Embed Size (px)
Citation preview
6. Short LJ, Bell DM. Risk of occupational infection with bloodborne pathogens inoperating and delivery room settings. Am J Infect Control 1993;21:343–350.
7. Owens DK, Nease RF. Occupational exposure to human immunodeficiencyvirus and hepatitis B virus: a comparative analysis of risk. Am J Med 1997;92:503–512.
8. Regnier SJ. ACS/CDS meeting explores risks of bloodborne pathogens. Bull AmColl Surg 1994;79:30–38.
9. Puro V, Petrosillo N, Ippolito G. Risk of hepatitis C seroconversion after occu-pational exposures in health care workers. Am J Infect Control 1995;23:273–277.
10. Poynard T, Marcellin P, Lee SS, et al. Randomized trial of interferon alpha2bplus ribavirin for 48 weeks versus interferon alpha2b plus placebo for 48 weeks fortreatment of chronic infection with hepatitis C virus. International HepatitisInterventional Therapy Group. Lancet 1998;352:1426–1432.
11. Jadoul M, Cornu C, van Ypersele de Strihou C. Universal precautions preventhepatitis C virus transmission: a 54 month follow-up of the Belgium MulticenterStudy. The Universitaires Cliniques St-Luc (UCL) Collaborative Group. KidneyInt 1998;53:1022–1025.
12. Smith JW, Nichols RL. Barrier efficiency of surgical gowns: are we really pro-tected from our patients’ pathogens? Arch Surg 1991;126:756–763.
13. Quebbeman EJ, Telford GL, Wadsworth K, et al. Double gloving: protectingsurgeons from blood contamination in the operating room. Arch Surg 1992;127:213–216.
14. Gani JS, Anseline PF, Bissett Rl. Efficacy of double versus single gloving inprotecting the operating team. Aust N Z J Surg 1990;60:171–175.
15. Popejoy SL, Fry DE. Blood contact and exposure in the operating room. SurgGynecol Obstet 1991;172:480–483.
Thoracic
Achalasia: Looking for the Best RouteGuest Reviewers: Stephen Hetz, COL, MC, USA,Charles Whitlow, MAJ, MC, USA, andJohn Schriver, MAJ, MC, USA
CURRENT THERAPIES FOR ACHALASIA: COMPARISON AND EFFICACY.Vaezi MF, Richter JE. J Clin Gastroenterol 1998;27:21–35.
Objective: Clinical review of achalasia.
Design: Literature review.
Methods: Review of published data on treatment of achalasia. Topics of reviewinclude pharmacological therapy, balloon dilation, surgical cardiomyotomy, botuli-num toxin injection, and comparison of outcomes.
Results: The best-studied pharmacologic agents are calcium channel blockers andisosorbide dinitrate. Because these agents are short acting and provide incomplete relief
REVIEWER COMMENTS
This article is a comprehensive review ofthe treatment of achalasia. It is well refer-enced and supplies much-needed infor-mation for treatment decisions. The ma-jor drawback is the attempt to compareclinical trials of different design. Thetreatment modalities and outcomes aredescribed in detail. The article supportseither dilation or surgical myotomy asprimary therapy in patients with achala-
420 CURRENT SURGERY • Volume 57/Number 5 • September/October 2000

of symptoms, their use is limited to patients who are poor candidates for other treat-ments.
Studies in which older dilators were used are no longer clinically valid. This includesthe only prospective, randomized trial comparing myotomy with balloon dilation.Currently, the most effective balloon dilator is the Rigiflex, which obtained good toexcellent results in 74% to 90% of patients and a perforation rate of 2%.
Surgical cardiomyotomy is reviewed as both an open and minimally invasive tech-nique. The open abdominal approach in a review of 2660 cases shows good to excellentresults in 83%, with a mean 6.6-year follow-up and reflux in 22%. Mortality was 0.2%.Open thoracic cardiomyotomy in a review of 1210 cases reveal good to excellent resultsin 83%, with a mean 7-year follow-up and 10% reflux. Mortality was 1%. The reviewof 82 patients who underwent thoracoscopic cardiomyotomy shows good to excellentresults in 84% with a mean 0.8-year follow-up and 50% reflux. No deaths occurred.The review of laparoscopic cardiomyotomy showed good to excellent results in 94%,with a 1-year follow-up and 11% reflux. No deaths occurred. These results wereinterpreted to favor laparoscopic cardiomyotomy with fundoplication as the treatmentof choice.
