Embed Size (px)
Citation preview

Abnormal response of motor cortex to photic
stimulation in idiopathic generalized epilepsy*ySergiu Groppa, yHartwig R. Siebner, zChristoph Kurth, *Ulrich Stephani,
and *Michael Siniatchkin
*Clinic for Neuropediatrics, Christian Albrechts University, Kiel, Germany; yClinic for Neurology, Christian
Albrechts University, Kiel, Germany; and zEpilepsy Center, Kork, Germany
SUMMARY
Background: Intermittent photic stimulation
(IPS) shortens the cortical silent period (CSP)
elicited by transcranial magnetic stimulation
(TMS) over the primary motor hand area
(M1HAND). This response is absent in healthy
individuals with a photoparoxysmal response
(PPR). Here we combined TMS of the M1HAND
with IPS to examine whether patients with idio-
pathic generalized epilepsy (IGE) exhibit an
abnormal cortical response pattern to IPS.
Methods: In 13 PPR-positive and 12 PPR-negative
patients with IGE and in 13 PPR-negative healthy
controls, we used focal TMS to the M1HAND to
study how cortical excitability is changed by con-
current IPS at 50 Hz.
Results: IPS at 50 Hz reduced the duration of the
CSP in healthy PPR-negative individuals, whereas
IPS had no effect on the CSP in PPR-positive and
PPR-negative patients with generalized epilepsy.
The failure of IPS to shorten the CSP was indepen-
dent of antiepileptic medication. Single-pulse or
paired-pulse TMS only without concurrent IPS
showed a higher motor threshold in PPR-positive
patients with epilepsy, presumably caused by
antiepileptic medication. No additional differ-
ences in cortical excitability were found among
groups.
Conclusions: Because the CSP is mediated by
intracortical GABAergic mechanisms, our results
indicate that IGEs are associated with an altered
responsiveness of GABAergic inhibitory circuits
in the M1HAND. This electrophysiological trait is
independent of photosensitivity. Excitability
changes at the cortical or thalamic level may
mediate this abnormal cortical response pattern
in patients with IGE.
KEY WORDS: Generalized epilepsy, Motor cor-
tex, Photosensitivity, Photoparoxysmal response,
Photic stimulation, Silent period, Transcranial
magnetic stimulation.
Photosensitivity or photoparoxysmal response (PPR) isdefined as an abnormal electroencephalographic responseof the human brain to visual stimulation. The PPR consistsof spikes or spike-and-wave discharges that are triggeredby intermittent photic stimulation (IPS). A wide range ofexperimental and natural visual stimuli may induce a PPR,including flashing light, patterns of lines, or gratings(Ferlazzo et al., 2005). In patients with certain types ofepilepsy, such as juvenile myoclonic epilepsy or juvenileabsence epilepsy, a PPR can be observed in 15%–20% ofthe patients (Shiraishi et al., 2001). The prevalence of an
abnormal PPR to IPS in a healthy population was 0.35%in 13,658 male applicants for Royal Air Force training and2.4% in 5,893 asymptomatic applicants for training in theDanish Air Force (Trojaborg, 1992; Gregory et al., 1993).
The pathophysiological mechanisms of the PPR and itslink to generalized epilepsies remain to be clarified. Inaddition to an alteration of occipital excitability,functional abnormalities in the motor cortex seem tocontribute to the development and propagation of thePPR. In a baboon model of photosensitive epilepsy, theneuronal origin of the light-induced epileptiform activityhas been located in the superficial layers of the primarymotor cortex (Lloyd et al., 1986; Menini C. 1998).Functional magnetic resonance imaging (fMRI) hasshown a stronger change in the blood oxygen leveldependent (BOLD) signal in the occipital and motorcortex as well as posterior cingulate cortex during IPS in
Accepted May 6, 2008; Early View publication July 8, 2008.Address correspondence to Sergiu Groppa, Department of Neurology,
Christian Albrechts University, Kiel, Schittenhelmstr 10, Germany.E-mail: [email protected]
Wiley Periodicals, Inc.ª 2008 International League Against Epilepsy
Epilepsia, 49(12):2022–2029, 2008doi: 10.1111/j.1528-1167.2008.01709.x
FULL-LENGTH ORIGINAL RESEARCH
2022

PPR-positive patients with epilepsy relative to PPRnegative healthy controls (Chiappa et al., 1999).
