Embed Size (px)
Citation preview

Rom J Leg Med [27] 247-253 [2019]DOI: 10.4323/rjlm.2019.247© 2019 Romanian Society of Legal Medicine
247
FORENSIC PATHOLOGY
Accessory spleens at autopsy: the incidence and the presence of myoepithelial cells in the spleen capsule
Carmen Corina Radu1, Dan Perju-Dumbravă2, Daniel Ureche2,*, Codrin Rebeleanu2, Diana Bulgaru-Iliescu3, Iuliu Fulga4, Andreea Cămărășan1, Ovidiu Pop1
_________________________________________________________________________________________ Abstract: Background. Accessory spleen represents a small body of splenic tissue that is situated elsewhere in the abdominal cavity than in its normal position, having a congenital origin. Methods. We have investigated 150 forensic autopsies, the purpose of the study being to discover the incidence, distribution, histological aspect and immunohistochemistry features of accessory spleens. Results. Accessory spleens were found in both sexes, 67% were detected at men and 33% at women. In 3 cases the accessory spleen was situated along the splenic hilum and the vascular pedicle of the spleen; in one case the accessory spleen was found around the head of the pancreas; in one case it was found along of the greater curvature of the stomach; and in one case it was situated retroperitoneal, in the perirenal adipose tissue, on the anterior surface. Histological exam revealed normal splenic tissue. The normal spleen and the accessory spleen are presenting myoepithelial cells in the capsule. Conclusions. In all of the research cases, accessory spleens were diagnosed post-mortem and none of it while the person was still alive. Accessory spleens are integrated in the immune response as a functional accessory organ, and also have immunological functions like the normal spleens. We discovered the existence of the myoepithelial cells in the spleen capsule. The proper management in spleen trauma in adults is in debate and the role and myoepithelial cells number need further studies Key Words: spleen, accessory, autopsy, forensic, immunohistochemistry, myoepithelial cells.
1) University of Oradea, Faculty of Medicine and Pharmacy, Oradea, Romania2) “Iuliu Hatieganu” University of Medicine and Pharmacy, Cluj-Napoca, Romania* Corresponding author: “Iuliu Hatieganu” University of Medicine and Pharmacy, 8 Victor Babeş Str., 400012, Cluj-Napoca, Romania, E-mail: [email protected]) “Grigore T. Popa” University of Medicine and Pharmacy, Iasi, Romania4) “Dunarea de Jos” University of Galaţi, Faculty of Medicine and Pharmacy, Galaţi, Romania
INTRODUCTION
The spleen, as an organ, can be met in various developmental abnormalities like agenesis, polysplenia syndrome, isolated small additional splenunculi and persistent lobulation (Radu, Muţiu and Pop, 2014). The accessory spleen represents a small body of spleen tissue, separated from the main body of the spleen, situated elsewhere in abdominal cavity that in its normal position, having congenital origin (Richard and Marc, 2010). Usually, accessory spleens are found incidentally on CT scans, in 20%-33% of the autopsies, and also in primary
spleen removal (20%) (Robert, Samuel and Thomas, 2003; Robert, F. Dondelinger; Baert, 2004; Richard and Marc, 2010). It can be found near the splenic hilum and also located in the abdominal cavity like: around the tail of the pancreas, in greater omentum, along the greater curvature of the stomach, near ovaries or testis, in Douglas' pouch, in the mesentery of the intestines (small or large) (Saadia, 2002; Radu, Muţiu and Pop, 2014). Its shape is usually round and up to 2 cm in diameter, but after spleen removal, splenic infarct, or other diseases of the spleen, an accessory spleen can become bigger, enlarging its diameter up to 6 cm (Robert, F. Dondelinger;

248
Radu C.C. et al. Accessory spleens at autopsy: the incidence and the presence of myoepithelial cells in the spleen capsule
Baert, 2004). The number of accessory spleens variate from 1 to maximum 6, their blood supply comes usually from a separate artery originary from the main splenic artery at the hilum (Radu, Muţiu and Pop, 2014). Sometimes, accessory spleen can be confused clinically and imagistically with malign tumor, especially when they are found attached on the pancreatic tail, that’s why the differential diagnosis depends on its location (R. A. Bisset; A. Khan Durr-e-sabih, 2008). When the splenic tissue is located in the splenic hilus and the patient is asymptomatic, the diagnosis can be made with confidence, but when it is situated in the left upper quadrant, it can simulate a tumor mass, so a neoplasm must be considered (Saadia, 2002). Histological exam usually show the normal splenic parenchyma (Radu, Muţiu and Pop, 2014). Accessory spleens are usually found via imagistic methods (ultrasound, CT, IRM) or in autopsies; they have no utility. At ultrasound, it has the same texture like the actual spleen, and in autopsies it usually has a spherical form, well delimited, a variable diameter between 0.5 and 6 cm, parenchymal consistency, and in section it has the same aspect like a normal spleen (Richard and Marc, 2010). Accessory spleens are a common phenomenon for both sexes and they can be found at all ages. Autopsy can be a way to determine the incidence and the characteristics of the splenunculi in the population. In 10–44% of autopsies accessory spleens are congenital without any manifestations (al-Ahmadi et al., 1998).