Studies comparing myotomy versus balloon dilation are reviewed and show similarinitial results with greater long-term failure of balloon dilation. Cost analysis indicatesthat initial treatment of achalasia with dilation and surgery for failures compared withinitial surgery resulted in decreased overall cost per patient from $10,800 (initialsurgery) to $3245 (initial dilation with surgery for nonresponders).
Botulinum toxin injection experience is reviewed with a total of 244 cases. Symptomimprovement decreased from an initial level of 85% to 42% by 1 year. In light of thelack of durable response, the authors do not favor botulinum toxin injection as primarytherapy for achalasia.
Conclusions: The authors conclude that symptomatic patients with achalasiashould be given the option of either graded pneumatic dilation or laparoscopic myot-omy. For pneumatic dilation failures, surgical myotomy through a laparoscopic ap-proach should be performed. For patients failing surgical myotomy, esophagectomyshould be considered. For those who are not surgical candidates, botulinum toxininjection may be used with nifedipine or isosorbide dinitrate for failures.
LAPAROSCOPIC HELLER’S MYOTOMY OR BOTULINUM TOXIN INJEC-TION FOR MANAGEMENT OF ESOPHAGEAL ACHALASIA: PATIENTCHOICE AND TREATMENT OUTCOMES. Andrews CN, Anvari M,Dobranowski J. Surg Endosc 1999;13:742–746.
Objective: Evaluate patient preference for laparoscopic Heller myotomy withoutfundoplication or botulinum toxin injection for the treatment of achalasia. Evaluatethe outcome of each treatment strategy.
Design: Prospective assessment of patients treated for achalasia by pretreatment andpost-treatment esophageal manometry, barium swallow, and dysphagia score. A singlesurgeon performed both treatments.
Setting: St. Joseph’s Hospital, McMaster University, Hamilton, Canada.
Participants: Twenty-two patients with idiopathic esophageal achalasia treated be-tween October 1993 and January 1998. Patients with coexisting esophageal pathologyfound on endoscopy were excluded. Four patients had treatment by esophageal dila-tion before entering the study.
Results: Eighteen patients chose botulinum toxin as initial therapy. Patients whochose botulinum toxin were significantly older (63 years vs 36 years) and had loweresophageal clearance than did those who opted for laparoscopic Heller myotomy. One
REVIEWER COMMENTS (Con’t)
sia. The pooled source data suggest thatthe laparoscopic route is preferred. Therate of reflux suggests the need for con-comitant fundoplication. However, nodirect comparison of fundoplicationtechniques or outcomes was presented.The authors also present a treatment al-gorithm based on their pooled data.
REVIEWER COMMENTS
Enthusiasm for the use of botulinumtoxin for achalasia is no doubt related tothe almost nonexistent risk of perforationassociated with its use compared withballoon dilation. An obvious flaw of thisstudy is the low number of patients. Be-cause the effects of botulinum toxin di-minishes over time and subsequent treat-ments are less likely to be effective,additional data would be more meaning-ful. Specifically, reporting the results ofadditional injection, duration of benefit,and percentage of patients with symp-tomatic relief at final follow-up would al-low a better comparison to laparoscopicHeller myotomy. As in other studies,botulinum toxin did not change bariumclearance or basal lower esophagealsphincter pressure, suggesting it may actonly to change esophageal sensation.
