
been few studies on the physiological effects of
Correspondence: Ying Cheong, Division of Developmental Origins of Adult Diseases (DOHaD), Level F, Princess Anne Hospital, Southampton, UK.
E-mail: [email protected]
Human Fertility, March 2010; 13(1): 3–12
ISSN 1464-7273 print/ISSN 1742-8149 online � British Fertility Society
DOI: 10.3109/14647270903438830
Hum
Fer
til (
Cam
b) D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Yor
k on
11/
18/1
4Fo
r pe
rson
al u
se o
nly.

acupuncture in the male and female reproductive
tract.
Aims
(a) To determine the effectiveness of acupuncture
alone or acupuncture with concurrent IVF on
the outcome of treating male and female sub-
fertility compared with the various forms of
IVF and with no treatment alone.
(b) To determine the effectiveness of Chinese
herbal medicine alone or with concurrent
IVF on the outcome of treating male and
female subfertility compared with the various
forms of IVF and no treatment alone.
Trial inclusion criteria
Acupuncture
Searches were conducted for all prospective ran-
domised controlled trials (RCTs) which compared
acupuncture treatment versus no treatment, placebo
acupuncture or sham acupuncture during ovarian
stimulation with or without IUI, IVF or frozen-
thawed embryo transfer (FET) treatment. The two
types of sham or placebo acupuncture commonly
used are (a) needling an area that is not a
recognised ‘point’, and (b) needling a point which
is believed to be ineffective for the particular
condition. Needling can be performed by using
real needling with skin penetration or using a sham
or placebo needle (for example, the Streitberger
placebo needle, Asiamed, Pullach, Germany).
Because the tip of the sham needle is blunted,
skin penetration will not occur. We included either
traditional acupuncture, in which needles are
inserted in classical meridian points, or contem-
porary acupuncture, in which the needles are
inserted in non-meridian or trigger points, regard-
less of the source of stimulation (for example,
hand, fine needle, moxibustion, which is a tradi-
tional Chinese treatment using moxa or mugwort
herb on acupuncture points, with warming needle
or electrical stimulation). We excluded studies of
acupuncture treatment without needling, such as
point injection, acupressure, laser acupuncture,
tap-pricking or cupping on pricked superficial
blood vessels. We also excluded trials comparing
different acupuncture treatments alone.
Chinese herbal medicine
Searches were conducted for all prospective RCTs
comparing Chinese medicinal herbs (single or
compound) with no intervention, placebo or stan-
dard medical interventions, such as clomiphene
citrate and GnRH agonists for ovulatory problems,
and immunological treatments for subfertility.
Search strategy
All the reports from RCTs of acupuncture and/or
Chinese herbal medicine in ART were obtained via
searches through The Cochrane Menstrual Dis-
orders and Sub-fertility Group’s Specialised Regis-
ter of controlled trials; the China Academic Journal
Electronic full text Database in China National
Knowledge Infrastructure, Index to Chinese Peri-
odical Literature, the National Research Register,
PsycINFO or the US equivalent Clinical Trials
register (http://www.clinicaltrials.gov). All refer-
ences of the studies included and excluded were
hand-searched for additional relevant reports. The
levels of evidence used are those shown in Table I.
Statistical analysis was performed in accordance
with the guidelines developed by the Menstrual
Disorders and Sub-fertility Group. Where possible,
the outcomes were pooled statistically. For dichot-
omous data (i.e. proportion of participants with a
specific adverse side effect), results were expressed
for each study as an odds ratio with 95%
confidence intervals (95% CI) and combined them
for meta-analysis with Cochrane Review Manager
software (RevMan 5) using Peto-modified Mantel–
Haenszel method. Continuous differences between
groups in the meta-analysis have been shown as a
weighted mean difference and 95% CI. The fixed
effects model was used. The heterogeneity between
the results of different studies was examined by
inspecting the scatter in the data points, the
overlap in their confidence intervals and, more
formally, by checking the results of the chi-squared
tests. Subgroup analysis and sensitivity analysis
were performed when there was significant clinical
or statistical heterogeneity.
Outcome measures
The outcome measures were determined prior to
starting the search, and comprised: live birth rate
(LBR), ongoing pregnancy rate, clinical pregnancy
rate (CPR), the incidence of ovarian hyperstimula-
tion syndrome (OHSS) and multiple pregnancy,
miscarriage rate and adverse effects arising from
treatment.
