Embed Size (px)
Citation preview

Available online at www.sciencedirect.com
Cognitive and Behavioral Practice 19 (2012) 463-471www.elsevier.com/locate/cabp
Acceptance-Enhanced Behavior Therapy for Trichotillomania in Adolescents
Kathi M. Fine, Michael R. Walther, Jessica M. Joseph, Jordan Robinson, Emily J. Ricketts,William E. Bowe, Douglas W. Woods, University of Wisconsin–Milwaukee
Keyw
1077© 20Publ
Although several studies have examined the efficacy of Acceptance Enhanced Behavior Therapy (AEBT) for the treatment oftrichotillomania (TTM) in adults, data are limited with respect to the treatment of adolescents. Our case series illustrates the use ofAEBT for TTM in the treatment of two adolescents. The AEBT protocol (Woods & Twohig, 2008) is a structured treatment manualthat was adapted to the individual clients’ needs and clinical progress. Both clients reported clinically significant gains in treatment asdetermined by at least 2 weeks of abstinence from pulling, and subjective reports of decreased distress and impairment, although onerequired a booster session due to relapse. AEBT is worth further exploration as a treatment for adolescents with TTM.
T RICHOTILLOMANIA (TTM) is characterized by therepeated pulling out of one's hair, resulting in
noticeable hair loss (American Psychiatric Association,2000). Other diagnostic criteria include a rising sense oftension or urge preceding the pulling episode and a senseof relief following a pulling episode, although childrenand adolescents may not readily report these symptoms(Franklin et al., 2008; Hanna, 1997; Tolin et al., 2008).TTM predominantly occurs in women by a ratio ofapproximately 8:1 (Christenson, Mackenzie, & Mitchell,1991; Cohen et al., 1995; Woods et al., 2006), althoughthis gender discrepancy may be less pronounced inchildren (Chang, Lee, Chiang, & Lü, 1991; Muller, 1987).
Individuals with TTM may pull from any site on thebody, but the most common include the scalp, eyebrows,and eyelashes (Cohen et al., 1995; Santhanam, Fairley, &Rogers, 2008). Patients with TTM may engage in pre-pulling behaviors such as hair stroking or twirling, as wellas post-pulling behaviors (i.e., hair ingestion, stroking hairstrands across the lips, and chewing, biting, or examiningthe hair root; du Toit, van Kradenburg, Niehaus, & Stein,2001).
Several studies have examined the efficacy of pharma-cological and nonpharmacological interventions for TTM.Research on various selective serotonin reuptake inhibitors(SSRIs) has beenmixed, with open trials showing a positive
ords: trichotillomania; ACT; habit reversal
-7229/11/463-471$1.00/011 Association for Behavioral and Cognitive Therapies.ished by Elsevier Ltd. All rights reserved.
effect on pulling (Koran, Ringold, &Hewlett, 1992; Stanley,Bowers, Swann, & Taylor, 1991; Winchel, Jones, Stanley,Molcho, & Stanley, 1992) but placebo-controlled double-blind crossover studies suggesting SSRIs produce no benefitover placebo (Bloch et al., 2007; Christenson, Mackenzie,Mitchell, & Callies, 1991; Streichenwein & Thornby, 1995).
Another antidepressant, clomipramine, has showngreater efficacy than SSRIs (Bloch et al., 2007). Morerecently, N-acetylcysteine (Grant, Odlaug & Kim, 2009)and olanzapine (Van Ameringen, Mancini, Patterson,Bennett & Oakman, 2010) have been shown to be moreefficacious than pill placebo in double-blind randomizedcontrolled studies. Unfortunately, controlled studies ofmedication for TTM have been conducted primarily withadults, leaving the efficacy of medications for childrenwith TTM untested.
Nonpharmacological treatments typically involve someform of behavior therapy. Various behavioral techniqueshave been used, either as stand-alone interventions or incombination with each other. These include relaxationtraining, self-monitoring, reinforcement programs, andstimulus control (Diefenbach, Tolin, Hannan, Maltby, &Crocetto, 2006; Salama & Salama, 1999; van Minnen,Hoogduin, Keijsers, Hellenbrand, & Hendriks, 2003).The behavioral intervention with the strongest empiricalsupport as a treatment for TTM is Habit Reversal Training(HRT). HRT consists of three primary techniques,including awareness, competing response, and socialsupport training (Azrin & Nunn, 1973). HRT or HRT-based treatment packages have demonstrated efficacy insingle-subject studies (Mouton & Stanley, 1996; Rapp,Miltenberger, Long, Elliot, & Lumley, 1998; Rosenbaum,1982; Tarnowski, Rosen, McGrath, & Drabman, 1987) and

464 Fine et al.
in group studies utilizing waitlist (van Minnen, et al;Woods, Wetterneck, & Flessner, 2006), alternate treat-ment (Azrin, Nunn, & Frantz, 1980), and pill placebo(Ninan, Rothbaum, Marstellar, Knight & Eccard, 2000)control conditions. Across these studies, HRT has beenfound to be more efficacious than the control conditions(Bloch et al., 2007).
