Embed Size (px)
Citation preview
ACC/AHA PRACTICE GUIDELINES
ACC/AHA Guidelines for theManagement of Patients With Unstable Anginaand Non–ST-Segment Elevation Myocardial InfarctionA Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines(Committee on the Management of Patients With Unstable Angina)
COMMITTEE MEMBERS
EUGENE BRAUNWALD, MD, FACC, Chair
ELLIOTT M. ANTMAN, MD, FACCJOHN W. BEASLEY, MD, FAAFPROBERT M. CALIFF, MD, FACCMELVIN D. CHEITLIN, MD, FACCJUDITH S. HOCHMAN, MD, FACCROBERT H. JONES, MD, FACCDEAN KEREIAKES, MD, FACC
JOEL KUPERSMITH, MD, FACCTHOMAS N. LEVIN, MD, FACCCARL J. PEPINE, MD, FACCJOHN W. SCHAEFFER, MD, FACCEARL E. SMITH III, MD, FACEPDAVID E. STEWARD, MD, FACPPIERRE THEROUX, MD, FACC
TASK FORCE MEMBERS
RAYMOND J. GIBBONS, MD, FACC, Chair
JOSEPH S. ALPERT, MD, FACCKIM A. EAGLE, MD, FACCDAVID P. FAXON, MD, FACCVALENTIN FUSTER, MD, PHD, FACC
TIMOTHY J. GARDNER, MD, FACCGABRIEL GREGORATOS, MD, FACCRICHARD O. RUSSELL, MD, FACCSIDNEY C. SMITH, JR, MD, FACC
TABLE OF CONTENTSPreamble................................................................................................971
I. Introduction ...............................................................................972
A. Organization of Committee and Evidence Review ....972B. Purpose of These Guidelines............................................973C. Overview of the Acute Coronary Syndrome ................973
1. Definition of Terms......................................................9732. Pathogenesis of UA/NSTEMI .................................9743. Presentations of UA/NSTEMI .................................975
II. Initial Evaluation and Management ......................................976A. Clinical Assessment ............................................................976
1. ED or Outpatient Facility Presentation ..................9782. Questions to be Addressed at the Initial
Evaluation .......................................................................978B. Early Risk Stratification.....................................................978
1. Estimation of the Level of Risk ................................9792. Rationale for Risk Stratification ...............................9793. The History ....................................................................980
Anginal Symptoms ...................................................980Demographics and History in Diagnosis andRisk Stratification ....................................................981
4. Noncardiac Causes of Exacerbation of SymptomsSecondary to Myocardial Ischemia ..........................981
5. Assessment of Risk of Death in Patients WithUA/NSTEMI ................................................................982
Physical Examination...............................................982
This document was approved by the American College of Cardiology Board ofTrustees in June 2000 and by the American Heart Association Science Advisory andCoordinating Committee in June 2000.
When citing this document, the American College of Cardiology and theAmerican Heart Association would appreciate the following citation format: Braun-wald E, Antman EM, Beasley JW, Califf RM, Cheitlin MD, Hochman JS, JonesRH, Kereiakes D, Kupersmith J, Levin TN, Pepine CJ, Schaeffer JW, Smith EE III,Steward DE, Theroux P. ACC/AHA guidelines for the management of patients withunstable angina and non–ST-segment elevation myocardial infarction: a report of theAmerican College of Cardiology/American Heart Association Task Force on PracticeGuidelines (Committee on the Management of Patients With Unstable Angina).J Am Coll Cardiol 2000;36:970–1062.
This document is available on the websites of the ACC (www.acc.org) and theAHA (www.americanheart.org). Reprints of this document (the complete guidelines)are available for $5 each by calling 800-253-4636 (US only) or writing the AmericanCollege of Cardiology, Educational Services, 9111 Old Georgetown Road, Bethesda,MD 20814-1699. Ask for reprint No. 71-0188. To obtain a reprint of the shorterversion (executive summary and summary of recommendations) published in the May4, 1999, issue of Circulation, ask for reprint No. 71-0187. To purchase additionalreprints (specify version and reprint number): up to 999 copies, call 800-611-6083(US only) or fax 413-665-2671; 1000 or more copies, call 214-706-1466, fax214-691-6342, or e-mail [email protected].
Journal of the American College of Cardiology Vol. 36, No. 3, 2000© 2000 by the American College of Cardiology and the American Heart Association, Inc. ISSN 0735-1097/00/$20.00Published by Elsevier Science Inc. PII S0735-1097(00)00889-5
6. Tools for Risk Stratification .......................................983Electrocardiogram.....................................................983
7. Decision Aids That Combine Clinical Features andECG Findings ...............................................................984
8. Biochemical Cardiac Markers ....................................984Creatine Kinase .........................................................984Cardiac Troponins....................................................984Myoglobin...................................................................985Comparison of Cardiac Markers...........................986
9. Integration of Clinical History With Serum MarkerMeasurements.................................................................986
Bedside Testing for Cardiac Markers ..................98710. Other Markers ...............................................................988
C. Immediate Management....................................................9881. Chest Pain Units ...........................................................989
Potential Expansion of the Use of Chest PainUnits for Intermediate-Risk Patients ..................991Triage of Patients ....................................................991
2. Discharge From ED or Chest Pain Unit................991
III. Hospital Care ..............................................................................992Overview ..................................................................................992
A. Anti-Ischemic Therapy ....................................................9931. General Care ..................................................................9942. Use of Anti-Ischemic Drugs .....................................994
Nitrates ........................................................................994Morphine Sulfate ......................................................996b-Adrenergic Blockers.............................................996Calcium Antagonists ................................................997Other............................................................................999
B. Antiplatelet and Anticoagulation Therapy....................9991. Antiplatelet Therapy (Aspirin, Ticlopidine,
Clopidogrel)..................................................................1000Aspirin.......................................................................1000Adenosine Diphosphate Receptor Antagonists andOther Antiplatelet Agents....................................1002
2. Anticoagulants .............................................................1003Unfractionated Heparin ........................................1003Low-Molecular-Weight Heparin .......................1004LMWH Versus UFH ...........................................1004Hirudin and Other Direct ThrombinInhibitors ..................................................................1006Long-Term Anticoagulation................................1007
3. Platelet GP IIb/IIIa Receptor Antagonists...........1007Thrombolysis ...........................................................1010
C. Risk Stratification..............................................................10101. Care Objectives............................................................10112. Noninvasive Test Selection .....................................10123. Selection for Coronary Angiography......................10134. Patient Counseling......................................................1013
D. Early Conservative Versus Invasive Strategies ...........10131. General Principles .......................................................1013
Rationale for the Early Conservative Strategy.....1014Rationale for the Early Invasive Strategy..............1014
Immediate Angiography .....................................1014Deferred Angiography.........................................1015
2. Care Objectives............................................................1015
IV. Coronary Revascularization ...................................................1018A. General Principles.............................................................1018B. Percutaneous Coronary Intervention ..........................1020
1. Platelet Inhibitors and PercutaneousRevascularization .........................................................1021
C. Surgical Revascularization ...............................................1023D. Conclusions .......................................................................1025
V. Hospital Discharge and Post–Hospital DischargeCare ...........................................................................................1025A. Medical Regimen ..............................................................1026
1. Long-Term Medical Therapy..................................1026B. Postdischarge Follow-Up ................................................1026C. Use of Medications .........................................................1028D. Risk Factor Modification ................................................1028E. Medical Record ................................................................1029
VI. Special Groups..........................................................................1029A. Women................................................................................1029
1. Stress Testing...............................................................10302. Management ...............................................................10303. Data on UA/NSTEMI..............................................10304. Conclusions .................................................................1031
B. Diabetes Mellitus ..............................................................10311. Coronary Revascularization.......................................10322. Conclusions...................................................................1033
C. Post-CABG Patients .......................................................10331. Pathological Findings.................................................10332. Clinical Findings and Approach ............................10333. Conclusions...................................................................1034
D. Elderly Patients .................................................................10341. Pharmacological Management .................................10342. Observations in UA/NSTEMI ..............................10343. Interventions and Surgery .........................................10354. Conclusions .................................................................1036
E. Cocaine................................................................................10361. Coronary Artery Spasm.............................................10372. Treatment ....................................................................1037
F. Variant (Prinzmetal’s) Angina .......................................10381. Clinical Picture ............................................................10382. Pathogenesis ................................................................10383. Diagnosis.......................................................................10394. Treatment ....................................................................10395. Prognosis .......................................................................1039
G. Syndrome X........................................................................10391. Definition and Clinical Picture................................10392. Treatment ....................................................................1040
Appendix 1.Definition of Terminology Related to UA........................1040
Appendix 2.Abbreviations.............................................................................1041
Staff ......................................................................................................1044References...........................................................................................1044
PREAMBLE
It is important that members of the medical profession playa significant role in the critical evaluation of the use ofdiagnostic procedures and therapies in the management andprevention of disease states. Rigorous and expert analysis ofthe available data that document the relative benefits andrisks of those procedures and therapies can produce helpfulguidelines that improve the effectiveness of care, optimize
971JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina

patient outcomes, and favorably affect the overall cost of carethrough a focus of resources on the most effective strategies.
The American College of Cardiology (ACC) and theAmerican Heart Association (AHA) have jointly engagedin the production of such guidelines in the area of cardio-vascular disease since 1980. This effort is directed by theACC/AHA Task Force on Practice Guidelines, whosecharge is to develop and revise practice guidelines forimportant cardiovascular diseases and procedures. Expertsin the subject under consideration are selected from bothorganizations to examine subject-specific data and to writeguidelines. The process includes additional representativesfrom other medical practitioner and specialty groups whereappropriate. Writing groups are specifically charged toperform a formal literature review, to weigh the strength ofevidence for or against a particular treatment or procedure,and to include estimates of expected health outcomes wheredata exist. Patient-specific modifiers, comorbidities, andissues of patient preference that might influence the choiceof particular tests or therapies are considered, as well asfrequency of follow-up and cost-effectiveness.
The ACC/AHA Task Force on Practice Guidelinesmakes every effort to avoid any actual or potential conflictsof interest that might arise as a result of an outsiderelationship or a personal interest of a member of thewriting panel. Specifically, all members of the writing panelare asked to provide disclosure statements of all such relation-ships that might be perceived as real or potential conflicts ofinterest. These statements are reviewed by the parent taskforce, reported orally to all members of the writing panel atthe first meeting, and updated as changes occur.
These practice guidelines are intended to assist physiciansin clinical decision making by describing a range of generallyacceptable approaches for the diagnosis, management, orprevention of specific diseases or conditions. These guide-lines represent an attempt to define practices that meet theneeds of most patients in most circumstances. The ultimatejudgment regarding the care of a particular patient must bemade by the physician and patient in light of all of theavailable information and the circumstances presented bythat patient.
The executive summary and recommendations are pub-lished in the September 5, 2000, issue of Circulation. Thefull text is published in the Journal of the American College ofCardiology. Reprints of the full text and the executivesummary are available from both organizations. Theseguidelines have been officially endorsed by the AmericanCollege of Emergency Physicians* and the Society forCardiac Angiography and Interventions.
Raymond J. Gibbons, MD, FACCChair, ACC/AHA Task Force on Practice Guidelines
I. INTRODUCTION
A. Organization of Committee and Evidence Review
The ACC/AHA Task Force on Practice Guidelines wasformed to make recommendations regarding the diagnosisand treatment of patients with known or suspected cardio-vascular disease. Coronary artery disease (CAD) is theleading cause of death in the United States. Unstable angina(UA) and the closely related condition non–ST-segmentelevation myocardial infarction (NSTEMI) are very com-mon manifestations of this disease. In recognition of theimportance of the management of this common entity andof the rapid advances in the management of this condition,the need to revise guidelines published by the Agency forHealth Care Policy and Research (AHCPR) and theNational Heart, Lung, and Blood Institute (NHLBI) in1994 (1) was evident. This Task Force therefore formed thecurrent committee to develop guidelines for the manage-ment of UA and NSTEMI, supported by the Agency forHealthcare Research and Quality’s USCF-StanfordEvidence-Based Practice Center. This document shouldserve as a useful successor to the 1994 AHCPR guideline.
The committee members reviewed and compiled pub-lished reports through a series of computerized literaturesearches of the English-language literature since 1994 and afinal manual search of selected articles. Details of thespecific searches conducted for particular sections are pro-vided when appropriate. Detailed evidence tables weredeveloped whenever necessary with the specific criteriaoutlined in the individual sections. The recommendationsmade were based primarily on these published data. Theweight of the evidence was ranked highest (A) if the datawere derived from multiple randomized clinical trials thatinvolved large numbers of patients and intermediate (B) ifthe data were derived from a limited number of randomizedtrials that involved small numbers of patients or from carefulanalyses of nonrandomized studies or observational regis-tries. A lower rank (C) was given when expert consensuswas the primary basis for the recommendation.
The customary ACC/AHA classifications I, II, and IIIare used in tables that summarize both the evidence andexpert opinion and provide final recommendations for bothpatient evaluation and therapy:
Class I: Conditions for which there is evidence and/orgeneral agreement that a given procedure ortreatment is useful and effective
Class II: Conditions for which there is conflicting ev-idence and/or a divergence of opinion about theusefulness/efficacy of a procedure or treatmentClass IIa: Weight of evidence/opinion is in
favor of usefulness/efficacyClass IIb: Usefulness/efficacy is less well es-
tablished by evidence/opinionClass III: Conditions for which there is evidence and/or
general agreement that the procedure/
*Endorsement by ACEP means that ACEP agrees with the general concepts in theguidelines and believes that the developers have begun to define a process of care thatconsiders the best interests of patients with unstable angina and non–ST-segmentelevation myocardial infarction.
972 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062

treatment is not useful/effective and in somecases may be harmful
A complete list of the thousands of publications onvarious aspects of this subject is beyond the scope of theseguidelines; only selected references are included. The Com-mittee consisted of acknowledged experts in general internalmedicine representing the American College of Physicians–American Society of Internal Medicine (ACP-ASIM),family medicine from the American Academy of FamilyPhysicians (AAFP), emergency medicine from the Ameri-can College of Emergency Physicians (ACEP), thoracicsurgery from the Society of Thoracic Surgeons (STS), andgeneral cardiology, as well as individuals with recognizedexpertise in more specialized areas, including noninvasivetesting, preventive cardiology, coronary intervention, andcardiovascular surgery. Both the academic and private prac-tice sectors were represented. The Agency for HealthcareResearch and Quality UCSF-Stanford Evidence-BasedPractice Center provided support for the guidelines. Thisdocument was reviewed by 3 outside reviewers nominatedby ACC, 3 outside reviewers nominated by AHA, 3 outsidereviewers nominated by ACEP, 1 outside reviewer nomi-nated by AAFP, 1 outside reviewer nominated by ACP-ASIM, 1 outside reviewer nominated by the EuropeanSociety of Cardiology, 1 outside reviewer nominated bySTS, and 29 outside reviewers nominated by the Commit-tee. This document was approved for publication by thegoverning bodies of ACC and AHA. These guidelines willbe reviewed 1 year after publication and yearly thereafter bythe Task Force to determine whether revision is necessary.These guidelines will be considered current unless the TaskForce revises them or withdraws them from distribution.
These guidelines overlap several previously published ACC/AHA practice guidelines, including the ACC/AHA Guide-lines for the Management of Patients With Acute MyocardialInfarction and the ACC/AHA/ACP-ASIM Guidelines forthe Management of Patients With Chronic Stable Angina.
B. Purpose of These Guidelines
These guidelines address the diagnosis and managementof patients with UA and the closely related conditionNSTEMI. These life-threatening disorders are a majorcause of emergency medical care and hospitalization in theUnited States. In 1996 alone, the National Center forHealth Statistics reported 1,433,000 hospitalizations forUA or NSTEMI (2). Nearly 60% of hospital admissions ofpatients with UA as the primary diagnosis were amongpersons .65 years old, and 46% of such patients of all ageswere women. In 1997, there were 5,315,000 visits to USemergency departments (EDs) for the evaluation of chestpain and related symptoms (3). The prevalence of thispresentation of CAD ensures that many healthcare provid-ers who are not cardiovascular specialists will encounterpatients with UA/NSTEMI in the course of the treatmentof other diseases, especially in outpatient and ED settings.
These guidelines are intended to assist both cardiovascularspecialists and nonspecialists in the proper evaluation andmanagement of patients with an acute onset of symptomssuggestive of these conditions. These clinical practice guide-lines also provide recommendations and supporting evi-dence for the continued management of patients with theseconditions in both inpatient and outpatient settings. Thediagnostic and therapeutic strategies that are recommendedare supported by the best available evidence and expertopinion. The application of these principles with carefullyreasoned clinical judgment reduces, but does not eliminate,the risk of cardiac damage and death in patients who presentwith symptoms suggestive of UA.
C. Overview of the Acute Coronary Syndrome
1. Definition of Terms. UA/NSTEMI constitutes a clin-ical syndrome that is usually, but not always, caused byatherosclerotic CAD and associated with an increased riskof cardiac death and myocardial infarction (MI). The resultsof angiographic and angioscopic studies suggest that UA/NSTEMI often results from the disruption of an athero-sclerotic plaque and a subsequent cascade of pathologicalprocesses that decrease coronary blood flow. Most patientswho die during UA/NSTEMI do so because of sudden deathor the development (or recurrence) of acute MI (AMI). Theefficient diagnosis and optimal management of these patientsmust derive from information readily available at the time ofthe initial clinical presentation. The clinical presentation ofpatients with a life-threatening acute coronary syndrome(ACS) often overlaps that of patients subsequently found notto have CAD. Moreover, some forms of MI cannot always bedifferentiated from UA at the time of initial presentation.
Acute coronary syndrome has evolved as a useful operationalterm to refer to any constellation of clinical symptoms thatare compatible with acute myocardial ischemia (Fig. 1). Itencompasses AMI (ST-segment elevation and depression,Q wave and non–Q wave) as well as UA. These guidelinesfocus on 2 components of this syndrome: UA andNSTEMI. In practice, the term possible ACS is oftenassigned first by ancillary personnel, such as emergencymedical technicians and triage nurses, early in the evaluationprocess. A guideline of the National Heart Attack AlertProgram (NHAAP) (4) summarizes the clinical informa-tion needed to make the diagnosis of possible ACS at theearliest phase of clinical evaluation (Table 1). The implica-tion of this early diagnosis for clinical management is that apatient who is considered to have an ACS should be placedin an environment with continuous electrocardiographic(ECG) monitoring and defibrillation capability, where a12-lead ECG can be obtained expeditiously and definitivelyinterpreted within 10 min. The most urgent priority of earlyevaluation is to identify patients with AMI who should beconsidered for immediate reperfusion therapy and to recog-nize other potentially catastrophic causes of sudden patientdecompensation, such as aortic dissection.
Patients diagnosed as having an AMI suitable for reper-
973JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
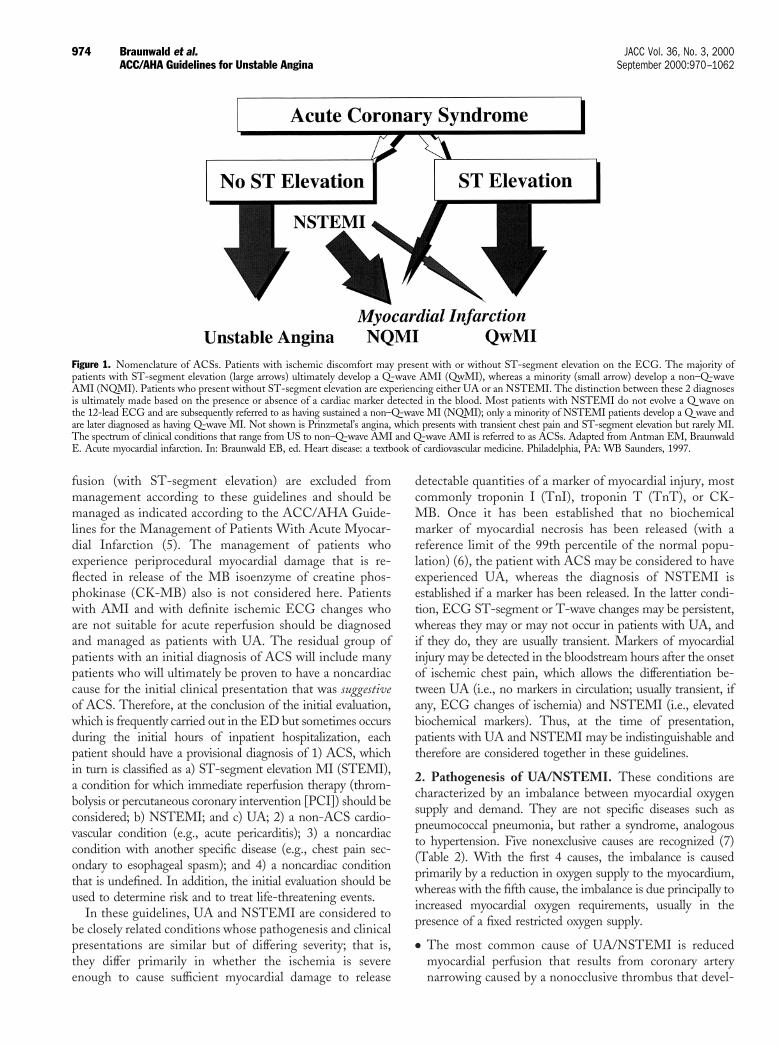
fusion (with ST-segment elevation) are excluded frommanagement according to these guidelines and should bemanaged as indicated according to the ACC/AHA Guide-lines for the Management of Patients With Acute Myocar-dial Infarction (5). The management of patients whoexperience periprocedural myocardial damage that is re-flected in release of the MB isoenzyme of creatine phos-phokinase (CK-MB) also is not considered here. Patientswith AMI and with definite ischemic ECG changes whoare not suitable for acute reperfusion should be diagnosedand managed as patients with UA. The residual group ofpatients with an initial diagnosis of ACS will include manypatients who will ultimately be proven to have a noncardiaccause for the initial clinical presentation that was suggestiveof ACS. Therefore, at the conclusion of the initial evaluation,which is frequently carried out in the ED but sometimes occursduring the initial hours of inpatient hospitalization, eachpatient should have a provisional diagnosis of 1) ACS, whichin turn is classified as a) ST-segment elevation MI (STEMI),a condition for which immediate reperfusion therapy (throm-bolysis or percutaneous coronary intervention [PCI]) should beconsidered; b) NSTEMI; and c) UA; 2) a non-ACS cardio-vascular condition (e.g., acute pericarditis); 3) a noncardiaccondition with another specific disease (e.g., chest pain sec-ondary to esophageal spasm); and 4) a noncardiac conditionthat is undefined. In addition, the initial evaluation should beused to determine risk and to treat life-threatening events.
In these guidelines, UA and NSTEMI are considered tobe closely related conditions whose pathogenesis and clinicalpresentations are similar but of differing severity; that is,they differ primarily in whether the ischemia is severeenough to cause sufficient myocardial damage to release
detectable quantities of a marker of myocardial injury, mostcommonly troponin I (TnI), troponin T (TnT), or CK-MB. Once it has been established that no biochemicalmarker of myocardial necrosis has been released (with areference limit of the 99th percentile of the normal popu-lation) (6), the patient with ACS may be considered to haveexperienced UA, whereas the diagnosis of NSTEMI isestablished if a marker has been released. In the latter condi-tion, ECG ST-segment or T-wave changes may be persistent,whereas they may or may not occur in patients with UA, andif they do, they are usually transient. Markers of myocardialinjury may be detected in the bloodstream hours after the onsetof ischemic chest pain, which allows the differentiation be-tween UA (i.e., no markers in circulation; usually transient, ifany, ECG changes of ischemia) and NSTEMI (i.e., elevatedbiochemical markers). Thus, at the time of presentation,patients with UA and NSTEMI may be indistinguishable andtherefore are considered together in these guidelines.
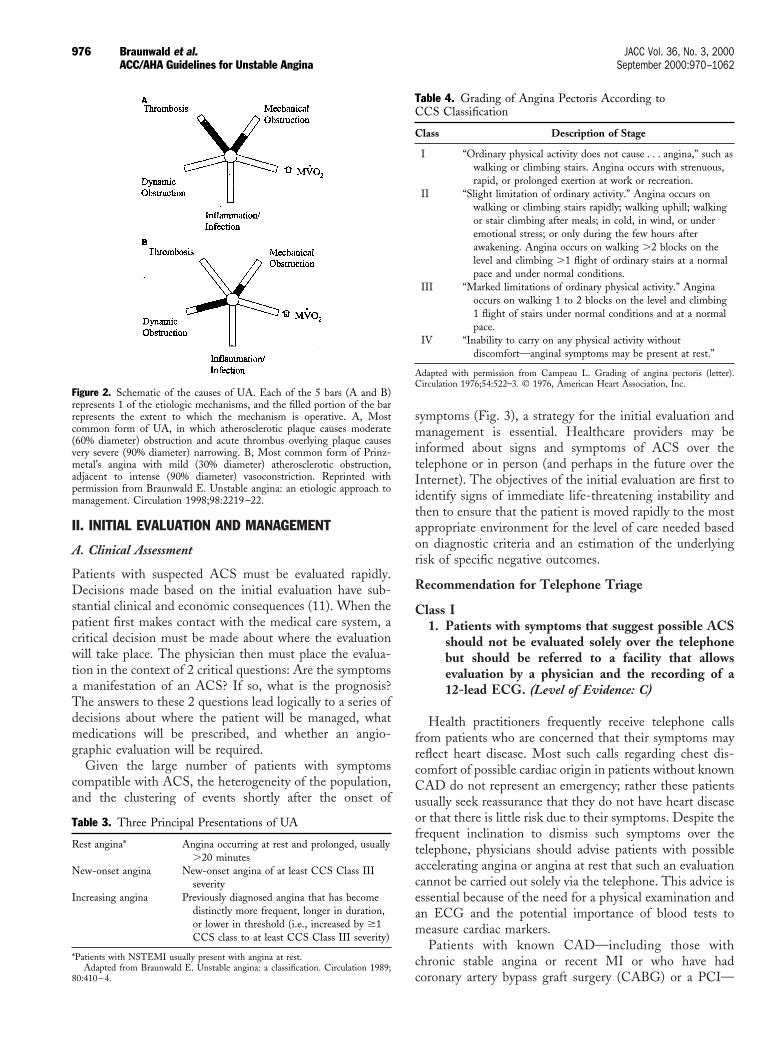
2. Pathogenesis of UA/NSTEMI. These conditions arecharacterized by an imbalance between myocardial oxygensupply and demand. They are not specific diseases such aspneumococcal pneumonia, but rather a syndrome, analogousto hypertension. Five nonexclusive causes are recognized (7)(Table 2). With the first 4 causes, the imbalance is causedprimarily by a reduction in oxygen supply to the myocardium,whereas with the fifth cause, the imbalance is due principally toincreased myocardial oxygen requirements, usually in thepresence of a fixed restricted oxygen supply.
● The most common cause of UA/NSTEMI is reducedmyocardial perfusion that results from coronary arterynarrowing caused by a nonocclusive thrombus that devel-
Figure 1. Nomenclature of ACSs. Patients with ischemic discomfort may present with or without ST-segment elevation on the ECG. The majority ofpatients with ST-segment elevation (large arrows) ultimately develop a Q-wave AMI (QwMI), whereas a minority (small arrow) develop a non–Q-waveAMI (NQMI). Patients who present without ST-segment elevation are experiencing either UA or an NSTEMI. The distinction between these 2 diagnosesis ultimately made based on the presence or absence of a cardiac marker detected in the blood. Most patients with NSTEMI do not evolve a Q wave onthe 12-lead ECG and are subsequently referred to as having sustained a non–Q-wave MI (NQMI); only a minority of NSTEMI patients develop a Q wave andare later diagnosed as having Q-wave MI. Not shown is Prinzmetal’s angina, which presents with transient chest pain and ST-segment elevation but rarely MI.The spectrum of clinical conditions that range from US to non–Q-wave AMI and Q-wave AMI is referred to as ACSs. Adapted from Antman EM, BraunwaldE. Acute myocardial infarction. In: Braunwald EB, ed. Heart disease: a textbook of cardiovascular medicine. Philadelphia, PA: WB Saunders, 1997.
974 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062

oped on a disrupted atherosclerotic plaque and is usuallynonocclusive. Microembolization of platelet aggregatesand components of the disrupted plaque is believed to beresponsible for the release of myocardial markers in manyof these patients.
● A less common cause is dynamic obstruction, which maybe caused by intense focal spasm of a segment of anepicardial coronary artery (Prinzmetal’s angina) (see Sec-tion VI. F). This local spasm is caused by hypercontrac-tility of vascular smooth muscle and/or by endothelialdysfunction. Dynamic coronary obstruction can also be
caused by the abnormal constriction of small intramuralresistance vessels.
● A third cause of UA is severe narrowing without spasm orthrombus. This occurs in some patients with progressiveatherosclerosis or with restenosis after a PCI.
● The fourth cause is arterial inflammation, perhapscaused by or related to infection, which may beresponsible for arterial narrowing, plaque destabiliza-tion, rupture, and thrombogenesis. Activated macro-phages and T-lymphocytes located at the shoulder of aplaque increase the expression of enzymes such as metal-loproteinases that may cause thinning and disruption ofthe plaque, which in turn may lead to UA/NSTEMI.
● The fifth cause is secondary UA, in which the precipitatingcondition is extrinsic to the coronary arterial bed. Thesepatients have underlying coronary atherosclerotic narrow-ing that limits myocardial perfusion, and they often havechronic stable angina. Secondary UA is precipitated byconditions that 1) increase myocardial oxygen require-ments, such as fever, tachycardia, and thyrotoxicosis; 2)reduce coronary blood flow, such as hypotension; or 3)reduce myocardial oxygen delivery, such as anemia orhypoxemia.
These 5 causes of UA/NSTEMI are not mutually exclusive(Fig. 2).
3. Presentations of UA. There are 3 principal presenta-tions of UA: 1) rest angina (angina commencing when thepatient is at rest), 2) new-onset severe angina, and 3)increasing angina (Table 3) (8). Criteria for the diagnosis ofUA are based on the duration and intensity of angina asgraded according to the Canadian Cardiovascular Society(CCS) classification (Table 4) (9).
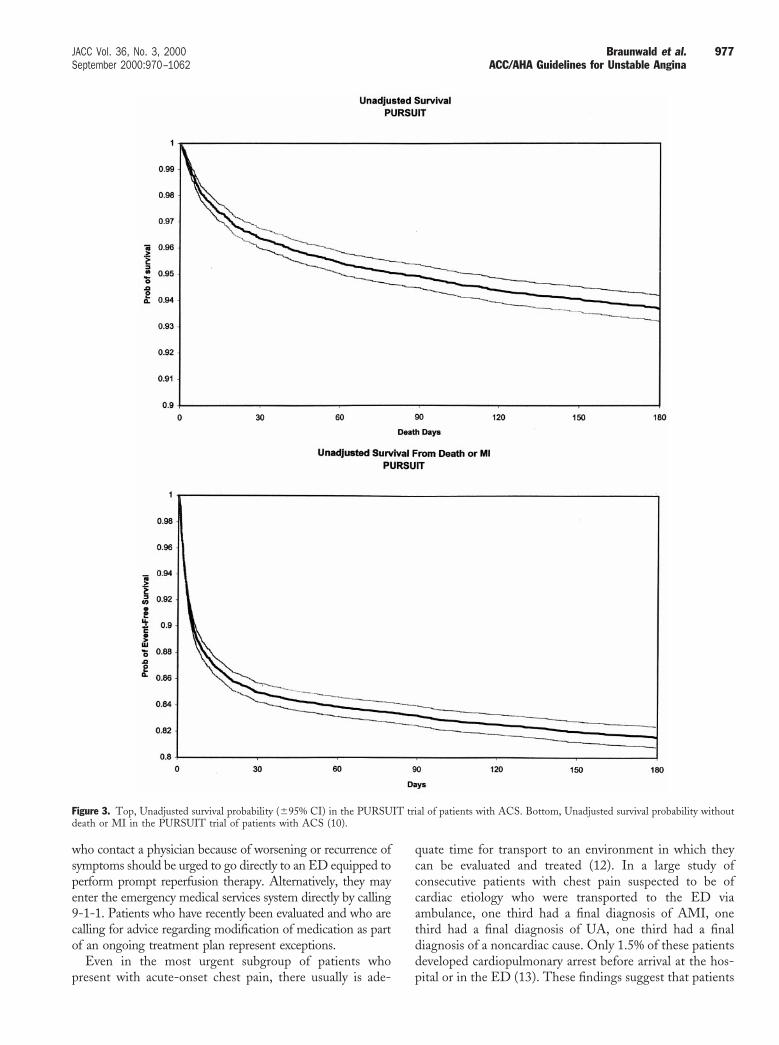
The strictness of the criteria used to define UA/NSTEMI, the rigor used in consistent application of thesecriteria, and the presence of comorbid conditions all greatlyinfluence reported mortality rates. Published series com-monly include only patients for whom a definitive diagnosisof UA has been established and do not include all patientsfrom the time of onset of symptoms. Therefore, mortalityrates observed in any series of carefully defined patients withUA/NSTEMI will tend to understate the risk. Data thatdepict survival rates and survival rates without MI, obtainedfrom 1 large trial (10) carried out with patients withUA/NSTEMI, indicate that the risk associated with anACS is greatest during the first 30 days after presentationand thereafter stabilizes at a lower rate (Fig. 3).
Table 2. Causes of UA*
Nonocclusive thrombus on pre-existing plaqueDynamic obstruction (coronary spasm or vasoconstriction)Progressive mechanical obstructionInflammation and/or infectionSecondary UA
*These causes are not mutually exclusive; some patients have $2 causes.Reprinted with permission from Braunwald E. Unstable angina: an etiologic
approach to management. Circulation 1998;98:2219–22.
Table 1. Guidelines for the Identification of ACS Patients byED Registration Clerks or Triage Nurses
Registration/Clerical StaffPatients with the following chief complaints require immediate
assessment by the triage nurse and should be referred for furtherevaluation:
Chief Complaint● Chest pain, pressure, tightness, or heaviness; pain that radiates to
neck, jaw, shoulders, back, or 1 or both arms● Indigestion or “heartburn”; nausea and/or vomiting associated with
chest discomfort● Persistent shortness of breath● Weakness, dizziness, lightheadedness, loss of consciousness
Triage NursePatients with the following symptoms and signs require immediate
assessment by the triage nurse for the initiation of the ACS protocol:
Chief Complaint● Chest pain or severe epigastric pain, nontraumatic in origin, with
components typical of myocardial ischemia or MI:Central/substernal compression or crushing chest painPressure, tightness, heaviness, cramping, burning, aching sensationUnexplained indigestion, belching, epigastric painRadiating pain in neck, jaw, shoulders, back, or 1 or both arms
● Associated dyspnea● Associated nausea and/or vomiting● Associated diaphoresis
If these symptoms are present, obtain stat ECG.
Medical HistoryThe triage nurse should take a brief, targeted, initial history with an
assessment of current or past history of:● CABG, angioplasty, CAD, angina on effort, or AMI● NTG use to relieve chest discomfort● Risk factors, including smoking, hyperlipidemia, hypertension,
diabetes mellitus, family history, and cocaine use
This brief history must not delay entry into the ACS protocol.
Special ConsiderationsWomen may present more frequently than men with atypical chest pain
and symptoms.
Diabetic patients may have atypical presentations due to autonomicdysfunction.
Elderly patients may have atypical symptoms such as generalizedweakness, stroke, syncope, or a change in mental status.
Adapted from National Heart Attack Alert Program. Emergency department: rapididentification and treatment of patients with acute myocardial infarction. USDepartment of Health and Human Services, US Public Health Service, NationalInstitutes of Health, National Heart, Lung, and Blood Institute; September 1993;NIH Publication No. 93-3278.
975JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
II. INITIAL EVALUATION AND MANAGEMENT
A. Clinical Assessment
Patients with suspected ACS must be evaluated rapidly.Decisions made based on the initial evaluation have sub-stantial clinical and economic consequences (11). When thepatient first makes contact with the medical care system, acritical decision must be made about where the evaluationwill take place. The physician then must place the evalua-tion in the context of 2 critical questions: Are the symptomsa manifestation of an ACS? If so, what is the prognosis?The answers to these 2 questions lead logically to a series ofdecisions about where the patient will be managed, whatmedications will be prescribed, and whether an angio-graphic evaluation will be required.
Given the large number of patients with symptomscompatible with ACS, the heterogeneity of the population,and the clustering of events shortly after the onset of
symptoms (Fig. 3), a strategy for the initial evaluation andmanagement is essential. Healthcare providers may beinformed about signs and symptoms of ACS over thetelephone or in person (and perhaps in the future over theInternet). The objectives of the initial evaluation are first toidentify signs of immediate life-threatening instability andthen to ensure that the patient is moved rapidly to the mostappropriate environment for the level of care needed basedon diagnostic criteria and an estimation of the underlyingrisk of specific negative outcomes.
Recommendation for Telephone Triage
Class I1. Patients with symptoms that suggest possible ACS
should not be evaluated solely over the telephonebut should be referred to a facility that allowsevaluation by a physician and the recording of a12-lead ECG. (Level of Evidence: C)
Health practitioners frequently receive telephone callsfrom patients who are concerned that their symptoms mayreflect heart disease. Most such calls regarding chest dis-comfort of possible cardiac origin in patients without knownCAD do not represent an emergency; rather these patientsusually seek reassurance that they do not have heart diseaseor that there is little risk due to their symptoms. Despite thefrequent inclination to dismiss such symptoms over thetelephone, physicians should advise patients with possibleaccelerating angina or angina at rest that such an evaluationcannot be carried out solely via the telephone. This advice isessential because of the need for a physical examination andan ECG and the potential importance of blood tests tomeasure cardiac markers.
Patients with known CAD—including those withchronic stable angina or recent MI or who have hadcoronary artery bypass graft surgery (CABG) or a PCI—
Figure 2. Schematic of the causes of UA. Each of the 5 bars (A and B)represents 1 of the etiologic mechanisms, and the filled portion of the barrepresents the extent to which the mechanism is operative. A, Mostcommon form of UA, in which atherosclerotic plaque causes moderate(60% diameter) obstruction and acute thrombus overlying plaque causesvery severe (90% diameter) narrowing. B, Most common form of Prinz-metal’s angina with mild (30% diameter) atherosclerotic obstruction,adjacent to intense (90% diameter) vasoconstriction. Reprinted withpermission from Braunwald E. Unstable angina: an etiologic approach tomanagement. Circulation 1998;98:2219–22.
Table 3. Three Principal Presentations of UA
Rest angina* Angina occurring at rest and prolonged, usually.20 minutes
New-onset angina New-onset angina of at least CCS Class IIIseverity
Increasing angina Previously diagnosed angina that has becomedistinctly more frequent, longer in duration,or lower in threshold (i.e., increased by $1CCS class to at least CCS Class III severity)
*Patients with NSTEMI usually present with angina at rest.Adapted from Braunwald E. Unstable angina: a classification. Circulation 1989;
80:410–4.
Table 4. Grading of Angina Pectoris According toCCS Classification
Class Description of Stage
I “Ordinary physical activity does not cause . . . angina,” such aswalking or climbing stairs. Angina occurs with strenuous,rapid, or prolonged exertion at work or recreation.
II “Slight limitation of ordinary activity.” Angina occurs onwalking or climbing stairs rapidly; walking uphill; walkingor stair climbing after meals; in cold, in wind, or underemotional stress; or only during the few hours afterawakening. Angina occurs on walking .2 blocks on thelevel and climbing .1 flight of ordinary stairs at a normalpace and under normal conditions.
III “Marked limitations of ordinary physical activity.” Anginaoccurs on walking 1 to 2 blocks on the level and climbing1 flight of stairs under normal conditions and at a normalpace.
IV “Inability to carry on any physical activity withoutdiscomfort—anginal symptoms may be present at rest.”
Adapted with permission from Campeau L. Grading of angina pectoris (letter).Circulation 1976;54:522–3. © 1976, American Heart Association, Inc.
976 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
who contact a physician because of worsening or recurrence ofsymptoms should be urged to go directly to an ED equipped toperform prompt reperfusion therapy. Alternatively, they mayenter the emergency medical services system directly by calling9-1-1. Patients who have recently been evaluated and who arecalling for advice regarding modification of medication as partof an ongoing treatment plan represent exceptions.
Even in the most urgent subgroup of patients whopresent with acute-onset chest pain, there usually is ade-
quate time for transport to an environment in which theycan be evaluated and treated (12). In a large study ofconsecutive patients with chest pain suspected to be ofcardiac etiology who were transported to the ED viaambulance, one third had a final diagnosis of AMI, onethird had a final diagnosis of UA, one third had a finaldiagnosis of a noncardiac cause. Only 1.5% of these patientsdeveloped cardiopulmonary arrest before arrival at the hos-pital or in the ED (13). These findings suggest that patients
Figure 3. Top, Unadjusted survival probability (695% CI) in the PURSUIT trial of patients with ACS. Bottom, Unadjusted survival probability withoutdeath or MI in the PURSUIT trial of patients with ACS (10).
977JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina

with acute chest pain might be better served by transport toan adequately staffed and equipped ED than by sendingthem to a less well staffed and equipped facility, therebycompromising the quality of the care environment in anattempt to shorten the initial transport time.
Patients must retain the ultimate responsibility for decid-ing whether to seek medical attention and, if so, in whatenvironment. The physician cannot be expected to assumeresponsibility for a patient with a potentially serious acutecardiac disorder who does not present in person for urgentevaluation and declines after being advised to do so. Phy-sicians should be cautious not to inappropriately reassurepatients who are inclined not to seek further medicalattention.
1. ED or Outpatient Facility Presentation
Recommendation
Class I1. Patients with a suspected ACS with chest discom-
fort at rest for >20 min, hemodynamic instability,or recent syncope or presyncope should be stronglyconsidered for immediate referral to an ED or aspecialized chest pain unit. Other patients with asuspected ACS may be seen initially in an ED, achest pain unit, or an outpatient facility. (Level ofEvidence: C)
Although no data are available that compare outcome asa function of the location of the initial assessment, thisrecommendation is based on evidence that symptoms andsigns of an ACS may lead to a clinical decision that requiresa sophisticated level of intervention. When symptoms havebeen unremitting for .20 min, the possibility of STEMImust be considered. Given the strong evidence for arelationship between delay in treatment and death (14–16),an immediate assessment that includes a 12-lead ECG isessential. Patients who present with hemodynamic instabil-ity require an environment in which therapeutic interven-
tions can be provided, and for those with presyncope orsyncope, the major concern is the risk of sudden death. Suchpatients should be encouraged to seek emergency transpor-tation when it is available. Transport as a passenger in aprivate vehicle is an acceptable alternative only if the wait foran emergency vehicle would impose a delay of .20 to30 min.
Patients without any of these high-risk features may beseen initially in an outpatient facility.
2. Questions to Be Addressed at the Initial Evaluation.The initial evaluation should be used to provide informationabout the diagnosis and prognosis. The attempt should bemade to simultaneously answer 2 questions:
● What is the likelihood that the signs and symptomsrepresent ACS secondary to obstructive CAD (Table 5)?
● What is the likelihood of an adverse clinical outcome(Table 6)? Outcomes of concern include death, MI (orrecurrent MI), stroke, heart failure, recurrent symptom-atic ischemia, and serious arrhythmia.
For the most part, the answers to these questions form asequence of contingent probabilities. Thus, the likelihoodthat the signs and symptoms represent ACS is contingenton the likelihood that the patient has underlying CAD.Similarly, the prognosis is contingent on the likelihood thatthe symptoms represent acute ischemia.
B. Early Risk Stratification
Recommendations for Early Risk Stratification
Class I1. A determination should be made in all patients with
chest discomfort of the likelihood of acute ischemiacaused by CAD as high, intermediate, or low.(Level of Evidence: C)
2. Patients who present with chest discomfort shouldundergo early risk stratification that focuses onanginal symptoms, physical findings, ECG find-
Table 5. Likelihood That Signs and Symptoms Represent an ACS Secondary to CAD
FeatureHigh Likelihood
Any of the following:
Intermediate LikelihoodAbsence of high-likelihood features
and presence of any of the following:
Low LikelihoodAbsence of high- or intermediate-likelihood features but may have:
History Chest or left arm pain or discomfort aschief symptom reproducing priordocumented angina
Known history of CAD, including MI
Chest or left arm pain or discomfortas chief symptom
Age .70 yearsMale sexDiabetes mellitus
Probable ischemic symptoms in absenceof any of the intermediate likelihoodcharacteristics
Recent cocaine use
Examination Transient MR, hypotension, diaphoresis,pulmonary edema, or rales
Extracardiac vascular disease Chest discomfort reproduced by palpation
ECG New, or presumably new, transient ST-segment deviation ($0.05 mV) orT-wave inversion ($0.2 mV) withsymptoms
Fixed Q wavesAbnormal ST segments or T waves
not documented to be new
T-wave flattening or inversion in leadswith dominant R waves
Normal ECG
Cardiac markers Elevated cardiac TnI, TnT, or CK-MB Normal Normal
Braunwald E, Mark DB, Jones RH, et al. Unstable angina: diagnosis and management. Rockville, MD: Agency for Health Care Policy and Research and the National Heart,Lung, and Blood Institute, US Public Health Service, US Department of Health and Human Services; 1994; AHCPR Publication No. 94-0602.
978 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
ings, and biomarkers of cardiac injury. (Level ofEvidence: B)
3. A 12-lead ECG should be obtained immediately(within 10 min) in patients with ongoing chestdiscomfort and as rapidly as possible in patientswho have a history of chest discomfort consistentwith ACS but whose discomfort has resolved by thetime of evaluation. (Level of Evidence: C)
4. Biomarkers of cardiac injury should be measured inall patients who present with chest discomfortconsistent with ACS. A cardiac-specific troponin isthe preferred marker, and if available, it should bemeasured in all patients. CK-MB by mass assay isalso acceptable. In patients with negative cardiacmarkers within 6 h of the onset of pain, anothersample should be drawn in the 6- to 12-h timeframe (e.g., at 9 h after the onset of symptoms).(Level of Evidence: C)
Class IIa1. For patients who present within 6 h of the onset of
symptoms, an early marker of cardiac injury (e.g.,myoglobin or CK-MB subforms) should be consid-ered in addition to a cardiac troponin. (Level ofEvidence: C)
Class IIb1. C-reactive protein (CRP) and other markers of
inflammation should be measured. (Level of Evi-dence: B)
Class III1. Total CK (without MB), aspartate aminotransfer-
ase (AST, SGOT), b-hydroxybutyric dehydroge-nase, and/or lactate dehydrogenase should be themarkers for the detection of myocardial injury inpatients with chest discomfort suggestive of ACS.(Level of Evidence: C)
1. Estimation of the Level of Risk. The medical history,physical examination, ECG, and biochemical cardiacmarker measurements in patients with symptoms suggestiveof ACS at the time of the initial presentation can beintegrated into an estimation of the risk of death andnonfatal cardiac ischemic events. The latter include new orrecurrent MI, recurrent UA, disabling angina that re-quires hospitalization, and/or urgent coronary revascular-ization. Estimation of the level of risk is a multivariableproblem that cannot be accurately quantified with asimple table; therefore, Tables 5 and 6 are meant to beillustrative of the general relationships between clinicaland ECG findings and the categorization of patients intothose at a low, an intermediate, or a high risk of events.
2. Rationale for Risk Stratification. Because patients withischemic discomfort at rest as a group are at an increasedrisk of cardiac death and nonfatal ischemic events, anassessment of the prognosis often sets the pace of the initialevaluation and treatment. An estimation of risk is useful in1) selection of the site of care (coronary care unit, monitored
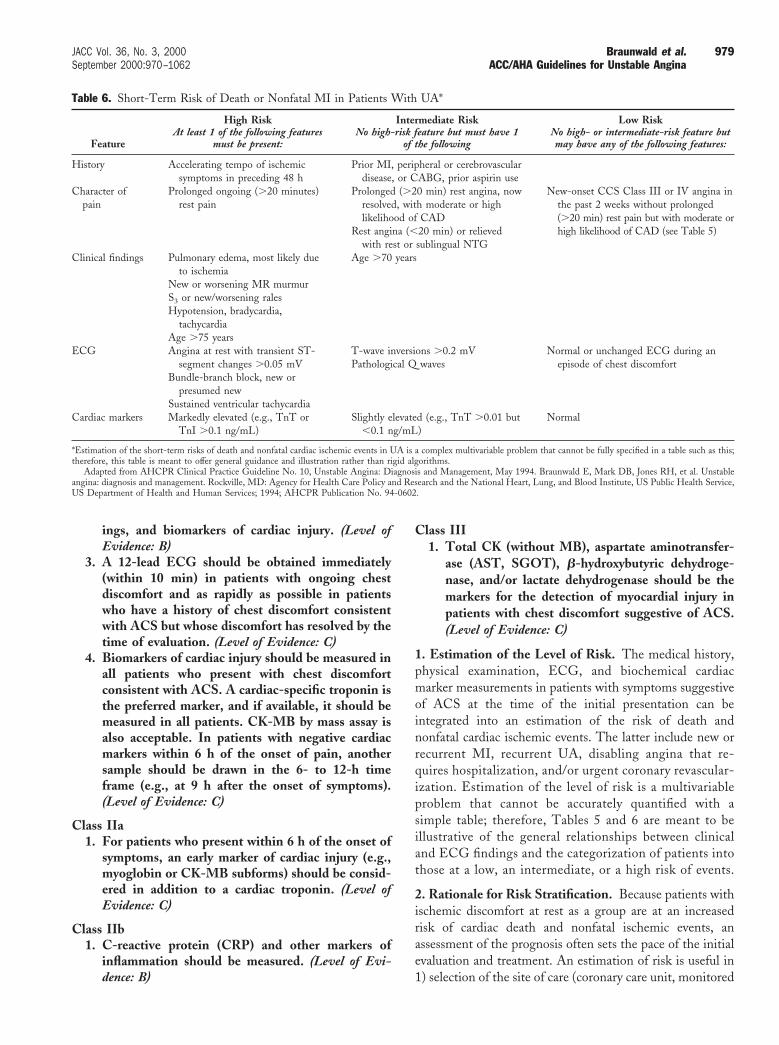
Table 6. Short-Term Risk of Death or Nonfatal MI in Patients With UA*
Feature
High RiskAt least 1 of the following features
must be present:
Intermediate RiskNo high-risk feature but must have 1
of the following
Low RiskNo high- or intermediate-risk feature butmay have any of the following features:
History Accelerating tempo of ischemicsymptoms in preceding 48 h
Prior MI, peripheral or cerebrovasculardisease, or CABG, prior aspirin use
Character ofpain
Prolonged ongoing (.20 minutes)rest pain
Prolonged (.20 min) rest angina, nowresolved, with moderate or highlikelihood of CAD
Rest angina (,20 min) or relievedwith rest or sublingual NTG
New-onset CCS Class III or IV angina inthe past 2 weeks without prolonged(.20 min) rest pain but with moderate orhigh likelihood of CAD (see Table 5)
Clinical findings Pulmonary edema, most likely dueto ischemia
New or worsening MR murmurS3 or new/worsening ralesHypotension, bradycardia,
tachycardiaAge .75 years
Age .70 years
ECG Angina at rest with transient ST-segment changes .0.05 mV
Bundle-branch block, new orpresumed new
Sustained ventricular tachycardia
T-wave inversions .0.2 mVPathological Q waves
Normal or unchanged ECG during anepisode of chest discomfort
Cardiac markers Markedly elevated (e.g., TnT orTnI .0.1 ng/mL)
Slightly elevated (e.g., TnT .0.01 but,0.1 ng/mL)
Normal
*Estimation of the short-term risks of death and nonfatal cardiac ischemic events in UA is a complex multivariable problem that cannot be fully specified in a table such as this;therefore, this table is meant to offer general guidance and illustration rather than rigid algorithms.
Adapted from AHCPR Clinical Practice Guideline No. 10, Unstable Angina: Diagnosis and Management, May 1994. Braunwald E, Mark DB, Jones RH, et al. Unstableangina: diagnosis and management. Rockville, MD: Agency for Health Care Policy and Research and the National Heart, Lung, and Blood Institute, US Public Health Service,US Department of Health and Human Services; 1994; AHCPR Publication No. 94-0602.
979JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina

step-down unit, or outpatient setting) and 2) selection oftherapy, especially platelet glycoprotein (GP) IIb/IIIa in-hibitors (see Section III. B) and coronary revascularization(see Section IV). For all modes of presentation of an ACS,a strong relationship exists between indicators of the likeli-hood of ischemia due to CAD and prognosis (Tables 5 and6). Patients with a high likelihood of ischemia due to CADare at a greater risk of an untoward cardiac event than arepatients with a lower likelihood of CAD. Therefore, anassessment of the likelihood of CAD is the starting pointfor the determination of prognosis in patients who presentwith symptoms suggestive of an ACS. Other importantelements for prognostic assessment are the tempo of thepatient’s clinical course, which relates to the short-term riskof future cardiac events, principally AMI, and the patient’slikelihood of survival should an AMI occur.
Patients may present with ischemic discomfort but with-out ST-segment elevation on the 12-lead ECG in a varietyof clinical scenarios, including no known prior history ofCAD, a prior history of stable CAD, soon after MI, andafter myocardial revascularization with CABG or PCI(7,17,18). As a clinical syndrome, ischemic discomfortwithout ST-segment elevation (UA and NSTEMI) sharesill-defined borders with severe chronic stable angina, acondition associated with lower risk, and with STEMI, apresentation with a higher risk of early death and cardiacischemic events. This fact is illustrated by data from theDuke Cardiovascular Databank that describe the rate ofcardiac death in 21,761 patients treated for CAD withoutinterventional procedures at Duke University Medical Cen-ter between 1985 and 1992 and that were published in theAHCPR-NHLBI guidelines (1), now supplemented withdata from large clinical trials in ACS (10) (Fig. 3). Thehighest risk of cardiac death was at the time of presentation,and the risk declined so that by 2 months, mortality rates forpatients with ACS were at the same level as those forpatients with chronic stable angina. Data from randomizedcontrolled trials of patients with UA/NSTEMI have alsoshown that the rate of nonfatal cardiac ischemic events suchas recurrent MI and recurrent angina is highest during theinitial hospitalization and declines thereafter (4,10,19–21).
Two large clinical trials, Platelet Glycoprotein IIb/IIIa inUnstable Angina: Receptor Suppression Using IntegrilinTherapy (PURSUIT) (10) and Efficacy and Safety ofSubcutaneous Enoxaparin in Non–Q wave CoronaryEvents (ESSENCE) (22), have evaluated the clinical andECG characteristics associated with an increased risk ofdeath and nonfatal MI in 24,774 patients with UA/NSTEMI. The critical clinical features associated with anincreased risk of death were age (.65 years), presence ofpositive markers for myocardial necrosis on admission,lighter weight, more severe (CCS Class III or IV) chronicangina before the acute admission, rales on physical exam-ination, and ST-segment depression on the admissionECG. In the PURSUIT trial, either tachycardia or brady-cardia and lower blood pressure were associated with a
higher risk of death or MI. These findings allow thestratification of patients with UA/NSTEMI into those athigher risk and those at lower risk.
3. The History. Patients with suspected UA/NSTEMImay be divided into those with and those without a historyof documented CAD. Particularly when the patient doesnot have a known history of CAD, the physician mustdetermine whether the patient’s presentation, with its con-stellation of specific symptoms and signs, is most consistentwith chronic ischemia, with acute ischemia, or with analternative disease process. The 5 most important factorsderived from the initial history that relate to the likelihoodof ischemia due to CAD, ranked in the order of importance,are 1) the nature of the anginal symptoms, 2) prior historyof CAD, 3) sex, 4) age, and 5) the number of traditional riskfactors present (23–25).
Anginal Symptoms
The characteristics of angina are described in the ACC/AHA/ACP-ASIM Guidelines for the Management ofPatients With Chronic Stable Angina (26). Angina ischaracterized as a deep, poorly localized chest or armdiscomfort that is reproducibly associated with physicalexertion or emotional stress and is relieved promptly (i.e.,,5 min) with rest and/or the use of sublingual nitroglycerin(NTG) (Table 5). Patients with UA may have discomfortthat has all of the qualities of typical angina except that theepisodes are more severe and prolonged, may occur at rest,or may be precipitated by less exertion than previously.Some patients may have no chest discomfort but presentsolely with jaw, neck, ear, arm, or epigastric discomfort. Ifthese symptoms have a clear relationship to exertion orstress or are relieved promptly with NTG, they should beconsidered equivalent to angina. Occasionally, such “anginalequivalents” that occur at rest are the mode of presentationof a patient with UA, but without the exertional history, itmay be difficult to recognize the cardiac origin. Otherdifficult presentations of the patient with UA include thosewithout any chest (or equivalent) discomfort. Isolated un-explained new-onset or worsened exertional dyspnea is themost common anginal equivalent symptom, especially inolder patients; others include nausea and vomiting, dia-phoresis, and unexplained fatigue. Elderly patients, espe-cially women with ACS, often present with atypical angina.
Features that are not characteristic of myocardial ischemiainclude the following:
● Pleuritic pain (i.e., sharp or knife-like pain brought on byrespiratory movements or cough)
● Primary or sole location of discomfort in the middle orlower abdominal region
● Pain that may be localized at the tip of 1 finger,particularly over the left ventricular (LV) apex
● Pain reproduced with movement or palpation of the chestwall or arms
● Constant pain that lasts for many hours
980 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062

● Very brief episodes of pain that last a few seconds or less● Pain that radiates into the lower extremities
Documentation of the evaluation of a patient with sus-pected UA/NSTEMI should include the physician’s opin-ion of whether the discomfort is in 1 of 3 categories: high,intermediate, or low likelihood of acute ischemia caused byCAD (Table 5).
Although typical characteristics substantially raise theprobability of CAD, features not characteristic of chestpain, such as sharp stabbing pain or reproduction of pain onpalpation, do not exclude the possibility of ACS. In theMulticenter Chest Pain Study, acute ischemia was diag-nosed in 22% of patients who presented to the ED withsharp or stabbing pain and in 13% of patients with pain withpleuritic qualities. Furthermore, 7% of patients whose painwas fully reproduced with palpation were ultimately recog-nized to have ACS (27). The Acute Cardiac IschemiaTime-Insensitive Predictive Instrument (ACI-TIPI)project (28,29) found that older age, male sex, the presenceof chest or left arm pain, and the identification of chest painor pressure as the most important presenting symptom allincreased the likelihood that the patient was experiencingacute ischemia.
Demographics and History in Diagnosis and RiskStratification
In most studies of ACS, a prior history of MI has beenassociated not only with a high risk of obstructive CAD (30)but also with an increased risk of multivessel CAD.
There are differences in the presentations of men andwomen with ACS (see Section VI. A). A smaller percentageof women than men present with STEMI, and of thepatients who present without ST-segment elevation, fewerwomen than men have MIs (31). Women with suspectedACS are less likely to have CAD than are men with asimilar clinical presentation, and when CAD is present inwomen, it tends to be less severe. If STEMI is present, theoutcome in women tends to be worse even when adjustmentis made for the older age and greater comorbidity of women.However, the outcome for women with UA is significantlybetter than the outcome for men, and the outcomes aresimilar for men and women with NSTEMI (32,33).
Older patients (see Section VI. D) have increased risks ofboth underlying CAD (34,35) and multivessel CAD; fur-thermore, they are at higher risk for an adverse outcomethan are younger patients. The slope of the increased risk issteepest beyond age 70. This increased risk is related in partto the greater extent and severity of underlying CAD andthe more severe LV dysfunction in older patients, but ageitself appears to exert an independent prognostic risk as well,perhaps because of comorbidities. Elderly patients are alsomore likely to have atypical symptoms on presentation.
In patients with symptoms of possible ACS, some of thetraditional risk factors for CAD (e.g., hypertension, hyper-cholesterolemia, cigarette smoking) are only weakly predic-
tive of the likelihood of acute ischemia (29,36) and are farless important than are symptoms, ECG findings, andcardiac markers. Therefore, the presence or absence of thesetraditional risk factors ordinarily should not be used to deter-mine whether an individual patient should be admitted ortreated for ACS. Although a family history of prematureCAD raises interesting issues of the genetic contribution tothe development of this syndrome, it has not been a usefulindicator of diagnosis or prognosis in patients evaluated forpossible symptoms of ACS. However, several of these riskfactors have important prognostic and therapeutic implica-tions. Diabetes and the presence of extracardiac (peripheralor carotid) arterial disease are major risk factors for pooroutcome in patients with ACS (see Section VI. B). For bothST-segment elevation (37) and non–ST-segment elevationACS (10), patients with these conditions have a signifi-cantly higher mortality rate and risk of acute heart failure.For the most part, this increase in risk is due to a greaterextent of underlying CAD and LV dysfunction, but in manystudies, diabetes carries prognostic significance over andabove these findings. Similarly, a history of hypertension isassociated with an increased risk of poor outcome.
Surprisingly, current smoking is associated with a lowerrisk of death in the setting of ACS (38–40), predominantlybecause of the less severe underlying CAD. This “smokers’paradox” seems to represent a tendency for smokers todevelop thrombi on less severe plaques and at an earlier agethan nonsmokers.
Cocaine use has been implicated as a cause of ACS,presumably due to the ability of this drug to cause coronaryvasospasm and thrombosis in addition to its direct effects onheart rate and arterial pressure and its myocardial toxicproperties (see Section VI. E). It is important to inquireabout the use of cocaine in patients with suspected ACS,especially younger patients (,40 years).
4. Noncardiac Causes of Exacerbation of SymptomsSecondary to Myocardial Ischemia
Recommendation
Class I1. The initial evaluation of the patient with suspected
ACS should include a search for noncoronarycauses that could explain the development of symp-toms. (Level of Evidence: C)
Information from the initial history, physical examina-tion, and ECG (Table 5) will enable the physician torecognize and exclude from further assessment patientsclassified as “not having ischemic discomfort.” This includespatients with noncardiac pain (e.g., musculoskeletal discom-fort, esophageal discomfort) or cardiac pain not caused bymyocardial ischemia (e.g., acute pericarditis). The remain-ing patients should undergo a more complete evaluation ofsecondary causes of UA that might alter management. Thisevaluation should include a physical examination for evi-
981JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina

dence of other cardiac disease, an ECG to screen forarrhythmias, measurement of body temperature and bloodpressure, and determination of hemoglobin or hematocrit.Cardiac disorders other than CAD that may cause myocar-dial ischemia include aortic stenosis and hypertrophic car-diomyopathy. In secondary angina, factors that increasemyocardial oxygen demand or decrease oxygen delivery tothe heart may provoke or exacerbate ischemia in thepresence of significant underlying CAD. Previously unrec-ognized gastrointestinal bleeding is a common secondarycause of worsened CAD and the development of ACSsymptoms due to anemia. Acute worsening of chronicobstructive pulmonary disease (COPD) (with or withoutsuperimposed infection) may lower oxygen saturation levelssufficiently to intensify ischemic symptoms in patients withCAD. Evidence of increased cardiac oxygen demand can bejudged from the presence of fever, signs of hyperthyroidism,sustained tachyarrhythmias, or markedly elevated bloodpressure. Another cause of increased myocardial oxygendemand is arteriovenous (AV) fistula in patients receivingdialysis.
The majority of patients seen in the ED with symptomsof possible ACS will be judged after their workup to not havea cardiac problem. A recent clinical trial of a predictiveinstrument evaluated 10,689 patients with suspected ACS(11). To participate, patients were required to be .30 yearsold with a chief symptom of chest, left arm, jaw, orepigastric pain or discomfort; shortness of breath; dizziness;palpitations; or other symptoms suggestive of acute isch-emia. After the evaluation, 7,996 patients (75%) weredeemed not to have acute ischemia.
5. Assessment of Risk of Death in Patients With UA/NSTEMI. In patients who meet the diagnostic criteria forUA/NSTEMI, the recent tempo of ischemic symptoms isthe strongest predictor of risk of death. The AHCPRguidelines Unstable Angina: Diagnosis and Managementidentified low-risk patients as those without rest or noctur-nal angina and with a normal or an unchanged ECG (1).High-risk patients were identified as those with pulmonaryedema; ongoing rest pain for .20 min in duration; anginawith S3 gallop, rales, or new or worsening mitral regurgita-tion (MR) murmur; hypotension; or dynamic ST-segmentchange of $1 mm. Patients without low- or high-riskfeatures were termed to be at “intermediate risk.”
These simple clinical criteria were prospectively tested ina consecutive sample of patients who presented with symp-toms suggestive of ACS (41). After prescreening wasconducted to exclude patients with AMI or cardiac arrest,patients receiving thrombolytic therapy, and patients diag-nosed as having noncardiac conditions, only 6% of theremaining patients diagnosed with UA were categorized asbeing at low risk. This low-risk population experienced nodeath or MI in the 30 days after the initial presentation tothe ED. In contrast, the 30-day mortality rate was 1.2% forpatients at intermediate risk and 1.7% for patients deemed
at high risk. These observations confirmed the managementrecommendations made in the earlier guidelines. Patientswith low-risk UA can be managed expeditiously as outpa-tients. Patients with high-risk UA deserve rapid clinicalstabilization in an acute care environment in the hospital.Patients at intermediate risk require individualization ofmanagement based on clinical judgment. These patientsshould usually be admitted to the hospital and requiremonitoring but do not ordinarily require an intensive careunit.
The tempo of angina is characterized by an assessment ofchanges in the duration of episodes, their frequency, and theanginal threshold. In particular, it is useful to determinewhether the amount of physical or emotional stress thatprovokes symptoms has declined, whether symptoms areoccurring at rest, and whether they awaken the patient fromsleep. The integration of these factors into a score canimprove the predictions of outcome (42,43). Althoughnew-onset angina itself is associated with greater risk than iscontinued stable angina, most of its contribution to anadverse prognosis is determined by its severity, frequency,and tempo (42,44).
Multiple studies have demonstrated that prior MI is amajor risk factor for poor outcome in both STEMI andUA/NSTEMI (10). Patients with symptoms of acuteand/or chronic heart failure are also at a substantially higherrisk.
Physical Examination
The major objectives of the physical examination are toidentify potential precipitating causes of myocardial isch-emia such as uncontrolled hypertension or thyrotoxicosisand comorbid conditions such as pulmonary disease and toassess the hemodynamic impact of the ischemic event.Every patient with suspected ACS should have his or hervital signs measured (blood pressure in both arms, heartrate, temperature) and undergo a thorough cardiovascularand chest examination. Patients with evidence of LVdysfunction on examination (rales, S3 gallop) or with acuteMR have a higher likelihood of severe underlying CAD andare at a high risk of a poor outcome. Just as the history ofextracardiac vascular disease is important, the physicalexamination of the peripheral vessels can also provideimportant prognostic information. The presence of bruits orpulse deficits that suggest extracardiac vascular disease(carotid, aortic, peripheral) identifies patients with a higherlikelihood of significant CAD.
Elements of the physical examination can be critical inmaking an important alternative diagnosis in patients withchest pain. In particular, several disorders carry a significantthreat to life and function if not diagnosed acutely. Aorticdissection is suggested by pain in the back, unequal pulses,or a murmur of aortic regurgitation. Acute pericarditis issuggested by a pericardial friction rub, and cardiac tampon-ade may be evidenced by pulsus paradoxus. Pneumothorax is
982 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062

suspected when acute dyspnea, pleuritic chest pain, anddifferential breath sounds are present.
Recently, the importance of cardiogenic shock in patientswith NSTEMI was emphasized. Although most literatureon cardiogenic shock has focused on STEMI, the SHouldwe emergently revascularize Occluded Coronaries for car-diogenic shocK (SHOCK) (45), Global Use of Strategies toOpen Occluded Coronary Arteries (GUSTO)-II (45a), andPURSUIT (10) trials have found that cardiogenic shockoccurs in up to 5% of patients with NSTEMI and thatmortality rates are .60%. Thus, hypotension and evidenceof organ hypoperfusion constitute a medical emergency inNSTEMI.
6. Tools for Risk Stratification
Electrocardiogram
The ECG is critical not only to add support to the clinicalsuspicion of CAD but also to provide prognostic informa-tion that is based on the pattern and magnitude of theabnormalities (46–49). A recording made during an episode ofthe presenting symptoms is particularly valuable. Importantly,transient ST-segment changes ($0.05 mV) that developduring a symptomatic episode at rest and that resolve whenthe patient becomes asymptomatic strongly suggest acuteischemia and a very high likelihood of underlying severeCAD. Patients whose current ECG suggests acute CADcan be assessed with greater diagnostic accuracy if a priorECG is available for comparison (Table 5) (50,51).
Although it is imperfect, the 12-lead ECG lies at thecenter of the decision pathway for the evaluation andmanagement of patients with acute ischemic discomfort(Fig. 1, Table 5). The diagnosis of AMI is confirmed withserial cardiac markers in .90% of patients who present withST-segment elevation of $0.1 mV in $2 contiguous leads,and such patients should be considered potential candidatesfor acute reperfusion therapy. Patients who present withST-segment depression are initially considered to haveeither UA or NSTEMI; the distinction between the 2diagnoses is based ultimately on the detection in the bloodof markers of myocardial necrosis (6,18,52).
Patients with UA and reversible ST-segment depressionhave an increase in thrombin activity reflected in elevatedlevels of circulating fibrinopeptides and complex lesions thatsuggest thrombosis on coronary angiography (53). Up to25% of patients with NSTEMI and elevated CK-MB go onto develop Q-wave MI, whereas the remaining 75% havenon–Q-wave MI. Acute reperfusion therapy is contraindi-cated for ACS patients without ST-segment elevation,except for those with isolated acute posterior infarctionmanifested as ST-segment depressions in leads V1 to V3and/or isolated ST-segment elevation in posterior chestleads (54). Inverted T waves may also indicate ischemia ornon–Q-wave infarction. In patients suspected on clinicalgrounds to have ACS, marked ($0.2 mV) symmetricalprecordial T-wave inversion strongly suggests acute isch-
emia, particularly that due to a critical stenosis of the leftanterior descending coronary artery (LAD) (55). Patientswith this ECG finding often exhibit hypokinesis of theanterior wall and are at high risk with medical treatment(56). Revascularization will often reverse both the T-waveinversion and wall motion disorder (57). Nonspecific ST-segment and T-wave changes, usually defined as ST-segment deviation of ,0.05 mV or T-wave inversion of#0.2 mV, are less helpful than the foregoing findings.Established Q waves $0.04 s are also less helpful in thediagnosis of UA, although by suggesting prior MI, they doindicate a high likelihood of significant CAD. Isolated Qwaves in lead III may be a normal finding, especially in theabsence of repolarization abnormalities in any of the inferiorleads. A completely normal ECG in a patient with chestpain does not exclude the possibility of ACS, because 1% to6% of such patients eventually are proved to have had anAMI (by definition, an NSTEMI), and $4% will be foundto have UA (47,58,59).
The common alternative causes of ST-segment andT-wave changes must be considered. In patients withST-segment elevation, the diagnoses of LV aneurysm,pericarditis, Prinzmetal’s angina, early repolarization, andWolff-Parkinson-White syndrome should be considered.Central nervous system events and drug therapy withtricyclic antidepressants or phenothiazines can cause deepT-wave inversion.
Several investigators have shown that a gradient of risk ofdeath and cardiac ischemic events can be established basedon the nature of the ECG abnormality (48,60,61). Patientswith ACS and confounding ECG patterns such as bundle-branch block, paced rhythm, or LV hypertrophy are at thehighest risk for death, followed by patients with ST-segment deviation (ST-segment elevation or depression); atthe lowest risk are patients with isolated T-wave inversionor normal ECG patterns. Importantly, the prognostic in-formation contained within the ECG pattern remains anindependent predictor of death even after adjustment forclinical findings and cardiac marker measurements (60–63).
In addition to the presence or absence of ST-segmentdeviation or T-wave inversion patterns as noted earlier,there is evidence that the magnitude of the ECG abnormal-ity provides important prognostic information. Thus,Lloyd-Jones et al. (64) reported that the diagnosis of acutenon–Q-wave MI was 3 to 4 times more likely in patientswith ischemic discomfort who had $3 ECG leads thatshowed ST-segment depression and/or ST-segment de-pression of $0.2 mV. Investigators from the ThrombolysisIn Myocardial Ischemia (TIMI) III registry (60) reportedthat the 1-year incidence of death or new MI in patientswith $0.05-mV ST-segment deviation was 16.3% com-pared with 6.8% for patients with isolated T-wave changesand 8.2% for patients with no ECG changes.
Because a single 12-lead ECG recording provides only asnapshot view of a dynamic process, the usefulness ofobtaining serial ECG tracings or performing continuous
983JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina

ST-segment monitoring was studied (46). Although serialECGs increase the ability to diagnose AMI (65–67), theyield is higher with serial cardiac marker measurements(68). Continuous 12-lead ECG monitoring to detect ST-segment shifts, both symptomatic and asymptomatic, can beperformed with microprocessor-controlled, programmabledevices. Clinical experience suggests that continuous ECGmonitoring identifies episodes of ischemia that are missedwith standard 12-lead ECGs obtained on presentation andthat such episodes of transient ischemia provide indepen-dent prognostic information that indicates an increased riskof death, nonfatal MI, and the need for urgent revascular-ization (69,70). However, the ultimate clinical usefulness ofcontinuous 12-lead ECG monitoring requires additionalclarification.
7. Decision Aids That Combine Clinical Features andECG Findings. ECG findings have been incorporatedinto mathematics-based decision aids for the triage ofpatients who present with chest pain (46). The goals ofthese decision aids include the identification of patients atlow risk of cardiac events, those with cardiac ischemia orAMI and the estimation of prognosis (28,58,71–76).
8. Biochemical Cardiac Markers. Biochemical cardiacmarkers are useful for both the diagnosis of myocardialnecrosis and the estimation of prognosis. The loss ofmembrane integrity of myocytes that undergo necrosisallows intracellular macromolecules to diffuse into the car-diac interstitium and then into the lymphatics and cardiacmicrovasculature (77). Eventually, these macromolecules,which are collectively referred to as biochemical cardiacmarkers, are detectable in the peripheral circulation. Foroptimum diagnostic usefulness, a marker of myocardialdamage in the bloodstream should be present in a highconcentration in the myocardium and absent from nonmyo-cardial tissue (52,77,78). It should be rapidly released intothe blood after myocardial injury with a direct proportionalrelationship between the extent of myocardial injury and themeasured level of the marker. Finally, the marker shouldpersist in blood for a sufficient length of time to provide aconvenient diagnostic time window with an easy, inexpen-sive, and rapid assay technique. Although no biochemicalcardiac marker available at the present satisfies all of theserequirements, as discussed later, the cardiac-specific tro-ponins have a number of attractive features and are gainingacceptance as the biochemical markers of choice in theevaluation of patients with ACS (6).
For patients who present without ST-segment elevation,in whom the diagnosis may be unclear, biochemical cardiacmarkers are useful to confirm the diagnosis of MI. Inaddition, they provide valuable prognostic information,because there is a quantitative relationship between themagnitude of elevation of marker levels and the risk of anadverse outcome (79).
Creatine Kinase
CK-MB has until recently been the principal serumcardiac marker used in the evaluation of ACS. Despite itscommon use, CK-MB has several limitations. Low levels ofCK-MB in the blood of healthy persons limit its specificityfor myocardial necrosis. CK-MB may also be elevated withsevere damage of skeletal muscle (52,80,81). CK-MB iso-forms exist in only 1 form in myocardial tissue (CK-MB2)but in different isoforms (or subforms) in plasma (CK-MB1). The use of an absolute level of CK-MB2 of .1 U/Land a ratio of CK-MB2 to CK-MB1 of .1.5 has improvedsensitivity for the diagnosis of MI within the first 6 hcompared with conventional assays for CK-MB, but thistest has the same lack of absolute cardiac specificity as thatof CK-MB itself (82). Moreover, the assay is not widelyavailable.
Cardiac Troponins
The troponin complex consists of 3 subunits: TnT, TnI,and troponin C (TnC) (81). Monoclonal antibody–basedimmunoassays have been developed to detect cardiac-specific TnT (cTnT) and cardiac-specific TnI (cTnI), be-cause the amino acid sequences of the skeletal and cardiacisoforms of both TnT and TnI have sufficient dissimilarity.Because cardiac and smooth muscle share isoforms for TnC,no immunoassays of TnC have been developed for clinicalpurposes. Therefore, in these guidelines, the term “cardiactroponins” refers to either cTnT or cTnI or to both.
Because cTnT and cTnI are not detected in the blood ofhealthy persons, the cutoff value for elevated cTnI and cTnIlevels may be set to slightly above the upper limit of theassay for a normal healthy population, leading some inves-tigators to use the term “minor myocardial damage” or“microinfarction” for patients with detectable troponin butno CK-MB in the blood (83). Case reports exist thatconfirm histological evidence of focal myocyte necrosis (e.g.,microinfarction) in patients with elevated cardiac troponinlevels and normal CK-MB values (6,84,85), indicating thatmyocardial necrosis can be recognized with increased sen-sitivity. It is estimated that '30% of patients who presentwith rest pain without ST-segment elevation and wouldotherwise be diagnosed as having UA because of a lack ofCK-MB elevation actually have NSTEMI when assessedwith cardiac-specific troponin assays.
Elevated levels of cTnT or cTnI convey prognosticinformation beyond that supplied by the clinical character-istics of the patient, the ECG at presentation, and apredischarge exercise test (61,62,86–88). Furthermore,among patients without ST-segment elevation and normalCK-MB levels, elevated cTnI or cTnT concentrationsidentify those at an increased risk of death (61,62). Finally,there is a quantitative relationship between the quantity ofcTnI or cTnT that is measured and the risk of death inpatients who present with an ACS (61,62,89) (Fig. 4). Theincremental risk of death or MI in troponin-positive vs.
984 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
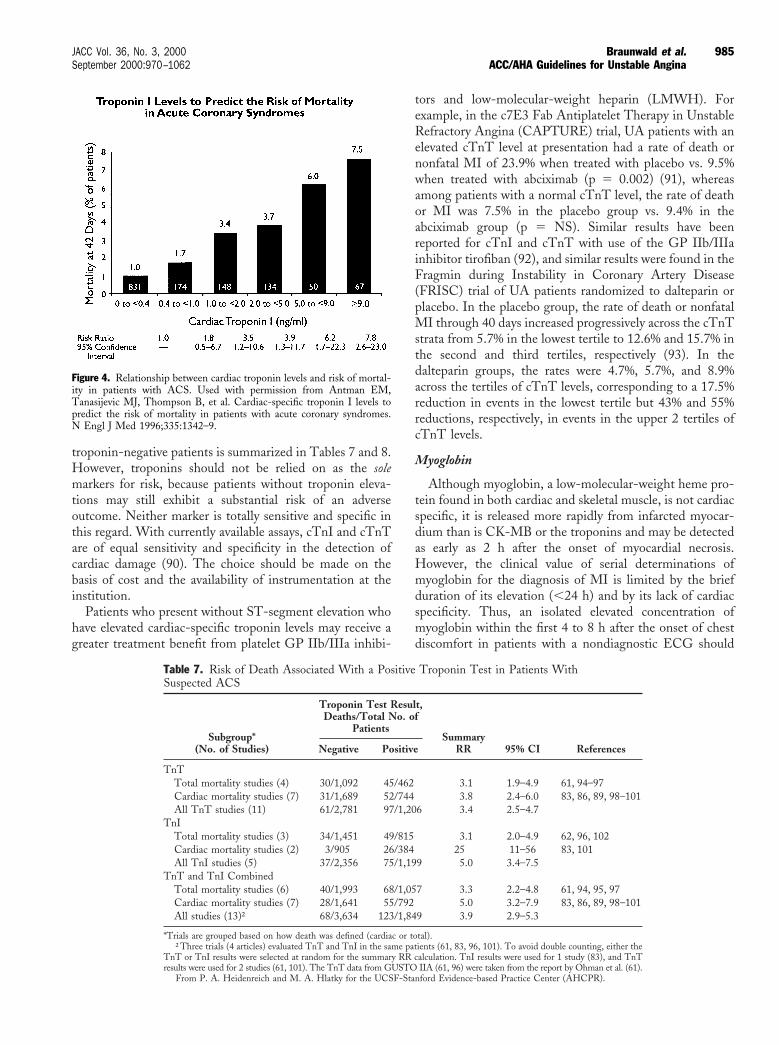
troponin-negative patients is summarized in Tables 7 and 8.However, troponins should not be relied on as the solemarkers for risk, because patients without troponin eleva-tions may still exhibit a substantial risk of an adverseoutcome. Neither marker is totally sensitive and specific inthis regard. With currently available assays, cTnI and cTnTare of equal sensitivity and specificity in the detection ofcardiac damage (90). The choice should be made on thebasis of cost and the availability of instrumentation at theinstitution.
Patients who present without ST-segment elevation whohave elevated cardiac-specific troponin levels may receive agreater treatment benefit from platelet GP IIb/IIIa inhibi-
tors and low-molecular-weight heparin (LMWH). Forexample, in the c7E3 Fab Antiplatelet Therapy in UnstableRefractory Angina (CAPTURE) trial, UA patients with anelevated cTnT level at presentation had a rate of death ornonfatal MI of 23.9% when treated with placebo vs. 9.5%when treated with abciximab (p 5 0.002) (91), whereasamong patients with a normal cTnT level, the rate of deathor MI was 7.5% in the placebo group vs. 9.4% in theabciximab group (p 5 NS). Similar results have beenreported for cTnI and cTnT with use of the GP IIb/IIIainhibitor tirofiban (92), and similar results were found in theFragmin during Instability in Coronary Artery Disease(FRISC) trial of UA patients randomized to dalteparin orplacebo. In the placebo group, the rate of death or nonfatalMI through 40 days increased progressively across the cTnTstrata from 5.7% in the lowest tertile to 12.6% and 15.7% inthe second and third tertiles, respectively (93). In thedalteparin groups, the rates were 4.7%, 5.7%, and 8.9%across the tertiles of cTnT levels, corresponding to a 17.5%reduction in events in the lowest tertile but 43% and 55%reductions, respectively, in events in the upper 2 tertiles ofcTnT levels.
Myoglobin
Although myoglobin, a low-molecular-weight heme pro-tein found in both cardiac and skeletal muscle, is not cardiacspecific, it is released more rapidly from infarcted myocar-dium than is CK-MB or the troponins and may be detectedas early as 2 h after the onset of myocardial necrosis.However, the clinical value of serial determinations ofmyoglobin for the diagnosis of MI is limited by the briefduration of its elevation (,24 h) and by its lack of cardiacspecificity. Thus, an isolated elevated concentration ofmyoglobin within the first 4 to 8 h after the onset of chestdiscomfort in patients with a nondiagnostic ECG should
Table 7. Risk of Death Associated With a Positive Troponin Test in Patients WithSuspected ACS
Subgroup*(No. of Studies)
Troponin Test Result,Deaths/Total No. of
PatientsSummary
RR 95% CI ReferencesNegative Positive
TnTTotal mortality studies (4) 30/1,092 45/462 3.1 1.9–4.9 61, 94–97Cardiac mortality studies (7) 31/1,689 52/744 3.8 2.4–6.0 83, 86, 89, 98–101All TnT studies (11) 61/2,781 97/1,206 3.4 2.5–4.7
TnITotal mortality studies (3) 34/1,451 49/815 3.1 2.0–4.9 62, 96, 102Cardiac mortality studies (2) 3/905 26/384 25 11–56 83, 101All TnI studies (5) 37/2,356 75/1,199 5.0 3.4–7.5
TnT and TnI CombinedTotal mortality studies (6) 40/1,993 68/1,057 3.3 2.2–4.8 61, 94, 95, 97Cardiac mortality studies (7) 28/1,641 55/792 5.0 3.2–7.9 83, 86, 89, 98–101All studies (13)† 68/3,634 123/1,849 3.9 2.9–5.3
*Trials are grouped based on how death was defined (cardiac or total).†Three trials (4 articles) evaluated TnT and TnI in the same patients (61, 83, 96, 101). To avoid double counting, either the
TnT or TnI results were selected at random for the summary RR calculation. TnI results were used for 1 study (83), and TnTresults were used for 2 studies (61, 101). The TnT data from GUSTO IIA (61, 96) were taken from the report by Ohman et al. (61).
From P. A. Heidenreich and M. A. Hlatky for the UCSF-Stanford Evidence-based Practice Center (AHCPR).
Figure 4. Relationship between cardiac troponin levels and risk of mortal-ity in patients with ACS. Used with permission from Antman EM,Tanasijevic MJ, Thompson B, et al. Cardiac-specific troponin I levels topredict the risk of mortality in patients with acute coronary syndromes.N Engl J Med 1996;335:1342–9.
985JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina

not be relied on to make the diagnosis of AMI but shouldbe supplemented by a more cardiac-specific marker, such asCK-MB, cTnI, or cTnT (106,107). However, because of itshigh sensitivity, a negative test for myoglobin when blood issampled within the first 4 to 8 h after onset is useful inruling out myocardial necrosis.
Comparison of Cardiac Markers
The Diagnostic Marker Cooperative Study was a large,prospective, multicenter, double-blind study of patients whopresented to the ED with chest pain in whom the diagnosticsensitivity and specificity for MI for total CK-MB (activityand mass), CK-MB subforms, myoglobin, and cTnI andcTnT were compared (108). CK-MB subforms and myo-globin were most efficient for the early diagnosis (within6 h) of MI, whereas cTnI and cTnT were highly cardiacspecific and were particularly efficient for the late diagnosisof MI.
Table 9 compares the advantages and disadvantages ofvarious cardiac markers for the evaluation and managementof patients with suspected ACS but without ST-segmentelevation on the 12-lead ECG. The troponins offer greaterdiagnostic sensitivity due to their ability to identify patientswith lesser amounts of myocardial damage, which has beenreferred to as “minor myocardial damage.” Nonetheless,these lesser amounts of damage confer a high risk in patientswith ACS, because they are thought to represent microin-farctions that result from microemboli from an unstableplaque; the instability of the plaque rather than the actualamount of myocardial necrosis may be what places thepatient at an increased risk. In addition, analyses fromclinical trials suggest that the measurement of cardiactroponin concentrations provides prognostic informationabove and beyond that contained in simple demographicdata such as the patient’s age, findings on the 12-lead ECG,and measurement of CK-MB (61,62). Thus, measurementof cardiac troponin concentrations provides an efficientmethod for simultaneously diagnosing MI and providingprognostic information. Although not quite as sensitive orspecific as the troponins, CK-MB by mass assay remains avery useful marker for the detection of more than minormyocardial damage. A normal CK-MB, however, does notexclude the minor myocardial damage and its attendant riskof adverse outcomes detectable by cardiac-specific tro-ponins. As noted earlier, the measurement of CK-MB
isoforms is useful for the extremely early diagnosis (,4 h) ofMI. However, to date, experience with the measurement ofCK-MB isoforms has been limited predominantly to ded-icated research centers, and its “field performance” inwidespread clinical use remains to be established. Because ofits poor cardiac specificity in the setting of skeletal muscleinjury and its rapid clearance from the bloodstream, myo-globin should not be used as the only diagnostic marker forthe identification of patients with NSTEMI, but its earlyappearance makes it quite useful for ruling out myocardialnecrosis.
Cardiac-specific troponins are gaining acceptance as theprimary biochemical cardiac marker in ACS. Commerciallyavailable assays are undergoing refinement, with severalversions of assays in clinical use with different diagnosticcutoffs, underscoring the need for careful review of thecardiac troponin results reported in local hospital laborato-ries (6,109). As with any new testing procedure, there maybe a period of adjustment as the laboratory introduces thetroponin assays and the clinician becomes familiar with theiruse. Clinicians are encouraged to work closely with theircolleagues in laboratory medicine to minimize the transitionphase in making troponin measurements available in theirinstitutions. The continued measurement of CK-MB massis advisable during this transition. It should be emphasizedthat troponin levels may not rise for 6 h after the onset ofsymptoms, and in the case of a negative troponin level at,6 h, the measurement should be repeated 8 to 12 h afterthe onset of pain.
9. Integration of Clinical History With Serum MarkerMeasurements. Given the overlapping time frame of therelease pattern of biochemical cardiac markers, it is impor-tant that clinicians incorporate the time from the onset ofthe patient’s symptoms into their assessment of the resultsof biochemical marker measurements (6,110,111,111a)(Fig. 5). The earliest marker of myocardial necrosis, myo-globin, is a sensitive test but lacks cardiac specificity. Laterappearing markers, such as TnT and TnI, are more specificbut have a lower sensitivity for the very early detection ofmyocardial necrosis (e.g., ,6 h) after the onset of symp-toms, and if an early (,6 h) troponin test is negative, ameasurement should be repeated 8 to 12 h after the onset ofsymptoms. Although the release kinetics of the troponinsprovide a wider diagnostic window for the diagnosis of MI
Table 8. Risk of Death or MI Associated With a Positive Troponin Test in Patients With UA
Subgroup(No. of Studies)
Troponin Test Result,Deaths/Total No. of
PatientsSummary
RR 95% CI ReferencesNegative Positive
TnT (5) 43/667 62/301 3.7 2.5–5.6 95TnI (2) 7/163 10/35 5.7 1.8–18.6 89, 103–105TnT and TnI combined* (6) 47/737 67/322 3.8 2.6–5.5 87, 103
*One trial evaluated TnT and TnI in the same patients (103). To avoid double counting, 1 marker (TnT) was selected at randomfor summary RR calculations.
From P. A. Heidenreich and M. A. Hlatky for the UCSF-Stanford Evidence-based Practice Center (AHCPR).
986 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
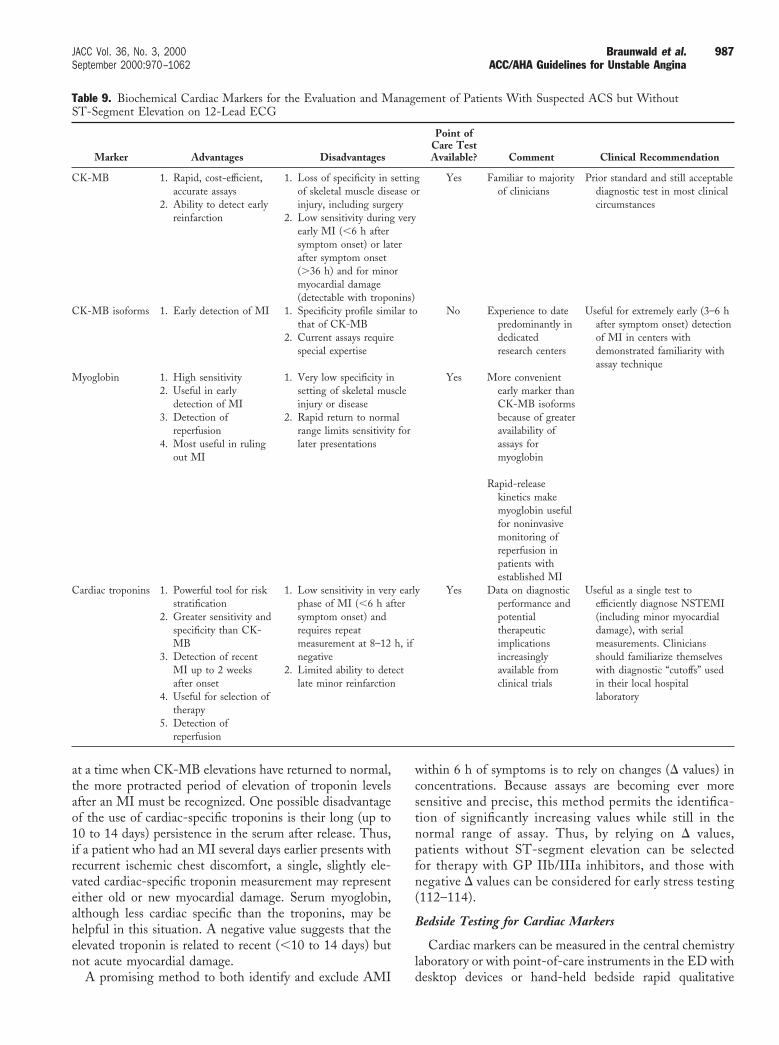
at a time when CK-MB elevations have returned to normal,the more protracted period of elevation of troponin levelsafter an MI must be recognized. One possible disadvantageof the use of cardiac-specific troponins is their long (up to10 to 14 days) persistence in the serum after release. Thus,if a patient who had an MI several days earlier presents withrecurrent ischemic chest discomfort, a single, slightly ele-vated cardiac-specific troponin measurement may representeither old or new myocardial damage. Serum myoglobin,although less cardiac specific than the troponins, may behelpful in this situation. A negative value suggests that theelevated troponin is related to recent (,10 to 14 days) butnot acute myocardial damage.
A promising method to both identify and exclude AMI
within 6 h of symptoms is to rely on changes (D values) inconcentrations. Because assays are becoming ever moresensitive and precise, this method permits the identifica-tion of significantly increasing values while still in thenormal range of assay. Thus, by relying on D values,patients without ST-segment elevation can be selectedfor therapy with GP IIb/IIIa inhibitors, and those withnegative D values can be considered for early stress testing(112–114).
Bedside Testing for Cardiac Markers
Cardiac markers can be measured in the central chemistrylaboratory or with point-of-care instruments in the ED withdesktop devices or hand-held bedside rapid qualitative
Table 9. Biochemical Cardiac Markers for the Evaluation and Management of Patients With Suspected ACS but WithoutST-Segment Elevation on 12-Lead ECG
Marker Advantages Disadvantages
Point ofCare TestAvailable? Comment Clinical Recommendation
CK-MB 1. Rapid, cost-efficient,accurate assays
2. Ability to detect earlyreinfarction
1. Loss of specificity in settingof skeletal muscle disease orinjury, including surgery
2. Low sensitivity during veryearly MI (,6 h aftersymptom onset) or laterafter symptom onset(.36 h) and for minormyocardial damage(detectable with troponins)
Yes Familiar to majorityof clinicians
Prior standard and still acceptablediagnostic test in most clinicalcircumstances
CK-MB isoforms 1. Early detection of MI 1. Specificity profile similar tothat of CK-MB
2. Current assays requirespecial expertise
No Experience to datepredominantly indedicatedresearch centers
Useful for extremely early (3–6 hafter symptom onset) detectionof MI in centers withdemonstrated familiarity withassay technique
Myoglobin 1. High sensitivity2. Useful in early
detection of MI3. Detection of
reperfusion4. Most useful in ruling
out MI
1. Very low specificity insetting of skeletal muscleinjury or disease
2. Rapid return to normalrange limits sensitivity forlater presentations
Yes More convenientearly marker thanCK-MB isoformsbecause of greateravailability ofassays formyoglobin
Rapid-releasekinetics makemyoglobin usefulfor noninvasivemonitoring ofreperfusion inpatients withestablished MI
Cardiac troponins 1. Powerful tool for riskstratification
2. Greater sensitivity andspecificity than CK-MB
3. Detection of recentMI up to 2 weeksafter onset
4. Useful for selection oftherapy
5. Detection ofreperfusion
1. Low sensitivity in very earlyphase of MI (,6 h aftersymptom onset) andrequires repeatmeasurement at 8–12 h, ifnegative
2. Limited ability to detectlate minor reinfarction
Yes Data on diagnosticperformance andpotentialtherapeuticimplicationsincreasinglyavailable fromclinical trials
Useful as a single test toefficiently diagnose NSTEMI(including minor myocardialdamage), with serialmeasurements. Cliniciansshould familiarize themselveswith diagnostic “cutoffs” usedin their local hospitallaboratory
987JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
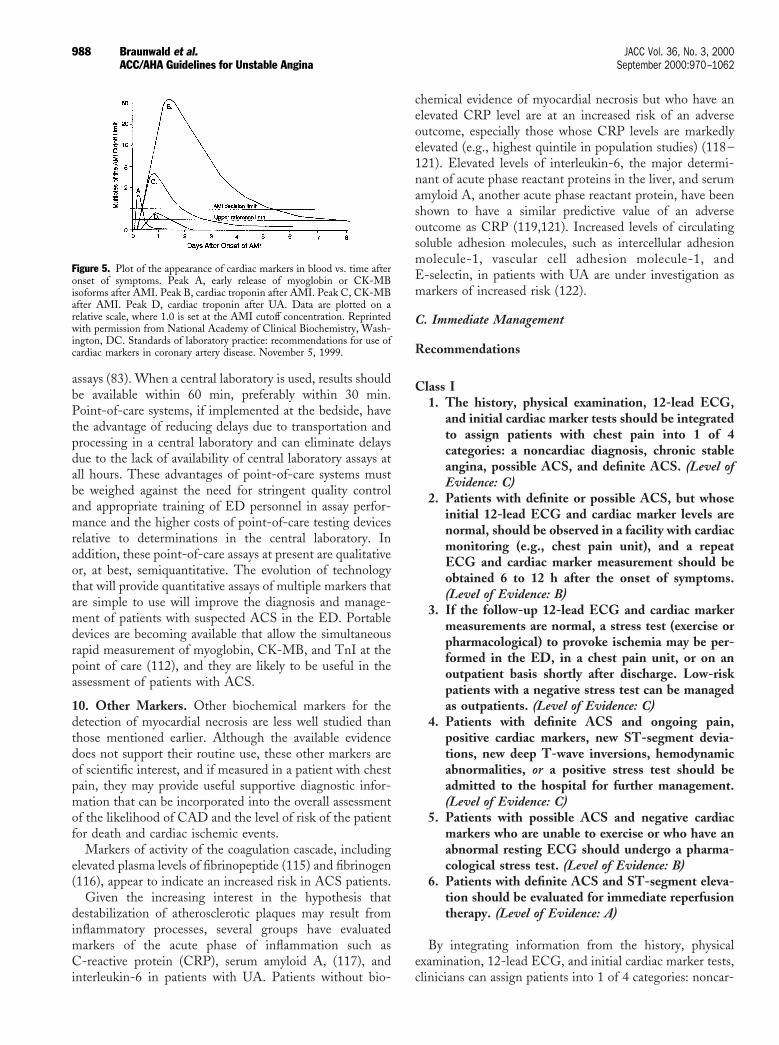
assays (83). When a central laboratory is used, results shouldbe available within 60 min, preferably within 30 min.Point-of-care systems, if implemented at the bedside, havethe advantage of reducing delays due to transportation andprocessing in a central laboratory and can eliminate delaysdue to the lack of availability of central laboratory assays atall hours. These advantages of point-of-care systems mustbe weighed against the need for stringent quality controland appropriate training of ED personnel in assay perfor-mance and the higher costs of point-of-care testing devicesrelative to determinations in the central laboratory. Inaddition, these point-of-care assays at present are qualitativeor, at best, semiquantitative. The evolution of technologythat will provide quantitative assays of multiple markers thatare simple to use will improve the diagnosis and manage-ment of patients with suspected ACS in the ED. Portabledevices are becoming available that allow the simultaneousrapid measurement of myoglobin, CK-MB, and TnI at thepoint of care (112), and they are likely to be useful in theassessment of patients with ACS.
10. Other Markers. Other biochemical markers for thedetection of myocardial necrosis are less well studied thanthose mentioned earlier. Although the available evidencedoes not support their routine use, these other markers areof scientific interest, and if measured in a patient with chestpain, they may provide useful supportive diagnostic infor-mation that can be incorporated into the overall assessmentof the likelihood of CAD and the level of risk of the patientfor death and cardiac ischemic events.
Markers of activity of the coagulation cascade, includingelevated plasma levels of fibrinopeptide (115) and fibrinogen(116), appear to indicate an increased risk in ACS patients.
Given the increasing interest in the hypothesis thatdestabilization of atherosclerotic plaques may result frominflammatory processes, several groups have evaluatedmarkers of the acute phase of inflammation such asC-reactive protein (CRP), serum amyloid A, (117), andinterleukin-6 in patients with UA. Patients without bio-
chemical evidence of myocardial necrosis but who have anelevated CRP level are at an increased risk of an adverseoutcome, especially those whose CRP levels are markedlyelevated (e.g., highest quintile in population studies) (118–121). Elevated levels of interleukin-6, the major determi-nant of acute phase reactant proteins in the liver, and serumamyloid A, another acute phase reactant protein, have beenshown to have a similar predictive value of an adverseoutcome as CRP (119,121). Increased levels of circulatingsoluble adhesion molecules, such as intercellular adhesionmolecule-1, vascular cell adhesion molecule-1, andE-selectin, in patients with UA are under investigation asmarkers of increased risk (122).
C. Immediate Management
Recommendations
Class I1. The history, physical examination, 12-lead ECG,
and initial cardiac marker tests should be integratedto assign patients with chest pain into 1 of 4categories: a noncardiac diagnosis, chronic stableangina, possible ACS, and definite ACS. (Level ofEvidence: C)
2. Patients with definite or possible ACS, but whoseinitial 12-lead ECG and cardiac marker levels arenormal, should be observed in a facility with cardiacmonitoring (e.g., chest pain unit), and a repeatECG and cardiac marker measurement should beobtained 6 to 12 h after the onset of symptoms.(Level of Evidence: B)
3. If the follow-up 12-lead ECG and cardiac markermeasurements are normal, a stress test (exercise orpharmacological) to provoke ischemia may be per-formed in the ED, in a chest pain unit, or on anoutpatient basis shortly after discharge. Low-riskpatients with a negative stress test can be managedas outpatients. (Level of Evidence: C)
4. Patients with definite ACS and ongoing pain,positive cardiac markers, new ST-segment devia-tions, new deep T-wave inversions, hemodynamicabnormalities, or a positive stress test should beadmitted to the hospital for further management.(Level of Evidence: C)
5. Patients with possible ACS and negative cardiacmarkers who are unable to exercise or who have anabnormal resting ECG should undergo a pharma-cological stress test. (Level of Evidence: B)
6. Patients with definite ACS and ST-segment eleva-tion should be evaluated for immediate reperfusiontherapy. (Level of Evidence: A)
By integrating information from the history, physicalexamination, 12-lead ECG, and initial cardiac marker tests,clinicians can assign patients into 1 of 4 categories: noncar-
Figure 5. Plot of the appearance of cardiac markers in blood vs. time afteronset of symptoms. Peak A, early release of myoglobin or CK-MBisoforms after AMI. Peak B, cardiac troponin after AMI. Peak C, CK-MBafter AMI. Peak D, cardiac troponin after UA. Data are plotted on arelative scale, where 1.0 is set at the AMI cutoff concentration. Reprintedwith permission from National Academy of Clinical Biochemistry, Wash-ington, DC. Standards of laboratory practice: recommendations for use ofcardiac markers in coronary artery disease. November 5, 1999.
988 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062

diac diagnosis, chronic stable angina, possible ACS, anddefinite ACS (Fig. 6).
Patients who arrive at a medical facility in a pain-freestate, have unchanged or normal ECGs, are hemodynami-cally stable, and do not have elevated cardiac markersrepresent more of a diagnostic than an urgent therapeuticchallenge. Evaluation begins in these patients by obtaininginformation from the history, physical examination, andECG (see Tables 5 and 6) to be used to confirm or reject thediagnosis of UA/NSTEMI.
Patients with a low likelihood of CAD should be evalu-ated for other causes of the presentation, including muscu-loskeletal pain; gastrointestinal disorders such as esophagealspasm, gastritis, peptic ulcer disease, or cholecystitis; in-trathoracic disease, such as pneumonia, pleurisy, pneumo-thorax; or pericarditis; and neuropsychiatric disease, such ashyperventilation or panic disorder (Fig. 6, B1). Patients whoare found to have evidence of one of these alternativediagnoses should be excluded from management with theseguidelines and referred for appropriate follow-up care (Fig.6, C1). Reassurance should be balanced with instructions toreturn for further evaluation if symptoms worsen or if thepatient fails to respond to symptomatic treatment.
Chronic stable angina may also be diagnosed in thissetting (Fig. 6, B2), and patients with this diagnosis shouldbe managed according to the ACC/AHA/ACP-ASIMGuidelines for the Management of Patients With ChronicStable Angina (26).
Patients with possible ACS (Fig. 6, B3 and D1) arecandidates for additional observation in a specialized facility(e.g., chest pain unit) (Fig. 6, E1). Patients with definiteACS (Fig. 6, B4) are triaged based on the pattern of the12-lead ECG. Patients with ST-segment elevation (Fig. 6,C3) are evaluated for immediate reperfusion therapy (Fig. 6,D3) and managed according to the ACC/AHA Guidelinesfor the Management of Patients With Acute MyocardialInfarction (5), whereas those without ST-segment elevation(Fig. 6, C2) are either managed by additional observation(Fig. 6, E1) or admitted to the hospital (Fig. 6, H3). Patientswith low-risk ACS (Table 5) without transient ST-segmentdepressions of $0.05 mV and/or T-wave inversions of $0.2mV, without positive cardiac markers, and without a positivestress test (Fig. 6, H1) may be discharged and treated asoutpatients (Fig. 6, I1).
1. Chest Pain Units. To facilitate a more definitive eval-uation while avoiding the unnecessary hospital admission ofpatients with possible ACS (Fig. 6, B3) and low-risk ACS(Fig. 6, F1) and the inappropriate discharge of patients withactive myocardial ischemia without ST-segment elevation(Fig. 6, C2), special units have been devised that arevariously referred to as “chest pain units” and “short-stayED coronary care units.” Personnel in these units use criticalpathways or protocols designed to arrive at a decision aboutthe presence or absence of myocardial ischemia and, ifpresent, to characterize it further as UA or NSTEMI and to
define the optimal next step in the care of the patient (e.g.,admission, acute intervention) (123). The goal is to arrive atsuch a decision after a finite amount of time, which usuallyis between 6 and 12 h but may extend up to 24 h dependingon the policies in individual hospitals. Although chest painunits are useful, other appropriate observation areas inwhich patients with chest pain can be evaluated may be usedas well.
The physical location of the chest pain unit or site wherepatients with chest pain are observed is variable, rangingfrom a specifically designated area of the ED to a separateunit with the appropriate equipment (124). Similarly, thechest pain unit may be administratively a part of the ED andstaffed by emergency physicians or may be administered andstaffed separately. Suggestions for the design of chest painunits have been presented by several authoritative bodiesand generally include provisions for continuous monitoringof the patient’s ECG, ready availability of cardiac resusci-tation equipment and medications, and appropriate staffingwith nurses and physicians. Given the evolving nature of thefield and the recent introduction of chest pain units intoclinical medicine, ACEP has published guidelines thatrecommend a program for the continuous monitoring ofoutcomes of patients evaluated in such units as well as theimpact on hospital resources (125). A Consensus Panelstatement from ACEP emphasized that chest pain unitsshould be considered 1 part of a multifaceted program thatalso includes efforts to minimize patient delays in seekingmedical care and delays in the ED itself (125).
Several groups have studied the impact of chest pain unitson the care of patients with chest pain who present to theED. It has been reported, both from studies with historicalcontrols and from randomized trials, that the use of chestpain units is cost saving compared with an in-hospitalevaluation to “rule-out MI” (126,127).
A common clinical practice is to minimize the chance of“missing” an MI in a patient with chest discomfort byadmitting to the hospital all patients with suspected ACSand by obtaining serial 12-lead ECGs and biochemicalcardiac marker measurements to either exclude or confirmthe diagnosis of MI. Such a practice typically results in a lowpercentage of admitted patients actually being confirmed tohave an MI. Given the inverse relationship between thepercentage of patients with a “rule-out MI evaluation” andthe “MI miss rate,” the potential cost savings of a chest painunit varies depending on the practice pattern for thedisposition of chest pain patients at individual hospitals(126). Hospitals with a high admission rate of low-riskpatients to “rule-out MI” (70% to 80%) will experience thelargest cost savings by implementing a chest pain unitapproach but will have the smallest impact on the number ofmissed MI patients. In contrast, hospitals with relatively lowadmission rates of such patients (30% to 40%) will experi-ence greater improvements in the quality of care becausefewer MI patients will be missed but will have a smallerimpact on costs because of the low baseline admission rate.
989JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
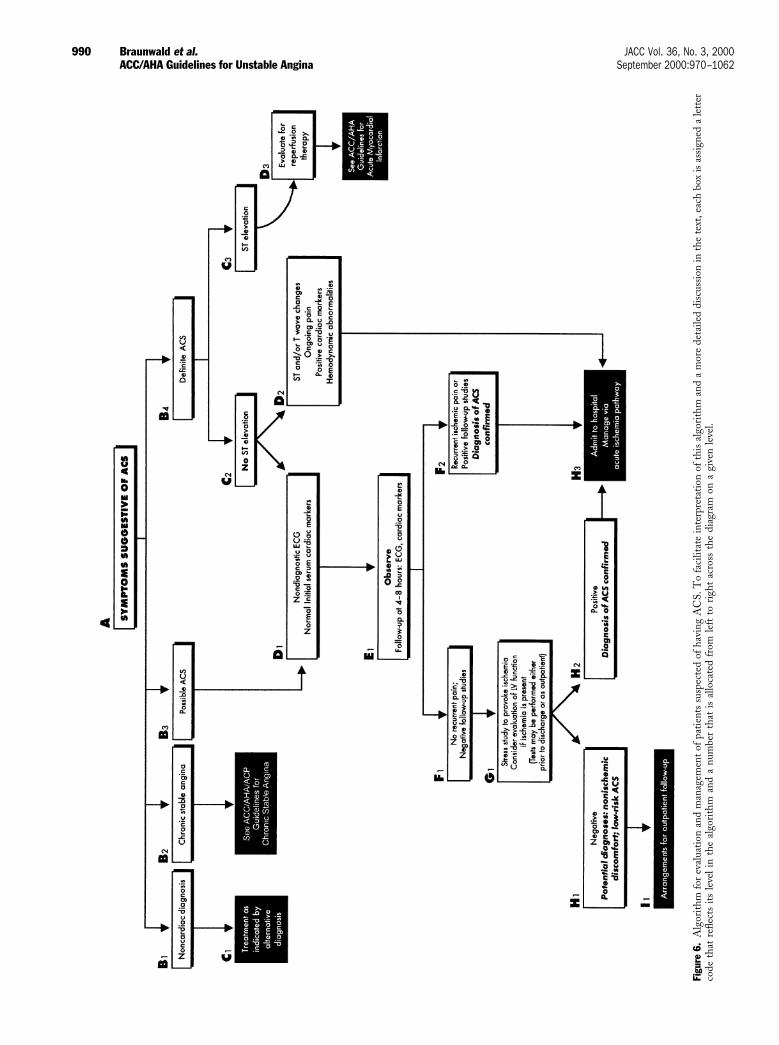
Figu
re6.
Alg
orith
mfo
rev
alua
tion
and
man
agem
ento
fpat
ient
ssu
spec
ted
ofha
ving
AC
S.T
ofa
cilit
ate
inte
rpre
tatio
nof
this
algo
rith
man
da
mor
ede
taile
ddi
scus
sion
inth
ete
xt,e
ach
box
isas
sign
eda
lett
erco
deth
atre
flect
sits
leve
lin
the
algo
rith
man
da
num
ber
that
isal
loca
ted
from
left
tori
ght
acro
ssth
edi
agra
mon
agi
ven
leve
l.
990 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062

Potential Expansion of the Use of Chest Pain Units forIntermediate-Risk Patients
Farkouh et al. (128) extended the use of a chest pain unitin a separate portion of the ED to include patients at anintermediate risk of adverse clinical outcome based on thepreviously published AHCPR guidelines for the manage-ment of UA (1) (Table 6). They reported a 46% reductionin the ultimate need for hospital admission in intermediate-risk patients after a median stay of 9.2 h in the chest painunit. Extension of the use of chest pain units tointermediate-risk patients in an effort to reduce inpatientcosts is facilitated by making available diagnostic testingmodalities such as treadmill testing and stress imaging(echocardiographic or nuclear) 7 days a week (129).
Triage of Patients
Patients with chest discomfort for whom a specificdiagnosis cannot be made after a review of the history,physical examination, initial 12-lead ECG, and biochemicalcardiac marker data should undergo a more definitiveevaluation. Several categories of patients should be consid-ered according to the algorithm shown in Fig. 6:
1. Patients with possible ACS (Fig. 6, B3) are those who hada recent episode of chest discomfort at rest not entirelytypical of ischemia but are pain free when initiallyevaluated, have a normal or unchanged ECG, and haveno elevations of cardiac markers.
2. Patients with a recent episode of typical ischemic dis-comfort that either is of new onset or severe or exhibitsan accelerating pattern of previous stable angina (espe-cially if it has occurred at rest or is within 2 weeks of apreviously documented MI) should initially be consid-ered to have a “definite ACS” (Fig. 6, B4). However,such patients may be at a low risk if their ECG obtainedat presentation has no diagnostic abnormalities and theinitial serum cardiac markers (especially cardiac-specifictroponins) are normal (Fig. 6, C2 and D1). As indicatedin the algorithm, patients with either “possible ACS”(Fig. 6, B3) or “definite ACS” (Fig. 6, B4) but withnondiagnostic ECG and normal initial cardiac markers(Fig. 6, D1) are candidates for additional observation inthe ED or in a specialized area such as a chest pain unit(E1). In contrast, patients who present without ST-segment elevation but have features indicative of activeischemia (ongoing pain, ST-segment and/or T-wavechanges, positive cardiac markers, or hemodynamic in-stability) (Fig. 6, D2) should be admitted to the hospital(H3).
2. Discharge From ED or Chest Pain Unit. The initialassessment of whether a patient has UA/NSTEMI andwhich triage option is most suitable generally should bemade immediately on the patient’s arrival at a medicalfacility. Rapid assessment of a patient’s candidacy foradditional observation can be accomplished based on the
status of the symptoms, ECG findings, and serum cardiacmarker measurements.
Patients who experience recurrent ischemic discomfort,evolve abnormalities on a follow-up 12-lead ECG or cardiacmarker measurements, or develop hemodynamic abnormal-ities such as new or worsening congestive heart failure (Fig.6, D2) should be admitted to the hospital (Fig. 6, H3) andmanaged as described in Section III.
Patients who are pain free, have either a normal ornondiagnostic ECG or one that is unchanged from previoustracings, and have a normal set of initial cardiac markermeasurements are candidates for further evaluation to screenfor nonischemic discomfort (Fig. 6, B1) vs. a low-risk ACS(Fig. 6, D1). If the patient is low risk (Table 6) and does notexperience any further ischemic discomfort and a follow-up12-lead ECG and cardiac marker measurements after 6 to8 h of observation are normal (Fig. 6, F1), the patient maybe considered for an early stress test to provoke ischemia(Fig. 6, G1). This test can be performed before the dischargeand should be supervised by an experienced physician.Alternatively, the patient may be discharged and return fora stress test as an outpatient within 72 h. The exact natureof the stress test may vary depending on the patient’s abilityto exercise on either a treadmill or bicycle and the localexpertise in a given hospital setting (e.g., availability ofdifferent testing modalities at different times of the day ordifferent days of the week) (130). Patients who are capableof exercise and are free of confounding features on thebaseline ECG, such as bundle-branch block, LV hypertro-phy, or paced rhythms, can be evaluated with routinesymptom-limited conventional exercise stress testing. Pa-tients who are incapable of exercise or who have anuninterpretable baseline ECG should be considered forpharmacological stress testing with either nuclear perfusionimaging or two-dimensional echocardiography (46,131).Because LV function is so integrally related to prognosisand heavily affects therapeutic options, strong considerationshould be given to the assessment of LV function withechocardiography or radionuclide ventriculography in pa-tients with documented ischemia. In sites at which stresstests are not available, low-risk patients may be dischargedand the test scheduled to be carried out within 72 h.
Patients who develop recurrent pain during observationor in whom the follow-up studies (12-lead ECG, cardiacmarkers) show new abnormalities (Fig. 6, F2) should beadmitted to the hospital (Fig. 6, H3).
Because continuity of care is important in the overallmanagement of patients with a chest pain syndrome, thepatient’s primary physician (if not involved in the care of thepatient during the initial episode) should be notified of theresults of the evaluation and should receive a copy of therelevant test results. Patients with a noncardiac diagnosisand those with low risk or possible ACS with a negativestress test should be counseled to make an appointment withtheir primary care physician as outpatients for furtherinvestigation into the cause of their symptoms (Fig. 6, I1).
991JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
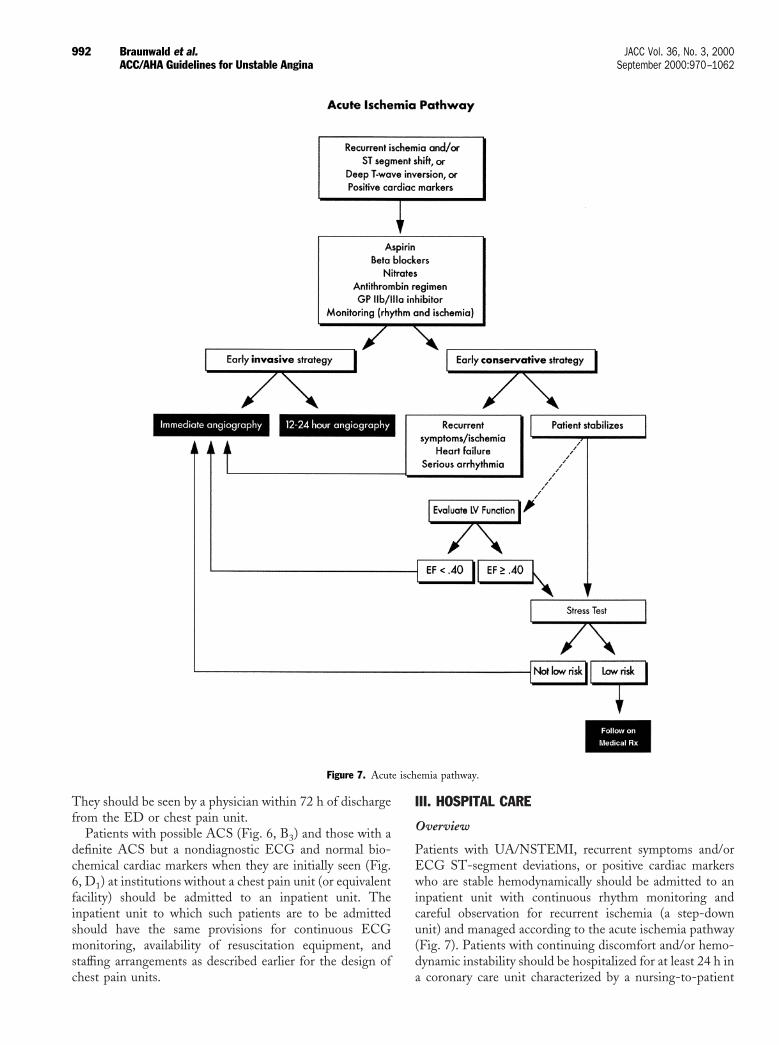
They should be seen by a physician within 72 h of dischargefrom the ED or chest pain unit.
Patients with possible ACS (Fig. 6, B3) and those with adefinite ACS but a nondiagnostic ECG and normal bio-chemical cardiac markers when they are initially seen (Fig.6, D1) at institutions without a chest pain unit (or equivalentfacility) should be admitted to an inpatient unit. Theinpatient unit to which such patients are to be admittedshould have the same provisions for continuous ECGmonitoring, availability of resuscitation equipment, andstaffing arrangements as described earlier for the design ofchest pain units.
III. HOSPITAL CARE
Overview
Patients with UA/NSTEMI, recurrent symptoms and/orECG ST-segment deviations, or positive cardiac markerswho are stable hemodynamically should be admitted to aninpatient unit with continuous rhythm monitoring andcareful observation for recurrent ischemia (a step-downunit) and managed according to the acute ischemia pathway(Fig. 7). Patients with continuing discomfort and/or hemo-dynamic instability should be hospitalized for at least 24 h ina coronary care unit characterized by a nursing-to-patient
Figure 7. Acute ischemia pathway.
992 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
ratio sufficient to provide 1) continuous rhythm monitoring,2) frequent assessment of vital signs and mental status, 3)documented ability to perform defibrillation quickly afterthe onset of ventricular fibrillation, and 4) adequate staff toperform these functions. Patients should be maintained atthat level of care until they have been observed for at least24 h without any of the following major complications:sustained ventricular tachycardia or fibrillation, sinus tachy-cardia, atrial fibrillation or flutter, high-degree AV block,sustained hypotension, recurrent ischemia documented bysymptoms or ST-segment change, new mechanical defect(ventricular septal defect or MR), or congestive heart failure.
Once a patient with documented high-risk ACS isadmitted, standard medical therapy is indicated as discussedlater. Unless a contraindication exists, these patients shouldbe treated with aspirin (ASA), a b-blocker, antithrombintherapy, and a GP IIb/IIIa inhibitor. Furthermore, criticaldecisions are required regarding the angiographic strategy.One option is a routine angiographic approach in whichcoronary angiography and revascularization are performedunless a contraindication exists. Within this approach, themost common strategy has called for a period of medicalstabilization. Some physicians are now taking a moreaggressive approach, with coronary angiography and revas-cularization performed within 24 h of admission; therationale for the more aggressive approach is the protectiveeffect of carefully administered antithrombin and antiplate-let therapy on procedural outcome. The alternative ap-proach, commonly referred to as the “initially conservativestrategy” (see Section III. D), is guided by ischemia, withangiography reserved for patients with recurrent ischemia ora “high-risk” stress test despite medical therapy. Regardlessof the angiographic strategy, an assessment of LV functionshould be strongly considered in patients with documentedischemia because of the imperative to treat patients whohave impaired LV function with angiotensin-convertingenzyme (ACE) inhibitors (ACEIs) and b-blockers and,when the coronary anatomy is appropriate (e.g., 3-vesselcoronary disease), with CABG (see Section IV). When thecoronary angiogram is obtained, a left ventriculogram can beobtained at the same time. When coronary angiography isnot scheduled, echocardiography or nuclear ventriculogra-phy can be used to evaluate LV function.
A. Anti-Ischemic Therapy
Recommendations for Anti-Ischemic Therapy
Class I1. Bed rest with continuous ECG monitoring for
ischemia and arrhythmia detection in patients withongoing rest pain. (Level of Evidence: C)
2. NTG, sublingual tablet or spray, followed by intra-venous administration, for the immediate relief ofischemia and associated symptoms. (Level of Evi-dence: C)
3. Supplemental oxygen for patients with cyanosis orrespiratory distress; finger pulse oximetry or arterialblood gas determination to confirm adequate arte-rial oxygen saturation (SaO2 >90%) and continuedneed for supplemental oxygen in the presence ofhypoxemia. (Level of Evidence: C)
4. Morphine sulfate intravenously when symptoms arenot immediately relieved with NTG or when acutepulmonary congestion and/or severe agitation ispresent. (Level of Evidence: C)
5. A b-blocker, with the first dose administered intra-venously if there is ongoing chest pain, followed byoral administration, in the absence of contraindica-tions. (Level of Evidence: B)
6. In patients with continuing or frequently recurringischemia when b-blockers are contraindicated, anondihydropyridine calcium antagonist (e.g., vera-pamil or diltiazem) as initial therapy in the absenceof severe LV dysfunction or other contraindica-tions. (Level of Evidence: B)
7. An ACEI when hypertension persists despite treat-ment with NTG and a b-blocker in patients with LVsystolic dysfunction or congestive heart failure and inACS patients with diabetes. (Level of Evidence: B)
Class IIa1. Oral long-acting calcium antagonists for recurrent
ischemia in the absence of contraindications andwhen b-blockers and nitrates are fully used. (Levelof Evidence: C)
2. An ACEI for all post-ACS patients. (Level ofEvidence: B)
3. Intra-aortic balloon pump (IABP) counterpulsa-tion for severe ischemia that is continuing or recursfrequently despite intensive medical therapy or forhemodynamic instability in patients before or aftercoronary angiography. (Level of Evidence: C)
Class IIb1. Extended-release form of nondihydropyridine cal-
cium antagonists instead of a b-blocker. (Level ofEvidence: B)
2. Immediate-release dihydropyridine calcium antag-onists in the presence of a b-blocker. (Level ofEvidence: B)
Class III1. NTG or other nitrate within 24 h of sildenafil
(Viagra) use. (Level of Evidence: C)2. Immediate-release dihydropyridine calcium antag-
onists in the absence of a b-blocker. (Level ofEvidence: A)
The optimal management of UA/NSTEMI has the twingoals of the immediate relief of ischemia and the preventionof serious adverse outcomes (i.e., death or MI/[re]infarc-tion). This is best accomplished with an approach thatincludes anti-ischemic therapy (Table 10), antiplatelet and
993JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina

antithrombotic therapy (see also Table 14), ongoing riskstratification, and the use of invasive procedures. Patientswho are at intermediate or high risk for adverse outcome,including those with ongoing ischemia refractory to initialmedical therapy and those with evidence of hemodynamicinstability, should if possible be admitted to a critical careenvironment with ready access to invasive cardiovasculardiagnosis and therapy procedures. Ready access is defined asensured, timely access to a cardiac catheterization laboratorywith personnel who have credentials in invasive coronaryprocedures, as well as to emergency or urgent cardiacsurgery, vascular surgery, and cardiac anesthesia (132).
The approach to the achievement of the twin goalsdescribed here includes the initiation of pharmacologicalmanagement and planning of a definitive treatment strategyfor the underlying disease process. Most patients are stableat presentation or stabilize after a brief period of intensivepharmacological management and, after appropriate coun-seling, will be able to participate in the choice of anapproach for definitive therapy. A few patients will requireprompt triage to emergency or urgent cardiac catheteriza-tion and/or the placement of an IABP. Some will prefer thecontinuation of a medical regimen without angiography.These patients require careful monitoring of the response toinitial therapy with noninvasive testing and surveillance forpersistent or recurrent ischemia, hemodynamic instability,or other features that may dictate a more invasive approach.Other patients prefer a more invasive strategy that involvesearly coronary angiography with a view toward revascular-ization.
1. General Care. The severity of symptoms dictates someof the general care that should be given during the initialtreatment. Patients should be placed at bed rest whileischemia is ongoing but can be mobilized to a chair andbedside commode when symptom free. Subsequent activityshould not be inappropriately restrictive; instead, it shouldbe focused on the prevention of recurrent symptoms andliberalized as judged appropriate when response to treat-ment occurs. Patients with cyanosis, respiratory distress, orother high-risk features should receive supplemental oxy-gen. Adequate arterial oxygen saturation should be con-firmed with direct measurement or pulse oximetry. Noevidence is available to support the administration of oxygento all patients with ACS in the absence of signs ofrespiratory distress or arterial hypoxemia. Oxygen use dur-ing initial evaluation should be limited to patients withquestionable respiratory status or those with documentedhypoxemia, because it consumes resources and evidence forits routine use is lacking. Inhaled oxygen should be admin-istered if the arterial oxygen saturation (SaO2) declines to,90%. Finger pulse oximetry is useful for the continuousmonitoring of SaO2 but is not mandatory in patients who donot appear to be at risk of hypoxia. Patients should undergocontinuous ECG monitoring during their ED evaluationand early hospital phase, because sudden, unexpected ven-tricular fibrillation is the major preventable cause of death inthis early period. Furthermore, monitoring for the recur-rence of ST-segment shifts provides useful diagnostic andprognostic information, although the system of monitoringfor ST-segment shifts must include specific methods in-tended to provide stable and accurate recordings.
2. Use of Anti-Ischemic Drugs
Nitrates
NTG reduces myocardial oxygen demand while enhanc-ing myocardial oxygen delivery. NTG, an endothelium-independent vasodilator, has both peripheral and coronaryvascular effects. By dilating the capacitance vessels (i.e., thevenous bed), it increases venous pooling to decrease myo-cardial preload, thereby reducing ventricular wall tension, adeterminant of myocardial oxygen consumption (MVO2).More modest effects on the arterial circulation decreasesystolic wall stress (afterload), contributing to further reduc-tions in MVO2. This decrease in myocardial oxygen demandis in part offset by reflex increases in heart rate andcontractility, which counteract the reductions in MVO2unless a b-blocker is concurrently administered. NTGdilates normal and atherosclerotic epicardial coronary arter-ies as well as smaller arteries that constrict with certainstressors (e.g., cold, mental or physical exercise). Withsevere atherosclerotic coronary obstruction and with lessseverely obstructed vessels with endothelial dysfunction,physiological responses to changes in myocardial blood floware often impaired (i.e., loss of flow-mediated dilation), somaximal dilation does not occur unless a direct-acting
Table 10. Class I Recommendations for Anti-Ischemic Therapyin the Presence or Absence of Continuing Ischemia orHigh-Risk Features*
Continuing Ischemia/Other Clinical High-Risk Features*
Present Absent
Bed rest with continuous ECGmonitoring
Supplemental O2 to maintainSaO2 .90%
NTG IV
b-Blockers, oral or IV b-Blockers, oral
Morphine IV for pain, anxiety,pulmonary congestion
IABP if ischemia orhemodynamic instabilitypersists
ACEI for control of hypertensionor LV dysfunction, after MI
ACEI for control of hypertensionor LV dysfunction, after MI
*Recurrent angina and/or ischemia-related ECG changes ($0.05-mV ST-segmentdepression or bundle-branch block) at rest or low-level activities; or ischemiaassociated with CHF symptoms, S3 gallop, or new or worsening mitral regurgitation;or hemodynamic instability or depressed LV function (EF ,0.40 on noninvasivestudy); or malignant ventricular arrhythmia.
994 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062

vasodilator like NTG is administered. Thus, NTG pro-motes the dilation of large coronary arteries as well ascollateral flow and redistribution of coronary blood flow toischemic regions. Inhibition of platelet aggregation alsooccurs with NTG (133), but the clinical significance of thisaction is not well defined.
Patients whose symptoms are not relieved with three0.4-mg sublingual NTG tablets or spray taken 5 min apart(Table 11) and the initiation of an intravenous b-blocker(when there are no contraindications), as well as all nonhy-potensive high-risk patients (Table 6), may benefit fromintravenous NTG, and such therapy is recommended in theabsence of contraindications (i.e., the use of sildenafil[Viagra] within the previous 24 h or hypotension). Silde-nafil inhibits the phosphodiesterase (PDE5) that degradescyclic guanosine monophosphate (cGMP), and cGMPmediates vascular smooth muscle relaxation by nitric oxide.Thus, NTG-mediated vasodilatation is markedly exagger-ated and prolonged in the presence of sildenafil. Nitrate usewithin 24 h after sildenafil or the administration of sildenafilin a patient who has received a nitrate within 24 h has beenassociated with profound hypotension, MI, and even death(134).
Intravenous NTG may be initiated at a rate of 10 mg/minthrough continuous infusion with nonabsorbing tubing andincreased by 10 mg/min every 3 to 5 min until somesymptom or blood pressure response is noted. If no responseis seen at 20 mg/min, increments of 10 and, later, 20 mg/mincan be used. If symptoms and signs of ischemia are relieved,there is no need to continue to increase the dose to effect ablood pressure response. If symptoms and signs of ischemiaare not relieved, the dose should be increased until a bloodpressure response is observed. Once a partial blood pressureresponse is observed, the dosage increase should be reducedand the interval between increments should be lengthened.Side effects include headache and hypotension. Cautionshould be used when systolic blood pressure falls to,110 mm Hg in previously normotensive patients or to.25% below the starting mean arterial blood pressure ifhypertension was present. Although recommendations for a
maximal dose are not available, a ceiling of 200 mg/min iscommonly used. Prolonged (2 to 4 weeks) infusion at 300 to400 mg/h does not increase methemoglobin levels (135).
Topical or oral nitrates are acceptable alternatives forpatients without ongoing refractory symptoms. Tolerance tothe hemodynamic effects of nitrates is dose and durationdependent and typically becomes important after 24 h ofcontinuous therapy with any formulation. Patients whorequire continued intravenous NTG beyond 24 h mayrequire periodic increases in infusion rate to maintainefficacy. An effort must be made to use non–tolerance-producing nitrate regimens (lower dose and intermittentdosing). When patients have been free of pain and othermanifestations of ischemia for 12 to 24 h, an attempt shouldbe made to reduce the dose of intravenous NTG and toswitch to oral or topical nitrates. It is not appropriate tocontinue intravenous NTG in patients who remain free ofsigns and symptoms of ischemia. When ischemia recursduring continuous intravenous NTG therapy, responsive-ness to nitrates can often be restored by increasing the doseand then, after symptoms have been controlled for severalhours, attempting to add a nitrate-free interval. This strat-egy should be pursued as long as symptoms are notadequately controlled. In stabilized patients, intravenousNTG should generally be converted within 24 h to anonparenteral alternative (Table 11) administered in anon–tolerance-producing regimen to avoid the potentialreactivation of symptoms.
Most studies of nitrate treatment in UA have been smalland uncontrolled, and there are no randomized, placebo-controlled trials that address either symptom relief orreduction in cardiac events. One small, randomized trialcompared intravenous NTG with buccal NTG and foundno significant difference in the control of ischemia (136). Anoverview of small studies of NTG in AMI from theprethrombolytic era suggested a 35% reduction in mortalityrates (137), although both the Fourth International Study ofInfarct Survival (ISIS-4) (138) and Gruppo Italiano per loStudio della Sopravvivenza nell’infarto Miocardico(GISSI-3) (139) trials formally tested this hypothesis in
Table 11. NTG and Nitrates in Angina
Compound Route Dose/Dosage Duration of Effect
NTG Sublingual tabletsSprayTransdermal
Intravenous
0.3–0.6 mg up to 1.5 mg0.4 mg as needed0.2–0.8 mg/h every 12 h
5–200 mg/min
1–7 minutesSimilar to sublingual tablets8–12 h during intermittent
therapyTolerance in 7–8 h
Isosorbide dinitrate OralOral, slow release
5–80 mg, 2 or 3 times daily40 mg 1 or 2 times daily
Up to 8 hUp to 8 h
Isosorbide mononitrate OralOral, slow release
20 mg twice daily60–240 mg once daily
12–24 h
Pentaerythritol tetranitrate Sublingual 10 mg as needed Not knownErythritol tetranitrate Sublingual
Oral5–10 mg as needed10–30 mg 3 times daily
Not knownNot known
Adapted from Table 28 in Gibbons RJ, Chatterjee K, Daley J, et al. ACC/AHA/ACP-ASIM guidelines for the managementof patients with chronic stable angina. J Am Coll Cardiol 1999;33:2092–197.
995JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina

patients with suspected AMI and failed to confirm thismagnitude of benefit. However, these large trials are con-founded by frequent prehospital and hospital use of NTG inthe “control” groups. The abrupt cessation of intravenousNTG has been associated with exacerbation of ischemicchanges on the ECG (140), and a graded reduction in thedose of intravenous NTG is advisable.
Thus, the rationale for NTG use in UA is extrapolatedfrom pathophysiological principles and extensive, althoughuncontrolled, clinical observations (133).
Morphine Sulfate
Morphine sulfate (1 to 5 mg intravenous [IV]) is recom-mended for patients whose symptoms are not relieved after3 serial sublingual NTG tablets or whose symptoms recurdespite adequate anti-ischemic therapy. Unless contraindi-cated by hypotension or intolerance, morphine may be admin-istered along with intravenous NTG, with careful bloodpressure monitoring, and may be repeated every 5 to 30 min asneeded to relieve symptoms and maintain patient comfort.
Morphine sulfate has potent analgesic and anxiolyticeffects, as well as hemodynamic effects that are potentiallybeneficial in UA/NSTEMI. No randomized trials havedefined the unique contribution of morphine to the initialtherapeutic regimen or its optimal administration schedule.Morphine causes venodilation and may produce modestreductions in heart rate (through increased vagal tone) andsystolic blood pressure to further reduce myocardial oxygendemand. The major adverse reaction to morphine is anexaggeration of its therapeutic effect, causing hypotension,especially in the presence of volume depletion and/orvasodilator therapy. This reaction usually responds to supineor Trendelenburg positioning or intravenous saline bolusesand atropine when accompanied by bradycardia; it rarelyrequires pressors or naloxone to restore blood pressure.Nausea and vomiting occur in '20% of patients. Respira-tory depression is the most serious complication of mor-phine; severe hypoventilation that requires intubation occursvery rarely in patients with UA/NSTEMI treated with thisagent. Naloxone (0.4 to 2.0 mg IV) may be administered for
morphine overdose with respiratory and/or circulatory de-pression. Meperidine hydrochloride can be substituted inpatients who are allergic to morphine.
b-Adrenergic Blockers
b-Blockers competitively block the effects of cat-echolamines on cell membrane b-receptors. b1-adrenergicreceptors are located primarily in the myocardium; inhibi-tion of catecholamine action at these sites reduces myocar-dial contractility, sinus node rate, and AV node conductionvelocity. Through this action, they blunt the heart rate andcontractility responses to chest pain, exertion, and otherstimuli. They also decrease systolic blood pressure. All ofthese effects reduce MVO2. b2-adrenergic receptors arelocated primarily in vascular and bronchial smooth muscle;the inhibition of catecholamine action at these sites pro-duces vasoconstriction and bronchoconstriction (141). InUA/NSTEMI, the primary benefits of b-blockers are dueto effects on b1-adrenergic receptors that decrease cardiacwork and myocardial oxygen demand. Slowing of the heartrate also has a very favorable effect, acting not only to reduceMVO2 but also to increase the duration of diastole anddiastolic pressure-time, a determinant of coronary flow andcollateral flow.
b-Blockers should be started early in the absence ofcontraindications. These agents should be administeredintravenously followed by oral administration in high-riskpatients as well as in patients with ongoing rest pain ororally for intermediate- and low-risk patients (Table 6).
The choice of b-blocker for an individual patient is basedprimarily on pharmacokinetic and side effect criteria, as wellas on physician familiarity (Table 12). There is no evidencethat any member of this class of agents is more effective thananother, except that b-blockers without intrinsic sympatho-mimetic activity are preferable. The initial choice of agentsincludes metoprolol, propranolol, or atenolol. Esmolol canbe used if an ultrashort-acting agent is required.
Patients with marked first-degree AV block (i.e., ECGPR interval [PR] of .0.24 s), any form of second- orthird-degree AV block in the absence of a functioning
Table 12. Properties of b-Blockers in Clinical Use
Drug SelectivityPartial Agonist
Activity Usual Dose for Angina
Propranolol None No 20–80 mg twice dailyMetoprolol b1 No 50–200 mg twice dailyAtenolol b1 No 50–200 mg/dNadolol None No 40–80 mg/dTimolol None No 10 mg twice dailyAcebutolol b1 Yes 200–600 mg twice dailyBetaxolol b1 No 10–20 mg/dBisoprolol b1 No 10 mg/dEsmolol (intravenous) b1 No 50–300 mgzkg21zmin21
Labetalol* None Yes 200–600 mg twice dailyPindolol None Yes 2.5–7.5 mg 3 times daily
*Labetalol is a combined a- and b-blocker.Adapted from Table 25 in Gibbons RJ, Chatterjee K, Daley J, et al. ACC/AHA/ACP-ASIM guidelines for the management
of patients with chronic stable angina. J Am Coll Cardiol 1999;33:2092–197.
996 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062

pacemaker, a history of asthma, or severe LV dysfunctionwith congestive heart failure (CHF) should not receiveb-blockers on an acute basis (26). Patients with significantsinus bradycardia (heart rate ,50 bpm) or hypotension(systolic blood pressure ,90 mm Hg) generally should notreceive b-blockers until these conditions have resolved.Patients with significant COPD who may have a compo-nent of reactive airway disease should be administeredb-blockers very cautiously; initially, low doses of a b1-selective agent should be used. If there are concerns aboutpossible intolerance to b-blockers, initial selection shouldfavor a short-acting b1-specific drug such as metoprolol.Mild wheezing or a history of COPD mandates a short-acting cardioselective agent at a reduced dose (e.g., 2.5 mgmetoprolol IV or 12.5 mg metoprolol orally or 25mgzkg21zmin21 esmolol IV as initial doses) rather than thecomplete avoidance of a b-blocker.
In the absence of these concerns, several regimens may beused. For example, intravenous metoprolol may be given in5-mg increments by slow intravenous administration (5 mgover 1 to 2 min), repeated every 5 min for a total initial doseof 15 mg. In patients who tolerate the total 15 mg IV dose,oral therapy should be initiated 15 min after the lastintravenous dose at 25 to 50 mg every 6 h for 48 h.Thereafter, patients should receive a maintenance dose of100 mg twice daily. Alternatively, intravenous propranolol isadministered as an initial dose of 0.5 to 1.0 mg, followed in1 to 2 h by 40 to 80 mg by mouth every 6 to 8 h. Intravenousesmolol is administered as a starting dose of 0.1mgzkg21zmin21 with titration in increments of 0.05mgzkg21zmin21 every 10 to 15 min as tolerated by thepatient’s blood pressure until the desired therapeutic re-sponse has been obtained, limiting symptoms develop, or adosage of 0.3 mgzkg21zmin21 is reached. A loading dose of0.5 mg/kg may be given by slow intravenous administration(2 to 5 min) for a more rapid onset of action. In patientssuitable to receive a longer-acting agent, intravenous ateno-lol can be initiated with a 5-mg IV dose followed 5 min laterby a second 5-mg IV dose and then 50 to 100 mg/d orallyinitiated 1 to 2 h after the intravenous dose. Monitoring duringintravenous b-blocker therapy should include frequent checksof heart rate and blood pressure and continuous ECG moni-toring, as well as auscultation for rales and bronchospasm.
After the initial intravenous load, patients without lim-iting side effects may be converted to an oral regimen. Thetarget resting heart rate is 50 to 60 bpm, unless a limitingside effect is reached. Selection of the oral agent should bebased on the clinician’s familiarity with the agent. Mainte-nance doses are given in Table 12.
Initial studies of b-blocker benefits in ACS were smalland uncontrolled. An overview of double-blind, randomizedtrials in patients with threatening or evolving MI suggestsan '13% reduction in the risk of progression to AMI (142).These trials lack sufficient power to assess the effects of thesedrugs on mortality rates for UA. However, randomizedtrials with other CAD patients (AMI, recent MI, stable
angina with daily life ischemia, and heart failure) have allshown reductions in mortality and/or morbidity rates. Thus,the rationale for b-blocker use in all forms of CAD,including UA, is very compelling and in the absence ofcontraindications is sufficient to make b-blockers a routinepart of care, especially in patients who are to undergocardiac or noncardiac surgery.
In conclusion, evidence for the beneficial effects of the useof b-blockers in patients with UA is based on limitedrandomized trial data, along with pathophysiological con-siderations and extrapolation from experience with CADpatients who have other types of ischemic syndromes (stableangina, AMI, or heart failure). The recommendation for theuse of intravenous b-blockers in high-risk patients withevolving pain is based on the demonstrated benefit in AMIpatients, as well as the hemodynamic objectives to reducecardiac work and myocardial oxygen demand. The durationof benefit with long-term oral therapy is uncertain.
Calcium Antagonists
These agents reduce cell transmembrane inward calciumflux, which inhibits both myocardial and vascular smoothmuscle contraction; some also slow AV conduction anddepress sinus node impulse formation. Agents in this classvary in the degree to which they produce vasodilation,decreased myocardial contractility, AV block, and sinusnode slowing. Nifedipine and amlodipine have the mostperipheral arterial dilatory effect but little or no AV or sinusnode effects, whereas verapamil and diltiazem have promi-nent AV and sinus node effects and some peripheral arterialdilatory effects as well. All 4 of these agents, as well as thenewer agents, have coronary dilatory properties that appearto be similar. Although different members of this class ofagents are structurally diverse and may have somewhatdifferent mechanisms of action, no reliable data demonstratethe superiority of 1 agent (or groups of agents) over anotherin ACS, except for the risks posed by rapid-release, short-acting dihydropyridines (Table 13). Beneficial effects inACS are believed to be due to variable combinations ofdecreased myocardial oxygen demand that relate to de-creased afterload, contractility, and heart rate and improvedmyocardial flow that relates to coronary artery and arteriolardilation (141,143). These agents also have theoretical ben-eficial effects on LV relaxation and arterial compliance.Major side effects include hypotension, worsening CHF,bradycardia, and AV block.
Calcium antagonists may be used to control ongoing orrecurring ischemia-related symptoms in patients who arealready receiving adequate doses of nitrates and b-blockers,in patients who are unable to tolerate adequate doses of 1 orboth of these agents, or in patients with variant angina (seeSection VI. F). In addition, these drugs have been used forthe management of hypertension in patients with recurrentUA (143). Rapid-release, short-acting dihydropyridines(e.g., nifedipine) must be avoided in the absence of adequate
997JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina

concurrent b-blockade in ACS because controlled trialssuggest increased adverse outcomes (144–146). Verapamiland diltiazem should be avoided in patients with pulmonaryedema or evidence of severe LV dysfunction (147,148).Amlodipine and felodipine, however, appear to be welltolerated by patients with chronic LV dysfunction (149).The choice of an individual calcium antagonist is basedprimarily on the type of agent; the hemodynamic state of thepatient; the risk of adverse effects on cardiac contractility,AV conduction, and sinus node function; and the physi-cian’s familiarity with the specific agent. Trials in patientswith acute CAD suggest that verapamil and diltiazem arepreferred if a calcium antagonist is needed (148,149).
There are several randomized trials that involve the use ofcalcium antagonists in ACS. Results generally confirm thatthese agents relieve or prevent symptoms and related isch-emia to a degree similar to that of b-blockers. The largestrandomized trial is the Danish Study Group on Verapamilin Myocardial Infarction (DAVIT) (150,151), in which3,447 patients with suspected ACS were administeredintravenous verapamil (0.1 mg/kg) at admission and then120 mg 3 times daily vs. placebo. After 1 week, verapamilwas discontinued in the patients (n 5 2,011) withoutconfirmed MI (presumably many of these patients had UA).Although there was no definitive evidence to suggest benefit(or harm) in this cohort, trends favored a reduction in theoutcome of death or nonfatal MI. In the Holland Interuni-versity Nifedipine/metoprolol Trial (HINT), nifedipine andmetoprolol were tested in a 2 3 2 factorial design in 515patients (146). Nifedipine alone increased the risk of MI orrecurrent angina relative to placebo by 16%, metoprololdecreased it by 24%, and the combination of metoprolol andnifedipine reduced this outcome by 20%. None of these
effects, however, were statistically significant because thestudy was stopped early because of concern for harm withthe use of nifedipine alone. However, in patients alreadytaking a b-blocker, the addition of nifedipine appearedfavorable because the event rate was reduced significantly(risk ratio [RR] 0.68) (152). Several meta-analyses thatcombined all of the calcium antagonists used in UA trialssuggested no overall effect (142,153). However, in light ofthe aforementioned differences between the rapid-releasedihydropyridines and the heart rate–slowing agents dilti-azem and verapamil, such analyses are not appropriate.When the data for verapamil are considered alone, abeneficial effect in patients with ACS is apparent (150).
Similarly, in the Diltiazem Reinfarction Study (DRS),576 patients were administered diltiazem or placebo 24 to72 h after the onset of non–Q-wave MI (145). Diltiazemwas associated with a reduction in CK-MB level–confirmedreinfarction and refractory angina at 14 days without asignificant increase in mortality rates. Retrospective analysisof the non–Q-wave MI subset of patients in the MulticenterDiltiazem Postinfarction Trial (MDPIT) suggested similarfindings without evidence of harm (154).
However, retrospective analyses of DAVIT and MDPITsuggested that the administration of verapamil and dilti-azem to suspected AMI patients who have LV dysfunction(many of whom had UA/NSTEMI) may have an overalldetrimental effect on mortality rates (145,147). Althoughthis caution is useful for clinical practice, more recent datasuggest that this issue should be readdressed. For example,in DAVIT-2, verapamil was associated with a significantreduction in diuretic use compared with placebo (155),suggesting that it did not further impair LV function.Furthermore, recent prospective trials with verapamil ad-
Table 13. Properties of Calcium Antagonists in Clinical Use
Drug Usual DoseDurationof Action Side Effects
DihydropyridinesNifedipine Immediate release: 30–90 mg
daily orallySlow release: 30–180 mg orally
Short Hypotension, dizziness, flushing,nausea, constipation, edema
Amlodipine 5–10 mg once daily Long Headache, edemaFelodipine 5–10 mg once daily Long Headache, edemaIsradipine 2.5–10 mg twice daily Medium Headache, fatigueNicardipine 20–40 mg 3 times daily Short Headache, dizziness, flushing, edemaNisoldipine 20–40 mg once daily Short Similar to nifedipineNitrendipine 20 mg once or twice daily Medium Similar to nifedipine
MiscellaneousBepridil 200–400 mg once daily Long Arrhythmias, dizziness, nauseaDiltiazem Immediate release: 30–80 mg
4 times dailySlow release: 120–320 mg
once daily
Short
Long
Hypotension, dizziness, flushing,bradycardia, edema
Verapamil Immediate release: 80–160 mg3 times daily
Short Hypotension, myocardial depression,heart failure, edema, bradycardia
Slow release: 120–480 mgonce daily
Long
Reprinted from Table 27 in Gibbons RJ, Chatterjee K, Daley J, et al. ACC/AHA/ACP-ASIM guidelines for the managementof patients with chronic stable angina. J Am Coll Cardiol 1999;33:2092–197.
998 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
ministered to AMI patients with heart failure who werereceiving an ACEI strongly suggest benefit (147,156). TheDiltiazem as Adjunctive Therapy to Activase (DATA) trialalso suggests that intravenous diltiazem in AMI patientsmay be safe; death, MI, or recurrent ischemia decreased by14% at 35 days and death, MI, or refractory ischemiadecreased by 23% at 6 months (157). These pilot data wereconfirmed in 874 AMI patients without heart failure inwhom long-acting diltiazem (300 mg/d) was administered36 to 96 h after thrombolysis (158) (W.E. Boden, oralpresentation, American Heart Association Scientific Ses-sions, Dallas, Texas, November 1998).
In conclusion, definitive evidence for benefit with allcalcium antagonists in UA is predominantly limited tosymptom control. For dihydropyridines, available random-ized trial data are not consistent with a beneficial effect onmortality or recurrent infarction rates but in fact providestrong evidence for an increase in these serious events whenthey are administered early as a rapid-release, short-actingpreparation without a b-blocker. Thus, these guidelinesrecommend reservation of the dihydropyridine calciumantagonists as second or third choices after the initiation ofnitrates and b-blockers. For the heart rate–slowing drugs(verapamil and diltiazem), there is no controlled trial evi-dence for harm when they are administered early to patientswith acute ischemic syndromes, and strong trends suggest abeneficial effect. Therefore, when b-blockers cannot beused, heart rate–slowing calcium antagonists offer an alter-native. When required for refractory symptom control, theseagents can be used early during the hospital phase, even inpatients with mild LV dysfunction, although the combina-tion of a b-blocker and calcium antagonist may act insynergy to depress LV function. The risks and benefits inUA of amlodipine and other newer agents relative to theolder agents in this class reviewed here remain undefined.
Other
ACEIs have been shown to reduce mortality rates inpatients with AMI or who recently had an MI and have LVsystolic dysfunction (159–161,161a), in diabetic patientswith LV dysfunction (162), and in a broad spectrum ofpatients with high-risk chronic CAD (163). Accordingly,ACEIs should be used in such patients as well as in thosewith hypertension that is not controlled with b-blockers andnitrates.
Other less extensively studied techniques for the relief ofischemia, such as spinal cord stimulation (164) and pro-longed external counterpulsation (165,166), are under eval-uation. Most experience has been gathered with spinal cordstimulation in “intractable angina” (167), in which anginalrelief has been described.
The KATP channel openers have hemodynamic andcardioprotective effects that could be useful in UA/NSTEMI. Nicorandil is such an agent that is approved in anumber of countries but not yet in the United States. In apilot double-blind, placebo-controlled study of 245 patients
with UA, the addition of this drug to conventional treat-ment significantly reduced the number of episodes oftransient myocardial ischemia (mostly silent) and of ventric-ular and supraventricular tachycardia (168). Further evalu-ation of this class of agents is under way.
B. Antiplatelet and Anticoagulation Therapy
Recommendations for Antiplatelet and AnticoagulationTherapy
Class I1. Antiplatelet therapy should be initiated promptly.
Aspirin is the first choice and is administered assoon as possible after presentation and is continuedindefinitely. (Level of Evidence: A)
2. A thienopyridine (clopidogrel or ticlopidine)should be administered to patients who are unableto take ASA because of hypersensitivity or majorgastrointestinal intolerance. (Level of Evidence: B)
3. Parenteral anticoagulation with intravenous un-fractionated heparin (UFH) or with subcutaneousLMWH should be added to antiplatelet therapywith ASA, or a thienopyridine. (Level of Evidence:B)
4. A platelet GP IIb/IIIa receptor antagonist shouldbe administered, in addition to ASA and UFH, topatients with continuing ischemia or with otherhigh-risk features (Table 6) and to patients inwhom a PCI is planned. Eptifibatide and tirofibanare approved for this use. (Level of Evidence: A)Abciximab can also be used for 12 to 24 h inpatients with UA/NSTEMI in whom a PCI isplanned within the next 24 h. (Level of Evidence: A)
Class III1. Intravenous thrombolytic therapy in patients with-
out acute ST-segment elevation, a true posteriorMI, or a presumed new left bundle-branch block(LBBB). (Level of Evidence: A)
Antithrombotic therapy is essential to modify the diseaseprocess and its progression to death, MI, or recurrent MI. Acombination of ASA, UFH, and a platelet GP IIb/IIIareceptor antagonist represents the most effective therapy.The intensity of treatment is tailored to individual risk, andtriple antithrombotic treatment is used in patients withcontinuing ischemia or with other high-risk features and inpatients oriented to an early invasive strategy (Table 14).Table 15 shows the recommended doses of the variousagents. An LMWH can be advantageously substituted forUFH, although experience with the former in PCI, inpatients referred for urgent CABG, and in combinationwith a GP IIb/IIIa antagonist and with a thrombolyticagent is limited. In the ESSENCE (169) and TIMI 11Btrials (170,171) in UA and NSTEMI, enoxaparin wasstopped 6 to 12 h before a planned percutaneous procedureor surgery and UFH was substituted. Trials are now under
999JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina

way to test the safety and efficacy of enoxaparin in patientsundergoing PCI and of enoxaparin and dalteparin com-bined with a GP IIb/IIIa antagonist and with a lytic agent.A pilot double-blind, randomized study of 55 patientscompared the combination of tirofiban and enoxaparin withthe combination of tirofiban and UFH. The results sug-
gested more reproducible inhibition of platelet aggregationwith enoxaparin and less prolongation in bleeding time.There was an excess of minor bleeding with enoxaparin butnot of major bleeding (172). Furthermore, there may beproblems in rapid reversal of the anticoagulation whenrequired, such as before CABG.
1. Antiplatelet Therapy (Aspirin, Ticlopidine,Clopidogrel)
Aspirin
Some of the strongest evidence available about thelong-term prognostic effects of therapy in patients withcoronary disease pertains to ASA (173). By irreversiblyinhibiting cyclooxygenase-1 within platelets, ASA preventsthe formation of thromboxane A2, thereby diminishingplatelet aggregation promoted by this pathway but not byothers. This platelet inhibition is the plausible mechanismfor clinical benefit of ASA because it is fully present withlow doses of ASA and because platelets represent one of theprincipal participants in thrombus formation after plaquedisruption. Alternative or additional mechanisms of actionfor ASA are possible, such as an anti-inflammatory effect(174), but they are unlikely at the low doses of ASA that areeffective in UA/NSTEMI.
Among all clinical investigations with ASA, trials inUA/NSTEMI have most consistently documented a strik-ing benefit of the drug independent of the differences instudy design, such as time of entry after the acute phase,duration of follow-up, and doses used (175–178) (Fig. 8).
No trial has directly compared the efficacy of differentdoses of ASA in patients who present with UA/NSTEMI.However, trials in secondary prevention of stroke, MI,death, and graft occlusion have not shown an added benefitfor ASA doses of .80 and 160 mg/d but have shown ahigher risk of bleeding. An overview of trials with differentdoses of ASA in long-term treatment of patients with CADsuggests similar efficacy for daily doses ranging from 75 to324 mg (173). A dose of 160 mg/d was used in the SecondInternational Study of Infarct Survival (ISIS-2) trial, whichdefinitively established the efficacy of ASA in suspected MI(185). It therefore appears reasonable to initiate ASAtreatment in patients with UA/NSTEMI at a dose of160 mg, as used in the ISIS-2 trial, or 325 mg. In patientswho present with suspected ACS who are not already receivingASA, the first dose may be chewed to rapidly establish a highblood level. Subsequent doses may be swallowed. Thereafter,daily doses of 75 to 325 mg are prescribed.
The prompt action of ASA and its ability to reducemortality rates in patients with suspected AMI enrolled inthe ISIS-2 trial led to the recommendation that ASA beinitiated immediately in the ED as soon as the diagnosis ofACS is made or suspected. In patients who are alreadyreceiving ASA, it should be continued. The protective effectof ASA has been sustained for at least 1 to 2 years in clinicaltrials in UA. Longer-term follow-up data in this population
Table 14. Class I Recommendations forAntithrombotic Therapy*
PossibleACS Likely/Definite ACS
Definite ACS With ContinuingIschemia or Other High-Risk
Features† or PlannedIntervention
Aspirin Aspirin Aspirin1 1
Subcutaneous LMWH IV heparinor 1
IV heparin IV platelet GP IIb/IIIa antagonist
*Clinical data on the combination of LMWH and platelet GP IIb/IIIa antagonists arelacking. Their combined use is not currently recommended.
†High-risk features are listed in Table 6; others include diabetes, recent MI, andelevated TnT or TnI.
Table 15. Clinical Use of Antithrombotic Therapy
Oral Antiplatelet TherapyAspirin Initial dose of 162–325 mg
nonenteric formulation followedby 75–160 mg/d of an enteric ora nonenteric formulation
Clopidogrel (Plavix) 75 mg/d; a loading dose of 4–8tablets (300–600 mg) can be usedwhen rapid onset of action isrequired
Ticlopidine ((Ticlid) 250 mg twice daily; a loading doseof 500 mg can be used whenrapid onset of inhibition isrequired; monitoring of plateletand white cell counts duringtreatment is required
HeparinsDalteparin (Fragmin) 120 IU/kg subcutaneously every 12
h (maximum 10,000 IU twicedaily)
Enoxaparin (Lovenox) 1 mg/kg subcutaneously every 12 h;the first dose may be preceded bya 30-mg IV bolus
Heparin (UFH) Bolus 60–70 U/kg (maximum 5000U) IV followed by infusion of12–15 Uzkg21zh21 (maximum1000 U/h) titrated to aPTT 1.5–2.5 times control
Intravenous Antiplatelet TherapyAbciximab (ReoPro) 0.25 mg/kg bolus followed by
infusion of 0.125 mgzkg21zmin21
(maximum 10 mg/min) for 12 to24 h
Eptifibatide (Integrilin) 180 mg/kg bolus followed byinfusion of 2.0 mgzkg21zmin21 for72 to 96 h*
Tirofiban (Aggrastat) 0.4 mgzkg21zmin21 for 30 minutesfollowed by infusion of 0.1mgzkg21zmin21 for 48 to 96 h*
*Different dose regimens were tested in recent clinical trials before percutaneousinterventions.
1000 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
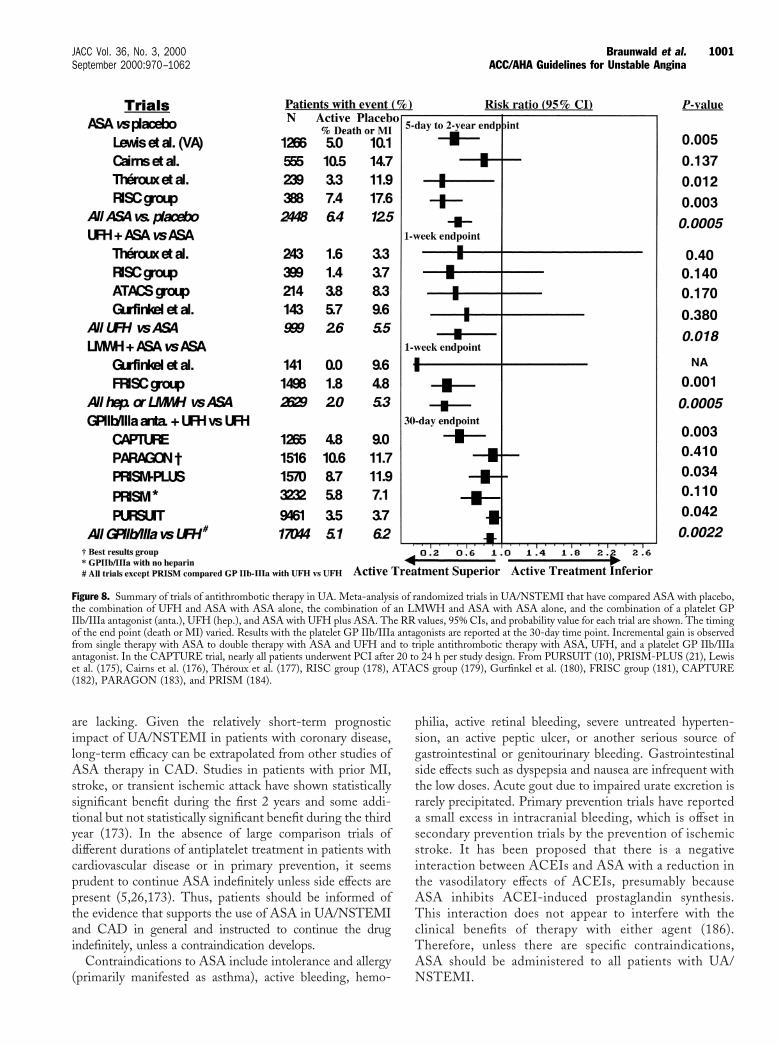
are lacking. Given the relatively short-term prognosticimpact of UA/NSTEMI in patients with coronary disease,long-term efficacy can be extrapolated from other studies ofASA therapy in CAD. Studies in patients with prior MI,stroke, or transient ischemic attack have shown statisticallysignificant benefit during the first 2 years and some addi-tional but not statistically significant benefit during the thirdyear (173). In the absence of large comparison trials ofdifferent durations of antiplatelet treatment in patients withcardiovascular disease or in primary prevention, it seemsprudent to continue ASA indefinitely unless side effects arepresent (5,26,173). Thus, patients should be informed ofthe evidence that supports the use of ASA in UA/NSTEMIand CAD in general and instructed to continue the drugindefinitely, unless a contraindication develops.
Contraindications to ASA include intolerance and allergy(primarily manifested as asthma), active bleeding, hemo-
philia, active retinal bleeding, severe untreated hyperten-sion, an active peptic ulcer, or another serious source ofgastrointestinal or genitourinary bleeding. Gastrointestinalside effects such as dyspepsia and nausea are infrequent withthe low doses. Acute gout due to impaired urate excretion israrely precipitated. Primary prevention trials have reporteda small excess in intracranial bleeding, which is offset insecondary prevention trials by the prevention of ischemicstroke. It has been proposed that there is a negativeinteraction between ACEIs and ASA with a reduction inthe vasodilatory effects of ACEIs, presumably becauseASA inhibits ACEI-induced prostaglandin synthesis.This interaction does not appear to interfere with theclinical benefits of therapy with either agent (186).Therefore, unless there are specific contraindications,ASA should be administered to all patients with UA/NSTEMI.
Figure 8. Summary of trials of antithrombotic therapy in UA. Meta-analysis of randomized trials in UA/NSTEMI that have compared ASA with placebo,the combination of UFH and ASA with ASA alone, the combination of an LMWH and ASA with ASA alone, and the combination of a platelet GPIIb/IIIa antagonist (anta.), UFH (hep.), and ASA with UFH plus ASA. The RR values, 95% CIs, and probability value for each trial are shown. The timingof the end point (death or MI) varied. Results with the platelet GP IIb/IIIa antagonists are reported at the 30-day time point. Incremental gain is observedfrom single therapy with ASA to double therapy with ASA and UFH and to triple antithrombotic therapy with ASA, UFH, and a platelet GP IIb/IIIaantagonist. In the CAPTURE trial, nearly all patients underwent PCI after 20 to 24 h per study design. From PURSUIT (10), PRISM-PLUS (21), Lewiset al. (175), Cairns et al. (176), Theroux et al. (177), RISC group (178), ATACS group (179), Gurfinkel et al. (180), FRISC group (181), CAPTURE(182), PARAGON (183), and PRISM (184).
1001JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
Adenosine Diphosphate Receptor Antagonists and OtherAntiplatelet Agents
Two thienopyridines—ticlopidine and clopidogrel—areadenosine diphosphate (ADP) antagonists that are currentlyapproved for antiplatelet therapy (187). The platelet effectsof ticlopidine and clopidogrel are irreversible but take severaldays to become completely manifest. Because the mechanismsof the antiplatelet effects of ASA and ADP antagonists differ,a potential exists for additive benefit with the combination.
Ticlopidine has been used successfully for the secondaryprevention of stroke and MI and for the prevention of stentclosure and graft occlusion. In an open-label trial (188), 652patients with UA were randomized to receive 250 mgticlopidine twice a day or standard therapy without ASA. At6-month follow-up, ticlopidine reduced the rate of fatal andnonfatal MI by 46% (13.6% vs. 7.3%, p 5 0.009). Thebenefit of ticlopidine in the study developed after only 2weeks of treatment, which is consistent with the delay of thedrug to achieve full effect.
The adverse effects of ticlopidine limit its usefulness:gastrointestinal problems (diarrhea, abdominal pain, nausea,vomiting), neutropenia in '2.4% of patients, severe neu-tropenia in 0.8% of patients, and, rarely, thrombotic throm-bocytopenia purpura (TTP) (189). Neutropenia usuallyresolves within 1 to 3 weeks of discontinuation of therapybut very rarely may be fatal. TTP, which also is a veryuncommon life-threatening complication, requires immedi-ate plasma exchange. Monitoring of ticlopidine therapyrequires a complete blood count that includes a differentialcount every 2 weeks for the first 3 months of therapy.
Most clinical experience with clopidogrel is derived fromthe Clopidogrel versus Aspirin in Patients at Risk ofIschaemic Events (CAPRIE) trial (190). A total of 19,185patients were randomized to receive 325 mg/d ASA or75 mg/d clopidogrel. Entry criteria consisted of atheroscle-rotic vascular disease manifested as recent ischemic stroke,recent MI, or symptomatic peripheral arterial disease.Follow-up extended for 1 to 3 years. The RR of ischemicstroke, MI, or vascular death was reduced by 8.7% in favorof clopidogrel from 5.83% to 5.32% (p 5 0.043). There wasa slightly increased, but minimal, incidence of rash anddiarrhea with clopidogrel treatment and slightly morebleeding with ASA. There was no excess neutropenia withclopidogrel, which contrasts with ticlopidine. The resultsprovide evidence that clopidogrel is at least as effective asASA and may be modestly more effective. In a recent report,11 severe cases of TTP were described as occurring within14 days after the initiation of clopidogrel; plasma exchangewas required in 10 of the patients, and 1 patient died (191).These cases occurred among more than 3 million patientstreated with clopidogrel.
Ticlopidine or clopidogrel is reasonable antiplatelet ther-apy for secondary prevention with an efficacy at least similarto that of ASA. These drugs are indicated in patients withUA/NSTEMI who are unable to tolerate ASA due to either
hypersensitivity or major gastrointestinal contraindications,principally recent significant bleeding from a peptic ulcer orgastritis. Care must be taken during the acute phase withthese drugs because of the delays required to achieve a fullantiplatelet effect. Clopidogrel is preferred to ticlopidinebecause it more rapidly inhibits platelets and appears to havea more favorable safety profile. Experience is being acquiredwith this drug in acute situations with a loading dose(300 mg) to achieve more rapid platelet inhibition. Initialtreatment with heparin (UFH or LMWH) and probablywith a GP IIb/IIIa antagonist is especially important inpatients with UA/NSTEMI who are treated with 1 of thethienopyridines because of their delayed onset of antiplateletactivity compared with ASA.
Two randomized trials were recently completed in whichclopidogrel was compared with ticlopidine. In 1 study, 700patients who successfully received a stent were randomizedto receive 500 mg ticlopidine or 75 mg clopidogrel, inaddition to 100 mg ASA, for 4 weeks (192). Cardiac death,urgent target vessel revascularization, angiographically doc-umented thrombotic stent occlusion, or nonfatal MI within30 days occurred in 3.1% of patients who received clopi-dogrel and 1.7% of patients who received ticlopidine (p 50.24), and noncardiac death, stroke, severe peripheral vas-cular hemorrhagic events, or any adverse event that resultedin the discontinuation of the study medication occurred in4.5% and 9.6% of patients, respectively (p 5 0.01). TheCLopidogrel ASpirin Stent International CooperativeStudy (CLASSICS) (P. Urban, A.H. Gershlick, H.-J.Rupprecht, M.E. Bertrands, oral presentation, AmericanHeart Association Scientific Sessions, Atlanta, Ga, Novem-ber 1999) was conducted in 1,020 patients. A loading doseof 300 mg clopidogrel followed by 75 mg/d was comparedto a daily dose of 75 mg without a loading dose and with aloading dose of 150 mg ticlopidine followed by 150 mgtwice a day (patients in each of the 3 arms also receivedASA). The first dose was administered 1 to 6 h after stentimplantation; the treatment duration was 28 days. The trialshowed better tolerance to clopidogrel with or without aloading dose than to ticlopidine. Stent thrombosis or majorcomplications occurred at the same frequency in the 3groups. The regimen of a loading dose (300 mg) followed bythe maintenance dose (75 mg/d) is used in the ongoing largeClopidogrel in Unstable angina to Prevent ischemic Events(CURE) trial, which compares the combination of clopi-dogrel and ASA with ASA alone in patients with UA/NSTEMI.
Sulfinpyrazone, dipyridamole, prostacyclin, and prostacy-clin analogs have not been associated with benefit in UA orNSTEMI and are not recommended. The thromboxanesynthase blockers and thromboxane A2 receptor antagonistshave been evaluated in ACS but have not shown anyadvantage over ASA. A number of other antiplatelet drugsare currently available, and still others are under activeinvestigation. Oral GP IIb/IIIa receptor blockers weretested in 1 PCI trial and 3 UA/NSTEMI trials; the 4 trials
1002 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062

failed to document a benefit and 2 showed an excessmortality rate (193,193a,193b).
ASA plus an intravenous GP IIb/IIIa antagonist remainsthe reference standard for antiplatelet therapy in patientswith UA/NSTEMI who are at higher risk. Ticlopidine isnot recommended during the acute phase because it takesseveral days to achieve its maximal antiplatelet effect.
2. Anticoagulants. Anticoagulants available for parenteraluse include UFH, various LMWHs, and hirudin, and fororal use, the antivitamin K drugs are available. Syntheticpentasaccharides and synthetic direct thrombin inhibitors(argatroban, bivaluridine) as well as oral direct and indirectthrombin inhibitors are under clinical investigation. Hiru-din is approved as an anticoagulant in patients with heparin-induced thrombocytopenia and for the prophylaxis of deepvein thrombosis after hip replacement.
Heparin exerts its anticoagulant effect by accelerating theaction of circulating antithrombin, a proteolytic enzyme thatinactivates factor IIa (thrombin), factor IXa, and factor Xa.It prevents thrombus propagation but does not lyse existingthrombi (194). UFH is a heterogeneous mixture of chains ofmolecular weights that range from 5,000 to 30,000 and havevarying effects on anticoagulant activity. UFH binds to anumber of plasma proteins, blood cells, and endothelialcells. The LMWHs are obtained through chemical orenzymatic depolymerization of the polysaccharide chains ofheparin to provide chains with different molecular weightdistributions. About 25% to 50% of the pentasaccharide-containing chains of LMWH preparations contain .18saccharide units, and these are able to inactivate boththrombin and factor Xa. However, LMWH chains that are,18 saccharide units retain their ability to inactivate factorXa but not thrombin. Therefore, LMWHs are relativelymore potent in the catalyzation of the inhibition of factorXa by antithrombin than in the inactivation of thrombin.Distinct advantages of LMWH over UFH include de-creased binding to plasma proteins and endothelial cells anddose-independent clearance with a longer half-life thatresults in more predictable and sustained anticoagulationwith once- or twice-a-day subcutaneous administration. Amajor advantage of LMWHs is that they do not usuallyrequire laboratory monitoring of activity. The pharmacody-namic and pharmacokinetic profiles of the different com-mercial preparations of LMWHs vary, with their meanmolecular weights ranging from 4,200 to 6,000. Accord-ingly, their ratios of anti–Xa factor to anti–IIa factor vary,ranging from 1.9 to 3.8 (195).
By contrast, the direct thrombin inhibitors very specifi-cally block thrombin effects without the need for a cofactorsuch as antithrombin. Hirudin binds directly to the anionbinding site and the catalytic sites of thrombin to producepotent and predictable anticoagulation (196). Several largetrials (see later) that compare hirudin with UFH in UA/NSTEMI have demonstrated a modest short-term reduc-
tion in the composite end point of death or nonfatal MIwith a modest increase in the risk of bleeding.
Bivalurudin (Hirulog) is a synthetic analog of hirudin thatbinds reversibly to thrombin. It has been compared withUFH in several small trials in UA/NSTEMI and in PCIwith some evidence of a reduction in death or MI and lessbleeding than with UFH (197–199).
Unfractionated Heparin
Seven randomized, placebo-controlled trials with UFHhave been reported (200–205). A placebo-controlled studyperformed by Theroux et al. (177) between 1986 and 1988tested treatments that consisted of ASA and a 5,000-U IVbolus of UFH followed by 1,000 U/h in a 2 3 2 factorialdesign. UFH reduced the risk of MI by 89% and the risk ofrecurrent refractory angina by 63%. An extension of thisstudy compared ASA and UFH in UA patients. MI (fatal ornonfatal) occurred in 3.7% of patients who received ASAand 0.8% of patients who received UFH (p 5 0.035) (202).
The Research Group in Instability in Coronary ArteryDisease (RISC) trial was a double-blind, placebo-controlledtrial with a 2 3 2 factorial design that was conducted in menwith UA or NSTEMI (178). ASA significantly reduced therisk of death or MI. UFH alone had no benefit, althoughthe group treated with the combination of ASA and UFHhad the lowest number of events during the initial 5 days.Neri-Seneri et al. (203) suggested that symptomatic andsilent episodes of ischemia in UA could be prevented by aninfusion of UFH but not by bolus injections or by ASA.Taken together, these trials indicate that the early admin-istration of UFH is associated with a reduction in theincidence of AMI and ischemia in patients with UA/NSTEMI.
The results of the studies that have compared the com-bination of ASA and heparin with ASA alone are shown inFig. 8. In the trials that used UFH, the reduction in the rateof death or MI during the first week was 54% (p 5 0.016),and in the trials that used either UFH or LMWH, thereduction was 63%. Two published meta-analyses haveincluded different studies. In 1 meta-analysis, which in-volved 3 randomized trials and an early end point (,5 days)(179), the risk of death or MI with the combination of ASAand heparin was reduced by 56% (p 5 0.03). In the secondmeta-analysis, which involved 6 trials and end points thatranged from 2 to 12 weeks, the RR was reduced by 33%(p 5 0.06) (206). Most of the benefits of the variousanticoagulants are short term, however, and not maintainedon a long-term basis. Reactivation of the disease processafter the discontinuation of anticoagulants may contributeto this loss of early gain that has been described with UFH(207), dalteparin (181), and hirudin (208,209). The combi-nation of UFH and ASA appears to mitigate this reactiva-tion in part (207,210), although there is hematologic evi-dence of increased thrombin activity after the cessation ofintravenous UFH even in the presence of ASA (211).Uncontrolled observations suggested a reduction in the
1003JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
“heparin rebound” by switching from intravenous to subcu-taneous UFH for several days before the drug is stopped.
UFH has important pharmacokinetic limitations that arerelated to its nonspecific binding to proteins and cells.These pharmacokinetic limitations of UFH translate intopoor bioavailability, especially at low doses, and markedvariability in anticoagulant response among patients (212).As a consequence of these pharmacokinetic limitations, theanticoagulant effect of heparin requires monitoring with theactivated partial thromboplastin time (aPTT), a test that issensitive to the inhibitory effects of UFH on thrombin(factor IIa), factor Xa, and factor IXa. Many clinicians havetraditionally prescribed a fixed initial dose of UFH (e.g.,5,000-U bolus, 1,000 U/h initial infusion); clinical trialshave indicated that a weight-adjusted dosing regimen couldprovide more predictable anticoagulation than the fixed-dose regimen (213–215). The weight-adjusted regimen isrecommended with an initial bolus of 60 to 70 U/kg(maximum 5,000 U) and an initial infusion of 12 to 15Uzkg21zh21 (maximum 1,000 U/h). The therapeutic rangeof the various nomograms differs due to variation in thelaboratory methods used to determine aPTT. The Ameri-can College of Chest Physicians consensus conference (212)has therefore recommended dosage adjustments of thenomograms to correspond to a therapeutic range equivalentto heparin levels of 0.3 to 0.7 U/mL by anti–factor Xadeterminations, which correlates with aPTT values between60 and 80 s. In addition to body weight, other clinicalfactors that affect the response to UFH include age, whichis associated with higher aPTT values, and smoking historyand diabetes mellitus, which are associated with loweraPTT values (212,216).
Thus, even though weight-based UFH dosing regimensare used, the aPTT should be monitored for adjustment ofUFH dosing. Because of variation among hospitals in thecontrol aPTT values, nomograms should be established ateach institution that are designed to achieve aPTT values inthe target range (e.g., for a control aPTT of 30 s, the targetrange [1.5 to 2.5 times control] would be 45 to 75 s).Measurements should be made 6 h after any dosage changeand used to adjust UFH infusion until the aPTT exhibits atherapeutic level. When 2 consecutive aPTT values aretherapeutic, the measurements may be made every 24 h and,if necessary, dose adjustment carried out. In addition, asignificant change in the patient’s clinical condition (e.g.,recurrent ischemia, bleeding, hypotension) should promptan immediate aPTT determination, followed by dose ad-justment, if necessary.
Serial hemoglobin/hematocrit and platelet measurementsare recommended at least daily during UFH therapy. Inaddition, any clinically significant bleeding, recurrent symp-toms, or hemodynamic instability should prompt theirimmediate determination. Serial platelet counts are neces-sary to monitor for heparin-induced thrombocytopenia.Mild thrombocytopenia may occur in 10% to 20% ofpatients who are receiving heparin, whereas severe throm-
bocytopenia (platelet count ,100,000) occurs in 1% to 2%of patients and typically appears after 4 to 14 days oftherapy. A rare but dangerous complication (,0.2% inci-dence) is autoimmune UFH-induced thrombocytopeniawith thrombosis (217). A high clinical suspicion mandatesthe immediate cessation of all heparin therapy (includingthat used to flush intravenous lines).
Most of the trials that evaluate the use of UFH inUA/NSTEMI have continued therapy for 2 to 5 days. Theoptimal duration of therapy remains undefined.
Low-Molecular-Weight Heparin
In a pilot open-label study, 219 patients with UA wererandomized to receive ASA (200 mg/d), to ASA plus UFH,or to ASA plus nadroparin, an LMWH. The combinationof ASA and LMWH significantly reduced the total isch-emic event rate, the rate of recurrent angina, and thenumber of patients requiring interventional procedures(180).
The FRISC study (181) randomized 1,506 patients withUA or non–Q-wave MI to receive subcutaneous adminis-tration of the LMWH dalteparin (120 IU/kg twice daily) orplacebo for 6 days and then once a day for the next 35 to 45days. Dalteparin was associated with a 63% risk reduction indeath or MI during the first 6 days (4.8% vs. 1.8%, p 50.001), matching the favorable experience observed withUFH. Although an excess of events was observed after thedose reduction to once daily after 6 days, a significantdecrease was observed at 40 days with dalteparin in thecomposite outcome of death, MI, or revascularization(23.7% vs. 18.0%, p 5 0.005), and a trend was noted in areduction in rates of death or MI (10.7% vs. 8.0%, p 50.07).
LMWH Versus UFH
Four large randomized trials have directly compared anLMWH with UFH (Fig. 9). In the FRagmin In unstableCoronary artery disease (FRIC) study, 1,482 patients withUA/NSTEMI received open-label dalteparin (120 IU/kgsubcutaneously twice a day) or UFH for 6 days (218). At day6 and until day 45, patients were randomized a second timeto double-blind administration of dalteparin (120 IU/kgonce a day) or placebo. During the first part of the study, therisk of death, MI, or recurrent angina was nonsignificantlyincreased with dalteparin (9.3% vs. 7.65%, p 5 0.33), and therisk of death or MI was unaffected (3.9% vs. 3.6%, p 5 0.8);death also tended to occur more frequently with dalteparin(1.5% vs. 0.4% with UFH, p 5 0.057). Between days 6 and45, the rates of death, MI, and recurrence of angina werecomparable between the active treatment and placebogroups.
The ESSENCE trial (169) compared enoxaparin(1 mg/kg twice daily subcutaneous administration) withstandard UFH (5,000 U bolus), followed by an infusiontitrated to an aPTT of 55 to 86 s, administered for 48 h to8 days (median duration in both groups of 2.6 days) (169).
1004 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
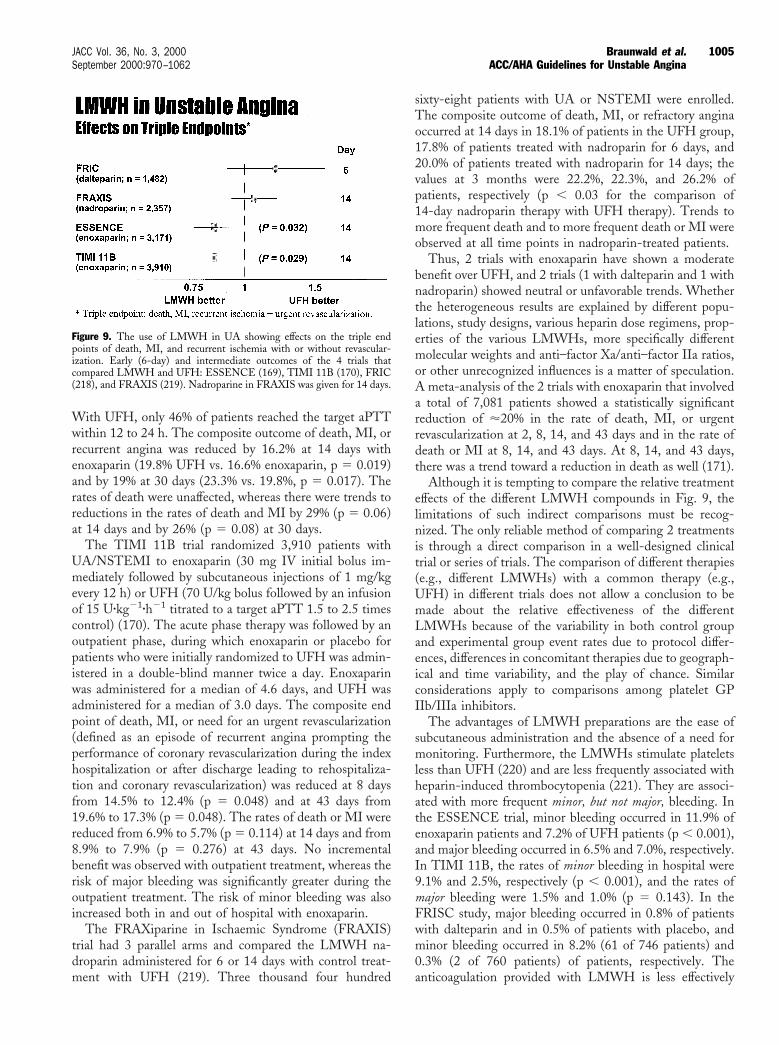
With UFH, only 46% of patients reached the target aPTTwithin 12 to 24 h. The composite outcome of death, MI, orrecurrent angina was reduced by 16.2% at 14 days withenoxaparin (19.8% UFH vs. 16.6% enoxaparin, p 5 0.019)and by 19% at 30 days (23.3% vs. 19.8%, p 5 0.017). Therates of death were unaffected, whereas there were trends toreductions in the rates of death and MI by 29% (p 5 0.06)at 14 days and by 26% (p 5 0.08) at 30 days.
The TIMI 11B trial randomized 3,910 patients withUA/NSTEMI to enoxaparin (30 mg IV initial bolus im-mediately followed by subcutaneous injections of 1 mg/kgevery 12 h) or UFH (70 U/kg bolus followed by an infusionof 15 Uzkg21zh21 titrated to a target aPTT 1.5 to 2.5 timescontrol) (170). The acute phase therapy was followed by anoutpatient phase, during which enoxaparin or placebo forpatients who were initially randomized to UFH was admin-istered in a double-blind manner twice a day. Enoxaparinwas administered for a median of 4.6 days, and UFH wasadministered for a median of 3.0 days. The composite endpoint of death, MI, or need for an urgent revascularization(defined as an episode of recurrent angina prompting theperformance of coronary revascularization during the indexhospitalization or after discharge leading to rehospitaliza-tion and coronary revascularization) was reduced at 8 daysfrom 14.5% to 12.4% (p 5 0.048) and at 43 days from19.6% to 17.3% (p 5 0.048). The rates of death or MI werereduced from 6.9% to 5.7% (p 5 0.114) at 14 days and from8.9% to 7.9% (p 5 0.276) at 43 days. No incrementalbenefit was observed with outpatient treatment, whereas therisk of major bleeding was significantly greater during theoutpatient treatment. The risk of minor bleeding was alsoincreased both in and out of hospital with enoxaparin.
The FRAXiparine in Ischaemic Syndrome (FRAXIS)trial had 3 parallel arms and compared the LMWH na-droparin administered for 6 or 14 days with control treat-ment with UFH (219). Three thousand four hundred
sixty-eight patients with UA or NSTEMI were enrolled.The composite outcome of death, MI, or refractory anginaoccurred at 14 days in 18.1% of patients in the UFH group,17.8% of patients treated with nadroparin for 6 days, and20.0% of patients treated with nadroparin for 14 days; thevalues at 3 months were 22.2%, 22.3%, and 26.2% ofpatients, respectively (p , 0.03 for the comparison of14-day nadroparin therapy with UFH therapy). Trends tomore frequent death and to more frequent death or MI wereobserved at all time points in nadroparin-treated patients.
Thus, 2 trials with enoxaparin have shown a moderatebenefit over UFH, and 2 trials (1 with dalteparin and 1 withnadroparin) showed neutral or unfavorable trends. Whetherthe heterogeneous results are explained by different popu-lations, study designs, various heparin dose regimens, prop-erties of the various LMWHs, more specifically differentmolecular weights and anti–factor Xa/anti–factor IIa ratios,or other unrecognized influences is a matter of speculation.A meta-analysis of the 2 trials with enoxaparin that involveda total of 7,081 patients showed a statistically significantreduction of '20% in the rate of death, MI, or urgentrevascularization at 2, 8, 14, and 43 days and in the rate ofdeath or MI at 8, 14, and 43 days. At 8, 14, and 43 days,there was a trend toward a reduction in death as well (171).
Although it is tempting to compare the relative treatmenteffects of the different LMWH compounds in Fig. 9, thelimitations of such indirect comparisons must be recog-nized. The only reliable method of comparing 2 treatmentsis through a direct comparison in a well-designed clinicaltrial or series of trials. The comparison of different therapies(e.g., different LMWHs) with a common therapy (e.g.,UFH) in different trials does not allow a conclusion to bemade about the relative effectiveness of the differentLMWHs because of the variability in both control groupand experimental group event rates due to protocol differ-ences, differences in concomitant therapies due to geograph-ical and time variability, and the play of chance. Similarconsiderations apply to comparisons among platelet GPIIb/IIIa inhibitors.
The advantages of LMWH preparations are the ease ofsubcutaneous administration and the absence of a need formonitoring. Furthermore, the LMWHs stimulate plateletsless than UFH (220) and are less frequently associated withheparin-induced thrombocytopenia (221). They are associ-ated with more frequent minor, but not major, bleeding. Inthe ESSENCE trial, minor bleeding occurred in 11.9% ofenoxaparin patients and 7.2% of UFH patients (p , 0.001),and major bleeding occurred in 6.5% and 7.0%, respectively.In TIMI 11B, the rates of minor bleeding in hospital were9.1% and 2.5%, respectively (p , 0.001), and the rates ofmajor bleeding were 1.5% and 1.0% (p 5 0.143). In theFRISC study, major bleeding occurred in 0.8% of patientswith dalteparin and in 0.5% of patients with placebo, andminor bleeding occurred in 8.2% (61 of 746 patients) and0.3% (2 of 760 patients) of patients, respectively. Theanticoagulation provided with LMWH is less effectively
Figure 9. The use of LMWH in UA showing effects on the triple endpoints of death, MI, and recurrent ischemia with or without revascular-ization. Early (6-day) and intermediate outcomes of the 4 trials thatcompared LMWH and UFH: ESSENCE (169), TIMI 11B (170), FRIC(218), and FRAXIS (219). Nadroparine in FRAXIS was given for 14 days.
1005JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina

reversed with protamine than it is with UFH. In addition,LMWH administered during PCI does not permit moni-toring of the activated clotting time (ACT) to titrate thelevel of anticoagulation. In the ESSENCE and TIMI 11Btrials, special rules were set to discontinue enoxaparin beforePCI and CABG. UFH was administered during PCI toachieve ACT values of .350 s. An economic analysis of theESSENCE trial suggested cost savings with enoxaparin(222). Additional experience with regard to the safety andefficacy of the concomitant administration of LMWHs withGP IIb/IIIa antagonists and thrombolytic agents is cur-rently being acquired.
The FRISC, FRIC, TIMI 11B, and Fast Revasculariza-tion During Instability in Coronary Artery Disease (FRISCII) trials evaluated the potential benefit of the prolongedadministration of an LMWH after hospital discharge. Thefirst 3 of these trials did not show a benefit of treatmentbeyond the acute phase. In the FRISC trial, reduced dosesof enoxaparin were administered between 6 days and 35 to45 days; in FRIC, patients were rerandomized after theinitial 6-day treatment period to receive dalteparin for anadditional 40 days; and the outpatient treatment periodlasted 5 to 6 weeks in TIMI 11B and 1 week in the FRAXIStrial. The FRISC II trial used a different study design.Dalteparin was administered to all patients for a minimumof 5 days (223). Patients were subsequently randomized toreceive placebo or the continued administration of daltepa-rin twice a day for up to 90 days. Analysis of the results fromthe time of randomization showed a significant reductionwith dalteparin in the composite end point of death or MIat 30 days (3.1% vs. 5.9%, p 5 0.002) but not at 3 months(6.7% vs. 8.0%, p 5 0.17). The composite of death, MI, orrevascularization during the total treatment period wasreduced at 3 months (29.1% vs. 33.4%, p 5 0.031). Thebenefits of prolonged dalteparin administration were limitedto patients who were managed medically and to patientswith elevated TnT levels at baseline. These results maymake a case for the prolonged use of an LMWH in selectedpatients who are managed medically or in whom angiogra-phy is delayed.
Hirudin and Other Direct Thrombin Inhibitors
Hirudin, the prototype of the direct thrombin inhibitors,has been extensively studied. The GUSTO-IIb trial ran-domly assigned 12,142 patients to 72 h of therapy witheither intravenous hirudin or UFH (224). Patients werestratified according to the presence of ST-segment elevationon the baseline ECG (4,131 patients) or its absence (8,011patients). The primary end point of death, nonfatal MI, orreinfarction at 30 days occurred in 9.8% of the UFH groupvs. 8.9% of the hirudin group (odds ratio [OR] 0.89, p 50.058). For patients without ST-segment elevation, therates were 9.1% and 8.3%, respectively (OR 0.90, p 5 0.22).At 24 h, the risk of death or MI was significantly lower inthe patients who received hirudin than in those whoreceived UFH (2.1% vs. 1.3%, p 5 0.001). However, the
Thrombolysis and Thrombin Inhibition in Myocardial In-farction (TIMI) 9B trial of hirudin as adjunctive therapy tothrombolytic therapy in patients with STEMI showed nobenefit of the drug over UFH either during study druginfusion or later (225). The GUSTO-IIb and TIMI 9Btrials used hirudin doses of 0.1 mg/kg bolus and 0.1mgzkg21zh21 infusion for 3 to 5 days after the documenta-tion of excess bleeding with the higher doses used in theGUSTO-IIA and Thrombolysis and Thrombin Inhibitionin Myocardial Infarction (TIMI) 9A trials (0.6 mg/kg bolusand 0.2 mgzkg21zh21 infusion) (224,226).
The Organization to Assess Strategies for IschemicSyndromes (OASIS) program evaluated hirudin in patientswith UA or non–Q-wave MI. OASIS 1 (227) was a pilottrial of 909 patients that compared the low hirudin dose of0.1 mg/h infusion and the medium hirudin dose of0.15 mg/h infusion with UFH. The latter dose provided thebest results, with a reduction in the rate of death, MI, orrefractory angina at 7 days (6.5% with UFH vs. 3.3% withhirudin, p 5 0.047). This medium dose was used in thelarge OASIS 2 (228) trial that consisted of 10,141 patientswith UA/NSTEMI who were randomized to receive UFH(5,000 IU bolus plus 15 Uzkg21zh21) or recombinanthirudin (0.4 mg/kg bolus and 0.15 mgzkg21zh21) infusionfor 72 h. The primary end point of cardiovascular death ornew MI at 7 days occurred in 4.2% in the UFH group vs.3.6% patients in the hirudin group (RR 0.84, p 5 0.064). Asecondary end point of cardiovascular death, new MI, orrefractory angina at 7 days was significantly reduced withhirudin (6.7% vs. 5.6%, RR 0.83, p 5 0.011). There was anexcess of major bleeds that required transfusion with hirudin(1.2% vs. 0.7% with heparin, p 5 0.014) but no excess inlife-threatening bleeds or strokes. A meta-analysis of theGUSTO-IIB, TIMI 9B, OASIS 1, and OASIS 2 trialsshowed risks of death or MI at 35 days relative to heparinafter randomization of 0.90 (p 5 0.015) with hirudincompared with UFH; RR values were 0.88 (p 5 0.13) forpatients receiving thrombolytic agents and 0.90 (p 5 0.054)for patients not receiving thrombolytic agents (228). At72 h, the RR values of death or MI were 0.78 (p 5 0.003),0.89 (p 5 0.34), and 0.72 (p 5 0.002), respectively.Additional trials of direct antithrombins in UA/NSTEMIappear warranted.
Hirudin (lepirudin) is presently indicated only for anti-coagulation in patients with heparin-induced thrombocyto-penia (221) and for the prophylaxis of deep vein thrombosisin patients undergoing hip replacement surgery. It should beadministered as a 0.4 mg/kg IV bolus over 15 to 20 sfollowed by a continuous intravenous infusion of 0.15mgzkg21zh21, with adjustment of the infusion to a targetrange of 1.5 to 2.5 times the control aPTT values.
Long-Term Anticoagulation
The long-term administration of warfarin has been eval-uated in a few pilot studies. Williams et al. (201) random-ized 102 patients with UA to UFH for 48 h followed by
1006 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
open-label warfarin for 6 months and reported a 65% riskreduction in the rate of MI or recurrent UA. In theAntithrombotic Therapy in Acute Coronary Syndromes(ATACS) trial, Cohen et al. (179) randomized 214 patientswith UA/NSTEMI to ASA alone or the combination ofASA plus UFH followed by warfarin. At 14 days, there wasa reduction in the composite end point of death, MI, andrecurrent ischemia with the combination therapy (27.0% vs.10.5%, p 5 0.004). In a small randomized pilot study of 57patients allocated to warfarin or placebo in addition to ASA,less evidence was noted of angiographic progression in theculprit lesion after 10 weeks of treatment with warfarin(33% for placebo vs. 4% for warfarin) and more regressionwas observed (229). The OASIS pilot study (230) compareda fixed dosage of 3 mg/d coumadin or a moderate dosetitrated to an INR of 2 to 2.5 in 197 patients for 7 monthsafter the acute phase. Low-intensity warfarin had no ben-efit, whereas the moderate-intensity regimen reduced therisk of death, MI, or refractory angina by 58% and the needfor rehospitalization for UA by 58%. However, these resultswere not reproduced in the larger OASIS 2 trial (228) of3,712 patients randomized to the moderate-intensity regi-men of warfarin or standard therapy, with all patientsreceiving ASA. The rate of cardiovascular death, MI, orstroke after 5 months was 7.65% with the anticoagulant and8.4% without (p 5 0.37) (231). Thus, the role, if any, oflong-term warfarin in patients with UA/NSTEMI remainsto be defined.
The Coumadin Aspirin Reinfarction Study (CARS)conducted in post MI patients was discontinued prema-turely due to a lack of evidence of benefit of reduced-doseASA (80 mg/d) with either 1 or 3 mg warfarin dailycompared with 160 mg/d ASA alone (232). The Combi-nation Hemotherapy And Mortality Prevention (CHAMP)study found no benefit of the use of warfarin (to an INR of1.5 to 2.5) plus 81 mg/d ASA vs. 162 mg/d ASA withrespect to total mortality, cardiovascular mortality, stroke,and nonfatal MI (mean follow-up of 2.7 years) after anindex AMI (233). Low- or moderate-intensity anticoagu-lation with fixed-dose warfarin is not recommended forroutine use after hospitalization for UA/NSTEMI. Warfa-rin should be prescribed, however, for UA/NSTEMI pa-tients with established indications for warfarin, such as atrialfibrillation and mechanical prosthetic heart valves.
3. Platelet GP IIb/IIIa Receptor Antagonists. The GPIIb/IIIa receptor (aIIbb3 integrin) is abundant on theplatelet surface. When platelets are activated, this receptorundergoes a change in configuration that increases itsaffinity for binding to fibrinogen and other ligands. Thebinding of molecules of fibrinogen to receptors on differentplatelets results in platelet aggregation. This mechanism isindependent of the stimulus for platelet aggregation andrepresents the final and obligatory pathway for plateletaggregation (234). The platelet GP IIb/IIIa receptor antag-onists act by occupying the receptors, preventing fibrinogen
binding, and thereby preventing platelet aggregation. Ex-perimental and clinical studies have suggested that occu-pancy of $80% of the receptor population and inhibition ofplatelet aggregation to ADP (5 to 20 mmol/L) by $80%results in potent antithrombotic effects (235). The variousGP IIb/IIIa antagonists, however, possess significantly dif-ferent pharmacokinetic and pharmacodynamic properties(236).
Abciximab is a Fab fragment of a humanized murineantibody that has a short plasma half-life but strong affinityfor the receptor, resulting in some receptor occupancy thatpersists for weeks. Platelet aggregation gradually returns tonormal 24 to 48 h after discontinuation of the drug.Furthermore, abciximab is not specific for GP IIb/IIIa andinhibits the vitronectin receptor (anb3) on endothelial cellsand the MAC-1 receptor on leukocytes (237,238). Theclinical relevance of occupancy of these receptors is notpresently known.
Eptifibatide is a cyclic heptapeptide that contains theKGD (Lys-Gly-Asp) sequence; tirofiban and lamifiban (adrug that is not yet approved) are nonpeptide mimetics ofthe RGD (Arg-Gly-Asp) sequence of fibrinogen (236,239–241). Receptor occupancy with these 3 synthetic antagonistsis in general in equilibrium with plasma levels. They have ahalf-life of 2 to 3 h and are highly specific for the GPIIb/IIIa receptor, with no effect on the vitronectin receptor(avb3 integrin). Thus, the median percent inhibition ofplatelet aggregation to 5 mmol/L ADP achieved after aloading dose of 0.4 mgzkg21zmin21 of tirofiban for 30 minis 86%, and the inhibition is sustained with an infusion of0.1 mgzkg21zmin21. A higher dose of 10 mg/kg over 3 minfollowed by an infusion of 0.15 mgzkg21zmin21 achieves90% inhibition within 5 min. Platelet aggregation returns tonormal in 4 to 8 h after discontinuation of the drug, afinding that is consistent with the relatively short half-life ofthe drug (242). GP IIb/IIIa antagonists may bind differentsites on the receptor and result in somewhat differentbinding properties that may modify their platelet effects andpotentially, paradoxically, activate the receptor (243). Oralantagonists to the receptor are currently under investigation,although these programs have been slowed by the afore-mentioned negative results of 4 large trials of 3 of thesecompounds (193,193a,193b).
The efficacy of GP IIb/IIIa antagonists in prevention ofthe complications associated with percutaneous interven-tions has been documented in numerous trials, many ofthem composed totally or largely of patients with UA(182,244–246) (see Figs. 13 and 14 in Section IV). Twotrials with tirofiban and 1 trial with eptifibatide have alsodocumented their efficacy in UA/NSTEMI patients, onlysome of whom underwent interventions (10,21). A trial hasbeen completed with lamifiban (183), and one is ongoingwith abciximab. Because the various agents have not beencompared directly with each other, their relative efficacy isnot known.
Abciximab has been studied primarily in PCI trials, in
1007JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
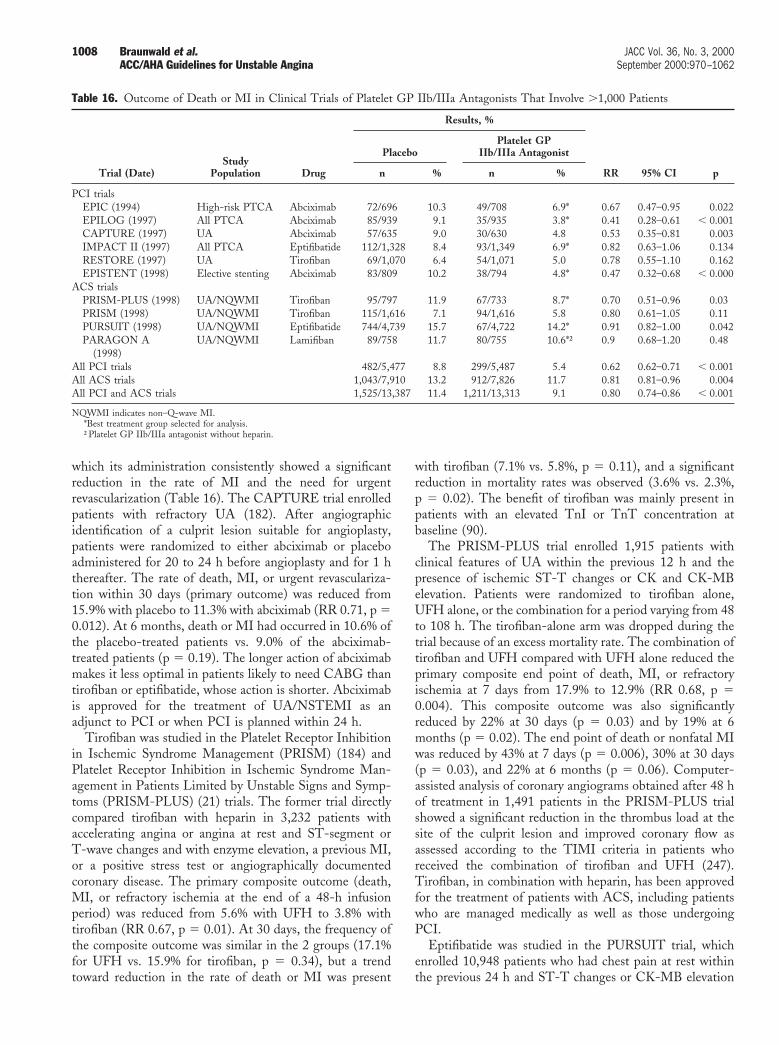
which its administration consistently showed a significantreduction in the rate of MI and the need for urgentrevascularization (Table 16). The CAPTURE trial enrolledpatients with refractory UA (182). After angiographicidentification of a culprit lesion suitable for angioplasty,patients were randomized to either abciximab or placeboadministered for 20 to 24 h before angioplasty and for 1 hthereafter. The rate of death, MI, or urgent revasculariza-tion within 30 days (primary outcome) was reduced from15.9% with placebo to 11.3% with abciximab (RR 0.71, p 50.012). At 6 months, death or MI had occurred in 10.6% ofthe placebo-treated patients vs. 9.0% of the abciximab-treated patients (p 5 0.19). The longer action of abciximabmakes it less optimal in patients likely to need CABG thantirofiban or eptifibatide, whose action is shorter. Abciximabis approved for the treatment of UA/NSTEMI as anadjunct to PCI or when PCI is planned within 24 h.
Tirofiban was studied in the Platelet Receptor Inhibitionin Ischemic Syndrome Management (PRISM) (184) andPlatelet Receptor Inhibition in Ischemic Syndrome Man-agement in Patients Limited by Unstable Signs and Symp-toms (PRISM-PLUS) (21) trials. The former trial directlycompared tirofiban with heparin in 3,232 patients withaccelerating angina or angina at rest and ST-segment orT-wave changes and with enzyme elevation, a previous MI,or a positive stress test or angiographically documentedcoronary disease. The primary composite outcome (death,MI, or refractory ischemia at the end of a 48-h infusionperiod) was reduced from 5.6% with UFH to 3.8% withtirofiban (RR 0.67, p 5 0.01). At 30 days, the frequency ofthe composite outcome was similar in the 2 groups (17.1%for UFH vs. 15.9% for tirofiban, p 5 0.34), but a trendtoward reduction in the rate of death or MI was present
with tirofiban (7.1% vs. 5.8%, p 5 0.11), and a significantreduction in mortality rates was observed (3.6% vs. 2.3%,p 5 0.02). The benefit of tirofiban was mainly present inpatients with an elevated TnI or TnT concentration atbaseline (90).
The PRISM-PLUS trial enrolled 1,915 patients withclinical features of UA within the previous 12 h and thepresence of ischemic ST-T changes or CK and CK-MBelevation. Patients were randomized to tirofiban alone,UFH alone, or the combination for a period varying from 48to 108 h. The tirofiban-alone arm was dropped during thetrial because of an excess mortality rate. The combination oftirofiban and UFH compared with UFH alone reduced theprimary composite end point of death, MI, or refractoryischemia at 7 days from 17.9% to 12.9% (RR 0.68, p 50.004). This composite outcome was also significantlyreduced by 22% at 30 days (p 5 0.03) and by 19% at 6months (p 5 0.02). The end point of death or nonfatal MIwas reduced by 43% at 7 days (p 5 0.006), 30% at 30 days(p 5 0.03), and 22% at 6 months (p 5 0.06). Computer-assisted analysis of coronary angiograms obtained after 48 hof treatment in 1,491 patients in the PRISM-PLUS trialshowed a significant reduction in the thrombus load at thesite of the culprit lesion and improved coronary flow asassessed according to the TIMI criteria in patients whoreceived the combination of tirofiban and UFH (247).Tirofiban, in combination with heparin, has been approvedfor the treatment of patients with ACS, including patientswho are managed medically as well as those undergoingPCI.
Eptifibatide was studied in the PURSUIT trial, whichenrolled 10,948 patients who had chest pain at rest withinthe previous 24 h and ST-T changes or CK-MB elevation
Table 16. Outcome of Death or MI in Clinical Trials of Platelet GP IIb/IIIa Antagonists That Involve .1,000 Patients
Trial (Date)Study
Population Drug
Results, %
RR 95% CI p
PlaceboPlatelet GP
IIb/IIIa Antagonist
n % n %
PCI trialsEPIC (1994) High-risk PTCA Abciximab 72/696 10.3 49/708 6.9* 0.67 0.47–0.95 0.022EPILOG (1997) All PTCA Abciximab 85/939 9.1 35/935 3.8* 0.41 0.28–0.61 , 0.001CAPTURE (1997) UA Abciximab 57/635 9.0 30/630 4.8 0.53 0.35–0.81 0.003IMPACT II (1997) All PTCA Eptifibatide 112/1,328 8.4 93/1,349 6.9* 0.82 0.63–1.06 0.134RESTORE (1997) UA Tirofiban 69/1,070 6.4 54/1,071 5.0 0.78 0.55–1.10 0.162EPISTENT (1998) Elective stenting Abciximab 83/809 10.2 38/794 4.8* 0.47 0.32–0.68 , 0.000
ACS trialsPRISM-PLUS (1998) UA/NQWMI Tirofiban 95/797 11.9 67/733 8.7* 0.70 0.51–0.96 0.03PRISM (1998) UA/NQWMI Tirofiban 115/1,616 7.1 94/1,616 5.8 0.80 0.61–1.05 0.11PURSUIT (1998) UA/NQWMI Eptifibatide 744/4,739 15.7 67/4,722 14.2* 0.91 0.82–1.00 0.042PARAGON A
(1998)UA/NQWMI Lamifiban 89/758 11.7 80/755 10.6*† 0.9 0.68–1.20 0.48
All PCI trials 482/5,477 8.8 299/5,487 5.4 0.62 0.62–0.71 , 0.001All ACS trials 1,043/7,910 13.2 912/7,826 11.7 0.81 0.81–0.96 0.004All PCI and ACS trials 1,525/13,387 11.4 1,211/13,313 9.1 0.80 0.74–0.86 , 0.001
NQWMI indicates non–Q-wave MI.*Best treatment group selected for analysis.†Platelet GP IIb/IIIa antagonist without heparin.
1008 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
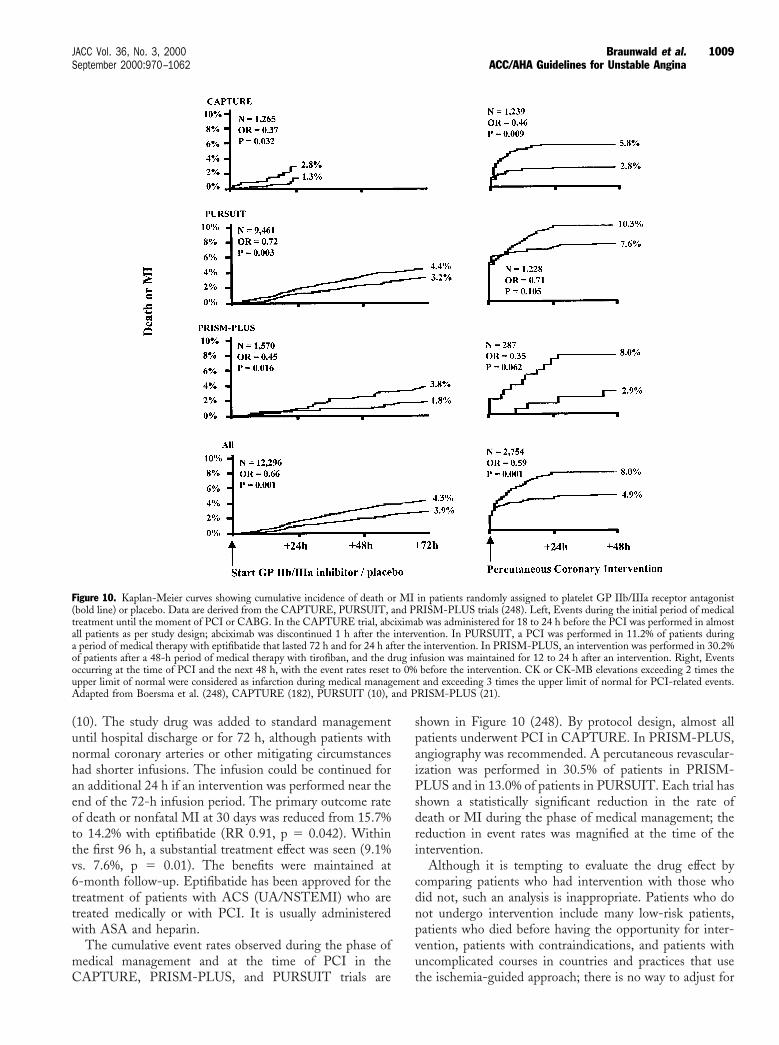
(10). The study drug was added to standard managementuntil hospital discharge or for 72 h, although patients withnormal coronary arteries or other mitigating circumstanceshad shorter infusions. The infusion could be continued foran additional 24 h if an intervention was performed near theend of the 72-h infusion period. The primary outcome rateof death or nonfatal MI at 30 days was reduced from 15.7%to 14.2% with eptifibatide (RR 0.91, p 5 0.042). Withinthe first 96 h, a substantial treatment effect was seen (9.1%vs. 7.6%, p 5 0.01). The benefits were maintained at6-month follow-up. Eptifibatide has been approved for thetreatment of patients with ACS (UA/NSTEMI) who aretreated medically or with PCI. It is usually administeredwith ASA and heparin.
The cumulative event rates observed during the phase ofmedical management and at the time of PCI in theCAPTURE, PRISM-PLUS, and PURSUIT trials are
shown in Figure 10 (248). By protocol design, almost allpatients underwent PCI in CAPTURE. In PRISM-PLUS,angiography was recommended. A percutaneous revascular-ization was performed in 30.5% of patients in PRISM-PLUS and in 13.0% of patients in PURSUIT. Each trial hasshown a statistically significant reduction in the rate ofdeath or MI during the phase of medical management; thereduction in event rates was magnified at the time of theintervention.
Although it is tempting to evaluate the drug effect bycomparing patients who had intervention with those whodid not, such an analysis is inappropriate. Patients who donot undergo intervention include many low-risk patients,patients who died before having the opportunity for inter-vention, patients with contraindications, and patients withuncomplicated courses in countries and practices that usethe ischemia-guided approach; there is no way to adjust for
Figure 10. Kaplan-Meier curves showing cumulative incidence of death or MI in patients randomly assigned to platelet GP IIb/IIIa receptor antagonist(bold line) or placebo. Data are derived from the CAPTURE, PURSUIT, and PRISM-PLUS trials (248). Left, Events during the initial period of medicaltreatment until the moment of PCI or CABG. In the CAPTURE trial, abciximab was administered for 18 to 24 h before the PCI was performed in almostall patients as per study design; abciximab was discontinued 1 h after the intervention. In PURSUIT, a PCI was performed in 11.2% of patients duringa period of medical therapy with eptifibatide that lasted 72 h and for 24 h after the intervention. In PRISM-PLUS, an intervention was performed in 30.2%of patients after a 48-h period of medical therapy with tirofiban, and the drug infusion was maintained for 12 to 24 h after an intervention. Right, Eventsoccurring at the time of PCI and the next 48 h, with the event rates reset to 0% before the intervention. CK or CK-MB elevations exceeding 2 times theupper limit of normal were considered as infarction during medical management and exceeding 3 times the upper limit of normal for PCI-related events.Adapted from Boersma et al. (248), CAPTURE (182), PURSUIT (10), and PRISM-PLUS (21).
1009JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
these imbalances. Accordingly, the analysis in Fig. 10includes the event rates for all patients during the time whenthey were treated medically. It then begins the analysis anewin patients who underwent PCI at the time of angiographywhile on drug or placebo. When the trials are combined, themessage is compelling: the GP IIb/IIIa inhibitors areeffective in reducing event rates in the acute phase ofmedical management of UA/NSTEMI, and this effect ismagnified if a PCI is performed. Therefore, it is recom-mended that a GP IIb/IIIa inhibitor be administered, alongwith ASA and UFH, to patients with UA/NSTEMI withactive ischemia or with any of the high-risk features shownin Table 6.
Although there is a temptation to use the comparison ofeach of these GP IIb/IIIa inhibitors with placebo to drawconclusions about relative efficacy, such an exercise could bemisleading. Each trial had different entry criteria, differentapproaches to angiographic evaluation, and different criteriafor end point measurement and took place in differentlocations in different time periods. The effects of thesedifferences cannot be accounted for in an indirect compar-ison. Head-to-head (direct) comparisons will be required todraw reliable conclusions about the relative efficacy of thesedifferent molecules.
Treatment with a GP IIb/IIIa antagonist increases therisk of bleeding, which is typically mucocutaneous or in-volves the access site of vascular intervention. Unfortunately,each trial also used a different definition of bleeding andreported differently with regard to bleeding related toCABG. In the PRISM trial with no interventions ontreatment, major bleeding (excluding CABG) occurred in0.4% of patients who received tirofiban and 0.4% of patientswho received UFH. In the PRISM-PLUS trial, majorbleeding according to the TIMI criteria was reported in1.4% of patients who received tirofiban and 0.8% of patientswho received placebo (p 5 0.23), whereas PURSUITreported major bleeding in 10.6% of patients who receivedeptifibatide and 9.1% of patients who received placebo (p 50.02). In the PURSUIT trial, with the exclusion of patientswho underwent CABG, the rates were 3.0% with eptifi-batide and 1.3% with placebo (p , 0.001). No trials haveshown an excess of intracranial bleeding with a GP IIb/IIIainhibitor. As with the efficacy data, the temptation to makeindirect comparisons should be tempered by the variabilityin protocol, circumstances, and definitions of the trial.
ASA has been used with the intravenous GP IIb/IIIareceptor blockers in all trials. A strong case can also be madefor the concomitant use of heparin with GP IIb/IIIareceptor blockers. The tirofiban arm without UFH in thePRISM-PLUS trial was discontinued early because of anexcess of deaths. In addition, the PURSUIT trial reported ahigher event rate in the 11% of patients who were nottreated with concomitant heparin (10). Current recommen-dations call for the concomitant use of heparin with GPIIb/IIIa inhibitors. It should be noted that an interactionexists between heparin and GP IIb/IIIa inhibitors with a
higher ACT for the combination and a need for lower dosesof heparin than usually recommended to achieve the bestoutcomes in the setting of PCI. Information is currentlybeing gained concerning the safety and efficacy of thecombination of LMWH and GP IIb/IIIa inhibitors.
Blood hemoglobin and platelet counts should be moni-tored and patient surveillance for bleeding should be carriedout daily during the administration of GP IIb/IIIa receptorblockers. Thrombocytopenia is an unusual complication ofthis class of agents. Severe thrombocytopenia defined bynadir platelet counts of ,50,000 mL21 is observed in 0.5%of patients, and profound thrombocytopenia defined bynadir platelet counts of ,20,000 mL21 is observed in 0.2%of patients. Although reversible, thrombocytopenia is asso-ciated with an increased risk of bleeding (249,250).
Thrombolysis
The failure of intravenous thrombolytic therapy to im-prove clinical outcomes in the absence of AMI withST-segment elevation or bundle-branch block was clearlydemonstrated in the TIMI IIIB, ISIS-2, and GruppoItaliano per lo Studio della Sopravvivenza nell’Infarto-1(GISSI) 1 trials (19,251,252). A meta-analysis of thrombo-lytic therapy in UA patients showed no benefit of throm-bolysis vs. standard therapy for the reduction of AMI (19).Thrombolytic agents had no significant beneficial effect andactually increased the risk of MI (19). Consequently, suchtherapy is not recommended for the management of pa-tients with an ACS without ST-segment elevation, aposterior wall MI, or a presumably new LBBB (see ACC/AHA Guidelines for the Management of Patients WithAcute Myocardial Infarction [5]).
C. Risk Stratification
Recommendations
Class I1. Noninvasive stress testing in low-risk patients (Ta-
ble 6) who have been free of ischemia at rest or withlow-level activity and of CHF for a minimum of 12to 24 h. (Level of Evidence: C)
2. Noninvasive stress testing in patients at intermedi-ate risk (Table 6) who have been free of ischemia atrest or with low-level activity and of CHF for aminimum of 2 or 3 days. (Level of Evidence: C)
3. Choice of stress test is based on the resting ECG,ability to perform exercise, local expertise, andtechnologies available. Treadmill exercise is suit-able in patients able to exercise in whom the ECGis free of baseline ST-segment abnormalities,bundle-branch block, LV hypertrophy, intraven-tricular conduction defect, paced rhythm, preexci-tation, and digoxin effect. (Level of Evidence: C)
4. An imaging modality is added in patients withresting ST-segment depression (>0.10 mV), LVhypertrophy, bundle-branch block, intraventricular
1010 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
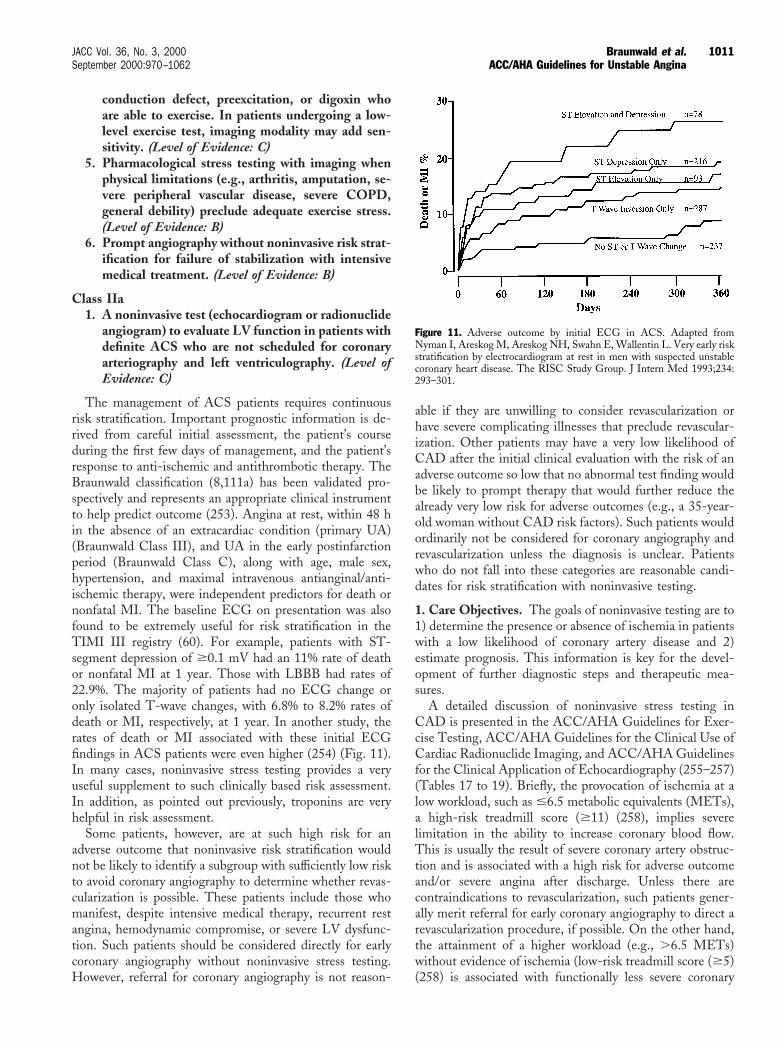
conduction defect, preexcitation, or digoxin whoare able to exercise. In patients undergoing a low-level exercise test, imaging modality may add sen-sitivity. (Level of Evidence: C)
5. Pharmacological stress testing with imaging whenphysical limitations (e.g., arthritis, amputation, se-vere peripheral vascular disease, severe COPD,general debility) preclude adequate exercise stress.(Level of Evidence: B)
6. Prompt angiography without noninvasive risk strat-ification for failure of stabilization with intensivemedical treatment. (Level of Evidence: B)
Class IIa1. A noninvasive test (echocardiogram or radionuclide
angiogram) to evaluate LV function in patients withdefinite ACS who are not scheduled for coronaryarteriography and left ventriculography. (Level ofEvidence: C)
The management of ACS patients requires continuousrisk stratification. Important prognostic information is de-rived from careful initial assessment, the patient’s courseduring the first few days of management, and the patient’sresponse to anti-ischemic and antithrombotic therapy. TheBraunwald classification (8,111a) has been validated pro-spectively and represents an appropriate clinical instrumentto help predict outcome (253). Angina at rest, within 48 hin the absence of an extracardiac condition (primary UA)(Braunwald Class III), and UA in the early postinfarctionperiod (Braunwald Class C), along with age, male sex,hypertension, and maximal intravenous antianginal/anti-ischemic therapy, were independent predictors for death ornonfatal MI. The baseline ECG on presentation was alsofound to be extremely useful for risk stratification in theTIMI III registry (60). For example, patients with ST-segment depression of $0.1 mV had an 11% rate of deathor nonfatal MI at 1 year. Those with LBBB had rates of22.9%. The majority of patients had no ECG change oronly isolated T-wave changes, with 6.8% to 8.2% rates ofdeath or MI, respectively, at 1 year. In another study, therates of death or MI associated with these initial ECGfindings in ACS patients were even higher (254) (Fig. 11).In many cases, noninvasive stress testing provides a veryuseful supplement to such clinically based risk assessment.In addition, as pointed out previously, troponins are veryhelpful in risk assessment.
Some patients, however, are at such high risk for anadverse outcome that noninvasive risk stratification wouldnot be likely to identify a subgroup with sufficiently low riskto avoid coronary angiography to determine whether revas-cularization is possible. These patients include those whomanifest, despite intensive medical therapy, recurrent restangina, hemodynamic compromise, or severe LV dysfunc-tion. Such patients should be considered directly for earlycoronary angiography without noninvasive stress testing.However, referral for coronary angiography is not reason-
able if they are unwilling to consider revascularization orhave severe complicating illnesses that preclude revascular-ization. Other patients may have a very low likelihood ofCAD after the initial clinical evaluation with the risk of anadverse outcome so low that no abnormal test finding wouldbe likely to prompt therapy that would further reduce thealready very low risk for adverse outcomes (e.g., a 35-year-old woman without CAD risk factors). Such patients wouldordinarily not be considered for coronary angiography andrevascularization unless the diagnosis is unclear. Patientswho do not fall into these categories are reasonable candi-dates for risk stratification with noninvasive testing.
1. Care Objectives. The goals of noninvasive testing are to1) determine the presence or absence of ischemia in patientswith a low likelihood of coronary artery disease and 2)estimate prognosis. This information is key for the devel-opment of further diagnostic steps and therapeutic mea-sures.
A detailed discussion of noninvasive stress testing inCAD is presented in the ACC/AHA Guidelines for Exer-cise Testing, ACC/AHA Guidelines for the Clinical Use ofCardiac Radionuclide Imaging, and ACC/AHA Guidelinesfor the Clinical Application of Echocardiography (255–257)(Tables 17 to 19). Briefly, the provocation of ischemia at alow workload, such as #6.5 metabolic equivalents (METs),a high-risk treadmill score ($11) (258), implies severelimitation in the ability to increase coronary blood flow.This is usually the result of severe coronary artery obstruc-tion and is associated with a high risk for adverse outcomeand/or severe angina after discharge. Unless there arecontraindications to revascularization, such patients gener-ally merit referral for early coronary angiography to direct arevascularization procedure, if possible. On the other hand,the attainment of a higher workload (e.g., .6.5 METs)without evidence of ischemia (low-risk treadmill score ($5)(258) is associated with functionally less severe coronary
Figure 11. Adverse outcome by initial ECG in ACS. Adapted fromNyman I, Areskog M, Areskog NH, Swahn E, Wallentin L. Very early riskstratification by electrocardiogram at rest in men with suspected unstablecoronary heart disease. The RISC Study Group. J Intern Med 1993;234:293–301.
1011JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
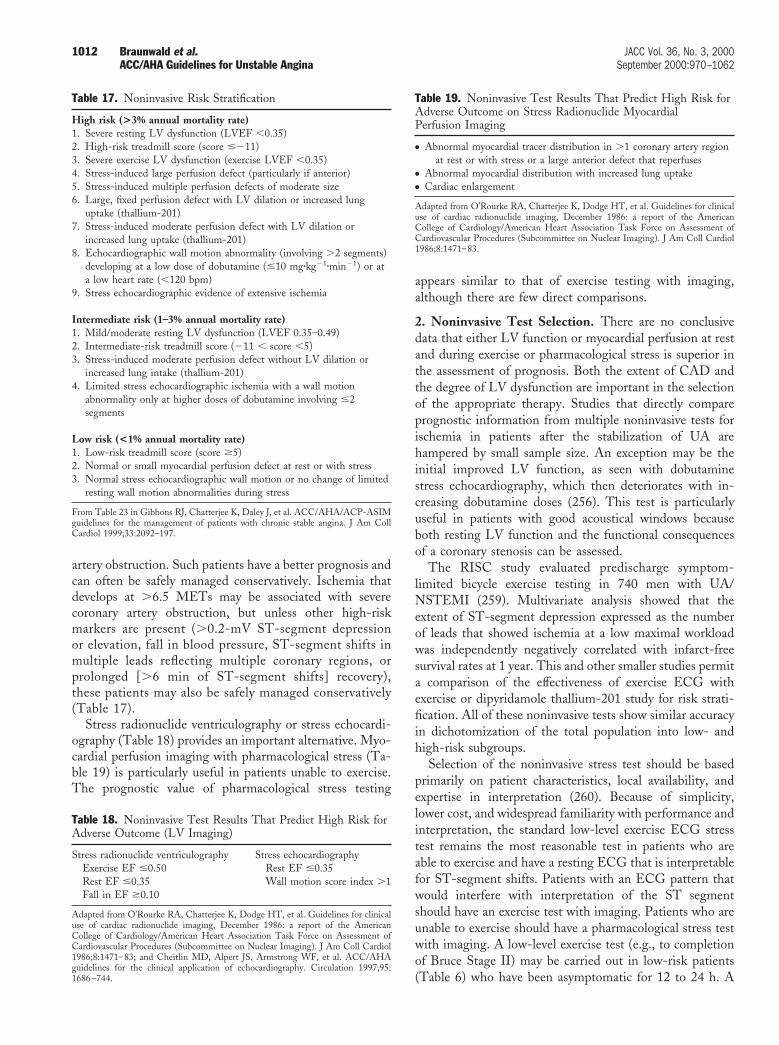
artery obstruction. Such patients have a better prognosis andcan often be safely managed conservatively. Ischemia thatdevelops at .6.5 METs may be associated with severecoronary artery obstruction, but unless other high-riskmarkers are present (.0.2-mV ST-segment depressionor elevation, fall in blood pressure, ST-segment shifts inmultiple leads reflecting multiple coronary regions, orprolonged [.6 min of ST-segment shifts] recovery),these patients may also be safely managed conservatively(Table 17).
Stress radionuclide ventriculography or stress echocardi-ography (Table 18) provides an important alternative. Myo-cardial perfusion imaging with pharmacological stress (Ta-ble 19) is particularly useful in patients unable to exercise.The prognostic value of pharmacological stress testing
appears similar to that of exercise testing with imaging,although there are few direct comparisons.
2. Noninvasive Test Selection. There are no conclusivedata that either LV function or myocardial perfusion at restand during exercise or pharmacological stress is superior inthe assessment of prognosis. Both the extent of CAD andthe degree of LV dysfunction are important in the selectionof the appropriate therapy. Studies that directly compareprognostic information from multiple noninvasive tests forischemia in patients after the stabilization of UA arehampered by small sample size. An exception may be theinitial improved LV function, as seen with dobutaminestress echocardiography, which then deteriorates with in-creasing dobutamine doses (256). This test is particularlyuseful in patients with good acoustical windows becauseboth resting LV function and the functional consequencesof a coronary stenosis can be assessed.
The RISC study evaluated predischarge symptom-limited bicycle exercise testing in 740 men with UA/NSTEMI (259). Multivariate analysis showed that theextent of ST-segment depression expressed as the numberof leads that showed ischemia at a low maximal workloadwas independently negatively correlated with infarct-freesurvival rates at 1 year. This and other smaller studies permita comparison of the effectiveness of exercise ECG withexercise or dipyridamole thallium-201 study for risk strati-fication. All of these noninvasive tests show similar accuracyin dichotomization of the total population into low- andhigh-risk subgroups.
Selection of the noninvasive stress test should be basedprimarily on patient characteristics, local availability, andexpertise in interpretation (260). Because of simplicity,lower cost, and widespread familiarity with performance andinterpretation, the standard low-level exercise ECG stresstest remains the most reasonable test in patients who areable to exercise and have a resting ECG that is interpretablefor ST-segment shifts. Patients with an ECG pattern thatwould interfere with interpretation of the ST segmentshould have an exercise test with imaging. Patients who areunable to exercise should have a pharmacological stress testwith imaging. A low-level exercise test (e.g., to completionof Bruce Stage II) may be carried out in low-risk patients(Table 6) who have been asymptomatic for 12 to 24 h. A
Table 18. Noninvasive Test Results That Predict High Risk forAdverse Outcome (LV Imaging)
Stress radionuclide ventriculography Stress echocardiographyExercise EF #0.50 Rest EF #0.35Rest EF #0.35 Wall motion score index .1Fall in EF $0.10
Adapted from O’Rourke RA, Chatterjee K, Dodge HT, et al. Guidelines for clinicaluse of cardiac radionuclide imaging, December 1986: a report of the AmericanCollege of Cardiology/American Heart Association Task Force on Assessment ofCardiovascular Procedures (Subcommittee on Nuclear Imaging). J Am Coll Cardiol1986;8:1471–83; and Cheitlin MD, Alpert JS, Armstrong WF, et al. ACC/AHAguidelines for the clinical application of echocardiography. Circulation 1997;95:1686–744.
Table 19. Noninvasive Test Results That Predict High Risk forAdverse Outcome on Stress Radionuclide MyocardialPerfusion Imaging
● Abnormal myocardial tracer distribution in .1 coronary artery regionat rest or with stress or a large anterior defect that reperfuses
● Abnormal myocardial distribution with increased lung uptake● Cardiac enlargement
Adapted from O’Rourke RA, Chatterjee K, Dodge HT, et al. Guidelines for clinicaluse of cardiac radionuclide imaging, December 1986: a report of the AmericanCollege of Cardiology/American Heart Association Task Force on Assessment ofCardiovascular Procedures (Subcommittee on Nuclear Imaging). J Am Coll Cardiol1986;8:1471–83.
Table 17. Noninvasive Risk Stratification
High risk (>3% annual mortality rate)1. Severe resting LV dysfunction (LVEF ,0.35)2. High-risk treadmill score (score #211)3. Severe exercise LV dysfunction (exercise LVEF ,0.35)4. Stress-induced large perfusion defect (particularly if anterior)5. Stress-induced multiple perfusion defects of moderate size6. Large, fixed perfusion defect with LV dilation or increased lung
uptake (thallium-201)7. Stress-induced moderate perfusion defect with LV dilation or
increased lung uptake (thallium-201)8. Echocardiographic wall motion abnormality (involving .2 segments)
developing at a low dose of dobutamine (#10 mgzkg21zmin21) or ata low heart rate (,120 bpm)
9. Stress echocardiographic evidence of extensive ischemia
Intermediate risk (1–3% annual mortality rate)1. Mild/moderate resting LV dysfunction (LVEF 0.35–0.49)2. Intermediate-risk treadmill score (211 , score ,5)3. Stress-induced moderate perfusion defect without LV dilation or
increased lung intake (thallium-201)4. Limited stress echocardiographic ischemia with a wall motion
abnormality only at higher doses of dobutamine involving #2segments
Low risk (<1% annual mortality rate)1. Low-risk treadmill score (score $5)2. Normal or small myocardial perfusion defect at rest or with stress3. Normal stress echocardiographic wall motion or no change of limited
resting wall motion abnormalities during stress
From Table 23 in Gibbons RJ, Chatterjee K, Daley J, et al. ACC/AHA/ACP-ASIMguidelines for the management of patients with chronic stable angina. J Am CollCardiol 1999;33:2092–197.
1012 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062

symptom-limited test can be conducted in patients withoutevidence of ischemia for 7 to 10 days.
The optimal testing strategy in women remains less welldefined than that in men (see Section VI. A), but there isevidence that imaging studies are superior to exercise ECGin women (260,261). Exercise testing has been reported tobe less accurate for diagnosis in women. At least a portionof the lower reported accuracy derives from a lower pretestlikelihood of CAD in women compared with men.
Results of a symptom-limited exercise test performed 3 to7 days after UA/NSTEMI were compared with results of atest conducted 1 month later in 189 patients (262). Thediagnostic and prognostic values of the tests were similar,but the earlier test identified patients who developed adverseevents during the first month, and this represented aboutone half of all events that occurred during the first year.These data illustrate the importance of early noninvasivetesting for risk stratification.
The Veterans Affairs Non–Q-Wave Infarction Strategiesin Hospital (VANQWISH) trial used symptom-limitedthallium exercise treadmill testing at 3 to 5 days to direct theneed for angiography in the 442 non–Q-wave MI patientsrandomized to an early conservative strategy (263). Thisstrategy included an effort to detect ischemia with nonin-vasive testing that would be associated with a high risk foradverse outcome. Cumulative death rates in the 238 con-servative strategy patients directed to angiography on thebasis of recurrent ischemia or high-risk stress test resultswere 3%, 10%, and 13% at 1, 6, and 12 months, respectively,whereas the rates were 1%, 3%, and 6% in the patients whowere not directed to angiography (no recurrent ischemia orhigh-risk test). These findings support the concept thatnoninvasive stress testing can be used successfully to identifya high-risk subset of patients who could be directed tocoronary angiography. It is unlikely that any angiographi-cally directed early revascularization strategy could alter thevery low early event rates observed in patients without ahigh-risk stress test.
Noninvasive tests are most useful for management deci-sions when risk can be stated in terms of events over time.A large population of patients must be studied to derive andtest equations needed to accurately predict individual pa-tient risk. No noninvasive study has been reported in asufficient number of patients after the stabilization of UA todevelop and test the accuracy of a multivariable equation toreport test results in terms of absolute risk. Therefore, datafrom studies of stable angina patients must be used for riskreported as events over time. Although the pathologicalprocess that evokes ischemia may be different in the 2 formsof angina, it is likely that the use of prognostic nomogramsderived from patients with stable angina are also predictiveof risk in patients with recent UA after stabilization. Withthis untested assumption, the much larger literature derivedfrom populations that include patients with both stableangina and UA provides equations for risk stratification that
convert physiological changes observed during noninvasivetesting into statements of risk expressed as events over time.
3. Selection for Coronary Angiography. In contrast to thenoninvasive tests, coronary angiography provides detailedstructural information to allow an assessment of prognosisand to provide direction for appropriate management.When combined with LV angiography, it also allows anassessment of global and regional LV function. Indicationsfor coronary angiography are interwoven with indicationsfor possible therapeutic plans such as PCI or CABG. Therecently revised ACC/AHA Guidelines for Coronary An-giography present greater details on this subject (264).
Coronary angiography is usually indicated in patientswith UA/NSTEMI who either have recurrent symptoms orischemia despite adequate medical therapy or are at highrisk categorized by clinical findings (CHF, malignant ven-tricular arrhythmias) or noninvasive test findings (significantLV dysfunction: ejection fraction [EF] ,0.35, large anterioror multiple perfusion defects) (Tables 17 to 19), as discussedin Section III. B. Patients with UA who have had previousPCI or CABG should also in general be considered for earlycoronary angiography, unless prior coronary angiographydata indicate that no further revascularization is likely to bepossible. The placement of an IABP may be useful inpatients with recurrent ischemia despite maximal medicalmanagement as well as in those with hemodynamic insta-bility until coronary angiography and revascularization canbe completed. Patients with suspected Prinzmetal’s variantangina are also candidates for coronary angiography (seeSection VI. F).
In all cases, the general indications for coronary angiog-raphy and revascularization are tempered by individualpatient characteristics and preferences. Patient and physi-cian judgments regarding risks and benefits are particularlyimportant for patients who may not be candidates forcoronary revascularization, such as very frail elderly personsand those with serious comorbid conditions (i.e., severehepatic, pulmonary, or renal failure; active or inoperablecancer).
4. Patient Counseling. Results of testing should be dis-cussed with the patient, his or her family, and/or his or heradvocate in language that is understood. Test results shouldbe used to help determine the advisability of coronaryangiography, the need for adjustments in the medicalregimen, and the need for secondary prevention measures(see Section V).
D. Early Conservative Versus Invasive Strategies
1. General Principles. Two different treatment strategies,termed “early conservative” and “early invasive,” haveevolved for patients with UA/NSTEMI. In the early con-servative strategy, coronary angiography is reserved forpatients with evidence of recurrent ischemia (angina at restor with minimal activity or dynamic ST-segment changes)or a strongly positive stress test, despite vigorous medical
1013JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
therapy. In the early invasive strategy, patients withoutclinically obvious contraindications to coronary revascular-ization are routinely recommended for coronary angiogra-phy and angiographically directed revascularization if pos-sible.
Recommendations
Class I1. An early invasive strategy in patients with UA/
NSTEMI and any of the following high-risk indi-cators. (Level of Evidence: B):a) Patients with recurrent angina/ischemia at rest
or with low-level activities despite intensiveanti-ischemic therapy
b) Recurrent angina/ischemia with CHF symp-toms, an S3 gallop, pulmonary edema, worsen-ing rales, or new or worsening MR
c) High-risk findings on noninvasive stress testingd) Depressed LV systolic function (e.g., EF <0.40
on noninvasive study)e) Hemodynamic instabilityf) Sustained ventricular tachycardiag) PCI within 6 monthsh) Prior CABG
2. In the absence of these findings, either an earlyconservative or an early invasive strategy in hospi-talized patients without contraindications for revas-cularization. (Level of Evidence: B)
Class IIa1. An early invasive strategy in patients with repeated
presentations for ACS despite therapy and withoutevidence for ongoing ischemia or high risk. (Levelof Evidence: C)
2. An early invasive strategy in patients >65 years oldor patients who present with ST-segment depres-sion or elevated cardiac markers and no contrain-dications to revascularization. (Level of Evidence: C)
Class III1. Coronary angiography in patients with extensive
comorbidities (e.g., liver or pulmonary failure, can-cer), in whom the risks of revascularization are notlikely to outweigh the benefits. (Level of Evidence:C)
2. Coronary angiography in patients with acute chestpain and a low likelihood of ACS. (Level ofEvidence: C)
3. Coronary angiography in patients who will notconsent to revascularization regardless of the find-ings. (Level of Evidence: C)
Rationale for the Early Conservative StrategyThree multicenter trials have shown similar outcomes
with early conservative and early invasive therapeutic strat-egies (19,265,266). The conservative strategy spares the useof invasive procedures with their risks and costs in all
patients. Recent trials (266,267) have emphasized the earlyrisk associated with revascularization procedures. When theearly conservative strategy is chosen, a plan for noninvasiveevaluation is required to detect severe ischemia that occursspontaneously or at a low threshold of stress and topromptly refer these patients for coronary angiography andrevascularization when possible. In addition, as in STEMI(268), an early echocardiogram should be considered toidentify patients with significant LV dysfunction (e.g., EF,0.40). Such a finding prompts consideration for angiog-raphy to identify left main or multivessel CAD, becausepatients with multivessel disease and LV dysfunction are athigh risk and may accrue a survival benefit from bypasssurgery (269,270). In addition, a stress test (e.g., exercise orpharmacological stress) for the assessment of ischemia isrecommended before discharge or shortly thereafter toidentify patients who may also benefit from revasculariza-tion. The use of either LMWH or platelet GP IIb/IIIareceptor blockers has reduced the incidence of adverseoutcomes in patients managed conservatively (see SectionIII. B) (10,169–171,182,184,247,248), suggesting that theearly conservative strategy may be advantageous becausecostly invasive procedures may be avoided in even morepatients.
Rationale for the Early Invasive Strategy
In patients with UA/NSTEMI without recurrent isch-emia in the first 24 h, the use of early angiography providesan invasive approach to risk stratification. It can identify the10% to 15% of patients with no significant coronary stenosesand the '20% with 3-vessel disease with LV dysfunction orleft main CAD. This latter group may derive a survivalbenefit from bypass surgery (see Section IV). In addition,early percutaneous revascularization of the culprit lesion hasthe potential to reduce the risk for subsequent hospitaliza-tion and the need for multiple antianginal drugs comparedwith the early conservative strategy (TIMI IIIB) (19).
Just as the use of improved antithrombotic therapy withLMWH and/or a platelet GP IIb/IIIa receptor blocker hasimproved the outcome in patients managed according to theearly conservative strategy, the availability of these agentsalso makes the early invasive approach more attractive,because the early hazard of percutaneous intervention islessened. The availability of GP IIb/IIIa receptor blockershas led to 2 alternatives for the invasive approach: immedi-ate angiography or deferred angiography.
Immediate AngiographySome believe that proceeding immediately to angiogra-
phy is an efficient approach for the ACS patient. Patientsfound not to have CAD may be discharged rapidly orshifted to a different management strategy. Patients withobvious culprit lesions amenable to percutaneous interven-tion could have a procedure performed immediately, thushastening discharge. Patients with left main CAD andpatients with multivessel disease and LV dysfunction could
1014 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062

be sent expeditiously to undergo bypass surgery, therebyavoiding a risky waiting period. However, only 1 observa-tional study (271) has addressed this approach directly, andthe results are not definitive.
Deferred Angiography
In most reports that involve use of the early invasivestrategy, angiography has been deferred for 12 to 48 h whileantithrombotic and anti-ischemic therapies are intensified.Several observational studies (272) have found a lower rateof complications in patients undergoing percutaneous inter-vention .48 h after admission, during which heparin andASA were administered, compared with early intervention.However, it should be noted that the value of medicalstabilization before angiography has never been assessedformally.
2. Care Objectives. The objective is to provide a strategythat has the most potential to yield the best clinicaloutcome. The purpose of coronary angiography is to providedetailed information about the size and distribution ofcoronary vessels, the location and extent of atheroscleroticobstruction, and the suitability for revascularization. TheLV angiogram, which is usually carried out along withcoronary arteriogram, provides an assessment of the extentof focal and global LV dysfunction and of the presence andseverity of coexisting disorders (e.g., valvular or congenitallesions). A detailed discussion of revascularization is pre-sented in Section IV of these guidelines, as well as in theACC/AHA Guidelines for Percutaneous TransluminalCoronary Angioplasty (273) and ACC/AHA Guidelinesfor Coronary Artery Bypass Graft Surgery (274). Althoughgeneral guidelines can be offered, the selection of appropri-ate procedures and the decision to refer patients for revas-cularization require both clinical judgment and counselingwith the patient and his or her family regarding expectedrisks and benefits. In this counseling, it is important toconsider that large registry and controlled clinical trial datagenerally show no or limited evidence of reduced death orMI rates when early coronary angiography followed byrevascularization is used in a routine and unselected mannerin patients with UA/NSTEMI.
Because the basis for acute ischemia is plaque rupture/erosion and/or severe obstructive CAD, it has been postu-lated that early revascularization would improve prognosis.This notion led to considerable investigation in patientswith stable coronary syndromes as well as AMI in the1970s. In selected circumstances, revascularization withCABG seems to be associated with lower morbidity andmortality rates compared with a more conservative strategy.These circumstances center around the documentation ofsevere ischemia (resting ECG and on noninvasive testing)or potential for severe ischemia (left main stenosis or severemultivessel CAD with impaired LV function). These data,however, are limited because both medical and surgicaltreatments have been markedly improved in the past 2
decades and the population of patients who present withCAD today has changed (e.g., a higher proportion ofwomen, elderly persons, minorities, and diabetics).
Although 2 recent studies were not conducted in patientswith UA/NSTEMI, they have addressed the value of stresstesting in guiding therapy. The DANish trial in AcuteMyocardial Infarction (DANAMI) studied 503 patientswith inducible ischemia (i.e., a positive exercise stress test)after thrombolytic therapy for first MI and compared anischemia-guided invasive strategy with a conservative strat-egy (275). The invasive strategy in the post-AMI patientswith inducible ischemia resulted in a reduction in theincidence of reinfarction, hospitalizations for UA, and stableangina. Similarly, in the Asymptomatic Cardiac IschemiaPilot (ACIP) (276,277), 558 clinically stable patients withischemia on stress testing and during daily life (ST-segmentdepression on exercise treadmill testing or perfusion abnor-mality on radionuclide pharmacological stress test if unableto exercise, in addition to ST-segment depression onambulatory ECG monitoring), of whom most had angina inthe previous 6 weeks, were randomized to 1 of 3 initialtreatment strategies: symptom-guided medical care, isch-emia-guided medical care, and revascularization. More thanone third of these patients had “complex” stenoses onangiography. Those randomized to early revascularizationexperienced less ambulatory ischemia at 12 weeks than didthose randomized to initial medical care in whom revascu-larization was delayed and symptom driven.
In ACS patients with UA/NSTEMI, the purpose ofnoninvasive testing is to identify ischemia as well as toidentify candidates at high risk for adverse outcome and todirect them to coronary angiography and revascularizationwhen possible. However, both randomized trials(19,265,266,278) and observational data (279–281) do notuniformly support an inherent superiority for the routine useof early coronary angiography and revascularization. In fact,the VANQWISH trial suggests that an early conservativestrategy, in which candidates for coronary angiography andrevascularization are selected from the results of ischemia-guided noninvasive testing, may be associated with fewerdeaths. Accordingly, the decision regarding which strategyto pursue for a given patient should be based on the patient’sestimated outcome risk assisted by clinical and noninvasivetest results, available facilities, previous outcome of revas-cularization by the team available and in the institution inwhich the patient is hospitalized, and patient preference.
Early coronary angiography may enhance prognosticstratification. This information may be used to guide med-ical therapy as well as to plan revascularization therapy, butit is important to emphasize that adverse outcome in ACSis very time dependent and that after 1 to 2 months, the riskfor adverse outcome is essentially the same as that forlow-risk chronic stable angina (Fig. 3). Furthermore, nu-merous studies in patients with stable angina, includingResearch Group in Instability in Coronary Artery Disease(RITA)-2 (267), have documented the significant early risk
1015JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina

of death or MI with an interventional strategy comparedwith medical management alone. Thus, the timing ofcoronary angiography and revascularization is critically im-portant if patients at high risk are to benefit. Unfortunately,the total number of operative complications is increasedwhen revascularization procedures are performed routinely,because some patients who are not in need of revasculariza-tion will be exposed to its hazards.
The population of patients with UA/NSTEMI includes asubgroup (i.e., those with left main coronary stenosis ormultivessel stenoses with reduced LV function) at high riskfor adverse outcome and therefore highly likely to benefitfrom revascularization. Clinical evaluation and noninvasivetesting will aid in the identification of most of thesehigh-risk patients who have markers of high risk such asadvanced age (.70 years), prior MI, revascularization,ST-segment deviation, CHF or depressed resting LV func-tion (i.e., EF ,0.40) on noninvasive study, or noninvasivestress test findings that suggest severe ischemia (see SectionIII. C). The remaining larger subgroup of patients, how-ever, do not have the findings that portend a high risk foradverse outcomes. Accordingly, they are not likely to receivesuch benefit from routine revascularization, and invasivestudy is optional for them. It can be safely deferred pendingfurther clinical developments. Decisions regarding coronaryangiography in patients who are not high risk according tofindings on clinical examination and noninvasive testing canbe individualized on the basis of patient preferences.
The data on which these recommendations are based arefrom 4 randomized trials, TIMI IIIB (19), VANQWISH(266), Medicine versus Angiography in Thrombolytic Ex-clusion (MATE) (265), and FRISC II (278); a largeprospective multinational registry, the OASIS registry(279); and 2 retrospective analyses (280,281).
In TIMI IIIB, 1,473 patients with UA (67%) orNSTEMI (33%) with chest pain of ,24-h duration wererandomized to either an invasive or early conservativestrategy. At 42 days, 16.2% of the early invasive patients haddied, had experienced a nonfatal MI, or had a stronglypositive exercise test vs. 18.1% of early conservative patients(p 5 0.33). Similarly, there was no difference in theoutcome of death or MI in a comparison of treatmentstrategies (4,282). An analysis of factors associated with thefailure of medical therapy in TIMI IIIB predicted patientswho could be directed to a more invasive strategy in acost-efficient manner. Among the 733 patients randomizedto the conservative strategy, the factors that independentlypredicted failure of medical therapy included ST-segmentdepression on the qualifying ECG, prior ASA use, andolder age. For most patients with $3 such risk factors,medical therapy had failed, defined as death, MI, restangina, or markedly abnormal stress test results at 6 weeks.A combination of factors should be considered in theselection of patients for expedited angiography and revas-cularization (282).
NSTEMI represents a high-risk acute ischemic syn-
drome. The VANQWISH Investigators randomly assigned920 patients with NSTEMI defined on the basis ofCK-MB to either early invasive (462 patients) or conserva-tive (458 patients) management within 72 h of the onset ofan NSTEMI (266). The number of patients with eitherdeath or recurrent nonfatal MI and the number who diedwere higher in the invasive strategy group at hospitaldischarge (36 vs. 15 patients, p 5 0.004 for death ornonfatal MI; 21 vs. 6, p 5 0.007 for death), and thesedifferences persisted at 1 month and at 1 year. Mortalityrates during the almost 2-year follow-up also showed astrong trend toward reduction in patients assigned to theconservative strategy compared with those assigned to theinvasive strategy (hazard ratio, 0.72; 95% confidence interval[CI], 0.51 to 1.01). The investigators concluded that mostpatients with NSTEMI do not benefit from routine, earlyinvasive management and that a conservative, ischemia-guided initial approach is both safe and effective even in thepredominantly high-risk male population of the VAN-QWISH.
The MATE trial (265) enrolled 201 patients with avariety of ACSs who were ineligible for thrombolytictherapy and were assigned to an early invasive or earlyconservative strategy. Although the incidence of total isch-emic in-hospital events was lower in the early invasivestrategy group, there were no differences between the groupsin the incidence of death and reinfarction. Follow-up at amedian of 21 months showed no significant differences inthe cumulative incidences of death, MI, rehospitalization,or revascularization.
Most recently, in the FRISC II study, 3,048 ACSpatients were treated with dalteparin for 5 to 7 days (278).Of these patients, 2,457 without acute problems who werenot at high risk of a revascularization procedure (e.g., theirage was not .75 years, and they did not have prior CABG)were randomized (2 3 2 factorial design) to continue toreceive either dalteparin or placebo (double blind) and eitheran invasive or a noninvasive treatment strategy. The latterpatients were revascularized only for refractory or recurrentsymptoms despite maximum medical therapy or severeischemia (ST-segment depression $0.3 mV) on symptom-limited exercise testing or AMI. At 6 months, there were nodifferences between continued dalteparin compared withplacebo. However, death or MI occurred in 9.4% of patientsassigned to the invasive strategy and in 12.1% of thoseassigned the noninvasive strategy (p , 0.031). At one yearthe mortality rate in the invasive strategy group was 2.2%compared with 3.9% in the noninvasive strategy group (p 50.016) (278a). It may be concluded from FRISC II thatpatients with UA/NSTEMI who are not at very high riskfor revascularization and who first receive an average of 6days of treatment with LMWH, ASA, nitrates, andb-blockers have a better outcome at 6 months with a(delayed) routine invasive approach than with a routineconservative approach.
Retrospective analysis of these trials identified 2 sub-
1016 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062

groups of patients who appear to benefit from an earlyinvasive strategy: patients who presented with ST-segmentdepression and those .65 years old. When these 2 sub-groups of patients were assigned to the conservative arm ofTIMI IIIB, they were at a higher risk of failing medicaltherapy (282), and they displayed a particularly strongbenefit from the invasive therapy in FRISC II (278).
It is important to note the differences between theserandomized trials. Baseline patient characteristics indicatethat risk was highest in VANQWISH, which enrolled onlyNSTEMI patients, and lowest in FRISC II, which hadfewer smokers, patients with previous MIs or hypertension,diabetics, and patients with NSTEMI (as opposed to UA).FRISC II excluded patients .75 years old and with priorCABG and treated all patients with LMWH for a medianof 6 days before deployment of the invasive strategy. FRISCII also had the most restrictive criteria for the use ofrevascularization in patients randomized to a conservativestrategy, requiring $0.3-mV ST-segment depression onstress testing. TIMI IIIB patients seem to be intermediatein risk, but again, the subgroup with NSTEMI had a higherrisk for death or reinfarction. Other differences may berelated to the lower mortality rates with surgical revascular-ization in FRISC II compared with VANQWISH. Thus,in VANQWISH, the poor outcome in the invasive arm wasobserved in high-risk patients with early intervention,whereas the favorable effect with the invasive arm in FRISCII was seen in patients at lower risk in whom interventionwas carried out after 5 to 7 days. FRISC II also used centersof excellence for CABG and had a very low peri-CABGmortality rate.
Data from recent observational studies support the con-clusion that an early invasive strategy does not reduce the“hard” end points of death and MI but does reduce recurrentstable angina or UA. The OASIS Registry Investigators(279) prospectively studied the relation between rates ofangiography and revascularization and rates of cardiovascu-lar death, nonfatal MI, stroke, refractory angina, and majorbleeding in a prospective registry-based study in 6 countrieswith widely varying intervention rates. A total of 7,987patients who presented with UA/NSTEMI were recruitedfrom 95 hospitals and followed for up to 6 months. Rates ofprocedure use were highest in patients in the United Statesand Brazil, intermediate in Canada and Australia, andlowest in Hungary and Poland. There were no significantdifferences in death or MI among these countries. Therewere no differences in the rates of death or MI in countrieswith the highest rates of invasive procedures (59%) vs. theremaining countries (21%). Higher rates of invasive andrevascularization procedures were associated with lowerrates of angina and readmission for UA but a higherincidence of stroke.
Although PCI has advanced with the development ofstents and platelet GP IIb/IIIa receptor blockers, the use ofthe latter has also been associated with a reduced need forrevascularization in non–ST-segment elevation ACS
(10,21). In this regard, an analysis from the GUSTO-IIband PURSUIT trials of patients who underwent coronaryangiography during initial hospitalization for non–ST-segment elevation ACS found that a conservative, ischemia-guided strategy was associated with improved outcomecompared with a routine invasive strategy (adjusted OR fordeath or MI, invasive vs. conservative: 6.61 at 30 days and1.98 at 6 months) (281). At 1 year, however, the outcomeswere similar.
Although data are not available to permit a formalcost-effectiveness analysis of these alternate strategies, anysavings realized initially in the group not receiving coronaryangiography and revascularization has the potential to beoffset by the need for initial longer hospitalization and forsubsequent care, as was observed in TIMI IIIB (4,19,282).However, the VANQWISH results showed a significantlylonger duration of hospitalization for the invasive strategy(266).
Based on these data, a routine early invasive strategy withangiography and revascularization is difficult to justify. TheFRISC II data suggest that a delayed invasive strategy after5 to 7 days of LMWH and b-blocker therapy in selectedpatients (,75 years old and no prior CABG) could be auseful approach, but the delay of angiography by 6 daysmitigates one of the advantages of the invasive strategy. Theearly use of angiography in patients deemed at high risk onthe basis of clinical and noninvasive test findings wouldappear to be an acceptable approach.
Some selected areas require additional comment. In apatient with UA, a history of prior PCI within the past 6months suggests the presence of restenosis, which often canbe effectively treated with repeat PCI. Coronary angiogra-phy without preceding functional testing is generally indi-cated. Patients with prior CABG represent another subgroupfor whom a strategy of early coronary angiography is usuallyindicated. The complex interplay between the progressionof native coronary disease and the development of graftatherosclerosis with ulceration and embolization is difficultto untangle noninvasively; all argue for early coronaryangiography. In addition, patients with known or suspectedreduced LV systolic function, including patients with prioranterior Q-wave MIs, those with prior measurements thatshow depressed LV function, and those who present withCHF, have sufficient risk that the possibility of benefit fromrevascularization procedures merits early coronary angiog-raphy without preceding functional testing.
In patients with UA/NSTEMI, coronary angiographytypically shows the following profile: 1) no severe epicardialstenosis in 10% to 20%, 2) 1-vessel stenosis in 30% to 35%,3) multivessel stenosis in 40% to 50%, and 4) significant(.50%) left main stenosis in 4% to 10%. In the earlyinvasive strategy in TIMI IIIB, no critical obstruction(,60% diameter stenosis) was found in 19% of patients,1-vessel stenosis in 38%, 2-vessel stenosis in 29%, 3-vesselstenosis in 15%, and left main stenosis (.50%) in 4%.Complex plaques are usually believed to be responsible for
1017JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina

the culprit lesions. These usually are eccentric and some-times have irregular borders, and correlate with intracoro-nary thrombi and an increased risk of recurrent ischemia atrest, MI, and cardiac death (283). Similar findings werenoted in .80% of the patients in the VANQWISH trial,and .1 complex lesion was found in most patients (284).Interestingly, in TIMI IIIB, many of the patients withoutsevere stenosis had reduced contrast clearance, which sug-gests microvascular dysfunction (285), which may contrib-ute to impaired myocardial perfusion.
Patients with severe 3-vessel stenosis and reduced LVfunction and those with left main stenosis should beconsidered for early CABG (see Section IV). In low-riskpatients, quality of life and patient preferences should begiven considerable weight in the selection of a treatmentstrategy. Low-risk patients whose symptoms do not respondwell to maximal medical therapy and who experience poorquality of life and functional status and are prepared toaccept the risks of revascularization should be considered forrevascularization.
The discovery that a patient does not have significantobstructive CAD can help avert improper “labeling” andprompt a search for the true cause of symptoms. Unfortu-nately, many such patients continue to have recurrentsymptoms, become disabled, are readmitted to the hospital,and continue to consume healthcare resources even withrepeated coronary angiography (286,287).
It is not presently possible to define the extent ofcomorbidity that would, in every case, make referral forcoronary angiography and revascularization inappropriate.The high-risk patient with significant comorbidities re-quires thoughtful discussion among the physician, patient,and family and/or patient advocate. A decision for or againstrevascularization must be made on a case-by-case basis.
Examples of extensive comorbidity that usually precluderevascularization include 1) advanced or metastatic malig-nancy with a projected life expectancy of #1 year, 2)intracranial pathology that contraindicates the use of sys-temic anticoagulation or causes severe cognitive disturbance(e.g., Alzheimer’s disease) or advanced physical limitations,3) end-stage cirrhosis with symptomatic portal hypertension(e.g., encephalopathy, visceral bleeding), and 4) CAD thatis known from previous angiography not to be amenable torevascularization. This list is not meant to be all inclusive.More difficult decisions involve patients with comorbiditiesnot as serious as those listed here; examples include patientswho have moderate or severe renal failure but are stable ondialysis.
Consultation with an interventional cardiologist andcardiac surgeon before coronary angiography is advised todefine technical options and likely risks and benefits. Theoperators who perform coronary angiography and revascu-larization and the facility in which these procedures arecarried out are important considerations because the avail-ability of interventional cardiologists and cardiac surgeonswho are experienced in high-risk and complex patients is
essential. As a general principle, the potential benefits ofcoronary angiography and revascularization must be care-fully weighed against the risks and the conflicting results ofthe clinical trials and registries.
IV. CORONARY REVASCULARIZATION
A. General Principles
As discussed in Section III, coronary angiography is usefulfor defining the coronary artery anatomy in patients withUA/NSTEMI and for identifying subsets of high-riskpatients who may benefit from early revascularization.Coronary revascularization (PCI or CABG) is carried out toimprove prognosis, relieve symptoms, prevent ischemiccomplications, and improve functional capacity. The deci-sion to proceed from diagnostic angiography to revascular-ization is influenced not only by the coronary anatomy butalso by a number of additional factors, including anticipatedlife expectancy, ventricular function, comorbidity, func-tional capacity, severity of symptoms, and quantity of viablemyocardium at risk. These are all important variables thatmust be considered before revascularization is recom-mended. For example, patients with distal obstructive cor-onary lesions or those who have large quantities of irrevers-ibly damaged myocardium are unlikely to benefit fromrevascularization, particularly if they can be stabilized withmedical therapy. Patients with high-risk coronary anatomyare likely to benefit from revascularization in terms of bothsymptom improvement and long-term survival (Fig. 12).The indications for coronary revascularization in patientswith UA/NSTEMI are similar to those for patients withchronic stable angina and are presented in greater detail inthe ACC/AHA/ACP-ASIM Guidelines for the Manage-ment of Patients With Chronic Stable Angina (26), as wellas in the ACC/AHA Guidelines for Coronary ArteryBypass Graft Surgery (274).
Plaque rupture with subsequent platelet aggregation andthrombus formation is most often the underlying patho-physiological cause of UA (1,18). The management of manypatients with UA/NSTEMI often involves revascularizationof the underlying CAD with either PCI or CABG. Selec-tion of the appropriate revascularization strategy oftendepends on clinical factors, operator experience, and extentof the underlying CAD. Many patients with UA/NSTEMIhave coronary disease that is amenable to either form oftherapy. However, some patients have high-risk features,such as reduced LV function, that places them in a group ofpatients who experience improved long-term survival rateswith CABG. In other patients, adequate revascularization withPCI may not be optimal or even possible, and CABG may bethe better revascularization choice.
Findings in large registries of patients with CAD suggestthat the mode of clinical presentation should have littlebearing on the subsequent revascularization strategy. In aseries of 9,263 patients with CAD, an admission diagnosisof UA (vs. chronic stable angina) had no influence on 5-year
1018 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
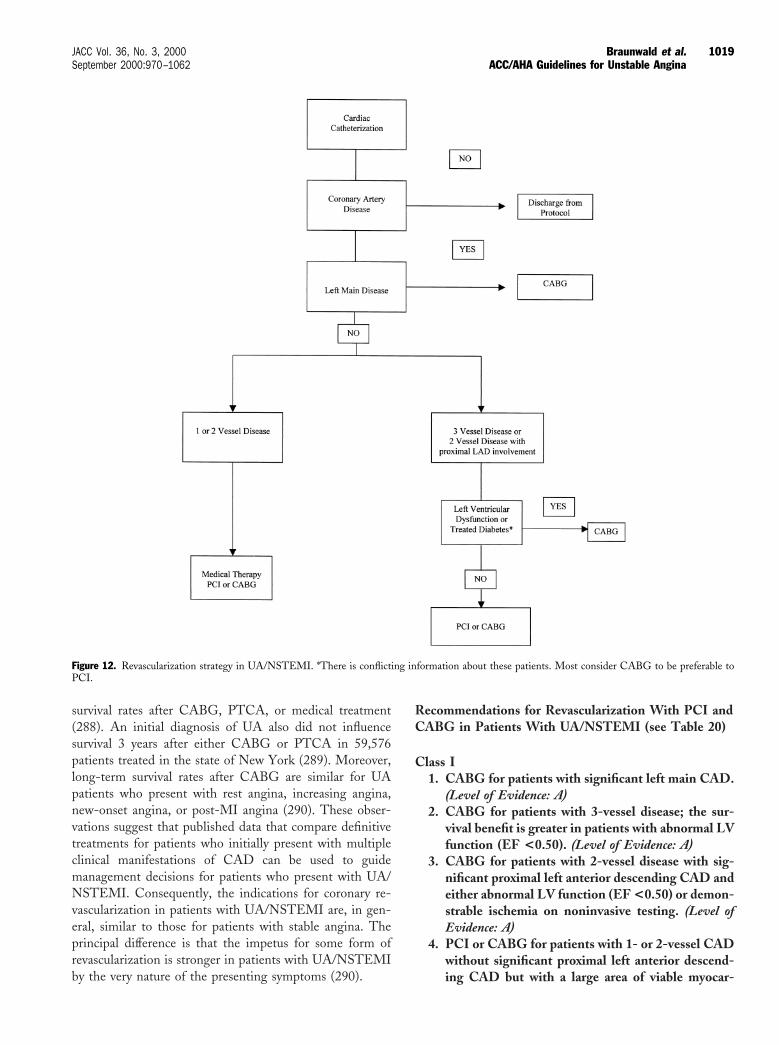
survival rates after CABG, PTCA, or medical treatment(288). An initial diagnosis of UA also did not influencesurvival 3 years after either CABG or PTCA in 59,576patients treated in the state of New York (289). Moreover,long-term survival rates after CABG are similar for UApatients who present with rest angina, increasing angina,new-onset angina, or post-MI angina (290). These obser-vations suggest that published data that compare definitivetreatments for patients who initially present with multipleclinical manifestations of CAD can be used to guidemanagement decisions for patients who present with UA/NSTEMI. Consequently, the indications for coronary re-vascularization in patients with UA/NSTEMI are, in gen-eral, similar to those for patients with stable angina. Theprincipal difference is that the impetus for some form ofrevascularization is stronger in patients with UA/NSTEMIby the very nature of the presenting symptoms (290).
Recommendations for Revascularization With PCI andCABG in Patients With UA/NSTEMI (see Table 20)
Class I1. CABG for patients with significant left main CAD.
(Level of Evidence: A)2. CABG for patients with 3-vessel disease; the sur-
vival benefit is greater in patients with abnormal LVfunction (EF <0.50). (Level of Evidence: A)
3. CABG for patients with 2-vessel disease with sig-nificant proximal left anterior descending CAD andeither abnormal LV function (EF <0.50) or demon-strable ischemia on noninvasive testing. (Level ofEvidence: A)
4. PCI or CABG for patients with 1- or 2-vessel CADwithout significant proximal left anterior descend-ing CAD but with a large area of viable myocar-
Figure 12. Revascularization strategy in UA/NSTEMI. *There is conflicting information about these patients. Most consider CABG to be preferable toPCI.
1019JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
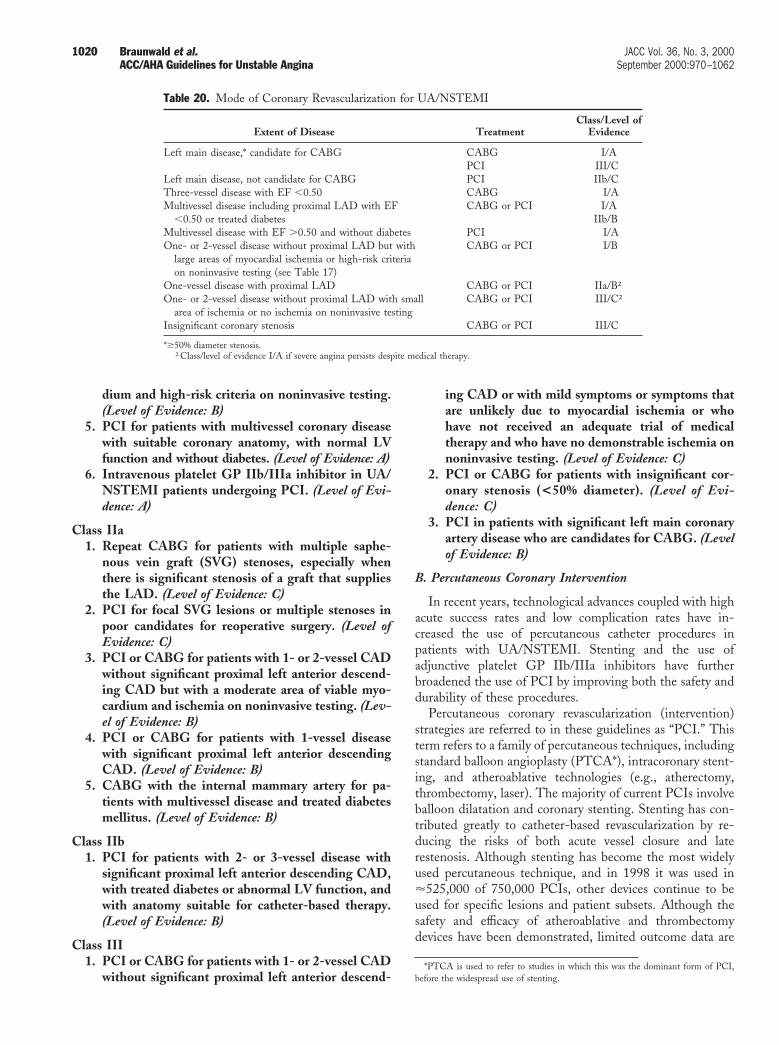
dium and high-risk criteria on noninvasive testing.(Level of Evidence: B)
5. PCI for patients with multivessel coronary diseasewith suitable coronary anatomy, with normal LVfunction and without diabetes. (Level of Evidence: A)
6. Intravenous platelet GP IIb/IIIa inhibitor in UA/NSTEMI patients undergoing PCI. (Level of Evi-dence: A)
Class IIa1. Repeat CABG for patients with multiple saphe-
nous vein graft (SVG) stenoses, especially whenthere is significant stenosis of a graft that suppliesthe LAD. (Level of Evidence: C)
2. PCI for focal SVG lesions or multiple stenoses inpoor candidates for reoperative surgery. (Level ofEvidence: C)
3. PCI or CABG for patients with 1- or 2-vessel CADwithout significant proximal left anterior descend-ing CAD but with a moderate area of viable myo-cardium and ischemia on noninvasive testing. (Lev-el of Evidence: B)
4. PCI or CABG for patients with 1-vessel diseasewith significant proximal left anterior descendingCAD. (Level of Evidence: B)
5. CABG with the internal mammary artery for pa-tients with multivessel disease and treated diabetesmellitus. (Level of Evidence: B)
Class IIb1. PCI for patients with 2- or 3-vessel disease with
significant proximal left anterior descending CAD,with treated diabetes or abnormal LV function, andwith anatomy suitable for catheter-based therapy.(Level of Evidence: B)
Class III1. PCI or CABG for patients with 1- or 2-vessel CAD
without significant proximal left anterior descend-
ing CAD or with mild symptoms or symptoms thatare unlikely due to myocardial ischemia or whohave not received an adequate trial of medicaltherapy and who have no demonstrable ischemia onnoninvasive testing. (Level of Evidence: C)
2. PCI or CABG for patients with insignificant cor-onary stenosis (<50% diameter). (Level of Evi-dence: C)
3. PCI in patients with significant left main coronaryartery disease who are candidates for CABG. (Levelof Evidence: B)
B. Percutaneous Coronary Intervention
In recent years, technological advances coupled with highacute success rates and low complication rates have in-creased the use of percutaneous catheter procedures inpatients with UA/NSTEMI. Stenting and the use ofadjunctive platelet GP IIb/IIIa inhibitors have furtherbroadened the use of PCI by improving both the safety anddurability of these procedures.
Percutaneous coronary revascularization (intervention)strategies are referred to in these guidelines as “PCI.” Thisterm refers to a family of percutaneous techniques, includingstandard balloon angioplasty (PTCA*), intracoronary stent-ing, and atheroablative technologies (e.g., atherectomy,thrombectomy, laser). The majority of current PCIs involveballoon dilatation and coronary stenting. Stenting has con-tributed greatly to catheter-based revascularization by re-ducing the risks of both acute vessel closure and laterestenosis. Although stenting has become the most widelyused percutaneous technique, and in 1998 it was used in'525,000 of 750,000 PCIs, other devices continue to beused for specific lesions and patient subsets. Although thesafety and efficacy of atheroablative and thrombectomydevices have been demonstrated, limited outcome data are
*PTCA is used to refer to studies in which this was the dominant form of PCI,before the widespread use of stenting.
Table 20. Mode of Coronary Revascularization for UA/NSTEMI
Extent of Disease TreatmentClass/Level of
Evidence
Left main disease,* candidate for CABG CABGPCI
I/AIII/C
Left main disease, not candidate for CABG PCI IIb/CThree-vessel disease with EF ,0.50 CABG I/AMultivessel disease including proximal LAD with EF
,0.50 or treated diabetesCABG or PCI I/A
IIb/BMultivessel disease with EF .0.50 and without diabetes PCI I/AOne- or 2-vessel disease without proximal LAD but with
large areas of myocardial ischemia or high-risk criteriaon noninvasive testing (see Table 17)
CABG or PCI I/B
One-vessel disease with proximal LAD CABG or PCI IIa/B†One- or 2-vessel disease without proximal LAD with small
area of ischemia or no ischemia on noninvasive testingCABG or PCI III/C†
Insignificant coronary stenosis CABG or PCI III/C
*$50% diameter stenosis.†Class/level of evidence I/A if severe angina persists despite medical therapy.
1020 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062