AIM OF THE STUDY
We proceed to this study at Forensic Department from County Bihor, city of Oradea, the main purpose of it being to investigate the incidence, distribution and histological aspect, immunological features regarding the myoepithelial cells of accessory spleens vs. normal spleen in forensic autopsies.
METHODS
We proceed at a prospective observational study and we have investigated a number of 150 consecutive autopsy cases between 2015-2017. For finding out if there is any difference between the immunoprofile of the myoepithelial cells expression in the normal spleen and the same immunoprofile of the accessory spleens. Normal spleens are composed of a red and a white pulp (Mark F. Cesta, 2006); the red pulp of the accessory spleens showed normal vascular structures (Martin and Kearney, 2002; Parker and Papenfuss, 2017). In all of these 6 cases there was made an histological exam, which revealed normal splenic tissue (Figs 8-10). The tissue was preserved 48 hours in buffered formalin.
The sections prepared from formalin-fixed paraffin embedded tissue were cut at 4µm thickness and after that were stain by hematoxylin-eosin (Stoicescu et al., 2017). For finding out if there is any difference between the immunoprofile of the tissue from normal spleens and immunoprofile of the accessory spleens, an immunohistochemical analysis was performed on 4 μm-thick sections, prepared with formalin-fixed paraffin embedded tissue by using an automated immunostainer (Ventana BenchMark GX) according with to the manufacturer’s instructions. After that, using EZprep solution, slides were de-paraffinized (Ventana Medical Systems, Inc.) at 90°C, and both reagent and incubation time was chosen as directed on the antibody’s package inserts. With OmniMap DAB(3,3’-diaminobenzidine) detection kit (Ventana Medical Systems, Inc.) and counterstained with Hematoxylin, the slides were developed. All the tissue samples were incubated according with the manufacturer insert with Basal Cell Cocktail (34ßE12+p63) and Smooth Muscle Actin. The anti-p63 (clone 4A4) is nuclear expressed, the anti-keratin (34ßE12) is cytoplasm expressed and the smoothe muscle actin (clone 1A4will be express in the cytoplasm. The negative control was done in the some manner but with omission of the monoclonal antibodies. The positive control was done with appendix and prostate sample (Roche, no date).
RESULTS
All of the accessory spleens regarding our study were diagnosed post-mortem, and no members of the deceased could offer us details about possible signs and symptoms of the deceased that we could associate with this condition. In some cases, accessory spleens can produce symptoms like recurrent abdominal pain in left lower quadrant (Morris et al., 1999; Vural et al., 1999), being need of laparoscopic procedure with the excision of the masses, epigastric pain and weight loss (Itano et al., 2010) in other cases can mimic an endocrine tumor of the pancreas (Uchiyama and Chijiiwa, 2008), but in most cases their presence remain silent. Accessory spleens were discovered in 4% of them, represented by 6 cases. Accessory spleens were found in both sexes, 67% (4 cases) were detected at men and 33% (2 cases) at women. In most of them, meaning 3 cases (50%), accessory spleen was seen along the splenic hilum and vascular pedicle of the spleen, in 1 case (16.6%) accessory spleen was found around the head of the pancreas, 1 case (16.6.%) accessory spleen was seen along of the grater curvature of the stomach, and in 1 case (16.6%) it was situated retroperitoneal in perirenal adipose tissue, on anterior surface (Fig. 1). Its shape was round or oval with variable diameters from 0.8/0.5 cm. to 3/2 cm. In each case there were found

Romanian Journal of Legal Medicine Vol. XXVII, No 3(2019)
249
Figure 1. Distribution of accessory spleens.