Although HRT has been found to be effective inreducing TTM symptoms, there are limitations. First,treatment research has rarely included children andadolescents, although the one published open trial inchildren suggests that HRT in conjunction with stimuluscontrol (i.e., a group of techniques designed to preventpulling and provide alternative tactile reinforcement) canbe effective in this population (Tolin, Franklin, Diefenbach,Anderson,&Meunier, 2007). Second, there is little evidenceto suggest that complete elimination of pulling is a standardoutcome. Reasons are unclear, but may have to do with thedifferent styles of pulling believed to bepresent inmanywithTTM.One style, automatic pulling, is a habitual pattern thatoften occurs out of awareness and is likelymaintained by thesensory consequences of the hair pulling act itself. HRTplusstimulus control has been suggested as particularly well-suited to treat this style of pulling (Walther, Ricketts,Conelea, & Woods, 2010). Focused pulling, on the otherhand, appears more purposeful and is believed to serve anemotional regulatory function. Unfortunately, there isevidence suggesting HRT does not significantly impactnegative emotions (Teng, Woods, & Twohig, 2006), andthus may be less effective in treating the focused style ofpulling. Because both styles of pulling are believed to bepresent in most adolescents and adults who pull (Flessner,Woods, Franklin, Keuthen, & Piacentini, 2009), when onlyHRT and stimulus control are used, our clinical experienceindicates that treatment gainsmay be incomplete if a personalso engages in focused pulling.
To address this concern in adults, a combined Accep-tance and Commitment Therapy (ACT) and HRT ap-proach, labeled Acceptance Enhanced Behavior Therapy(AEBT) for TTM was developed. ACT is based on theassumption that psychological problems are brought about,in large part, by experiential avoidance (Hayes, Strosahl, &Wilson, 1999), or the person's tendency to avoid, control, orescape from unwanted private experiences such asthoughts, urges, or emotions. In TTM, it is believed thatthe act of pulling regulates these internal experiences andas such, the pulling itself is used to avoid or escape fromunwanted private events (Wetterneck & Woods, 2007).Indeed, data exist showing a link betweenTTM severity andexperiential avoidance (Begotka, Woods, & Wetterneck,2004), and other evidence suggests that experientialavoidance mediates the relationship between thoughtsand emotions and pulling severity (Norberg, Wetterneck,Woods, Conelea, 2007).
Researchers have begun to examine the efficacy of thiscombined approach in adult samples with TTM. Apreliminary investigation of AEBT using a multiplebaseline design showed that treatment was effective inreducing the number of hairs pulled to rates approachingzero in 80% of the participants (Twohig & Woods, 2004).In a follow-up study comparing AEBT to a waitlist control,AEBT was found to be effective in decreasing hair-pullingseverity, number of hairs pulled, overall impairment,experiential avoidance, and symptoms of anxiety anddepression (Woods, Wetterneck, et al., 2006). Evidencewas provided for the differential impact of the ACT andHRT components on TTM symptoms in a study byFlessner, Busch, Heideman, and Woods (2008).
Although several studies have examined the efficacy ofAEBT for the treatment of TTM in adults, data are limitedwith respect to the treatment of adolescents, despite the factthat both focused and automatic pulling occur commonly inadolescents with TTM. Our case series illustrates the use ofAEBT for TTM in the treatment of two adolescents withTTM. These cases were selected from a larger set to illustratevarying presentations of TTM. Protocol adaptations for theadolescents were made throughout treatment based on thespecific needs of each adolescent.
Assessment
Patients seeking treatment in the Trichotillomania/Body Focused Repetitive Behavior Disorders SpecialtyClinic (TTM/BFRB) at the University of Wisconsin-Milwaukee are administered a standard assessmentbattery prior to the commencement of therapy. Potentialpsychiatric disorders are evaluated using a structuredclinical interview, which is a computerized version of theNational Institutes of Mental Health Diagnostic InterviewSchedule for Children (NIMH-DISC-IV; Columbia (C-DISC) Development Group, 1999) and IQ estimates areobtained by using the 2 subtest version of the WechslerAbbreviated Scale of Intelligence (WASI; Wechsler,1999). To better characterize the patients and evaluatetreatment response, relative strengths of focused andautomatic pulling styles are assessed using the MilwaukeeInventory for Styles of Trichotillomania-Child Version(MIST-C; Flessner et al., 2007). The MIST-C is a 25-itemscale designed to assess the strength of both focused (21items—possible scores ranging from 0–189) and auto-matic (4 items—possible scores ranging from 0–36)pulling styles. In a community sample of adolescentswith TTM, the mean MIST-C Focused pulling score was95.9 (SD=35.5) and the mean automatic pulling score was13.3 (SD=8.7). The Trichotillomania Scale for Children(TSC; Tolin et al., 2008) is completed by the patient at thestart of each session to assess pulling severity. The TSC is a12-item measure assessing both pulling severity andpulling-related distress/impairment. Total scores range

465TTM in Adolescents
from 0.0–4.0. In a community sample of adolescents withTTM, the mean TSC total score was 2.11 (SD= .73). TheMIST-C and TSC (along with self-monitoring) were theonly measures of assessment used throughout treatment.
Case Descriptions1
Patient 1 (JG)
JG was a 16-year-old female Caucasian student wholived with her parents and a 12-year-old brother. Althoughseparated, her parents were attempting a reconciliation.She reported doing well in school, although she felt hergrades could have been better. On the CDISC she metcriteria for trichotillomania, but did not meet for anyother psychological disorder. Her IQ fell in the averagerange (107).
JG's mother reported that JG could be disrespectful,cynical, inflexible, irritable, anxious, intense, and hard onherself and others. The client's mother stated that she andher husband had been trying to do things to help theirdaughter. A history of generalized anxiety disorder wasendorsed and the client had been on Prozac for thisdisorder. In 7th and 8th grade, JG received behaviortherapy for her pulling and anxiety. In addition totreatment, they had purchased hair extensions and hairpieces to cover the damage.