Results
Acupuncture
Overall, 14 trials (a total of 2670 subjects) were
included in the meta-analysis. The reports were of
three types: (a) those in which acupuncture was
4 Y. Cheong et al.
Hum
Fer
til (
Cam
b) D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Yor
k on
11/
18/1
4Fo
r pe
rson
al u
se o
nly.

undertaken around the time of oocyte retrieval
(Stener-Victorin et al., 1999, 2003; Humaidan &
Stener-Victorin, 2004; Gejervall et al., 2005;
Sator-Katzenschlager et al., 2006); (b) those in
which acupuncture was done on the day of
Embryo Transfer only (Paulus et al., 2002,
2003; Benson et al., 2006; Smith et al., 2006;
Westergaard et al., 2006; Craig et al., 2007;
Domar et al., 2008; So et al., 2009) and (c) those
in which acupuncture was performed on the
Table I. Grading of evidence.
Hierarchy of evidence
1a Systematic review and meta-analysis of randomised controlled trials (RCTs).
1b At least one randomised controlled trial.
2a At least one well-designed controlled study without randomisation.
2b At least one other type of well-designed quasi-experimental study.
3 Well designed non experimental descriptive studies, such as comparative studies, correlation studies or case studies.
4 Expert committee reports or opinions and/or clinical experience of respected authorities.
Grade strength of evidence
A Requires at least one RCT as part of a body of literature of overall good quality and consistency addressing the specific
recommendations. (Evidence levels 1a, 1b)
B Requires the availability of well controlled clinical studies but no randomised clinical trials on the topics of recommendation. (Evidence
levels 2a, 2b, 3)
C Requires evidence obtained from expert committee reports of opinions and/or clinical experiences of respected authorities. Indicates an
absence of directly applicable clinical studies of good quality. (Evidence level 4)
GPP Good practice point.
Table II. Description of location of the four most commonly used acupuncture points.
Acupuncture points Intended treatment
GV 20 (Baihui) Location: on the midline of the head, 7 cun directly above the posterior hairline, approximately on the midpoint
of the line connecting the apexes of the two auricles.
Indications: Headache, vertigo, tinnitus, nasal obstruction, aphasia by apoplexy, coma, mental disorders,
prolapse of the rectum and the uterus.
Traditional action: Clears the mind, lifts the spirits, tonifies yang, strengthens the ascending function of the spleen,
eliminates interior wind, promotes resuscitation.
Location: in the middle of the 2nd metacarpal bone on the radial side.
Precautions: no moxa, no needle in pregnancy.
Point associations: Yuan source point, entry point, command point for face, nose, mouth and jaw
LI 4 (Hegu) Actions and effects:
Releases the exterior for wind-cold or wind-heat syndromes
Strengthens the wei qi, improves immunity.
Regulates the sweat glands, for excessive sweating tonify LI 4 then disperse KD 7 and vice versa
Any problem on the face - sense organs, mouth, teeth, jaw, toothache, allergies, rhinitis, hay fever, acne,
eye problems, etc.
Toothache use both LI 4 & ST 44 - LI for the lower jaw & ST for the upper jaw
Headache, especially frontal, sinus (yangming area)
Chronic pain
Influence the circulation of Qi and blood - use the four gates, LI 4 & LV 3 to strongly move the Qi and blood
in the body clearing stagnation and alleviating pain.
Promote labor or for retained placenta
SP 6 (Sanyinjiao) Location: 3 cun directly above the tip of the medial malleolus on the posterior border of the tibia
Precautions: no needle in pregnancy
Point associations:
Intersection point of the SP, LV and KD (3 leg yin meridians)
Actions and effects:
Tonify Yin and blood, all spleen disorders.
Digestive disorders, sinking or prolapse.
Gynaecological issues, male sexual issues, difficult labour (expel foetus)
Bleeding disorders, cool blood in hot skin diseases
Insomnia and other anxiety-related emotions
Location: 2 cun lateral to the AML level with CV 3
ST29 (Guilai) Actions and effects:
Excess or cold/deficient disorders of the lower warmer - amenorrhoea, irregular menstruation, qi stagnation/masses
Running Piglet disorder
Acupuncture and herbal medicine 5
Hum
Fer
til (
Cam
b) D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Yor
k on
11/
18/1
4Fo
r pe
rson
al u
se o
nly.