available that describe the use of these new strategiesspecifically in patients with UA/NSTEMI (291).
In the absence of active thrombus, rotational atherectomyis useful to debulk arteries that contain large atheromatousburdens and to modify plaques in preparation for moredefinitive treatment with adjunctive balloon angioplasty orstenting. This approach is particularly well suited for use inhard, calcific lesions, in which it preferentially ablatesinelastic tissue. Rotational atherectomy, even in patientswith stable angina, may result in the release of CK-MBisoenzymes after seemingly uncomplicated procedures. Thisoften reflects distal embolization of microparticulate matterand platelet activation, and the clinical outcome has beencorrelated with the magnitude of the enzyme elevation(292). The magnitude and frequency of postproceduralmyocardial necrosis reflected in CK-MB enzyme rises canbe reduced with concomitant treatment with a platelet GPIIb/IIIa inhibitor (293,294).
Other new techniques and devices, such as the use ofAngiojet thrombectomy and extraction atherectomy (trans-luminal extraction catheter), are being tested for the treat-ment of thrombi that are visible within a coronary artery(295). In addition, there is some evidence that extractionatherectomy can be used to treat SVG disease through theremoval of degenerated graft material and thrombus (296).In this situation, it often is used as an adjunct to moredefinitive therapy with balloon angioplasty and stents.
The reported clinical efficacy of PCI in UA/NSTEMIhas varied. This is likely attributable to differences in studydesign, treatment strategies, patient selection, and operatorexperience. Nevertheless, the success rate of PCI in patientswith UA/NSTEMI is often quite high. In TIMI IIIB, forexample, angiographic success was achieved in 96% ofpatients with UA/NSTEMI who underwent balloon angio-plasty. With clinical criteria, periprocedural MI occurred in2.7%, emergency bypass surgery was required in 1.4%, andthe death rate from the procedure was 0.5% (4,19,297).
The use of balloon angioplasty has been evaluated inseveral other trials of patients with UA vs. stable angina(298–303). A large retrospective study compared the resultsof angioplasty in patients with stable angina with that inpatients with UA (299). After an effort to control patientswith UA with medical therapy, PTCA was carried out anaverage of 15 days after hospital admission. In comparisonwith patients with stable angina, UA patients showed nosignificant differences with respect to primary clinical suc-cess (92% for UA vs. 94% for stable angina), in-hospitalmortality rates (0.3% vs. 0.1%), or the number of adverseevents at 6-month follow-up (299). These findings suggestthat PTCA results in immediate and 6-month outcomesthat are comparable in patients with stable angina and UA.In addition, in a retrospective analysis, the results in UApatients were similar regardless of whether the procedurewas performed early (,48 h) or late (.48 h) after hospitalpresentation (298).
Although other earlier studies (predominantly from the1980s) have suggested that patients with UA who undergoballoon PTCA have higher rates of MI and restenosiscompared with patients with stable angina (300–304),contemporary catheter revascularization often involves cor-onary stenting and adjunctive use of platelet GP IIb/IIIareceptor inhibitors, which are likely to affect not onlyimmediate- but also long-term outcome (246). Historically,PTCA has been limited by acute vessel closure, whichoccurs in '5% of patients, and by coronary restenosis,which occurs in '35% to 45% of treated lesions during a6-month period. Coronary stenting offers an importantalternative to PTCA because of its association with both amarked reduction in acute closure and lower rates ofrestenosis. By preventing acute or threatened closure, stent-ing reduces the incidence of procedure-related STEMI andneed for emergency bypass surgery and may also preventother ischemic complications.
In a comparison of the use of the Palmaz-Schatz coronarystent in patients with stable angina and patients with UA,no significant differences were found with respect to in-hospital outcome or restenosis rates (305). Another studyfound similar rates of initial angiographic success andin-hospital major complications in stented patients with UAcompared with those with stable angina (306). Majoradverse cardiac events at 6 months were also similar betweenthe 2 groups, whereas the need for repeat PCI and targetvessel revascularization was actually less in the UA group.On the other hand, other recent data have suggested thatUA increases the incidence of adverse ischemic outcomes inpatients undergoing coronary stent deployment despitetherapy with ticlopidine and ASA, which suggests the needfor more potent antiplatelet therapy in this patient popula-tion (307,308).
1. Platelet Inhibitors and Percutaneous Revasculariza-tion. An important advance in the treatment of patientswith UA/NSTEMI who are undergoing PCI has been theintroduction of platelet GP IIb/IIIa receptor inhibitors (seeSection III. B) (10,18,21,244–246,309–311). This therapytakes advantage of the fact that platelets play an importantrole in the development of ischemic complications that mayoccur in patients with UA/NSTEMI or during coronaryrevascularization procedures. Currently, 3 platelet GP IIb/IIIa inhibitors are approved by the Food and Drug Admin-istration based on the outcome of a variety of clinical trials:abciximab (ReoPro), tirofiban (Aggrastat), and eptifibatide(Integrilin). The Evaluation of c7E3 for the Prevention ofIschemic Complications (EPIC), Evaluation of PTCA andImprove Long-term Outcome by c7E3 GP IIb/IIIa recep-tor blockade (EPILOG), CAPTURE, and Evaluation ofPlatelet IIb/IIIa Inhibitor for STENTing (EPISTENT)trials investigated the use of abciximab; the PRISM,PRISM-PLUS, and Randomized Efficacy Study of Tirofi-ban for Outcomes and REstenosis (RESTORE) trialsevaluated tirofiban; and the Integrilin to Minimize Platelet
1021JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
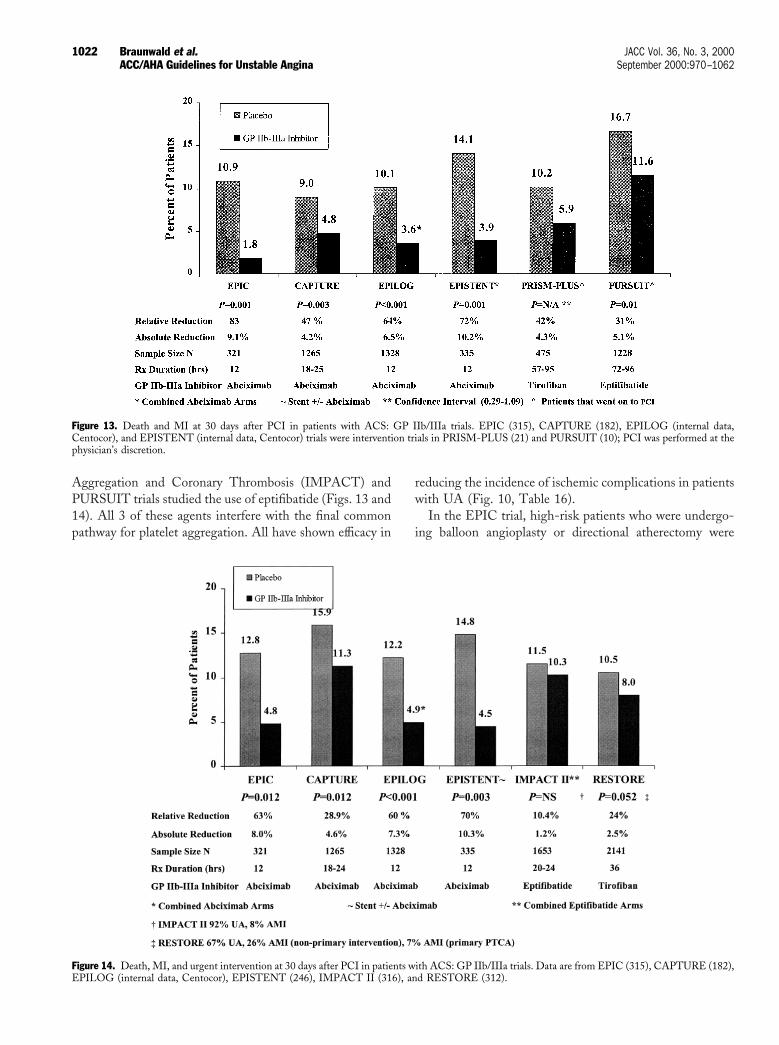
Aggregation and Coronary Thrombosis (IMPACT) andPURSUIT trials studied the use of eptifibatide (Figs. 13 and14). All 3 of these agents interfere with the final commonpathway for platelet aggregation. All have shown efficacy in
reducing the incidence of ischemic complications in patientswith UA (Fig. 10, Table 16).
In the EPIC trial, high-risk patients who were undergo-ing balloon angioplasty or directional atherectomy were
Figure 13. Death and MI at 30 days after PCI in patients with ACS: GP IIb/IIIa trials. EPIC (315), CAPTURE (182), EPILOG (internal data,Centocor), and EPISTENT (internal data, Centocor) trials were intervention trials in PRISM-PLUS (21) and PURSUIT (10); PCI was performed at thephysician’s discretion.
Figure 14. Death, MI, and urgent intervention at 30 days after PCI in patients with ACS: GP IIb/IIIa trials. Data are from EPIC (315), CAPTURE (182),EPILOG (internal data, Centocor), EPISTENT (246), IMPACT II (316), and RESTORE (312).
1022 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062

randomly assigned to 1 of 3 treatment regimens: placebobolus followed by placebo infusion for 12 h; weight-adjustedabciximab bolus (0.25 mg/kg) and 12-h placebo infusion; orweight-adjusted abciximab bolus and 12-h infusion (10mg/min) (244,309). In this trial, high risk was defined assevere UA, evolving MI, or high-risk coronary anatomydefined at cardiac catheterization. The administration ofbolus and continuous infusion of abciximab reduced the rateof ischemic complications (death, MI, revascularization) by35% at 30 days (12.8 vs. 8.3%, p 5 0.0008), by 23% at 6months, and by 13% at 3 years (244,309,310). The favorablelong-term effect was mainly due to a reduction in the needfor bypass surgery or repeat PCI in patients with an initiallysuccessful procedure.
The administration of abciximab in the EPIC trial wasassociated with an increased bleeding risk and transfusionrequirement. In the subsequent EPILOG trial, which usedweight-adjusted dosing of concomitant heparin, the inci-dence of major bleeding and transfusion associated withabciximab and low-dose weight-adjusted heparin (70 U/kg)was similar to that seen with placebo (245). The cohort ofpatients with UA undergoing PCI in the EPILOG trialdemonstrated a 64% reduction (10.1% to 3.6%, p 5 0.001)in the composite occurrence of death, MI, or urgentrevascularization to 30 days with abciximab therapy comparedwith placebo (standard-dose weight-adjusted heparin).
The RESTORE trial was a randomized double-blindstudy that evaluated the use of tirofiban vs. placebo in 2,139patients with UA or AMI, including patients with non–Q-wave MI who underwent PCI (balloon PTCA or direc-tional atherectomy) within 72 h of hospitalization (312).The trial was designed to evaluate both clinical outcomesand restenosis. Although the infusion of tirofiban (bolus of10 mg/kg followed by a 36-h infusion at 0.15 mgzkg21zmin21)had no significant effect on the reduction in restenosis at 6months, a trend was observed for a reduction in thecombined clinical end point of death/MI, emergencyCABG, unplanned stent placement for acute or threatenedvessel closure, and recurrent ischemia compared with pla-cebo at 6 months (27.1% vs. 24.1%, p 5 0.11).
The clinical efficacy of tirofiban was further evaluated inthe PRISM-PLUS trial, which enrolled patients with UA/NSTEMI within 12 h of presentation (21) (see Section III).Among patients who underwent PCI, the 30-day incidenceof death, MI, refractory ischemia, or rehospitalization forUA was 15.3% in the group that received heparin alonecompared with 8.8% in the tirofiban/heparin group. AfterPCI, death or nonfatal MI occurred in 10.2% of thosereceiving heparin vs. 5.9% of tirofiban-treated patients.
Eptifibatide, a cyclic heptapeptide GP IIb/IIIa inhibitor,has also been administered to patients with ACS. In thePURSUIT trial, nearly 11,000 patients who presented withan ACS were randomized to receive either UFH and ASAor eptifibatide, UFH, and ASA (10). In patients undergoingPCI within 72 h of randomization, eptifibatide administra-
tion resulted in a 31% reduction in the combined end pointof nonfatal MI or death at 30 days (17.7 vs. 11.6%, p 5 0.01).
The EPISTENT trial was designed to evaluate theefficacy of abciximab as an adjunct to elective coronarystenting (246,313). Of the nearly 2,400 patients who wererandomized, 20% of the stented patients had UA within48 h of the procedure. Patients were randomly assigned toeither stent deployment with placebo, stent plus abciximab,or PTCA plus abciximab. Nineteen percent of the PTCAgroup had provisional coronary stent deployment for asuboptimal angioplasty result. All stented patients in thistrial received oral ASA (325 mg) and oral ticlopidine(250 mg twice daily for 1 month). The adjunctive use ofabciximab was associated with a significant reduction in thecomposite clinical end point of death, MI, or urgentrevascularization. The 30-day primary end point occurred in10.8% of the stent-plus-placebo group, 5.3% of the stent-plus-abciximab group, and 6.9% of the PTCA-plus-abciximab group. Most of the benefit from abciximab wererelated to a reduction in the incidence of moderate to largeMI (CK .5 times the upper limit of normal or Q-waveMI); these reductions occurred in 5.8% of the stent-plus-placebo group, 2.6% of the balloon-plus-abciximab group,and 2.0% of the stent-plus-abciximab group.
At 1 year of follow-up, stented patients who receivedbolus and infusion abciximab had reduced mortality ratescompared with patients who received stents without abcix-imab (1.0% vs. 2.4%, representing a 57% risk reduction; p 50.037) (314). In diabetics, target vessel revascularization at 6months was markedly and significantly reduced (51%, p 50.02) in stented patients who received abciximab comparedwith those who did not. Although a similar trend was alsoobserved in nondiabetic patients, it did not reach statisticalsignificance.
In summary, data from both retrospective observationsand randomized clinical trials indicate that PCI can lead toangiographic success in most patients with UA/NSTEMI(Figs. 13 and 14). The safety of these procedures in thesepatients is enhanced by the addition of intravenous plateletGP IIb/IIIa receptor inhibitors to the standard regimen ofASA, heparin, and anti-ischemic medications.
C. Surgical Revascularization
Two randomized trials conducted in the early years ofCABG compared medical and surgical therapy in UA. TheNational Cooperative Study Group randomized 288 pa-tients at 9 centers between 1972 and 1976 (317). TheVeterans Administration (VA) Cooperative Study random-ized 468 patients between 1976 and 1982 at 12 hospitals(269,319–321). Both trials included patients with progres-sive or rest angina accompanied by ST-T–wave changes.Patients .70 years old or with a recent MI were excluded;the VA study included only men. In the National Cooper-ative Study, the hospital mortality rate was 3% for patientsundergoing medical therapy and 5% after CABG (p 5 NS).Follow-up to 30 months showed no differences in survival
1023JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina

rates between the treatment groups. In the VA CooperativeStudy, survival rates to 2 years were similar after medicaltherapy and CABG overall and in subgroups defined by thenumber of diseased vessels. A post hoc analysis of patientswith depressed LV function, however, showed a significantsurvival advantage with CABG regardless of the number ofbypassed vessels (321).
All randomized trials of CABG vs. medical therapy(including those in stable angina) have reported improvedsymptom relief and functional capacity with CABG. How-ever, long-term follow-up in these trials has suggested thatby 10 years, there is a significant attenuation of both thesymptom relief and survival benefits previously conferred byCABG, although these randomized trials reflect an earlierera for both surgical and medical treatment. Improvementsin anesthesia and surgical techniques, including internalthoracic artery grafting to the LAD, and improved intraop-erative myocardial protection with cold potassium cardio-plegia, are not reflected in these trials. In addition, theroutine use of heparin and ASA in the acute phase ofmedical therapy and the range of additional therapeuticagents that are now available (e.g., LMWH, GP IIb/IIIainhibitors) represent significant differences in current prac-tice from the era in which these trials were performed.
A meta-analysis was performed on the results of 6 trialsconducted between 1972 and 1978 to compare long-termsurvival in CAD patients treated medically or with CABG(142). A clear survival advantage was documented forCABG in patients with left main and 3-vessel coronarydisease that was independent of LV function. No survivaldifference was documented between the 2 therapies forpatients with 1- or 2-vessel coronary disease.
Pocock et al. (322) performed a meta-analysis on theresults of 8 randomized trials completed between 1986 and1993 and compared the outcomes of CABG and PTCA in3,371 patients with multivessel CAD before widespreadstent use. Many of these patients presented with UA. At1-year follow-up, no difference was documented betweenthe 2 therapies in cardiac death or MI, but a lower incidenceof angina and need for revascularization was associated withCABG.
The Bypass Angioplasty Revascularization Investigation(BARI) trial is the largest randomized comparison ofCABG and PTCA in 1,829 patients with 2- or 3-vesselCAD (323,324). UA was the admitting diagnosis in 64% ofthese patients, and 19% had treated diabetes. A statisticallysignificant advantage in survival without MI independent ofthe severity of presenting symptoms was observed in theentire group for CABG over PCI 7 years after study entry(84.4% vs. 80.9%, p 5 0.04) (325). However, subgroupanalysis demonstrated that the survival benefit seen withCABG was confined to diabetic patients treated withinsulin or oral hypoglycemic agents. At 7 years, the survivalrate for diabetics was 76.4% with CABG compared with55.7% among patients treated with PTCA (p 5 0.001). Inpatients without diabetes, survival rates were virtually iden-
tical (CABG vs. PTCA, 86.4% vs. 86.8%, p 5 0.71).Subsequent analysis of the Coronary Angioplasty versusBypass Revascularisation Investigation (CABRI) trial re-sults also showed a survival benefit for the use of CABG incomparison with PTCA in diabetic patients with multives-sel CAD (326). These observations have been confirmed ina study from Emory University, which showed that withcorrection for baseline differences, there were improvedsurvival rates for insulin-requiring patients with multivesseldisease who were revascularized with CABG rather thanwith PTCA (327) (see Section VI. C).
Other nonrandomized analyses have compared CABG,PTCA, and medical therapy. With statistical adjustment fordifferences in baseline characteristics of 9,263 consecutiveCAD patients entered into a large registry, the 5-yearsurvival rates were compared for patients who were treatedmedically and those who underwent PTCA and CABGbetween 1984 and 1990 (288). Patients with 3- or 2-vesseldisease with a proximal severe ($95%) LAD stenosistreated with CABG had significantly better 5-year survivalrates than did those who received medical treatment orPTCA. In patients with less severe 2-vessel CAD or with1-vessel CAD, either form of revascularization improvedsurvival relative to medical therapy. The 2 revascularizationtreatments were equivalent for patients with nonsevere2-vessel disease. PTCA provided better survival rates thanCABG in patients with 1-vessel disease except for thosewith severe proximal LAD stenosis, for whom the 2revascularization strategies were equivalent. However, inpatients with 1-vessel disease, all therapies were associatedwith high 5-year survival rates, and the differences amongthe treatment groups were very small.
Hannan et al. (289) compared 3-year risk-adjusted sur-vival rates in patients undergoing revascularization in thestate of New York in 1993. The 29,646 CABG patients and29,930 PTCA patients had different baseline and angio-graphic characteristics evaluated with Cox multivariablemodels. The anatomic extent of disease was the onlyvariable that interacted with the specific revascularizationtherapy that influenced long-term survival. Although thelimitations of such observational studies must be recog-nized, it is of interest that UA or diabetes did not result intreatment-related differences in long-term survival rates.Patients with 1-vessel disease not involving the LAD orwith ,70% LAD stenosis had statistically significant higheradjusted 3-year survival rates with PTCA (95.3%) than withCABG (92.4%). Patients with proximal LAD stenosis of$70% had statistically significant higher adjusted 3-yearsurvival rates with CABG than with PTCA regardless ofthe number of diseased coronary vessels. Patients with3-vessel disease had statistically significant higher adjusted3-year survival rates with CABG regardless of proximalLAD disease. Patients with other 1- or 2-vessel disease hadno treatment-related difference in survival rates.
Thus, large cohort trials with statistical adjustmentshowed that survival differences between CABG and PTCA
1024 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062

were related to the anatomic extent of disease, in contrast tothe randomized trials of multivessel disease that showed nodifferences. This difference may be due to the smallernumbers of patients in the randomized trials and, hence,their lower power and to the fact that a broad range ofangiographic characteristics were not included in the ran-domized trials in comparison with the patient cohortstudies. The location of a coronary stenosis in the LAD,especially if it is severe and proximal, appears to be acharacteristic associated with higher mortality rates and,therefore, with a more favorable outcome with CABG. Asalready noted, the finding in the BARI and CABRIrandomized trials that diabetes appeared to identify a subsetof patients who had a better outcome with CABG thanwith PTCA was not confirmed in the 2 cohort studies(323,324,326). Analysis of the diabetic subgroup was notproposed at the time of trial design in either the BARI orCABRI trial. Moreover, this treatment-related effect wasnot reproduced in the BARI registry population (328). Areasonable explanation is that in the cohort studies, physi-cians may be able to recognize characteristics of coronaryarteries of diabetic patients that will permit them to moresafely undergo one or another of the revascularizationtherapies. However, when all diabetic patients are randomlyassigned to therapies without the added insight of clinicaljudgment, a treatment advantage is apparent for CABG.Until further studies that compare newer percutaneousdevices (in particular, stents) and surgical techniques canmore clearly resolve these differences, it is reasonable toconsider CABG as the preferred revascularization strategyfor most patients with 3-vessel disease, especially if itinvolves the proximal LAD and patients with multivesseldisease and treated diabetes or LV dysfunction. Alterna-tively, it would be unwise to deny the advantages of PCI toa patient with diabetes and less severe coronary disease onthe basis of the current information.
An important consideration in a comparison of differentrevascularization strategies is that none of the large random-ized trials reflect the current practice of interventionalcardiology that includes the routine use of stents and theincreasing use of platelet receptor inhibitors. Coronarystenting improves procedural safety and reduces restenosisin comparison with PTCA. The adjuvant use of plateletinhibitors, particularly in high-risk patients, is also associ-ated with improved short- and intermediate-term out-comes. Although the effects of coronary stenting andplatelet GP IIb/IIIa inhibitors would have likely improvedthe PCI results observed, their added benefit relative toCABG cannot be assessed on the basis of the previouslyreported randomized trials or large registries. Refinement ofsurgical management with right internal mammary arterygrafts, radial artery grafts, retroperfusion, and less invasivemethodology may reduce the morbidity rates for CABG,but no recent advance has been shown to influence long-term survival more favorably than the current standardoperative technique. Therefore, decisions regarding appro-
priate revascularization strategies in the future will have tobe made on the basis of information that compares long-term outcome for these 2 techniques and the effects ofadjunctive pharmacotherapy.
D. Conclusions
In general, the indications for PCI and CABG inUA/NSTEMI are similar to those for stable angina(324,329–333). High-risk patients with LV systolic dys-function, patients with diabetes mellitus, and those with2-vessel disease with severe proximal LAD involvement orsevere 3-vessel or left main disease should be considered forCABG (Fig. 12). Many other patients will have less-severeCAD that does not put them at high risk for cardiac death.However, even less-severe disease can have a substantialnegative impact on the quality of life. Compared withhigh-risk patients, low-risk patients will receive negligiblyor very modestly increased chances of long-term survivalwith CABG. Therefore, in low-risk patients, quality of lifeand patient preferences are given more weight than are strictclinical outcomes in the selection of a treatment strategy.Low-risk patients whose symptoms do not respond well tomaximal medical therapy and who experience a significantnegative impact on their quality of life and functional statusshould be considered for revascularization. Patients in thisgroup who are unwilling to accept the increased short-termprocedural risks to gain long-term benefits or who aresatisfied with their existing capabilities should be managedmedically at first and followed carefully as outpatients.Other patients who are willing to accept the risks ofrevascularization and who want to improve their functionalstatus or to decrease symptoms may be considered appro-priate candidates for early revascularization.
V. HOSPITAL DISCHARGE AND POST–HOSPITALDISCHARGE CARE
The acute phase of UA/NSTEMI is usually over within 2months. The risk of progression to MI or the developmentof recurrent MI or death is highest during that period. At 1to 3 months after the acute phase, most patients resume aclinical course similar to that of patients with chronic stablecoronary disease (Fig. 3).
The broad goals during the hospital discharge phase, asdescribed in this section, are 2-fold: 1) to prepare the patientfor normal activities to the extent possible and 2) to use theacute event as an opportunity to reevaluate long-term care,particularly lifestyle and risk factor modification. Aggressiverisk factor modification is the mainstay of the long-termmanagement of stable CAD. Patients who have undergonesuccessful PCI with an uncomplicated course are usuallydischarged the next day, and patients who undergo uncom-plicated CABG are generally discharged 4 to 7 days afterCABG. Medical management of low-risk patients afternoninvasive stress testing and coronary arteriography cantypically be accomplished rapidly with discharge on the day
1025JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina

of or the day after testing. Medical management of ahigh-risk group of patients who are unsuitable for orunwilling to undergo revascularization may require a pro-longed hospitalization period to achieve the goals of ade-quate symptom control and minimization of the risk ofsubsequent cardiac events.
A. Medical Regimen
In most cases, the inpatient anti-ischemic medical regi-men used in the nonintensive phase (other than intravenousNTG) should be continued after discharge and the anti-platelet/anticoagulant medications should be changed to anoutpatient regimen. The goals for continued medical ther-apy after discharge relate to potential prognostic benefits(primarily shown for ASA, b-blockers, cholesterol-loweringagents, and ACEIs, especially for EF ,0.40), control ofischemic symptoms (nitrates, b-blockers, and calcium an-tagonists), and treatment of major risk factors such ashypertension, smoking, hyperlipidemia, and diabetes melli-tus (see later). Thus, the selection of a medical regimen isindividualized to the specific needs of each patient based onthe in-hospital findings and events, the risk factors forCAD, drug tolerability, or the type of recent procedure. Themnemonic ABCDE (Aspirin and antianginals; Beta-blockers and blood pressure; Cholesterol and cigarettes;Diet and diabetes; Education and exercise) has been foundto be useful in guiding treatment (26).
An effort by the entire staff (physicians, nurses, dietitians,pharmacists, rehabilitation specialists, and physical andoccupational therapists) is often necessary to prepare thepatient for discharge. Both the patient and family shouldreceive instructions about what to do if symptoms occur inthe future (333a). Direct patient instruction is importantand should be reinforced and documented with writteninstruction sheets. Enrollment in a cardiac rehabilitationprogram after discharge may enhance patient education andenhance compliance with the medical regimen.
Recommendations
Class I1. Drugs required in the hospital to control ischemia
should be continued after hospital discharge inpatients who do not undergo coronary revascular-ization, patients with unsuccessful revasculariza-tion, or patients with recurrent symptoms afterrevascularization. Upward or downward titration ofthe doses may be required. (Level of Evidence: C)
2. All patients should be given sublingual or sprayNTG and instructed in its use. (Level of Evidence: C)
3. Before discharge, patients should be informedabout symptoms of AMI and should be instructedin how to seek help if symptoms occur. (Level ofEvidence: C)
1. Long-Term Medical Therapy. Many patients withUA/NSTEMI have chronic stable angina at hospital dis-
charge. The management of the patient with stable CAD isdetailed in the ACC/AHA/ACP-ASIM Guidelines for theManagement of Patients With Chronic Stable Angina (26).The following are recommendations for pharmacotherapyto prevent death and MI.
Recommendations
Class I1. Aspirin 75 to 325 mg/d in the absence of contrain-
dications. (Level of Evidence: A)2. Clopidogrel 75 qd for patients with a contraindica-
tion to ASA. (Level of Evidence: B)3. b-Blockers in the absence of contraindications.
(Level of Evidence: B)4. Lipid-lowering agents and diet in post ACS pa-
tients, including patients post revascularization,with low-density lipoprotein (LDL) cholesterol of>130 mg/dL. (Level of Evidence: A)
5. Lipid-lowering agents if LDL cholesterol level afterdiet is >100 mg/dL. (Level of Evidence: C)
6. ACEIs for patients with CHF, LV dysfunction (EF<0.40), hypertension, or diabetes. (Level of Evi-dence: A)
A reduction in the rates of mortality and vascular eventswas reported in the Heart Outcomes Prevention Evaluation(HOPE) Study (163) with the long-term use of an ACEIin moderate-risk patients with CAD, many of whom hadpreserved LV function, as well as patients at high risk ofdeveloping CAD. Other agents that may be used inpatients with chronic CAD are listed in Table 21 and arediscussed in detail in the ACC/AHA/ACP-ASIM Guide-lines for the Management of Patients With Chronic StableAngina (26).
Although observational data suggest a protective effect ofhormone replacement therapy (HRT) for coronary events,the only randomized trial of HRT for secondary preventionof death and MI that has been completed (Heart andEstrogen/progestin Replacement Study [HERS]) failed todemonstrate a beneficial effect (334). Disturbingly, therewas an excess risk for death and MI early after HRT initiation.It is recommended that postmenopausal women who receiveHRT may continue but that HRT should not be initiated forthe secondary prevention of coronary events. There may,however, be other indications for HRT in postmenopausalwomen (e.g., prevention of flushing, osteoporosis).
B. Postdischarge Follow-Up
Recommendation
Class I1. Discharge instructions should include a follow-up
appointment. Low-risk medically treated patientsand revascularized patients should return in 2 to 6weeks, and higher-risk patients should return in 1to 2 weeks. (Level of Evidence: C)
1026 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062

2. Patients managed initially with a conservative strat-egy who experience recurrent unstable angina orsevere (CCS Class III) chronic stable angina de-spite medical management who are suitable forrevascularization should undergo coronary arte-riography. (Level of Evidence: B)
3. Patients who have tolerable stable angina or noanginal symptoms at follow-up visits should bemanaged with long-term medical therapy for stableCAD. (Level of Evidence: B)
The risk of death within 1 year can be predicted on thebasis of clinical information and the ECG. For 515 survi-vors of hospitalization for NSTEMI, risk factors includepersistent ST-segment depression, CHF, advanced age, andST-segment elevation at discharge (335). Patients with allhigh-risk markers present had a 14-fold greater mortalityrate than did patients with all markers absent. Elevatedcardiac TnT levels have also been demonstrated to provideindependent prognostic information for cardiac events at 1to 2 years. For patients with all ACS in a GUSTO-IIasubstudy, age, ST-segment elevation on admission, priorCABG, TnT, renal insufficiency, and severe COPD wereindependently associated with risk of death at 1 year(100,336). For UA/NSTEMI patients, prior MI, TnTpositivity, accelerated angina before admission, and recur-rent pain or ECG changes were independently associated
with risk of death at 2 years. Patients managed with aninitial conservative strategy (see Section III) should bereassessed at the time of return visits for the need for cardiaccatheterization and revascularization. Specifically, the pres-ence and severity of angina should be ascertained. Rates ofrevascularization during the first year have been reported tobe high (337). Long-term (7 years) follow-up of 282patients with UA demonstrated high event rates during thefirst year (MI 11%, death 6%, PTCA 30%, CABG 27%).However, after the first year, event rates were low (337).Independent risk factors for death/MI were age .70 years,diabetes, and male sex. Mental depression has also beenreported to be an independent risk factor for cardiac eventsafter MI and occurs in up to 25% of such patients (338).Patients recognized to be at high risk for a cardiac event afterdischarge deserve earlier and more frequent follow-up thanlow-risk patients.
The overall long-term risk for death or MI 2 months afteran episode of UA/NSTEMI is similar to that of other CADpatients with similar characteristics. van Domburg et al.(337) reported low rates of admission for recurrent chestpain (5%, 4%, 3%, and 2% at 1, 3, 5, and 7 years,respectively). When the patient has returned to the baselinelevel, typically 6 to 8 weeks after hospitalization, arrange-ments should be made for long-term regular follow-upvisits, as for stable CAD. Cardiac catheterization with
Table 21. Medications Used for Stabilized UA/NSTEMI
Anti-Ischemic and Antithrombotic/Antiplatelet Agent Drug Action Class/Level of Evidence
Aspirin Antiplatelet I/AClopidogrel* or ticlopidine Antiplatelet when aspirin is contraindicated I/Bb-Blockers Anti-ischemic I/AACEI EF ,0.40 or CHF
EF .0.40I/AIIa/B
Nitrates Antianginal I/CFor ischemic symptoms
Calcium antagonists (short-acting dihydropyridineantagonists should be avoided)
Antianginal I for ischemic symptomsWhen b-blockers are not successful
(level of evidence: B)Or contraindicated or cause unacceptable side
effects (level of evidence: C)Warfarin low intensity with or without aspirin Antithrombotic IIb/BDipyridamole Antiplatelet III/A
Agent Risk Factor Class/Level of Evidence
HMG-CoA reductase inhibitors LDL cholesterol .130 mg/dL I/AHMG-CoA reductase inhibitors LDL cholesterol 100–130 mg/dL IIa/CGemfibrozil HDL cholesterol ,40 mg/dL IIa/BNiacin HDL cholesterol ,40 mg/dL IIa/BNiacin or gemfibrozil Triglycerides .200 mg/dL IIa/BFolate Elevated homocysteine IIb/CAntidepressant Treatment of depression IIb/CTreatment of hypertension Blood pressure .135/85 mm Hg I/AHRT (initiation)† Postmenopausal state III/BHRT (continuation)† Postmenopausal state IIa/C
*Preferred to ticlopidine.†For risk reduction of CAD.
1027JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
coronary angiography is recommended for any of thefollowing situations: 1) significant increase in anginal symp-toms, including recurrent UA; 2) high-risk pattern (e.g.,$2-mm ST-segment depression, systolic blood pressuredecline of $10 mm Hg) on exercise test; 3) CHF; 4) anginawith mild exertion (inability to complete Stage 2 of theBruce protocol for angina); and 5) survivors of sudden cardiacdeath. Revascularization is recommended based on the coro-nary anatomy and ventricular function (see Section IV andACC/AHA/ACP-ASIM Guidelines for the Management ofPatients With Chronic Stable Angina [26]).
C. Use of Medications
Recommendations
Class I1. Before hospital discharge, patients and/or desig-
nated responsible caregivers should be providedwith well-understood instructions with respect tomedication type, purpose, dose, frequency, andpertinent side effects. (Level of Evidence: C)
2. Anginal discomfort lasting >2 or 3 min shouldprompt the patient to discontinue the activity orremove himself or herself from the stressful event.If pain does not subside immediately, the patientshould be instructed to take NTG. If the first tabletor spray does not provide relief within 5 min, thena second and third dose, at 5-min intervals, shouldbe taken. Pain that lasts >15 to 20 min or persistentpain despite 3 NTG doses should prompt thepatient to seek immediate medical attention bycalling 9-1-1 and going to the nearest hospital ED,preferably via ambulance or the quickest availablealternative. (Level of Evidence: C)
3. If the pattern of anginal symptoms change (e.g.,pain is more frequent or severe or is precipitated byless effort or now occurs at rest), the patient shouldcontact his or her physician to determine the needfor additional treatment or testing. (Level of Evi-dence: C)
Either formal or informal telephone follow-up can serveto reinforce in-hospital instruction, provide reassurance, andanswer the patient’s questions (339). If personnel and budgetresources are available, the healthcare team may considerestablishing a follow-up system in which nurses call patients onthe telephone approximately once a week for the first 4 weeksafter discharge. This structured program can gauge theprogress of the patient’s recovery, reinforce the CAD educationtaught in the hospital, address patient questions and concerns,and monitor progress in meeting risk factor modification goals.
D. Risk Factor Modification
Recommendations
Class I1. Specific instructions should be given on the following:
a) Smoking cessation and achievement or mainte-
nance of optimal weight, daily exercise, and diet(Level of Evidence: B)
b) HMG-CoA reductase inhibitors for LDL choles-terol >130 mg/dL (Level of Evidence: A)
c) Lipid-lowering agent if LDL cholesterol after dietis >100 mg/dL (Level of Evidence: B)
d) Hypertension control to a blood pressure of<130/85 mm Hg (Level of Evidence: A)
e) Tight control of hyperglycemia in diabetes (Levelof Evidence: B)
2. Consider the referral of patients who are smokers toa smoking cessation program or clinic and/or anoutpatient cardiac rehabilitation program. (Level ofEvidence: B)
Class IIa1. Gemfibrozil or niacin for patients with high-
density lipoprotein (HDL) cholesterol of <40mg/dL and triglycerides of >200 mg/dL. (Level ofEvidence: B)
The healthcare team should work with patients and theirfamilies to educate them regarding specific targets for LDLcholesterol, blood pressure, weight, and exercise. The familymay be able to further support the patient by makingchanges in risk behavior (e.g., cooking low-fat meals for theentire family, exercising together). This is particularly im-portant when a screening of the family members revealscommon risk factors, such as hyperlipidemia, hypertension,and obesity.
There is a wealth of evidence that cholesterol-loweringtherapy for patients with CAD and hypercholesterolemia(340) and for patients with mild cholesterol elevation (mean209 to 218 mg/dL) after MI and UA reduces vascular eventsand death (341,342). Patients should be educated regardingcholesterol reduction and their current and target choles-terol levels. Patients who have undergone PTCA or CABGderive benefit from cholesterol lowering (343) and deservespecial counseling lest they mistakenly believe that revascu-larization obviates the need for change. NCEP 2 recom-mends a target LDL cholesterol level ,100 mg/dL, alow-saturated-fat diet for persons with an LDL cholesterollevel .100 mg/dL, and the addition of medication forpersons with an LDL cholesterol level .130 mg/dL (343a,343b). The treatment of hypertriglyceridemia and lowHDL cholesterol (,35 mg/dL) with gemfibrozil hasresulted in reduced cardiovascular events in men withcoronary heart disease (217). Either niacin or gemfibrozilmay be added to the diet when fasting triglycerides are.200 mg/dL (5).
Despite the overwhelming evidence for the benefits ofstatin therapy in patients with elevated LDL cholesterollevels, almost no data exist about the timing of the initiationof therapy in ACS. Fewer than 300 patients have beenentered into the currently completed trials within 4 monthsof ACS. These trials excluded ACS patients in the acutephase because of several concerns. In the acute setting, the
1028 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062

LDL cholesterol level drops, so the implications of furtheracute depression of levels are unclear. A theoretical argu-ment can be made that the inhibition of vascular smoothmuscle cell proliferation with statins could prevent plaquestabilization, and the beneficial effects of statin therapy havenot been observed in the first several months of therapy inlong-term trials. These theoretical concerns must beweighed against substantial evidence that if lipid-loweringtherapy is not instituted in the acute setting, it often isforgotten. Another potential benefit of early treatment withstatins is the rapid improvement in endothelial functionthey induce. Before pharmacological LDL-lowering therapyis begun, a baseline of 2 or 3 fasting lipoprotein measure-ments should be obtained; metabolic stability should beattained before such therapy is begun (343c).
Blood pressure control is an important goal, and hyper-tensive patients should be educated regarding this goal(344). Systolic and diastolic blood pressures should be in thenormal range (systolic ,135 mm Hg, diastolic,85 mm Hg). Particular attention should be paid tosmoking cessation. Daly et al. (345) quantified the long-term effects of smoking on patients with ACS. Men ,60years old who continued to smoke had a risk of death fromall causes 5.4 times that of men who stopped smoking (p ,0.05). Referral to a smoking cessation program and the useof nicotine patches or gum are recommended (346). Bupro-pion, an anxiolytic agent and weak inhibitor of neuronaluptake of neurotransmitters, has been effective when addedto brief regular counseling sessions in helping patients toquit smoking. The treatment of 615 study subjects for 7weeks resulted in smoking cessation rates of 28.8% for the100 mg/d dosage and 44.2% for 300 mg/d dosage comparedwith 19.6% for placebo-assigned patients (p , 0.001) Theabstinence rate at 1 year was 23.0% for those treated with300 mg/d bupropion vs. 12.4% for those receiving placebo(346). Family members who live in the same householdshould also be encouraged to quit smoking to help reinforcethe patient’s effort and to decrease the risk of second-handsmoke for everyone.
Tight glucose control in diabetics during and after MI(DIGAMI study) has been shown to lower acute and 1-yearmortality rates in ACS (347). Tight glucose control (HbA1c,7.0%) reduces microvascular disease (348,349) and isstrongly recommended. The recently published UK Pros-pective Diabetes Study (UKPDS) (349–351) demonstratedthat the control of glycemia reduced diabetes-related events,including MI (16% reduction, p 5 0.052), for newlydetected type 2 diabetics aged 25 to 65 years withoutsymptomatic macrovascular disease.
Overweight patients should be instructed in a weight lossregimen, with emphasis on the importance of regular exerciseand a life-long prudent diet to maintain ideal weight.
Although there is an association of elevated homocysteineblood levels and CAD, a reduction in homocysteine levelswith folate has not yet been demonstrated to reduce the riskof CAD events (352,353).
Very often, patients will not ask their physicians or otherhealthcare providers about the resumption of sexual activityafter hospital discharge. When appropriate, patients need tobe reassured that sexual activity is still possible. The re-sumption of sexual activity can typically occur within 7 to 10days in stable patients. Nitrates and sildenafil should not beused together within 24 h of each other. Patients shouldavoid sildenafil if angina or CHF symptoms have recentlyincreased (134).
Recommendation
Class I1. Beyond the instructions for daily exercise, patients
require specific instruction on activities (e.g., heavylifting, climbing stairs, yard work, household activ-ities) that are permissible and those that should beavoided. Specific mention should be made regard-ing resumption of driving and return to work.(Level of Evidence: C)
Daily walking can be encouraged immediately after dis-charge. Driving regulations vary among states. Typically,patients may begin driving 1 week after discharge, but theymust comply with all state department of motor vehiclerestrictions, which may include the need to be accompaniedand to avoid stressful circumstances such as rush hours,inclement weather, night driving, heavy traffic, and highspeeds. Commercial air travel may be undertaken by stablepatients (without fear of flying) within the first 2 weeks ofdischarge if they travel with a companion, carry sublingualNTG, and request airport transportation to avoid rushing.
E. Medical Record
The patient’s medical record from the time of hospitaldischarge should indicate the discharge medical regimen,the major instructions about postdischarge activities andrehabilitation, and the patient’s understanding and plan foradherence to the recommendations. After resolution of theacute phase of UA/NSTEMI, the medical record shouldsummarize cardiac events, current symptoms, and medica-tion changes since hospital discharge or the last outpatientvisit and should document the plan for future care.
VI. SPECIAL GROUPS
A. Women
Recommendation
Class I1. Women with UA/NSTEMI should be managed in
a manner similar to men. Specifically, women, likemen with UA/NSTEMI, should receive ASA aresimilar in women and men. Indications for nonin-vasive and invasive testing are similar in womenand men. (Level of Evidence: B)
1029JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
Although at any age women have a lower incidence ofCAD than men, they account for a considerable proportionof UA/NSTEMI patients, and UA/NSTEMI is a seriousand common condition among women. It is important toovercome long-held notions that severe coronary manifes-tations are uncommon in this population; however, womenmay manifest CAD somewhat differently than men. Womenwho present with chest discomfort are more likely than men tohave noncardiac causes, as well as nonatherosclerotic cardiaccauses, such as coronary vasospasm (354–356). Women withCAD are, on average, older than men and are more likely tohave comorbidities such as hypertension, diabetes, and CHF(32,357–359); to manifest angina rather than AMI; and,among angina and MI patients, to have atypical symptoms.
1. Stress Testing. In general, ECG exercise testing is lesspredictive in women than in men (261,360–362), primarilybecause of the lower pretest probability of CAD. Breastattenuation may be a problem with thallium-201 stresstesting but not with dobutamine echocardiography. Stressechocardiography (dobutamine or exercise) is therefore anaccurate and cost-effective technique for CAD detection inwomen (261). Recommendations for noninvasive testing inwomen are the same as in men (see Section III) (26,363). Areport of 976 women who underwent treadmill exercisesuggests that the Duke Treadmill Score (DTS) providesaccurate diagnostic and prognostic estimates in women aswell as in men (364). The DTS actually performed betterfor women than for men in the exclusion of CAD. Therewere fewer low-risk women than men with any significantCAD ($1 vessel with $75% stenosis: 20% in women vs.47% in men, p , 0.001).
Regarding dobutamine stress echocardiography, pilotphase data from the Women’s Ischemia Syndrome Evalu-ation (WISE) study (365) indicated that in women, the testreliably detects multivessel disease (sensitivity 81.8%, similarto that in men) but not 1-vessel disease. Several studies haveindicated that women with positive stress tests tend not tobe evaluated as aggressively as men (366).
2. Management. In studies that span the spectrum ofCAD, women tend to receive less intensive pharmacologicaltreatment than men (357), which is perhaps related in partto a less serious view of the impact of CAD in women.Although the specifics vary regarding b-blockers and otherdrugs (32,357,366), a consistent (and disturbing) pattern isthat women are prescribed ASA as well as other antithrom-botic agents less frequently than men (32).
Although it has been widely believed that women fareworse with PCI and CABG than do men because oftechnical factors (e.g., smaller artery size, greater age, andmore comorbidities) (367–371), recent studies cast doubt onthis (32,358). In the case of PCI, it has been suggested thatangiographic success and late outcomes are similar inwomen and men, although in some series, early complica-tions occur more frequently in women (367,368,372–375).However, the outlook for women undergoing PTCA ap-
pears to have improved as evidenced by the NHLBI registry(376). Earlier studies of women undergoing CABG showedthat women were less likely to receive internal mammaryarteries or complete revascularization and had a highermortality rate (RRs 1.4 to 4.4) than men (367,368,372–380). However, more recent studies in CABG patients withACS show a more favorable outlook for women (see later)(32,358) than previously thought.
3. Data on UA/NSTEMI. Considerable clinical informa-tion about UA/NSTEMI in women has emerged from theTIMI III trial (32) (which examined the use of tissueplasminogen activator and invasive strategies in ACS) andthe TIMI III registry (357). There were 497 women in theformer population and 1,640 in the latter. As in other formsof CAD, women were older and had more comorbidities(diabetes and hypertension), as well as stronger familyhistories (32,357–359). Women were less likely to have hada previous MI or cardiac procedures (Fig. 15) (357) and hadless LV dysfunction. However, they presented with symp-toms of similar frequency, duration, pattern, and ST-segment changes to those of the men. As in other studies,medication use, most particularly ASA, was less in womenthan in men in the week before the event, during hospital-ization, and at discharge. However, no differences betweenmen and women were evident in the results of medicaltherapy. In the registry, women underwent exercise testing in asimilar proportion to that of men. The frequencies of stress testpositivity were also similar, although women were less likely tohave a high-risk stress test result. However, women were lesslikely to undergo angiography (RR 0.71, p , 0.001), perhapsrelated to the lower percentage with high-risk test results onnoninvasive testing (357).
Coronary angiograms in both the TIMI III trial andregistry, as well as in other studies (285,381), revealed lessextensive CAD in women, of whom a higher proportionhad no CAD. In the registry, women were also less likelythan men to undergo revascularization (RR 0.66, p ,0.001) (357); in the TIMI III trial (in which angiographywas mandated), there was no gender difference in thepercent of patients undergoing PTCA, but less CABG wasperformed in women, presumably because of a lower inci-dence of multivessel disease. Importantly, gender was not anindependent predictor of the outcome of revascularization.Thus, a key observation in the TIMI III trial and registry(32,357) was that gender was not an independent prognosticfactor, with outcomes of death, MI, and recurrent ischemiasimilar in women and men.
Two additional studies were consistent with the TIMIdata on interventions in ACS. A Mayo Clinic review of3,014 patients (941 women) with UA who underwent PCIreported that women had similar early and late results tomen (358). The BARI trial of 1,829 patients comparedPTCA and CABG, primarily in patients with UA, andshowed that the results of revascularization were, if any-thing, better in women than men, when corrected for other
1030 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
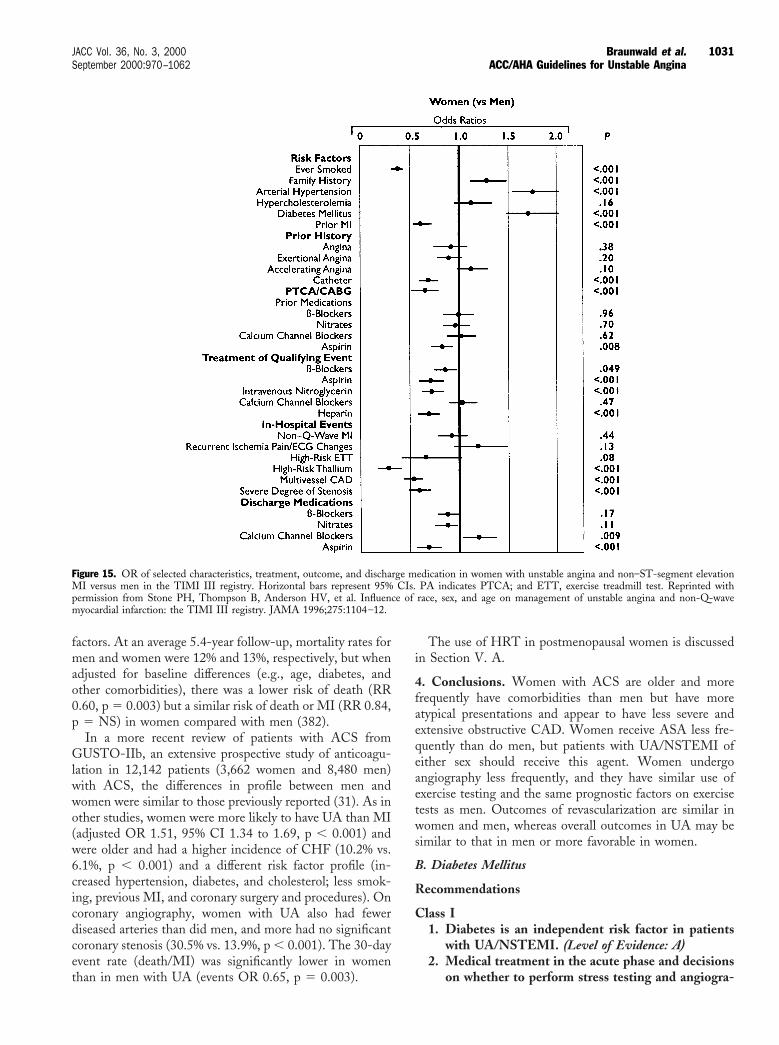
factors. At an average 5.4-year follow-up, mortality rates formen and women were 12% and 13%, respectively, but whenadjusted for baseline differences (e.g., age, diabetes, andother comorbidities), there was a lower risk of death (RR0.60, p 5 0.003) but a similar risk of death or MI (RR 0.84,p 5 NS) in women compared with men (382).
In a more recent review of patients with ACS fromGUSTO-IIb, an extensive prospective study of anticoagu-lation in 12,142 patients (3,662 women and 8,480 men)with ACS, the differences in profile between men andwomen were similar to those previously reported (31). As inother studies, women were more likely to have UA than MI(adjusted OR 1.51, 95% CI 1.34 to 1.69, p , 0.001) andwere older and had a higher incidence of CHF (10.2% vs.6.1%, p , 0.001) and a different risk factor profile (in-creased hypertension, diabetes, and cholesterol; less smok-ing, previous MI, and coronary surgery and procedures). Oncoronary angiography, women with UA also had fewerdiseased arteries than did men, and more had no significantcoronary stenosis (30.5% vs. 13.9%, p , 0.001). The 30-dayevent rate (death/MI) was significantly lower in womenthan in men with UA (events OR 0.65, p 5 0.003).
The use of HRT in postmenopausal women is discussedin Section V. A.
4. Conclusions. Women with ACS are older and morefrequently have comorbidities than men but have moreatypical presentations and appear to have less severe andextensive obstructive CAD. Women receive ASA less fre-quently than do men, but patients with UA/NSTEMI ofeither sex should receive this agent. Women undergoangiography less frequently, and they have similar use ofexercise testing and the same prognostic factors on exercisetests as men. Outcomes of revascularization are similar inwomen and men, whereas overall outcomes in UA may besimilar to that in men or more favorable in women.
B. Diabetes Mellitus
Recommendations
Class I1. Diabetes is an independent risk factor in patients
with UA/NSTEMI. (Level of Evidence: A)2. Medical treatment in the acute phase and decisions
on whether to perform stress testing and angiogra-
Figure 15. OR of selected characteristics, treatment, outcome, and discharge medication in women with unstable angina and non–ST-segment elevationMI versus men in the TIMI III registry. Horizontal bars represent 95% CIs. PA indicates PTCA; and ETT, exercise treadmill test. Reprinted withpermission from Stone PH, Thompson B, Anderson HV, et al. Influence of race, sex, and age on management of unstable angina and non-Q-wavemyocardial infarction: the TIMI III registry. JAMA 1996;275:1104–12.
1031JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
phy and revascularization should be similar indiabetic and nondiabetic patients. (Level of Evi-dence: C)
3. Attention should be directed toward tight glucosecontrol. (Level of Evidence: B)
4. For patients with multivessel disease, CABG withuse of the internal mammary arteries is preferredover PCI in patients being treated for diabetes.(Level of Evidence: B)
Class IIa1. PCI for diabetic patients with 1-vessel disease and
inducible ischemia. (Level of Evidence: B)2. Abciximab for diabetics treated with coronary
stenting. (Level of Evidence: B)
CAD accounts for 75% of all deaths in diabetics (32–34),and '20% to 25% of all patients with UA/NSTEMI arediabetic (197,324,357,383–385). Among patients with UA/NSTEMI, diabetics have more severe CAD (383,386,387),and diabetes is an important independent predictor foradverse outcomes (death, MI, or readmission with UA at 1year) (RR 4.9) (388–391). Also, many diabetics who presentwith UA/NSTEMI are post-CABG (392).
Diabetics tend to have more extensive noncoronary vas-cular comorbidities, hypertension, LV hypertrophy, cardio-myopathy, and CHF. In addition, autonomic dysfunction,which occurs in approximately one third of diabetics,influences heart rate and blood pressure, raises the thresholdfor the perception of angina, and may be accompanied byLV dysfunction (393–395). On coronary angioscopy, dia-betic patients with UA have a greater proportion of ulcer-ated plaques (94% vs. 60%, p 5 0.01) and intracoronarythrombi (94% vs. 55%, p 5 0.004) than nondiabetics. Thesefindings suggest a higher risk of instability (396).
Although b-blockers may mask the symptoms of hypo-glycemia or lead to it by blunting the hyperglycemicresponse, they should nevertheless be used with appropriatecaution in diabetics with ACS. Diuretics that cause hypo-kalemia may inhibit insulin release and thereby worsenglucose intolerance.
1. Coronary Revascularization. Approximately 20% of allpatients who undergo CABG (397) and PCI (368,369,372,373,386,387) have diabetes. Data regarding outcomesare complex. In the Coronary Artery Surgery Study (CASS)of CABG, diabetics had a 57% higher mortality rate thannondiabetics. A striking advantage for CABG over PTCAwas found in treated diabetics in the BARI trial (383), arandomized trial of PTCA vs. CABG in 1,829 stablepatients with multivessel disease, of whom 19% were dia-betics (see Section IV). Diabetics, as in other studies, hadincreased comorbidity rates. Five years after randomization,patients who required treatment for diabetes had a lowersurvival rate than nondiabetics (73.1% vs. 91.3%, p ,0.0001), whereas survival rates in nondiabetics and diabeticswho did not require hypoglycemic treatment were similar
(93.3% vs. 91.1%, p 5 NS). Outcomes for CABG in treateddiabetics were far better than those for PTCA (80.6% vs.65.5% survival, p 5 0.0003). An interesting finding was thatthe mortality rate during the 5.4 years of the study indiabetics who received SVGs (18.2%) was similar to that ofpatients who underwent PTCA (20.6%), whereas the mor-tality rate in patients who received internal mammaryarteries was much lower (2.9%). Results of the EmoryAngioplasty versus Surgery Trial (EAST) at 8 years showeda similar trend but were less conclusive (398). The increasedmortality rate noted in randomized trials in PTCA-treateddiabetics has been confirmed in a registry study from EmoryUniversity (327). Uncorrected, there was little difference inlong-term mortality rates. The CABG patients had moresevere disease, and with correction for baseline differences,there was an improved survival rate in insulin-requiringpatients with multivessel disease who were revascularizedwith CABG rather than with PTCA. That the moreseverely diseased patients, in a nonrandomized registry,were selectively sent more often for CABG than for PTCAprobably represents good clinical decision making.
A 9-year follow-up of the NHLBI registry showed asimilar disturbing pattern for diabetics undergoing PTCA.Immediate angiographic success and completeness of revas-cularization were similar, but compared with nondiabetics,diabetics (who, again, had more severe CAD and comor-bidities) had increased rates of hospital mortality (3.2% vs.0.5%), nonfatal MI (7.0% vs. 4.1%), death and MI (10.0%vs. 4.5%), and the combined end point of death, MI, andCABG (11% vs. 6.7%, p , 0.01 for all). At 9 years, rates ofmortality (35.9% vs. 17.9%), MI (29% vs. 18.5%), repeatPTCA (43.0% vs. 36.5%), and CABG (37.6% vs. 27.4%)were all higher in diabetics than in nondiabetics (386).
However, as pointed out in Section IV, other data pointto less of a differential effect of PCI in diabetics. Forexample, data from the BARI registry varied from those ofthe trial. In the registry, there was no significant differencein cardiac survival for diabetics undergoing PTCA (92.5%)and CABG (94%) (NS) (328,399). In the Duke Universityregistry, patients with diabetes and PTCA or CABG werematched with the BARI population. The outcome indiabetics was worse than that in nondiabetics with eitherCABG or PTCA, but there was no differential effect. The5-year survival rate for PTCA and CABG adjusted forbaseline characteristics was 86% and 89% in diabetics and92% and 93% in nondiabetics, respectively (400).
Stents may offer diabetics a much improved outcome forPCI. In a recent study with historical controls, the outcomeafter coronary stenting was superior to that after PTCA indiabetics, and the restenosis rate after stenting was reduced(63% vs. 36%, diabetics vs. nondiabetics with balloonPTCA at 6 months, p 5 0.0002) compared with 25% and27% with stents (p 5 NS) (398). On the other hand,diabetics who underwent atherectomy had a substantialrestenosis rate (60% over 6 months) (401).
Finally, 3 recent trials have shown that abciximab con-
1032 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
siderably improved the outcome of PCI in diabetics. In theEPILOG trial, abciximab resulted in a greater decline indeath/MI over 6 months after PTCA in diabetics (hazardratio 0.36, 95% CI 0.21 to 0.61) than in nondiabetics (0.60,95% CI 0.44 to 0.829) (402). Similar results have beenreported for tirofiban in the PRISM-PLUS trial (314).EPISTENT was a randomized trial that compared stentplus placebo with stent plus abciximab and balloon plusabciximab in 2,399 patients, of whom 20.5% had diabetesand 20.3% had UA (246). The 30-day event rate (death,MI, urgent revascularization) in diabetics declined from12.1% (stent plus placebo) to 5.6% (stent plus abciximab)(p 5 0.040). At 6 months, the drug reduced revasculariza-tion of target arteries in diabetics (16.6% vs. 8.1%, p 50.02). Death or MI was reduced to a similar degree indiabetics as that of nondiabetics (313). These benefits weremaintained at 1 year (403). Thus, in the 6-month data, thedrug, as well as stents, considerably improved the safety ofPCI in diabetics.
2. Conclusions. Diabetes occurs in about one fifth ofpatients with UA/NSTEMI and is an independent predic-tor of adverse outcomes. It is associated with more extensiveCAD, unstable lesions, frequent comorbidities, and lessfavorable long-term outcomes with coronary revasculariza-tion, especially with PTCA. It is unclear whether thesedifferences are due to more frequent restenosis and/or severeprogression of the underlying disease (386). The use ofstents, particularly with abciximab, appears to provide morefavorable results in diabetics, although more data areneeded. Clinical outcomes with CABG, especially with theuse of 1 or both internal mammary arteries, are better thanthose with PTCA but are still less favorable than innondiabetics.
C. Post-CABG Patients
Recommendations
Class I1. Medical treatment for post-CABG patients should
follow the same guidelines as for non–post-CABGpatients with UA/NSTEMI. (Level of Evidence: C)
2. Because of the many anatomic possibilities thatmight be responsible for recurrent ischemia, thereshould be a low threshold for angiography in post-CABG patients with UA/NSTEMI. (Level of Evi-dence: B)
Class IIa1. Repeat CABG is recommended for multiple SVG
stenoses, especially when there is significant steno-sis of a graft that supplies the LAD. PCI isrecommended for focal saphenous vein stenosis.(Level of Evidence: C)
2. Stress testing should generally involve imaging inpost-CABG patients. (Level of Evidence: C)
Overall, up to 20% of patients presenting with UA/NSTEMI have previously undergone CABG (392). Con-versely, '20% of post-CABG patients develop UA/NSTEMI during an interval of 7.5 years (404), with ahighly variable postoperative time of occurrence (405).Post-CABG patients who present with UA/NSTEMI areat higher risk, with more extensive CAD and LV dysfunc-tion than those patients who have not previously undergonesurgery.
1. Pathological Findings. Pathologically, intimal hyper-plasia or atherosclerosis may develop in SVGs, and there isa particular tendency for thrombotic lesions to develop inthese vessels (in 72% of grafts resected in 1 study) (406–409). In addition, post-CABG patients may develop ath-erosclerosis in their native vessels and this may also lead toUA/ NSTEMI (409,410). However, obstructive lesions aremore likely to occur in SVGs (53% within 5 years, 76% at5 to 10 years, 92% at .10 years) (411). Spasm in grafts ornative vessels (412,413) and technical complications mayalso play a role in the development of UA/NSTEMI duringthe early postoperative period (404,414). Both angioscopicand angiographic findings indicate that SVG disease is aserious and unstable process. Angioscopically, friableplaques occur uniquely in SVGs (44% vs. 0% in nativecoronary arteries), whereas rough and white plaques occur inboth SVGs and native coronary arteries (415). Angio-graphically, the SVGs more frequently have complex lesions(i.e., overhanging edges, irregular borders, ulcerations, orthrombosis), thrombi (37% vs. 12%, p 5 0.04), and totalocclusions (49% vs. 24%, p 5 0.02) (411).
2. Clinical Findings and Approach. Compared with UA/NSTEMI patients without prior CABG, post-CABG pa-tients are more often male (presumably because more menthan women have undergone CABG), older, and diabetic.They have more extensive native vessel CAD and moreprevious MIs and LV dysfunction. Symptomatically, thesepatients have more prolonged chest pain than ACS patientswithout prior CABG. More than 30% of post-CABGpatients have resting ECG abnormalities, and ECG stresstests are therefore less conclusive (416). However, a test thatbecomes positive after having been negative is helpful in thediagnosis of ischemia. Myocardial stress perfusion imagingand dobutamine echocardiography are often helpful diag-nostically (417).
The outcomes of UA/NSTEMI in post-CABG patientsare less favorable than those in patients who have notundergone CABG. There is a high rate of embolization ofatherosclerotic material from friable grafts at the time ofintervention, making these procedures more difficult andassociated with higher rates of complications (418). In 1matched-control study of UA, the initial course was similar,but post-CABG patients had twice the incidence of adverseevents (death, MI, recurrent UA) during the first year. Thiswas attributed to a lower rate of complete revascularization,which was possible in only 9 of 42 post-CABG patients
1033JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina

compared with 39 of 52 patients who had not previouslyundergone CABG (p 5 0.001) (405). Results were direc-tionally similar in the TIMI III registry of ACS, in which16% of patients were post-CABG. Here again, early out-comes in post-CABG patients and others were equivalent,but at 1 year, 39.3% vs. 30.2% experienced adverse events(death, MI, recurrent ischemia) (p 5 0.002) (419).
Revascularization with either PCI or reoperation is oftenindicated and possible in post-CABG patients with UA/NSTEMI. In a randomized control trial that comparedstents with PTCA of obstructed SVGs, there was nostatistically significant difference in restenosis during 6months, although a trend favored stents: 34% vs. 46%.Although hemorrhagic complications were higher in thestent group, clinical outcomes (freedom from MI or repeatrevascularization) were better (73% vs. 58%, p 5 0.03)(420). Reoperation of patients with stenotic SVGs has beensuccessful in reducing symptoms of recurrent ischemia, andit appears to improve survival rates in patients .5 years aftersurgery, especially with disease in the LAD, for whichsurvival rates were 74% vs. 53% (p 5 0.004) (reoperated vs.nonreoperated post-CABG patients) (421,422).
3. Conclusions. Post-CABG patients, especially thosewith only SVGs, are at high risk of UA/NSTEMI. There isa higher likelihood of disease in SVGs than in native arteriesand this difference increases with postoperative time. Patho-logically and angiographically, disease in SVGs has charac-teristics associated with instability. There also are difficultieswith treadmill ECG testing and less favorable outcomeswith repeat revascularization than in patients who have notundergone previous CABG.
D. Elderly Patients
Recommendations
Class I1. Decisions on management should reflect consider-
ations of general health, comorbidities, cognitivestatus, and life expectancy. (Level of Evidence: C)
2. Attention should be paid to altered pharmacokinet-ics and sensitivity to hypotensive drugs. (Level ofEvidence: B)
3. Intensive medical and interventional managementof ACS may be undertaken but with close observa-tion for adverse effects of these therapies. (Level ofEvidence: B)
In this discussion, patients $75 years are considered to be“elderly,” although a number of studies have used othercutoff ages, such as 65 or 70 years. Elderly persons constituteabout one tenth of ACS patients (357) and present with anumber of special problems. They are more likely to havecardiac and noncardiac comorbidities; these include a di-minished b-sympathetic response, increased cardiac after-load due to decreased arterial compliance and arterial
hypertension, cardiac hypertrophy, and ventricular dysfunc-tion, especially diastolic dysfunction (423).
CAD is more common and more severe in elderlypersons, who, when they develop UA/NSTEMI, are alsomore likely to present with atypical symptoms, includingdyspnea and confusion, rather than with the ischemic chestpain that is typical for younger patients. There also is ahigher incidence of unrecognized prior MI than in youngerpatients (424). Conversely, comorbid conditions such ashiatus hernia are also more frequent and may be associatedwith chest pain at rest and may mimic UA. The greaterlikelihood of comorbidity in elderly persons (e.g., COPD,renal failure, and cerebral disease) also increases the mor-bidity and mortality rates for cardiac events and interven-tions in this population.
It may be difficult for elderly persons to perform exercisetests because of muscle weakness and orthopedic problems.In such patients, a pharmacological stress test may beperformed (see Section III). The higher prevalence ofpreexisting resting ECG abnormalities (389), arrhythmias(425,426), and cardiac hypertrophy complicates the inter-pretation of stress ECG and may require the use of imaging.
1. Pharmacological Management. Reductions in cardiacoutput and in renal and hepatic perfusion and functionreduce the elimination of drugs in elderly persons. Drugssuch as propranolol that undergo first-pass hepatic metab-olism exhibit increased bioavailability (427). Pharmacody-namic responses to drugs are influenced by the lower cardiacoutput, plasma volume, and vasomotor tone and the bluntedbaroreceptor and b-adrenergic responses.
Elderly persons are particularly vulnerable to drugs withhypotensive actions (e.g., nitrates and calcium antagonists)and cerebral effects (e.g., b-blockers). Responses tob-blockers are influenced by 2 competing factors. Theremay be a blunted response to b-blockers because of de-creased adrenergic activity in elderly persons. On the otherhand, baseline sympathetic tone may be decreased. Thus,the magnitude of response to b-blockers is not entirelypredictable. Clearance of warfarin may be reduced, andsensitivity to it may be increased with age (428); heparindosage requirements also appear to be reduced (210).Overall, however, it should be emphasized that all of thedrugs commonly used in the management of youngerpatients with UA/NSTEMI are useful in elderly patients,provided these differences are recognized and proper pre-cautions are taken (i.e., beginning with lower doses than inyounger patients and, in particular, careful observation fortoxicity).
2. Observations in UA/NSTEMI. The TIMI III registry(357) provided data on elderly patients (.75 years old), who(by design) composed 25% of the 3,318 patients. This grouphad fewer atherosclerotic risk factors (smoking, hypercho-lesterolemia, family history), more previous angina, andfewer previous procedures (Fig. 16) (357), and in otherstudies, they had more CHF (429,430). They were less
1034 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
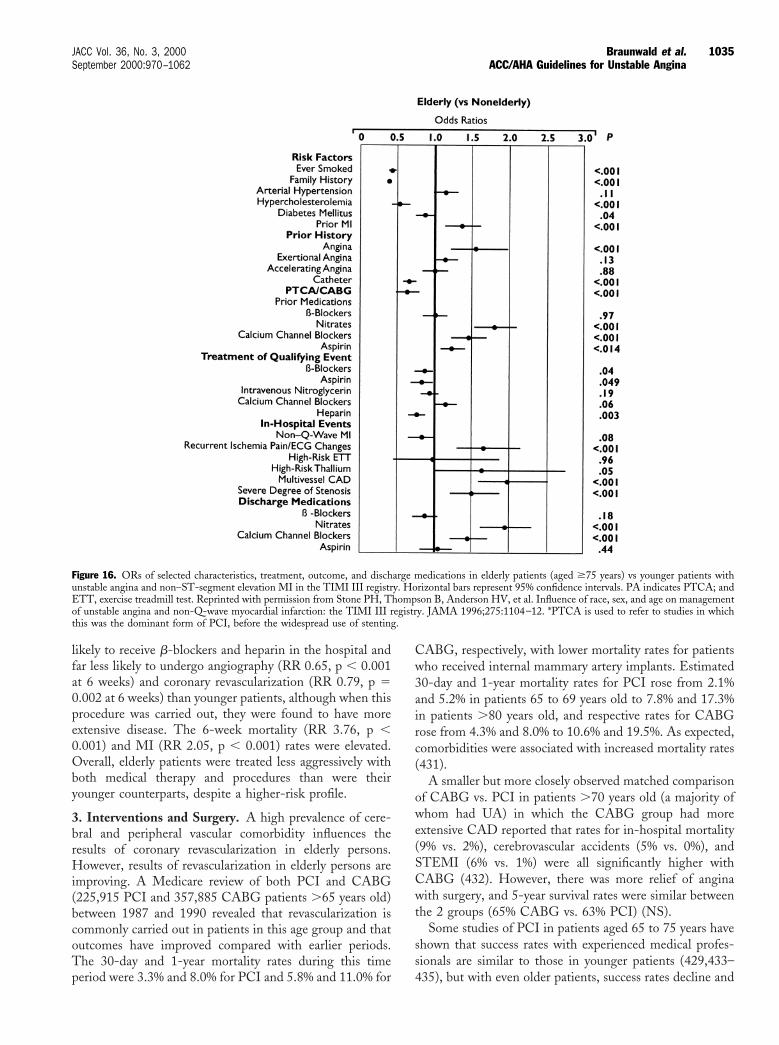
likely to receive b-blockers and heparin in the hospital andfar less likely to undergo angiography (RR 0.65, p , 0.001at 6 weeks) and coronary revascularization (RR 0.79, p 50.002 at 6 weeks) than younger patients, although when thisprocedure was carried out, they were found to have moreextensive disease. The 6-week mortality (RR 3.76, p ,0.001) and MI (RR 2.05, p , 0.001) rates were elevated.Overall, elderly patients were treated less aggressively withboth medical therapy and procedures than were theiryounger counterparts, despite a higher-risk profile.
3. Interventions and Surgery. A high prevalence of cere-bral and peripheral vascular comorbidity influences theresults of coronary revascularization in elderly persons.However, results of revascularization in elderly persons areimproving. A Medicare review of both PCI and CABG(225,915 PCI and 357,885 CABG patients .65 years old)between 1987 and 1990 revealed that revascularization iscommonly carried out in patients in this age group and thatoutcomes have improved compared with earlier periods.The 30-day and 1-year mortality rates during this timeperiod were 3.3% and 8.0% for PCI and 5.8% and 11.0% for
CABG, respectively, with lower mortality rates for patientswho received internal mammary artery implants. Estimated30-day and 1-year mortality rates for PCI rose from 2.1%and 5.2% in patients 65 to 69 years old to 7.8% and 17.3%in patients .80 years old, and respective rates for CABGrose from 4.3% and 8.0% to 10.6% and 19.5%. As expected,comorbidities were associated with increased mortality rates(431).
A smaller but more closely observed matched comparisonof CABG vs. PCI in patients .70 years old (a majority ofwhom had UA) in which the CABG group had moreextensive CAD reported that rates for in-hospital mortality(9% vs. 2%), cerebrovascular accidents (5% vs. 0%), andSTEMI (6% vs. 1%) were all significantly higher withCABG (432). However, there was more relief of anginawith surgery, and 5-year survival rates were similar betweenthe 2 groups (65% CABG vs. 63% PCI) (NS).
Some studies of PCI in patients aged 65 to 75 years haveshown that success rates with experienced medical profes-sionals are similar to those in younger patients (429,433–435), but with even older patients, success rates decline and
Figure 16. ORs of selected characteristics, treatment, outcome, and discharge medications in elderly patients (aged $75 years) vs younger patients withunstable angina and non–ST-segment elevation MI in the TIMI III registry. Horizontal bars represent 95% confidence intervals. PA indicates PTCA; andETT, exercise treadmill test. Reprinted with permission from Stone PH, Thompson B, Anderson HV, et al. Influence of race, sex, and age on managementof unstable angina and non-Q-wave myocardial infarction: the TIMI III registry. JAMA 1996;275:1104–12. *PTCA is used to refer to studies in whichthis was the dominant form of PCI, before the widespread use of stenting.
1035JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
complications rates rise. In a recent VA study, in patients.70 years old, the angiographic success rate was 86%, theclinical success rate was 79%, and the in-hospital mortalityrate was 11% (all rates were less favorable than those foryounger patients), and the urgent CABG rate was ,1%(436). In 1 report of 26 patients .90 years old, of whom 20had UA, the procedural success rate for PTCA was 92%,whereas the acute clinical success rate was only 65%, with anin-hospital mortality rate of 23% (437).
On the other hand, a Mayo Clinic review of PCI inpatients .65 years old (of whom 75% had UA) revealed anoverall success rate of 93.5%, an immediate in-hospitalmortality rate of 1.4%, and a need for emergency CABGrate of only 0.7%. Angiographic outcome changed littlebetween the 65- to 69-year-old group and the .75-year-oldgroup, and the 1-year event rate (death, MI, CABG, repeatPCI, or severe angina) was 45.1% in all patients .65 yearsold (429). Predictors of outcomes (i.e., extent and severity ofCAD and comorbidities) after PCI in the elderly were thesame as those in younger patients (435). Similarly, a reviewof coronary stenting in the elderly reported that proceduralsuccess rates were high (95% to 98%) and periproceduralcomplication rates were low (MI 1.2% to 2.8%, urgentCABG 0.9% to 1.8%, repeat PCI 0% to 0.6%) in the elderlywith little difference between those .75 years old and those,65 years old (430). Subgroup analyses in both TIMI IIIB(19) and FRISC II (278) showed a greater advantage of theinvasive strategy in patients .65 years old.
A review of 15,679 CABG procedures carried out inpatients .70 years old from The Toronto Hospital (438)reported encouraging results. Operative mortality rates de-clined from 7.2% in 1982 to 1986 to 4.4% in 1987 to 1991(from 17.2% to 9.1% for high-risk patients) but showedlittle further change in the period of 1992 to 1996. Predic-tors of operative death (LV dysfunction, previous CABG,peripheral vascular disease, and diabetes) were similar tothose in younger patients. When adjusted for these riskfactors, age (i.e., a comparison of patients .75 years oldwith those 70 to 74 years old) was not a significant riskfactor.
In octogenarians, early mortality rates with CABG werefound to be '2.5 times those in patients 65 to 70 years old(431); stroke occurred in '8% (439), and less seriouscerebral complications were even more common (433,440).However, in a review of patients studied between 1985 and1989, the 3-year survival rate for octogenarian CABGpatients was better than that in comparably aged patientswith CAD who did not undergo surgery (77% vs. 55%, p 50.0294) (440), and in another study, the quality of life ofpatients 80 to 93 years old was improved with CABG (441).
4. Conclusions. Elderly patients with UA/NSTEMI tendto have atypical presentations of disease, substantial comor-bidity, ECG stress tests that are more difficult to interpret,and different responses to pharmacological agents comparedwith younger patients. Their outcomes with interventions
and surgery are not as favorable as those of younger patients,in part because of greater comorbidities. However, coronaryrevascularization can be performed when the same group ofprognostic risk factors that play a role in the younger agegroup are taken into account. The approach to thesepatients also must consider general medical and mentalstatus and anticipated life expectancy. Very frail elderlypatients represent a high-risk group and should be evaluatedfor revascularization on a case-by-case basis. In many ofthese patients, even those with diffuse coronary arterialdisease, PCI, with its lower morbidity rates, may be pref-erable to CABG. In ESSENCE (169) and TIMI 11B(170), the benefits or LMWH in patients .65 year old wereparticularly impressive. In the case of platelet GP IIb/IIIainhibitors, the relative benefits for older patients weresimilar to those of younger patients, but with the higherevent rate in elderly patients, this translated into a greaterabsolute benefit.
E. Cocaine
Recommendations for Patients With Chest Pain AfterCocaine Use
Class I1. NTG and oral calcium antagonists for patients with
ST-segment elevation or depression that accompa-nies ischemic chest discomfort. (Level of Evidence:C)
2. Immediate coronary arteriography, if possible, inpatients whose ST segments remain elevated afterNTG and calcium antagonists; thrombolysis (withor without PCI) if thrombus is detected. (Level ofEvidence: C)
Class IIa1. Intravenous calcium antagonists for patients with
ST-segment deviation suggestive of ischemia.(Level of Evidence: C)
2. b-Blockers for hypertensive patients (systolic bloodpressure >150 mm Hg) or those with sinus tachy-cardia (pulse >100 min21). (Level of Evidence: C)
3. Thrombolytic therapy if ST segments remain ele-vated despite NTG and calcium antagonists andcoronary arteriography is not possible. (Level ofEvidence: C)
4. Coronary arteriography, if available, for patientswith ST-segment depression or isolated T-wavechanges not known to be old and who are unre-sponsive to NTG and calcium antagonists. (Level ofEvidence: C)
Class III1. Coronary arteriography in patients with chest pain
without ST-T–wave changes. (Level of Evidence: C)
The use of cocaine is associated with a number of cardiaccomplications that can produce myocardial ischemia andcan cause and present as UA/NSTEMI (442–445). The
1036 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062

widespread use of cocaine makes it mandatory to considerthis cause, because its recognition mandates special man-agement.
The action of cocaine is to block presynaptic reuptake ofneurotransmitters such as norepinephrine and dopamine,producing excess concentrations at the postsynaptic recep-tors that lead to sympathetic activation and the stimulationof dopaminergic neurons (446). There may also be a directcontractile effect on vascular smooth muscle (443). Detox-ification occurs with plasma and liver cholinesterases, whichform metabolic products that are excreted in the urine.Infants, elderly patients, and patients with hepatic dysfunc-tion lack sufficient plasma cholinesterase to metabolize thedrug (447) and therefore are at high risk of adverse effectswith cocaine use.
1. Coronary Artery Spasm. The basis for coronary spasmhas been demonstrated in both in vitro (447) and in vivo(443,448–452) experiments in animals and humans. Re-versible vasoconstriction of rabbit aortic rings has beendemonstrated with cocaine in concentrations of 1023 to1028 mol/L. Pretreatment with calcium antagonists mark-edly inhibits the cocaine-induced vasoconstriction. Coro-nary injection of cocaine produces vasoconstriction inminiswine with experimentally induced nonocclusive ath-erosclerotic lesions (453).
Nademanee et al. (454) performed 24-h ECG monitor-ing in 21 male cocaine users after admission to a substanceabuse treatment center and found that 8 had frequentepisodes of ST-segment elevation, most during the first 2weeks of withdrawal. In cocaine users with prolongedmyocardial ischemia, coronary arteriography may revealcoronary artery spasm with otherwise normal appearingcoronary arteries or with underlying minimally obstructivecoronary atherosclerosis (443,445,448). The cocaine-induced increase in coronary vascular resistance is reversedwith calcium antagonists (449,455). Cocaine increases theresponse of platelets to arachidonic acid, thus increasingthromboxane A2 production and platelet aggregation (456).In addition, reversible combined reduction in protein C andantithrombin III has been observed in patients withcocaine-related arterial thrombosis (457). All of these effectsfavor coronary thrombosis (443,450,458). Coronary throm-bus may also develop as a consequence of coronary spasm.
Cocaine users may develop ischemic chest discomfortthat is indistinguishable from the UA/NSTEMI secondaryto coronary atherosclerosis. The patient who presents withprolonged myocardial ischemia should be questioned aboutthe use of cocaine. In a study by Hollander et al., thepresence or absence of cocaine use was assessed in only 13%of patients who presented to the ED with chest pain (458).Table 22 lists the clinical characteristics of a typical patientwith cocaine-related chest pain or MI (445).
Most patients who present to the ED with cocaine-associated chest pain do not develop MI (460); MI devel-
opment has been reported to occur in 6% of such patients(445).
Accelerated coronary atherosclerosis has been reported inchronic users of cocaine (461,462); coronary artery spasm ismore readily precipitated at sites of atherosclerotic plaques(448). Cocaine causes sinus tachycardia, an increase in bloodpressure, and myocardial contractility, thereby increasingmyocardial oxygen demand (449). These increases mayprecipitate myocardial ischemia and UA/NSTEMI in boththe presence and absence of obstructive coronary atheroscle-rosis and coronary spasm.
Aortic dissection (463) and coronary artery dissection(443,463) have been reported as consequences of cocaineuse. Other reported cardiac complications are myocarditis(462) and cardiomyopathy (464,465).
2. Treatment. When a patient with or suspected of cocaineuse is seen in the ED with chest pain compatible withmyocardial ischemia and ST-segment elevation, NTG and acalcium antagonist (e.g., 20 mg diltiazem) should be ad-ministered intravenously (443,452). If there is no response,immediate coronary arteriography should be performed, ifpossible. If thrombus is present, thrombolytic agents areadministered if there are no contraindications (466, 467). Ifcatheterization is not available, thrombolytic agents may beconsidered.
If the ECG is normal or shows only minimal T-wavechanges and there is a history of chest pain compatible withacute myocardial ischemia, the patient should receive NTGand an oral calcium antagonist and be observed. Aftercocaine use, increased motor activity, skeletal muscle injury,and rhabdomyolysis can occur, causing CK and evenCK-MB elevation in the absence of MI (468). TnI or TnTis more specific for myocardial injury and therefore ispreferred. Blood should be drawn twice for serum markersof myocardial necrosis at 6-h intervals. If the ECG showsST-segment changes and the biochemical markers arenormal, the patient should be observed in the hospital in amonitored bed for 24 h; most complications will occurwithin 24 h (459). If the patient’s clinical condition isunchanged and the ECG remains unchanged after 24 h, thepatient can be discharged (469).
Many observers believe that b-blockers are contraindi-cated in cocaine-induced coronary spasm, because there is
Table 22. Clinical Characteristics in the Typical Patient WithCocaine-Related Chest Pain, UA, or MI
Young age, usually ,40 yearsMale genderCigarette smokers, but no other risk factors for atherosclerosisChronic or first-time cocaine userSymptom onset minutes or even several hours after cocaine useAssociated with all routes of administrationMay occur with small or large dosesOften associated with concomitant use of cigarettes and/or alcohol
Reprinted with permission from Pitts WR, Lange RA, Cigarroa JE, Hillis LD.Cocaine-induced myocardial ischemia and infarction: pathophysiology, recognition,and management. Prog Cardiovasc Dis 1997;40:65–76.
1037JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
evidence from a single double-blind, randomized, placebo-controlled trial that b-adrenergic blockade augmentscocaine-induced coronary artery vasoconstriction (470).Others believe that if the patient has a high sympatheticstate with sinus tachycardia and hypertension, thenb-blockers should be used (443). Labetalol, an a/b-blocker,has been advocated, but in the doses commonly used, itsb-adrenergic–blocking action predominates over its a-ad-renergic–blocking activity (471). Therefore, in cocaine-induced myocardial ischemia and vasoconstriction, NTGand calcium antagonists are the preferred drugs. Both NTGand verapamil have been shown to reverse cocaine-inducedhypertension and coronary arterial vasoconstriction(452,470) and tachycardia (verapamil).
F. Variant (Prinzmetal’s) Angina
Recommendations
Class I1. Coronary arteriography in patients with episodic
chest pain and ST-segment elevation that resolveswith NTG and/or calcium antagonists. (Level ofEvidence: B)
2. Treatment with nitrates and calcium antagonists inpatients whose coronary arteriogram is normal orshows only nonobstructive lesions. (Level of Evi-dence: B)
Class IIa1. Provocative testing in patients with a nonobstruc-
tive lesion on coronary arteriography, the clinicalpicture of coronary spasm, and transient ST-segment elevation. (Level of Evidence: B)
Class IIb1. Provocative testing without coronary arteriography.
(Level of Evidence: C)2. In the absence of significant CAD on coronary
arteriography, provocative testing with methyler-gonovine, acetylcholine, or methacholine when cor-onary spasm is suspected but there is no ECGevidence of transient ST-segment elevation. (Levelof Evidence: C)
Class III1. Provocative testing in patients with high-grade
obstructive lesions on coronary arteriography. (Lev-el of Evidence: B)
Variant angina (Prinzmetal’s angina) is a form of UA thatusually occurs spontaneously, is characterized by transientST-segment elevation, and most commonly resolves withoutprogression to MI (472). The earliest stages of AMI may alsobe associated with cyclic ST-segment elevations. AlthoughPrinzmetal was not the first to describe this condition (473),he was the first to offer the hypothesis that it is caused bytransient coronary artery spasm; this was subsequentlyproved with coronary arteriography (474). The spasm is
most commonly focal and can occur simultaneously at .1site (475). Even coronary segments that are apparentlynormal on coronary angiography often have evidence ofmural atherosclerosis on intravascular ultrasonography(476). This can result in localized endothelial dysfunctionand coronary spasm.
Patients with Prinzmetal’s angina frequently have coro-nary artery plaques that can be nonobstructive or producesignificant stenosis (477). Walling et al. (478) reported in217 patients that coronary arteriography showed 1-vesseldisease in 81 (39%) patients and multivessel disease in 40(19%) patients. Rovai et al. (479) found a similar highprevalence of obstructive disease in 162 patients with variantangina.
1. Clinical Picture. Although chest discomfort in thepatient with variant angina can be precipitated by exercise,it usually occurs without any preceding increase in myocar-dial oxygen demand; the majority of patients have normalexercise tolerance, and stress testing may be negative.Because the anginal discomfort usually occurs at rest with-out precipitating cause, it simulates UA/NSTEMI second-ary to coronary atherosclerosis. Episodes of Prinzmetal’sangina often occur in clusters with prolonged weeks tomonths of asymptomatic periods. However, attacks can beprecipitated by hyperventilation (480), exercise (481), andexposure to cold (482). There tends to be a circadianvariation in the episodes of angina, with most attacksoccurring in the early morning (483). Compared withpatients with chronic stable angina, patients with variantangina are younger and, except for smoking, have fewercoronary risk factors (484,485). Some studies have shown anassociation of variant angina with other vasospastic disor-ders such as migraine headache and Raynaud’s phenomenon(486).
Most often, the attacks resolve spontaneously withoutevidence of MI. However, if the coronary vasospasm isprolonged, MI, a high degree of AV block, life-threateningventricular tachycardia, or sudden death may occur(487,488).
2. Pathogenesis. The pathogenesis of focal coronary spasmin this condition is not well understood. The probableunderlying defect is the presence of dysfunctional endothe-lium that exposes the medial smooth muscle to vasocon-strictors such as catecholamines, thromboxane A2, seroto-nin, histamine, and endothelin (489). Endothelialdysfunction may also impair coronary flow-dependent va-sodilatation due to the decreased production and release ofnitric oxide (490) and enhance phosphorylation of myosinlight chains, an important step for smooth muscle contrac-tion (491). There may be an imbalance betweenendothelium-produced vasodilator factors (i.e., prostacylin,nitric oxide) and vasoconstrictor factors (i.e., endothelin,angiotensin II), to favor the latter (492). There also isevidence for involvement of the autonomic nervous systemwith reduced parasympathetic tone and enhanced reactivity
1038 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062

of the a-adrenergic vascular receptors (490,493,494). Regard-less of the mechanism, the risk for focal spasm is transientbut recurrent.
3. Diagnosis. The diagnosis of variant angina is made bydemonstrating ST-segment elevation in a patient duringtransient chest discomfort (which usually occurs at rest) thatresolves when the chest discomfort abates. On coronaryarteriography, if the artery is found to be angiographicallynormal or exhibits only nonobstructive plaques, then coro-nary artery spasm is the most likely explanation. If thepatient has a spontaneous episode of pain and ST-segmentelevation in the course of coronary arteriography, severefocal spasm of an epicardial coronary artery may be visual-ized. If the spasm is persistent, MI can occur; this is a rarecomplication in patients with variant angina who havenormal or near-normal coronary arteries on arteriography.However, MI is common when coronary spasm complicatesmultivessel obstructive CAD (478). Coronary arteriographycan show obstructive lesions, and increased arterial tone at asite of stenosis can precipitate total occlusion and the pictureof impending infarction that is reversed on resolution of theincreased vasomotor tone.
When the coronary arteriogram is normal or shows onlynonobstructive plaques and if transient ST-segment eleva-tion can be demonstrated at the time at which the patienthas the discomfort, the presumptive diagnosis of Prinzmet-al’s angina can be made and no further tests are necessary.The key is to observe the ECG at the time of the attacks. Ifattacks occur frequently, a 24-h ambulatory ECG may behelpful in establishing the diagnosis.
In the absence of ST-segment elevation that accompanieschest discomfort, a number of provocative tests (methyler-gonovine, acetylcholine, and methacholine) can precipitatecoronary artery spasm that can be visualized angiographi-cally and is accompanied by ST-segment elevation inpatients with Prinzmetal’s variant angina (495). The pa-tients should be withdrawn from nitrates and calciumantagonists before provocative testing. Hyperventilationperformed for 6 min in the morning alone or after exerciseis another test for coronary artery spasm (496). Patients witha positive hyperventilation test are more likely to have ahigher frequency of attacks, multivessel spasm, and a highdegree of AV block or ventricular tachycardia than arepatients with a negative hyperventilation test (496). Becausethese provocative tests can occasionally cause prolongedintense and even multivessel spasm that requires intracoro-nary NTG or calcium antagonists for relief, the tests thatrequire intravenous injections should be conducted in acatheterization laboratory with the catheter positioned inthe coronary artery to deliver these drugs (497). Theaforementioned drugs that are used to precipitate coronaryartery spasm are not always readily available, so hyperven-tilation may be used.
4. Treatment. Coronary spasm is usually very responsive toNTG, long-acting nitrates, and calcium antagonists (498–
500). Smoking should be discontinued. Usually, a calciumantagonist at a high dose (e.g., 240 to 480 mg/d verapamil,120 to 360 mg/d diltiazem, 60 to 120 mg/d nifedipine) isstarted. If the episodes are not completely eliminated, asecond calcium antagonist from another class or a long-acting nitrate should be added. a-Receptor blockers havebeen reported to be of benefit, especially in patients who arenot responding completely to calcium antagonists andnitrates (491). In patients who develop coronary spasm(with or without provocation) during coronary angiography,0.3 mg NTG should be infused directly into the coronaryartery that is involved.
5. Prognosis. The prognosis is usually excellent in patientswith variant angina who receive medical therapy. Yasue etal. (501) reported an 89% to 97% overall 5-year survival rate.The prognosis is especially favorable in patients with normalor near-normal coronary arteries on arteriography. In a7-year follow-up in '300 patients, the incidence of suddendeath was 3.6%, and the incidence of MI was 6.5% (501).Patients with coronary artery vasospasm superimposed on afixed obstructive CAD have a worse prognosis. In a study of162 patients with variant angina by Rovai et al. (479), thepatients with normal coronary arteries and 1-vessel diseasehad a 5-year survival rate of 95% compared with a rate of80% for those with multivessel disease. Almost identicalsurvival rates were reported in an earlier study by Walling etal. (478).
G. Syndrome X
Recommendations
Class I1. Reassurance and medical therapy with nitrates,
b-blockers, and calcium antagonists alone or incombination. (Level of Evidence: B)
2. Risk factor reduction. (Level of Evidence: C)
Class IIb1. Intracoronary ultrasound to rule out missed ob-
structive lesions. (Level of Evidence: B)2. If no ECGs are available during chest pain and
coronary spasm cannot be ruled out, coronary arte-riography and provocative testing with methyler-gonovine, acetylcholine, or methacholine. (Level ofEvidence: C)
3. HRT in postmenopausal women unless there is acontraindication. (Level of Evidence: C)
4. Imipramine for continued pain despite Class Imeasures. (Level of Evidence: C)
Class III1. Medical therapy with nitrates, b-blockers, and cal-
cium antagonists for patients with noncardiac chestpain. (Level of Evidence: C)
1. Definition and Clinical Picture. The term “syndromeX” is used to describe patients with angina or angina-like
1039JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina

discomfort with exercise, ST-segment depression on tread-mill testing, and normal or nonobstructed coronary arterieson arteriography. This entity should be differentiated fromthe “metabolic syndrome X,” which describes patients withinsulin resistance, hyperinsulinemia, dyslipidemia, hyper-tension, and abdominal obesity. It should also be differen-tiated from noncardiac chest pain. Syndrome X is morecommon in women than in men (354,502). Chest pain canvary from that of typical angina pectoris to chest pain withatypical features to chest pain that simulates UA, secondaryto CAD (502). Other atypical features can be prolongedchest pain at rest and chest pain that is unresponsive toNTG (503). Most often, the chest pain occurs with activityand simulates angina pectoris due to stable CAD. However,because chest pain may accelerate in frequency or intensityor occur at rest, the patient may present with the clinicalpicture of UA. Therefore, this syndrome is discussed in thisguideline.
The cause of the discomfort and ST-segment depressionin patients with syndrome X is not well understood. Themost frequently proposed causes are impaired endothelium-dependent arterial vasodilatation with decreased nitric oxideproduction, increased sensitivity to sympathetic stimulation,or coronary vasoconstriction in response to exercise(355,504,505). There is increasing evidence that thesepatients frequently also have an increased responsiveness topain and an abnormality in pain perception.
The diagnosis of syndrome X is one of the exclusion ofcritical obstruction of an epicardial coronary artery inpatients with exertional chest discomfort who have ST-segment depression on treadmill exercise. Other causes ofangina-like chest discomfort not associated with cardiacdisease, such as esophageal dysmotility, fibromyalgia, andcostochondritis, must also be eliminated. In addition, inpatients with a clinical presentation consistent with variantangina, coronary spasm must be ruled out by the absence ofST-segment elevation with the anginal discomfort or byprovocative testing. Myocardial perfusion scanning may beabnormal due to a patchy abnormal response to exercise ofthe microvasculature that may lead to reduced coronary flowto different regions of the myocardium (355).
The intermediate-term prognosis of patients with syn-drome X is excellent (502,503,506). The CASS registryreported a 96% 7-year survival rate in patients with anginalchest pain, normal coronary arteriograms, and an LVEF of.0.50 (507). Long-term follow-up shows that ventricularfunction usually remains normal (503), although there havebeen reports of progressive LV dysfunction, and many patientscontinue to have chest pain that requires medication (508).
2. Treatment. Because the long-term prognosis is excel-lent, the most important therapy consists of reassurance andsymptom relief. However, persistence of symptoms is com-mon, and many patients do not return to work (503). Thedemonstration of normal coronary arteries on angiographycan be reassuring. In 1 study, after a normal coronary
arteriogram, there was a reduced need for hospitalization aswell as a reduced number of hospital days for cardiac reasons(286).
Both b-blockers and calcium antagonists have beenfound to be effective in reducing the number of episodes ofchest discomfort (509,510). Beneficial effects with nitratesare seen in about one half of patients (511). The use ofa-adrenergic blockers would appear to be a rational therapy,but the results of small trials are inconsistent (512). Imip-ramine 50 mg qd has been successful in some chronic painsyndromes, including syndrome X, reducing the frequencyof chest pain by 50% (513). Estrogen replacement inpostmenopausal women with angina and normal coronaryarteriograms has been shown to reverse the acetylcholine-induced coronary arterial vasoconstriction, presumably byimproving endothelium-dependent coronary vasomotion(514). In a double-blind, placebo-controlled study, Rosanoet al. (515) found that cutaneous estrogen patches in 25postmenopausal women with syndrome X reduced thefrequency of chest pain episodes by 50%.
It is recommended that patients be reassured of theexcellent intermediate-term prognosis and treated withlong-acting nitrates. If the patient continues to have epi-sodes of chest pain, a calcium antagonist or b-blocker can bestarted (510). Finally, 50 mg imipramine qd has beensuccessful in reducing the frequency of chest pain episodes.If symptoms persist, other causes of chest pain, especiallyesophageal dysmotility, should be ruled out.
APPENDIX 1. DEFINITION OF TERMINOLOGYRELATED TO UA
● Acute coronary syndrome—any constellation of clinicalsigns or symptoms suggestive of AMI or UA. Thissyndrome includes patients with AMI, STEMI,NSTEMI, enzyme-diagnosed MI, biomarker-diagnosedMI, late ECG-diagnosed MI, and UA. This term isuseful to generically refer to patients who ultimately proveto have 1 of these diagnoses to describe managementalternatives at a time before the diagnosis is ultimatelyconfirmed. This term is also used prospectively to identifythose patients at a time of initial presentation who shouldbe considered for treatment of AMI or UA. Probableacute coronary syndrome is a term that is commonlyused, and this represents the primary consideration ofpatients on initial presentation. Possible acute coronarysyndrome is useful as a secondary diagnosis when analternate diagnosis seems more likely but an acute isch-emic process has not been excluded as a possible cause ofthe presenting symptoms.
● Acute myocardial infarction—an acute process of myo-cardial ischemia with sufficient severity and duration toresult in permanent myocardial damage. Clinically, thediagnosis of permanent myocardial damage is typicallymade when there is a characteristic rise and fall in cardiacbiomarkers indicative of myocardial necrosis that may or
1040 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
may not be accompanied by the development of Q waveson the ECG. Permanent myocardial damage may also bediagnosed when histological evidence of myocardial ne-crosis is observed on pathological examination.
● Angina pectoris—a clinical syndrome typically character-ized by a deep, poorly localized chest or arm discomfortthat is reproducibly associated with physical exertion oremotional stress and relieved promptly (i.e., ,5 min) withrest or sublingual NTG. The discomfort of angina is oftenhard for patients to describe, and many patients do notconsider it to be “pain.” Patients with UA may havediscomfort with all the qualities of typical angina exceptthat episodes are more severe and prolonged and mayoccur at rest with an unknown relationship to exertion orstress. In most, but not all, patients, these symptomsreflect myocardial ischemia that results from significantunderlying CAD.
● Angiographically significant coronary artery disease—CAD is typically judged “significant” at coronary angiog-raphy if there is $70% diameter stenosis, assessed visu-ally, of $1 major epicardial coronary segments or $50%diameter stenosis of the left main coronary artery. Theterm “significant CAD” used in these guidelines does notimply clinical significance but refers only to an angio-graphically significant stenosis.
● Coronary artery disease—although a number of diseaseprocesses other than atherosclerosis can involve coronaryarteries, in these guidelines, the term “CAD” refers to theatherosclerotic narrowing of the major epicardial coronaryarteries.
● Enzyme- or biomarker-diagnosed acute myocardialinfarction—diagnostic elevation of cardiac enzymes orbiomarkers (e.g., troponin) that indicates definite myo-cardial injury in the absence of diagnostic ECG changes(Q waves or ST-segment deviation).
● Ischemic heart disease—a form of heart disease withprimary manifestations that result from myocardial isch-emia due to atherosclerotic CAD. This term encompassesa spectrum of conditions, ranging from the asymptomaticpreclinical phase to AMI and sudden cardiac death.
● Likelihood—used in these guidelines to refer to theprobability of an underlying diagnosis, particularly signif-icant CAD.
● Myocardial ischemia—a condition in which oxygen de-livery to and metabolite removal from the myocardiumfall below normal levels, with oxygen demand exceedingsupply. As a consequence, the metabolic machinery ofmyocardial cells is impaired, leading to various degrees ofsystolic (contractile) and diastolic (relaxation) dysfunc-tion. Ischemia is usually diagnosed indirectly throughtechniques that demonstrate reduced myocardial bloodflow or its consequences on contracting myocardium.
● Non–Q-wave myocardial infarction—an AMI that isnot associated with the evolution of new Q waves on theECG. The diagnosis of non–Q-wave MI is often difficultto make soon after the event and is commonly made only
retrospectively on the basis of elevated cardiac enzymelevels.
● Non–ST-segment elevation myocardial infarction—NSTEMI is an acute process of myocardial ischemia withsufficient severity and duration to result in myocardialnecrosis (see Acute Myocardial Infarction). The initialECG in patients with NSTEMI does not show ST-segment elevation; the majority of patients who presentwith NSTEMI do not develop new Q waves on the ECGand are ultimately diagnosed as having had a non–Q-wave MI. NSTEMI is distinguished from UA by thedetection of cardiac markers indicative of myocardialnecrosis in NSTEMI and the absence of abnormalelevation of such biomarkers in patients with UA.
● Post–myocardial infarction angina—UA occurringfrom 1 to 60 days after an AMI.
● Reperfusion-eligible acute myocardial infarction—acondition characterized by a clinical presentation compat-ible with AMI accompanied by ST-segment elevation ornew LBBB or anterior ST-segment depression withupright T waves on ECG.
● Unstable angina—an acute process of myocardial isch-emia that is not of sufficient severity and duration to resultin myocardial necrosis. Patients with UA typically do notpresent with ST-segment elevation on the ECG and donot release biomarkers indicative of myocardial necrosisinto the blood.
● Variant angina—a clinical syndrome of rest pain andreversible ST-segment elevation without subsequent en-zyme evidence of AMI. In some patients, the cause of thissyndrome appears to be coronary vasospasm alone, oftenat the site of an insignificant coronary plaque, but amajority of patients with variant angina have angiographi-cally significant CAD.
APPENDIX 2. ABBREVIATIONS
AAFP 5 American Academy of FamilyPhysicians
ACC 5 American College of Cardiology
ACE 5 angiotensin-converting enzyme
ACEP 5 American College of EmergencyPhysicians
ACEI 5 angiotensin-converting enzymeinhibitor
ACIP 5 Asymptomatic Cardiac IschemiaPilot
ACP-ASIM 5 American College of Physicians–American Society of InternalMedicine
ACS 5 acute coronary syndrome
ACT 5 activated clotting time
1041JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
ADP 5 adenosine diphosphate
AHA 5 American Heart Association
AHCPR 5 Agency for Health Care Policyand Research
AMI 5 acute myocardial infarction
aPTT 5 activated partial thromboplastintime
ASA 5 aspirin
ATACS 5 Antithrombotic Therapy inAcute Coronary Syndromes
AV 5 atrioventricular
BARI 5 Bypass AngioplastyRevascularization Investigation
CABG 5 coronary artery bypass graftsurgery
CABRI 5 Coronary Angioplasty versusBypass RevascularisationInvestigation
CAD 5 coronary artery disease
CAPRIE 5 Clopidogrel versus Aspirin inPatients at Risk of IschaemicEvents
CAPTURE 5 c7E3 Fab Antiplatelet Therapyin Unstable Refractory Angina
CARS 5 Coumadin Aspirin ReinfarctionStudy
CASS 5 Coronary Artery Surgery Study
CCS 5 Canadian Cardiovascular Society
CHAMP 5 Combination Hemotherapy AndMortality Prevention
cGMP 5 cyclic guanosine monophosphate
CHF 5 congestive heart failure
CI 5 confidence interval
CK 5 creatine kinase
CLASSICS 5 CLopidogrel ASpirin StentInternational Cooperative Study
COPD 5 chronic obstructive pulmonarydisease
CRP 5 C-reactive protein
cTnI 5 cardiac-specific TnI
cTnT 5 cardiac-specific TnT
CURE 5 Clopidogrel in Unstable anginato Prevent ischemic Events
DANAMI 5 DANish trial in AcuteMyocardial Infarction
DATA 5 Diltiazem as Adjunctive Therapyto Activase
DAVIT 5 Danish Study Group onVerapamil in Myocardial Infarc-tion
DRS 5 Diltiazem Reinfarction Study
DTS 5 Duke Treadmill Score
EAST 5 Emory Angioplasty versusSurgery Trial
ECG 5 12-lead electrocardiogram,electrocardiographic
ED 5 emergency department
EF 5 ejection fraction (left ventricle)
EPIC 5 Evaluation of c7E3 for thePrevention of IschemicComplications
EPILOG 5 Evaluation of PTCA to ImproveLong-term Outcome by c7E3GPIIb/IIIA receptor blockade
EPISTENT 5 Evaluation of Platelet IIb/IIIaInhibitor for STENTing
ESSENCE 5 Efficacy and Safety ofSubcutaneous Enoxaparin inNon–Q wave Coronary Events
FRAXIS 5 FRAxiparine in IschaemicSyndrome
FRIC 5 FRagmin In unstable Coronaryartery disease study
FRISC 5 Fragmin during Instability inCoronary Artery Disease
FRISC II 5 Fast Revascularization DuringInstability in Coronary ArteryDisease
GABI 5 German Angioplasty BypassSurgery Investigation
GISSI-1 5 Gruppo Italiano per lo Studiodella Sopravvivenza nell’Infarto-1
GISSI-3 5 Gruppo Italiano per lo Studiodella Sopravvivenza nell’infartoMiocardico
GP 5 glycoprotein
1042 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
GUSTO-II 5 Global Use of Strategies to OpenOccluded Coronary Arteries-II
HDL 5 high-density lipoprotein
HERS 5 Heart and Estrogen/progestinReplacement Study
HINT 5 Holland Interuniversity Nifedi-pine/metoprolol Trial
HOPE 5 Heart Outcomes PreventionEvaluation
HRT 5 hormone replacement therapy
IABP 5 intra-aortic balloon pump
IMPACT 5 Integrilin to Minimise PlateletAggregation and CoronaryThrombosis
IV 5 intravenous
ISIS 5 International Study of InfarctSurvival
LAD 5 left anterior descending coronaryartery
LBBB 5 left bundle-branch block
LDL 5 low-density lipoprotein
LMWH 5 low-molecular-weight heparin
LV 5 left ventricular, left ventricle
MATE 5 Medicine versus Angiography inThrombolytic Exclusion
MDPIT 5 Multicenter Diltiazem Postinfarc-tion Trial
MET 5 metabolic equivalent
MB 5 cardiac muscle isoenzyme ofcreatine kinase
MI 5 myocardial infarction
MM 5 skeletal muscle isoenzyme ofcreatine kinase
MR 5 mitral regurgitation
MVO2 5 myocardial oxygen consumption
NCEP 5 National Cholesterol EducationProgram
NHAAP 5 National Heart Attack AlertProgram
NHLBI 5 National Heart, Lung, and BloodInstitute
NSTEMI 5 non–ST-segment elevationmyocardial infarction
NTG 5 nitroglycerin
OASIS 5 Organization to Assess Strategiesfor Ischemic Syndromes
OR 5 odds ratio
PCI 5 percutaneous coronaryintervention
PR ECG 5 PR segment
PRISM 5 Platelet Receptor Inhibition inIschemic Syndrome Management
PRISM-PLUS 5 Platelet Receptor Inhibition inIschemic Syndrome Managementin Patients Limited by UnstableSigns and Symptoms
PTCA 5 percutaneous transluminalcoronary angioplasty
PURSUIT 5 Platelet Glycoprotein IIb/IIIa inUnstable Angina: ReceptorSuppression Using IntegrilinTherapy
RESTORE 5 Randomized Efficacy Study ofTirofiban for Outcomes andREstenosis
RISC 5 Research Group in Instability inCoronary Artery Disease
RITA 5 Randomized InterventionTreatment of Angina
RR 5 relative risk
SHEP 5 Systolic Hypertension in theElderly Program
SHOCK 5 SHould we emergentlyrevascularize OccludedCoronaries for cardiogenic shocK
STEMI 5 ST-segment elevation myocardialinfarction
STS 5 Society of Thoracic Surgeons
SVG 5 saphenous vein graft
TIMI 5 Thrombolysis In Myocardial In-farction
TIMI 9A and 9B 5 Thrombolysis and ThrombinInhibition in Myocardial Infarc-tion
TnC 5 troponin C
TnI 5 troponin I
TnT 5 troponin T
1043JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina

TTP 5 thrombotic thrombocytopeniapurpura
UA 5 unstable angina
UFH 5 unfractionated heparin
UKPDS 5 UK Prospective Diabetes Study
VA 5 Veterans Administration
VANQWISH 5 Veterans Affairs Non–Q-WaveInfarction Strategies in Hospital
WISE 5 Women’s Ischemia SyndromeEvaluation
STAFF
American College of Cardiology
Christine W. McEntee, Executive Vice PresidentDawn R. Phoubandith, MSW, Assistant Director, Practice
GuidelinesKristi R. Mitchell, MPH, Researcher, Scientific and Re-
search ServicesGwen C. Pigman, MLS, Assistant Director, On-Line and
Library Services
American Heart Association
Rodman D. Starke, MD, FACC, Senior Vice PresidentKathryn A. Taubert, PhD, Director, Division of Cardio-
vascular Science
Agency for Healthcare Research and Quality
UCSF-Stanford Evidence-based Practice CenterMark A. Hlatky, MD, FACC, Center Co-DirectorPaul A. Heidenreich, MD, FACC, Principal InvestigatorAlan Go, MD, Co-InvestigatorKathryn Melsop, MS, Research AssociateKathryn McDonald, MM, Center Coordinator
REFERENCES
1. Braunwald E, Mark DB, Jones RH, et al. Unstable angina: diagnosisand management. Rockville, MD: Agency for Health Care Policyand Research and the National Heart, Lung, and Blood Institute, USPublic Health Service, US Department of Health and HumanServices; 1994:1; AHCPR Publication No 94-0602.
2. National Center for Health Statistics. Detailed diagnoses and pro-cedures: National Hospital Discharge Survey, 1996. Hyattsville, MD:National Center for Health Statistics; 1998:13; data from Vital andHealth Statistics.
3. Nourjah P. National Hospital Ambulatory Medical Care Survey:1997 emergency department summary. Hyattsville, MD: NationalCenter for Health Statistics; 1999:304; advance data from Vital andHealth Statistics.
4. Anderson HV, Cannon CP, Stone PH, et al. One-year results of theThrombolysis In Myocardial Infarction (TIMI) IIIB clinical trial: arandomized comparison of tissue-type plasminogen activator versusplacebo and early invasive versus early conservative strategies inunstable angina and non-Q wave myocardial infarction. J Am CollCardiol 1995;26:1643–50.
5. Ryan TJ, Anderson JL, Antman EM, et al. ACC/AHA guidelinesfor the management of patients with acute myocardial infarction: areport of the American College of Cardiology/American Heart
Association Task Force on Practice Guidelines (Committee onManagement of Acute Myocardial Infarction). 1999 update; http://www.acc.org/clinical/guidelines/ami.html (accessed August 30,1999).
6. Wu AH, Apple FS, Gibler WB, Jesse RL, Warshaw MM, ValdesRJ. National Academy of Clinical Biochemistry Standards of Labo-ratory Practice: recommendations for the use of cardiac markers incoronary artery diseases. Clin Chem 1999;45:1104–21.
7. Braunwald E. Unstable angina: an etiologic approach to management(editorial). Circulation 1998;98:2219–22.
8. Braunwald E. Unstable angina: a classification. Circulation 1989;80:410–14.
9. Campeau L. Grading of angina pectoris (letter). Circulation 1976;54:522–3.
10. The PURSUIT Trial Investigators. Inhibition of platelet glycopro-tein IIb/IIIa with eptifibatide in patients with acute coronary syn-dromes. The PURSUIT Trial Investigators: Platelet GlycoproteinIIb/IIIa in Unstable Angina: Receptor Suppression Using IntegrilinTherapy. N Engl J Med 1998;339:436–43.
11. Selker HP, Beshansky JR, Griffith JL, et al. Use of the acute cardiacischemia time-insensitive predictive instrument (ACI-TIPI) to assistwith triage of patients with chest pain or other symptoms suggestiveof acute cardiac ischemia: a multicenter, controlled clinical trial. AnnIntern Med 1998;129:845–55.
12. Ghali JK, Cooper RS, Kowatly I, Liao Y. Delay between onset ofchest pain and arrival to the coronary care unit among minority anddisadvantaged patients. J Natl Med Assoc 1993;85:180–4.
13. Hargarten K, Chapman PD, Stueven HA, et al. Prehospital prophy-lactic lidocaine does not favorably affect outcome in patients withchest pain. Ann Emerg Med 1990;19:1274–9.
14. Newby LK, Califf RM, Guerci A, et al. Early discharge in thethrombolytic era: an analysis of criteria for uncomplicated infarctionfrom the Global Utilization of Streptokinase and t-PA for OccludedCoronary Arteries (GUSTO) trial. J Am Coll Cardiol 1996;27:625–32.
15. Maynard C, Weaver WD, Lambrew C, Bowlby LJ, Rogers WJ,Rubison RM. Factors influencing the time to administration ofthrombolytic therapy with recombinant tissue plasminogen activator(data from the National Registry of Myocardial Infarction). Partici-pants in the National Registry of Myocardial Infarction. Am JCardiol 1995;76:548–52.
16. Weaver WD, Cerqueira M, Hallstrom AP, et al. Prehospital-initiated vs hospital-initiated thrombolytic therapy: the MyocardialInfarction Triage and Intervention Trial. JAMA 1993;270:1211–6.
17. Pope JH, Ruthazer R, Beshansky JR, Griffith JL, Selker HP. Clinicalfeatures of emergency department patients presenting with symptomssuggestive of acute cardiac ischemia: a multicenter study. J ThrombThrombolysis 1998;6:63–74.
18. Theroux P, Fuster V. Acute coronary syndromes: unstable angina andnon–Q-wave myocardial infarction. Circulation 1998;97:1195–206.
19. Effects of tissue plasminogen activator and a comparison of earlyinvasive and conservative strategies in unstable angina and non–Q-wave myocardial infarction: results of the TIMI IIIB trial. Throm-bolysis In Myocardial Ischemia. Circulation 1994;89:1545–56.
20. SHEP Cooperative Research Group. Prevention of stroke by anti-hypertensive drug treatment in older persons with isolated systolichypertension: final results of the Systolic Hypertension in the ElderlyProgram (SHEP). JAMA 1991;265:3255–64.
21. Platelet Receptor Inhibition in Ischemic Syndrome Management inPatients Limited by Unstable Signs and Symptoms (PRISM-PLUS)Study Investigators. Inhibition of the platelet glycoprotein IIb/IIIareceptor with tirofiban in unstable angina and non–Q-wave myocar-dial infarction [erratum appears in N Engl J Med 1998;339:415].N Engl J Med 1998;338:1488–97.
22. Cohen M, Stinnett S, Weatherley B, et al. Predictors of recurrentischemic events and death in unstable coronary artery disease aftertreatment with combination antithrombotic therapy. Am Heart J2000;139:962–70.
23. Chaitman BR, Bourassa MG, Davis K, et al. Angiographic preva-lence of high-risk coronary artery disease in patient subsets (CASS).Circulation 1981;64:360–7.
24. Pryor DB, Harrell FEJ, Lee KL, Califf RM, Rosati RA. Estimatingthe likelihood of significant coronary artery disease. Am J Med1983;75:771–80.
1044 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
25. Pryor DB, Shaw L, McCants CB, et al. Value of the history andphysical in identifying patients at increased risk for coronary arterydisease. Ann Intern Med 1993;118:81–90.
26. Gibbons RJ, Chatterjee K, Daley J, et al. ACC/AHA/ACP-ASIMguidelines for the management of patients with chronic stable angina.J Am Coll Cardiol 1999;33:2092–197.
27. Lee TH, Cook EF, Weisberg M, Sargent RK, Wilson C, GoldmanL. Acute chest pain in the emergency room: identification andexamination of low-risk patients. Arch Intern Med 1985;145:65–9.
28. Pozen MW, D’Agostino RB, Selker HP, Sytkowski PA, Hood WBJ.A predictive instrument to improve coronary-care-unit admissionpractices in acute ischemic heart disease: a prospective multicenterclinical trial. N Engl J Med 1984;310:1273–8.
29. Selker HP, Griffith JL, D’Agostino RB. A tool for judging coronarycare unit admission appropriateness, valid for both real-time andretrospective use. A time-insensitive predictive instrument (TIPI) foracute cardiac ischemia: a multicenter study [erratum appears in MedCare 1992;30:188]. Med Care 1991;29:610–27.
30. Brieger DB, Mak KH, White HD, et al. Benefit of early sustainedreperfusion in patients with prior myocardial infarction (theGUSTO-I trial): Global Utilization of Streptokinase and TPA forOccluded Arteries. Am J Cardiol 1998;81:282–7.
31. Hochman JS, Tamis JE, Thompson TD, et al. Sex, clinical presen-tation, and outcome in patients with acute coronary syndromes.Global Use of Strategies to Open Occluded Coronary Arteries inAcute Coronary Syndromes IIb Investigators. N Engl J Med 1999;341:226–32.
32. Hochman JS, McCabe CH, Stone PH, et al. Outcome and profile ofwomen and men presenting with acute coronary syndromes: a reportfrom TIMI IIIB. TIMI Investigators. Thrombolysis In MyocardialInfarction. J Am Coll Cardiol 1997;30:141–8.
33. Scirica BM, Moliterno DJ, Every NR, et al. Differences between menand women in the management of unstable angina pectoris (theGUARANTEE Registry). The GUARANTEE Investigators. Am JCardiol 1999;84:1145–50.
34. Holmes DRJ, White HD, Pieper F, Ellis SG, Califf RM, Topol EJ.Effect of age on outcome with primary angioplasty versus thrombol-ysis. J Am Coll Cardiol 1999;33:412–9.
35. White HD, Barbash GI, Califf RM, et al. Age and outcome withcontemporary thrombolytic therapy: results from the GUSTO-I trial.Global Utilization of Streptokinase and TPA for Occluded coronaryarteries trial. Circulation 1996;94:1826–33.
36. Jayes RLJ, Beshansky JR, D’Agostino RB, Selker HP. Do patients’coronary risk factor reports predict acute cardiac ischemia in theemergency department? A multicenter study. J Clin Epidemiol1992;45:621–6.
37. Mak KH, Moliterno DJ, Granger CB, et al. Influence of diabetesmellitus on clinical outcome in the thrombolytic era of acutemyocardial infarction. GUSTO-I Investigators. Global Utilization ofStreptokinase and Tissue Plasminogen Activator for Occluded Cor-onary Arteries. J Am Coll Cardiol 1997;30:171–9.
38. Mueller HS, Cohen LS, Braunwald E, et al. Predictors of earlymorbidity and mortality after thrombolytic therapy of acute myocar-dial infarction. Analyses of patient subgroups in the Thrombolysis InMyocardial Infarction (TIMI) trial, phase II. Circulation 1992;85:1254–64.
39. Barbash GI, White HD, Modan M, et al. Significance of smoking inpatients receiving thrombolytic therapy for acute myocardial infarc-tion: experience gleaned from the International Tissue PlasminogenActivator/Streptokinase Mortality Trial. Circulation 1993;87:53–8.
40. Barbash GI, White HD, Modan M, et al. Acute myocardialinfarction in the young—the role of smoking. The Investigators ofthe International Tissue Plasminogen Activator/Streptokinase Mor-tality Trial. Eur Heart J 1995;16:313–6.
41. Katz DA, Griffith JL, Beshansky JR, Selker HP. The use of empiricclinical data in the evaluation of practice guidelines for unstableangina. JAMA 1996;276:1568–74.
42. Califf RM, Mark DB, Harrell FEJ, et al. Importance of clinicalmeasures of ischemia in the prognosis of patients with documentedcoronary artery disease. J Am Coll Cardiol 1988;11:20–6.
43. Califf RM, Phillips HR, Hindman MC, et al. Prognostic value of acoronary artery jeopardy score. J Am Coll Cardiol 1985;5:1055–63.
44. White LD, Lee TH, Cook EF, et al. Comparison of the natural
history of new onset and exacerbated chronic ischemic heart disease.The Chest Pain Study Group. J Am Coll Cardiol 1990;16:304–10.
45. Hochman JS, Sleeper LA, Godfrey E, et al. SHould we emergentlyrevascularize Occluded Coronaries for cardiogenic shocK: an inter-national randomized trial of emergency PTCA/CABG-trial design.The SHOCK Trial Study Group. Am Heart J 1999;137:313–21.
45a. Holmes DR Jr, Berger BP, Hochman JS, et al. Cardiogenic shock inpatients with acute ischemic syndromes with and without ST-segment elevation. Circulation 1999;100:2067–73.
46. Selker HP, Zalenski RJ, Antman EM, et al. An evaluation oftechnologies for identifying acute cardiac ischemia in the emergencydepartment: a report from a National Heart Attack Alert ProgramWorking Group [erratum appears in Ann Emerg Med 1997;29:310].Ann Emerg Med 1997;29:13–87.
47. Rouan GW, Lee TH, Cook EF, Brand DA, Weisberg MC,Goldman L. Clinical characteristics and outcome of acute myocardialinfarction in patients with initially normal or nonspecific electrocar-diograms (a report from the Multicenter Chest Pain Study). Am JCardiol 1989;64:1087–92.
48. Zaacks SM, Liebson PR, Calvin JE, Parrillo JE, Klein LW. Unstableangina and non–Q wave myocardial infarction: does the clinicaldiagnosis have therapeutic implications? J Am Coll Cardiol 1999;33:107–18.
49. Savonitto S, Ardissino D, Granger CB, et al. Prognostic value of theadmission electrocardiogram in acute coronary syndromes. JAMA1999;281:707–13.
50. Lee TH, Cook EF, Weisberg MC, Rouan GW, Brand DA,Goldman L. Impact of the availability of a prior electrocardiogram onthe triage of the patient with acute chest pain. J Gen Intern Med1990;5:381–8.
51. Fesmire FM, Percy RF, Wears RL. Diagnostic and prognosticimportance of comparing the initial to the previous electrocardiogramin patients admitted for suspected acute myocardial infarction [seecomments]. South Med J 1991;84:841–6.
52. Adams JE, Abendschein DR, Jaffe AS. Biochemical markers ofmyocardial injury: is MB creatine kinase the choice for the 1990s?Circulation 1993;88:750–63.
53. Eisenberg PR, Kenzora JL, Sobel BE, Ludbrook PA, Jaffe AS.Relation between ST segment shifts during ischemia and thrombinactivity in patients with unstable angina. J Am Coll Cardiol 1991;18:898–903.
54. Matetzky S, Freimark D, Feinberg MS, et al. Acute myocardialinfarction with isolated ST-segment elevation in posterior chest leadsV7–9: “hidden” ST-segment elevations revealing acute posteriorinfarction. J Am Coll Cardiol 1999;34:748–53.
55. de Zwaan C, Bar FW, Janssen JH, et al. Angiographic and clinicalcharacteristics of patients with unstable angina showing an ECGpattern indicating critical narrowing of the proximal LAD coronaryartery. Am Heart J 1989;117:657–65.
56. Haines DE, Raabe DS, Gundel WD, Wackers FJ. Anatomic andprognostic significance of new T-wave inversion in unstable angina.Am J Cardiol 1983;52:14–8.
57. Renkin J, Wijns W, Ladha Z, Col J. Reversal of segmental hypoki-nesis by coronary angioplasty in patients with unstable angina,persistent T wave inversion, and left anterior descending coronaryartery stenosis. Additional evidence for myocardial stunning inhumans [see comments]. Circulation 1990;82:913–21.
58. McCarthy BD, Wong JB, Selker HP. Detecting acute cardiacischemia in the emergency department: a review of the literature.J Gen Intern Med 1990;5:365–73.
59. Slater DK, Hlatky MA, Mark DB, Harrell FEJ, Pryor DB, CaliffRM. Outcome in suspected acute myocardial infarction with normalor minimally abnormal admission electrocardiographic findings. Am JCardiol 1987;60:766–70.
60. Cannon CP, McCabe CH, Stone PH, et al. The electrocardiogrampredicts one-year outcome of patients with unstable angina andnon–Q wave myocardial infarction: results of the TIMI III RegistryECG Ancillary Study. Thrombolysis In Myocardial Ischemia. J AmColl Cardiol 1997;30:133–40.
61. Ohman EM, Armstrong PW, Christenson RH, et al. Cardiactroponin T levels for risk stratification in acute myocardial ischemia.GUSTO IIA Investigators. N Engl J Med 1996;335:1333–41.
62. Antman EM, Tanasijevic MJ, Thompson B, et al. Cardiac-specific
1045JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
troponin I levels to predict the risk of mortality in patients with acutecoronary syndromes. N Engl J Med 1996;335:1342–9.
63. Hyde TA, French JK, Wong CK, Straznicky IT, Whitlock RM,White HD. Four-year survival of patients with acute coronarysyndromes without ST-segment elevation and prognostic significanceof 0.5-mm ST-segment depression. Am J Cardiol 1999;84:379–85.
64. Lloyd-Jones DM, Camargo CAJ, Lapuerta P, Giugliano RP,O’Donnell CJ. Electrocardiographic and clinical predictors of acutemyocardial infarction in patients with unstable angina pectoris. Am JCardiol 1998;81:1182–6.
65. Kudenchuk PJ, Maynard C, Cobb LA, et al. Utility of the prehospitalelectrocardiogram in diagnosing acute coronary syndromes: the Myo-cardial Infarction Triage and Intervention (MITI) Project. J Am CollCardiol 1998;32:17–27.
66. Langer A, Freeman MR, Armstrong PW. ST segment shift inunstable angina: pathophysiology and association with coronaryanatomy and hospital outcome. J Am Coll Cardiol 1989;13:1495–502.
67. Langer A, Freeman MR, Armstrong PW. Relation of angiographicdetected intracoronary thrombus and silent myocardial ischemia inunstable angina pectoris. Am J Cardiol 1990;66:1381–2.
68. Hedges JR, Young GP, Henkel GF, Gibler WB, Green TR,Swanson JR. Serial ECGs are less accurate than serial CK-MB resultsfor emergency department diagnosis of myocardial infarction. AnnEmerg Med 1992;21:1445–50.
69. Patel DJ, Holdright DR, Knight CJ, et al. Early continuous STsegment monitoring in unstable angina: prognostic value additionalto the clinical characteristics and the admission electrocardiogram.Heart 1996;75:222–8.
70. Patel DJ, Knight CJ, Holdright DR, et al. Long-term prognosis inunstable angina: the importance of early risk stratification usingcontinuous ST segment monitoring. Eur Heart J 1998;19:240–9.
71. McNutt RA, Selker HP. How did the acute ischemic heart diseasepredictive instrument reduce unnecessary coronary care unit admis-sions? Med Decis Making 1988;8:90–4.
72. Wasson JH, Sox HC, Neff RK, Goldman L. Clinical predictionrules: applications and methodological standards. N Engl J Med1985;313:793–9.
73. Goldman L, Weinberg M, Weisberg M, et al. A computer-derivedprotocol to aid in the diagnosis of emergency room patients withacute chest pain. N Engl J Med 1982;307:588–96.
74. Goldman L, Cook EF, Brand DA, et al. A computer protocol topredict myocardial infarction in emergency department patients withchest pain. N Engl J Med 1988;318:797–803.
75. Lee TH, Juarez G, Cook EF, et al. Ruling out acute myocardialinfarction: a prospective multicenter validation of a 12-hour strategyfor patients at low risk. N Engl J Med 1991;324:1239–46.
76. Grijseels EW, Deckers JW, Hoes AW, et al. Pre-hospital triage ofpatients with suspected myocardial infarction: evaluation of previ-ously developed algorithms and new proposals. Eur Heart J 1995;16:325–32.
77. Ellis AK. Serum protein measurements and the diagnosis of acutemyocardial infarction. Circulation 1991;83:1107–9.
78. Roberts R, Kleiman NS. Earlier diagnosis and treatment of acutemyocardial infarction necessitates the need for a “new diagnosticmind-set.” Circulation 1994;89:872–81.
79. Roberts R, Fromm RE. Management of acute coronary syndromesbased on risk stratification by biochemical markers: an idea whosetime has come. Circulation 1998;98:1831–3.
80. Tsung SH. Several conditions causing elevation of serum CK-MBand CK-BB. Am J Clin Pathol 1981;75:711–5.
81. Mair J, Morandell D, Genser N, Lechleitner P, Dienstl F, Puschen-dorf B. Equivalent early sensitivities of myoglobin, creatine kinaseMB mass, creatine kinase isoform ratios, and cardiac troponins I andT for acute myocardial infarction. Clin Chem 1995;41:1266–72.
82. Puleo PR, Meyer D, Wathen C, et al. Use of a rapid assay ofsubforms of creatine kinase-MB to diagnose or rule out acutemyocardial infarction. N Engl J Med 1994;331:561–6.
83. Hamm CW, Goldmann BU, Heeschen C, Kreymann G, Berger J,Meinertz T. Emergency room triage of patients with acute chest painby means of rapid testing for cardiac troponin T or troponin I.N Engl J Med 1997;337:1648–53.
84. Antman EM, Grudzien C, Mitchell RN, Sacks DB. Detection of
unsuspected myocardial necrosis by rapid bedside assay for cardiactroponin T. Am Heart J 1997;133:596–8.
85. Apple FS, Falahati A, Paulsen PR, Miller EA, Sharkey SW.Improved detection of minor ischemic myocardial injury with mea-surement of serum cardiac troponin I. Clin Chem 1997;43:2047–51.
86. Pettijohn TL, Doyle T, Spiekerman AM, Watson LE, Riggs MW,Lawrence ME. Usefulness of positive troponin-T and negativecreatine kinase levels in identifying high-risk patients with unstableangina pectoris. Am J Cardiol 1997;80:510–1.
87. Galvani M, Ottani F, Ferrini D, et al. Prognostic influence ofelevated values of cardiac troponin I in patients with unstable angina.Circulation 1997;95:2053–9.
88. Lindahl B, Andren B, Ohlsson J, Venge P, Wallentin L. Riskstratification in unstable coronary artery disease: additive value oftroponin T determinations and pre-discharge exercise tests. FRISKStudy Group. Eur Heart J 1997;18:762–70.
89. Lindahl B, Venge P, Wallentin L. Relation between troponin T andthe risk of subsequent cardiac events in unstable coronary arterydisease. The FRISC Study Group. Circulation 1996;93:1651–7.
90. Wu AH. A comparison of cardiac troponin T and cardiac troponin Iin patients with acute coronary syndromes. Coron Artery Dis1999;10:69–74.
91. Hamm CW, Heeschen C, Goldmann B, et al. Benefit of abciximabin patients with refractory unstable angina in relation to serumtroponin T levels: c7E3 Fab Antiplatelet Therapy in UnstableRefractory Angina (CAPTURE) Study Investigators. N Engl J Med1999;340:1623–9.
92. Heeschen C, Hamm CW, Goldmann B, Deu A, Langenbrink L,White HD. Troponin concentrations for stratification of patientswith acute coronary syndromes in relation to therapeutic efficacy oftirofiban. PRISM Study Investigators. Platelet Receptor Inhibition inIschemic Syndrome Management. Lancet 1999;354:1757–62.
93. Lindahl B, Venge P, Wallentin L. Troponin T identifies patientswith unstable coronary artery disease who benefit from long-termantithrombotic protection. Fragmin in Unstable Coronary ArteryDisease (FRISC) Study Group. J Am Coll Cardiol 1997;29:43–8.
94. Antman EM, Sacks DB, Rifai N, McCabe CH, Cannon CP,Braunwald E. Time to positivity of a rapid bedside assay forcardiac-specific troponin T predicts prognosis in acute coronarysyndromes: a Thrombolysis In Myocardial Infarction (TIMI) 11Asubstudy. J Am Coll Cardiol 1998;31:326–30.
95. Hamm CW, Ravkilde J, Gerhardt W, et al. The prognostic value ofserum troponin T in unstable angina. N Engl J Med 1992;327:146–50.
96. Christenson RH, Duh SH, Newby LK, et al. Cardiac troponin T andcardiac troponin I: relative values in short-term risk stratification ofpatients with acute coronary syndromes. GUSTO-IIa Investigators.Clin Chem 1998;44:494–501.
97. Gokhan CV, Gok H, Kaptanoglu B. The prognostic value of serumtroponin T in unstable angina. Int J Cardiol 1996;53:237–44.
98. Ravkilde J, Nissen H, Horder M, Thygesen K. Independent prog-nostic value of serum creatine kinase isoenzyme MB mass, cardiactroponin T and myosin light chain levels in suspected acute myocar-dial infarction: analysis of 28 months of follow-up in 196 patients.J Am Coll Cardiol 1995;25:574–81.
99. Ravkilde J, Horder M, Gerhardt W, et al. Diagnostic performanceand prognostic value of serum troponin T in suspected acutemyocardial infarction. Scand J Clin Lab Invest 1993;53:677–85.
100. Stubbs P, Collinson P, Moseley D, Greenwood T, Noble M.Prospective study of the role of cardiac troponin T in patientsadmitted with unstable angina. BMJ 1996;313:262–4.
101. Luscher MS, Thygesen K, Ravkilde J, Heickendorff L. Applicabilityof cardiac troponin T and I for early risk stratification in unstablecoronary artery disease: TRIM Study Group. Thrombin Inhibition inMyocardial ischemia. Circulation 1997;96:2578–85.
102. Brscic E, Chiappino I, Bergerone S, et al. Prognostic implications ofdetection of troponin I in patients with unstable angina pectoris.Am J Cardiol 1998;82:971–3.
103. Olatidoye AG, Wu AH, Feng YJ, Waters D. Prognostic role oftroponin T versus troponin I in unstable angina pectoris for cardiacevents with meta-analysis comparing published studies. Am J Cardiol1998;81:1405–10.
104. Rebuzzi AG, Quaranta G, Liuzzo G, et al. Incremental prognosticvalue of serum levels of troponin T and C-reactive protein on
1046 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
admission in patients with unstable angina pectoris. Am J Cardiol1998;82:715–9.
105. Yang Z, Zhang W, Liu Y. Prognostic efficacy of troponin Tmeasurement in angina pectoris. Chin Med J (Engl) 1995;108:626–30.
106. Kontos MC, Anderson FP, Schmidt KA, Ornato JP, Tatum JL, JesseRL. Early diagnosis of acute myocardial infarction in patients withoutST-segment elevation. Am J Cardiol 1999;83:155–8.
107. Zaninotto M, Altinier S, Lachin M, Celegon L, Plebani M.Strategies for the early diagnosis of acute myocardial infarction usingbiochemical markers. Am J Clin Pathol 1999;111:399–405.
108. Zimmerman J, Fromm R, Meyer D, et al. Diagnostic MarkerCooperative Study for the diagnosis of myocardial infarction. Circu-lation 1999;99:1671–7.
109. Apple FS. Clinical and analytical standardization issues confrontingcardiac troponin I [see comments]. Clin Chem 1999;45:18–20.
110. Kontos MC, Anderson FP, Hanbury CM, Roberts CS, Miller WG,Jesse RL. Use of the combination of myoglobin and CK-MB massfor the rapid diagnosis of acute myocardial infarction. Am J EmergMed 1997;15:14–9.
111. Lindahl B, Venge P, Wallentin L. Early diagnosis and exclusion ofacute myocardial infarction using biochemical monitoring. TheBIOMACS Study Group. Biochemicals Markers of Acute CoronarySyndromes. Coron Artery Dis 1995;6:321–8.
111a. Hamm CW, Braunwald E. A classification of unstable anginarevisited. Circulation 2000;102:118–22.
112. Apple FS, Christenson RH, Valdes RJ, et al. Simultaneous rapidmeasurement of whole blood myoglobin, creatine kinase MB, andcardiac troponin I by the triage cardiac panel for detection ofmyocardial infarction. Clin Chem 1999;45:199–205.
113. Fesmire FM, Percy RF, Bardoner JB, Wharton DR, Calhoun FB.Serial creatinine kinase (CK) MB testing during the emergencydepartment evaluation of chest pain: utility of a 2-hour deltaCK-MBof 11.6 ng/ml. Am Heart J 1998;136:237–44.
114. Fesmire FM. Delta CK-MB outperforms delta troponin I at 2 hoursduring the initial EF evaluation of chest pain. Am J Emerg Med2000;18:1–8.
115. Ardissino D, Merlini PA, Gamba G, et al. Thrombin activity andearly outcome in unstable angina pectoris. Circulation 1996;93:1634–9.
116. Becker RC, Cannon CP, Bovill EG, et al. Prognostic value of plasmafibrinogen concentration in patients with unstable angina and non-Q-wave myocardial infarction (TIMI IIIB trial). Am J Cardiol1996;78:142–7.
117. Morrow DA, Rifai N, Antman EM, et al. Serum amyloid A predictsearly mortality in acute coronary syndromes: a TIMI 11A substudy.J Am Coll Cardiol 2000;35:358–62.
118. Oltrona L, Ardissino D, Merlini PA, Spinola A, Chiodo F, PezzanoA. C-reactive protein elevation and early outcome in patients withunstable angina pectoris. Am J Cardiol 1997;80:1002–6.
119. Biasucci LM, Vitelli A, Liuzzo G, et al. Elevated levels ofinterleukin-6 in unstable angina. Circulation 1996;94:874–7.
120. Haverkate F, Thompson SG, Pyke SD, Gallimore JR, Pepys MB.Production of C-reactive protein and risk of coronary events in stableand unstable angina. European Concerted Action on Thrombosisand Disabilities Angina Pectoris Study Group. Lancet 1997;349:462–6.
121. Morrow DA, Rifai N, Antman EM, et al. C-reactive protein is apotent predictor of mortality independently of and in combinationwith troponin T in acute coronary syndromes: a TIMI 11A substudy.Thrombolysis In Myocardial Infarction. J Am Coll Cardiol 1998;31:1460–5.
122. Ghaisas NK, Shahi CN, Foley B, et al. Elevated levels of circulatingsoluble adhesion molecules in peripheral blood of patients withunstable angina. Am J Cardiol 1997;80:617–9.
123. Cannon CP, O’Gara PT. Critical pathways for acute coronarysyndromes. In: Cannon CP, ed. Management of acute coronarysyndromes. Totowa, NJ: Humana Press; 1999:611–27.
124. Graff L, Joseph T, Andelman R, et al. American College ofEmergency Physicians information paper: Chest pain units in emer-gency departments: a report from the Short-Term ObservationServices Section. Am J Cardiol 1995;76:1036–9.
125. Brillman J, Mathers-Dunbar L, Graff L, et al. Management ofobservation units. Ann Emerg Med 1995;25:823–30.
126. Graff LG, Dallara J, Ross MA, et al. Impact on the care of theemergency department chest pain patient from the Chest PainEvaluation Registry (CHEPER) study. Am J Cardiol 1997;80:563–8.
127. Gomez MA, Anderson JL, Karagounis LA, Muhlestein JB, MooersFB. An emergency department-based protocol for rapidly ruling outmyocardial ischemia reduces hospital time and expense: results of arandomized study (ROMIO). J Am Coll Cardiol 1996;28:25–33.
128. Farkouh ME, Smars PA, Reeder GS, et al. A clinical trial of achest-pain observation unit for patients with unstable angina. ChestPain Evaluation in the Emergency Room (CHEER) Investigators.N Engl J Med 1998;339:1882–8.
129. Newby LK, Mark DB. The chest-pain unit—ready for prime time(editorial)? N Engl J Med 1998;339:1930–2.
130. Kuntz KM, Fleischmann KE, Hunink MGM, Douglas PS. Cost-effectiveness of diagnostic strategies for patients with chest pain. AnnIntern Med 1999;130:709–8.
131. Garber AM, Solomon NA. Cost-effectiveness of alternative teststrategies for the diagnosis of coronary artery disease. Ann InternMed 1999;130:719–28.
132. Pepine CJ, Allen HD, Bashore TM, et al. ACC/AHA guidelines forcardiac catheterization and cardiac catheterization laboratories.American College of Cardiology/American Heart Association AdHoc Task Force on Cardiac Catheterization. J Am Coll Cardiol1991;18:1149–82.
133. Armstrong PW. Stable Ischemic Syndromes. In: Topol EJ, ed.Textbook of cardiovascular medicine. Philadelphia, PA: Lippincott-Raven; 1998:333–64.
134. Cheitlin MD, Hutter AMJ, Brindis RG, et al. ACC/AHA expertconsensus document: use of sildenafil (Viagra) in patients withcardiovascular disease: American College of Cardiology/AmericanHeart Association. J Am Coll Cardiol 1999;33:273–82.
135. Physicians’ desk reference, ed 53. Mountvale, NJ: Medical EconomicCo, Inc; 1999.
136. Dellborg M, Gustafsson G, Swedberg K. Buccal versus intravenousnitroglycerin in unstable angina pectoris. Eur J Clin Pharmacol1991;41:5–9.
137. Yusuf S, Collins R, MacMahon S, Peto R. Effect of intravenousnitrates on mortality in acute myocardial infarction: an overview ofthe randomised trials. Lancet 1988;1:1088–92.
138. ISIS-4 (Fourth International Study of Infarct Survival) CollaborativeGroup. ISIS-4: a randomised factorial trial assessing early oralcaptopril, oral mononitrate, and intravenous magnesium sulphate in58,050 patients with suspected acute myocardial infarction. Lancet1995;345:669–85.
139. GISSI-3. Effects of lisinopril and transdermal glyceryl trinitratesingly and together on 6-week mortality and ventricular function afteracute myocardial infarction. Gruppo Italiano per lo Studio dellaSopravvivenza nell’infarto Miocardico. Lancet 1994;343:1115–22.
140. Figueras J, Lidon R, Cortadellas J. Rebound myocardial ischaemiafollowing abrupt interruption of intravenous nitroglycerin infusion inpatients with unstable angina at rest. Eur Heart J 1991;12:405–11.
141. Armstrong PW. Stable ischemic syndromes. Section 2: ClinicalCardiology (Section ed. Califf, RM) In: Topol EJ, ed. Textbook ofcardiovascular medicine. Philadelphia, PA: Lippincott-Raven; 1998:351–53.
142. Yusuf S, Wittes J, Friedman L. Overview of results of randomizedclinical trials in heart disease, II: unstable angina, heart failure,primary prevention with aspirin, and risk factor modification. JAMA1988;260:2259–63.
143. White HD. Unstable angina: Ischemic Syndromes. In: Topol EJ, ed.Textbook of cardiovascular medicine. Philadelphia, PA: Lippincott-Raven; 1998:365–93.
144. Furberg CD, Psaty BM, Meyer JV. Nifedipine: dose-related increasein mortality in patients with coronary heart disease. Circulation1995;92:1326–31.
145. Gibson RS, Boden WE, Theroux P, et al. Diltiazem and reinfarctionin patients with non-Q-wave myocardial infarction: results of adouble-blind, randomized, multicenter trial. N Engl J Med 1986;315:423–9.
146. Lubsen J, Tijssen JG. Efficacy of nifedipine and metoprolol in theearly treatment of unstable angina in the coronary care unit: findingsfrom the Holland Interuniversity Nifedipine/metoprolol Trial(HINT). Am J Cardiol 1987;60:18A–25A.
1047JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
147. Hansen JF, Hagerup L, Sigurd B, et al. Cardiac event rates after acutemyocardial infarction in patients treated with verapamil and tran-dolapril versus trandolapril alone. Danish Verapamil Infarction Trial(DAVIT) Study Group. Am J Cardiol 1997;79:738–41.
148. Opie LH. Pharmacologic options for treatment of ischemic heartdisease. In: Smith TW, ed. Cardiovascular therapeutics: a companionto Braunwald’s heart disease. Philadelphia, PA: WB Saunders;1996:22–57.
149. Beevers DG, Sleight P. Short acting dihydropyridine (vasodilating)calcium channel blockers for hypertension: is there a risk? BMJ1996;312:1143–5.
150. Pepine CJ, Faich G, Makuch R. Verapamil use in patients withcardiovascular disease: an overview of randomized trials. Clin Cardiol1998;21:633–41.
151. The Danish Study Group on Verapamil in Myocardial Infarction.Verapamil in acute myocardial infarction. Eur Heart J 1984;5:516–28.
152. Tijssen JG, Lubsen J. Nifedipine and metoprolol in unstable angina:findings from the Holland Interuniversity Nifedipine/metoprololTrial (HINT). J Cardiovasc Pharmacol 1987;10 Suppl 2:S15–24.
153. Held PH, Yusuf S, Furberg CD. Calcium channel blockers in acutemyocardial infarction and unstable angina: an overview. BMJ 1989;299:1187–92.
154. Boden WE, Krone RJ, Kleiger RE, et al. Electrocardiographic subsetanalysis of diltiazem administration on long-term outcome after acutemyocardial infarction. The Multicenter Diltiazem Post-InfarctionTrial Research Group. Am J Cardiol 1991;67:335–42.
155. The Danish Study Group on Verapamil in Myocardial Infarction.Secondary prevention with verapamil after myocardial infarction.Am J Cardiol 1990;66:33I–40I.
156. Hansen JF, Tingsted L, Rasmussen V, Madsen JK, Jespersen CM.Verapamil and angiotensin-converting enzyme inhibitors in patientswith coronary artery disease and reduced left ventricular ejectionfraction. Am J Cardiol 1996;77:16D–21D.
157. Theroux P, Gregoire J, Chin C, Pelletier G, de Guise P, Juneau M.Intravenous diltiazem in acute myocardial infarction: Diltiazem asAdjunctive Therapy to Activase (DATA) trial. J Am Coll Cardiol1998;32:620–8.
158. Boden WE, Scheldewaert R, Walters EG, et al. Design of aplacebo-controlled clinical trial of long-acting diltiazem and aspirinversus aspirin alone in patients receiving thrombolysis with a firstacute myocardial infarction. Incomplete Infarction Trial of EuropeanResearch Collaborators Evaluating Prognosis Post-Thrombolysis(diltiazem) (INTERCEPT) Research Group. Am J Cardiol 1995;75:1120–3.
159. Yusuf S, Pepine CJ, Garces C, et al. Effect of enalapril on myocardialinfarction and unstable angina in patients with low ejection fractions.Lancet 1992;340:1173–8.
160. Rutherford JD, Pfeffer MA, Moye LA, et al. Effects of captopril onischemic events after myocardial infarction: results of the Survival andVentricular Enlargement trial: SAVE Investigators. Circulation1994;90:1731–8.
161. ACE Inhibitor Myocardial Infarction Collaborative Group. Indica-tions for ACE inhibitors in the early treatment of acute myocardialinfarction: systematic overview of individual data from 100,000patients in randomized trials. Circulation 1998;97:2202–12.
161a. Flather M, Yusuf S, Kober L, et al. Long-term ACE-inhibitortherapy in patients with heart failure or left ventricular dysfunction:a systematic overview of data from individual patients. Lancet2000;355:1575–81.
162. Gustafsson I, Torp-Pedersen C, Kober L, Gustafsson F, HildebrandtP. Effect of the angiotensin-converting enzyme inhibitor trandolaprilon mortality and morbidity in diabetic patients with left ventriculardysfunction after acute myocardial infarction. Trace Study Group.J Am Coll Cardiol 1999;34:83–9.
163. Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais G. Effectsof an angiotensin-converting-enzyme inhibitor, ramipril, on cardio-vascular events in high-risk patients. The Heart Outcomes Preven-tion Evaluation Study Investigators. N Engl J Med 2000;342:145–53.
164. TenVaarwerk IA, Jessurun GA, DeJongste MJ, et al. Clinicaloutcome of patients treated with spinal cord stimulation for thera-peutically refractory angina pectoris. The Working Group on Neu-rocardiology. Heart 1999;82:82–8.
165. Arora RR, Chou TM, Jain D, et al. The multicenter study of
enhanced external counterpulsation (MUST-EECP): effect of EECPon exercise-induced myocardial ischemia and anginal episodes. J AmColl Cardiol 1999;33:1833–40.
166. Conti CR. EECP-enhanced external counterpulsation. J Am CollCardiol 1999;33:1841–2.
167. Hautvast RW, DeJongste MJ, Staal MJ, van Gilst WH, Lie KI.Spinal cord stimulation in chronic intractable angina pectoris: arandomized, controlled efficacy study. Am Heart J 1998;136:1114–20.
168. Patel DJ, Purcell HJ, Fox KM. Cardioprotection by opening of theK(ATP) channel in unstable angina. Is this a clinical manifestation ofmyocardial preconditioning? Results of a randomized study withnicorandil. CESAR 2 investigation. Clinical European studies inangina and revascularization. Eur Heart J 1999;20:51–7.
169. Cohen M, Demers C, Gurfinkel EP, et al. A comparison oflow-molecular-weight heparin with unfractionated heparin for un-stable coronary artery disease. Efficacy and Safety of SubcutaneousEnoxaparin in Non–Q-Wave Coronary Events Study Group. N EnglJ Med 1997;337:447–52.
170. Antman EM, McCabe CH, Gurfinkel EP, et al. Enoxaparin pre-vents death and cardiac ischemic events in unstable angina/non–Q-wave myocardial infarction: results of the Thrombolysis In Myocar-dial Infarction (TIMI) 11B trial. Circulation 1999;100:1593–601.
171. Antman EM, Cohen M, Radley D, et al. Assessment of thetreatment effect of enoxaparin for unstable angina/non–Q-wavemyocardial infarction: TIMI 11B-ESSENCE meta-analysis. Circu-lation 1999;100:1602–8.
172. Cohen M, Theroux P, Weber S, et al. Combination therapy withtirofiban and enoxaparin in acute coronary syndromes. Int J Cardiol1999;71:273–81.
173. Antiplatelet Trialists’ Collaboration. Collaborative overview of ran-domised trials of antiplatelet therapy, I: prevention of death, myo-cardial infarction, and stroke by prolonged antiplatelet therapy invarious categories of patients [erratum appears in BMJ 1994;308:1540]. BMJ 1994;308:81–106.
174. Ridker PM, Cushman M, Stampfer MJ, Tracy RP, Hennekens CH.Inflammation, aspirin, and the risk of cardiovascular disease inapparently healthy men [erratum appears in N Engl J Med 1997;337:356]. N Engl J Med 1997;336:973–9.
175. Lewis HDJ, Davis JW, Archibald DG, et al. Protective effects ofaspirin against acute myocardial infarction and death in men withunstable angina: results of a Veterans Administration CooperativeStudy. N Engl J Med 1983;309:396–403.
176. Cairns JA, Gent M, Singer J, et al. Aspirin, sulfinpyrazone, or bothin unstable angina: results of a Canadian multicenter trial. N EnglJ Med 1985;313:1369–75.
177. Theroux P, Ouimet H, McCans J, et al. Aspirin, heparin, or both totreat acute unstable angina. N Engl J Med 1988;319:1105–11.
178. The RISC Group. Risk of myocardial infarction and death duringtreatment with low dose aspirin and intravenous heparin in men withunstable coronary artery disease. Lancet 1990;336:827–30.
179. Cohen M, Adams PC, Parry G, et al. Combination antithrombotictherapy in unstable rest angina and non–Q-wave infarction innonprior aspirin users: primary end points analysis from the ATACStrial. Antithrombotic Therapy in Acute Coronary Syndromes Re-search Group. Circulation 1994;89:81–8.
180. Gurfinkel EP, Manos EJ, Mejail RI, et al. Low molecular weightheparin versus regular heparin or aspirin in the treatment of unstableangina and silent ischemia. J Am Coll Cardiol 1995;26:313–8.
181. Fragmin during Instability in Coronary Artery Disease (FRISC)Study Group. Low-molecular-weight heparin during instability incoronary artery disease. Lancet 1996;347:561–8.
182. Randomised placebo-controlled trial of abciximab before and duringcoronary intervention in refractory unstable angina: the CAPTUREStudy [erratum appears in Lancet 19976;350:744]. Lancet 1997;349:1429–35.
183. The PARAGON Investigators. International, randomized, con-trolled trial of lamifiban (a platelet glycoprotein IIb/IIIa inhibitor),heparin, or both in unstable angina. Platelet IIb/IIIa Antagonism forthe Reduction of Acute coronary syndrome events in a GlobalOrganization Network. Circulation 1998;97:2386–95.
184. Platelet Receptor Inhibition in Ischemic Syndrome Management(PRISM) Study Investigators. A comparison of aspirin plus tirofiban
1048 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
with aspirin plus heparin for unstable angina. N Engl J Med1998;338:1498–505.
185. ISIS-2. ISIS-2 (Second International Study of Infarct Survival)Collaborative Group. Randomised trial of intravenous streptokinase,oral aspirin, both, or neither among 17,187 cases of suspected acutemyocardial infarction. Lancet 1988;2:349–60.
186. Song KH, Fedyk R, Hoover R. Interaction of ACE inhibitors andaspirin in patients with congestive heart failure. Ann Pharmacother1999;33:375–7.
187. Schror K. The basic pharmacology of ticlopidine and clopidogrel.Platelets 1993;4:252–61.
188. Balsano F, Rizzon P, Violi F, et al. Antiplatelet treatment withticlopidine in unstable angina: a controlled multicenter clinical trial.The Studio della Ticlopidina nell’Angina Instabile Group. Circula-tion 1990;82:17–26.
189. Love BB, Biller J, Gent M. Adverse haematological effects ofticlopidine. Prevention, recognition and management. Drug Safety1998;19:89–98.
190. CAPRIE Steering Committee. A randomised, blinded, trial ofClopidogrel versus Aspirin in Patients at Risk of Ischaemic Events(CAPRIE). Lancet 1996;348:1329–39.
191. Bennett CL, Connors JM, Carwile JM, et al. Thrombotic thrombo-cytopenic purpura associated with clopidogrel. N Engl J Med2000;342:1773–7.
192. Muller C, Buttner HJ, Petersen J, Roskamm H. A randomizedcomparison of clopidogrel and aspirin versus ticlopidine and aspirinafter the placement of coronary-artery stents. Circulation 2000;101:590–3.
193. The SYMPHONY Investigators. Comparison of sibrafiban withaspirin for prevention of cardiovascular events after acute coronarysyndromes: a randomised trial. Sibrafiban versus Aspirin to YieldMaximum Protection from Ischemic Heart Events Post-acute Cor-onary Syndromes. Lancet 2000;355:337–45.
193a. Cannon CP, McCabe CH, Wilcox RG, et al. Oral glycoproteinIIb/IIIa inhibition with orbofiban in patients with unstable coronarysyndromes (OPUS-TIMI 16) Trial. Circulation 2000;102:149–56.
193b. O’Neill WW, Serruys P, Knudtson M, et al. Long-term treatmentwith a platelet glycoprotein-receptor antagonist after percutaneouscoronary revascularization. N Engl J Med 2000;342:1316–24.
194. Hirsh J. Heparin. N Engl J Med 1991;324:1565–74.195. Weitz JI. Low-molecular-weight heparins [erratum appears in
N Engl J Med 1997;337:1567]. N Engl J Med 1997;337:688–98.196. Stone SR, Hofsteenge J. Kinetics of the inhibition of thrombin by
hirudin. Biochemistry 1986;25:4622–8.197. Bittl JA, Strony J, Brinker JA, et al. Treatment with bivalirudin
(Hirulog) as compared with heparin during coronary angioplasty forunstable or postinfarction angina. Hirulog Angioplasty Study Inves-tigators. N Engl J Med 1995;333:764–9.
198. Fuchs J, Cannon CP. Hirulog in the treatment of unstable angina:results of the Thrombin Inhibition in Myocardial Ischemia (TIMI) 7trial. Circulation 1995;92:727–33.
199. Kong DF, Topol EJ, Bittl JA, et al. Clinical outcomes of bivalirudinfor ischemic heart disease. N Engl J Med 1999;100:2049–53.
200. Telford AM, Wilson C. Trial of heparin versus atenolol in preventionof myocardial infarction in intermediate coronary syndrome. Lancet1981;1:1225–8.
201. Williams DO, Kirby MG, McPherson K, Phear DN. Anticoagulanttreatment of unstable angina. Br J Clin Pract 1986;40:114–6.
202. Theroux P, Waters D, Qiu S, McCans J, de Guise P, Juneau M.Aspirin versus heparin to prevent myocardial infarction during theacute phase of unstable angina. Circulation 1993;88:2045–8.
203. Neri SG, Gensini GF, Poggesi L, et al. Effect of heparin, aspirin, oralteplase in reduction of myocardial ischaemia in refractory unstableangina [erratum appears in Lancet 1990;335:868]. Lancet 1990;335:615–8.
204. Holdright D, Patel D, Cunningham D, et al. Comparison of theeffect of heparin and aspirin versus aspirin alone on transientmyocardial ischemia and in-hospital prognosis in patients withunstable angina. J Am Coll Cardiol 1994;24:39–45.
205. Cohen M, Adams PC, Hawkins L, Bach M, Fuster V. Usefulness ofantithrombotic therapy in resting angina pectoris or non-Q-wavemyocardial infarction in preventing death and myocardial infarction(a pilot study from the Antithrombotic Therapy in Acute CoronarySyndromes Study Group). Am J Cardiol 1990;66:1287–92.
206. Oler A, Whooley MA, Oler J, Grady D. Adding heparin to aspirinreduces the incidence of myocardial infarction and death in patientswith unstable angina: a meta-analysis. JAMA 1996;276:811–5.
207. Theroux P, Waters D, Lam J, Juneau M, McCans J. Reactivation ofunstable angina after the discontinuation of heparin. N Engl J Med1992;327:141–5.
208. Serruys PW, Herrman JP, Simon R, et al. A comparison of hirudinwith heparin in the prevention of restenosis after coronary angio-plasty. Helvetica Investigators. N Engl J Med 1995;333:757–63.
209. The Global Use of Strategies to Open Occluded Coronary Arteries(GUSTO) IIb Investigators. A comparison of recombinant hirudinwith heparin for the treatment of acute coronary syndromes. N EnglJ Med 1996;335:775–82.
210. Granger CB, Hirsch J, Califf RM, et al. Activated partial thrombo-plastin time and outcome after thrombolytic therapy for acutemyocardial infarction: results from the GUSTO-I trial. Circulation1996;93:870–8.
211. Granger CB, Miller JM, Bovill EG, et al. Rebound increase inthrombin generation and activity after cessation of intravenousheparin in patients with acute coronary syndromes. Circulation1995;91:1929–35.
212. Hirsh J, Warkentin TE, Raschke R, Granger C, Ohman EM, DalenJE. Heparin and low-molecular-weight heparin: mechanisms ofaction, pharmacokinetics, dosing considerations, monitoring, efficacy,and safety. Chest 1998;114:489S–510S.
213. Hassan WM, Flaker GC, Feutz C, Petroski GF, Smith D. Improvedanticoagulation with a weight-adjusted heparin nomogram in pa-tients with acute coronary syndromes: a randomized trial. J ThrombThrombolysis 1995;2:245–9.
214. Becker RC, Ball SP, Eisenberg P, et al. A randomized, multicentertrial of weight-adjusted intravenous heparin dose titration and point-of-care coagulation monitoring in hospitalized patients with activethromboembolic disease: Antithrombotic Therapy Consortium In-vestigators. Am Heart J 1999;137:59–71.
215. Hochman JS, Wali AU, Gavrila D, et al. A new regimen for heparinuse in acute coronary syndromes. Am Heart J 1999;138:313–8.
216. Wali A, Hochman JS, Berkowitz S, et al. Failure to achieve optimalanticoagulation with commonly used heparin regimens: a review ofGUSTO IIb (abstr). J Am Coll Cardiol 1998;31:79A.
217. Rubins HB, Robins SJ, Collins D, et al. Gemfibrozil for thesecondary prevention of coronary heart disease in men with low levelsof high-density lipoprotein cholesterol. N Engl J Med 1999;341:410–8.
218. Klein W, Buchwald A, Hillis SE, et al. Comparison of low-molecular-weight heparin with unfractionated heparin acutely andwith placebo for 6 weeks in the management of unstable coronaryartery disease. FRagmin In unstable Coronary artery disease study(FRIC) [erratum appears in Circulation 1998;97:413]. Circulation1997;96:61–8.
219. The FRAXIS study group. Comparison of two treatment durations(6 days and 14 days) of a low molecular weight heparin with a 6-daytreatment of unfractionated heparin in the initial management ofunstable angina or non-Q wave myocardial infarction: FRAX.I.S.(FRAXiparine in Ischaemic Syndrome). Eur Heart J 1999;20:1553–62.
220. Xiao Z, Theroux P. Platelet activation with unfractionated heparin attherapeutic concentrations and comparisons with a low-molecular-weight heparin and with a direct thrombin inhibitor. Circulation1998;97:251–6.
221. Warkentin TE, Levine MN, Hirsh J, et al. Heparin-induced throm-bocytopenia in patients treated with low-molecular-weight heparin orunfractionated heparin. N Engl J Med 1995;332:1330–5.
222. Mark DB, Cowper PA, Berkowitz SD, et al. Economic assessment oflow-molecular-weight heparin (enoxaparin) versus unfractionatedheparin in acute coronary syndrome patients: results from theESSENCE randomized trial. Efficacy and Safety of SubcutaneousEnoxaparin in Non-Q wave Coronary Events [unstable angina ornon–Q-wave myocardial infarction]. Circulation 1998;97:1702–7.
223. FRagmin and Fast Revascularisation during InStability in Coronaryartery disease Investigators. Long-term low-molecular-mass heparinin unstable coronary-artery disease: FRISC II prospective random-ised multicentre study. Lancet 1999;354:701–7.
224. The Global Use of Strategies to Open Occluded Coronary Arteries(GUSTO) IIa Investigators. Randomized trial of intravenous heparin
1049JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
versus recombinant hirudin for acute coronary syndromes. Circula-tion 1994;90:1631–7.
225. Antman EM. Hirudin in acute myocardial infarction: Thrombolysisand Thrombin Inhibition in Myocardial Infarction (TIMI) 9B trial.Circulation 1996;94:911–21.
226. Antman EM. Hirudin in acute myocardial infarction: safety reportfrom the Thrombolysis and Thrombin Inhibition in MyocardialInfarction (TIMI) 9A trial. Circulation 1994;90:1624–30.
227. Organization to Assess Strategies for Ischemic Syndromes (OASIS)Investigators. Comparison of the effects of two doses of recombinanthirudin compared with heparin in patients with acute myocardialischemia without ST elevation: a pilot study. Circulation 1997;96:769–77.
228. Organisation to Assess Strategies for Ischemic Syndromes(OASIS-2) Investigators. Effects of recombinant hirudin (lepirudin)compared with heparin on death, myocardial infarction, refractoryangina, and revascularisation procedures in patients with acutemyocardial ischaemia without ST elevation: a randomised trial.Lancet 1999;353:429–38.
229. Williams MJ, Morison IM, Parker JH, Stewart RA. Progression ofthe culprit lesion in unstable coronary artery disease with warfarin andaspirin versus aspirin alone: preliminary study. J Am Coll Cardiol1997;30:364–9.
230. Anand SS, Yusuf S, Pogue J, Weitz JI, Flather M. Long-term oralanticoagulant therapy in patients with unstable angina or suspectednon-Q-wave myocardial infarction: Organization to Assess Strategiesfor Ischemic Syndromes (OASIS) pilot study results. Circulation1998;98:1064–70.
231. Anand SS, Yusuf S. Oral anticoagulant therapy in patients withcoronary artery disease: a meta-analysis. JAMA 1999;282:2058–67.
232. Coumadin Aspirin Reinfarction Study (CARS) Investigators. Ran-domised double-blind trial of fixed low-dose warfarin with aspirin aftermyocardial infarction [see comments]. Lancet 1997;350:389–96.
233. The Combination Hemotherapy and Mortality Prevention(CHAMP) Study: Presented at the 72nd Scientific Session, Ameri-can Heart Association, 1999.
234. Lefkovits J, Plow EF, Topol EJ. Platelet glycoprotein IIb/IIIareceptors in cardiovascular medicine. N Engl J Med 1995;332:1553–9.
235. Coller BS. Monitoring platelet GP IIb/IIIa [corrected] antagonisttherapy [corrected in Circulation 1998;97:5–9]. Circulation 1997;96:3828–32.
236. Topol EJ, Byzova TV, Plow EF. Platelet GPIIb-IIIa blockers.Lancet 1999;353:227–31.
237. Coller BS. Potential non-glycoprotein IIb/IIIa effects of abciximab.Am Heart J 1999;138:S1–S5.
238. Tam SH, Sassoli PM, Jordan RE, Nakada MT. Abciximab (ReoPro,chimeric 7E3 Fab) demonstrates equivalent affinity and functionalblockade of glycoprotein IIb/IIIa and avb3 integrins. Circulation1998;98:1085–91.
239. Phillips DR, Scarborough RM. Clinical pharmacology of eptifi-batide. Am J Cardiol 1997;80:11B–20B.
240. Kleiman NS. Pharmacology of the intravenous platelet receptorglycoprotein IIb-IIIa antagonists. Cor Art Dis 1998;9:603–16.
241. Lynch JJ Jr, Cook JJ, Sitko GR, et al. Nonpeptide glycoproteinIIb/IIIa inhibitors. 5. Antithrombotic effects of MK-0383. J Phar-macol Exp Ther 1995;272:20–32.
242. Theroux P. Tirofiban. Drugs of Today. 1999;35:59–73.243. Peter K, Schwarz M, Ylanne J, et al. Induction of fibrinogen binding
and platelet aggregation as a potential intrinsic property of variousglycoprotein IIb/IIIa (aIIbb3) inhibitors. Blood 1998;92:3240–9.
244. Use of a monoclonal antibody directed against the platelet glycopro-tein IIb/IIIa receptor in high-risk coronary angioplasty. The EPICInvestigation. N Engl J Med 1994;330:956–61.
245. The EPILOG Investigators. Platelet glycoprotein IIb/IIIa receptorblockade and low-dose heparin during percutaneous coronary revas-cularization. N Engl J Med 1997;336:1689–96.
246. The EPISTENT Investigators. Randomised placebo-controlled andballoon-angioplasty-controlled trial to assess safety of coronary stent-ing with use of platelet glycoprotein-IIb/IIIa blockade. Evaluation ofPlatelet IIb/IIIa Inhibitor for Stenting. Lancet 1998;352:87–92.
247. Zhao XQ, Theroux P, Snapinn SM, Sax FL. Intracoronary thrombusand platelet glycoprotein IIb/IIIa receptor blockade with tirofibanin unstable angina or non–Q-wave myocardial infarction: angio-
graphic results from the PRISM-PLUS trial. Circulation 1999;100:1609 –15.
248. Boersma E, Akkerhuis KM, Theroux P, Califf RM, Topol EJ,Simoons ML. Platelet glycoprotein IIb/IIIa receptor inhibition innon–ST-elevation acute coronary syndromes: early benefit duringmedical treatment only, with additional protection during percuta-neous coronary intervention. Circulation 1999;100:2045–8.
249. Berkowitz SD, Sane DC, Sigmon KN, et al. Occurrence and clinicalsignificance of thrombocytopenia in a population undergoing high-risk percutaneous coronary revascularization. Evaluation of c7E3 forthe Prevention of Ischemic Complications (EPIC) Study Group.J Am Coll Cardiol 1998;32:311–9.
250. McClure MW, Berkowitz SD, Sparapani R, et al. Clinical signifi-cance of thrombocytopenia during a non–ST-elevation acute coro-nary syndrome. The platelet glycoprotein IIb/IIIa in unstable angina:receptor suppression using Integrilin therapy (PURSUIT) trial expe-rience. Circulation 1999;99:2892–900.
251. Baigent C, Collins R, Appleby P, Parish S, Sleight P, Peto R. ISIS-2:10 year survival among patients with suspected acute myocardialinfarction in randomised comparison of intravenous streptokinase, oralaspirin, both, or neither. The ISIS-2 (Second International Study ofInfarct Survival) Collaborative Group. BMJ 1998;316:1337–43.
252. Franzosi MG, Santoro E, De Vita C, et al. Ten-year follow-up of thefirst megatrial testing thrombolytic therapy in patients with acutemyocardial infarction: results of the Gruppo Italiano per lo Studiodella Sopravvivenza nell’Infarto-1 study. The GISSI Investigators.Circulation 1998;98:2659–65.
253. Miltenburg-van Zijl AJ, Simoons ML, Veerhoek RJ, Bossuyt PM.Incidence and follow-up of Braunwald subgroups in unstable anginapectoris. J Am Coll Cardiol 1995;25:1286–92.
254. Nyman I, Areskog M, Areskog NH, Swahn E, Wallentin L. Veryearly risk stratification by electrocardiogram at rest in men withsuspected unstable coronary heart disease. The RISC Study Group.J Intern Med 1993;234:293–301.
255. Gibbons RJ, Balady GJ, Beasley JW, et al. ACC/AHA guidelines forexercise testing: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Com-mittee on Exercise Testing). J Am Coll Cardiol 1997;30:260–311.
256. Cheitlin MD, Alpert JS, Armstrong WF, et al. ACC/AHA guide-lines for the clinical application of echocardiography: a report ofthe American College of Cardiology/American Heart AssociationTask Force on Practice Guidelines (Committee on ClinicalApplication of Echocardiography). Developed in collaborationwith the American Society of Echocardiography. Circulation1997;95:1686 –744.
257. Ritchie JL, Bateman TM, Bonow RO, et al. Guidelines for theclinical use of cardiac radionuclide imaging. Report of the AmericanCollege of Cardiology/American Heart Association Task Force onAssessment of Diagnostic and Therapeutic Cardiovascular Proce-dures (Committee on Radionuclide Imaging). Developed in collab-oration with the American Society of Nuclear Cardiology. J Am CollCardiol 1995;25:521–47.
258. Mark DB, Shaw L, Harrell FEJ, et al. Prognostic value of a treadmillexercise score in outpatients with suspected coronary artery disease.N Engl J Med 1991;325:849–53.
259. Nyman I, Larsson H, Areskog M, Areskog NH, Wallentin L. Thepredictive value of silent ischemia at an exercise test before dischargeafter an episode of unstable coronary artery disease. RISC StudyGroup. Am Heart J 1992;123:324–31.
260. Starling MR, Crawford MH, Kennedy GT, O’Rourke RA. Tread-mill exercise tests predischarge and six weeks post-myocardial infarc-tion to detect abnormalities of known prognostic value. Ann InternMed 1981;94:721–7.
261. Marwick TH, Anderson T, Williams MJ, et al. Exercise echocardi-ography is an accurate and cost-efficient technique for detection ofcoronary artery disease in women. J Am Coll Cardiol 1995;26:335–41.
262. Larsson H, Areskog M, Areskog NH, et al. Should the exercise test(ET) be performed at discharge or one month later after an episodeof unstable angina or non-Q-wave myocardial infarction? Int J CardImaging 1991;7:7–14.
1050 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
263. Russo CA, Dai H, Chow BK, et al. Analysis of death during the firsttwelve months among non-Q wave MI patients randomized to an“invasive” vs. “conservative” management strategy: results from theVANQWISH trial (abstr). Circulation 1998;98 Suppl I:I-492.
264. Scanlon PJ, Faxon DP, Audet A, et al. ACC/AHA guidelines forcoronary angiography: a report of the American College of Cardiol-ogy/American Heart Association Task Force on Practice Guidelines(Committee on Coronary Angiography). J Am Coll Cardiol 1999;33:1756–824.
265. McCullough PA, O’Neill WW, Graham M, et al. A prospectiverandomized trial of triage angiography in acute coronary syndromesineligible for thrombolytic therapy. Results of the Medicine versusAngiography in Thrombolytic Exclusion (MATE) trial. J Am CollCardiol 1998;32:596–605.
266. Boden WE, O’Rourke RA, Crawford MH, et al. Outcomes inpatients with acute non-Q-wave myocardial infarction randomlyassigned to an invasive as compared with a conservative managementstrategy. Veterans Affairs Non–Q-Wave Infarction Strategies inHospital (VANQWISH) Trial Investigators [erratum appears inN Engl J Med 1998;339:1091]. N Engl J Med 1998;338:1785–92.
267. RITA-2 Trial Participants. Coronary angioplasty versus medicaltherapy for angina: the second Randomised Intervention Treatmentof Angina (RITA-2) trial. Lancet 1997;350:461–8.
268. Peterson ED, Shaw LJ, Califf RM. Risk stratification after myocar-dial infarction. Ann Intern Med 1997;126:561–82.
269. Luchi RJ, Scott SM, Deupree RH. Comparison of medical andsurgical treatment for unstable angina pectoris: results of a VeteransAdministration Cooperative Study. N Engl J Med 1987;316:977–84.
270. Takaro T, Hultgren H, Lipton MJ, et al. The VA CooperativeRandomized Study of Surgery for Coronary Arterial OcclusiveDisease, II: subgroup with significant left main lesions. Circulation1976;54 Suppl III:III-107–III-17.
271. Kereiakes DJ, McDonald M, Broderick TM, et al. Abciximabprovides cost efficient, safely expedited care for unstable angina(abstr). Cathet Cardiovasc Diagn 1999;47:137.
272. Laskey MA, Deutsch E, Barnathan E, Laskey WK. Influence ofheparin therapy on percutaneous transluminal coronary angioplastyoutcome in unstable angina pectoris. Am J Cardiol 1990;65:1425–9.
273. Smith SC, Dove JT, Jacobs AK, et al. ACC/AHA guidelines forpercutaneous transluminal coronary angioplasty: a report of theAmerican College of Cardiology/American Heart Association TaskForce on Practice Guidelines (Committee on Percutaneous Translu-minal Coronary Angioplasty). J Am Coll Cardiol (in review).
274. Eagle KA, Guyton RA, Davidoff R, et al. ACC/AHA guidelines forcoronary artery bypass graft surgery: a report of the American Collegeof Cardiology/American Heart Association Task Force on PracticeGuidelines (Committee on Coronary Artery Bypass Graft Surgery).J Am Coll Cardiol 1999;34:1262–347.
275. Madsen JK, Grande P, Saunamaki K, et al. Danish multicenterrandomized study of invasive versus conservative treatment in pa-tients with inducible ischemia after thrombolysis in acute myocardialinfarction (DANAMI). DANish trial in Acute Myocardial Infarc-tion. Circulation 1997;96:748–55.
276. Pepine CJ, Geller NL, Knatterud GL, et al. The AsymptomaticCardiac Ischemia Pilot (ACIP) study: design of a randomized clinicaltrial, baseline data and implications for a long-term outcome trial [seecomments] [erratum appears in J Am Coll Cardiol 1995;26:842].J Am Coll Cardiol 1994;24:1–10.
277. Knatterud GL, Bourassa MG, Pepine CJ, et al. Effects of treatmentstrategies to suppress ischemia in patients with coronary arterydisease: 12-week results of the Asymptomatic Cardiac Ischemia Pilot(ACIP) study [see comments] [erratum appears in J Am Coll Cardiol1995;26:842]. J Am Coll Cardiol 1994;24:11–20.
278. FRagmin and Fast Revascularisation during InStability in Coronaryartery disease Investigators. Invasive compared with non-invasivetreatment in unstable coronary-artery disease: FRISC II prospectiverandomised multicentre study. Lancet 1999;354:708–15.
278a. Wallentin L, Lagerqvist B, Husted S, et al. Outcome at one yearafter an invasive compared with a non-invasive strategy in unstablecoronary artery disease: the FRISC II invasive randomized trial.Lancet 2000;356:9–16.
279. Yusuf S, Flather M, Pogue J, et al. Variations between countries ininvasive cardiac procedures and outcomes in patients with suspectedunstable angina or myocardial infarction without initial ST elevation.
OASIS (Organisation to Assess Strategies for Ischaemic Syndromes)Registry Investigators. Lancet 1998;352:507–14.
280. Ghazzal P, Chalasani Y, Weintraub WS. Long term outcome ofpatients with non-Q wave myocardial infarction with or withoutrevascularization (abstr). J Am Coll Cardiol 1998;31:14A.
281. Roe MT, Lauer MA, Houghtaling P, et al. An ischemia-guidedstrategy of cardiac catheterization in patients with non-ST-segmentelevation acute coronary syndromes may be associated with improvedoutcomes (abstr). J Am Coll Cardiol 1999;33:391A.
282. Stone PH, Thompson B, Zaret BL, et al. Factors associated withfailure of medical therapy in patients with unstable angina and non-Qwave myocardial infarction: a TIMI IIIB database study. Eur Heart J1999;20:1084–93.
283. Bugiardini R, Pozzati A, Borghi A, et al. Angiographic morphologyin unstable angina and its relation to transient myocardial ischemiaand hospital outcome. Am J Cardiol 1991;67:460–4.
284. Boden WE, Kerensky RA, Bertolet BD, et al. Coronary angiographicfindings after non-Q wave myocardial infarction: an analysis from theVANQWISH trial (abstr). Eur Heart J 1997;18:123.
285. Diver DJ, Bier JD, Ferreira PE, et al. Clinical and arteriographiccharacterization of patients with unstable angina without criticalcoronary arterial narrowing (from the TIMI-IIIA trial). Am JCardiol 1994;74:531–7.
286. Albertsson P, Emanuelsson H, Karlsson T, et al. Morbidity and useof medical resources in patients with chest pain and normal ornear-normal coronary arteries. Am J Cardiol 1997;79:299–304.
287. Potts SG, Bass CM. Psychosocial outcome and use of medical resourcesin patients with chest pain and normal or near-normal coronary arteries:a long-term follow-up study. Q J Med 1993;86:583–93.
288. Jones RH, Kesler K, Phillips HR, et al. Long-term survival benefitsof coronary artery bypass grafting and percutaneous transluminalangioplasty in patients with coronary artery disease. J Thorac Car-diovasc Surg 1996;111:1013–25.
289. Hannan EL, Racz MJ, McCallister BD, et al. A comparison ofthree-year survival after coronary artery bypass graft surgery andpercutaneous transluminal coronary angioplasty. J Am Coll Cardiol1999;33:63–72.
290. Rahimtoola SH, Nunley D, Grunkemeier G, Tepley J, Lambert L,Starr A. Ten-year survival after coronary bypass surgery for unstableangina. N Engl J Med 1983;308:676–81.
291. Levin TN, Holloway S, Feldman T. Acute and late clinical outcomeafter rotational atherectomy for complex coronary disease. CathetCardiovasc Diagn 1998;45:122–30.
292. Califf RM, Abdelmeguid AE, Kuntz RE, et al. Myonecrosis afterrevascularization procedures. J Am Coll Cardiol 1998;31:241–51.
293. Braden GA, Applegate RJ, Young TM. Abciximab decreases boththe incidence and magnitude of creatinine kinase elevation duringrotational atherectomy (abstr). J Am Coll Cardiol 1997;29 SupplA:499A.
294. Buchbinder MA, Braden GA, Sharma SK, et al. A pilot study ofReoPro with rotational atherectomy (RA) to reduce creatinine kinase(CK) elevation postprocedure (abstr). Circulation 1996;94 Suppl I:I-197.
295. Rosenblum J, Pensabene JF, Kramer B. The transluminal extractioncatheter device: atherectomy and removal of an intracoronary throm-bus. J Invest Cardiol 1991;3:10–2.
296. Lasorda DM, Incorvati DL, Randall RR. Extraction atherectomyduring myocardial infarction in a patient with prior coronary arterybypass surgery. Cathet Cardiovasc Diagn 1992;26:117–21.
297. Williams DO, Braunwald E, Thompson B, Sharaf BL, Buller CE,Knatterud GL. Results of percutaneous transluminal coronary angio-plasty in unstable angina and non–Q-wave myocardial infarction:observations from the TIMI IIIB trial. Circulation 1996;94:2749–55.
298. Moreyra AE, Palmeri ST, Wilson AC, Kulkarni A, Kulkarni R.Coronary angioplasty in unstable angina: contemporary experience.Can J Cardiol 1995;11:385–90.
299. Stammen F, De Scheerder I, Glazier JJ, et al. Immediate andfollow-up results of the conservative coronary angioplasty strategy forunstable angina pectoris. Am J Cardiol 1992;69:1533–7.
300. Perry RA, Seth A, Hunt A, Shiu MF. Coronary angioplasty inunstable angina and stable angina: a comparison of success andcomplications. Br Heart J 1988;60:367–72.
301. Safian RD, Snyder LD, Synder BA, et al. Usefulness of percutaneoustransluminal coronary angioplasty for unstable angina pectoris afternon-Q-wave acute myocardial infarction. Am J Cardiol 1987;59:263–6.
1051JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
302. Kamp O, Beatt KJ, De Feyter PJ, et al. Short-, medium-, andlong-term follow-up after percutaneous transluminal coronary angio-plasty for stable and unstable angina pectoris. Am Heart J 1989;117:991–6.
303. Cairns J, Theroux P, Armstrong P, et al. Unstable angina: reportfrom a Canadian expert roundtable. Can J Cardiol 1996;12:1279–92.
304. Khan MM, Ellis SG, Aguirre FV, et al. Does intracoronary thrombusinfluence the outcome of high risk percutaneous transluminal coro-nary angioplasty? Clinical and angiographic outcomes in a largemulticenter trial. EPIC Investigators. Evaluation of IIb/IIIa PlateletReceptor Antagonist 7E3 in Preventing Ischemic Complications.J Am Coll Cardiol 1998;31:31–6.
305. Malosky SA, Hirshfeld JWJ, Herrmann HC. Comparison of resultsof intracoronary stenting in patients with unstable vs. stable angina.Cathet Cardiovasc Diagn 1994;31:95–101.
306. Marzocchi A, Piovaccari G, Marrozzini C, et al. Results of coronarystenting for unstable versus stable angina pectoris. Am J Cardiol1997;79:1314–8.
307. Schuhlen H, Kastrati A, Dirschinger J, et al. Intracoronary stentingand risk for major adverse cardiac events during the first month.Circulation 1998;98:104–11.
308. Angidi M, Danchin N, Gangtoff C, et al. Ticlopidine-aspirin asanti-thrombotic regimen for intracoronary stenting for unstableangina: is there a need for further antiplatelet therapy (abstr)? J AmColl Cardiol 1998;31:100A.
309. Topol EJ, Califf RM, Weisman HF, et al. Randomised trial ofcoronary intervention with antibody against platelet IIb/IIIa integrinfor reduction of clinical restenosis: results at six months. The EPICInvestigators. Lancet 1994;343:881–6.
310. Topol EJ, Ferguson JJ, Weisman HF, et al. Long-term protectionfrom myocardial ischemic events in a randomized trial of briefintegrin b3 blockade with percutaneous coronary intervention. EPICInvestigator Group. Evaluation of Platelet IIb/IIIa Inhibition forPrevention of Ischemic Complication. JAMA 1997;278:479–84.
311. Kong DF, Califf RM, Miller DP, et al. Clinical outcomes oftherapeutic agents that block the platelet glycoprotein IIb/IIIaintegrin in ischemic heart disease. Circulation 1998;98:2829–35.
312. The RESTORE Investigators. Effects of platelet glycoprotein IIb/IIIa blockade with tirofiban on adverse cardiac events in patients withunstable angina or acute myocardial infarction undergoing coronaryangioplasty. Randomized Efficacy Study of Tirofiban for Outcomesand REstenosis. Circulation 1997;96:1445–53.
313. Lincoff AM, Califf RM, Moliterno DJ, et al. Complementary clinicalbenefits of coronary-artery stenting and blockade of platelet glyco-protein IIb/IIIa receptors: Evaluation of Platelet IIb/IIIa Inhibitionin Stenting Investigators. N Engl J Med 1999;341:319–27.
314. Theroux P, Ghannam A, Nasmith J, Barr E, Snapinn S, Sax FL.Improved cardiac outcomes in diabetic unstable angina/non–Q-wavemyocardial infarction patients treated with tirofiban and heparin(abstr). Circulation 1998;98 Suppl I:I-359.
315. Lincoff AM, Califf RM, Anderson KM, et al. Evidence for preven-tion of death and myocardial infarction with platelet membraneglycoprotein IIb/IIIa receptor blockade by abciximab (c7E3 Fab)among patients with unstable angina undergoing percutaneous coronaryrevascularization. EPIC Investigators. Evaluation of 7E3 in PreventingIschemic Complications. J Am Coll Cardiol 1997;30:149–56.
316. Randomised placebo-controlled trial of effect of eptifibatide oncomplications of percutaneous coronary intervention: IMPACT-II.Integrilin to Minimise Platelet Aggregation and CoronaryThrombosis-II. Lancet 1997;349:1422–8.
317. National Cooperative Study Group to Compare Surgical and MedicalTherapy. Unstable angina pectoris. Am J Cardiol 1978;42:839–48.
318. Scott SM, Deupree RH, Sharma GA, Luchi RJ. VA study ofunstable angina. 10-year results show duration of surgical advantagefor patients with impaired ejection fraction. Circulation 1994;90:II120–II123.
319. Parisi AF, Khuri S, Deupree RH, Sharma GV, Scott SM, LuchiRJ. Medical compared with surgical management of unstable angina:5-year mortality and morbidity in the Veterans AdministrationStudy. Circulation 1989;80:1176–89.