JG had a history of nail biting and in 4th grade bit hercheeks so severely that large open sores were created. JGcontinued occasionally to bite her cheeks and pick atscabs. JG began pulling the hair on her head at the end of5th grade and pulling her eyelashes soon after her parentsseparated when she was at the end of 6th grade. JG wascurrently pulling from her scalp, eyebrows, and eyelashes,and had a grapefruit-sized bald patch on the back of herhead. JG reported pulling both when she was and was notaware of doing so. She reported having frequent urges.
JG reported that pulling interfered with her life a greatdeal and stated that it interfered with her involvement indesired activities. The pulling, and parental attempts tostop it, also created frequent family discord. For example,in order to make JG more aware, JG's brother and hermother sometimes teased her about the pulling, and JG'smother tried to make JG wear her hair down so she couldnot hide her bald patch. Difficulties with family relation-ships seemed to increase JG's hair pulling.
JG's focused pulling scale score on the MIST-C was 122and her automatic scale score was 1, suggesting a highlyfocused pattern of pulling. She frequently pulled in front ofa mirror and used a pair of tweezers. At times she pulledwithout awareness. She also reported pulling while watch-ing TV or playing video games, and engaged in post-pulling
1 Details about these cases have been modified to protect theidentities of the clients.
behaviors such as discarding hairs on the floor or in thetrash can and examining the pulled hair. It appeared asthough JG's pulling functioned to reduce aversive emo-tional states (i.e., anxiety) but also may have beenreinforced by sensory stimulation such as stroking thehair and twisting or playing with the hair.
Patient 2 (RH)
RHwas a 15-year-old Caucasian female who lived with herbiological parents, one sister, and one brother. RH reportedthat she got along well with her family, but that school wasdifficult and not enjoyable. RH's mother reported that herdaughter was having difficulties in the following areas: socialskills, eating problems, irritability, fearfulness, attention span,relating to adults, and hyperactivity. RH had been previouslydiagnosed with ADHD and OCD and was currently seeinganother psychologist for those issues and other concernsrelated to anxiety. When assessed with the CDISC, she metcriteria for trichotillomania and oppositional-defiant disor-der. Her IQ was estimated at 100.
RH's mother reported that RH used to have long, thickeyelashes and first pulled the eyelashes a month ago. RHadmitted to having pulled on two or three occasions, duringwhich many eyelashes were pulled. RH did not discuss herpulling with anyone. When two of her friends asked abouther eyelashes, RH reported being honest on one occasionand lying on another. RHhad not sought prior treatment forhair pulling.RHrecently beganpullingher scalpbecause shefelt her hair looked “uneven.” RH reported an urge to pulland was extremely bothered by her pulling. She believed itinterfered with her daily life because she (a) worried aboutother people's reactions to her pulling, (b) was teased by herbrother for pulling, and (c) was concerned that her friendswould find out about her pulling.
RH reported that almost all her pulling was due toanxiety or when she felt that her eyelashes were poking herin the eye. She also reported pulling when she was boredand felt tension around her eyelashes. RH engaged in post-pulling behaviors such as discarding hair on the floor andexamining the pulled hair. It appeared as though RH'spulling functioned primarily to reduce aversive emotionalstates (i.e., anxiety) but may also have been reinforced bysensory stimulation such as finding a thick hair or a roughor coarse hair.
Overview of AEBT
AEBT (Woods & Twohig, 2008) is a structured 10-session treatment. Consistent with many structuredtreatment manuals, clinicians are encouraged to modifythe content and number of sessions to fit the individualpatient's needs and clinical progress. As originallydeveloped, psychoeducation about TTM is conducted inSession 1. Stimulus control procedures and habit reversaltraining are introduced in Session 2 and are revisited

466 Fine et al.
throughout the remaining treatment sessions. Thesetreatment components are designed to make pullingmore difficult and to teach the client to engage in acompeting response when pulling occurs or is about tooccur. ACT components are introduced in Session 3 andcomprise the bulk of treatment through Session 9. Thesecomponents are designed to establish private events asstimuli that do not need to be controlled. Instead, the clientis encouraged to behave in ways consistent with their self-identified values. Specifically, in Session 3, the concept ofvalues is introduced and patients are encouraged to makedecisions regarding their behavior on the basis of theirvalues rather than whether something provides someimmediate relief or gratification. In Session 4, the patientis introduced to the idea that unwanted private experiences(urges, cravings, emotions) are, in the long-run, essentiallyuncontrollable, though it is likely that pulling offers theillusion of control because it is effective in the short-term. InSession 5, the patient is asked to experience the idea thatwillingness to experience unwanted private events mayultimately be more effective in allowing them to live outtheir values rather than pulling in order to control suchprivate events. As homework, patients are encouraged topractice being willing to experience these private events,while behaving in ways consistent with their values. InSessions 6 through 8, patients learn to experience thedifference between treating unwanted private experiences(i.e., urges, thoughts, emotions) as real things that require aresponse, to events occurring within one's own body thatcan simply be observed. This is a process termed defusion.Session 9 continues these activities and introduces relapseprevention techniques. In Session 10, all therapeuticcontent is reviewed and relapse prevention is furtherdiscussed.
Course of Treatment and Assessment of Progress
Patient 1 (JG)JG received 11weekly sessions. Sessions 1 and 2 consisted
of completing initial assessment measures, conducting afunctional assessment of pulling, and providing thetreatment rationale and psychoeducation about TTM.HRT and SC were implemented in Session 3. Sessions 4through 9 focused on various ACT techniques. Sessions 10and 11 consisted of developing solutions to potentialbarriers to maintaining treatment gains and discussingoptions for dealing with anxiety in other areas of JG's life.Below, we describe specific components for the HRT,stimulus control (SC), and ACT interventions as theyoccurred in each session.
