Embed Size (px)
Citation preview

antibodies after cardiopulmonary bypass surgery. Br JHaematol 1998;101:653–5.
2. Pouplard C, May MA, Iochmann S, et al. Antibodies toplatelet factor 4-heparin after cardiopulmonary bypass inpatients anticoagulated with unfractionated heparin or alow-molecular-weight heparin: clinical implications for hep-arin-induced thrombocytopenia. Circulation 1999;99:2530–6.
3. Wilhelm MJ, Schmid C, Kececioglu D, Mollhoff T, OstermannH, Scheld HH. Cardiopulmonary bypass in patients withheparin-induced thrombocytopenia using Org 10172. AnnThorac Surg 1996;61:920–4.
4. Kawada T, Kitagawa H, Hoson M, Okada Y, Shiomura J.Clinical application of argatroban as an alternative anticoag-ulant for extracorporeal circulation. Hematol Oncol ClinNorth Am 2000;14:445–57.
5. D’Ancona G, Donias HW, Karamanoukian RL, Bergsland J,Karamanoukian HL. OPCAB therapy survey: off-pump clopi-dogrel, aspirin or both therapy survey. Heart Surg Forum2001;4:354–8.
6. Carrier M, Robitaille D, Perrault LP, et al. Heparin versusdanaparoid in off-pump coronary bypass grafting: results of aprospective randomized clinical trial. J Thorac CardiovascSurg 2003;125:325–9.
7. Walenga JM, Fasanella AR, Iqbal O, et al. Coagulation labo-ratory testing in patients treated with argatroban. SeminThromb Hemost 1999;25(Suppl 1):61–6.
8. Berry CN, Girardot C, Lecoffre C, Lunven C. Effects of thesynthetic thrombin inhibitor argatroban on fibrin- or clot-incorporated thrombin: comparison with heparin and recom-binant Hirudin. Thromb Haemost 1994;72:381–6.
Accessory Mitral Valve TissueCausing Severe Left VentricularOutflow Tract Obstruction in anAdultYoshikazu Aoka, MD, Naoko Ishizuka, MD, PhD,Yasunari Sakomura, MD, PhD,Hirotaka Nagashima, MD, PhD,Masatoshi Kawana, MD, PhD,Akihiko Kawai, MD, PhD, andHiroshi Kasanuki, MD, PhD
Departments of Cardiology and Cardiovascular Surgery, TheHeart Institute of Japan, Tokyo Women’s Medical University,Tokyo, Japan
Accessory mitral valve (AMV) is a rare cause of leftventricular outflow tract (LVOT) obstruction and is ex-tremely rare in adults. We report a case of an older adultwith an AMV that caused severe LVOT obstruction. Aparachute-like piece of tissue (the AMV) protruding intothe LVOT during systole was first detected in a 45-year-old woman by echocardiography. Because the pressuregradient and dyspnea gradually progressed, she finallyunderwent a successful operation for removal when shewas 48 years old.
(Ann Thorac Surg 2004;77:713–5)© 2004 by The Society of Thoracic Surgeons
Accessory mitral valve (AMV) is a rare cause of leftventricular outflow tract (LVOT) obstruction in
childhood and is extremely rare in adults. MacLean andassociates [1] first described this rare condition in 1963.At least 63 cases of AMV have been reported in theliterature. Of these, 59 patients underwent operations,and only 7 were adults [2]. In most reported cases, thisanomaly was found in the first decade of life, mainlybecause of a heart murmur [3]. We report a case of AMVin an adult patient that caused severe LVOT obstructionand was found in the 40 s. The AMV was removed in asuccessful operation after 3 years of medical follow-up.
A heart murmur was first detected in a healthy 38-year-old woman at an annual checkup. Because she had nosymptoms, she did not undergo further examination anda diagnosis was not made at that time. When she was 45years old, she began to experience chest tightness onexertion and was referred to the Tokyo Women’s MedicalUniversity Hospital.
A harsh, systolic ejection murmur was audible in theaortic valve area (grade 3/6), and it radiated to the neck.The upslope of the carotid pulse was sluggish, and herblood pressure was 140/80 mm Hg. The electrocardio-gram (ECG) showed typical left ventricular hypertrophy(high voltages with an ST-T strain pattern). Transthoracicechocardiography (TTE) revealed marked concentric, leftventricular hypertrophy and a parachute-like piece ofabnormal tissue protruding into the LVOT during sys-tole. Color Doppler revealed a mosaic flow pattern,which meant that there was a mechanical obstruction inthe LVOT. The peak pressure gradient (PG) across theLVOT, estimated by Doppler measurement of peak flowvelocity, was about 80 to 100 mm Hg.