day of ET and then 2–3 days after ET (repeated
acupuncture) (Dieterle et al., 2006; Westergaard
et al., 2006). Data relating to LBR were
obtained from six trials (Paulus et al., 2002,
2003; Stener-Victorin et al., 2003; Humaidan &
Stener-Victorin, 2004; Benson et al., 2006;
Dieterle et al., 2006; Domar et al., 2008).
The most commonly used acupuncture points
appeared to be GV 20, LI 4, SP6 and ST 29
(Table II).
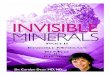
Acupuncture versus Control (all categories) (Figure 1)
Live birth rate. In the pooled results from seven
trials (Stener-Victorin et al., 1999; Paulus et al.,
2002, 2003; Humaidan & Stener-Victorin, 2004;
Dieterle et al., 2006; Westergaard et al., 2006; So
et al., 2009) (a total of 1601 subjects), the LBR was
32% (258/805) in the acupuncture group and 29%
(229/796) in the control group (odds ratio 1.31, 95%
CI 0.88–1.95).
Clinical pregnancy rate. In the pooled results from
14 trials (n¼ 2670) (Stener-Victorin et al., 1999,
2003; Paulus et al., 2002, 2003; Humaidan &
Stener-Victorin, 2004; Gejervall et al., 2005;
Benson et al., 2006; Dieterle et al., 2006; Sator-
Katzenschlager et al., 2006; Smith et al., 2006;
Westergaard et al., 2006; Craig et al., 2007;
Domar et al., 2008; So et al., 2009), the CPR
Figure 1. Outcomes of acupuncture versus control (all categories): (a) Live birth. (b) Clinical pregnancy. (c) Miscarriage.
6 Y. Cheong et al.
Hum
Fer
til (
Cam
b) D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Yor
k on
11/
18/1
4Fo
r pe
rson
al u
se o
nly.

was 38% (531/1406) in the acupuncture group and
35% (440/1264) in the control group (odds ratio
1.21, 95% CI 0.9–1.63).
Miscarriage. In the pooled results from three
trials (Dieterle et al., 2006; Smith et al., 2006;
Westergaard et al., 2006; So et al., 2009) (a total
of 908 subjects), the miscarriage rate was 13% (65/
492) in the acupuncture group and 12% (54/416) in
the control group (odds ratio 1.21, 95% CI 0.8–
1.83).
Acupuncture around the time of oocyte retrieval
(Figure 2)
Live birth rate. Only two trials reported on LBR
(Stener-Victorin et al., 2003; Humaidan & Stener-
Victorin, 2004) (a total of 464 subjects). There was no
difference in the LBR between the patients who had
acupuncture (75/229, 33%) and the control group (84/
235, 36%) (odds ratio 0.87, 95% CI 0.59–1.29).
Clinical pregnancy rate. In the pooled results from
five trials (Stener-Victorin et al., 1999, 2003; Humai-
dan & Stener-Victorin, 2004; Gejervall et al., 2005;
Sator-Katzenschlager et al., 2006) (a total of 868
subjects), the CPR in the treatment group was 37%
(165/448) and in the control group was 35% (146/
420) (odds ratio 1.08, 95% CI 0.82–1.44).
Miscarriage rate. The pooled results from four trials
(Stener-Victorin et al., 1999, 2003; Humaidan &
Stener-Victorin, 2004; Sator-Katzenschlager et al.,
2006) (a total of 378 subjects) showed no difference
in the miscarriage rate between the treatment group
and controls (9/71, 13% and 12/68, 16%; odds ratio
0.81, 95% CI 0.46–1.46).
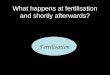
Acupuncture on the day of ET (Figure 3)
Live birth rate. In the pooled results from four trials
(Paulus et al., 2002, 2003; Westergaard et al., 2006;
So et al., 2009) (n¼ 912 subjects), the LBR was 33%
(151/460) in the acupuncture group and 29% (130/
452) in the control group (odds ratio 1.43, 95% CI
0.77–2.65). There was no statistical difference in
LBR in the acupuncture compared to the control
group.
Figure 2. Outcomes of acupuncture during oocyte retrieval versus control: (a) Live birth. (b) Clinical pregnancy. (c)
Miscarriage.
Acupuncture and herbal medicine 7
Hum
Fer
til (
Cam
b) D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Yor
k on
11/
18/1
4Fo
r pe
rson
al u
se o
nly.