Session 3. HRT and SC procedures were implementedin Session 3. JG chose “folding her arms” as a competingresponse and was asked to do the behavior for 1 minute
every time she caught herself pulling her hair or noticingher hand moving toward her head. The assessmentconducted in Sessions 1 and 2 showed that JG was mostlikely to pull while alone and in bed or in front of a mirror.To reduce the likelihood of pulling, JG was asked to keepher bedroom door open, lay in bed only when tired andready to sleep, and limit the use of a mirror to 10 minutesper day. JG agreed to these techniques.
Session 4. JG reported pulling twice over the pastweek, once because she had an urge, and another becauseshe was “stressed.” The session focused on establishingJG's values. JG discussed how fighting her urges hadaffected her life, and she wrote her epitaph stating thatshe valued others knowing who she really was.
Sessions 5 and 6. JG reported that she had pulled twotimes since the last session. One of the times she pulled 30hairs due to a strong urge. JG and the therapist discussedthe possibility that internal experiences such as urges maynot be controllable, and in fact, attempts to control themmay paradoxically intensify them in the long run. JG didnot pull before Session 6, and was praised for not pulling.In Session 6, the therapist and RG discussed acceptance asan alternative to attempts at controlling unwanted privateexperiences. The difference between the patient's abilityto control her internal vs. external behavior wereexplored through various metaphorical examples. Forhomework, JG was asked to practice following her valueswhile practicing the principles of acceptance. For eachhomework exercise, JG chose to engage in something thatwas consistent with her desire to be more fully known byothers, despite any urges that might appear. Readersexperienced in exposure and response prevention (ERP)should see overlap between these exercises and ERPprocedures, though the AEBT homework was donewithout specific use of a hierarchy, nor was it done withan implicit goal of increasing the unpleasant experiencesneeded for habituation to occur. JG determined that forher first behavioral commitment exercise she would styleher hair and wear it down a few times during the week.
Sessions 7 and 8. JG pulled once before Session 7 andonce before Session 8. When she noticed she was pulling,she stopped and did her competing response. BeforeWeek 7 she did the behavioral commitment of wearingher hair down and even dyed her hair. She was willing toaccept any urges that appeared. In Session 7, the “Talkingfor the Client” exercise was completed. In this defusionexercise, the client has the opportunity to see her urges topull hair in a different way, by having the therapist sayaloud what she believes the client to be thinking while theclient pretends to pull. After this exercise JG seemed toexperience the possibility that she could do what she

0
0.5
1
1.5
2
2.5
3
1 2 3 4 5 6 7 8 9 10 11
Session
TS
C S
core
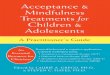
Figure 1. TSC scores by session for JG.
467TTM in Adolescents
wanted regardless of her thoughts and urges, and that shewas ultimately in control of her own actions. Exerciseswere completed in which she experienced (a) thedifference between trying to control her thoughts versuschanging her reactions to them, (b) that she had thechoice to behave consistently with her values regardless ofher private experiences, (c) taking thoughts and urgesless literally and seriously, (d) that feelings are notdangerous, and (e) that the more she struggles to controlher urges, the stronger they will become.
Session 9. The client pulled 30 eyelashes in oneperiod since Session 8. She was very upset at herself forhaving pulled and stated that at the time she pulled, shetried as hard as she could not to pull, but the urge was sostrong she had no other option. Stimulus controlprocedures were reviewed, and the patient and therapistdiscussed the difference between the urge's ability tomake her want to pull and its ability to make her pull. Forhomework JG had completed the “Taking Your UrgesWith You” exercise, in which she wrote a verbaldescription of the urge on a card and carried it with herevery day. The purpose was to help her see that in thepulling moment, pulling-related thoughts and urges feel“bad and dangerous,” but outside of that moment theyare easy to experience as just experiences. The main partof session was spent asking JG to experience internal cuesto pulling as a way to practice ACT skills.
Session 10. JG had not pulled at all the previous week.She did her homework and reported being open to anyurges that showed up. Acceptance was practiced in sessionby JG looking in a mirror while playing with her hair. JGreported that she was willing to have urges, although theydid not happen to show up this time. For relapseprevention, the strategies that had been learned intherapy were reviewed. The importance of continuingto practice cognitive defusion exercises was discussed. JGreported that she was willing to continue to engage in allthe activities she wanted to despite her urges to pull. Theclient was reminded of steps to take should she notice anincrease in pulling behavior.
Session 11. JG did not pull at all in the prior week. Itwas discussed that JG's general tendency to unsuccessfullymanage anxiety may be a useful target for futuretreatment. It was decided that this would be the lasttreatment session for TTM, as JG had completed thestandard treatment protocol, had not pulled any hair inthe last two sessions, and JG, her parents, and thetherapist were pleased with the treatment outcome. Thetherapist reminded the family that booster sessions couldbe very helpful in the future, and if JG needed furthersupport they should not hesitate to contact the clinic.
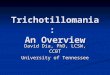
Outcomes for JG. JG reported gains in treatment (seeFigure 1 and Figure 2). Data clearly show a large decreasein pulling following the implementation of HRT/SCprocedures (i.e., the drop seen after Session 3) andadditional drops after Sessions 5 (i.e., controllability of theurge) and 9 (i.e., acceptance/defusion). Both focusedand automatic pulling on the MIST-C had droppeddramatically by the end of treatment.
Patient 2 (RH)The client received 12 weekly sessions. Sessions 1 and 2
consisted of completing initial assessment measures,conducting a functional assessment of her pulling andproviding the treatment rationale and psychoeducationabout TTM.
