Embed Size (px)
Citation preview

Accountability Agreement Tool Kit
0 P:\Smart Tools\Tools\2_Current\Accountability_Agreement_Tool_Kit.doc 10/05/2013

Accountability Agreement Tool Kit
1 P:\Smart Tools\Tools\2_Current\Accountability_Agreement_Tool_Kit.doc 10/05/2013
Organization-Wide
Leadership Accountability Agreement
Effective Date:
I. HCAHPS Goals (Provider of Choice)
# 12 Mos
High
12 Mos
Low
Year 1
(Date)
Year 2
(Date)
Year 3
(Date)
1. Communication with nurses
2. Communication with doctors
3. Responsiveness of hospital staff
4. Pain Management
5. Communications about Medications
6. Cleanliness of hospital environment
7. Quietness of hospital environment
8. Discharge Information
9. Overall
10. Willingness to Recommend
II. Patient Satisfaction Mean Score Goals (Provider of Choice)
# Overall Scores 12 Mos
High
12 Mos
Low
Year 1
(Date)
Year 2
(Date)
Year 3
(Date)
1. Inpatient
2. Outpatient
3. Ambulatory Services
4. ER
5. Clinics
6. Long Term Care
III. Internal Support Services Scorecard Goals (Provider & Employer of Choice)
# Hospital Overall 6 Mos (baseline - if applicable)
(Date)
12 Mos
(Date
1. Timeliness of Service
2. Telephone Etiquette
3. Quality of Service
4. Professionalism & Attitude
5. Overall
IV. Employee Satisfaction (Employer of Choice)
# Hospital Overall Current (baseline)
(Date)
6 Mos (if applicable)
(Date)
12 Mos
(Date)
1. Hospital Overall
V. Employee Turnover (Employer of Choice)
# By Position, Department or Overall Turnover Staff Turnover
Current
Turnover Goal
Year 1(Date)
Year 2
(Date)
Year 3
(Date)
Total # # % # % % %
1. Clinical
2. Non-Clinical
VI. Service Excellence Goals (Provider & Employer of Choice)
# 6 Mos (baseline - if applicable)
(Date)
12 Mos
(Date)
1. Service Huddles
2. DO IT Meetings

Accountability Agreement Tool Kit
2 P:\Smart Tools\Tools\2_Current\Accountability_Agreement_Tool_Kit.doc 10/05/2013
Department-Specific
Leadership Accountability Agreement
Department/Unit:
Leader Name:
Position:
Reports to:
I. HCAHPS Goals (Provider of Choice)
# Domain 12 Months High 12 Months Low Year 1 Goal (Date)
1. Communication with nurses
2. Communication with doctors
3. Responsiveness of hospital staff
4. Pain Management
5. Communications about Medications
6. Cleanliness of hospital environment
7. Quietness of hospital environment
8. Discharge Information
9. Overall
10. Willingness to Recommend
II. Patient Satisfaction Mean Score Goals (Provider of Choice)
# Specific survey vendor questions as they pertain
to your department.
12 Months High 12 Months Low Year 1 Goal (Date)
1.
2.
III. Internal Support Services Scorecard Goals (Provider & Employer of Choice)
# Criteria 6 Months (baseline - if
applicable)
(Date)
12 Months
(Date)
1. Timeliness of Service
2. Telephone Etiquette
3. Quality of Service
4. Professionalism & Attitude
5. Overall
IV. Employee Satisfaction (Employer of Choice)
# Domain (if applicable) Current (baseline)
(Date)
6 Months (if
applicable)
(Date)
12 Months
(Date)
1.
2.
V. Employee Turnover (Employer of Choice)
# May be by Position Staff Turnover
Current
Turnover Goal
Year 1 (Date)
Total # # % # %
1. RNs
2.
VI. Service Excellence Goals (Provider / Employer of Choice)
# Responsibilities 6 Months (baseline - if
applicable)
(Date)
12 Months
(Date)
1. Service Huddles
2. DO IT Meetings
Agreement: Effective today’s date, I accept full responsibility and accountability for the above noted goals, including gaining buy-in
and support from my staff. I further acknowledge that __________% of my performance review will be linked to the outcome of these
goals.
Signature: Date:

Accountability Agreement Tool Kit
3 P:\Smart Tools\Tools\2_Current\Accountability_Agreement_Tool_Kit.doc 10/05/2013
Individual
Leadership Accountability Agreement Department/Unit:
Leader Name:
Position:
Reports to:
I. Semi-Annual Leadership Empowerment Survey
# Survey Questions 6 Months (baseline)
(Date)
12 Months Goal
(Date)
1. Visionary & Change Agent: This Leader helps me understand change
and to see the “Big Picture”.
2. Builder of Trust & Personal Effectiveness: This Leader practices what
he/she preaches, is a good role model, and treats me with courtesy and
respect.
3. Communicator: This Leader keeps me informed so that I truly feel like
a knowledgeable “insider”.
4. Customer Service & Survey Literate: This Leader does a good job of
inspiring patient-centered service in my department and is always
aware of feedback from our satisfaction surveys.
5. Team Leader: This Leader promotes teamwork within our department
and with other departments/units.
6. Meeting Leader: This Leader runs meetings/huddles that inspire me
and encourage me to speak up.
7. Project & Time Management: This Leader ensures that I have the tools
and training to do my job in a timely and effective way.
8. Creative Problem Involver: This Leader encourages open and creative
problem-solving in my department.
9. Empowerer/Delegator: This Leader gives me clear assignments and
empowers me to do my best.
10. Employee Developer & Coach: This Leader is effective at coaching
me, developing my skills and keeping me on track.
11. Performance & Conflict Manager: This Leader is timely and
appropriate with both positive feedback and corrective action.
12. Hardwirer: This Leader is actively engaged in the Service Excellence
Initiative™ Process. (Year II and beyond)
13. Overall I rate my working relationship with this Leader as:
II. Service Excellence Goals
# Responsibilities 6 Months (baseline - if
applicable) (Date)
12 Months
(Date)
1. Attendance at Training Sessions
2. Participation on OASIS Teams
3. Patient Rounding (if applicable)
4. Staff Rounding
Agreement: Effective today’s date, I accept full responsibility and accountability for the above noted goals. I further
acknowledge that __________% of my performance review will be linked to the outcome of these goals.
Signature: Date:

Accountability Agreement Tool Kit
4 P:\Smart Tools\Tools\2_Current\Accountability_Agreement_Tool_Kit.doc 10/05/2013
Department-Specific
Leadership Accountability Agreement
Department/Unit:
Leader Name:
Position:
Reports to:
I. HCAHPS Goals (Provider of Choice)
# Domain 12 Months High 12 Months Low Year 1 Goal (Date)
1. Communication with nurses
2. Communication with doctors
3. Responsiveness of hospital staff
4. Pain Management
5. Communications about Medications
6. Cleanliness of hospital environment
7. Quietness of hospital environment
8. Discharge Information
9. Overall
10. Willingness to Recommend
II. Patient Satisfaction Mean Score Goals (Provider of Choice)
# Specific survey vendor questions as they pertain
to your department.
12 Months High 12 Months Low Year 1 Goal (Date)
1.
2.
III. Internal Support Services Scorecard Goals (Provider & Employer of Choice)
# Criteria 6 Months (baseline - if
applicable)
(Date)
12 Months
(Date)
1. Timeliness of Service
2. Telephone Etiquette
3. Quality of Service
4. Professionalism & Attitude
5. Overall
IV. Employee Satisfaction (Employer of Choice)
# Domain (if applicable) Current (baseline)
(Date)
6 Months (if
applicable)
(Date)
12 Months
(Date)
1.
2.
V. Employee Turnover (Employer of Choice)
# May be by Position Staff Turnover
Current
Turnover Goal
Year 1 (Date)
Total # # % # %
1. RNs
2.
VI. Service Excellence Goals (Provider / Employer of Choice)
# Responsibilities 6 Months (baseline - if
applicable)
(Date)
12 Months
(Date)
1. Service Huddles
2. DO IT Meetings
Agreement: Effective today’s date, I accept full responsibility and accountability for the above noted goals, including gaining buy-in
and support from my staff. I further acknowledge that __________% of my performance review will be linked to the outcome of these
goals.
Signature: Date:
Accountability Agreement Tool Kit
5 P:\Smart Tools\Tools\2_Current\Accountability_Agreement_Tool_Kit.doc 10/05/2013
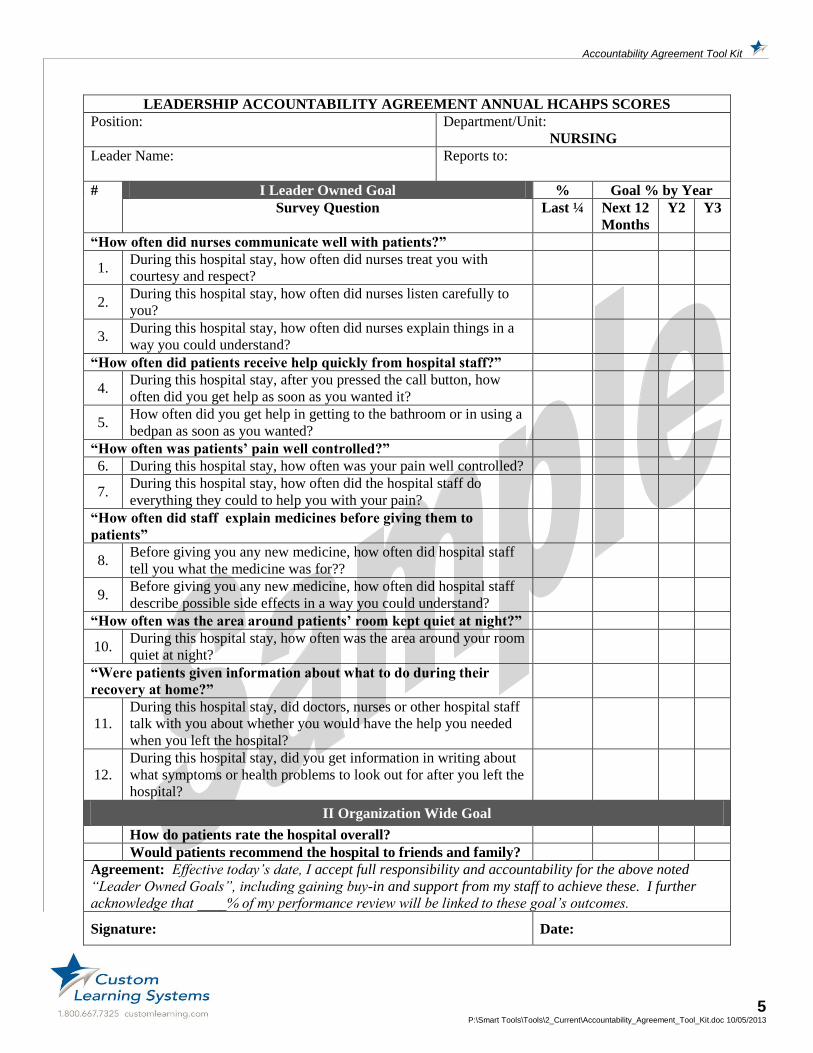
LEADERSHIP ACCOUNTABILITY AGREEMENT ANNUAL HCAHPS SCORES
Position:
Department/Unit:
NURSING
Leader Name:
Reports to:
# I Leader Owned Goal % Goal % by Year
Survey Question Last ¼ Next 12
Months
Y2 Y3
“How often did nurses communicate well with patients?”
1. During this hospital stay, how often did nurses treat you with
courtesy and respect?
2. During this hospital stay, how often did nurses listen carefully to
you?
3. During this hospital stay, how often did nurses explain things in a
way you could understand?
“How often did patients receive help quickly from hospital staff?”
4. During this hospital stay, after you pressed the call button, how
often did you get help as soon as you wanted it?
5. How often did you get help in getting to the bathroom or in using a
bedpan as soon as you wanted?
“How often was patients’ pain well controlled?”
6. During this hospital stay, how often was your pain well controlled?
7. During this hospital stay, how often did the hospital staff do
everything they could to help you with your pain?
“How often did staff explain medicines before giving them to
patients”
8. Before giving you any new medicine, how often did hospital staff
tell you what the medicine was for??
9. Before giving you any new medicine, how often did hospital staff
describe possible side effects in a way you could understand?
“How often was the area around patients’ room kept quiet at night?”
10. During this hospital stay, how often was the area around your room
quiet at night?
“Were patients given information about what to do during their
recovery at home?”
11.
During this hospital stay, did doctors, nurses or other hospital staff
talk with you about whether you would have the help you needed
when you left the hospital?
12.
During this hospital stay, did you get information in writing about
what symptoms or health problems to look out for after you left the
hospital?
II Organization Wide Goal
How do patients rate the hospital overall?
Would patients recommend the hospital to friends and family?
Agreement: Effective today’s date, I accept full responsibility and accountability for the above noted
“Leader Owned Goals”, including gaining buy-in and support from my staff to achieve these. I further
acknowledge that ____% of my performance review will be linked to these goal’s outcomes.
Signature: Date:

Accountability Agreement Tool Kit
6 P:\Smart Tools\Tools\2_Current\Accountability_Agreement_Tool_Kit.doc 10/05/2013
LEADERSHIP ACCOUNTABILITY AGREEMENT
ANNUAL PATIENT SATISFACTION SCORES
Position:
Department/Unit:
CASE MANAGEMENT
Leader Name:
Reports to:
# I Leader Owned Goal %tile Range Goal %tile
Survey Question 12
Month
High
12
Month
Low
Last
¼
Next 12
Months
Year
2
Year
3
1. Discharge
2. Extent felt ready discharge
3. Speed of discharge process
4. Help arranging homecare services
II Organization Wide Goal
Inpatient
Outpatient
Emergency Department
Ambulatory
Physician Clinics
Long Term Care
Home Health
Agreement: Effective today’s date, I accept full responsibility and accountability for the above
noted “Leader Owned Goals”, including gaining buy-in and support from my staff to achieve
these. I further acknowledge that ____% of my performance review will be linked to these goal’s
outcomes.
Signature: Date:

Accountability Agreement Tool Kit
7 P:\Smart Tools\Tools\2_Current\Accountability_Agreement_Tool_Kit.doc 10/05/2013
LEADERSHIP ACCOUNTABILITY AGREEMENT
ANNUAL PATIENT SATISFACTION SCORES
Position:
Department/Unit:
DIETARY
Leader Name:
Reports to:
# I Leader Owned Goal %tile Range Goal %tile
Survey Question 12
Month
High
12
Month
Low
Last
¼
Next 12
Months
Year
2
Year
3
1. Meals
2. Special/restricted diet explained
3. Temperature of food
4. Quality of the food
II Organization Wide Goal
Inpatient
Outpatient
Emergency Department
Ambulatory
Physician Clinics
Long Term Care
Home Health
Agreement: Effective today’s date, I accept full responsibility and accountability for the above
noted “Leader Owned Goals”, including gaining buy-in and support from my staff to achieve
these. I further acknowledge that ____% of my performance review will be linked to these goal’s
outcomes.
Signature: Date:

Accountability Agreement Tool Kit
8 P:\Smart Tools\Tools\2_Current\Accountability_Agreement_Tool_Kit.doc 10/05/2013
LEADERSHIP ACCOUNTABILITY AGREEMENT
ANNUAL PATIENT SATISFACTION SCORES
Position:
Department/Unit:
ENVIRONMENTAL SERVICES
Leader Name:
Reports to:
# I Leader Owned Goal %tile Range Goal %tile
Survey Question 12
Month
High
12
Month
Low
Last
¼
Next 12
Months
Year
2
Year
3
1. Room temperature
2. TV, call button, etc. worked
3. Helpfulness People Info desk
II Organization Wide Goal
Inpatient
Outpatient
Emergency Department
Ambulatory
Physician Clinics
Long Term Care
Home Health
Agreement: Effective today’s date, I accept full responsibility and accountability for the above
noted “Leader Owned Goals”, including gaining buy-in and support from my staff to achieve
these. I further acknowledge that ____% of my performance review will be linked to these goal’s
outcomes.
Signature: Date:

Accountability Agreement Tool Kit
9 P:\Smart Tools\Tools\2_Current\Accountability_Agreement_Tool_Kit.doc 10/05/2013
LEADERSHIP ACCOUNTABILITY AGREEMENT
ANNUAL HCAHPS SCORES Position:
Department/Unit:
ENVIRONMENTAL SERVICES
Leader Name:
Reports to:
# I Leader Owned Goal % Goal % by Year
Survey Question Last
¼
Next 12
Months
Year
2
Year
3
“How often were the patients’ rooms and bathrooms kept clean?”
1. During this hospital stay, how often were your room and
bathroom kept clean?
How do patients rate the hospital overall?
Would patients recommend the hospital to friends and
family?
Agreement: Effective today’s date, I accept full responsibility and accountability for the above noted
“Leader Owned Goals”, including gaining buy-in and support from my staff to achieve these. I further
acknowledge that ____% of my performance review will be linked to these goal’s outcomes.
Signature: Date:

Accountability Agreement Tool Kit
10 P:\Smart Tools\Tools\2_Current\Accountability_Agreement_Tool_Kit.doc 10/05/2013
LEADERSHIP ACCOUNTABILITY AGREEMENT
ANNUAL PATIENT SATISFACTION SCORES
Position:
Department/Unit:
HOUSEKEEPING
Leader Name:
Reports to:
# I Leader Owned Goal %tile Range Goal %tile
Survey Question 12
Month
High
12
Month
Low
Last
¼
Next 12
Months
Year
2
Year
3
1. Room
2. Pleasantness of room décor
3. Room cleanliness
4. Courtesy of person cleaning room
II Organization Wide Goal
Inpatient
Outpatient
Emergency Department
Ambulatory
Physician Clinics
Long Term Care
Home Health
Agreement: Effective today’s date, I accept full responsibility and accountability for the above
noted “Leader Owned Goals”, including gaining buy-in and support from my staff to achieve
these. I further acknowledge that ____% of my performance review will be linked to these goal’s
outcomes.
Signature: Date:

Accountability Agreement Tool Kit
11 P:\Smart Tools\Tools\2_Current\Accountability_Agreement_Tool_Kit.doc 10/05/2013
LEADERSHIP ACCOUNTABILITY AGREEMENT
ANNUAL PATIENT SATISFACTION SCORES
Position:
Department/Unit:
PHYSICIANS
Leader Name:
Reports to:
# I Leader Owned Goal %tile Range Goal %tile
Survey Question 12
Month
High
12
Month
Low
Last
¼
Next 12
Months
Year
2
Year
3
1. Physician
2. Time physician spent with you
3. Physician concern question/worries
4. Physician kept you informed
5. Friendliness/courtesy of physician
6. Skill of physician
7. Staff include decisions restatement
II Organization Wide Goal
Inpatient
Outpatient
Emergency Department
Ambulatory
Physician Clinics
Long Term Care
Home Health
Agreement: Effective today’s date, I accept full responsibility and accountability for the above
noted “Leader Owned Goals”, including gaining buy-in and support from my staff to achieve
these. I further acknowledge that ____% of my performance review will be linked to these goal’s
outcomes.
Signature: Date:

Accountability Agreement Tool Kit
12 P:\Smart Tools\Tools\2_Current\Accountability_Agreement_Tool_Kit.doc 10/05/2013
LEADERSHIP ACCOUNTABILITY AGREEMENT
ANNUAL PATIENT SATISFACTION SCORES
Position:
Department/Unit:
LAB
Leader Name:
Reports to:
# I Leader Owned Goal %tile Range Goal %tile
Survey Question 12
Month
High
12
Month
Low
Last
¼
Next 12
Months
Year
2
Year
3
1. Test & Treatments
2. Wait time for test & treatments
3. Concern/comfort during T&T
4. Skill of person took blood
5. Courtesy of person started IV
6. Courtesy of X-ray Staff
II Organization Wide Goal
Inpatient
Outpatient
Emergency Department
Ambulatory
Physician Clinics
Long Term Care
Home Health
Agreement: Effective today’s date, I accept full responsibility and accountability for the above
noted “Leader Owned Goals”, including gaining buy-in and support from my staff to achieve
these. I further acknowledge that ____% of my performance review will be linked to these goal’s
outcomes.
Signature: Date:

Accountability Agreement Tool Kit
13 P:\Smart Tools\Tools\2_Current\Accountability_Agreement_Tool_Kit.doc 10/05/2013
LEADERSHIP ACCOUNTABILITY AGREEMENT
ANNUAL PATIENT SATISFACTION SCORES
Position:
Department/Unit:
OCCUPATIONAL THERAPY
Leader Name:
Reports to:
# I Leader Owned Goal %tile Range Goal %tile
Survey Question 12
Month
High
12
Month
Low
Last
¼
Next 12
Months
Year
2
Year
3
1. Test & Treatments
2. Wait time for test & treatments
3. Concern/comfort during T&T
4. Skill of person took blood
5. Courtesy of person started IV
6. Courtesy of X-ray Staff
II Organization Wide Goal
Inpatient
Outpatient
Emergency Department
Ambulatory
Physician Clinics
Long Term Care
Home Health
Agreement: Effective today’s date, I accept full responsibility and accountability for the above
noted “Leader Owned Goals”, including gaining buy-in and support from my staff to achieve
these. I further acknowledge that ____% of my performance review will be linked to these goal’s
outcomes.
Signature: Date:

Accountability Agreement Tool Kit
14 P:\Smart Tools\Tools\2_Current\Accountability_Agreement_Tool_Kit.doc 10/05/2013
LEADERSHIP ACCOUNTABILITY AGREEMENT
ANNUAL PATIENT SATISFACTION SCORES
Position:
Department/Unit:
PHYSICAL THERAPY
Leader Name:
Reports to:
# I Leader Owned Goal %tile Range Goal %tile
Survey Question 12
Month
High
12
Month
Low
Last
¼
Next 12
Months
Year
2
Year
3
1. Test & Treatments
2. Wait time for test & treatments
3. Concern/comfort during T&T
4. Skill of person took blood
5. Courtesy of person started IV
6. Courtesy of X-ray Staff
II Organization Wide Goal
Inpatient
Outpatient
Emergency Department
Ambulatory
Physician Clinics
Long Term Care
Home Health
Agreement: Effective today’s date, I accept full responsibility and accountability for the above
noted “Leader Owned Goals”, including gaining buy-in and support from my staff to achieve
these. I further acknowledge that ____% of my performance review will be linked to these goal’s
outcomes.
Signature: Date:

Accountability Agreement Tool Kit
15 P:\Smart Tools\Tools\2_Current\Accountability_Agreement_Tool_Kit.doc 10/05/2013
LEADERSHIP ACCOUNTABILITY AGREEMENT
ANNUAL PATIENT SATISFACTION SCORES
Position:
Department/Unit:
RADIOLOGY
Leader Name:
Reports to:
# I Leader Owned Goal %tile Range Goal %tile
Survey Question 12
Month
High
12
Month
Low
Last
¼
Next 12
Months
Year
2
Year
3
1. Test & Treatments
2. Wait time for test & treatments
3. Concern/comfort during T&T
4. Skill of person took blood
5. Courtesy of person started IV
6. Courtesy of X-ray Staff
II Organization Wide Goal
Inpatient
Outpatient
Emergency Department
Ambulatory
Physician Clinics
Long Term Care
Home Health
Agreement: Effective today’s date, I accept full responsibility and accountability for the above
noted “Leader Owned Goals”, including gaining buy-in and support from my staff to achieve
these. I further acknowledge that ____% of my performance review will be linked to these goal’s
outcomes.
Signature: Date:

Accountability Agreement Tool Kit
16 P:\Smart Tools\Tools\2_Current\Accountability_Agreement_Tool_Kit.doc 10/05/2013
LEADERSHIP ACCOUNTABILITY AGREEMENT
ANNUAL PATIENT SATISFACTION SCORES
Position:
Department/Unit:
RESPIRATORY THERAPY
Leader Name:
Reports to:
# I Leader Owned Goal %tile Range Goal %tile
Survey Question 12
Month
High
12
Month
Low
Last
¼
Next 12
Months
Year
2
Year
3
1. Test & Treatments
2. Wait time for test & treatments
3. Concern/comfort during T&T
4. Skill of person took blood
5. Courtesy of person started IV
6. Courtesy of X-ray Staff
II Organization Wide Goal
Inpatient
Outpatient
Emergency Department
Ambulatory
Physician Clinics
Long Term Care
Home Health
Agreement: Effective today’s date, I accept full responsibility and accountability for the above
noted “Leader Owned Goals”, including gaining buy-in and support from my staff to achieve
these. I further acknowledge that ____% of my performance review will be linked to these goal’s
outcomes.
Signature: Date:

Accountability Agreement Tool Kit
17 P:\Smart Tools\Tools\2_Current\Accountability_Agreement_Tool_Kit.doc 10/05/2013
LEADERSHIP ACCOUNTABILITY AGREEMENT
ANNUAL PATIENT SATISFACTION SCORES
Position:
Department/Unit:
OVERALL
Leader Name:
Reports to:
# I Leader Owned Goal %tile Range Goal %tile
Survey Question 12
Month
High
12
Month
Low
Last
¼
Next 12
Months
Year
2
Year
3
1. Staff sensitivity to inconvenience
2. Extent staff wore ID badges
3. Info. family re-condition/treatment
II Organization Wide Goal
Inpatient
Outpatient
Emergency Department
Ambulatory
Physician Clinics
Long Term Care
Home Health
Agreement: Effective today’s date, I accept full responsibility and accountability for the above
noted “Leader Owned Goals”, including gaining buy-in and support from my staff to achieve
these. I further acknowledge that ____% of my performance review will be linked to these goal’s
outcomes.
Signature: Date:






















![Grant Agreement [TF099878] Ethiopia Protection of Basic Services Social Accountability Program (ESAP2) 1 SAIPs Finance, Grant and Operation training Presentation](https://img.dokumen.tips/doc/110x75/56649edf5503460f94bef416/grant-agreement-tf099878-ethiopia-protection-of-basic-services-social-accountability.jpg)