Clinical pregnancy rate. In the pooled results of
seven trials (Paulus et al., 2002, 2003; Benson et al.,
2006; Smith et al., 2006; Westergaard et al., 2006;
Domar et al., 2008; So et al., 2009) (n¼ 1486
subjects), the CPR was 39% (294/751) in the
acupuncture treatment group and 37% (273/735)
in the controls (odds ratio 1.14, 95% CI 0.76–1.69).
There was no evidence of benefit for the use of
acupuncture treatment in terms of CPR compared to
the controls.
Miscarriage rate. Only three trials (Smith et al.,
2006; Westergaard et al., 2006; So et al., 2009)
(n¼ 592) evaluated the possible impact of acupunc-
ture on the day of embryo transfer on miscarriage.
There was no difference between the acupuncture
treatment group (22%: 64/285) and the control
group (18% (55/307), odds ratio 1.38, 95% CI 0.90–
2.11).
Repeated acupuncture after ET (Figure 4)
Live birth rate. The pooled results of three studies
(Dieterle et al., 2006; Westergaard et al., 2006; So
et al., 2009) (n¼ 403) indicated that there was no
statistical difference in the LBR between the acu-
puncture treatment and the control groups when
acupuncture was performed at the time of ET and
repeated 2–3 days later. The LBR was 28% (57/207)
in the acupuncture group compared to 17% (34/196)
in the control group (OR 1.83, 95% CI 1.00–3.85;
P¼ 0.05).
Clinical pregnancy rate. From the pooled results of
two trials (Dieterle et al., 2006; Westergaard et al.,
2006) (n¼ 403), the CPR of the acupuncture
treatment group was 35% (72/207) compared to
19% (38/196) for the control group (OR 2.23, 95%
CI 1.41–3.51; P¼ 0.0006).
Figure 3. Outcomes of acupuncture on the day of ET versus control: (a) Live birth. (b) Clinical pregnancy. (c)
Miscarriage.
8 Y. Cheong et al.
Hum
Fer
til (
Cam
b) D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Yor
k on
11/
18/1
4Fo
r pe
rson
al u
se o
nly.

Miscarriage rate. Two trials (n¼ 403) evaluated the
impact of repeated acupuncture on miscarriage
(Dieterle et al., 2006; Westergaard et al., 2006).
There was no statistical difference in the miscarriage
rate between acupuncture and the controls when
acupuncture was performed around ET and repeated
2–3 days later. The miscarriage rate in the acupunc-
ture group was 14% (30/207) compared to 9% (18/
196) in the control group (OR 1.68, 95% CI 0.90–
3.12; P¼ 0.10).
Side effects
None of the 14 trials reported on the occurrence of
OHSS. Smith et al. (2006) were the only ones to
report on patients’ experiences. The authors found
no difference in the quality of life (SF-36 scores)
between the study and control groups. The most
frequently reported outcome in that particular trial
was relaxation; subjects in the control group (who
did not received acupuncture) reported being more
relaxed compared to the study group.
Sensitivity analysis (Figure 5): acupuncture versus sham
controls around the time of ET
Live birth rate. There was no evidence of benefit
of acupuncture treatment in the sham group
(Paulus et al., 2003; Dieterle et al., 2006; So
et al., 2009) (Odds Ratio 1.12, 95% CI 0.83–
1.52). However, the group having acupuncture had
a favourable LBR, in the pooled results where non-
sham controls were used (Paulus et al., 2002;
Westergaard et al., 2006) (odds ratio 2.17, 95% CI
1.32–3.54).
Clinical pregnancy rate. The odds ratio for CPR in
studies with a sham acupuncture control group
(Paulus et al., 2002; Benson et al., 2006;
Westergaard et al., 2006; Craig et al., 2007; Domar
et al., 2008; So et al., 2009) was 1.33 (95% CI 0.72–
2.45) whilst that in studies with no sham acupunc-
ture control was 1.18 (95% CI 0.64–2.18) (Paulus
et al., 2002; Benson et al., 2006; Westergaard et al.,
2006; Craig et al., 2007; Domar et al., 2008). There
was no evidence of benefit for the use of acupuncture
versus control in terms of CPR.
Chinese herbal medicine
Meta-analytical pooling was not feasible as there
were no RCTs on the use of Chinese herbal
medicine in ART.