Session 3. In Session 3, HRT was implemented. Inreal time, the client identified her own pre-pullingbehaviors. Folding her hands and putting them in herlap (or having her hands hang straight down in the centerof her body if standing) was chosen as the competingresponse. Stimulus control procedures were discussedand included removing the large mirror on her bedroomdoor and keeping her bedroom door open, since she wasless likely to pull when others could see her.
Session 4. The client discussed the situations in whichshe had pulled over the past week. The therapist discussedvarious strategies the client could use in those situations.RH had used the competing response a few times. Theimportance of doing the competing response for everyurge and pre-pulling behavior was discussed. The sessionfocused primarily on determining the client's values andexploring how her fights against her urges have held herback from living the life she wanted. The notion thatinternal experiences do not necessarily have to causebehavior was demonstrated by asking the client to use herthoughts to influence the therapist's behavior, which shefound was to no avail.

Figure 2. MIST-C scores by session for JG.
468 Fine et al.
Sessions 5 and 6. In both sessions, the notion ofacceptance of the client's thoughts on the power of herurges was discussed. The majority of session was spentdiscussing what the client did to control her urges, and theidea that those strategies only work in the short term, butnot in the long term. The client agreed to try letting go ofattempts to control her urges. In addition, as a way topromote acceptanceof internal experiences, the differencebetween the client's ability to control her internal vs.external behavior was demonstrated and acceptance wasdefined as willfully allowing the urges to exist. Forhomework, RH was asked to engage in a valued activityduring which her urges tended to emerge (she chosetalking on the phone with a friend while sitting in front of amirror) while willfully allowing any urges to be present thatmay show up during the activity.
Sessions 7, 8, and 9. RH did not pull before any ofthese sessions. The focus of Session 7 was to change thecontext of language from language that supports privateevents as real, to language that supports private events asjust something to be experienced. Exercises werecompleted in which RH learned (a) that she has a choiceof whether to pull or not, (b) that she cannot control herthoughts but can change her reactions to them, and (c)the notion that urges cannot interfere with her values ifshe does not let them. In Session 8, defusion exerciseswere completed. The “Talking for the Client” exercise wascompleted. After this exercise, RH seemed to betterunderstand that she could do what she wanted regardlessof her thoughts and that she was ultimately in control ofher own actions. She learned (a) how to take her thoughtsand urges less literally, (b) that feelings are notdangerous, and (c) that the more she struggles to controlher urges, the stronger they will be. The differencebetween the urge's ability to make her want to pull and itsability to make her actually pull was discussed. The mainpart of session was spent with the client engaging in high-
risk pulling situations while practicing ACT skills. Theclient stated that embracing the urge was hard for her andit was discovered that she was not fully completing thebehavioral commitment exercises. She admitted shehoped not to get urges during the exercises. Whenasked to share her thoughts on the point of these variousexercises, she had some difficulty articulating what shehad learned.
Sessions 10 and 11. Sessions 9 and 10 of the manualwere completed. The client was wearing mascara for thefirst time since therapy began because she noticed thatshe had more eyelashes and she was very proud of this.The majority of sessions were spent reviewing theconcepts from therapy. The client showed an under-standing of almost all concepts, and concepts about whichshe was unclear were reviewed. The importance ofcontinued monitoring after therapy termination wasdiscussed. The difference between a lapse and relapsewas discussed. The client and her mother were encour-aged to contact the clinic for follow-up treatment if theydeemed it would be beneficial.
Session 12. The client came in for a booster session 2months after her final session because she had startedpulling again. RH reported having not been using thecompeting response consistently. She reported pullingbecause her eyelashes were bothering her and feltuneven. Lack of acceptance towards internal sensationswas discussed, as this appeared to be a contributor to theproblem. The client reported forgetting that trying tocontrol her urges does not work, and she admitted tocontinuing to try and control them. The concepts oftherapy were reviewed, with a focus on stimulus control,including doing activities around others and removingthe mirror from her bedroom. The therapist recom-mended that RH continue to come in for further sessions.RH reported that she wanted to try the techniques on herown first, and her mother did not call for additionalappointments.
Outcomes for RH. Immediately after the secondsession (completing a functional assessment and psychoe-ducation about TTM), RH demonstrated a dramaticdecrease in pulling (Figure 3 and Figure 4). There was aslight increase following HRT/SC, though pulling waslower than at the beginning of treatment. Pullingdecreased again following the discussion of values inSession 4, where it remained low until 2 months after theinitial course of treatment had ended. RH did not pull forthe last 5 sessions of treatment and was very pleased withtreatment progress. RH returned 2 months after her finalsession because she had started pulling again (after notpulling for a month after the last session). RH had a brief

0
0.5
1
1.5
2
2.5
1 2 3 4 5 6 7 8 9 10 11 12Session
TS
C S
core
Figure 3. TSC scores by session for RH.
469TTM in Adolescents
TTM history when she came in for treatment. Given thewaxing and waning nature of pulling, it is possible thatinitial symptom remission was a spontaneous occurrence.