CURRENT SURGERY • Volume 57/Number 5 • September/October 2000 421

patient complained of chest pain after botulinum toxin injection. One mucosal per-foration occurred in the laparoscopic Heller myotomy group in a patient who hadundergone botulinum toxin injection. Five patients who were originally treated withbotulinum toxin underwent laparoscopic Heller myotomy a mean of 565 days afterinitial treatment. The operative time was longer in these patients than in those who hadnot received botulinum toxin. Seventy-eight percent of patients who received botuli-num toxin required additional injections. There were no treatment failures in thelaparoscopic Heller myotomy group. Patients who underwent botulinum toxin injec-tion had significant decrease in their dysphagia score and nadir lower esophagealsphincter (LES) pressure at 1 week and 2 months post-treatment. Body weight wassignificantly higher two months afterward. LES basal pressure and barium retentionwere not significantly changed. In the laparoscopic Heller myotomy patients, dyspha-gia score, basal and nadir LES pressures, and barium retention were significantly lower6 months after myotomy. Initial treatment by botulinum toxin injection did notchange these results. There was a statistically greater decrease in LES nadir and basalpressures and barium retention in laparoscopic Heller myotomy patients comparedwith botulinum toxin patients. Improvements in dysphagia score and weight gain werenot statistically different between the two treatments.
Conclusions: Botulinum toxin injection and laparoscopic Heller myotomy signifi-cantly reduce symptoms of achalasia. Only laparoscopic Heller myotomy reduces basalLES pressure and esophageal barium clearance. Recurrence of symptoms requiringadditional therapy is common with botulinum toxin injection. Younger patients favorlaparoscopic Heller myotomy. The efficacy of laparoscopic Heller myotomy is notchanged by previous botulinum toxin treatment.
LAPAROSCOPIC HELLER MYOTOMY AND FUNDOPLICATION FOR ACHA-LASIA. Hunter JG, Trus TL, Branum GD, Waring JP. Ann Surg 1997;225:655–665.
Objective: Review results of initial experience with laparoscopic cardiomyotomyand partial fundoplication for achalasia.
Design: A review of patients undergoing laparoscopic Heller myotomy and fundo-plication between August 1992 and November1996.
Setting: Emory University Hospital, Emory University School of Medicine, Atlanta,Georgia.
Participants: Forty patients underwent laparoscopic Heller myotomy and fundo-plication for a preoperative diagnosis of achalasia.
Results: All operations were completed laparoscopically with a mean operating timeof 199 6 36.2 minutes. Thirty-two patients underwent posterior fundoplication, and7 underwent anterior fundoplication. Thirty-seven patients were discharged less than72 hours after operation. Patients scored their symptoms preoperatively and postop-eratively on a 5-point scale (0 5 absent, 4 5 disabling). At a mean follow-up of 12.5months, dysphagia was eliminated or rare (score 0–1) in 90% (p , 0.001), andregurgitation was eliminated in 95% (p , 0.01). Statistically significant improvementswere seen in heartburn and chest pain (p , 0.01). Sixty-four percent of patients treatedbefore surgery by nonsurgical means reported greater improvement with cardiomyo-tomy. Mucosal perforation occurred in 6 (15%) patients. Postoperative complicationswere pneumonia in 2 patients and a bleeding gastroesophageal junction ulcer in 1patient.
Conclusions: Laparoscopic cardiomyotomy and fundoplication is a safe, effectiveprocedure for the treatment of achalasia.
REVIEWER COMMENTS (Con’t)
Botulinum toxin injection also served tomake subsequent myotomy more diffi-cult. Other authors have noted this. Be-cause of these factors, botulinum toxinshould be reserved for patients who arepoor candidates for balloon dilation orsurgery. Further study may show subsetsof patients who would obtain greaterbenefit from botulinum toxin.
REVIEWER COMMENTS
The transition from open to thoraco-scopic to laparoscopic cardiomytomy is arecent one. This article reviews the initialexperience with laparoscopic cardiomyo-tomy at a single institution. An excellenttechnical description of the operativetechnique is provided. The effectivenessand complication rate in this series com-pares favorably with other operative se-ries. Technical issues that should be fur-ther studied include what type offundoplication is the best antireflux pro-cedure to perform with cardiomytomy,does esophageal diameter affect whichtype of fundoplication should be per-formed, and what is the best way to de-termine intraoperatively the optimallength of the myotomy. As experiencewith this treatment increases, compari-son to modern balloon dilation with im-proved balloon technology will definewhat role laparoscopic Heller myotomywill have in the treatment of achalasia.
422 CURRENT SURGERY • Volume 57/Number 5 • September/October 2000

THORACOSCOPIC VERSUS LAPAROSCOPIC MODIFIED HELLER MYOT-OMY FOR ACHALASIA: EFFICACY AND SAFETY IN 87 PATIENTS. StewartKC, Finley RJ, Clifton HC, et al. J Am Coll Surg 1999;189:164–170.