Discussion
This meta-analysis shows that there is no evidence of
benefit from having acupuncture around the time of
Figure 4. Outcomes of repeated acupuncture versus control: (a) Live birth. (b) Clinical pregnancy. (c) Miscarriage.
Acupuncture and herbal medicine 9
Hum
Fer
til (
Cam
b) D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Yor
k on
11/
18/1
4Fo
r pe
rson
al u
se o
nly.

Figure 5. Sensitivity analysis – outcomes of acupuncture on the day of ET versus control: (a) Live birth. (b) Clinical pregnancy.
(c) Miscarriage.
10 Y. Cheong et al.
Hum
Fer
til (
Cam
b) D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Yor
k on
11/
18/1
4Fo
r pe
rson
al u
se o
nly.

assisted conception. This finding results from the
inclusion of the most recent trials and is contrary to
many previous studies. There is however, a sub-
stantial amount of clinical heterogeneity in all these
studies, in particular in the use of sham acupuncture
as a control versus no sham, the timing of the
acupuncture treatment during the course of the
assisted conception and the lack of controls for the
placebo effect. Evidence to recommend the use of
herbal medicine during IVF treatment is currently
lacking.
Acupuncture clearly has the advantages of being
painless and having no serious adverse effects.
Nevertheless, before routine treatment can be
accepted into mainstream medicine, it needs to have
proven efficacy. Acupuncture has to be demonstrably
more effective than placebo, which in this context is
relatively difficult to show. In the RCTs included in
this meta-analysis, a variety of placebos were used in
the control groups, ranging from no intervention to
the use of Sham acupuncture needles (Dieterle et al.,
2006; Smith et al., 2006). Sham needles are regarded
as the gold standard placebo although they have been
criticised as possibly inducing an ‘acupressure
effect’. The placement of a needle in any position
elicits a biological response that complicates the
interpretation of studies involving Sham needle
acupuncture. Furthermore, placebo acupoints,
whether with real or Sham needling, can mean
needling on acupoints that are unrelated to fertility,
or on points that are next to, but not on the real,
acupuncture points. There is as yet no national or
international professional group consensus regarding
what constitutes a good placebo in trials examining
the effects of acupuncture. The placebo effect in any
of these combinations of sham or placebo acupunc-
ture can be quite strong and it may well be that the
time and attention given to the patient, especially
around the time of ET, induces relaxation and
generates better outcomes.
Acupuncture is a complex intervention that has
different effects on different patients with similar
medical conditions. The number and length of
treatments needed and the specific points used
may vary among individuals and during the course
of treatment. Although all the trials included in
this review examined the effect of acupuncture in
improving the outcome of IVF, it is unclear why
different acupuncture points were selected to
achieve the same objective. In Western medicine,
where standardisation of methodology is of key
importance in medical research, the absence of
complete concordance of the acupuncture points in
these studies, which were all designed to improve
IVF pregnancy outcome, is an unfamiliar concept.
There is no consensus amongst practicing acu-
puncturists as to what constitutes reasonable
variation of an acupuncture treatment ‘protocol’.
There is also no consensus as to how much
experience and training an acupuncturist requires
in order to provide an effective acupuncture
treatment.
With regards to the safety of acupuncture and the
likelihood of miscarriage, these data provide a degree
of reassurance to both patients and practitioners
though a robust evidence base is lacking and the
current meta-analysis has not examined studies
where acupuncture has been performed in early
pregnancy.
In conclusion, the results of this meta-analysis
suggest that there is no evidence of benefit in the use
of acupuncture during assisted conception. Further
studies should attempt to explore the potential
placebo as well as treatment effects of this compli-
mentary therapy. Essential elements for a quality
RCT will be the size of the trial, the use of a
standardised acupuncture method and of placebo
needles.
References
Benson, M.R., Elkind-Hirsch, K.E., Theall, A., Fong, K., Hogan,
R.B., & Scott, R.T. (2006). Impact of acupuncture before and
after embryo transfer on the outcome of in vitro fertilization
cycles: a prospective single blind randomized study. Fertility &
Sterility, 86, S135.
Boivin, J., Bunting, L., Collins, J.A., & Nygren, K.G. (2007).
International estimates of infertility prevalence and
treatment-seeking: potential need and demand for infertility
medical care. Human Reproduction, 22, 1506–1512.
Craig, L.B., Criniti, A.R., Hansen, K.R., Marshall, L.A., &
Soules, M.R. (2007). Acupuncture lowers pregnancy rates
when performed before and after embryo transfer. Fertility &
Sterility, 88, S40.
