Embed Size (px)
Citation preview
292
Accelerated rehabilitation after anteriorcruciate ligament reconstruction *
K. DONALD SHELBOURNE,† MD, AND PAUL NITZ, MD
From the Methodist Sports Medicine Center, Indianapolis, Indiana
ABSTRACT
To overcome many of the complications after ACLreconstruction (prolonged knee stiffness, limitation ofcomplete extension, delay in strength recovery, anteriorknee pain), yet still maintain knee stability, we devel-oped a rehabilitation protocol that emphasizes full kneeextension on the first postoperative day and immediateweightbearing according to the patient’s tolerance. Of800 patients who underwent intraarticular ACL patellartendon-bone graft reconstruction, performed by thesame surgeon, the last 450 patients have followed theaccelerated rehabilitation schedule as outlined in the
protocol. A longer than 2 year followup is recorded for73 of the patients in the accelerated rehabilitation
group. On the 1 st postoperative day, we encouragedthese patients to walk with full weightbearing and fullknee extension. By the 2nd postoperative week, thepatients with a 100° range of motion participated in aguided exercise and strengthening program. By the 4thweek, patients were permitted unlimited activities of
daily living and were allowed to return to light sportsactivities as early as the 8th week if the Cybex strengthscores of the involved extremity exceeded 70% of thescores of the noninvolved extremity and the patienthad completed a sport-specific functional/agility pro-gram. The patient database was compiled from fre-
quent clinical examinations, periodic knee question-naires, and objective information, such as range ofmotion measurements, KT-1000 values, and Cybexstrength scores. A series of graft biopsies obtained atvarious times have revealed no adverse histologic re-action. The evidence indicates that in this population,the accelerated rehabilitation program has been moreeffective than our initial program in reducing limitationsof motion (particularly knee extension) and loss of
strength while maintaining stability and preventing an-terior knee pain.
Rehabilitation after ACL reconstruction plays a major rolein the functional outcome of the extremity. 3,6,9, 16, 23 Proto-cols for rehabilitation programs2, 3, 5, 6 locus on range of mo-tion, weightbearing, strength recovery, and functional returnto activities. The protocols that have been
published2, ~’ 6, ~’ 16, ~~ vary as far as prescribed length of re-habilitation and expected rate of recovery. Within the lastseveral years, there has been a trend toward earlier range ofmotion and muscle strengthening exercises,4, 16, 25, 26 despiteadverse conclusions obtained from laboratory studies withanimals and cadaver specimens.7, 17 Clinical rehabilitationprotocols have been tempered by constraints advocatingpostoperative immobilization followed by a gradual progres-sion in range of motion and strengthening exercises beforereturn to full activities. The lengthy rehabilitation, alongwith the technical intricacies of intraarticular reconstructionand its potential complications has caused both surgeonsand patients to be hesitant in choosing this form of treat-ment.10, 11,13,20
