Embed Size (px)
Citation preview

Accuracy of mammographic fine-needle aspiration
appearances after breast
William H. Hindle, MD, a' b and Emy C. Chen, BA a
Los Angeles, California
OBJECTIVE: The objective of this study was to document the observation that fine-needle aspiration of palpable breast masses by use of a modified technique performed shortly before mammography need not adversely interfere with mammographic interpretation nor produce falsely suspicious mammographic lesions that delay meaningful evaluation and management in this breast clinic. STUDY DESIGN: In a retrospective record review 1007 women who were seen in the Breast Diagnostic Center at Women's and Children's Hospital from January 1992 until April 1995 and who had fine-needle aspiration of a palpable solid breast mass within 2 weeks before mammography were analyzed overall and in 10-year age group subsets. The mammographic reports of "suspicious" lesions were correlated with having had a prior fine-needle aspiration (within 2 weeks). RESULTS: Of the 1007 women undergoing fine-needle aspirations, 91 had a cytologic or tissue biopsy specimen diagnosis of malignancy. Of these, 72 had "suspicious" mammograms and 19 had "nonsuspicious" mammograms. The calculated positive predictive value was 58%. The negative predictive value was 98%. Mammographic sensitivity was 79%. Specificity was 94%. Age stratification did not reveal any meaningful trends. Of the 916 patients with benign cytologic results of fine-needle aspiration specimens, 52 had "suspicious" mammograms and 864 had "nonsuspicious" mammograms. CONCLUSION: For patient convenience and expeditious diagnosis of a palpable breast mass, fine- needle aspiration can be performed on the initial visit and mammograms subsequently taken within 2 weeks without undue clinical confusion or misleading mammographic findings. Concordance of the diagnostic triad consisting of (1) clinical impression (by history and examination), (2) fine-needle aspiration, and (3) mammography gives a reliable conclusion and can appropriately be used as the basis for clinical management of a breast mass. However, when there is doubt or anxiety about the diagnosis either on the part of the patient or the physician, a definitive histologic tissue diagnosis should obtained. (Am J Obstet Gynecol 1997;176:1286-92.)
Key words: Fine-needle aspiration, mammography, breast cancer, palpable breast mass
Fine-needle aspiration and mammography are essential components of the diagnostic triad (also known as triple diagnosis, triple test, or triple assessment) consisting of clinical breast examination, fine-needle aspiration, and mammography for evaluation of a palpable dominant breast mass. Previous studies have repor ted that the timing and sequence of fine-needle aspiration affects the accuracy of the mammographie readings? ' 2 Needle lo- calization procedures have been shown to produce he- matomas, ~ which presumably account for the perceived mammographic changes that may be seen when a mam- mogram is taken within 2 weeks of fine-needle aspiration.
From the Department of Obstetrics and Gynecology, University of Southern California School of Medicine, a and the Breast Diagnostic Center, Women's and Children's Hospital, Los Angeles County-Univer- sity of Southern California Medical Center. b Presented at the Sixty-third Annual Meeting of the Pacific Coast Obstetrical and Gynecological Society, Sunriver, Oregon, October 2-6, 1996. Reprint requests: William H. Hindle, MD, Women's and Children's Hospital, L-1022, 1240 N. Mission Road, Los Angeles, CA 90033. Copyright © 1997 by Mosby-Year Book, Inc. 0002-9378/97 $5.00 + 0 6/6/80919
However, for patient convenience (and compliance) some physicians and breast clinics have mammograms taken on the same day that the fine-needle aspiration is performed. Does this adversely affect the evaluation of a palpable breast mass? Horobin et al. 4 compared mam- mograms done before and after fine-needle aspirations and found changes in 3 of 52. However, it was concluded that the difference did not alter the final mammographic diagnosis. Harlow et al., 5 in an ultrasonography study of presumed hematoma and edema after tissue core-needle breast biopsy, concluded that ultrasonographic changes do occur (7/31) but that the changes are not adversely meaningful in the final ultrasonography interpretation. On the other hand, Svensson et al. 6 noted ultrasono- graphic features suggestive of malignancy in 18% of women after fine-needle aspiration. Barzilai 7 repor ted a case of bleeding into a cyst after fine-needle aspiration, which gave the ultrasonographic appearance of an intra- cystic mass. These studies underscore the necessity of having the consultant mammographer-ul t rasonographer made aware of the per t inent clinical information (par-
1286

Volume 176, Number 6 Hindte and Chen 1287 AmJ Obslet Oynecol
ticularly the prior performance of fine-needle aspira-
tion) to correlate the imaging findings before the final written report. Correlation of the information obtained by the diagnostic triad is critical for appropriate clinical evaluation and management.