To obtain more detailed information, transesophagealechocardiography (TEE) was performed (Fig 1A, 1B). Thisrevealed that the abnormal tissue was not part of themitral valve and that no other cardiac anomalies werepresent. The abnormal tissue was diagnosed as an AMV.Surgical removal was recommended, but the patientrefused to undergo an operation. An infusion of disopyr-amide reduced the mean PG across the LVOT from 60 to40 mm Hg. She was placed on oral disopyramide andfollowed.
The patient remained well until chest tightness onexertion began to occur 3 years after cardiac catheteriza-tion was performed. Echocardiography revealed that themaximum pressure gradient across the LVOT was morethan 140 mm Hg, even though she was still takingdisopyramide. She then decided to undergo surgicalrepair.
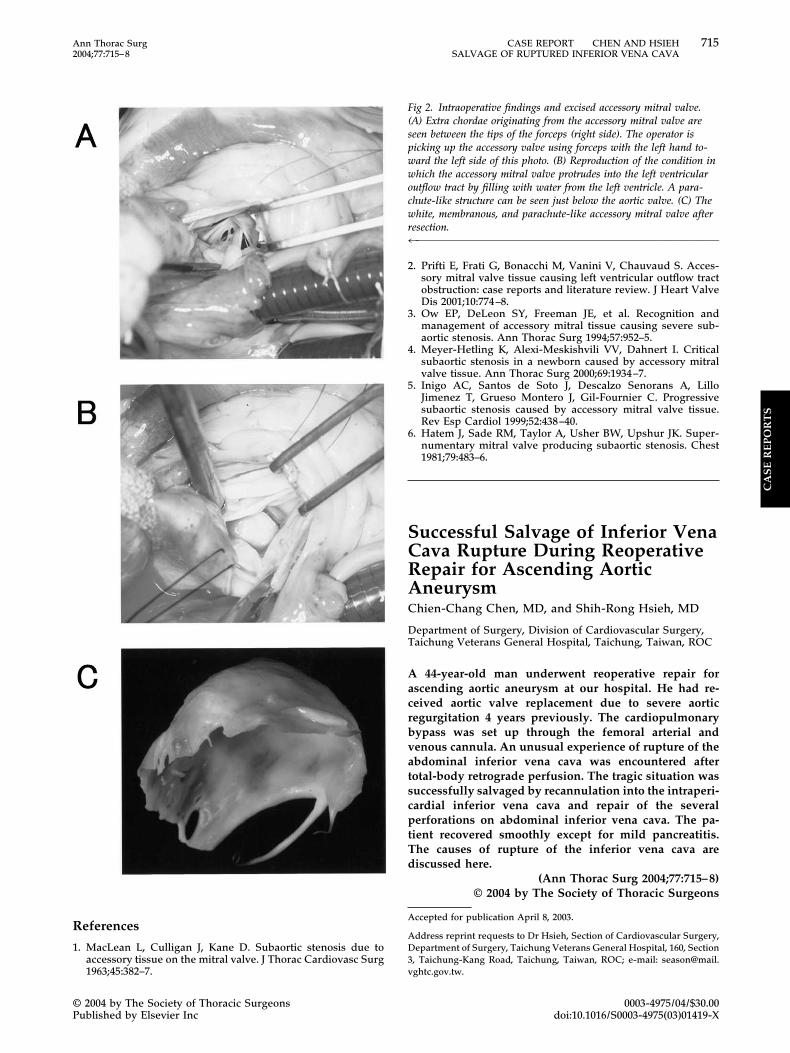
A median sternotomy was followed by an aortotomy,and the AMV was observed beneath the noncoronarycusp. It had three separate chordae that were all con-nected to the posteromedial papillary muscle. Part of theAMV was also attached to the noncoronary cusp as wellas the ventricular septum below the noncoronary cuspand the aorto-mitral continuity. Because the AMV didnot contribute to mitral valve function, it was excisedcompletely without any destruction of the valve.
Accepted for publication April 9, 2003.
Address reprint requests to Dr Aoka, 8-1 Kawada-cho Shinjuku-ku,Tokyo 162-8666, Japan; e-mail: [email protected].