Cases with accessory
spleens Location of accessory spleens
Number of accessory
spleens
1 Hilum and vascular pedicle of the spleen 1
2 Hilum and vascular pedicle of the spleen 1
3 Hilum and vascular pedicle of the spleen 2
4 Around the head of the pancreas 3
5 Along of the grater curvature of the stomach 1
6 Retroperitoneal in perirenal adipose tissue 1
Table 1. Number of accessory spleens
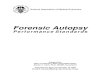
Figure 2. Woman, 62-years old, accessory spleen situated in splenic hilum, dim. 3/2 cm.
Figure 3. Man, 52-years old, accessory spleen situated in splenic hilum, dim. 2,5/2 cm.
Figure 4. Male, 45 years old, 3 accessory spleens situated around the head of pancreas, dim. 1.5/1 cm, 1/0.8 cm and 0,8/0,5 cm.
Figure 5. Man 43-years old, 2 accessory spleens situated in splenic hilum, dim. 1.5/1 cm. and 0.8/0.5 cm.
Figure 6. Woman, 32 years old, accessory spleen situated in perirenal adipose tissue of left kidney, anterior surface, dim. 1.5/0.6 cm.
Figure 7. Man, 67 years old, accessory spleen situated along the greater curvature of the stomach, dim. 3/2 cm.

250
Radu C.C. et al. Accessory spleens at autopsy: the incidence and the presence of myoepithelial cells in the spleen capsule
from 1 to 3 accessory spleens (9 overall), so that: in one human corpse with accessory spleens along the splenic hilum, 2 accessory spleens were discovered; 3 accessory spleens were discovered around the head of the pancreas in another case. Microscopic appearance of the accessory spleens
revealed normal splenic tissue with white and red pulp. So accessory spleens look like normal spleens in structure and also in immunologic functions. Normal spleens are composed of a red and a white pulp (Mark F Cesta, 2006); the red pulp of the accessory spleens showed normal vascular aspects (Martin and Kearney, 2002; Parker and
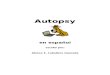
8 9 10
Figures 8, 9, 10. Histological exam shows normal aspect with red pulp around the white pulp. In the center of white pulp area can be seen the central arteriole. Hematoxilin-eosine 40X, 100X, 200X.
Figure 13. Positive expression to anti-smooth muscle actin in the accessory spleen capsule. 400X.
Figure 14. Positive expression to basal cell cocktail in the spleen capsule. 100X.
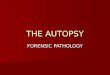
Figure 11. Positive expression to anti-smooth muscle actin in the spleen capsule. 400X.
Figure 12. Positive expression to basal cell cockteil in the spleen capsule. 100X.

Romanian Journal of Legal Medicine Vol. XXVII, No 3(2019)
251
Papenfuss, 2017). All the slides were stain with Basal Cell Cocktail (34ßE12+p63) and Smooth Muscle Actin. The myoepithelial cells are positive for SMA, p63 and high molecular keratin 34ßE12 (includes CK5 and CK15). According with our study the normal spleen samples presented positivity to the connective tissue capsule. The SMA expression is not limited only to the myoepithelial cells. The smooth muscle cells are positive too (brown stain - Fig. 11). The expression of SMA can be noticed around the arterioles and septa. In the study we correlated the SMA expression in the capsule with the expression of the myoepithelial markers (34ßE12+p63). In the image can be detected brown positive expression in the nucleus for p63 and in the cytoplasm for high molecular keratin (Fig 12). In all 6 cases of accessory spleen found out by us and included in the study, we identified the presence of myoepithelial cells in the connective tissue capsule. Like in the normal spleen specimens can be seen in the SMA expression mor cells stained because here are included both smooth muscle cells and myoepithelial cells (Fig 13). The distribution of the smooth muscle cells are seen in trabecula and in the blood vessels wall. When we analyzed the expression of the high molecular keratin all accessory spleen cases were satin in brown in the cytoplasm and for the p63 the expression is seen in the nucleus (Fig. 14). No differences could be seen between the two spleen types: accessory and normal.