In 1982, we began to treat ACL deficient knees selectedfor surgical management with a modified Jones patellartendon-bone graft procedure, followed by immobilization.Full weightbearing without braces was not permitted for 6to 8 weeks. In 1983, the program of rigid immobilization wasdiscarded in favor of immediate continuous passive motion.&dquo;For the next 2 years we used a rehabilitation protocol slightlymodified from that used by Noyes et al.1’ and Paulos et allWhen comparing the patients’ results to compliance withrehabilitation protocol, we found that patients who werenoncompliant (in that they progressed as they desired andobtained full extension earlier than instructed) returned tonormal function (without developing instability) sooner
than patients who complied with the regimen. To ensurethat no adverse effects were occurring as a result of earlyfull extension and weightbearing, we carefully followed non-compliant patients and found they had no adverse sequelae.From that point, we gradually advanced the rehabilitation
’Presented at the 15th annual meeting of the AOSSM, Traverse City,Michigan, July 1989
t Address correspondence and reprnt requests to. K Donald Shelbourne,MD, Methodist Sports Medicine Center, 1815 North Capitol Avenue, Suite 600,Indianapolis, IN 46202
293
schedule, maintaining the objective and subjective databasesfor comparison with previously obtained data. Based on thecontinued and long-term success of the accelerated rehabil-itation protocol, we discontinued use of the orthosis, allowedearly weightbearing to tolerance, and permitted return toactivities at the time the patient felt he or she was ready (ifobjective goals other than time since surgery were met).Over the next several years, analysis of subjective and ob-jective data confirmed clinical impressions that full range ofmotion was obtained more quickly and more completely,severe muscle atrophy was prevented or reversed sooner,and patellofemoral joint symptoms occurred less frequentlyunder the accelerated program than under the initial pro-gram of rehabilitation that was used in the group of patientstreated in the early 1980s. By the end of 1986, the rehabili-tation protocol for all patients surgically treated for ACLreconstruction was changed to the program advocated inthis paper, i.e., the accelerated rehabilitation protocol.To document clinical impressions of the effect of the
accelerated rehabilitation, we devised a comparative studywhere the subjective and objective data gathered from pa-tients who followed the initial form of rehabilitation were
compared to the data obtained from patients who followedthe accelerated protocol of rehabilitation. The results of thisstudy indicate that after ACL reconstruction, full knee mo-tion and leg strength can return more quickly than previ-ously thought, without adverse effects on stability. Theadvantages of the accelerated rehabilitation protocol include1) increased patient cooperation and compliance, 2) earlierreturn to normal function and athletic activities, 3) decreasein incidence of patellofemoral joint symptoms, and 4)marked decrease in the number of procedures required toobtain full knee extension.
MATERIALS AND METHODS
Patient population
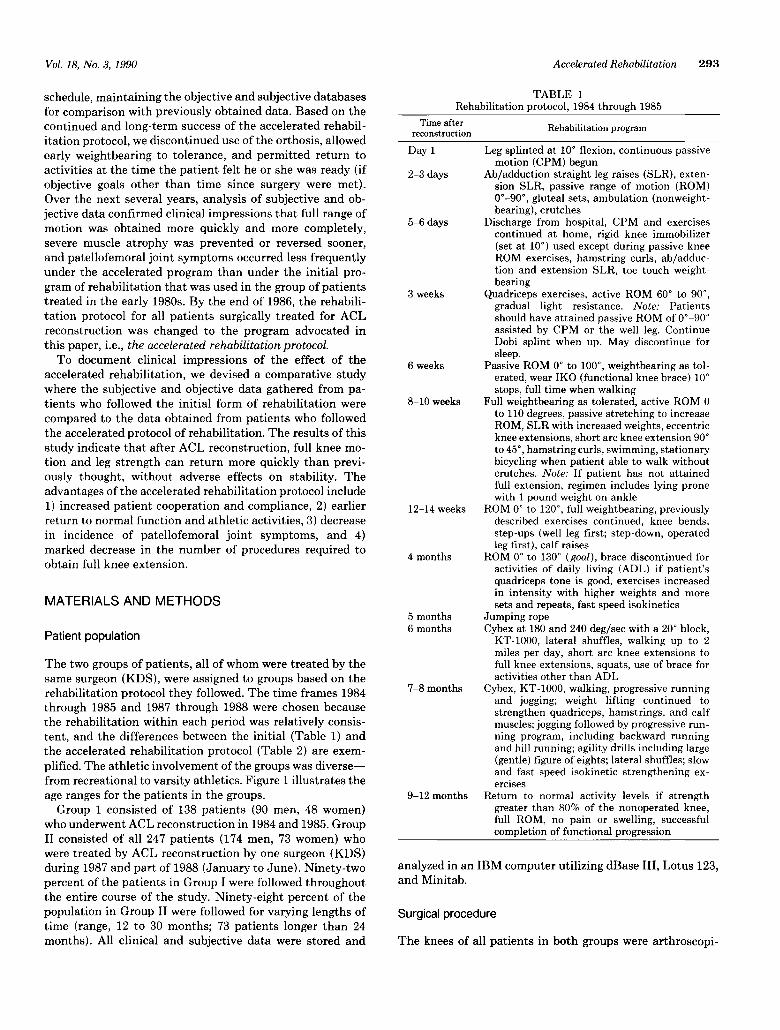