713Ann Thorac Surg CASE REPORT AOKA ET AL2004;77:713–5 ACCESSORY MITRAL VALVE IN AN ADULT
© 2004 by The Society of Thoracic Surgeons 0003-4975/04/$30.00Published by Elsevier Inc doi:10.1016/S0003-4975(03)01217-7
CA
SE
RE
PO
RT
S
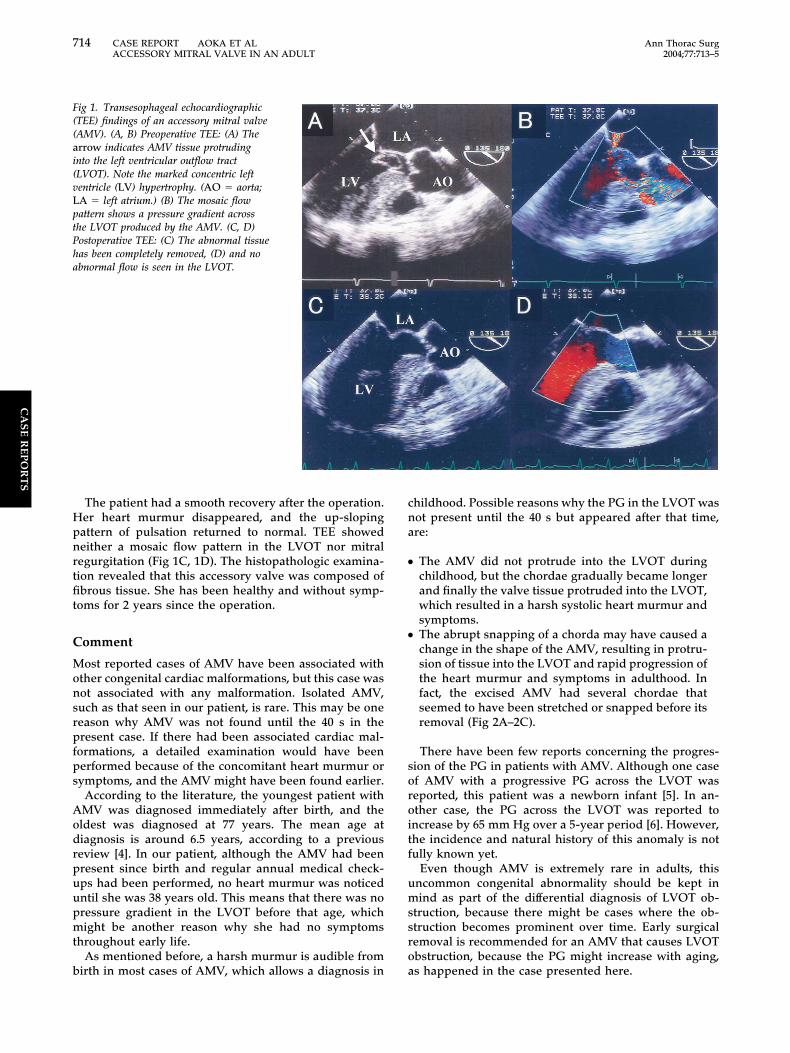
The patient had a smooth recovery after the operation.Her heart murmur disappeared, and the up-slopingpattern of pulsation returned to normal. TEE showedneither a mosaic flow pattern in the LVOT nor mitralregurgitation (Fig 1C, 1D). The histopathologic examina-tion revealed that this accessory valve was composed offibrous tissue. She has been healthy and without symp-toms for 2 years since the operation.
Comment
Most reported cases of AMV have been associated withother congenital cardiac malformations, but this case wasnot associated with any malformation. Isolated AMV,such as that seen in our patient, is rare. This may be onereason why AMV was not found until the 40 s in thepresent case. If there had been associated cardiac mal-formations, a detailed examination would have beenperformed because of the concomitant heart murmur orsymptoms, and the AMV might have been found earlier.
According to the literature, the youngest patient withAMV was diagnosed immediately after birth, and theoldest was diagnosed at 77 years. The mean age atdiagnosis is around 6.5 years, according to a previousreview [4]. In our patient, although the AMV had beenpresent since birth and regular annual medical check-ups had been performed, no heart murmur was noticeduntil she was 38 years old. This means that there was nopressure gradient in the LVOT before that age, whichmight be another reason why she had no symptomsthroughout early life.
As mentioned before, a harsh murmur is audible frombirth in most cases of AMV, which allows a diagnosis in
childhood. Possible reasons why the PG in the LVOT wasnot present until the 40 s but appeared after that time,are:
● The AMV did not protrude into the LVOT duringchildhood, but the chordae gradually became longerand finally the valve tissue protruded into the LVOT,which resulted in a harsh systolic heart murmur andsymptoms.
● The abrupt snapping of a chorda may have caused achange in the shape of the AMV, resulting in protru-sion of tissue into the LVOT and rapid progression ofthe heart murmur and symptoms in adulthood. Infact, the excised AMV had several chordae thatseemed to have been stretched or snapped before itsremoval (Fig 2A–2C).
There have been few reports concerning the progres-sion of the PG in patients with AMV. Although one caseof AMV with a progressive PG across the LVOT wasreported, this patient was a newborn infant [5]. In an-other case, the PG across the LVOT was reported toincrease by 65 mm Hg over a 5-year period [6]. However,the incidence and natural history of this anomaly is notfully known yet.