Objective: To determine which minimally invasive approach to the modified Hellermyotomy, laparoscopic vs thoracoscopic is most efficacious in the treatment of acha-lasia.
Design: A retrospective review of all minimally invasive modified Heller myotomiesperformed at 2 hospitals between December 1991 and February 1998.
Setting: The Vancouver General Hospital, Vancouver, and Victoria Hospital, Lon-don, Canada.
Participants: Eighty-seven patients underwent minimally invasive modified Hellermyotomy, 24 undergoing thoracoscopic and 63 laparoscopic. Demographics weresimilar among groups, and all patients had preoperative dysphagia and regurgitation.The patients undergoing thoracoscopic did not undergo a concomitant antirefluxprocedure. Of the 63 patients that underwent laparoscopic, 8 did not have an antire-flux procedure, 53 had an anterior (Dor) fundoplication, and 2 had a posterior (Tou-pet) fundoplication. Two consultant (senior staff) general surgeons experienced inboth thoracic and abdominal esophageal surgery performed all of the operations. Theprocedure was determined by surgeon choice.
Results: Mean operating room times were 4.3 hours for thoracoscopic and 3.0 hoursfor laparoscopic. Three perforations (X%) occurred, and 5 patients (X%) were con-verted to open procedures in the thoracoscopic group. Reasons for conversion were torepair the perforations and inability to visualize the anatomy. Two perforations (Y%)occurred, and 1 patient (Y%) was converted to open in the laparoscopic group. Lengthof stay postoperatively averaged 6.1 days for thoracoscopic and 4.0 days for laparo-scopic. The authors noted that both the average operating room time and length of staydecreased significantly in the laparoscopic group between the first 24 and last 24procedures, whereas there was no significant difference in either length of stay oroperating room time in the thoracoscopic group between the first 12 and last 12procedures. Follow-up was available on 49 (78%) of laparoscopic (median 17 months)and 15 (63%) of thoracoscopic (median 42 months). No or minimal dysphagia waspresent in 44 out of 49 (90%) after laparoscopic and 4 out of 13 (31%) after thoraco-scopic. No or minimal heartburn was present in 41 out of 46 (89%) after laparoscopicand 8 out of 12 (67%) after thoracoscopic.
Conclusions: In this study, the laparoscopic approach to the modified Heller my-otomy has shorter operating room time, lower open conversion rate, and decreasedlength of stay when compared with the thoracoscopic approach. In addition, relief ofdysphagia and heartburn is better in the laparoscopic approach. Laparoscopic modifiedHeller myotomy may be the preferred approach to the surgical treatment of achalasia.
REVIEWER SUMMARY
Achalasia is an uncommon disorder of the esophagus characterized by a lack of primaryperistalsis and failure of relaxation of the lower esophageal sphincter.1 Although theorigin of the disease remains elusive, it results from destruction of the myenteric plexusneurons with accompanying motor dysfunction.2,3 Achalasia presents with symptomsof chest pain, heartburn, dysphagia, and regurgitation. Diagnosis is made by bariumswallow with fluoroscopy or esophageal manometry. Radiographic features includeaperistalsis, esophageal dilation, and “bird beak” appearance of the gastroesophagealjunction. Manometric findings are aperistalsis, incomplete relaxation of the loweresophageal sphincter and increased basal lower esophageal sphincter pressures. Esopha-gogastroduodenoscopy is necessary to rule out pseudoachalasia caused by malignancy
REVIEWER COMMENTS
The authors present a large series of min-imally invasive modified Heller myot-omies. Although not stated, it appearsthat most of the thoracoscopically per-formed procedures occurred early in theirexperience (mean follow-up for thoraco-scopic was 42 months, as compared with17 months for laparoscopic). They feltstrongly that experience significantly de-creased operating room time and lengthof stay in the laparoscopic group, whereasin the thoracoscopic group, no similarbenefit was seen. The larger number oflaparoscopic vs thoracoscopic (63 vs 24)seems to indicate that they favor the lapa-roscopic approach. The decreased lengthof stay, operating room time, and conver-sion rate, coupled with superior relief ofsymptoms seems to justify this prefer-ence. No comparison of postoperativesymptoms was made among the differentsubgroups of laparoscopic (anterior fun-doplication vs posterior fundoplicationvs no antireflux procedure). Unfortu-nately, the retrospective nature of thisstudy, relatively incomplete follow-updata, and the lack of postoperative phys-iologic testing does not lend compellingpower to the study. Nonetheless, the au-thors offer additional evidence that thelaparoscopic modified Heller myotomy,coupled with an antireflux procedure, ap-pears to be the preferred surgical treat-ment for achalasia. Further study isneeded to determine which antirefluxprocedure is optimal using the laparo-scopic approach.