Transcranial magnetic stimulation (TMS) provides awell-established means of studying the excitability of theintact primary motor cortex in awake human individuals(Curr� et al., 2002). Using single or paired pulses, TMSoffers an array of electrophysiological measures thatprobe distinct aspects of cortical excitability (Kobayashi& Pascual-Leone, 2003). In a recent study, we used TMSof the primary motor hand area (M1HAND) to examinechanges in the cortical silent period (CSP) during IPS inhealthy subjects with and without PPR (Siniatchkin et al.,2007). The CSP is transcranially evoked by a TMS pulsein the preinnervated muscle. The duration of the CSPreflects the excitability of intracortical GABABergic cir-cuits (Siebner et al., 1998; Werhahn et al., 1999). WhileIPS shortened the CSP in PPR-negative control subjects, ithad no effect on the duration of the CSP in PPR-positiveindividuals. Following upon this work, we combined TMSof the M1HAND and IPS to examine whether patients withidiopathic generalized epilepsies (IGE) show an abnormalresponsiveness of intracortical inhibitory circuits to visualstimulation. We studied patients with and without PPRto clarify whether an abnormal response profile to IPS isspecific to PPR-positive IGE.
Methods
ParticipantsThirty-eight right-handed individuals were recruited in
the period 2004–2007 from the register of the Departmentof Child Neurology. They fulfilled the following inclusioncriteria: patients had to be free of seizures for at least 6months at the time of the study, no metallic implants orelectrical devices, no drug abuse, alcoholism, or preg-nancy, no neurological deficits and other health problems,and no developmental problems or learning disabilities.The study was performed according to the Declarationof Helsinki. All subjects, and in the case of minors, theirparents, gave written informed consent for participation.The study was approved by the Ethical Committee of theMedical Faculty of the University of Kiel.
We investigated three groups of subjects matched forage and gender: 12 patients with IGE without PPR (meanage, 15.6 years; range, 12–19 years; 5 males), 13 patientswith IGE and PPR (mean age, 14.7 years; range, 12–22years; 3 males), and 13 healthy control subjects withoutPPR (mean age, 16.7 years; range, 13–23 years; 3 males).Clinical details are given in Table 1. Eight of the 25patients were treated with sodium valproate. One patientadditionally received lamotrigine.
ElectroencephalographyIn all participants, standard 32-channel electroencepha-
lography (EEG) was recorded twice before entering the
study, including IPS. Prior to the TMS measurements, anadditional EEG measurement with and without IPS wascarried out in concordance with internationally recom-mended guidelines (Epilepsia Commission, 1989). IPSwas performed using a standard procedure in accordancewith published guidelines (Waltz et al., 1992). The elec-troencephalograms were inspected by two experiencedchild neurologists who assessed the presence and the typeof the PPR (Waltz et al., 1992). All subjects with PPR hadgeneralized PPR with propagation to anterior brainregions (Waltz et al., 1992).
Transcranial magnetic stimulationTMS was delivered to the left M1HAND through a figure-
of-eight-shaped coil (70 mm internal diameter) connectedto two Magstim-200 HP magnetic stimulators via a BiStimmodule (Magstim Company, Dyfed, Wales, UK). The pro-cedures used for TMS were identical to those described inour previous study (Siniatchkin et al., 2007). Motor evokedpotentials (MEPs) were recorded from the right APB mus-cle with Ag/AgCl electrodes using a tendon-belly arrange-ment. The electromyographic (EMG) signal was amplified
Table 1. Clinical characteristics of the
patients
Patient PPR Syndromic
number Age Sex Group grade Medication diagnosis
1 16 F EP 4 none GTCA
2 13 F EP 4 VLP JAE
3 12 M EP 3 none JAE
4 12 F EP 4 none JAE
5 14 M EP 4 VLP GTCA
6 16 F EP 4 none JAE
7 12 F EP 2 VLP JAE
8 22 F EP 2 VLP JAE
9 16 F EP 2,3 none GTCA
10 13 M EP 4 none JAE
11 12 F EP 2 none JAE
12 13 F EP 4 none JAE
13 20 F EP 4 none GTCA
14 12 F E none none JAE
15 19 F E none none JAE
16 14 F E none none JAE
17 13 M E none none JAE
18 17 F E none VLP GTCA
19 16 M E none none JAE
20 13 M E none VLP JAE
21 16 F E none VLP, LMG JME
22 17 F E none none JAE
23 14 M E none none JAE
24 19 M E none VLP JAE
25 18 F E none none JAE
VLP, valproic acid; LMG, lamotrigine; E, patients with gener-
alized epilepsy and no photosensitivity; EP, patients with gener-
alized epilepsy and photosensitivity; JAE, juvenile absence
epilepsy; GTCA, IGE with tonic–clonic seizures alone; JME,
juvenile myoclonic epilepsy.