Use of ACT With Adolescents
AEBT was modified for use with adolescents in variousways. Some adjustments were planned ahead of time whilethe majority occurred throughout therapy with eachindividual adolescent. Alterations were made with regardsto support persons, the language used, amount ofrepetition that was needed and the examples provided.One adjustment made a priori was that parents wereincluded in treatment, whereas with adults oftentimes thesupport person is a significant other (if there is one at all).At times when the adolescent disagreed with their parentsabout the need for therapy, the therapist helped theteenagerbecome ready to engage in therapy by consideringthe benefits and possible drawbacks. Although the adoles-cents had the same workbook as adult clients, the therapistsused their clinical judgment in choosing language duringtherapy that would be most understandable to the clients.The therapists also used their clinical judgment for theamount of repetition that would be necessary for eachadolescent to fully understand the concepts, and choseexamples (for the concepts) that would be relatable to the
Figure 4. MIST-C scores by session for RH.
adolescent clients. For example, in the exercise “Evaluationvs. Description,” the client is to take away the context andcognitive evaluations of their sensation and just focus on thesensation itself. In explaining this to the client, the therapistdecided how some of the feelings the client called“uncomfortable” might actually be physiologically similarto sensations that she feels when she is going to a new classormeets new people at a party. The adaptationsmentionedhere appeared to be helpful and are recommended asguidance for future adaptations with adolescents.
Although the adolescents understood many of theabstract concepts included in ACT, there were a handfulof concepts that the adolescents had difficulty under-standing. Clinical observation suggested that adults whounderwent the same protocol also had some minordifficulties understanding the abstract concepts, althoughthey appeared to understand them more completely andwith greater ease. The adolescents were able to grasp themajority of the concepts after therapists changed thelanguage used, offered more thorough explanations, andprovided extra, age-appropriate examples.
Perhaps the greatest difficulty for the adolescents wasgrasping the concept that the urge itself is not the problem,it is their attempt to control the urge that causes difficulties.Further, they had problems remembering to move towardstheir values without fighting against the urges. Likewise, theadolescents had some difficulty articulating what they hadlearned from the experiential exercises.
The majority of the more abstract concepts wereeventually understood by the adolescents, although eachadolescent had particular concepts, for which they neededfurther explanations and examples, before they werecompletely understood. For JG, it was difficult to under-stand that the urge could not make her pull no matter howstrong it was. JG remain fused with the belief that she couldcontrol her pulling if the urge was not too overpoweringand if she did not have too many urges. The concept ofhaving a “choice” whether she was going to pull or notregardless of the strengthof the urge needed tobe reviewedand experienced multiple times. JG also forgot duringtreatment that trying to control her urges does not work,and that attempts to control pulling are not effective in thelong run and more damaging than useful.
RH had difficulty thinking of her values as unattainableaspirations as opposed to short-term achievable goals. Shealso needed to be reminded numerous time that thebehavioral commitment exercises were not about “toughingout” the urges. One exercise that gave her some trouble wasthe “paper in the shoe” exercise in which she wrote down aprivate event that she attempted to control through thepulling, and then put the piece of paper it was written oninside her shoe for a week. The following explanation wasoffered to RH: The more she interacted with the paper inher shoe, the more she noticed it, in the same way that the

470 Fine et al.
more she interacted with her internal sensations, the moresalient they became. After additional explanations, RH wasable to understand this concept.
Limitations
Although it cannot be known from this study whetherACT was a necessary component for these adolescents’treatment outcomes, the authors postulate that ACTprovided important tools that allowed initial gains intreatment to be maintained, aiding in both the continuedreduction of hair pulling as well as in increasing theclients’ quality of life. Although not tested in this caseseries, it is possible that ACT was particularly useful intreating the clients’ focused pulling via reduction ofexperiential avoidance (Woods & Twohig, 2008). Futureresearch should attempt empirical analyses to determinethe relative contributions of ACT and HRT/SC compo-nents. In addition, ACT was specifically chosen in thisstudy to enhance HRT as there is a larger empirical bodyof support toward integrating HRT and ACT in thetreatment of TTM relative to other enhancementmethods. Nevertheless, it is worth noting that otherHRT-enhancement methods, such as dialectical behaviortherapy (DBT), may be effective. In at least one open trial,DBT has shown some efficacy for adults with TTM andrecently has exhibited encouraging long-term treatmentgains (Keuthen et al., 2011).
Another limitation common to clinical cases includesthe reliance on self-report measures of TTM severity. Inaddition, future studies should include pre-post measuresof acceptance or experiential avoidance and longerfollow-up assessments. Finally, these findings clearlyneed to be replicated in a larger controlled trial, andsuch a trial should include more clients of varying agesthroughout adolescence and possibly preadolescence.Inclusion of a wider age range could help determine theefficacy parameters of AEBT and, done properly, begin togive guidance as to which treatment components couldmost effectively be applied at different ages.
Summary
Trichotillomania is believed to serve multiple behav-ioral functions, including both tactile/sensory andemotional regulation functions. AEBT, a treatmentdesigned to address both sets of controlling variables,has been developed (Woods & Twohig, 2008) and testedin adult TTM samples (Twohig & Woods, 2004; Woods,Wetterneck, et al., 2006) but not in younger samples,despite the fact that the onset of TTM typically occurs inadolescence (Christensen, Mackenzie, & Mitchell, 1991).The current case series was a downward extension ofAEBT to two adolescents with TTM.
References
American Psychiatric Association. (2000). Diagnostic and statisticalmanual of mental disorders (4th ed., text revision). Washington,DC: Author.