CURRENT SURGERY • Volume 57/Number 5 • September/October 2000 423

at the gastroesophageal junction. The use of whalebone and sponge dilation for thetreatment of achalasia was described in 1674.4 Ernst Heller performed the first surgicalcardiomyotomy in 1913.5 Modern treatments focus on decreasing the lower esopha-geal sphincter pressure and include the use of drugs, botulinum toxin, balloon dilation,surgical myotomy, and, in rare circumstances, esophagectomy. Although laparoscopicmodified Heller myotomy appears to offer the highest rate of symptom resolution anddurability, balloon dilation may be the most cost-effective initial therapy in the treat-ment of achalasia.6
MEDICAL THERAPY
The whalebone and sponge have been replaced by 3 major medical therapies: calciumchannel blockers, balloon dilation, and botulinum toxin injection. Calcium channelblockers work by lowering resting lower esophageal sphincter pressure. Several studies,most using sublingual nifedipine, show a temporary decrease in lower esophagealsphincter pressure by 13% to 46%.7–9 Patients improved in 53% to 77%; however,symptom improvement is generally incomplete, and the response is short lived. Sideeffects include ankle edema, headaches, nausea, and dizziness. Pasricha et al10 de-scribed injection of the lower esophageal sphincter with botulinum toxin as a treatmentfor achalasia in 1995. The toxin inhibits calcium-dependent release of acetylcholinefrom motor nerve endings, resulting in smooth muscle relaxation. Many studies showan average initial symptom relief rate of 85%, which drops to 42% at 6 months.11
Pneumatic dilation is typically performed to a diameter of 3.5 cm to 4.5 cm. Severalprospective studies have shown good to excellent results in 61% to 84%.12–14 Perfo-ration rates are reported in collective reviews of about 2.5% and generally requiresurgical repair.11 Botulinum toxin injection was compared with dilation by Vaezi etal,15 with a similar 1-month response of 64% vs 75%. However, at 12 months, thesymptom improvement of botulinum toxin was 32% vs 70% for dilation. In patientsreceiving botulinum toxin injection before cardiomyotomy, increased technical diffi-culties and operative times have been reported.16,17 In light of inferior long-termresults and possible increased future surgical risks, pneumatic dilation appears to be thesuperior medical therapy.
SURGICAL MANAGEMENT
Since Heller’s original description of simultaneous anterior and posterior cardiomyo-tomies for the surgical treatment of achalasia, his operation has been modified toinclude only the anterior myotomy. This modified Heller myotomy is an effective anddurable treatment for achalasia. A prospective, randomized trial of dilation vs surgicalmyotomy resulted in 5-year symptom improvement of 51% vs 95%.12 The modifiedHeller myotomy may be performed through the chest or abdomen. Reported results ofthe abdominal compared with the thoracic approach show the 2 procedures to offerequal symptom relief.18 The rate of reflux is about twice as high when performedthrough the abdomen (22% vs 10%).11 This increased reflux is felt to be caused by thedisruption of the phrenoesophageal ligament when the operation is performed throughthe abdomen. The addition of a partial fundoplication, such as the Dor or Toupetprocedure, seems to significantly reduce the reflux.19 Minimally invasive modifiedHeller myotomy appears to offer the same relief of symptoms and patient satisfactionas the open surgical approach with the advantages of less pain, postoperative disability,and shorter hospital stay.11,20 The reviewed article by Stewart et al supports laparo-scopic modified Heller myotomy with partial fundoplication as the procedure ofchoice for the surgical treatment of achalasia.