Material and methods
A retrospective chart review was performed of the women
seen at the Breast Diagnostic Center at Women's and Children's Hospital, Los Angeles County-University of
Southern California Medical Center, Los Angeles, from
January" 1992 to April 1995. The demographics of the ambulatory-care patients seen in Women's and Chil-
dren's Hospital (1992) showed an age range of 12 to 73 years with a mean of 33.1 years. The ethnicity was 79.0% Hispanic:, 12.5% white, 5.8% black, 1.4% Asian, and 1.3%
others as designated by the Los Angeles County Health Services. During the study period 5577 women were seen in the Breast Diagnostic Center, of whom 1424 (25%) had fine-needle aspiration performed on a palpable dominant breast mass. Except for those who had previ-
ous (original) mammographic fihns taken within 1 year, all women ~>25 years old in accordance with our clinical
protocol, had mammograms as a component of the
diagnostic triad workup. Reports were available on 1007 women (aged 14 to 82 years with a mean age of 33.7
years) who had a mammogram within 2 weeks of fine- needle aspiration of a palpable dominant breast mass; most had the mammogram within 2 hours of the fine- needle aspiration. The other 417 women did not have a
mammogram taken within 2 weeks of the fine-needle aspiration. The remaining 4570 women (aged 14 to 91 years with a mean age of 45.0 years) did not have a
palpable dominant breast mass by examination and therefore did not have fine-needle aspiration.
At the Breast Diagnostic Center fine-needle aspiration of a palpable dominant mass is most often performed
with a 22-gauge, 1-inch needle by use of the needle-alone technique, s Single-pass fine-needle aspirations are per-
formed by obstetrics and gynecology resident physicians (under faculty supervision) who rotate through the ob- stetrics and gynecology breast service. When microscopic
evaluation shows that a paucity of cellular material has been obtained, a second procedure is performed with a
10 ml syringe and a small plastic syringe holder. ~ This approach is in contrast to the classic fine-needle aspira- tion technique used at the Karolinska Aspiration Clinic (Stockholm) described by Zajicek et al. 1° and illustrated by Frable. 11
After the mass is palpated, the aspirator uses the index and middle fingers of the nonaspirating hand to trap the mass under the taut skin and immobilize it over a rib. The skin is then cleaned with an alcohol wipe and the needle is inserted at a slightly slanted angle (close to perpendicular). When the needle reaches the middle of
the mass, it is moved up and down in quick thrusts (30
times with the needle-alone technique, 20 times when using negative pressure in a syringe with a syringe holder) while the tip of the needle remains within the mass. After removal of the needle, a 4 × 4- inch sterile
gauze pad is folded on itself into fourths and used to apply pressure over the puncture site for -->2 minutes. This pressure minimizes hematoma formation within the breast tissue and usually eliminates ecchymosis forma-
tion in the skin. The cellular material collected in the
needle is quickly ejected (by air in a syringe) onto a slide,
which is immediately fixed (or alternately air dried) and subsequently stained. The patient has a mammogram the
same day (usually within 2 hours) or as soon as possible thereafter. With this technique, patients rarely complain
of tenderness at the fine-needle aspiration site or of increased discomfort during subsequent mammographic compression.
The 1007 cases in this study were taken from comput- erized mammography reports of women who had a fine-needle aspiration of a palpable solid breast mass
and a mammogram within 2 weeks of the procedure. For the purpose of this analysis the mammogram reports
were classified as "suspicious" if a perceived abnormality,
in the area of the palpable mass was recorded as suspi- cious for malignancy (code 4) or "highly suspicious" for
malignancy (code 5) and as "nonsuspicious" (codes 1, 2, 3, and 6, Table I). The fine-needle aspiration cytology and biopsy final reports were correlated with the mam-
mographic readings to determine the clinical accuracy
of the mammograms performed after the fine-needle aspirations.
Results
Of the 1007 fine-needle aspirations reviewed in this
study, 91 (0.09%) were diagnostic of malignancy (Table
II). The remaining 916 women had nonmalignant (be- nign) conditions by cytologic diagnosis. Of these, 864 had "nonsuspicious" mammograms and 52 had "suspi-
cious" mammograms. Mammogram reports were divided into those recorded as radiologically "suspicious" (codes 4 and 5) or "nonsuspicious" for those recorded as showing no evidence of malignancy (codes 1, 2, 3, and 6). The 72 true-positive* results were in women diag-
nosed with cancer by fine-needle aspiration who had "suspicious" mammograms after the fine-needle aspira-
tion. Similarly, 864 women had nonmalignant lesions and mammograms without perceived "suspicious" le-
*The cytologic (fine-negdle aspiration) diagnosis of malig- nancy was used as the basis for these calculations. Histologic confirmation of the malignant diagnosis was confirmed in all 72 of the mammographic "true positives" and in all 19 of the mammographi.c "false negatives." No "missed" carcinomas were identified. All patients were instructed to return if the lesions progressed or recurred. However, with this indigent population follow-up is problematic.