The two groups of patients, all of whom were treated by thesame surgeon (KDS), were assigned to groups based on therehabilitation protocol they followed. The time frames 1984through 1985 and 1987 through 1988 were chosen becausethe rehabilitation within each period was relatively consis-tent, and the differences between the initial (Table 1) andthe accelerated rehabilitation protocol (Table 2) are exem-plified. The athletic involvement of the groups was diverse-from recreational to varsity athletics. Figure 1 illustrates theage ranges for the patients in the groups.Group 1 consisted of 138 patients (90 men, 48 women)
who underwent ACL reconstruction in 1984 and 1985. GroupII consisted of all 247 patients (174 men, 73 women) whowere treated by ACL reconstruction by one surgeon (KDS)during 1987 and part of 1988 (January to June). Ninety-twopercent of the patients in Group I were followed throughoutthe entire course of the study. Ninety-eight percent of thepopulation in Group II were followed for varying lengths oftime (range, 12 to 30 months; 73 patients longer than 24months). All clinical and subjective data were stored and
TABLE 1Rehabilitation protocol, 1984 through 1985
analyzed in an IBM computer utilizing dBase III, Lotus 123,and Minitab.
Surgical procedure
The knees of all patients in both groups were arthroscopi-

294
TABLE 2Accelerated rehabilitation program, 1987 through 1988
cally evaluated and any internal lesions arthroscopicallymanaged (for example, repair or partial excision of themeniscus, depending on the nature of the tear) before ACLreconstruction was performed using the modified Jones tech-nique. 14 A 6 cm anteromedial arthrotomy incision was usedto expose the intercondylar notch and to place the tibial andfemoral bone tunnels-both of which were drilled with can-nulated reamers free-handed over a guide pin. A 10 mm widecentral portion of patellar tendon with 2.5 cm of patellarand tibial bone at each end of the tendon graft was securedwith three #2 Polydec (Deknatel, Inc., Floral Park, NY)sutures in the bone at each end of the graft. These sutureswere tied over a convex 19 mm button (Biomet, Inc., War-saw, IN) that was snugly interfaced to the recipient bone
Figure 1. Distribution of patient population (Groups I and II)by age.
surface with the concave surface of the button facing thebone so that the graft could self-adjust. An additional 3 cmlongitudinal incision was required over the distal lateralfemoral surface to permit fixation of the graft on the proxi-mal side. After fixation of the graft, the knee was put througha full range of motion to ensure proper tightness of the graftand to guarantee that the graft was not impinged in theintercondylar notch. Additional notchplasty and/or retight-ening of the graft at one of the ends was performed ifindicated.
Rehabilitation
Rehabilitation protocol, 1984 and 1985. Group I patientsunderwent the rehabilitation protocol used at that time(Table 1). The involved leg was splinted in slight flexion.The patient was allowed to bear partial weight with crutchesduring the first 6 weeks. The agility program began 7 to 8months after the ACL reconstruction. By 9 months, a returnto all activities with a knee brace was permitted it Cybexstrength results were greater than 80% of the noninvolvedextremity, range of motion was near normal, and the func-tional progression had been completed. Most patients, how-ever, were unable to return to their preinjury activity levelsat 9 months and expressed their dissatisfaction with thedelay.