DISCUSSION
In forensic medicine, post-traumatic accessory spleen ruptures are very rarely met because most of accessory spleens are small and relatively well protected by other organs. However, an accessory spleen can be the cause of acute intra-abdominal symptoms with internal hemorrhage leading even to death (Richmond, Humphrey and Nichols, 1992). Also, because accessory spleens can enlarge after the spleen removal, they can suffer hypertrophy changes, so spontaneous ruptures take place and cause acute abdomen pain. Such a case is presented by Leon L et al.: 45-years old woman being admitted to the emergency room with sudden and sharp abdominal pain in left upper quadrant, the woman was diagnosed with spontaneous rupture of a 6 cm hypertrophied accessory spleen after she had a car accident 25 years earlier and at that time she suffered spleen removal after a splenic rupture, moment in which the doctors discovered a 2 cm accessory spleen (Leon et al., 2006). A study by Dogan N. made on a number of 720 consecutive autopsy cases and concluded that in 48 cases they found 54 accessory spleens, 28 from them in hilum of the main spleen, 13 in great omentum, 5 pancreas cases and 2 in pelvis (Dogan et al., 2011). Our study
investigated 150 consecutive autopsies and only in 6 cases (4%) accessory spleens were found. Usually at autopsies it is found only one accessory spleen (85%), rarely (14%) and extremely rarely three or more (1%), and their maximum size is not larger than 2 cm in diameter (Zhang and Zhang, 2011). The most common location is at the hilum of the spleen in the gastrosplenic ligament (50%), but they can be found also around the pancreas (30%) or rarely within the greater omentum of the stomach. It can also be found at the mesentery of the small intestine, mesocolon, pancreas, kidney and pelvis (Richard and Marc, 2010). From all of the 6 cases that we presented, only in one case we discovered 3 accessory spleens (the case with peripancreatic accessory spleen) and one case with 2 accessory spleens situated in splenic hilum. The splenunculis found by us were situated in splenic hilum (50%), around the head of the pancreas (17%), in the fat of the anterior surface of left kidney (17%), along of the grater curvature of the stomach (17%). Most patients have no clinical manifestations, but sometimes, depending on its position, it can produce symptoms by compressing adjacent organs. Torsion of an accessory spleen rarely occurs, but when it takes place the patient can bear recurrent abdominal pain, although a few cases have been reported in the literature. Most cases occur in children, and in most cases the diagnosis is made during the surgery. Without treatment, torsion of an accessory spleen can lead to hemorrhagic shock, peritonitis, bowel obstruction and finally to death. (Sadro and Lehnert, 2015) Other acute symptoms related to accessory spleens are given by spontaneous rupture or infarction. When the accessory spleen has a long vascular pedicle, it can mimic acute appendicitis. Differential diagnosis is made with: tumors (benign or malign), splenosis, splenules surrounding the spleen. They probably result from the failure of embryonic splenic buds to unite or extreme lobulation of the spleen. The morphologic appearance is identical to that of the normal spleen(Richard and Marc, 2010). According to the literature there is an increased incidence of accessory spleens in patients with hematologic disorders (Termos et al., 2017). In cases with hematological disorders like chronic immune thrombocytopenic purpura, laparascopic spleen removal is needed, but after a while, sometimes years after the surgery, recurrence of thrombocytopenia may occur in association with a functional accessory spleen(Walters, Roberts and Votaw, 1998; Sotomayor-Ramirez, 2009). A study performed by Morris KT et al., 17 patients with spleen removal made for idiopatic thrombocytopenic purpura established that one patient developed, after the surgery, recurrent thrombocytopenia, so imagistic exams were performed on all 17 patients and 2 other patients were discovered with accessory spleens, so they proceeded in all 3 cases to laparoscopic spleen removal in order to remove the accessory spleens. All three

252
Radu C.C. et al. Accessory spleens at autopsy: the incidence and the presence of myoepithelial cells in the spleen capsule