1288 Hindle and Chen June 1997 Am J Obstet Gynecol
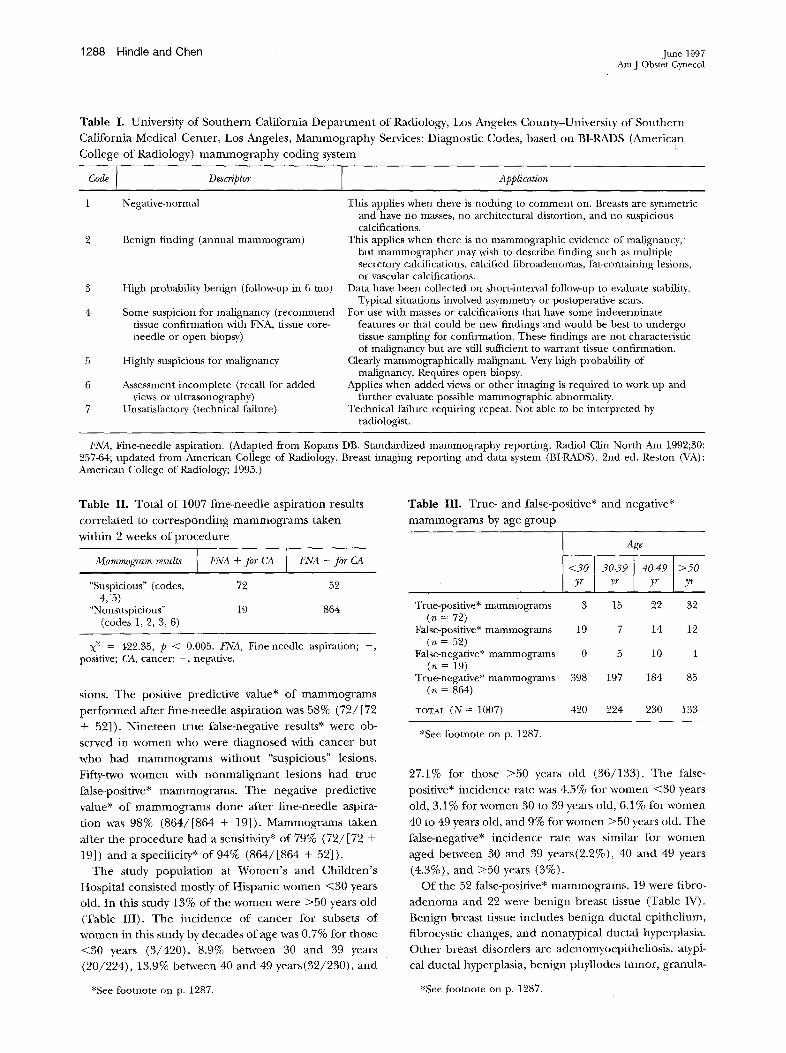
Table I. University of Southern California Depa r tmen t of Radiology, Los Angeles County-Univers i ty of Southern
California Medical Center , Los Angeles, Mammography Services: Diagnostic Codes, based on BI-RADS (American
College of Radiology) m a m m o g r a p h y coding system
Code I Descriptor [ Application
1 Negative-normal This applies when there is nothing to comment on. Breasts are symmetric
Benign finding (annual mammogram)
High probability benign (follow-up in 6 too)
Some suspicion for malignancy (recommend tissue confirmation with FNA, tissue core- needle or open biopsy)
Highly suspicious for malignancy
Assessment incomplete (recall for added views or ultrasonography)
Unsatisfactory (technical failure)
and have no masses, no architectural distortion, and no suspicious calcifications.
This applies when there is no mammographic evidence of malignancy, but mammographer may wish to describe finding such as multiple secretory calcifications, calcified fibroadenomas, fat-containing lesions, or vascular calcifications.
Data have been collected on short-interval follow-up to evaluate stability. Typical situations involved asymmetry or postoperative scars.
For use with masses or calcifications that have some indeterminate features or that could be new findings and would be best to undergo tissue sampling for confirmation. These findings are not characteristic of malignancy but are still suificient to warrant tissue confirmation.
Clearly mammographically malignant. Very high probability of malignancy. Requires open biopsy.
Applies when added views or other imaging is required to work up and further evaluate possible mammographic abnormality.
Technical failure requiring repeat. Not able to be interpreted by radiologist.
FNA, Fine-needle aspiration. (Adapted from Kopans DB. Standardized mammography reporting. Radiol Clin North Am 1992;30: 257-64; updated from American College of Radiology, Breast imaging reporting and data system (BI-RADS). 2nd ed. Reston (VA) : American College of Radiology; 1995.)