Rehabilitation protocol, 1987 and 1988. Group II patientsfollowed the accelerated schedule of rehabilitation (Table2), which was notable for the comparatively rapid achieve-ment of various goals, particularly full extension equal tothe opposite knee. The patient’s leg was not immobilizedafter the procedure; continuous passive motion and weight-bearing began on Day 1, and the patient usually returned tolight sports activities by 2 months and full activity 4 to 6months after the reconstruction. Frequent follow-up exam-inations were performed on all patients by the surgeon(KDS) during the first 4 weeks; we feel this is the criticaltime for obtaining full extension. Initial Cybex assessmentalong with the initial KT-1000 evaluations was accom-

295
plished 5 to 6 weeks postoperation. Similar testing wasscheduled at 10 weeks, 16 weeks, 6 months, 8 to 10 months,1 year, and yearly thereafter. KT-1000 measurements wereroutinely performed on each patient by the same therapistin order to avoid interobserver discrepancies for any onepatient’s clinical course. To facilitate the return of kines-thetic sense about the knee while improving patient compli-ance with the protocol, athletic activities, such as shootingbasketballs and hitting a tennis ball, were permitted as soonas they could be tolerated by the patient. Return to fullcompetition, however, was generally not condoned until atleast 4 to 6 months after surgery. Permission to return to
sports was contingent upon achieving near normal strengthin the involved extremity, full knee extension, no kneeeffusion, and completion of a running program. A functionalknee brace (Indiana Knee Orthosis, Indiana Brace Com-pany, Indianapolis, IN) was recommended during partici-pation in athletic competition for the lst postoperative year.
Clinical follow-up evaluation and analysis
The clinical examinations for both groups included range ofmotion assessment and stability tests (Lachman and pivotshift). Objective assessment included KT-1000 measure-ments, range of motion measurements, and Cybex strengthevaluations. The difference between the KT-1000 scores ofthe involved and noninvolved knees at 20 pounds of forcewas recorded for analysis. Although Cybex evaluations wereperformed at 60, 180, and 240 deg/sec, only the quadricepsstrength of the index extremity at 180 deg/sec was analyzedfor this study. Subjective assessment of the knee was doneperiodically during the postoperative course using a modifiedNoyes’ knee rating scale (Fig. 2), with overall activity level(20 points walking, 10 points running, 10 points stairs, 5points jumping, and 5 points twisting) accounting for 50 ofthe 100 points. The remaining 50 points were assigned topain (20 points), stability (20 points), and swelling (10points). For comparison, the questionnaire was also admin-istered to 140 competitive athletes with normal knees (Table1).The data from the two groups of patients were compared
at corresponding time intervals. Also, the incidence of post-operative complications requiring additional treatment wasrecorded, and comparisons were made between subgroups.Unpaired t-tests were completed on all data from the twogroups.
RESULTS
The average range of motion values for each group are listedin Table 3. Compared to the averages for Group I, Group IIaverage scores indicate an earlier and more completeachievement of extension equal to the opposite knee, whichwas maintained throughout the 2 year follow-up period.Final average flexion was reached earlier by Group II thanGroup I.The Cybex average scores for quadriceps strength at 180
deg/sec appear in Table 4. At the early testing times, the
Group II mean percentage was higher than in Group I, butby 1 year there was, as expected, no difference betweenGroup I and II.The average KT-1000 arthrometer measurements of the
tibiofemoral excursion at a 20 pound force appear in Table5, Figure 3, and Figure 4.The average subjective scores on the questionnaire show
only a few points difference in the results as perceived bythe patients in both groups (Table 6). However, the resultscannot reflect the number of noncompliant patients in
Group I. The percentage of patients with a self-rated stabil-ity of 20 out of a possible 20 was 95% in Group I and 98%in II. The subjective ratings of 140 athletes (from a DivisionI NCAA school) with normal knees (Table 7) are in thesame range as the average scores of the patients who hadACL reconstructions.
Complications
Patients who had persistent difficulty in achieving full kneeextension equal to the noninvolved knee in spite of theaccelerated rehabilitation and who also had associated an-terior knee pain were offered surgical intervention. Arthros-copy was performed to excise the scar tissue at the base ofthe ACL graft and to enlarge the notch anteriorly andlaterally if necessary (Table 8). This procedure, which al-lowed for complete extension and required casting for a fewdays to ensure maintenance of full extension, was requiredin 12% of Group I patients and 4% of Group II patients.