Dieterle, S., Ying, G., Hatzmann, W., & Neuer, A. (2006). Effect
of acupuncture on the outcome of in vitro fertilization
and intracytoplasmic sperm injection: a randomized, prospec-
tive, controlled clinical study. Fertility & Sterility, 85, 1347–
1351.
Domar, A.D., Meshay, I., Kelliher, J., Alper, M., & Powers, R.D.
(2008). The impact of acupuncture on in vitro fertilization
outcome. Fertility & Sterility, 91, 723–726.
Recommendation and guidance for practice
There is no evidence of benefit for the use of
acupuncture in IVF treatment. A
Further research is required to optimise and
standardise the acupuncture technique em-
ployed. GPP
There is currently no evidence to recommend
the use of Chinese herbal medicine in IVF
treatment.
Acupuncture and herbal medicine 11
Hum
Fer
til (
Cam
b) D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Yor
k on
11/
18/1
4Fo
r pe
rson
al u
se o
nly.

Gejervall, A.L., Stener-Victorin, E., Moller, A., Janson, P.O.,
Werner, C., & Bergh, C. (2005). Electro-acupuncture versus
conventional analgesia: a comparison of pain levels during
oocyte aspiration and patients’ experiences of well-being after
surgery. Human Reproduction, 20, 728–735.
Humaidan, P., & Stener-Victorin, E. (2004). Pain relief during
oocyte retrieval with a new short duration electro-acupuncture
technique – an alternative to conventional analgesic methods.
Human Reproduction, 19, 1367–1372.
Paulus, W.E., Zhang, M., Strehler, E., El-Danasouri, I., & Sterzik,
K. (2002). Influence of acupuncture on the pregnancy rate in
patients who undergo assisted reproduction therapy. Fertility
& Sterility, 77, 721–724.
Paulus, W.E., Zhang, M., Strehler, E., Seybold, B., & Sterzik, K.
(2003). Placebo-controlled trial acupuncture effects in
assisted reproductive therapy. Human Reproduction, 18,
xviii18.
Sator-Katzenschlager, S.M., Wolfler, M.M., Kozek-Langenecker,
S.A., Sator, K., Sator, P. G., Li, B., et al. (2006). Auricular
electro-acupuncture as an additional perioperative analgesic
method during oocyte aspiration in IVF treatment. Human
Reproduction, 21, 2114–2120.
Schmidt, L., Munster, K., & Helm, P. (1995). Infertility and the
seeking of infertility treatment in a representative population.
British Journal of Obstetrics and Gynaecology, 102, 978–984.
Smith, C., Coyle, M., & Norman, R. J. (2006). Influence of
acupuncture stimulation on pregnancy rates for women
undergoing embryo transfer. Fertility & Sterility, 85, 1352–
1358.
So, E.W.S., Ng, E.H.Y., Wong, Y.Y., Lau, E.Y.L., Yeung,
W.S.B., & Ho, P.C. (2009). A randomized double blind
comparison of real and placebo acupuncture in IVF treatment.
Human Reproduction, 24, 341–348.
Stener-Victorin, E., Waldenstrom, U., Nilsson, L., Wikland, M., &
Janson, P.O. (1999). A prospective randomized study of electro-
acupuncture versus alfentanil as anaesthesia during oocyte
aspiration in in vitro fertilization. Human Reproduction, 14,
2480–2484.
Stener-Victorin, E., Waldenstrom, U., Wikland, M., Nilsson, L.,
Hagglund, L., & Lundeberg, T. (2003). Electro-acupuncture
as a peroperative analgesic method and its effects on
implantation rate and neuropeptide Y concentrations in
follicular fluid. Human Reproduction, 18, 1454–1460.
Vickers, A., & Zollman, C. (1999). ABC of complementary
medicine: Acupuncture. British Medical Journal, 319, 973–976.
Westergaard, L.G., Mao, Q., Krogslund, M., Sandrini, S., Lenz,
S., & Grinsted, J. (2006). Acupuncture on the day of embryo
transfer significantly improves the reproductive outcome in
infertile women: a prospective, randomized trial. Fertility &
Sterility, 85, 1341–1346.
12 Y. Cheong et al.
Hum
Fer
til (
Cam
b) D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Yor
k on
11/
18/1
4Fo
r pe
rson
al u
se o
nly.