Table II. Total of 1007 f ine-needle aspiration results
corre la ted to cor responding m a m m o g r a m s taken
within 2 weeks of p rocedure
Mammogram results FNA + for CA FNA - for CA
"Suspicious" (codes, 72 52 4, 5)
"Nonsuspicious" 19 864 (codes 1, 2, 3, 6)
X 2 = 422.35, p < 0.005. FNA, Fine-needle aspiration; +, positive; CA, cancer; - , negative.
sions. The positive predictive value* of m a m m o g r a m s
p e r f o r m e d after f ine-needle aspiration was 58% (72/ [72
+ 52]). N ine teen true false-negative results* were ob-
served in w o m e n who were diagnosed with cancer but
who had m a m m o g r a m s without "suspicious" lesions.
Fifty-two w o m e n with nonma l ignan t lesions had true
false-positive* mammograms . The negative predictive
value* of mamrnograms done after f ine-needle aspira-
t ion was 98% (864/ [864 + 19]). Mammograms taken
after the p rocedure had a sensitivity* of 79% (72/ [72 +
19]) and a specificity* o f 94% (864/ [864 + 52]).
The study popula t ion at W o m e n ' s and Chi ldren ' s
Hospital consisted mostly of Hispanic w o m e n <30 years
old. In this study 13% of the women were >50 years old
(Table III). The inc idence of cancer for subsets of
w o m e n in this study by decades of age was 0.7% for those
<30 years (3/420) , 8.9% between 30 and 39 years
(20/224) , 13.9% between 40 and 49 years(32/230) , and
Table III. True- and false-positive* and negative*
m a m m o g r a m s by age group
Age
<30 lyr 30-39 l y r 40-491>50yr yr
True-positive* mammograms 3 15 22 32 (n = 72)
False-positive* mammograms 19 7 14 12 (n = 52)
False-negative* mammograms 0 5 10 4 (n = 19)
True-negative* mammograms 398 197 184 85 (n = 864)
TOTAL (N = 1007) 420 224 230 133
*See footnote on p. 1287.
27.1% for those >50 years old (36/133) . The false-
positive* inc idence rate was 4.5% for w o m e n <30 years
old, 3.1% for w o m e n 30 to 39 years old, 6.1% for women
40 to 49 years old, and 9% for w o m e n >50 years old. The
false-negative* inc idence rate was similar for w o m e n
aged between 30 and 39 years(2.2%), 40 and 49 years
(4.3%), and >50 years (3%).
Of the 52 false-positive* mammograms , 19 were fibro-
a d e n o m a and 22 were ben ign breast tissue (Table IV).
Benign breast tissue includes ben ign ductal epi thel ium,
fibrocystic changes, and nonatypical ductal hyperplasia.
O the r breast disorders are adenomyoepithel iosis , atypi-
cal ductal hyperplasia, ben ign phyllodes tumor, granula-
*See footnote on p. 1287. *See footnote on p. 1287.
Volume 176, Number 6 Hinctle and Chen 1289 Am J Obstet Gynecol
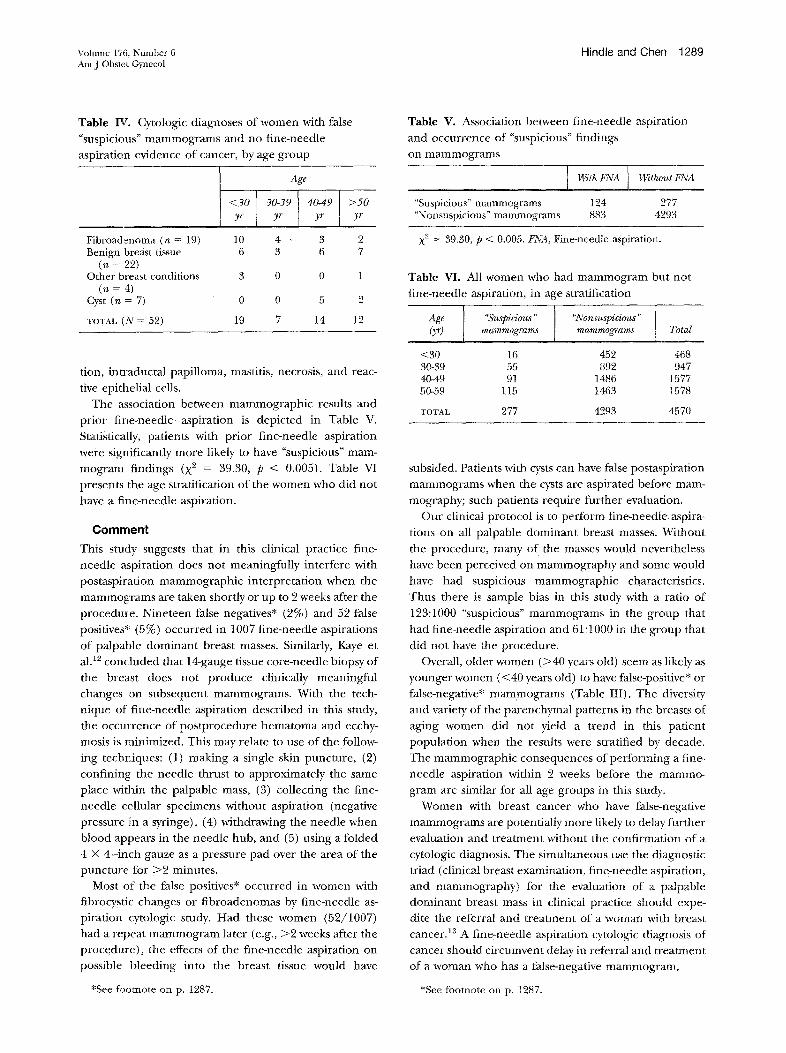
Table IV. "suspicious" mammograms and no fine-needle
aspiration evidence of cancer, by age group
Age
<30 30-39 I 40-49 >50 yr yr [ yr
Cytologic diagnoses of women with false
yr
Fibroadenoma (n = 19) 10 4 • 3 2 Benign breast tissue 6 3 6 7
(n = 22) Other breast conditions 3 0 0 1
(n = 4) Cyst (n = 7) 0 0 5 2
TOTAL (N = 52) 19 7 14 12
tion, intraductal papilloma, masntis, necrosis, and reac-
tive epithelial cells. The association between mammographic results and
prior fine-needle aspiration is depicted in Table V.