DISCUSSION
The purpose of this retrospective study was to evaluate froma clinical perspective the results obtained in two patientpopulations-one group who followed an accelerated reha-bilitation program and another who followed our initialrehabilitation program after being treated by ACL recon-struction with the same technique by the same surgeon(KDS). We compared objective and subjective data fromboth groups of patients. We have followed patients from ourinitial regimen (Group I) for 4 to 5 years, and of the patientsin the accelerated program (Group II), we have followed 73for more than 2 years, and 174 patients for 1 year or more.The rehabilitation was not changed in cases of concomitantmeniscal repair, and since January of 1987, only one of the87 repaired menisci have clinically retorn.We sought answers regarding the range of motion
achieved, quadriceps strength, stability, and patient satis-faction. We questioned our data: Were there any adverseeffects or contraindications of the accelerated program?Were there any advantages, and did the combination ofsurgical procedure and rehabilitation program accomplishthe goal of obtaining a functional knee, sufficiently stablefor competitive athletics and free of anterior pain? To thebest of our knowledge, this is the first clinical study tocompare two different rehabilitation protocols in two groupsof men and women treated by the same technique by thesame surgeon.

296
Figure 2. Postoperative questionnaire (Noyes, reproduced by permission).
In comparing the objective data, we observed that kneeextension returned much more quickly in Group II patientsthan in Group I patients. The accelerated rehabilitationprotocol emphasizes extension, in contrast to the immobili-zation in flexion and restrictions on extension outlined inthe past. We intentionally made this change because we hadobserved through the years that after the patient returns tosports participation, extension loss frequently resulted inpatient dissatisfaction secondary to extremity pain and fa-tigue. The benefit of obtaining early full extension is re-
flected in the significant decline in the number of patientsin Group II (compared to Group I) who required surgicalmanagement for symptomatic extensor loss.
Closed kinetic exercises are emphasized in the accelerated
rehabilitation protocol, and open kinetic quadriceps exer-cises are avoided. Closed kinetic chain exercises are per-formed with the foot placed on a surface (floor, step, pedal,etc.) and the entire limb bearing a load. This causes all ofthe joints in the extremity to be compressed by the load. Inopen kinetic chain exercises (i.e., leg extensions) where thefoot is free, a relatively larger shear stress is applied to thejoint with less joint compression. In closed kinetic exercises(generally performed nearer full extension), patellofemoraljoint forces are markedly decreased compared to those forcesgenerated when the open kinetic exercises are performed inthe zone of 30° to 90° of knee flexion. 3,15,27,28 In addition,closed kinetic chain activities place functional stresses onthe joint and the extremity in ways that are similar to normal

297
TABLE 3
Range of motion (average) results for each group by time afterreconstruction
° Significantly different from Group I, P < 0.01.6 Significantly different from Group I, P < 0.05.‘ ROM measurements; a/b/c: a is degrees of hyperextension past
0, b is degrees short of 0° of extension, and c is degrees of flexion.
TABLE 4
-
Cybex quadriceps percentages at 180 deg/sec -
Q Significantly different from Group I, P < 0.01.
TABLE 5KT-1000 average differences [injured knee compared to
non injured knee (millimeters)] at 20 pounds’
° P > 0.1 at each time.
Figure 3. Differences (average) in KT-1000 measurements ofinjured knee compared to noninjured knee at 20 pounds.
weightbearing activities. We reasoned that the jointcompression that occurs when the extremity is loaded bybody weight provides inherent joint stability and allowsmore strenuous strengthening workouts without the degreeof shearing forces that occur with conventional open kineticexercises. Group II patients began closed kinetic exercises
Figure 4. Distribution of differences (average) in KT-1000measurements of injured knee compared to noninjured kneeat 20 pounds.
TABLE 6
Postoperative subjective ratings&dquo; (average) of the involved kneeb
° Scale = 1 to 100.~P>0.1 at each time.‘ No. of questionnaires averaged.
TABLE 7Subjective ratings of normal knees in 140 athletes
° Scale = 1 to 100.