Azrin, N. H., & Nunn, R. G. (1973). Habit reversal: A method ofeliminating nervous habits and tics. Behaviour Research and Therapy,11, 619–628. doi:10.1016/0005-7967(73)90119-8
Azrin,N.H., Nunn, R.G., & Frantz, S. E. (1980). Treatment of hairpulling(trichotillomania): A comparative study of habit reversal andnegativepractice training. Journal of Behavior Therapy and ExperimentalPsychiatry, 11, 13–20. doi:10.1016/0005-7916(80)90045-2
Begotka, A. M., Woods, D. W., & Wetterneck, C. T. (2004). Therelationship between experiential avoidance and the severity oftrichotillomania in a nonreferred sample. Journal of BehaviorTherapy and Experimental Psychiatry, 35, 17–24. doi:10.1016/j.jbtep.2004.02.001
Bloch, M. H., Landeros-Weisenberger, A., Dombrowski, P., Kelmendi, B.,Wegner, R., Nudel, J.,…Coric, V. (2007). Systematic review:Pharmacological and behavioral treatment for Trichotillomania.Biological Psychiatry, 62, 839–846. doi:10.1016/j.biopsych.2007.05.019
Chang, C. H., Lee, M. B., Chiang, Y. C., Lü, Y. C. (1991).Trichotillomania: A clinical study of 36 patients. Journal of theFormosan Medical Association, 90, 176–180.
Christenson, G. A., Mackenzie, T. B., & Mitchell, J. E. (1991).Characteristics of 60 adult chronic hair pullers. The AmericanJournal of Psychiatry, 148, 365–370.
Christenson,G.A.,Mackenzie, T.B.,Mitchell, J. E., &Callies, A. L. (1991).A placebo-controlled, double blind crossover study of fluoxetinetreatment. The American Journal of Psychiatry, 148, 1566–1571.
Cohen, L. J., Stein, D. J., Simeon, D., Spadaccini, E., Rosen, J.,Aronowitz, B., & Hollander, E. (1995). Clinical profile, comor-bidity, and treatment history in 123 hair pullers: A survey study.Journal of Clinical Psychiatry, 56, 319–326.
Columbia DISC Development Group. (1999). Computerized DiagnosticInterview Schedule for Children, (4th ed.). New York: Author.
Diefenbach, G. J., Tolin, D. F., Hannan, S., Maltby, N., & Crocetto, J.(2006). Group treatment for trichotillomania: Behavior therapyversus supportive therapy. Behavior Therapy, 37, 353–363. doi:10.1016/j.beth.2006.01.006
du Toit, P. L., van Kradenburg, J., Niehaus, D. J. H., & Stein, D. J.(2001). Characteristics and phenomenology of hair pulling: Anexploration of subtypes. Comprehensive Psychiatry, 42, 247–256. doi:10.1053/comp. 2001.23134
Flessner, C. A., Busch, A. M., Heideman, P. W., & Woods, D. W. (2008).Acceptance Enhanced Behavior Therapy (AEBT) for trichotillo-mania and chronic skin picking: Exploring the effects ofcomponent sequencing. Behavior Modification, 32, 579–594. doi:10.1177/0145445507313800
Flessner, C.A.,Woods, D.W., Franklin,M.E., Keuthen,N. J., & Piacentini,J. (2009). Cross-sectional study of women with trichotillomania: Apreliminary examination of pulling styles, severity, phenomenology,and functional impact. Child Psychiatry and Human Development, 40,153–167. doi:10.1007/s10578-008-0118-5
Flessner, C. A.,Woods, D.W., Franklin,M. E., Keuthen,N. J., Piacentini, J.C., Cashin, S. E., &Moore, P. S. (2007). TheMilwaukee Inventory forStyles of Trichotillomania-Child Version (MIST-C): The assessmentof pulling subtypes in children and adolescents. Behavior Modifica-tion, 31, 896–918. doi:10.1177/0145445507302521
Franklin,M. E., Flessner, C. A.,Woods, D.W., Keuthen,N. J., Piacentini, J.C., Moore, P.,… Wilson, M. A. (2008). The Child and AdolescentTrichotillomania Impact Project (CA-TIP): Descriptive psychopa-thology, comorbidity, functional impairment, and treatmentutilization. Journal of Developmental and Behavioral Pediatrics, 29,493–500. doi:10.1097/DBP.0b013e31818d4328
Grant, J. E., Odlaug, B. L., & Kim, S. W. (2009). N-acetylcysteine, aglutamate modulator, in the treatment of trichotillomania: Adouble-blind placebo-controlled study. Archives of General Psychiatry,66, 756–763. doi:10.1001/archgenpsychiatry.2009.60
Hanna, G. L. (1997). Trichotillomania and related disorders inchildren and adolescents. Psychiatry and Human Development, 27,255–268. doi:10.1007/BF02353354

471TTM in Adolescents
Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (1999). Acceptance andcommitment therapy: An experiential approach to behavior change. NewYork: The Guilford Press.
Keuthen, N. J., Rothbaum, B. O., Falkenstein, M. J., Meunier, S.,Timpano, K. R., Jenike, M. A., and Welch, S. S. (2011). DBT-enhanced habit reversal treatment for trichotillomania: 3-and 6-month follow-up results. Depression and Anxiety, 28, 310–313.
Koran, L. M., Ringold, A., & Hewlett, W. (1992). Fluoxetine fortrichotillomania: An open clinical trial. Psychopharmacology Bulletin,28, 145–149.
Mouton, S. G., & Stanley, M. A. (1996). Habit reversal training fortrichotillomania: A group approach. Cognitive Behavioral Practice, 3,159–182. doi:10.1016/S1077-7229(96)80036-8
Muller, S. A. (1987). Trichotillomania. Dermatologic Clinics, 5, 595–601.Ninan, P. T., Rothbaum, B. O., Marsteller, F. A., Knight, B. T., &
Eccard, M. B. (2000). A placebo-controlled trial of cognitivebehavior therapy and clomipramine. The Journal of ClinicalPsychiatry, 61, 47–50.