Statistically, patients with prior fine-needle aspiration
were significantly more likely to have "suspicious" mam- mogram findings (X 2 = 39.30, p < 0.005). Table VI
presents the age stratification of the women who did not
have a fine-needle aspiration.
Comment
This study suggests that in this clinical practice tine- needle a:~piration does not meaningfully interfere with postaspiration mammographic interpretation when the
mammograms are taken shortly or up to 2 weeks after the
procedure. Nineteen false negatives* (2%) and 52 false positives* (5%) occurred in 1007 fine-needle aspirations
of palpable dominant breast masses. Similarly, Kaye et al. 12 concluded that 14-gauge tissue core-needle biopsy of the breast does not produce clinically meaningful changes on subsequent mammograms. With the tech- nique of fine-needle aspiration described in this study,
the occurrence of postprocedure hematoma and ecchy- mosis is minimized. This may relate to use of the follow-
ing techrAques: (1) making a single skin puncture, (2) confining the needle thrust to approximately the same place within the palpable mass, (3) collecting the fine- needle cellular specimens without aspiration (negative
pressure in a syringe), (4) withdrawing the needle when blood appears in the needle hub, and (5) using a folded 4 × 4-imzh gauze as a pressure pad over the area of the puncture for >2 minutes.
Most o~ the false positives* occurred in women with fibrocystic changes or fibroadenomas by fine-needle as- piration cytologic study. Had these women (52/1007) had a repeat mammogram later (e.g., >2 weeks after the procedure), the effects of the fine-needle aspiration on possible bleeding into the breast tissue would have
Table V. Association between fine-needle aspiration
and occurrence of "suspicious" findings
on mammograms
With FNA I Without FNA
"Suspicious" mammograms 124 277 "Nonsuspicious" mammograms 883 4293
X 2 = 39.30, p < 0.005. FNA, Fine-needle aspiration.
Table VI. All women who had mammogram but not
fine-needle aspiration, in age stratification
Age "Suspicious . . . . Nonsuspicious " O,r) m a m m o g r a m s mamrao~'ams Total
<30 16 452 468 30-39 55 892 947 40-49 91 1486 1577 50-59 115 1463 1578
TOTAL 277 4293 4570
subsided. Patients with cysts can have false postaspiration
mammograms when the cysts are aspirated before mam- mography; such patients require further evaluation.
Our clinical protocol is to perform fine-needle aspira- tions on all palpable dominant breast masses. Without
the procedure, many of the masses would nevertheless
have been perceived on mammography and some would have had suspicious mammographic characteristics.
Thus there is sample bias in this study with a ratio of
123:1000 "suspicious" mammograms in the group that had fine-needle aspiration and 61:1000 in the group that
did not have the procedure. Overall, older women (>40 years old) seem as likely as
younger women (<40 years old) to have false-positive* or
false-negative* mammograms (Table III). The diversity and variety of the parenchymal patterns in the breasts of
aging women did not yield a trend in this patient population when the results were stratified by decade. The mammographic consequences of performing a fine-
needle aspiration within 2 weeks before tile mammo- gram are similar for all age groups in this study.
Women with breast cancer who have false-negative
mammograms are potentially more likely to delay further evaluation and treatment without the confirmation of a cytologic diagnosis. The simultaneous use the diagnostic triad (clinical breast examination, fine-needle aspiration, and mammography) for the evaluation of a palpable dominant breast mass in clinical practice should expe- dite the referral and treatment of a woman with breast
cancer. 13 A fine-needle aspiration cytologic diagnosis of cancer should circumvent delay in referral and treatment of a woman who has a false-negative mammogram.