TABLE 8Scar resections to obtain full extension
a No. of questionnaires averaged.
as soon as full, unsupported weightbearing on the involvedextremity was possible. We have noted that the closedkinetic exercises used in the accelerated program help de-crease postoperative anterior knee pain as well as increasesubjective stability of the involved knee and the patient’sconfidence in ambulation.
Group II averaged a quicker return of quadriceps musclestrength than Group I. However, return of quadricepsstrength appeared to depend more on the individual’s mo-

298
tivation than any other variable. The patient’s pain toler-ance and control of postoperative knee effusion seemed tointerplay with the motivational factor. Some of the compet-itive athletes in Group II regained 85% to 90% of quadricepsstrength as early as 10 weeks postoperation. These highlymotivated athletes were followed closely to determine if
there are any adverse effects resulting from allowing thepatient to proceed at his or her own pace under our guidance.To date, we have seen no complications as a result of theaccelerated program. Perhaps programs such as the one weused from 1984 through 1985 (Table 1) are excessivelyrestrictive, and activity limitations should be determined foreach patient individually. In this population, it appearedthat graft strength was sufficient to allow earlier activitiesthan previously believed without causing failure from earlyreturn to sports.
Analysis of the KT-1000 results (Figs. 3 and 4, Table 5)indicated that, as a whole, Group II patients had averagevalues equal to or better than those in Group I at correspond-ing postoperative dates. There was no tendency in eithergroup to demonstrate increasing displacement of the tibiaon the femur with advancing time from date of reconstruc-tion. Furthermore, out of 20 possible points on the subjectivestability scale, 95% of Group I patients and 98% of GroupII patients scored 20 on their most recent semiannual survey.These data confirm clinical impressions of improved recov-ery and thus provide further support for the safety of theaccelerated rehabilitation protocol.
Subjective knee evaluations were comparable for bothgroups, except that in the early postoperative course, pa-tients in Group I indicated discontent and discomfort. Manypatients in Group I had difficulty with protocol compliance,meaning they wanted to progress more rapidly than allowedby the protocol. We realized that a number of them werenoncompliant, yet they showed no adverse effects from theirincreased activity. Hence, with the revision of the protocol,Group II patients were, by the 3rd to 4th postoperative week,allowed to reti-irn to normal 1 Rrtivitip~ nf daily living. fredof encumbering braces and walking aids, and (usually) hada normal gait. We believe that these factors had much to dowith their satisfaction with the reconstruction.
With our last 450 patients having followed this protocol,we now feel confident that the accelerated rehabilitation
program will not necessarily cause graft weakening andsubsequent failure at a later time. We performed a histologicanalysis (unpublished data) of graft tissue from patients inGroups I and II who required arthroscopic procedures sub-sequent to the ACL reconstruction with autogenous patellartendon. Twelve graft biopsies were obtained from 12 pa-tients. These were longitudinal tissue samples of the graftobtained from 6 weeks to 4 3~4 years after implantation. Thetransplanted tissue had remained consistently viable, attain-ing maximum fibroblast size and number by the 6th post-operative month and proceeding in maturation to &dquo;ligamen-tization.&dquo;’, 1 24 None of the biopsy samples demonstratedmore than a partial central necrosis. These findings supportour theory that grafts can match physical stresses inherent
in the accelerated rehabilitation after ACL reconstructionwithout deleterious sequelae.The evidence from this retrospective study comparing the
objective and subjective findings in both groups shows thatan accelerated rehabilitation program, individually paced,with patients undergoing regular follow-up evaluations, of-fers advantages over conventional rehabilitation programsin terms of patient compliance and satisfaction and graftviability. Patients in the accelerated program returned tonormal function and athletic activities sooner than patientsin the conventional rehabilitation program. We detectedfewer problems with patellofemoral joint symptoms in thesepatients, and the number of procedures required to obtainfull knee extension was reduced from 12% (Group I) to 4%(Group II). Furthermore, comparative data from the twogroups in this study population demonstrate that range ofmotion, strength, and function can be achieved by an accel-erated rehabilitation regimen without compromising stabilityor putting the graft at risk.