Even though AMV is extremely rare in adults, thisuncommon congenital abnormality should be kept inmind as part of the differential diagnosis of LVOT ob-struction, because there might be cases where the ob-struction becomes prominent over time. Early surgicalremoval is recommended for an AMV that causes LVOTobstruction, because the PG might increase with aging,as happened in the case presented here.
Fig 1. Transesophageal echocardiographic(TEE) findings of an accessory mitral valve(AMV). (A, B) Preoperative TEE: (A) Thearrow indicates AMV tissue protrudinginto the left ventricular outflow tract(LVOT). Note the marked concentric leftventricle (LV) hypertrophy. (AO � aorta;LA � left atrium.) (B) The mosaic flowpattern shows a pressure gradient acrossthe LVOT produced by the AMV. (C, D)Postoperative TEE: (C) The abnormal tissuehas been completely removed, (D) and noabnormal flow is seen in the LVOT.
714 CASE REPORT AOKA ET AL Ann Thorac SurgACCESSORY MITRAL VALVE IN AN ADULT 2004;77:713–5
CA
SE
RE
PO
RT
S
References
1. MacLean L, Culligan J, Kane D. Subaortic stenosis due toaccessory tissue on the mitral valve. J Thorac Cardiovasc Surg1963;45:382–7.
2. Prifti E, Frati G, Bonacchi M, Vanini V, Chauvaud S. Acces-sory mitral valve tissue causing left ventricular outflow tractobstruction: case reports and literature review. J Heart ValveDis 2001;10:774–8.
3. Ow EP, DeLeon SY, Freeman JE, et al. Recognition andmanagement of accessory mitral tissue causing severe sub-aortic stenosis. Ann Thorac Surg 1994;57:952–5.
4. Meyer-Hetling K, Alexi-Meskishvili VV, Dahnert I. Criticalsubaortic stenosis in a newborn caused by accessory mitralvalve tissue. Ann Thorac Surg 2000;69:1934–7.
5. Inigo AC, Santos de Soto J, Descalzo Senorans A, LilloJimenez T, Grueso Montero J, Gil-Fournier C. Progressivesubaortic stenosis caused by accessory mitral valve tissue.Rev Esp Cardiol 1999;52:438–40.
6. Hatem J, Sade RM, Taylor A, Usher BW, Upshur JK. Super-numentary mitral valve producing subaortic stenosis. Chest1981;79:483–6.
Successful Salvage of Inferior VenaCava Rupture During ReoperativeRepair for Ascending AorticAneurysmChien-Chang Chen, MD, and Shih-Rong Hsieh, MD
Department of Surgery, Division of Cardiovascular Surgery,Taichung Veterans General Hospital, Taichung, Taiwan, ROC
A 44-year-old man underwent reoperative repair forascending aortic aneurysm at our hospital. He had re-ceived aortic valve replacement due to severe aorticregurgitation 4 years previously. The cardiopulmonarybypass was set up through the femoral arterial andvenous cannula. An unusual experience of rupture of theabdominal inferior vena cava was encountered aftertotal-body retrograde perfusion. The tragic situation wassuccessfully salvaged by recannulation into the intraperi-cardial inferior vena cava and repair of the severalperforations on abdominal inferior vena cava. The pa-tient recovered smoothly except for mild pancreatitis.The causes of rupture of the inferior vena cava arediscussed here.
(Ann Thorac Surg 2004;77:715–8)© 2004 by The Society of Thoracic Surgeons
Accepted for publication April 8, 2003.
Address reprint requests to Dr Hsieh, Section of Cardiovascular Surgery,Department of Surgery, Taichung Veterans General Hospital, 160, Section3, Taichung-Kang Road, Taichung, Taiwan, ROC; e-mail: [email protected].
Fig 2. Intraoperative findings and excised accessory mitral valve.(A) Extra chordae originating from the accessory mitral valve areseen between the tips of the forceps (right side). The operator ispicking up the accessory valve using forceps with the left hand to-ward the left side of this photo. (B) Reproduction of the condition inwhich the accessory mitral valve protrudes into the left ventricularoutflow tract by filling with water from the left ventricle. A para-chute-like structure can be seen just below the aortic valve. (C) Thewhite, membranous, and parachute-like accessory mitral valve afterresection.4™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™
715Ann Thorac Surg CASE REPORT CHEN AND HSIEH2004;77:715–8 SALVAGE OF RUPTURED INFERIOR VENA CAVA
© 2004 by The Society of Thoracic Surgeons 0003-4975/04/$30.00Published by Elsevier Inc doi:10.1016/S0003-4975(03)01419-X
CA
SE
RE
PO
RT
S





