*See footnote on p. 1287. *See footnote on p. 1287.

1290 Hindle and Chen June 1997 Am J Obstet Gynecol
Fine-needle aspiration performed by the modified 22-gauge needle-alone technique described in this study
does not cause clinically meaningful hematomas or alter- ations in the mammographic appearance when the mam-
mograms are taken shortly (up to within 2 weeks) after the aspiration procedure. The percentage of false-nega-
tive and false-positive mammograms was small and did not interfere with the clinical evaluation and manage-
ment of a breast mass when the diagnostic triad of clinical breast examination, fine-needle aspiration, and
mammography was used. Women <40 years old were just
as likely to have these false mammograms as were women >40 years old.
We thank the following for their input and critique of this article: Dr. Sue Ellen Martin, Director of Cytology, University of Southern California-Norris Breast Center; Dr. Richard J. Paulson, Chief, Endocrine-Infertility Divi- sion, Department of Obstetrics and Gynecology, and Dr. John G. Pearce, Chief of Radiology and Director of the University of Southern California Mammography Ser- vices of the Los Angeles County-University of Southern California Medical Center; and Dr. Dorit D. Adler, Associate Director, Division of Breast Imaging, University of Michigan Medical Center.
REFERENCES
1. Klein DL, Sickles EA. Effects of needle aspiration on the mammographic appearance of the breast: a guide to the proper timing of the mammography examination. Radiol- ogy 1982;145:44.
2. Sickles EA, Klein DL, Goodson WH, Hunt TK. Mammogra- phy after needle aspiration of palpable breast masses. Am J Surg 1983;145:395-7.
3. Sistrom CL, de Paredes ES, Abbitt PL, Wilhehn MC. Breast hematoma following needle localization: case report. Va Med 1988;115:78-9.
4. HorobinJM, Matthew BM, Preece PE, Thompson AJ. Effects of fine needle aspiration on subsequent mammograms. BrJ Surg 1992;79:52-4.
5. Harlow CL, Schackmuth EM, Bregman PS, Zeligman BE, Coffin CT. Sonographic detection of hematomas and fluid after imaging guided core breast biopsy. J Ultrasound Med 1994;13:877-82.
6. Svensson WE, Tohno E, Cosgrove DO, Powles TJ, A1 Mur- rani B, Jones AL. Effects of fine-needle aspiration on the US appearance of the breast. Radiology 1992;185:709-11.
7, Barzilai M. The impact of fine-needle aspiration on a palpable breast mass on the sonographic features of the lesion. Breast Dis 1995;8:315-8.
8, Zajdela A, Zillhardt P, Voillemot N. Cytological diagnosis by fine needle sampling without aspiration. Cancer 1987;59: 1201-5.
9. Hindle WH, Payne PA, Pan EY. The use of fine-needle aspiration in the evaluation of persistent palpable dominant breast masses. Am J Obstet Gynecol 1993;168:1814-9.
10. Zajicek J; Franzen S, Jakobsson P, Rubio C, Unsgaard B. Aspiration biopsy of mammary tumors in diagnosis and research--a critical review of 2,200 cases. Acta Cytol 1967; 11:169-75.
11. Frable WJ. Thin-needle aspiration biopsy: a personal expe- rience with 469 cases. AmJ Clin Pathol 1976;65:168-82.
12. Kaye MD, Vicinanza-Admni CA, Sullivan ML. Mammo- graphic findings after stereotaxic biopsy of the breast per- formed with large-core needles. Radiology 1994;192:149-51.
13. Hindle WH. The diagnostic evaluation. Obstet Gynecol Clin North Am 1994;21:499-517.
Editors' note: This manuscript was revised after these discussions were presented.
Discussion
DR. HOWARD G. McQuaRRI~, Salt Lake City, Utah. Dr. Hindle is well known to have advocated the triad of diagnostic elements for managing palpable breast masses with clinical palpation, fine-needle aspiration, and mam- mography. The sequential order of evaluation has been selected for patient convenience and expedited cyto- pathologic interpretation to reach an early diagnosis. The ability to provide this service is clearly related to the motivation of the directors, the cytopathologist, and the imaging service. It has proved to be functional and efficient in the author's hands. The clinical palpation will give information about the size of the lesion and the fine-needle aspiration will define the cytopathologic fea- tures. The role for mammography, with knowledge of cytopathologic characteristics and size of the mass ac- complished, is not explained. If the mammogram is to detect nonpalpable disease, the timing of the fine-needle aspiration will make no difference to the interpretation of the mammography. If the mammogram is for evalua- tion of the palpable mass itself, there are other observa- tions.