REFERENCES
1. Amiel D, Ing D, Kleiner JB, et al The natural history of the anterior cruciateligament autograft of patellar tendon origin Am J Sports Med 14 449-462, 1986
2 Antich TB, Brewster CE. Rehabilitation of the nonreconstructed anteriorcruciate ligament-deficient knee Clin Sports Med 7 813-826, 1988
3. Arms SW, Pope MH, Johnson RJ, et al The biomechanics of anteriorcruciate ligament rehabilitation and reconstruction. Am J Sports Med 12.8-18, 1984
4 Bilko TE, Paulos LE, Feagin JA, et al. Current trends in repair andrehabilitation of complete (acute) anterior cruciate ligament injuries. Analy-sis of 1984 questionnaire completed by ACL study group Am J SportsMed 14. 143-147, 1986
5 Blackburn TA Rehabilitation of anterior cruciate ligament injuries. OrthopClin North Am 16. 241-269, 1985
6 Brewster CE, Moyens DR, Jobe FR Rehabilitation for anterior cruciatereconstruction J Orthop Sports Phys Ther 5 121-126, 1983
7 Clancy WG Jr, Narechania RG, Rosenberg TF, et al Anterior and posteriorcruciate ligament reconstruction in Rhesus monkeys A histological, mi-croangiographic and biochemical analysis. J Bone Joint Surg 63A. 1270-1284, 1981
8 Clancy WG Jr, Ray M, Zoltan DJ: Acute tears of the anterior cruciateligament Surgical versus conservative treatment J Bone Joint Surg 70A.1483-1488, 1988
9. Feagin JA. The syndrome of the torn anterior cruciate ligament OrthopClin North Am 10 81-90, 1979
10 Fullerton LR Jr, Andrews JR: Mechanical block to extension followingaugmentation of the anterior cruciate ligament A case report. Am J SportsMed 12: 166-168, 1984
11 Graf B, Uhr F Complications of intraarticular anterior cruciate reconstruc-tion Clin Sports Med 7. 835-848, 1988
12 Hughston JC. Complications of anterior cruciate ligament surgery. OrthopClin North Am 16: 237-240, 1985
13. Jones KG. Reconstruction of the anterior cruciate ligament A techniqueusing the central one-third of the patellar ligament J Bone Joint Surg 45A:925-932, 1963
14 Junst KA, Otis JC Anteropostenor tibiofemoral displacements duringisometric extension efforts The roles of external load and knee flexion
angle Am J Sports Med 13. 254-258, 198515. King S, Butterwick DJ, Cuerrier JP: The anterior cruciate ligament: A
review of recent concepts J Orthop Sports Phys Ther 8 110-122, 198616. Noyes FR, Butler DL, Grood ES, et al: Biomechanical analysis of human
ligament grafts used in knee-ligament repairs and reconstructions J BoneJoint Surg 66A 344-352, 1984
17 Noyes FR, Mangine RE, Barber S Early knee motion after open andarthroscopic anterior cruciate ligament reconstruction. Am J Sports Med15:149-160, 1987
18 Paulos L, Noyes FR, Grood ES, et al. Knee rehabilitation after anteriorcruciate ligament reconstruction and repair. Am J Sports Med 9 140-149,1981

299
19 Paulos LE, Rosenberg TD, Drawbert J, et al: Infrapatellar contracturesyndrome An unrecognized cause of knee stiffness with patella entrap-ment and patella infera Am J Sports Med 15: 331-341, 1987
20 Shelbourne KD, Whitaker HJ, McCarroll JR, et al. Anterior cruciate ligamentinjury Evaluation of intraarticular reconstruction of acute tears without
repair Am J Sports Med, in press, 199021 Skyhar MJ, Danzig LA, Hargens AR, et al: Nutrition of the anterior cruciate
ligament Effects of continuous passive motion Am J Sports Med 13 415-418,1985
22 Thomee R, Renstrom P, Grimby G, et al Slow or fast isokinetic trainingafter knee ligament surgery J Orthop Sports Phys Ther 8 475-479, 1987
23. Walla DJ, Albright JP, McAuley E, et al Hamstnng control and the unstableanterior cruciate ligament-deficient knee Am J Sports Med 13 34-39,1985
24 Yasuda K, Sasaki T. Muscle exercise after anterior cruciate ligamentreconstruction Biomechanics of the simultaneous isometric contractionmethod of the quadriceps and the hamstrings. Clin Orthop 220: 266-274,1987
25 Yasuda K, Sasaki T Exercise after anterior cruciate ligament reconstruc-tion The force exerted on the tibia by separate isometric contractions ofthe quadriceps or the hamstrings Clin Orthop 220: 275-283, 1987