320. Scott SM, Luchi RJ, Deupree RH. Veterans Administration Coop-erative Study for treatment of patients with unstable angina: results inpatients with abnormal left ventricular function. Circulation 1988;78Suppl I:I-113–21.
321. Sharma GV, Deupree RH, Khuri SF, Parisi AF, Luchi RJ, Scott SM.Coronary bypass surgery improves survival in high-risk unstableangina: results of a Veterans Administration Cooperative study withan 8-year follow-up. Veterans Administration Unstable AnginaCooperative Study Group. Circulation 1991;84 Suppl III:III-260–7.
322. Pocock SJ, Henderson RA, Rickards AF, et al. Meta-analysis ofrandomised trials comparing coronary angioplasty with bypass sur-gery. Lancet 1995;346:1184–9.
323. Writing Group for the Bypass Angioplasty Revascularization Inves-tigation (BARI) Investigators. Five-year clinical and functional out-come comparing bypass surgery and angioplasty in patients withmultivessel coronary disease: a multicenter randomized trial. JAMA1997;277:715–21.
324. The Bypass Angioplasty Revascularization Investigation (BARI)Investigators. Comparison of coronary bypass surgery with angio-plasty in patients with multivessel disease [erratum appears in N EnglJ Med 1997;336:147]. N Engl J Med 1996;335:217–25.
325. National Heart, Lung, and Blood Institute, Bethesda, Maryland;Graduate School of Public Health, University of Pittsburgh, Pitts-burgh, Pennsylvania; and the BARI Investigative Sites. Seven-Yearoutcome in the Bypass Angioplasty Revascularization Investigation(BARI) by treatment and diabetic status. J Am Coll Cardiol2000;35:1122–9.
326. CABRI Trial Participants. First-year results of CABRI (CoronaryAngioplasty versus Bypass Revascularisation Investigation). Lancet1995;346:1179–84.
327. Weintraub WS, Stein B, Kosinski A, et al. Outcome of coronarybypass surgery versus coronary angioplasty in diabetic patients withmultivessel coronary artery disease. J Am Coll Cardiol 1998;31:10–9.
328. Detre KM, Guo P, Holubkov R, et al. Coronary revascularization indiabetic patients: a comparison of the randomized and observationalcomponents of the Bypass Angioplasty Revascularization Investiga-tion (BARI). Circulation 1999;99:633–40.
329. Yusuf S, Zucker D, Peduzzi P, et al. Effect of coronary artery bypassgraft surgery on survival: overview of 10-year results from randomisedtrials by the Coronary Artery Bypass Graft Surgery Trialists Collab-oration [erratum appears in Lancet 1994;344:1446]. Lancet 1994;344:563–70.
330. The Veterans Administration Coronary Artery Bypass Surgery Co-operative Study Group. Eleven-year survival in the Veterans Admin-istration randomized trial of coronary bypass surgery for stableangina. N Engl J Med 1984;311:1333–9.
331. Coronary Artery Surgery Study (CASS): a randomized trial of coronaryartery bypass surgery. Survival data. Circulation 1983;68:939–50.
332. De Feyter PJ, Serruys PW, Arnold A, et al. Coronary angioplasty ofthe unstable angina related vessel in patients with multivessel disease.Eur Heart J 1986;7:460–7.
333. Mock MB, Fisher LD, Holmes DRJ, et al. Comparison of effects ofmedical and surgical therapy on survival in severe angina pectoris andtwo-vessel coronary artery disease with and without left ventriculardysfunction: a Coronary Artery Surgery Study Registry Study. Am JCardiol 1988;61:1198–203.
333a. Dracup K, Alonzo AA, Atkins JM, et al. The physician’s role inminimizing prehospital delay in patients at high risk for acutemyocardial infarction: recommendations from the National HeartAttack Alert Program. Ann Intern Med 1997;126:645–51.
334. Hulley S, Grady D, Bush T, et al. Randomized trial of estrogen plusprogestin for secondary prevention of coronary heart disease inpostmenopausal women. Heart and Estrogen/progestin ReplacementStudy (HERS) Research Group. JAMA 1998;280:605–13.
335. Schechtman KB, Capone RJ, Kleiger RE, et al. Risk stratification ofpatients with non–Q wave myocardial infarction: the critical role ofST segment depression. The Diltiazem Reinfarction Study ResearchGroup. Circulation 1989;80:1148–58.
336. Newby LK, Christenson RH, Ohman EM, et al. Value of serialtroponin T measures for early and late risk stratification in patientswith acute coronary syndromes. The GUSTO-IIa Investigators.Circulation 1998;98:1853–9.
337. van Domburg RT, Miltenburg-van Zijl AJ, Veerhoek RJ, SimoonsML. Unstable angina: good long-term outcome after a complicatedearly course. J Am Coll Cardiol 1998;31:1534–9.
338. Frasure-Smith N, Lesperance F, Talajic M. Depression and 18-month prognosis after myocardial infarction [erratum appears inCirculation 1998;97:708]. Circulation 1995;91:999–1005.
1052 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
339. Beckie T. A supportive-educative telephone program: impact onknowledge and anxiety after coronary artery bypass graft surgery.Heart Lung 1989;18:46–55.
340. Randomised trial of cholesterol lowering in 4444 patients withcoronary heart disease: the Scandinavian Simvastatin Survival Study(4S). Lancet 1994;344:1383–9.
341. The Long-Term Intervention with Pravastatin in Ischaemic Disease(LIPID) Study Group. Prevention of cardiovascular events and deathwith pravastatin in patients with coronary heart disease and a broadrange of initial cholesterol levels. N Engl J Med 1998;339:1349–57.
342. Sacks FM, Pfeffer MA, Moye LA, et al. The effect of pravastatin oncoronary events after myocardial infarction in patients with averagecholesterol levels. Cholesterol and Recurrent Events Trial Investiga-tors. N Engl J Med 1996;335:1001–9.
343. Flaker GC, Warnica JW, Sacks FM, et al. Pravastatin preventsclinical events in revascularized patients with average cholesterolconcentrations. Cholesterol and Recurrent Events CARE Investiga-tors. J Am Coll Cardiol 1999;34:106–12.
343a. National Cholesterol Education Program. Second report of theExpert Panel on Detection, Evaluation, and Treatment of HighBlood Cholesterol in Adults (Adult Treatment Panel II). Washing-ton, DC: US Dept of Health and Human Services; 1993. NIHpublication No. 93-3096.
343b. Grundy SM, Balady GJ, Criqui MH, et al. When to startcholesterol-lowering therapy in patients with coronary heart disease.Circulation 1997;95:1683–5.
343c. Dupuis J, Tardif J-C, Cernacek P, Theroux P. Cholesterol reductionrapidly improves endothelial function after acute coronary syn-dromes: the RECIFE (REduction of Cholesterol in Ischemia andFunction of the Endothelium) trial. Circulation 1999;99:3227–33.
344. National High Blood Pressure Education Program NN. The sixthreport of the Joint National Committee on Prevention, Detection,Evaluation, and Treatment of High Blood Pressure. Bethesda, MD:National Institutes of Health; 1997; NIH Publication No. 98-4080.
345. Daly LE, Mulcahy R, Graham IM, Hickey N. Long term effect onmortality of stopping smoking after unstable angina and myocardialinfarction. Br Med J (Clin Res Ed) 1983;287:324–6.
346. Smoking cessation. Rockville, MD: Agency for Health Care Policyand Research and the National Heart, Lung, and Blood Institute, USPublic Health Service, US Department of Health and HumanServices; 1996; AHCPR Publication No 96-0692.
347. Malmberg K, Ryden L, Efendic S, et al. Randomized trial ofinsulin-glucose infusion followed by subcutaneous insulin treatment indiabetic patients with acute myocardial infarction (DIGAMI study):effects on mortality at 1 year. J Am Coll Cardiol 1995;26:57–65.
348. American Diabetes Association. Standards of medical care for pa-tients with diabetes mellitus (position statement). Diabetes Care1999;22 Suppl 1:S32–41.
349. UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with con-ventional treatment and risk of complications in patients with type 2diabetes (UKPDS 33). Lancet 1998;352:837–53.
350. UK Prospective Diabetes Study (UKPDS) Group. Effect of intensiveblood-glucose control with metformin on complications in over-weight patients with type 2 diabetes (UKPDS 34) [erratum appears inLancet 1998;352:1557]. Lancet 1998;352:854–65.
351. UK Prospective Diabetes Study Group. Tight blood pressure controland risk of macrovascular and microvascular complications in type 2diabetes: UKPDS 38. BMJ 1998;317:703–13.
352. Stampfer MJ, Malinow MR, Willett WC, et al. A prospective studyof plasma homocysteine and risk of myocardial infarction in USphysicians. JAMA 1992;268:877–81.
353. Ubbink JB, Vermaak WJ, van der Merwe A, Becker PJ. VitaminB-12, vitamin B-6, and folate nutritional status in men withhyperhomocysteinemia. Am J Clin Nutr 1993;57:47–53.
354. Sullivan AK, Holdright DR, Wright CA, Sparrow JL, CunninghamD, Fox KM. Chest pain in women: clinical, investigative, andprognostic features. BMJ 1994;308:883–6.
355. Cannon RO, Camici PG, Epstein SE. Pathophysiological dilemmaof syndrome X. Circulation 1992;85:883–92.
356. DeSanctis RW. Clinical manifestations of coronary artery disease:chest pain in women. In: Wenger NK, Speroff L, Packard B, eds.Cardiovascular health and disease in women. Greenwich, CT: LeJacq Communications, Inc; 1993:67.
357. Stone PH, Thompson B, Anderson HV, et al. Influence of race, sex,and age on management of unstable angina and non-Q-wave myo-cardial infarction: the TIMI III registry. JAMA 1996;275:1104–12.
358. Keelan ET, Nunez BD, Grill DE, Berger PB, Holmes DRJ, BellMR. Comparison of immediate and long-term outcome of coronaryangioplasty performed for unstable angina and rest pain in men andwomen. Mayo Clin Proc 1997;72:5–12.
359. Robertson T, Kennard ED, Mehta S, et al. Influence of gender onin-hospital clinical and angiographic outcomes and on one-yearfollow-up in the New Approaches to Coronary Intervention (NACI)registry. Am J Cardiol 1997;80:26K–39K.
360. Morise AP, Diamond GA. Comparison of the sensitivity andspecificity of exercise electrocardiography in biased and unbiasedpopulations of men and women. Am Heart J 1995;130:741–7.
361. Williams MJ, Marwick TH, O’Gorman D, Foale RA. Comparisonof exercise echocardiography with an exercise score to diagnosecoronary artery disease in women. Am J Cardiol 1994;74:435–8.
362. Robert AR, Melin JA, Detry JM. Logistic discriminant analysisimproves diagnostic accuracy of exercise testing for coronary arterydisease in women. Circulation 1991;83:1202–9.
363. Melin JA, Wijns W, Vanbutsele RJ, et al. Alternative diagnosticstrategies for coronary artery disease in women: demonstration of theusefulness and efficiency of probability analysis. Circulation 1985;71:535–42.
364. Alexander KP, Shaw LJ, DeLong ER, Mark DB, Peterson ED.Value of exercise treadmill testing in women. J Am Coll Cardiol1998;32:1657–64.
365. Lewis JF, Lin L, McGorray S, et al. Dobutamine stress echocardi-ography in women with chest pain: pilot phase data from theNational Heart, Lung and Blood Institute Women’s Ischemia Syn-drome Evaluation (WISE). J Am Coll Cardiol 1999;33:1462–8.
366. Shaw LJ, Miller DD, Romeis JC, Kargl D, Younis LT, ChaitmanBR. Gender differences in the noninvasive evaluation and manage-ment of patients with suspected coronary artery disease. Ann InternMed 1994;120:559–66.
367. Cowley MJ, Mullin SM, Kelsey SF, et al. Sex differences in early andlong-term results of coronary angioplasty in the NHLBI PTCARegistry. Circulation 1985;71:90–7.
368. Kelsey SF, James M, Holubkov AL, Holubkov R, Cowley MJ, DetreKM. Results of percutaneous transluminal coronary angioplasty inwomen: 1985–1986 National Heart, Lung, and Blood Institute’sCoronary Angioplasty Registry. Circulation 1993;87:720–7.
369. Bell MR, Holmes DRJ, Berger PB, Garratt KN, Bailey KR, GershBJ. The changing in-hospital mortality of women undergoing percuta-neous transluminal coronary angioplasty. JAMA 1993;269:2091–5.
370. Fisher LD, Kennedy JW, Davis KB, et al. Association of sex, physicalsize, and operative mortality after coronary artery bypass in theCoronary Artery Surgery Study (CASS). J Thorac Cardiovasc Surg1982;84:334–41.
371. Loop FD, Golding LR, MacMillan JP, Cosgrove DM, Lytle BW,Sheldon WC. Coronary artery surgery in women compared withmen: analyses of risks and long-term results. J Am Coll Cardiol1983;1:383–90.
372. Arnold AM, Mick MJ, Piedmonte MR, Simpfendorfer C. Genderdifferences for coronary angioplasty. Am J Cardiol 1994;74:18–21.
373. Weintraub WS, Wenger NK, Kosinski AS, et al. Percutaneoustransluminal coronary angioplasty in women compared with men.J Am Coll Cardiol 1994;24:81–90.
374. Welty FK, Mittleman MA, Healy RW, Muller JE, Shubrooks SJJ.Similar results of percutaneous transluminal coronary angioplasty forwomen and men with postmyocardial infarction ischemia. J Am CollCardiol 1994;23:35–9.
375. Eysmann SB, Douglas PS. Coronary heart disease: therapeuticprinciples. In: Douglas PS, ed. Cardiovascular health and disease inwomen. Philadelphia, PA: WB Saunders; 1993:43.
376. Jacobs AK, Kelsey SF, Yeh W, et al. Documentation of decline inmorbidity in women undergoing coronary angioplasty (a report fromthe 1993–94 NHLBI Percutaneous Transluminal Coronary Angio-plasty Registry). National Heart, Lung, and Blood Institute. Am JCardiol 1997;80:979–84.
377. Hannan EL, Bernard HR, Kilburn HCJ, O’Donnell JF. Genderdifferences in mortality rates for coronary artery bypass surgery. AmHeart J 1992;123:866–72.
378. O’Connor GT, Morton JR, Diehl MJ, et al. Differences between men
1053JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
and women in hospital mortality associated with coronary arterybypass graft surgery. The Northern New England CardiovascularDisease Study Group. Circulation 1993;88:2104–10.
379. Rahimtoola SH, Bennett AJ, Grunkemeier GL, Block P, Starr A.Survival at 15 to 18 years after coronary bypass surgery for angina inwomen. Circulation 1993;88 Suppl II:II-71–78.
380. Weintraub WS, Wenger NK, Jones EL, Craver JM, Guyton RA.Changing clinical characteristics of coronary surgery patients: differ-ences between men and women. Circulation 1993;88 Suppl II:II-79–86.
381. Safstrom K, Nielsen NE, Bjorkholm A, Wiklund G, Swahn E.Unstable coronary artery disease in post-menopausal women: identi-fying patients with significant coronary artery disease by basic clinicalparameters and exercise test. IRIS Study Group. Eur Heart J1998;19:899–907.
382. Jacobs AK, Kelsey SF, Brooks MM, et al. Better outcome for womencompared with men undergoing coronary revascularization: a reportfrom the Bypass Angioplasty Revascularization Investigation(BARI). Circulation 1998;98:1279–85.
383. Influence of diabetes on 5-year mortality and morbidity in a random-ized trial comparing CABG and PTCA in patients with multivesseldisease: the Bypass Angioplasty Revascularization Investigation(BARI). Circulation 1997;96:1761–9.
384. Theroux P, Kouz S, Roy L, et al. Platelet membrane receptorglycoprotein IIb/IIIa antagonism in unstable angina. The CanadianLamifiban Study. Circulation 1996;94:899–905.
385. Topol EJ, Fuster V, Harrington RA, et al. Recombinant hirudin forunstable angina pectoris: a multicenter, randomized angiographictrial. Circulation 1994;89:1557–66.
386. Kip KE, Faxon DP, Detre KM, Yeh W, Kelsey SF, Currier JW.Coronary angioplasty in diabetic patients: the National Heart, Lung,and Blood Institute Percutaneous Transluminal Coronary Angio-plasty Registry. Circulation 1996;94:1818–25.
387. Stein B, Weintraub WS, Gebhart SP, et al. Influence of diabetesmellitus on early and late outcome after percutaneous transluminalcoronary angioplasty. Circulation 1995;91:979–89.
388. Wilcox I, Freedman SB, Allman KC, et al. Prognostic significance ofa predischarge exercise test in risk stratification after unstable anginapectoris. J Am Coll Cardiol 1991;18:677–83.
389. Karlson BW, Herlitz J, Pettersson P, Hallgren P, Strombom U,Hjalmarson A. One-year prognosis in patients hospitalized with ahistory of unstable angina pectoris. Clin Cardiol 1993;16:397–402.
390. Fava S, Azzopardi J, Agius-Muscat H. Outcome of unstable anginain patients with diabetes mellitus. Diabet Med 1997;14:209–13.
391. Garcia-Rubira JC, Cruz JM, Lopez V, Plaza L, Navas JC. Outcomeof patients with diabetes and unstable angina: a subgroup analysis inthe Spanish Multicentre Trial of trifusal in unstable angina. Grupo deEstudio del Trifusal en la Angina Inestable. Int J Cardiol 1994;46:175–8.
392. Theroux P, Waters D. Unstable angina: special considerations in thepost-bypass patient. In: Waters D, Bourassa MG, Brest AN, eds.Care of the patient with previous coronary bypass surgery. Philadel-phia, PA: FA Davis; 1991:169–91.
393. Marchant B, Umachandran V, Stevenson R, Kopelman PG, TimmisAD. Silent myocardial ischemia: role of subclinical neuropathy inpatients with and without diabetes. J Am Coll Cardiol 1993;22:1433–7.
394. Ambepityia G, Kopelman PG, Ingram D, Swash M, Mills PG,Timmis AD. Exertional myocardial ischemia in diabetes: a quanti-tative analysis of anginal perceptual threshold and the influence ofautonomic function. J Am Coll Cardiol 1990;15:72–7.
395. Zola B, Kahn JK, Juni JE, Vinik AI. Abnormal cardiac function indiabetic patients with autonomic neuropathy in the absence ofischemic heart disease. J Clin Endocrinol Metab 1986;63:208–14.
396. Silva JA, Escobar A, Collins TJ, Ramee SR, White CJ. Unstableangina: a comparison of angioscopic findings between diabetic andnondiabetic patients. Circulation 1995;92:1731–6.
397. Jones EL, Weintraub WS, Craver JM, Guyton RA, Cohen CL.Coronary bypass surgery: is the operation different today? J ThoracCardiovasc Surg 1991;101:108–15.
398. King SB, III, Kosinski A, Guyton RA, Lembo NJ, Weintraub WS.Eight year mortality in the Emory Angioplasty vs Surgery Trial(EAST). J Am Coll Cardiol 2000;35:1116–21.
399. Kuntz RE. Importance of considering atherosclerosis progressionwhen choosing a coronary revascularization strategy: the diabetes-
percutaneous transluminal coronary angioplasty dilemma. Circulation1999;99:847–51.
400. Barsness GW, Peterson ED, Ohman EM, et al. Relationshipbetween diabetes mellitus and long-term survival after coronarybypass and angioplasty. Circulation 1997;96:2551–6.
401. Levine GN, Jacobs AK, Keeler GP, et al. Impact of diabetes mellituson percutaneous revascularization (CAVEAT-I). CAVEAT-I Inves-tigators. Coronary Angioplasty Versus Excisional Atherectomy Trial.Am J Cardiol 1997;79:748–55.
402. Kleiman NS, Lincoff AM, Kereiakes DJ, et al. Diabetes mellitus,glycoprotein IIb/IIIa blockade, and heparin: evidence for a complexinteraction in a multicenter trial. EPILOG Investigators. Circulation1998;97:1912–20.
403. Topol EJ, Mark DB, Lincoff AM, et al. Outcomes at 1 year andeconomic implications of platelet glycoprotein IIb/IIIa blockade inpatients undergoing coronary stenting: results from a multicentrerandomised trial. EPISTENT Investigators. Evaluation of PlateletIIb/IIIa Inhibitor for Stenting. Lancet 1999;354:2019–24.
404. Lambert M, Kouz S, Campeau L. Preoperative and operativepredictive variables of late clinical events following saphenous veincoronary artery bypass graft surgery. Can J Cardiol 1989;5:87–92.
405. Waters DD, Walling A, Roy D, Theroux P. Previous coronary arterybypass grafting as an adverse prognostic factor in unstable anginapectoris. Am J Cardiol 1986;58:465–9.
406. Grondin CM, Campeau L, Lesperance J, Enjalbert M, BourassaMG. Comparison of late changes in internal mammary artery andsaphenous vein grafts in two consecutive series of patients 10 yearsafter operation. Circulation 1984;70 Suppl I:I-208–12.
407. Neitzel GF, Barboriak JJ, Pintar K, Qureshi I. Atherosclerosis inaortocoronary bypass grafts: morphologic study and risk factoranalysis 6 to 12 years after surgery. Arteriosclerosis 1986;6:594–600.
408. Waller BF, Rothbaum DA, Gorfinkel HJ, Ulbright TM, LinnemeierTJ, Berger SM. Morphologic observations after percutaneous trans-luminal balloon angioplasty of early and late aortocoronary saphenousvein bypass grafts. J Am Coll Cardiol 1984;4:784–92.
409. Walts AE, Fishbein MC, Sustaita H, Matloff JM. Ruptured ather-omatous plaques in saphenous vein coronary artery bypass grafts: amechanism of acute, thrombotic, late graft occlusion. Circulation1982;65:197–201.
410. Hwang MH, Meadows WR, Palac RT, et al. Progression of nativecoronary artery disease at 10 years: insights from a randomized studyof medical versus surgical therapy for angina. J Am Coll Cardiol1990;16:1066–70.
411. Chen L, Theroux P, Lesperance J, Shabani F, Thibault B, de GuiseP. Angiographic features of vein grafts versus ungrafted coronaryarteries in patients with unstable angina and previous bypass surgery.J Am Coll Cardiol 1996;28:1493–9.
412. Waters DD, Theroux P, Crittin J, Dauwe F, Mizgala HF. Previouslyundiagnosed variant angina as a cause of chest pain after coronaryartery bypass surgery. Circulation 1980;61:1159–64.
413. Baduini G, Marra S, Angelino PF. Sudden occlusion of a saphenousvein bypass graft relieved by direct injection of nitroglycerin. CathetCardiovasc Diagn 1981;7:87–95.
414. Lawrie GM, Morris GCJ, Silvers A, et al. The influence of residualdisease after coronary bypass on the 5-year survival rate of 1274 menwith coronary artery disease. Circulation 1982;66:717–23.
415. Silva JA, White CJ, Collins TJ, Ramee SR. Morphologic comparisonof atherosclerotic lesions in native coronary arteries and saphenousvein graphs with intracoronary angioscopy in patients with unstableangina. Am Heart J 1998;136:156–63.
416. Ritchie JL, Narahara KA, Trobaugh GB, Williams DL, HamiltonGW. Thallium-201 myocardial imaging before and after coronaryrevascularization: assessment of regional myocardial blood flow andgraft patency. Circulation 1977;56:830–6.
417. Verani MS, Marcus ML, Spoto G, Rossi NP, Ehrhardt JC, RazzakMA. Thallium-201 myocardial perfusion scintigrams in the evalua-tion of aorto-coronary saphenous bypass surgery. J Nucl Med1978;19:765–72.
418. Carlino M, De Gregorio J, di Mario C, et al. Prevention of distalembolization during saphenous vein graft lesion angioplasty: experi-ence with a new temporary occlusion and aspiration system. Circu-lation 1999;99:3221–3.
419. Kleiman NS, Anderson HV, Rogers WJ, Theroux P, Thompson B,Stone PH. Comparison of outcome of patients with unstable angina
1054 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
and non-Q-wave acute myocardial infarction with and without priorcoronary artery bypass grafting (Thrombolysis in Myocardial Isch-emia III Registry). Am J Cardiol 1996;77:227–31.
420. Savage MP, Douglas JSJ, Fischman DL, et al. Stent placementcompared with balloon angioplasty for obstructed coronary bypassgrafts. Saphenous Vein De Novo Trial Investigators. N Engl J Med1997;337:740–7.
421. Lytle BW, Loop FD, Taylor PC, et al. The effect of coronaryreoperation on the survival of patients with stenoses in saphenousvein bypass grafts to coronary arteries. J Thorac Cardiovasc Surg1993;105:605–12.
422. Lytle BW, Loop FD, Taylor PC, et al. Vein graft disease: the clinicalimpact of stenoses in saphenous vein bypass grafts to coronaryarteries. J Thorac Cardiovasc Surg 1992;103:831–40.
423. Lakatta EG, Gerstenblith G, Weisfeldt ML. The aging heart:structure, function, and disease. In: Braunwald E, ed. Heart disease,5th ed. Philadelphia, PA: WB Saunders; 1997:1687–703.
424. Nadelmann J, Frishman WH, Ooi WL, et al. Prevalence, incidenceand prognosis of recognized and unrecognized myocardial infarctionin persons aged 75 years or older: the Bronx Aging Study. Am JCardiol 1990;66:533–7.
425. Vasilomanolakis EC. Geriatric cardiology: when exercise stress test-ing is justified. Geriatrics 1985;40:47–4, 57.
426. Kasser IS, Bruce RA. Comparative effects of aging and coronary heartdisease on submaximal and maximal exercise. Circulation 1969;39:759–74.
427. Stein B, Kupersmith J. Principles and practice of pharmacotherapy.In: Kupersmith J, Deedwania PC, eds. The pharmacologic manage-ment of heart disease, 1st ed. Baltimore, MD: Williams & Wilkins;1997:3–38.
428. Montamat SC, Cusack BJ, Vestal RE. Management of drug therapyin the elderly. N Engl J Med 1989;321:303–9.
429. Thompson RC, Holmes DRJ, Grill DE, Mock MB, Bailey KR.Changing outcome of angioplasty in the elderly. J Am Coll Cardiol1996;27:8–14.
430. Nasser TK, Fry ET, Annan K, et al. Comparison of six-monthoutcome of coronary artery stenting in patients ,65, 65–75, and .75years of age. Am J Cardiol 1997;80:998–1001.
431. Peterson ED, Jollis JG, Bebchuk JD, et al. Changes in mortality aftermyocardial revascularization in the elderly: the national Medicareexperience. Ann Intern Med 1994;121:919–27.
432. O’Keefe JHJ, Sutton MB, McCallister BD, et al. Coronary angio-plasty versus bypass surgery in patients .70 years old matched forventricular function. J Am Coll Cardiol 1994;24:425–30.
433. Kaul TK, Fields BL, Wyatt DA, Jones CR, Kahn DR. Angioplastyversus coronary artery bypass in octogenarians. Ann Thorac Surg1994;58:1419–26.
434. Laster SB, Rutherford BD, Giorgi LV, et al. Results of directpercutaneous transluminal coronary angioplasty in octogenarians.Am J Cardiol 1996;77:10–3.
435. Thompson RC, Holmes DRJ, Gersh BJ, Bailey KR. Predicting earlyand intermediate-term outcome of coronary angioplasty in theelderly. Circulation 1993;88:1579–87.
436. Morrison DA, Bies RD, Sacks J. Coronary angioplasty for elderlypatients with “high risk” unstable angina: short-term outcomes andlong-term survival. J Am Coll Cardiol 1997;29:339–44.
437. Weyrens FJ, Goldenberg I, Mooney JF, et al. Percutaneous translu-minal coronary angioplasty in patients aged . or 5 90 years. Am JCardiol 1994;74:397–8.
438. Ivanov J, Weisel RD, David TE, Naylor CD. Fifteen-year trends inrisk severity and operative mortality in elderly patients undergoingcoronary artery bypass graft surgery. Circulation 1998;97:673–80.
439. Freeman WK, Schaff HV, O’Brien PC, Orszulak TA, Naessens JM,Tajik AJ. Cardiac surgery in the octogenarian: perioperative outcomeand clinical follow-up. J Am Coll Cardiol 1991;18:29–35.
440. Ko W, Gold JP, Lazzaro R, et al. Survival analysis of octogenarianpatients with coronary artery disease managed by elective coronaryartery bypass surgery versus conventional medical treatment. Circu-lation 1992;86 Suppl II:II-191–7.
441. Glower DD, Christopher TD, Milano CA, et al. Performance statusand outcome after coronary artery bypass grafting in persons aged 80to 93 years. Am J Cardiol 1992;70:567–71.
442. Chakko S, Myerburg RJ. Cardiac complications of cocaine abuse.Clin Cardiol 1995;18:67–72.
443. Isner JM, Chokshi SK. Cardiovascular complications of cocaine.Curr Probl Cardiol 1991;16:89–123.
444. Kloner RA, Hale S, Alker K, Rezkalla S. The effects of acute andchronic cocaine use on the heart. Circulation 1992;85:407–19.
445. Pitts WR, Lange RA, Cigarroa JE, Hillis LD. Cocaine-inducedmyocardial ischemia and infarction: pathophysiology, recognition,and management. Prog Cardiovasc Dis 1997;40:65–76.
446. Lange RA, Flores ED, Cigarroa RG, Hillis LD. Cocaine-inducedmyocardial ischemia. Cardio 1990;7:74–5, 78–9.
447. Loper KA. Clinical toxicology of cocaine. Med Toxicol AdverseDrug Exp 1989;4:174–85.
448. Flores ED, Lange RA, Cigarroa RG, Hillis LD. Effect of cocaine oncoronary artery dimensions in atherosclerotic coronary artery disease:enhanced vasoconstriction at sites of significant stenoses. J Am CollCardiol 1990;16:74–9.
449. Lange RA, Cigarroa RG, Yancy CWJ, et al. Cocaine-inducedcoronary-artery vasoconstriction. N Engl J Med 1989;321:1557–62.
450. Zimmerman FH, Gustafson GM, Kemp HGJ. Recurrent myocardialinfarction associated with cocaine abuse in a young man with normalcoronary arteries: evidence for coronary artery spasm culminating inthrombosis. J Am Coll Cardiol 1987;9:964–8.
451. Bedotto JB, Lee RW, Lancaster LD, Olajos M, Goldman S. Cocaineand cardiovascular function in dogs: effects on heart and peripheralcirculation. J Am Coll Cardiol 1988;11:1337–42.
452. Brogan WC, Lange RA, Kim AS, Moliterno DJ, Hillis LD.Alleviation of cocaine-induced coronary vasoconstriction by nitro-glycerin. J Am Coll Cardiol 1991;18:581–6.
453. Isner JM, Chokshi SK. Cocaine and vasospasm. N Engl J Med1989;321:1604–6.
454. Nademanee K, Gorelick DA, Josephson MA, et al. Myocardialischemia during cocaine withdrawal. Ann Intern Med 1989;111:876–80.
455. Vitullo JC, Karam R, Mekhail N, Wicker P, Engelmann GL,Khairallah PA. Cocaine-induced small vessel spasm in isolated rathearts. Am J Pathol 1989;135:85–91.
456. Togna G, Tempesta E, Togna AR, Dolci N, Cebo B, Caprino L.Platelet responsiveness and biosynthesis of thromboxane and prosta-cyclin in response to in vitro cocaine treatment. Haemostasis 1985;15:100–7.
457. Chokshi SK, Miller G, Rogione A, Isner JM. Cocaine and cardio-vascular diseases. Leading Edge Cardiol 1989;3:1ff.
458. Stenberg RG, Winniford MD, Hillis LD, Dowling GP, Buja LM.Simultaneous acute thrombosis of two major coronary arteries followingintravenous cocaine use. Arch Pathol Lab Med 1989;113:521–4.
459. Hollander JE, Hoffman RS, Gennis P, et al. Prospective multicenterevaluation of cocaine-associated chest pain. Cocaine AssociatedChest Pain (COCHPA) Study Group. Acad Emerg Med 1994;1:330–9.
460. Gitter MJ, Goldsmith SR, Dunbar DN, Sharkey SW. Cocaine andchest pain: clinical features and outcome of patients hospitalized torule out myocardial infarction. Ann Intern Med 1991;115:277–82.
461. Dressler FA, Malekzadeh S, Roberts WC. Quantitative analysis ofamounts of coronary arterial narrowing in cocaine addicts. Am JCardiol 1990;65:303–8.
462. Virmani R, Robinowitz M, Smialek JE, Smyth DF. Cardiovasculareffects of cocaine: an autopsy study of 40 patients. Am Heart J1988;115:1068–76.
463. Rashid J, Eisenberg MJ, Topol EJ. Cocaine-induced aortic dissec-tion. Am Heart J 1996;132:1301–4.
464. Willens HJ, Chakko SC, Kessler KM. Cardiovascular manifestationsof cocaine abuse: a case of recurrent dilated cardiomyopathy. Chest1994;106:594–600.
465. Chokshi SK, Moore R, Pandian NG, Isner JM. Reversible cardio-myopathy associated with cocaine intoxication. Ann Intern Med1989;111:1039–40.
466. Yao SS, Spindola-Franco H, Menegus M, Greenberg M, GoldbergerM, Shirani J. Successful intracoronary thrombolysis in cocaine-associated acute myocardial infarction. Cathet Cardiovasc Diagn1997;42:294–7.
467. Hollander JE. The management of cocaine-associated myocardialischemia. N Engl J Med 1995;333:1267–72.
468. Tokarski GF, Paganussi P, Urbanski R, Carden D, Foreback C,Tomlanovich MC. An evaluation of cocaine-induced chest pain. AnnEmerg Med 1990;19:1088–92.
1055JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
469. Hollander JE, Hoffman RS, Burstein JL, Shih RD, Thode HCJ.Cocaine-associated myocardial infarction. Mortality and complica-tions. Cocaine-Associated Myocardial Infarction Study Group. ArchIntern Med 1995;155:1081–6.
470. Lange RA, Cigarroa RG, Flores ED, et al. Potentiation of cocaine-induced coronary vasoconstriction by beta-adrenergic blockade. AnnIntern Med 1990;112:897–903.
471. Boehrer JD, Moliterno DJ, Willard JE, Hillis LD, Lange RA.Influence of labetalol on cocaine-induced coronary vasoconstrictionin humans. Am J Med 1993;94:608–10.
472. Prinzmetal M, Goldman A, Shubin H, et al. Angina pectoris II. AmHeart J 1959;57:530–43.
473. Parkinson J, Bedford DE. Electrocardiographic changes during briefangina pectoris. Lancet 1931;1:1–20.
474. Maseri A, Pesola A, Marzilli M, et al. Coronary vasospasm in anginapectoris. Lancet 1977;1:713–7.
475. Ozaki Y, Keane D, Serruys PW. Fluctuation of spastic location inpatients with vasospastic angina: a quantitative angiographic study.J Am Coll Cardiol 1995;26:1606–14.
476. Yamagishi M, Miyatake K, Tamai J, Nakatani S, Koyama J, NissenSE. Intravascular ultrasound detection of atherosclerosis at the site offocal vasospasm in angiographically normal or minimally narrowedcoronary segments. J Am Coll Cardiol 1994;23:352–7.
477. Maseri A, Severi S, Nes MD, et al. “Variant” angina: one aspect of acontinuous spectrum of vasospastic myocardial ischemia. Pathogeneticmechanisms, estimated incidence and clinical and coronary arterio-graphic findings in 138 patients. Am J Cardiol 1978;42:1019–35.
478. Walling A, Waters DD, Miller DD, Roy D, Pelletier GB, TherouxP. Long-term prognosis of patients with variant angina. Circulation1987;76:990–7.
479. Rovai D, Bianchi M, Baratto M, et al. Organic coronary stenosis inPrinzmetal’s variant angina. J Cardiol 1997;30:299–305.
480. Previtali M, Ardissino D, Barberis P, Panciroli C, Chimienti M,Salerno JA. Hyperventilation and ergonovine tests in Prinzmetal’svariant angina pectoris in men. Am J Cardiol 1989;63:17–20.
481. Matsuda Y, Ozaki M, Ogawa H, et al. Coronary arteriography andleft ventriculography during spontaneous and exercise-induced STsegment elevation in patients with variant angina. Am Heart J1983;106:509–15.
482. Raizner AE, Chahine RA, Ishimori T, et al. Provocation of coronaryartery spasm by the cold pressor test: hemodynamic, arteriographic andquantitative angiographic observations. Circulation 1980;62:925–32.
483. Ogawa H, Yasue H, Oshima S, Okumura K, Matsuyama K, ObataK. Circadian variation of plasma fibrinopeptide A level in patientswith variant angina. Circulation 1989;80:1617–26.
484. Nobuyoshi M, Abe M, Nosaka H, et al. Statistical analysis of clinicalrisk factors for coronary artery spasm: identification of the mostimportant determinant. Am Heart J 1992;124:32–8.
485. Sugiishi M, Takatsu F. Cigarette smoking is a major risk factor forcoronary spasm. Circulation 1993;87:76–9.
486. Miller DD, Waters DD, Szlachcic J, Theroux P. Clinical character-istics associated with sudden death in patients with variant angina.Circulation 1982;66:588–92.
487. Fukai T, Koyanagi S, Takeshita A. Role of coronary vasospasm in thepathogenesis of myocardial infarction: study in patients with nosignificant coronary stenosis. Am Heart J 1993;126:1305–11.
488. MacAlpin RN. Cardiac arrest and sudden unexpected death invariant angina: complications of coronary spasm that can occur in theabsence of severe organic coronary stenosis. Am Heart J 1993;125:1011–17.
489. Willerson JT, Hillis LD, Winniford M, Buja LM. Speculationregarding mechanisms responsible for acute ischemic heart diseasesyndromes. J Am Coll Cardiol 1986;8:245–50.
490. Kugiyama K, Yasue H, Okumura K, et al. Nitric oxide activity isdeficient in spasm arteries of patients with coronary spastic angina.Circulation 1996;94:266–71.
491. Yasue H, Touyama M, Kato H, Tanaka S, Akiyama F. Prinzmetal’svariant form of angina as a manifestation of alpha-adrenergicreceptor-mediated coronary artery spasm: documentation by coronaryarteriography. Am Heart J 1976;91:148–55.
492. Shephard JT, Katsie ZJ. Endothelium derived vasoactive factors, I:endothelium-dependent relaxation. Hypertension 1991;18(SupplIII):III-76–85.
493. Yasue H, Horio Y, Nakamura N, et al. Induction of coronary arteryspasm by acetylcholine in patients with variant angina: possible role ofthe parasympathetic nervous system in the pathogenesis of coronaryartery spasm. Circulation 1986;74:955–63.
494. Katsumata N, Shimokawa H, Seto M, et al. Enhanced myosin lightchain phosphorylations as a central mechanism for coronary artery spasmin a swine model with interleukin-1b. Circulation 1997;96:4357–63.
495. Mayer S, Hillis LD. Prinzmetal’s variant angina. Clin Cardiol1998;21:243–6.
496. Nakao K, Ohgushi M, Yoshimura M, et al. Hyperventilation as aspecific test for diagnosis of coronary artery spasm. Am J Cardiol1997;80:545–9.
497. Pepine CJ. Ergonovine echocardiography for coronary spasm: factsand wishful thinking. J Am Coll Cardiol 1996;27:1162–3.
498. Opie LH. Calcium channel antagonists in the management ofanginal syndromes: changing concepts in relation to the role ofcoronary vasospasm. Prog Cardiovasc Dis 1996;38:291–314.
499. Chahine RA, Feldman RL, Giles TD, et al. Randomized placebo-controlled trial of amlodipine in vasospastic angina. AmlodipineStudy 160 Group. J Am Coll Cardiol 1993;21:1365–70.
500. Lombardi M, Morales MA, Michelassi C, Moscarelli E, Distante A,L’Abbate A. Efficacy of isosorbide-5-mononitrate versus nifedipinein preventing spontaneous and ergonovine-induced myocardial isch-aemia: a double-blind, placebo-controlled study. Eur Heart J 1993;14:845–51.
501. Yasue H, Takizawa A, Nagao M, et al. Long-term prognosis for patientswith variant angina and influential factors. Circulation 1988;78:1–9.
502. Rosen SD, Uren NG, Kaski JC, Tousoulis D, Davies GJ, CamiciPG. Coronary vasodilator reserve, pain perception, and sex in patientswith syndrome X. Circulation 1994;90:50–60.
503. Kaski JC, Rosano GM, Collins P, Nihoyannopoulos P, Maseri A,Poole-Wilson PA. Cardiac syndrome X: clinical characteristics andleft ventricular function: long-term follow-up study. J Am CollCardiol 1995;25:807–14.
504. Mohri M, Koyanagi M, Egashira K, et al. Angina pectoris caused bycoronary microvascular spasm. Lancet 1998;351:1165–9.
505. Camici PG, Marraccini P, Lorenzoni R, et al. Coronary hemody-namics and myocardial metabolism in patients with syndrome X:response to pacing stress. J Am Coll Cardiol 1991;17:1461–70.
506. Anselmi M, Golia G, Marino P, et al. Comparison of left ventricularfunction and volumes during transesophageal atrial pacing combinedwith two-dimensional echocardiography in patients with syndromeX, atherosclerotic coronary artery disease, and normal subjects. Am JCardiol 1997;80:1261–5.
507. Kemp HG, Kronmal RA, Vlietstra RE, Frye RL. Seven year survivalof patients with normal or near normal coronary arteriograms: aCASS registry study. J Am Coll Cardiol 1986;7:479–83.
508. Opherk D, Schuler G, Wetterauer K, Manthey J, Schwarz F, KublerW. Four-year follow-up study in patients with angina pectoris andnormal coronary arteriograms (“syndrome X”). Circulation 1989;80:1610–6.
509. Cannon RO, Watson RM, Rosing DR, Epstein SE. Efficacy ofcalcium channel blocker therapy for angina pectoris resulting fromsmall-vessel coronary artery disease and abnormal vasodilator reserve.Am J Cardiol 1985;56:242–6.
510. Bugiardini R, Borghi A, Biagetti L, Puddu P. Comparison ofverapamil versus propranolol therapy in syndrome X. Am J Cardiol1989;63:286–90.
511. Maseri A. Ischemic heart disease: a rationale basis for clinical practiceand clinical research. New York, NY: Churchill Livingstone; 1995.
512. Galassi AR, Kaski JC, Pupita G, Vejar M, Crea F, Maseri A. Lackof evidence for alpha-adrenergic receptor-mediated mechanisms inthe genesis of ischemia in syndrome X. Am J Cardiol 1989;64:264–9.
513. Cannon RO, Quyyumi AA, Mincemoyer R, et al. Imipramine inpatients with chest pain despite normal coronary angiograms. N EnglJ Med 1994;330:1411–7.
514. Roque M, Heras M, Roig E, et al. Short-term effects of transdermalestrogen replacement therapy on coronary vascular reactivity inpostmenopausal women with angina pectoris and normal results oncoronary angiograms. J Am Coll Cardiol 1998;31:139–43.
515. Rosano GM, Peters NS, Lefroy D, et al. 17-beta-Estradiol therapylessens angina in postmenopausal women with syndrome X. J AmColl Cardiol 1996;28:1500–5.
1056 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
Subject Index
Page references followed by “t” denote tables; those followed by “f” denote figures
AAbciximab
description of, 1007–1008in diabetes mellitus patient, 1032–1033percutaneous coronary intervention use
balloon angioplasty, 1021description of, 1021stenting procedures, 1023
Ablation procedures. See AtherectomyAcebutolol, 997tActivated partial thromboplastin time, 1004Acute coronary syndrome. See also Non–ST-segment
elevation myocardial infarction; Unstableangina
assessment ofevaluative questions, 976telephone triage approach, 976–978
clinical presentation of, 973cocaine use and, 981definition of, 1040demographic considerations, 981diagnosis of
benefits, 973National Heart Attack Alert Program guidelines,
973, 975tdifferential diagnosis, 974gender predilection, 981high-risk period, 975, 977finitial examination of, 974National Heart Attack Alert Program guidelines for
diagnosing, 973, 975tnomenclature associated with, 973, 974fpossible, 973, 989, 991, 1040probable, 1040prognostic indicators, 979risk stratification
class-based recommendations, 978–979criteria for, 979demographics, 981estimating level of risk, 979history, 981noninvasive stress tests and, 1011rationale for, 980
suspectedalgorithm for evaluating, 990fanginal symptoms, 980–981criteria for evaluating, 978thospital admittance of, 989, 991ischemic discomfort, 980noncardiac causes, 981–982signs and symptoms, 978t, 980
terminology associated with, 973–974in women vs. men, 981
Acute myocardial infarction. See also Myocardial infarc-tion
biochemical markers of, 979definition of, 1040management of, 973–974reperfusion-eligible, 973, 1041unstable angina and, 973
Adenosine diphosphate receptor antagonistsclopidogrel
adverse effects, 1002coronary artery disease use, 1027tdosing of, 1000tefficacy studies, 1002
ticlopidineadverse effects of, 1002dosing of, 1000tefficacy studies of, 1002mechanism of action, 1002
Amlodipine, 997, 998tAngina
characteristics of, 980definition of, 1040–1041Prinzmetal’s. See Variant anginasigns and symptoms of, 980tempo assessments, 982unstable. See Unstable anginavariant. See Variant angina
Angiography. See Coronary angiographyAngioplasty. See Percutaneous transluminal coronary
angioplastyAngiotensin-converting enzyme inhibitors
anti-ischemic uses, 999aspirin and, 1001coronary artery disease use, 1027t
Anticoagulant therapycoumadin, 1007description of, 1003direct thrombin inhibitors, 1003heparin. See Heparinhirudin, 1006long-term, 1007recommendations, 999–1000warfarin, 1007, 1027t
Anti-ischemic therapyalgorithm for, 993fangiotensin-converting enzyme inhibitors, 999b-blockers
coronary artery disease use, 1027tin diabetes mellitus patient, 1032efficacy studies of, 997in elderly patient, 1034mechanism of action, 996physiologic effects of, 996regimens, 996–997selection criteria, 996for syndrome X, 1040types of, 997t
calcium antagonistscoronary artery disease use, 1027tdosing of, 998tefficacy studies of, 998–999indications, 998mechanism of action, 997physiologic effects of, 997side effects of, 997summary overview of, 999for syndrome X, 1040types of, 998tfor variant angina, 1039
general care, 994goals of, 994
morphine sulfate, 996nitrates
administration routes, 995tcoronary artery disease use, 1027tdosing of, 995, 995tduration of effect, 995tefficacy studies, 995–996nitroglycerin, 995, 995toral, 995physiologic effects of, 994–995sildenafil and, 1029for syndrome X, 1040topical, 995
post-discharge use, 1025–1026recommendations, 992–994
Antiplatelet therapyaspirin
angiotensin-converting enzyme inhibitors and,1001
clinical trials of, 1000contraindications, 1001–1002coronary artery disease use, 1027dosing of, 1000tdrug interactions, 1001–1002glycoprotein IIb/IIIa receptor antagonists and,
concomitant therapy using, 1010initiation of, 1000–1001mechanism of action, 1000onset of action, 1000unfractionated heparin and, 1003–1004
clopidogreladverse effects, 1002coronary artery disease use, 1027tdosing of, 1000tefficacy studies, 1002
dosing of, 1000trecommendations, 999–1000ticlopidine
adverse effects of, 1002dosing of, 1000tefficacy studies of, 1002mechanism of action, 1002
Antithrombotic Therapy in Acute CoronarySyndromes (ATACS) trial, 1007
Arteriography, 1039ASA. See AspirinAspirin
angiotensin-converting enzyme inhibitors and, 1001clinical trials of, 1000contraindications, 1001–1002coronary artery disease use, 1027dosing of, 1000tdrug interactions, 1001–1002glycoprotein IIb/IIIa receptor antagonists and,
concomitant therapy using, 1010initiation of, 1000–1001mechanism of action, 1000onset of action, 1000unfractionated heparin and, 1003–1004
Asymptomatic Cardiac Ischemia Pilot (ACIP), 1015Atenolol, 997t
Atherectomyextraction, 1020glycoprotein IIb/IIIa receptor inhibitors use, 1021rotational, 1020
BBalloon angioplasty. See Percutaneous transluminal
coronary angioplastyBepridil, 998tBetaxolol, 997tBiochemical cardiac markers. See Cardiac markersBiomarkers. See Cardiac markersBisoprolol, 997tBivalurudin, 1003b-Blockers
for cocaine-induced coronary spasm, 1037–1038coronary artery disease use, 1027tin diabetes mellitus patient, 1032efficacy studies of, 997in elderly patient, 1034mechanism of action, 996physiologic effects of, 996regimens, 996–997selection criteria, 996for syndrome X, 1040types of, 997t
Blood pressure control, 1029Bypass Angioplasty Revascularization Investigation
(BARI) trial, 1024, 1030, 1032Bypass grafting. See Coronary artery bypass grafting
CCalcium antagonists
coronary artery disease use, 1027tdosing of, 998tefficacy studies of, 998–999indications, 998mechanism of action, 997physiologic effects of, 997side effects of, 997summary overview of, 999for syndrome X, 1040types of, 998tfor variant angina, 1039
Cardiac death. See also Mortalitycauses of, 973clinical features associated with, 980rates of, 975risk assessments, 979t
Cardiac markersbedside testing for, 988comparisons of, 987t, 9986creatine kinase
advantages of, 987tcharacteristics of, 987tdescription of, 984diagnostic uses, 984disadvantages of, 987tMB isoenzyme, 984
definition of, 1041description of, 984mortality risks and, 985fmyoglobin
advantages of, 987tcharacteristics of, 987tdisadvantages of, 987tmyocardial infarction and, 985–986risk stratification using, 985–986
testing for, 988troponins
advantages of, 987tcharacteristics of, 987tdiagnostic sensitivity of, 986
disadvantages of, 987tI, 974, 984–985P, 974, 984–985T, 974, 984–985, 1027
Cardiogenic shock, 983c7E3, 985, 1008, 1021, 1033c7E3 Fab Antiplatelet Therapy in Unstable
Refractory Angina (CAPTURE) trial, 985,1008
Chest painchest pain unit evaluations, 991cocaine-induced. See Cocainerecurrent, 991–992in syndrome X patient, 1040telephone triage considerations, 976–978in variant angina patient, 1038
Chest pain unitscost savings, 991description of, 989discharge from, 991–992efficacy studies of, 989expanded use of, 991function of, 989intermediate-risk patient evaluation, 991patient classification, 991physical location of, 989triage use, 991
Cholesterol-lowering therapy, 1028Chronic obstructive pulmonary disease
b-blockers for, 996description of, 982
CK. See Creatine kinaseClass I
cocaine-related chest pain recommendations, 1036diabetes mellitus recommendations, 1031–1032elderly recommendations, 1034emergency department or outpatient facility
considerations, 978hospital care recommendations
anticoagulant therapy, 999anti-ischemic therapies, 992, 994tantiplatelet therapy, 999discharge instructions, 1026
hospital discharge recommendations, 1026, 1028immediate management guidelines, 988–989invasive treatment strategy, 1014medical regimens
long-term, 1026postdischarge, 1026
noninvasive stress test recommendations, 1010–1011revascularization recommendations, 1019–1020risk factor modifications, 1028risk stratification recommendations, 978–979syndrome X recommendations, 1039telephone triage considerations, 976variant angina recommendations, 1038
Class IIaanti-ischemic therapy recommendations, 993cocaine-related chest pain recommendations, 1036diabetes mellitus recommendations, 1032invasive treatment strategy, 1014noninvasive stress test recommendations, 1011revascularization recommendations, 1020risk stratification recommendations, 979variant angina recommendations, 1038
Class IIbanti-ischemic therapy recommendations, 993revascularization recommendations, 1020risk stratification recommendations, 979syndrome X recommendations, 1039variant angina recommendations, 1038
Class IIIcocaine-related chest pain recommendations, 1036hospital care recommendations
anticoagulant therapy, 999anti-ischemic therapy, 993–994antiplatelet therapy, 999
invasive treatment strategy, 1014revascularization recommendations, 1020risk stratification recommendations, 979syndrome X recommendations, 1039variant angina recommendations, 1038
Clopidogreladverse effects, 1002coronary artery disease use, 1027tdosing of, 1000tefficacy studies, 1002
CLopidrogel ASpirin Stent International CooperativeStudy (CLASSICS), 1002
CLopidrogel in Unstable Angina to Prevent IschemicEvents (CURE) trial, 1002
Clopidrogel versus Aspirin in Patients at Risk ofIschaemic Events (CAPRIE) trial, 1002
Cocaineaccelerated atherosclerosis caused by, 1037acute coronary syndrome and, 981b-blockers and, 1037–1038cardiac physiology effects, 1036–1037chest pain secondary to, 1037, 1037tclassification-based recommendations, 1036coronary artery spasm secondary to, 1037detoxification processes, 1037electrocardiographic evaluations, 1037treatment regimens, 1037–1038user demographics, 1037t
Combination Hemotherapy And Mortality Prevention(CHAMP), 1007
Coronary angiographydeferred, 1014–1015findings, 1013, 1017–1018immediate
characteristics of, 1014–1015indications, 1017for prior CABG patient, 1017for reduced LV systolic function patient, 1017
indications, 1013, 1018, 1027–1028post-discharge indications, 1027–1028preprocedural consultations, 1018purpose of, 1015referral indications, 1011
Coronary Angioplasty versus Bypass RevascularizationInvestigation (CABRI) trial, 1024
Coronary arteriesdynamic obstruction of, 975inflammation of, 975mechanical obstruction of, 975vasospasm of
calcium antagonists for, 1039cocaine-induced
b-blockers and, 1037–1038cardiac physiology effects, 1036–1037chest pain secondary to, 1037, 1037tclassification-based recommendations, 1036coronary artery spasm secondary to, 1037detoxification processes, 1037electrocardiographic evaluations, 1037treatment regimens, 1037–1038user demographics, 1037t
nitroglycerin for, 1039noninvasive tests for, 1039variant anginal cause of. See Variant angina
Coronary arteriography, 1039Coronary artery bypass grafting
cholesterol-reducing therapy after, 1028classification-based recommendations, 1019–1020in diabetes mellitus patient, 1032–1033early
for high-risk patient, 1025
1058 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
indications, 1018efficacy studies of, 1023in elderly patient, 1035–1036hospital discharge, 1025for low-risk patient, 1025medical therapy and, comparisons between, 1023outcome evaluations, 1023–1024percutaneous transluminal coronary angioplasty and,
comparisons between, 1024prevalence of, 1033prior
clinical findings and approach, 1033–1034early coronary angiography indications, 1017electrocardiographic findings, 1033outcomes, 1033pathological findings, 1033revascularization, 1033–1034saphenous vein graft, 1033–1034stenting vs. percutaneous transluminal coronary
angioplasty, 1034studies of, 1024survival rates, 1023in women, 1030
Coronary artery diseasedefinition of, 1041history of, 980ischemia and, 980long-term therapy for, 1027tin older adults, 981risk assessments
description of, 980evaluative approach based on, 989
risk factors, 981telephone triage considerations, 976–978
Coronary Artery Surgery Study (CASS), 1032, 1040Coronary revascularization
algorithm, 1019fcomorbidity that precludes, 1018glycoprotein IIb/IIIa receptor inhibitors
balloon angioplasty, 1021benefits, 1021complications reductions, 1021, 1022tdescription of, 1007–1008evaluative studies, 1021, 1022tmortality reductions, 1021, 1022t
indications, 1018, 1028noninvasive stress testing for, 1016percutaneous coronary interventions
balloon angioplasty, 1021definition of, 1020in diabetes mellitus patient, 1032efficacy evaluations, 1020–1021glycoprotein IIb/IIIa receptor inhibitor use with.
See Coronary revascularization, glycoproteinIIb/IIIa receptor inhibitors
hospital discharge, 1025indications, 1025procedures, 1020rotational atherectomy, 1020selection factors, 1018–1019stenting, 1020in women, 1030
platelet inhibitors. See Coronary revascularization,glycoprotein IIb/IIIa receptor inhibitors
in post-CABG patient, 1033–1034principles of, 1018–1019procedure selection
clinical presentation and, 1018–1019coronary artery bypass grafting. See Coronary
artery bypass graftingdisease severity indicators, 1026tfactors that influence, 1018percutaneous coronary interventions. See
Percutaneous coronary interventions
strategy for, 1019fsurgical. See Coronary artery bypass grafting
Coumadin, 1007Coumadin Aspirin Reinfarction Study (CARS), 1007C-reactive protein, 988Creatine kinase
advantages of, 987tcharacteristics of, 987tdescription of, 984diagnostic uses, 984disadvantages of, 987tMB isoenzyme, 984rotational atherectomy effects, 1020
DDanish Study Group on Verapamil in Myocardial
Infarction (DAVIT), 998–999DANish trial in Acute Myocardial Infarction
(DANAMI), 1015Death. See MortalityDepression, 1027Diabetes mellitus
abciximab use, 1032–1033b-blockers and, 1032classification-based recommendations, 1031–1032coronary artery bypass grafting and, 1032–1033coronary artery disease and, 1032glucose control guidelines, 1029mortality rates, 1032percutaneous coronary interventions and, 1032percutaneous transluminal coronary angioplasty and,
1032summary overview of, 1033
Diagnostic Marker Cooperative Study, 986Diltiazem, 998tDiltiazem Reinfarction Study (DRS), 998Dipyridamole, 1027tDirect thrombin inhibitors
description of, 1003hirudin. See Hirudin
Discharge from hospitalafter coronary artery bypass grafting, 1025after percutaneous coronary interventions, 1025anti-ischemic regimen
follow-up, 1028patient and family instructions regarding, 1025recommendations, 1025–1026
cardiac rehabilitation program, 1025care guidelines
blood pressure control, 1029cholesterol reductions, 1028–1029exercise, 1029risk factor modification, 1028–1029sexual activity, 1029smoking cessation, 1029
dietary modifications, 1028follow-up after
classification-based recommendations, 1026–1027
coronary angiography indications, 1027–1028mortality risk assessments, 1027–1028telephone visits, 1028
goals, 1025medical record, 1029
Duke Treadmill Score, 1030Dynamic obstruction, 975
EECG. See ElectrocardiogramEchocardiography, stress
diagnostic uses of, 1030dobutamine, 1030in women, 1030
Efficacy and Safety of Subcutaneous Enoxaparin inNon-Q wave Coronary Events (ESSENCE),980, 1000, 1004–1006, 1036
Elderlyb-blocker considerations, 1034classification-based recommendations, 1034comorbid conditions, 1034–1035coronary artery disease in, 1034exercise testing considerations, 1034interventions in
coronary artery bypass grafting, 1035–1036overview of, 1036percutaneous coronary, 1035–1036
pharmacologic considerations, 1034summary overview of, 1036TIMI III registry data regarding, 1034–1035,
1035fElectrocardiogram
diagnostic and evaluative usescocaine-related chest pain, 1037post-CABG patient, 1033suspected acute coronary syndrome, 979syndrome X, 1040variant angina, 1038–1039
mortality risk assessments using, 1027risk stratification using, 983–984serial recordings, 984ST-segment findings, 983T-wave findings, 98312-lead, 983–984
Emergency departmentassessments, 978discharge from, 991–992
Emory Angioplasty versus Surgery Trial (EAST),1032
Enoxaparin, 1004–1005Eptifibatide
characteristics of, 1007, 1009efficacy studies of, 1022t, 1023percutaneous coronary intervention use, 1022t, 1023
Erythritol tetranitrate, 995tEsmolol, 997tEvaluation of c7E3 for the Prevention of Ischemic
Complications (EPIC), 1021Evaluation of Platelet IIb/IIIa Inhibitor for
STENTing (EPISTENT) trial, 1021, 1023,1033
Evaluation of PTCA to Improve Long-term Outcomeby C7E3 GPIIb/IIIa receptor blockade(EPILOG), 1021, 1033
Exercise, 1029Exercise testing
description of, 1013in elderly patient, 1034in women, 1030
FFast Revascularization During Instability in Coronary
Artery Disease (FRISC II), 1006, 1016–1017Felodipine, 998tFibrinogen, 988Fibrinopeptide, 988Folate, 1027tFragmin during Instability in Coronary Artery Disease
(FRISC), 1004, 1006FRagmin In unstable Coronary artery disease (FRIC)
study, 1004FRAXiparine in Ischaemic Syndrome (FRAXIS) trial,
1005
GGemfibrozil, 1027tGlobal Use of Strategies to Open Occluded Coronary
1059JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
Arteries-II (GUSTO), 983, 1006, 1017, 1027,1031
Glycoprotein IIb/IIIa receptor inhibitorsabciximab
description of, 1007–1008in diabetes mellitus patient, 1032–1033percutaneous coronary intervention use, 1021
adverse effects, 1010aspirin and, 1010in balloon angioplasty, 1021bleeding risks associated with, 1010description of, 1007in diabetes mellitus patient, 1032–1033eptifibatide
characteristics of, 1007, 1009efficacy studies of, 1022t, 1023percutaneous coronary intervention use, 1022t,
1023heparin and, 1010indications, 985mechanism of action, 1007, 1021monitoring guidelines, 1010mortality rate reductions secondary to, 1008, 1009fin percutaneous coronary interventions
benefits, 1021complications reductions, 1021, 1022tdescription of, 1007–1008evaluative studies, 1021, 1022tmortality reductions, 1021, 1022tpercutaneous transluminal coronary angioplasty,
1021studies of, 1007, 1008t, 1021thienopyridine treatment and, 1002thrombolysis, 1010tirofiban
description of, 1008percutaneous coronary intervention use, 1021–
1023Gruppo Italiano per lo Studio della Sopravvivenza
nell’Infarto-1 (GISSI-1), 1010Gruppo Italiano per lo Studio della Sopravvivenza
nell’infarto Miocardico (GISSI-3), 996
HHeparin
in elderly patient, 1034glycoprotein IIb/IIIa receptor antagonists and,
concomitant therapy using, 1010low-molecular-weight
advantages of, 1005–1006anticoagulant properties of, 1006efficacy studies of, 1004indications, 985mechanism of action, 1003postdischarge administration, 1006unfractionated heparin and, comparisons
between, 1004–1006mechanism of action, 1003thienopyridine treatment and, 1002unfractionated
activated partial thromboplastin time evaluations,1004
aspirin and, comparisons between, 1003–1004dosing of, 1004hirudin and, comparisons between, 1006limitations of, 1004low-molecular-weight heparin and, comparisons
between, 1004–1006mechanism of action, 1003monitoring tests, 1004pharmacokinetics of, 1004studies of, 1003
High-risk patientcomorbidities, 1018coronary angiography indications, 1018coronary artery bypass grafting indications, 1025revascularization procedure for, 1018treatment strategy considerations, 1018
Hirudindosing of, 1006mechanism of action, 1003studies of, 1006unfractionated heparin and, comparisons between,
1006Hirulog. See BivalurudinHMG-CoA reductase inhibitors, 1027tHolland Interuniversity Nifedipine/metoprolol Trial
(HINT), 998Homocysteine, 1029Hormone replacement therapy, 1026, 1027tHospital care
admittanceinitial care after, 992medical stabilization after, 992
anticoagulant therapycoumadin, 1007description of, 1003direct thrombin inhibitors, 1003heparin. See Heparinhirudin, 1006long-term, 1007recommendations, 999–1000warfarin, 1007, 1027t
anti-ischemic therapy. See Anti-ischemic therapyantiplatelet therapy. See Antiplatelet therapyconservative treatment
invasive treatment, 1017objectives of, 1015–1018principles of, 1013–1014rationale for, 1014recommendations, 1014
glycoprotein IIb/IIIa receptor antagonistsabciximab, 1007–1008adverse effects, 1010aspirin and, 1010bleeding risks associated with, 1010description of, 1007eptifibatide, 1007, 1009heparin and, 1010mechanism of action, 1007monitoring guidelines, 1010mortality rate reductions secondary to, 1008,
1009ffor percutaneous intervention-related
complications, 1007–1008studies of, 1007, 1008tthrombolysis, 1010tirofiban, 1008
indications, 992invasive treatment
deferred angiography, 1015efficacy studies for, 1016–1017immediate angiography, 1014–1015objectives of, 1015–1018principles of, 1013–1014rationale for, 1014recommendations, 1014
noninvasive stress testing. See Noninvasive stresstesting
overview of, 992Hospital discharge
after coronary artery bypass grafting, 1025after percutaneous coronary interventions, 1025anti-ischemic regimen
follow-up, 1028patient and family instructions regarding, 1025
recommendations, 1025–1026cardiac rehabilitation program, 1025care guidelines
blood pressure control, 1029cholesterol reductions, 1028–1029exercise, 1029risk factor modification, 1028–1029sexual activity, 1029smoking cessation, 1029
dietary modifications, 1028follow-up after
classification-based recommendations, 1026–1027
coronary angiography indications, 1027–1028mortality risk assessments, 1027–1028telephone visits, 1028
goals, 1025medical record, 1029
IInterleukin-6, 988International Study of Infarct Survival (ISIS-4), 996Interventional cardiology. See StentsIschemic heart disease, 1041Isosorbide dinitrate, 995tIsosorbide mononitrate, 995tIsradipine, 998t
LLabetalol, 997t, 1037–1038Lepirudin. See HirudinLow-molecular-weight heparin
advantages of, 1005–1006anticoagulant properties of, 1006efficacy studies of, 1004indications, 985mechanism of action, 1003postdischarge administration, 1006unfractionated heparin and, comparisons between,
1004–1006Low-risk patient
coronary artery bypass grafting for, 1025medical management of, after hospital discharge,
1025treatment strategy considerations, 1018
MMedicine versus Angiography in Thrombolytic
Exclusion (MATE), 1016Metoprolol, 997tMorphine sulfate, 996Mortality. See also Cardiac death
causes of, 973clinical features associated with, 980in elderly patients, 1035hormone replacement therapy and, 1026rates of, 975risk assessments
characteristics of, 979tdescription of, 982electrocardiogram evaluations, 1027physical examination, 982–983studies of, 1027troponin levels and, 985f, 985t
risk factorsindependent types of, 1027modification of, 1025–1029
Multicenter Diltiazem Postinfarction Trial, 998–999Myocardial infarction
acute. See Acute myocardial infarctioncardiac markers
bedside testing for, 988
1060 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062
comparisons of, 987t, 9986creatine kinase, 984, 987tdescription of, 984myoglobin, 985–986, 987ttroponins, 984–985, 987t
hormone replacement therapy and, 1026non-Q-wave, 983, 1041non-ST-segment elevation. See Non-ST-segment
elevation myocardial infarctionprior
in elderly patients, 1034risks associated with, 982
progression to, 1025recurrent, 980ST-segment elevation
emergency assessment of, 978treatment of, 974
Myocardial ischemiaabciximab use, 1021anti-ischemic therapy for. See Anti-ischemic
therapyassessment of, 980definition of, 1041myoglobin levels and, 985–986nondiagnostic findings, 980–981pathways, 993frisk stratification based on, 980symptoms secondary to, noncardiac causes of
exacerbation of, 981–982Myocardial perfusion
non–ST-segment elevation myocardial infarctionand, 974–975
unstable angina and, 974–975Myoglobin
advantages of, 987tcharacteristics of, 987tdisadvantages of, 987tmyocardial infarction and, 985–986risk stratification using, 985–986
NNadolol, 997tNational Heart Attack Alert Program, 973, 975tNeutropenia, 1002Niacin, 1027tNicardipine, 998tNifedipine
characteristics of, 997, 998tefficacy studies, 998
Nisoldipine, 998tNitrates
administration routes, 995tcoronary artery disease use, 1027tdosing of, 995, 995tduration of effect, 995tefficacy studies, 995–996nitroglycerin. See Nitroglycerinoral, 995physiologic effects of, 994–995sildenafil and, 995, 1029for syndrome X, 1040topical, 995
Nitrendipine, 998tNitroglycerin
for angina, 980for cocaine-induced coronary spasm, 1038for coronary artery spasm, 1039dosing of, 995tduration of effect, 995tintravenous, 995sublingual, 995
Noninvasive stress testingdescription of, 1011
echocardiography, 1012tefficacy studies of, 1013in high-risk patient, 1011indications, 1013mortality prevention secondary to, 1013objectives of, 1011–1012patient counseling, 1013purpose of, 1015radionuclide ventriculography, 1012trecommendations, 1010–1011risk stratification, 1012ttest selection, 1012–1013treadmill test, 1013in women, 1030
Non-ST-segment elevation myocardial infarctioncardiogenic shock and, 983clinical features of, 974clinical presentation of, 975, 976tdefinition of, 973, 1041diagnostic markers of, 974etiology of, 974–975, 975t, 976fhigh-risk patients, 982hospitalizations caused by, 973mortality
causes of, 973rates of, 975risk assessments, 982–983
pathogenesis of, 973, 974–975, 976fphysical examination, 982–983unstable angina and, comparisons between, 974
OOrganization to Assess Strategies for Ischemic
Syndromes (OASIS) program, 1006–1007,1017
PPentaerythritol tetranitrate, 995tPercutaneous coronary interventions
definition of, 1020in diabetes mellitus patient, 1032efficacy evaluations, 1020–1021in elderly patient, 1035–1036glycoprotein IIb/IIIa receptor inhibitors and
balloon angioplasty, 1021benefits, 1021complications reductions, 1021, 1022tdescription of, 1007–1008evaluative studies, 1021, 1022tmortality reductions, 1021, 1022t
hospital discharge, 1025indications, 1018, 1025percutaneous transluminal coronary angioplasty. See
Percutaneous transluminal coronaryangioplasty
procedures, 1020rotational atherectomy, 1020selection factors, 1018–1019stenting, 1020in women, 1030
Percutaneous transluminal coronary angioplastycholesterol-reducing therapy after, 1028coronary artery bypass grafting and, comparisons
between, 1024in diabetes mellitus patient, 1032efficacy studies of, 1021glycoprotein IIb/IIIa receptor inhibitors and
abciximab, 1021description of, 1021
limiting factors, 1021medical therapy and, comparisons between, 1024outcome evaluations, 1021in post-CABG patient, 1034
restenosis rates, 1021survival rates, 1024in women, 1030
Physical examination, 982–983Pindolol, 997tPlatelet Glycoprotein IIb/IIIa in Unstable Angina:
Receptor Suppression Using IntegrilinTherapy (PURSUIT), 980, 983, 1009–1010,1017
Platelet Receptor Inhibition in Ischemic SyndromeManagement in Patients Limited by UnstableSigns and Symptoms (PRISM-PLUS), 1008–1010, 1023, 1033
Platelet Receptor Inhibition in Ischemic SyndromeManagement (PRISM), 1008
Prinzmetal’s angina. See Variant anginaPropranolol, 997t
RRandomized Efficacy Study of Tirofiban for Outcomes
and REstenosis (RESTORE), 1021–1022Research Group in Instability in Coronary ARtery
Disease (RISC) trial, 1003, 1012Research Group in Instability in Coronary Artery
Disease (RITA), 1016Revascularization. See Coronary revascularizationRisk stratification
class-based recommendations, 978–979criteria for, 979demographics, 981electrocardiogram use, 983–984estimating level of risk, 979high-risk criteria, 1012thistory, 981intermediate-risk criteria, 1012tlow-risk criteria, 1012trationale for, 980using noninvasive stress testing
description of, 1011echocardiography, 1012tefficacy studies of, 1013in high-risk patient, 1011indications, 1013mortality prevention secondary to, 1013objectives of, 1011–1012patient counseling, 1013radionuclide ventriculography, 1012trecommendations, 1010–1011risk stratification, 1012ttest selection, 1012–1013treadmill test, 1013
Rotational atherectomy, 1020
SSecondary unstable angina, 975Sexual activity, 1029Sildenafil, 995, 1029Smoking
cessation recommendations, 1029risks associated with, 981
Statins, 1028–1029Stents
abciximab use, 1023, 1025benefits of, 1024–1025description of, 1020in diabetes mellitus patient, 1032glycoprotein IIb/IIIa receptor inhibitors, 1023,
1025indications, 1020in post-CABG patient, 1034restenosis rates, 1021
Stress echocardiographydiagnostic uses of, 1030
1061JACC Vol. 36, No. 3, 2000 Braunwald et al.September 2000:970–1062 ACC/AHA Guidelines for Unstable Angina
dobutamine, 1030in women, 1030
Stress testing. See Noninvasive stress testingST-segment elevation myocardial infarction
emergency assessment of, 978treatment of, 974
Suspected acute coronary syndromealgorithm for evaluating, 990fanginal symptoms, 980–981criteria for evaluating, 978thospital admittance of, 989, 991ischemic discomfort, 980noncardiac causes, 981–982signs and symptoms, 978t, 980
Syndrome Xclassification-based recommendations, 1039clinical features of, 1039–1040definition of, 1039diagnosis of, 1040electrocardiographic findings, 1040gender predilection, 1040prognosis, 1040treatment of, 1040
TThrombolysis in Myocardial Infarction study. See
TIMI IIIThrombotic thrombocytopenia purpura, 1002Thromboxane A2 receptor antagonists, 1002Ticlopidine
adverse effects of, 1002dosing of, 1000tefficacy studies of, 1002mechanism of action, 1002
TIMI IIIcare objectives, 1016description of, 983–984, 1000elderly, 1034–1035heparin studies, 1005women, 1030–1031, 1031f
Timolol, 997tTirofiban
description of, 1008percutaneous coronary intervention use, 1021–1023,
1022tTreadmill test
description of, 1013in women, 1030
Troponins
advantages of, 987tcharacteristics of, 987tdiagnostic sensitivity of, 986disadvantages of, 987tI, 974, 984–985mortality risk assessments, 1027P, 974, 984–985T, 974, 984–985, 1027
UUnfractionated heparin
activated partial thromboplastin time evaluations,1004
aspirin and, comparisons between, 1003–1004dosing of, 1004hirudin and, comparisons between, 1006limitations of, 1004low-molecular-weight heparin and, comparisons
between, 1004–1006mechanism of action, 1003monitoring tests, 1004pharmacokinetics of, 1004studies of, 1003
Unstable anginacharacteristics of, 980clinical features of, 974, 980clinical presentation
atypical, 980typical, 975, 976t
definition of, 973, 1041etiology of, 974–975, 975t, 976fgrading of, 976thigh-risk patients, 982mortality
causes of, 973clinical features associated with, 980rates of, 975risk assessments, 979t, 982–983
non-ST-segment elevation myocardial infarctionand, comparisons between, 974
pathogenesis of, 973, 974–975, 976f, 1018physical examination, 982–983progression to MI, 1025risk stratification
class-based recommendations, 978–979criteria for, 979demographics, 981estimating level of risk, 979history, 981rationale for, 980
secondary, 975stable angina and, 980suspected
CAD history and, 980criteria for evaluating, 978tischemic discomfort, 980signs and symptoms, 978t, 980
tempo assessments, 982
VVariant angina
characteristics of, 1038circadian variation in onset of, 1038classification-based recommendations, 1038clinical presentation of, 1038coronary spasm secondary to, 1038–1039definition of, 1038, 1041diagnosis of, 1038–1039electrocardiographic findings, 1038–1039pathogenesis of, 1038precipitating factors, 1038prognosis, 1039provocative testing methods, 1039survival rates, 1039treatment of, 1039without ST-segment elevation, 1039
Verapamil, 998tVeterans Affairs Non-Q-Wave Infarction Strategies in
Hospital (VANQWISH) trial, 1013, 1015–1018
Viagra. See Sildenafil
WWarfarin, 1007, 1027tWomen
chest discomfort, 1030classification-based recommendations, 1029–1030clinical study data regarding, 1030–1031coronary artery bypass grafting in, 1030coronary artery disease
management of, 1030prevalence of, 1030
hormone replacement therapy, 1026, 1027tpercutaneous transluminal coronary angioplasty,
1030stress testing, 1030TIMI III registry data regarding, 1030–1031,
1031f
1062 Braunwald et al. JACC Vol. 36, No. 3, 2000ACC/AHA Guidelines for Unstable Angina September 2000:970–1062