2023
Motor Cortex Excitability in IGE
Epilepsia, 49(12):2022–2029, 2008doi: 10.1111/j.1528-1167.2008.01709.x

using Neuropack-2 device (Nikon Kohden EMG Device;Nikon Kohden, Tokyo, Japan), band pass filtered (2–2000Hz), and stored at a sampling rate of 5 kHz using a CED‘‘Micro-1622’’ A/D-converter and Signal 3.0 software(CED Co., Cambridge, U.K.). Auditory feedback of therecorded EMG activity was provided to help subjects tomaintain full relaxation (at rest) or produce a constant forcelevel (during tonic contraction). The mean interval betweentwo consecutive trials was 5 s, ranging from 4 to 6 s.
Corticomotor excitability was measured at baselinebefore IPS to better characterize motor cortex excitabilityat rest and to exclude substantial differences in the excit-ability profile among groups. We first determined the rest-ing motor threshold (RMT), which was defined as theminimum stimulus intensity at which the TMS pulseinduced at least five MEPs in 10 consecutive trials(Rossini et al., 1994). We applied single-pulse TMS at110%, 130%, and 150% of individual RMT to character-ize the stimulus-response relationship in the completelyrelaxed abductor pollicis brevis (APB) muscle. Werecorded blocks of 15 consecutive trials at each stimulusintensity. The mean MEP amplitude was calculated ateach stimulus intensity for each subject.
A second set of TMS measurements was then per-formed while participants performed a moderate toniccontraction of the APB muscle at 20% of maximum forcelevel. Blocks of 15 consecutive trials were recorded at astimulus intensity of 110%, 130%, and 150% of individualRMT. The duration of the CSP was measured in individualtrials and defined as the period from the first turning pointof the MEP to the resumption of any level of tonic EMGactivity (Orth & Rothwell, 2004). CSP measurementswere performed manually by an experienced neurophysi-ologist who was blinded to the different groups. The meanCSP duration was calculated at each stimulus intensity.
A third set of measurements involved paired-pulseTMS to measure short-latency intracortical inhibition(SICI) and intracortical facilitation (ICF) at rest. Using theconditioning-test paradigm introduced by Kujirai andcoworkers (Kujirai et al., 1993), two monophasic mag-netic stimuli were given through the same stimulating coilover the M1HAND, and the effect of the first conditioningstimulus on the second test stimulus was investigated. Theintensity of the first and second stimulus was adjusted to80% and 120% of RMT, respectively. The interstimulusinterval (ISI) between the two stimuli was set at 2 ms toprobe SICI, while the magnitude of ICF was examined atan ISI of 15 ms. Fifteen trials were recorded at each ISIand randomly intermingled with 15 trials in which uncon-ditioned MEPs were elicited by the test stimulus alone.Mean MEP amplitude was calculated for each stimulationcondition. The magnitude of SICI at an ISI of 2 ms andICF at an ISI of 15 was expressed as ratio between themean amplitudes of the conditioned and unconditionedMEP.
After baseline measurements without IPS, we measuredthe duration of the CSP at 110%, 130%, and 150% of theRMT as well as SICI and ICF, while participants receivedphotic stimulation at a repetition rate of 50 Hz. Weassessed only those excitability measures during IPS thatspecifically probed intracortical excitability of the pri-mary motor cortex (i.e., the CSP, SICI, and ICF). Theinput-output curve and motor threshold were not mea-sured, because both measures are influenced by excitabil-ity changes at the cortical and spinal level. IPS started5 s before the first magnetic stimulus was given and wascontinued until the TMS measurements were completed.During IPS, each measure was obtained in blocks. Thesequence of measurements was pseudorandomly variedacross subjects to avoid order effect.