Norberg, M. M., Wetterneck, C. T., Woods, D. W., & Conelea, C. A.(2007). Experiential avoidance as a mediator of relationshipsbetween cognitions and severity of chronic hairpulling. BehaviorModification, 31, 367–381. doi:10.1177/0145445506297343
Rapp, J. T., Miltenberger, R. G., Long, E. S., Elliott, A., & Lumley, V.(1998). Simplified habit reversal treatment for chronic hair-pulling in three adolescents: A clinical replication with directobservation. Journal of Applied Behavior Analysis, 31, 299–302. doi:10.1901/jaba.1998.31-299
Rosenbaum, M. S. (1982). Treating hair pulling in a 7-year old male:Modified habit reversal for use in pediatric settings. Journal ofDevelopmental and Behavioral Pediatrics, 3, 241–243. doi:10.1097/00004703-198212000-00013
Salama, S. A., & Salama, A. A. (1999). New behavioral approach totrichotillomania. The American Journal of Psychiatry, 156, 1469–1470.
Santhanam, R., Fairley, M., & Rogers, M. (2008). Is it Trichotillomania?Hair pulling inChildhood:Adevelopmental perspective.Clinical ChildPsychology and Psychiatry, 13, 409–418. doi:10.1177/1359104508090604
Stanley, M. A., Bowers, T. C., Swann, A. C., & Taylor, D. J. (1991).Treatment of trichotillomania with fluoxetine. The Journal ofClinical Psychiatry, 52, 282.
Streichenwein, S. M., & Thornby, J. I. (1995). A long-term, double-blind placebo controlled study crossover trial of the efficacy offluoxetine for trichotillomania. The American Journal of Psychiatry,152, 1192–1196.
Tarnowski, K. J., Rosen, L. A., McGrath, M. L., & Drabman, R. S.(1987). A modified habit reversal procedure in a recalcitrant caseof trichotillomania. Journal of Behavior Therapy & ExperimentalPsychiatry, 18, 157–163. doi:10.1016/0005-7916(87)90030-9
Teng, E. J., Woods, D. W., & Twohig, M. P. (2006). Habit reversal as atreatment for chronic skin picking: A pilot investigation. BehaviorModification, 30, 411–422. doi:10.1177/0145445504265707
Tolin,D. F., Diefenbach,G. J., Flessner,C.A., Franklin,M. E., Keuthen,N.J., Moore, P.,…Woods, D. W. (2008). The trichotillomania scale forchildren: Development and validation. Child Psychiatry and HumanDevelopment, 39, 331–349. doi:10.1007/s10578-007-0092-3
Tolin, D. F., Franklin, M. E., Diefenbach, G. J., Anderson, E., &Meunier, S. A. (2007). Pediatric trichotillomania: Descriptivepsychopathology and an open trial of cognitive-behavioraltherapy. Cognitive Behaviour Therapy, 36, 129–144. doi:10.1080/16506070701223230
Twohig, M. P., & Woods, D. W. (2004). A preliminary investigation ofacceptance and commitment therapy and habit reversal as atreatment for trichotillomania. Behavior Therapy, 35, 803–820. doi:10.1016/S0005-7894(04)80021-2
VanAmeringen,M.,Mancini, C., Patterson, B., Bennett,M., &Oakman, J.(2010). A randomized, double-blind, placebo-controlled trial ofolanzapine in the treatment of trichotillomania.The Journal of ClinicalPsychiatry, 71, 1336–1343.
van Minnen, A., Hoogduin, K. A., Keijsers, G. P., Hellenbrand, I., &Hendriks, G. J. (2003). Treatment of trichotillomania withbehavioral therapy or fluoxetine: A randomized, waiting-listcontrolled study. Archives of General Psychiatry, 60, 517–522. doi:10.1001/archpsyc.60.5.517
Walther, M. R., Ricketts, E. J., Conelea, C. A., & Woods, D. W. (2010).Recent advances in the understanding and treatment oftrichotillomania. Journal of Cognitive Psychotherapy, 24, 46–64. doi:10.1891/0889-8391.24.1.46
Wechsler, D. A. (1999). Wechsler abbreviated scale of intelligence. SanAntonio, TX: The Psychological Corporation.
Wetterneck, C. T. & Woods, D. W. (2007). A contemporary behavioranalytic model of trichotillomania. In D. W. Woods, & J. Kanter(Eds.), Understanding behavior disorders: A contemporary behavioralperspective (pp. 157–180). Reno, NV: Context Press.
Winchel, R. M., Jones, J. S., Stanley, B., Molcho, A., & Stanley, M.(1992). Clinical characteristics of trichotillomania and itsresponse to fluoxetine. Journal of Clinical Psychiatry, 53, 304–308.
Woods, D. W., Flessner, C. A., Franklin, M. E., Keuthen, N. J., Goodwin,R. D., Stein, D. J. …Trichotillomania Learning Center ScientificAdvisory Board. (2006). The trichotillomania impact project(TIP): Exploring phenomenology, functional impairment, andtreatment utilization. The Journal of Clinical Psychiatry, 2006,1877–1888. doi:10.4088/JCP.v67n1207
Woods, D. W. & Twohig, M. P. (2008). Acceptance-enhanced behaviortherapy for trichotillomania (Therapist's guide). New York: OxfordUniversity Press.
Woods, D. W., Wetterneck, C. T., & Flessner, A. (2006). A controlledevaluation of acceptance and commitment therapy plus habitreversal for trichotillomania. Behaviour Research and Therapy, 44,639–656. doi:10.1016/j.brat.2005.05.006
Address correspondence to Douglas W. Woods, Ph.D., Department ofPsychology, University of Wisconsin-Milwaukee, Milwaukee, WI 53211;e-mail: [email protected].
Received: February 17, 2011Accepted: October 21, 2011Available online 13 December 2011