patients had a good clinical feedback, two of them with asymptomatic accessory spleens have never developed recurrent thrombocytopenia, as for the patient who had recurrent thrombocytopenia, disease went into remission. To minimize the risk of missing an accessory spleen, a systematic search should be made at the beginning of the laparoscopic operation(Morris et al., 1999). Therefore, at living persons, for a sustained remission of this pathology, identification of the accessory spleen is the most important step and after the identification, resection of the accessory spleen is needed (Walters, Roberts and Votaw, 1998). In our study we analyzed the presence or the absence of the myoepithelial cells in the spleen capsule. The normal histology aspects are not refer to the presence of this cell type. Normally the capsule is described like a connective tissue capsule admix with smooth muscle cells. Only one article is reported in the literature about the importance of the capsule myoepithelial cells in the non-operative management of spleen trauma. In the article is no any mention about the presence of this myoepithelial cell in the spleen. The higher myoepithelial cells in children is associated with a better outcome in non-operative treatment for spleen trauma (Fernandes et al., 2013). We could not find any accessory spleen in children to make an analyze regarding the number of myoepithelial cells. On the one hand our study proved the presence of the myoepithelial cells in the spleen capsule but on the other hand we gone forward to make a complete analyze between the normal spleen capsule and accessory spleen capsule. According to the age of the patients we found not any differences regarding the myoepithelial cells. Powell et al. stated that the non-operative management of spleen trauma in children has a lower risk of failure while in the adults the rate of failure is higher. The monoclonal antibodies used by us were Basal Cell Cocktail (34ßE12+p63) and Smooth Muscle Actin (SMA). The reason why we choose this antibodies was the exclude the reaction of the mesothelial cell with CK 5 (CK5 is included in the 34ßE12). The mesothelial cells are not stained with p63 and SMA. The used of this antibodies acts as a double-checking for myoepithelial cell (Pearl et al., 1989).
In conclusion, at living persons accessory spleens are usually discovered accidentally, imagistic at CT or IRM. At cadavers, during forensic autopsies, they are rarely to find, therefore we proceed at finding them in the forensic autopsies that were performed at the Forensic Department of Forensic Medicine, Bihor County, Romania. Our study investigated 150 consecutive autopsies with the purpose of establishing features such as incidence, distribution, and in only 6 cases (4%) accessory spleens were found. From all 6 cases that we presented, the accessory spleens found by us were situated in splenic hilum (50%), around the head of the pancreas (17%), in the fat of the anterior surface of left kidney (17%), along of the grater curvature of the stomach (17%). All cases with accessory spleens were discovered post-mortem and none of the cases had been previously diagnosed when the person was still alive. Histopathology exams were made and all of them were confirmed as being accessory spleens, having the same structure like the normal spleen. The normal spleen and the accessory spleen are presenting myoepithelial cells in the capsule. The proper management in spleen trauma in adults is in debate and the role and myoepithelial cells number need further studies.
Conflict of interest. The authors whose names are listed above certify that they have NO affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultations, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript. Funding. This work was supported by University of Oradea. Authors’ contributions. CR found, analyzed and interpreted the data. DBI performed the histological examination of the accessory spleen. All authors read and approved the final manuscript.
References1. al-Ahmadi M, Brundage S, Brody F, Jacobs L, Sackier JM. Splenosis of the mesoappendix: case report and review of the literature. J R Coll
Surg Edinb. 1998;43(3):200-202.2. Cesta MF. Normal structure, function, and histology of the spleen. Toxicol Pathol. 2006;34(5):455–465.3. Unver Dogan N, Uysal II, Demirci S, Dogan KH, Kolcu G. Accessory spleens at autopsy. Clin Anat. 2011;24(6):757-762.4. Fernandes TM, Dorigatti AE, Pereira BM, Cruvinel Neto J, Zago TM, Fraga GP. Nonoperative management of splenic injury grade IV is
safe using rigid protocol. Rev Col Bras Cir. 2013;40(4):323-329.5. Itano O, Chiba N, Wada T, Yuasa Y, Sato T, Ishikawa H, Koyama Y, Matsui H, Kitagawa Y. Laparoscopic resection of an epidermoid cyst
originating from an intrapancreatic accessory spleen: report of a case. Surg Today. 2010;40(1):72-75.6. Leon L, Labropoulos N, Hudlin CI, Macbeth AG, Matolo N, Andrus C. Accessory spleen rupture in a patient with previous traumatic

Romanian Journal of Legal Medicine Vol. XXVII, No 3(2019)
253
splenectomy. J Trauma. 2006;60(4):901-903.7. Martin F, Kearney JF. Marginal-zone B cells. Nature Reviews Immunology. Nature Publishing Group. 2002; 2: 323. Available at: https://doi.
org/10.1038/nri799.8. Morris KT, Horvath KD, Jobe BA, Swanstrom LL. Laparoscopic management of accessory spleens in immune thrombocytopenic purpura.