DISCUSSION
Frank R. Noyes, MD, Cincinatti, Ohio: It is a pleasure todiscuss this very important paper. I fully agree with theauthors after bone-patellar tendon-bone ACL reconstruc-tion that full extension can be obtained, even right aftersurgery and certainly by 3 to 4 weeks. I also agree that theearly return of flexion is possible, certainly by 6 weeks. Earlyprogressive weightbearing, protected functional exercises(mini-squats, etc., rather than weighted, flexed heavy resist-ance exercises) are also areas of agreement. The serial ar-thrometer measurements taken postoperatively to follow APdisplacement are another good part of the authors’ program.We have also reported the success of a similar program,
although there is one exception in protocol. The results ofthis study probably apply only to bone-ligament-bone grafts;we do not know to what extent we can apply the results toother grafts. For this program, the authors performed asubsequent arthroscopic lysis of adhesions and contractureon only 11 of 247 patients. We recorded only 3 of 227 patientswho required a subsequent arthroscopic lysis for adhesions.The most frequent and common complication of ACL sur-gery is joint stiffness and contracture, which then cascadesinto further atrophy. Articular cartilage degeneration and asymptomatic knee are entirely avoidable. Surgeons shouldlook critically at their complication rates and see how theymay wish to modify their postoperative programs.
There is one aspect of this study with which I do have todisagree, and that is that the authors allow at 5 to 6 weeksafter surgery, jump roping, agility drills, and stairclimbers.In my own series, I have seen graft stretchout and patello-femoral crepitus develop in a small and I will emphasize,small, but important group of patients. I think this need notoccur. I also caution against full sports as early as 4 monthsafter surgery. We have seen arthroscopic and MRI evidenceof delayed graft maturation, again, in a small group, but whyrisk it? The authors really do not present how many of theirpatients actually got involved in these early exercises orreturned to sports at 4 months. Were there any that showeda stretchout? In the 20% of the patients with a KT-1000over 3 mm, they report a very slight stretchout. When didthis occur? And if this did occur (documented by the serialKT-1000 measurement), did they modify the program? Weneed more data on this one controversial point. Aside fromthis objection, the early protected motion and early use ofthe leg with weightbearing as these authors have presentedshould be one of the mainstays after ACL surgery.
Authors’ Reply: I would like to reiterate what Dr. Noyeshas said, in that this program has only been used in autog-enous bone-patellar tendon-bone ACL reconstructions. Thequestion as to whether a similar program can be used withother graft sources is unanswered by this study.By obtaining full extension immediately after surgery, we
attempt to prevent anterior scar formation and flexion con-tractures. We feel that flexion contractures give falsely&dquo;tight&dquo; KT-1000 results. In following our patients we havefound no tendency for the KT-1000 to change with time(unpublished data). Perhaps KT-1000 changes with time areseen with graft sources other than autogenous patellar ten-don, or as patients regain their range of motion. Once fullmotion is achieved, KT-1000 results have not changed.Most of our rehabilitation is based on guidelines and not
actual enforced protocol. If patients develop any problemsduring the rehabilitation, we adjust our guidelines appropri-ately. With the large number of closely followed patientstreated by all of the doctors in our clinic in a similar fashion,we can now confidently allow our patients to follow thisrehabilitation protocol with a high degree of success andpatient satisfaction.




