The result of this retrospective study shows a 94% sensitivity of the mammogram, or a false-negative and false-positive mammogram rate of 6%. The authors state that this did not interfere with the evaluation and management of the patient. The rnammography litera- ture suggests that a false-negative mammogram may occur in up to 10% to 15% of the nonpalpable breast cancers. Screening mammography accuracy, however, is improving and progressively detecting nonpalpable can- cers in increased frequency, because of public awareness programs and advanced technology. Fine-needle aspira- tion, although not discussed, may adversely affect the value of breast ultrasonography, an adjunctive tool used to delineate between cystic and solid masses. It has been reported that the false-positive ultrasonographic changes may be as high as 21% if a fine-needle aspiration is done before the ultrasonographic study, particularly in the younger woman with benign mastopathy.
This study importantly demonstrates, in motivated and interested clinicians, a sequence of evaluations is predict- ably accurate and the findings usable for determining clinical management of palpable breast masses in women. One wonders, however, if an alternative se- quence to compare examination, mammography, and then fine-needle aspiration would not be also reasonable, preserving the more accurate use of breast ultrasonogra- phy if needed for the diagnostic imaging and definition. The fine-needle aspiration, if the mammogram is being done to further evaluate the mass, may also be directed with ultrasonographic guidance. This may achieve an even more favorable diagnostic outcome.

Volume 176, Number 6 Hindle and Chen t291 Am J Obstet Gynecol
Because chart retrieval is so impressive, this question might be determined by broadening the retrospective search to include a control arm or by using this study to design a prospective study to clarify the question with a control group.
I have, the following questions. (1) For what purpose is the mammogram performed when the clinical sizing and cytopathologic study results are available? (2) Would it have been feasible to retrospectively find a control group, age related, to compare the outcome of a differ- ent sequence (i.e., clinical evaluation, mammography, and then fine-needle aspiration) to avoid the small but important false-positive and false-negative mammogra- phies? t3) Although small with mammography, and more importantly with uhrasonography, is the sequence of fine-needle aspiration before mammography (and possibly uhrasonography) worth the risk of even a small false-positive and false-negative image from both an economic and quality of an outcome when the mammog- raphy is used to evaluate only the palpable breast mass? (4) Would a prospective study be of value?
DR. S. GAINER PILLSBURY, JR., Long Beach, California. Most of the mammograms seem to have been done on the sam,: day as the fine-needle aspiration. This is a different scenario than many of us have in our practices, where we see a patient with a mass, do a fine-needle aspiration, but the patient cannot have her mammogram until 2 to 3 days later. Do you have enough cases to show whether that mammogram is as valid as when done the same day as the fine-needle aspiration?
I)R. M~URILYN K. LAUGHEAD, Phoenix, Arizona. Was any kind of ultrasonography done to guide the needle? If not, do you think it would be helpful as a positioning guide for the needle?
DR. M~mK D. NICHOLS, Portland, Oregon. Could you comment on your technique in terms of decreasing the possibiliD, of a positive mammogram done after the fine-needle aspiration? Specifically, how do you reduce the risk of bleeding into the lesion itself?. Do you have the patient apply pressure for a certain amount of time? Second, what do you do with a young patient who has a mass tha: seems to be benign by palpation and on fine-needle aspiration, but you feel the patient is too young for a mammogram, such as a 22-year-old woman with what feels like a fibroadenoma?
DR. HINDLE (Closing). Answering the questions in reverse order, first, at the time the study was done, an outside vendor contract gave us complete control of the mammography. We were interested in finding out the value, if any, of mammography in young patients and whether there should be an age cutoff age below which nothing of clinical importance was found on the films. Second, we have a referral breast diagnostic center. If a young patient has a palpable dominant mass, the primary concern is not about the mammographic impression of the mass, but we don ' t want to send a patient away who has a nonpalpable lesion, especially a malignancy, in the other breast or somewhere else in the breast being evaluated. The protocol for the Breast Diagnostic Cen-
ter, particularly for teaching purposes, is to do mammog- raphy on every patient who is seen in our clinic because, by definition, they are all "diagnostic" breast problems. Currently, the radiology department is doing our mam- mography and they will not do a mammogram on a woman <30 years old unless my clinical impression is that she has a cancer. In the case of clinically suspected malignancy, they will perform mammography at any age. At the time of this study mammography was done on all these young patients to evaluate its effectiveness. If there is any doubt in the concordance of the diagnostic triad (clinical breast examination, mammography, and fine- needle aspiration), then we proceed to tissue-core needle biopsy, which we do in the clinic on the same visit.
Dr. Laughead, although we have the capability of doing tissue core-needle biopsies with ultrasonographic guidance, wfith a large palpable mass the ultrasonography is unnecessary and is not used routinely. If the biopsy is unsuccessful in obtaining tissue, ultrasonographic guid- ance i sused as a second step. After that, if a definitive diagnosis still does not exist, an open surgical excision biopsy is performed. Thus, if a mass is clinically suspi- cious, the diagnostic technique ladder is climbed until a definitive diagnosis is achieved.