Surg Endosc. 1999;13(5):520-522.9. Parker GA, Papenfuss TL. Basic Immunobiology BT - Immunopathology in Toxicology and Drug Development: Volume 1. Immunobiology,
Investigative Techniques, and Special Studies’, in Parker GA. (ed.). Cham: Springer International Publishing. 2017: 1–93. doi: 10.1007/978-3-319-47377-2_1.
10. Pearl RH, Wesson DE, Spence LJ, Filler RM, Ein SH, Shandling B, Superina RA. Splenic injury: a 5-year update with improved results and changing criteria for conservative management. J Pediatr Surg. 1989;24(1):121-124; discussion 124-125.
11. Bisset RA, Khan Durr-e-sabih A. Liver, Biliary System, Pancreas and Spleen.’, in Diferrential Diagnosis in Abdominal Ultrasound. 3rd edn. New York: Sounders Elsevier. 2008: 160–161.
12. Radu CC, Muţiu G, Pop O. Accessory spleen. Rom J Morphol Embryol. 2014;55(3 Suppl):1243–1246.13. Richard, G. and Marc, L. (2010) High-yield Imaging: Gastrointestinal. Spleen. Edited by Saunders Elsevier. Philadelphia: Saunders Elsevier.14. Richmond R, Humphrey P, Nichols WK. Isolated traumatic accessory splenic rupture: a case report and literature review. Mo Med.
1992;89(6):351-353. PMID: 1620088.15. Dondelinger RF, Baert AL. Imaging and Intervention in Abdominal Trauma. Injuries of the Spleen. Edited by Springer. New York: Springer.
2004.16. Robert IH, Samuel EL, Thomas PS. Blood: Principles and Practice of Hematology. 2nd edn. Philadelphia: Lippincott Williams and Wilkins.
2003.17. Roche (no date) Anatomic pathology instruments and reagents. Available at: www.ventana.com.18. Saadia R. The Complete Spleen: Structure, Function, and Clinical Disorders. 2nd ed’, Canadian Journal of Surgery. Canadian Medical
Association. 2002; 45(3): 226. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3686962/.19. Sadro CT, Lehnert BE. Torsion of an accessory spleen: Case report and review of the literature. Radiol Case Rep. 2015;8(1):802. 20. Sotomayor-Ramírez RK. Efficacy and safety of laparoscopic splenectomy: review of 14 adult cases using the lateral approach. Bol Asoc Med
P R. 2009;101(2):43-49. PMID: 19954101.21. Stoicescu M, Bungău SG, Ţiţ DM, Muţiu G, Purza AL, Iovan VC, Pop OL. Carcinogenic uterine risk of repeated abortions: hormone
receptors tumoral expression. Rom J Morphol Embryol. 2017;58(4):1429-1434. PMID: 29556637.22. Termos S, Redha A, Zbibo R, Alduwaisan A, AlKabbani M, Elyousif N, Alali M. Torsion of huge wandering accessory spleen. Case report
and review of literature. Int J Surg Case Rep. 2017;38:131-135.23. Uchiyama S, Chijiiwa K, Hiyoshi M, Ohuchida J, Imamura N, Nagano M, Hidaka H, Yorita K, Akiyama Y, Nishiura M. Intrapancreatic
accessory spleen mimicking endocrine tumor of the pancreas: case report and review of the literature. J Gastrointest Surg. 2008;12(8):1471-1473.
24. Vural M, Kacar S, Koşar U, Altin L. Symptomatic wandering accessory spleen in the pelvis: sonographic findings. J Clin Ultrasound. 1999;27(9):534-536.
25. Walters DN, Roberts JL, Votaw M. Accessory splenectomy in the management of recurrent immune thrombocytopenic purpura. Am Surg. 1998;64(11):1077–1078.
26. Zhang C, Zhang XF. Accessory spleen in the greater omentum. Am J Surg. 2011;202(3):e28-30.