CONCLUSIONS
Because of the low success rate, calcium channel blockers and botulinum toxin shouldbe used only in those patients who are either not candidates for or refuse pneumatic
424 CURRENT SURGERY • Volume 57/Number 5 • September/October 2000
dilation or surgery. The modified Heller myotomy, coupled with a partial fundopli-cation, provides the highest success rate and patient satisfaction for uncomplicatedachalasia. The laparoscopic approach appears to be the preferred method of accom-plishing the aforementioned procedure. Even in advanced cases of achalasia withsigmoid esophagus, laparoscopic modified Heller myotomy should be attempted.21
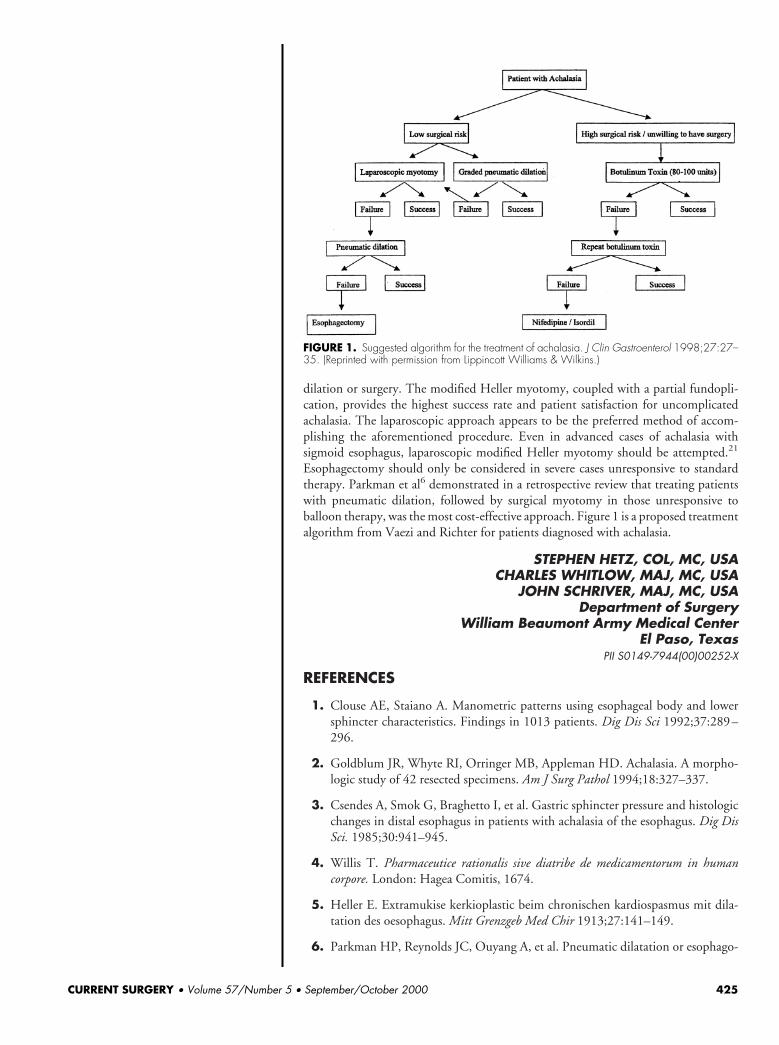
Esophagectomy should only be considered in severe cases unresponsive to standardtherapy. Parkman et al6 demonstrated in a retrospective review that treating patientswith pneumatic dilation, followed by surgical myotomy in those unresponsive toballoon therapy, was the most cost-effective approach. Figure 1 is a proposed treatmentalgorithm from Vaezi and Richter for patients diagnosed with achalasia.
STEPHEN HETZ, COL, MC, USACHARLES WHITLOW, MAJ, MC, USA
JOHN SCHRIVER, MAJ, MC, USADepartment of Surgery
William Beaumont Army Medical CenterEl Paso, Texas
PII S0149-7944(00)00252-X
REFERENCES
1. Clouse AE, Staiano A. Manometric patterns using esophageal body and lowersphincter characteristics. Findings in 1013 patients. Dig Dis Sci 1992;37:289–296.