Dr. Nelson, a specific cytologic diagnosis (e.g., fibro- adenoma) is required and "benign" is not definitive. If the mammogram is "suspicious," to come up with a definite diagnosas, a tissue core-needle biopsy is used for a palpable mass and, usually, on a nonpalpable lesion mammographic needle localization with exclslonal bi- opsy is performed by the surgery department.
Dr. Nichols, our technique of fine-needle aspiration is described in detail in the article. With the pressure technique described, ecchymosis rarely occurs. Suction is not used routinely. If an adequate cell sample is not obtained with the first aspiration, a second, separate puncture is performed, but this is necessary < 10% of the time. As mentioned, a "benign" diagnosis on fine-needle aspiration is unacceptable and a more specific cytologic diagnosis is used in the context of the diagnostic triad. If there is concordance of the diagnostic triad, clinical management follows. If there is agreement between the clinical impression (on the basis of history and examina- tion) and the cytologic diagnosis (e.g., a fibroadenoma) a mammogram is not required for women <30 years old.
Dr. Pillsbury, although we have not broken them out as a separate category for this presentation, some of the mammograms were done after the initial visit and there is no indication that this created a problem in interpre- tation. The pioneering reports of Klein and Sickles form the basis for the clinical rule that mammography should be performed before fine-needle aspiration or >2 weeks afterwards. Both looked at the accuracy of mammo- graphic interpretation when a mammogram was taken within 1 week of an fine-needle aspiration. Of 58 solid masses, 25 were benign and 16 were malignant by mammography and biopsy. The other 17 (29%) were "incorrect" (their word) mammographic interpretations

1292 Hindle and Chen June 1997 Am J Obstet Oynecol
because of postprocedure bleeding into the tissue. Of the 36 cysts that were mammographically benign, no interpretat ion problems occurred. No mammograms were performed between 1 and 2 weeks after fine-needle aspiration. Their conclusions were, "Previous aspiration does not preclude the ability of mammography to detect breast cancer and does not impair the ability o f mam- mography to identify benign lesions correctly." The data were not broken down to identify any mammograms taken on the same day as the fine-needle aspiration.
Dr. McQnarrie, it would be nice to have had controls and long-term follow-up. However, in the setting of this study (within the Los Angeles County Medical Center System), that is not logistically possible. Mammograms were ordered on all patients to find out about the remaining breast tissue and the contralateral breast. This was not a controlled or randomized study, but a clinical observation of our experience.
At the National Cancer Institute breast fine-needle aspiration conference last month, Dr. Miguel Sanchez, chief of the Depar tment of Pathology at Englewood Hospital (NJ.), which is associated with Mt. Sinai Medi- cal School, said that for many years in a high-volume cytology service their routine was to do the breast fine- needle aspiration followed shortly by mammography. Although he stated that they had no difficulty with subsequent mammographic interpretation, the data have not been published.
A poster presentation from the Cardiff Breast Clinic of the University of Wales College of Medicine repor ted on 314 fine-needle aspirations performed before mammog- raptly, of which 138 were performed within 10 days.. Five (3.6%) of these patients had hematomas, which "did not compromise the imaging," and the report concluded
that "the results presented suggest that the imaging of the breast can be safely carried out without a delay after fine-needle aspiration."
Eighty percent of our Breast Diagnostic Center pa- tients are physician referred and 20% are self-referred. More than 80% of our patients are Hispanics, who, as a group, have a lower incidence of breast cancer. Accord- ing to American Cancer Society statistics, the incidence rate of breast cancer for Hispanics is less than half the incidence rate for non-Hispanic white women. Our mean patient age was 33 years. The youth and Hispanic ethnic- ity of our patient population may influence the results of this study. However, because these patients are referred and come into a women's hospital-based county health service clinic, their presenting breast complaints more closely approximate those seen in primary-care clinical practice, whereas the women studied at the University of California Medical Center in San Francisco, where the Klein and Sickels data were collected, came from a university medical center surgical clinic. More than the timing, the modification of our technique makes a significant difference in decreasing ecchymosis and he- matoma formation. Klein and Sickles used a different method with multiple punctures, similar to the classic Karolinska technique. The use of multiple punctures and changing the angle of the needle for radial aspirations has the potential of incieasing bleeding within the breast. As noted, a single puncture is done in our clinic, keeping the needle in the same plane. Unless there is failure to obtain an adequate cellular harvest, a repeat aspiration is not done. Currently, studies in our clinic to evaluate these variables, to correlate the findings with histologic diagnoses, and to obtain long-term outcome results are being carried out.





