2. Goldblum JR, Whyte RI, Orringer MB, Appleman HD. Achalasia. A morpho-logic study of 42 resected specimens. Am J Surg Pathol 1994;18:327–337.
3. Csendes A, Smok G, Braghetto I, et al. Gastric sphincter pressure and histologicchanges in distal esophagus in patients with achalasia of the esophagus. Dig DisSci. 1985;30:941–945.
4. Willis T. Pharmaceutice rationalis sive diatribe de medicamentorum in humancorpore. London: Hagea Comitis, 1674.
5. Heller E. Extramukise kerkioplastic beim chronischen kardiospasmus mit dila-tation des oesophagus. Mitt Grenzgeb Med Chir 1913;27:141–149.
6. Parkman HP, Reynolds JC, Ouyang A, et al. Pneumatic dilatation or esophago-
FIGURE 1. Suggested algorithm for the treatment of achalasia. J Clin Gastroenterol 1998;27:27–35. (Reprinted with permission from Lippincott Williams & Wilkins.)
CURRENT SURGERY • Volume 57/Number 5 • September/October 2000 425
myotomy treatment for idiopathic achalasia: clinical outcomes and cost analysis.Dig Dis Sci 993;38:75–85.
7. Hongo M, Traube M, McAllister RG, McCallum RW. Effects of nifedipine onesophageal motor function in humans: correlation with plasma nifedipine con-centration. Gastroenterology 1984;86:8–12.
8. Traube M, Hongo M, Magyar L, McCallum RW. Effects of nifedipine in acha-lasia in patients with high amplitude peristaltic esophageal contractions. JAMA1984;252:1733–1736.
9. Bortolotti M, Labo G. Clinical and manometric effects of nifedipine in patientswith esophageal achalasia. Gastroenterology 1981;80:39–44.
10. Pasricha PJ, Ravich WJ, Henrix TR, et al. Intraspinteric botulinum toxin for thetreatment of achalasia. N Engl J Med 1995;322:774–778.
11. Vaezi MF, Richter JE. Current therapies for achalasia: comparison and efficacy.Clin Gastroenterol 1998;27:21–35.
12. Csendes A, Braghetto I, Henriquez A, Cortes C. Late results of a prospectiverandomized study comparing forceful dilatation and esophagomyotomy in pa-tients with achalasia. Gut 1989;30:299–304.
13. Heimlich HJ, O’Connor TW, Flores DC. Case for pneumatic dilatation inachalasia. Ann Otol 1978;87:519–522.
14. Eckhardt VF, Aignherr C, Bernhard C. Predictors of outcome in patients withachalasia treated by pneumatic dilation. Gastroenterology 1992;103:1732–1738.
15. Vaezi M, Richter J, Wilcox M, Schroeder P, Slaughter R. One-year follow-up:pneumatic dilatation more effective than botulinum toxin [abstract]. Gastroen-terology 1997;112:A318.
16. Horgan S, Hudda K, Eubanks T, McAllister J, Pellegrini CA. Does botulinumtoxin injection make esophagomytomy a more difficult operation? Surg Endosc1999;13:576–579.
17. Andrews CN, Anvari M, Dobranowski J. Laparoscopic Heller’s myotomy orbotulinum toxin injection for management of esophageal achalasia. Surg Endosc1999;13:742–746.
18. Hunter JG, Richardson WS. Surgical management of achalasia. Surg Clin NorthAm 1997;77:993–1015.
19. Bonavina L, Nosadini A, Bardini R, Baessato M, Peracchia A. Primary treatmentof esophageal achalasia: long-term results of myotomy and Dor fundoplication.Arch Surg 1992;127:222–227.
20. Dempsey DT, Kalan MM, Gerson RS, Parkman HP, Maier WP. Comparison ofoutcomes following open and laparoscopic esophagomyotomy for achalasia. SurgEndosc 1999;13:747–750.
21. Patti MG, Feo CV, Diener U, et al. Laparoscopic Heller myotomy relievesdysphagia in achalasia when the esophagus is dilated. Surg Endosc 1999;13:843–847.
426 CURRENT SURGERY • Volume 57/Number 5 • September/October 2000




