In a previous study on healthy individuals with and with-out PPR (Siniatchkin et al., 2007), we had applied TMSduring IPS at 18 and 50 Hz. IPS at 18 Hz is more efficientto provoke a PPR than 50 Hz. Therefore, we only appliedIPS at a repetition rate of 50 Hz to minimize the risk toinduce a seizure with IPS. The purpose of this experimentwas to modify the duration of the CSP rather than to effec-tively induce a PPR. Since our previous study had shownthat IPS at 18 or 50 Hz was equally effective in shorteningthe CSP, we only applied IPS at 50 Hz and kept the totalperiod of IPS as short as possible. The same equipment wasused for IPS during TMS as for routine evaluation of thePPR (see above). The light in the room was half dimmedand subjects closed their eyes during IPS.
Data analysisBetween-group differences in RMT, SICI, and ICF
were determined with one-way analysis of variance(ANOVA) and post hoc Bonferroni tests (version 10.0;SPSS Inc., Chicago, IL, U.S.A.). Mean amplitudes of theunconditioned MEPs at rest and mean duration of the CSPwere analyzed using two-factorial ANOVAs with thebetween-subjects factor Group (3 levels: PPR-positivepatients, PPR-negative patients, PPR-negative healthycontrols) and the within-subject factor TMS intensity(3 levels: 110%, 130%, and 150% of RMT). In order toinvestigate the effect of IPS on the duration of the CSP,the ANOVA model included Visual stimulation as addi-tional within-subject factor (2 levels: no IPS and IPS at 50Hz). The effects of IPS on SICI and ICF were evaluatedusing ANOVA with the factors Group and Visual stimula-tion. Conditional of a significant effect of Group, separateANOVAs with the factors TMS intensity and Visual stim-ulation were carried out to characterize changes in theresponse to IPS in each group. For post hoc comparisons,a Bonferroni a adjustment was applied, and the correctedsignificance level was consi-dered at p < 0.05.
To estimate the influence of antiepileptic drugs on ourresults, we computed an additional ANOVA that classi-fied patients according to their status of medication.
2024
S. Groppa et al.
Epilepsia, 49(12):2022–2029, 2008doi: 10.1111/j.1528-1167.2008.01709.x

Results
Apart from one patient with PPR who felt dizzy duringIPS, participants noticed no adverse effects during andafter the experimental procedures. In the patient whodeveloped dizziness during IPS, we immediately stoppedthe experiment, and dizziness disappeared spontaneously.This patient was excluded from the data analysis. Inanother patient, TMS at 150% of RMT was not possiblebecause of a high RMT. TMS evoked no clinically appar-ent seizures in any of the participants.
Measurements of intracortical motor cortexexcitability during photic stimulation
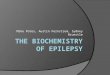
The CSP increased with the TMS intensity of stimula-tion [F (2, 62)¼ 146.06; p < 0.001). The ANOVA showedno interaction between the factors Group and TMS inten-sity (p > 0.3), indicating that the prolongation of the CSPwith increasing stimulus intensity was consistently presentin patients and controls. Moreover, there was a significantinteraction between Visual stimulation and Group [F (2,31)¼ 5.42; p¼ 0.010]. These results indicate that IPS hada differential effect on the duration of the CSP in the threegroups. Indeed, the intermittent IPS initiated a shorteningof the CSP in healthy controls, but failed to modifythe duration of the CSP in patients with or without PPR(Fig. 2). ANOVAs, which were calculated for each groupseparately, demonstrated that only healthy PPR-negativecontrol subjects showed a main effect of Visual stimula-tion [F (1, 12) ¼ 14.97; p ¼ 0.002], while no main effectwas found in patients with and without PPR (p > 0.3). Thetests showed also no interaction between Visual stimula-tion and TMS intensity for any of the three groups.
The ANOVAs that were calculated for the ICF or SICIas dependent variables disclosed no main effects of Visualstimulation and Group and no interaction between Groupand Visual stimulation, showing that IPS had no modula-tory effects on the magnitude of ICF or SICI in any of thethree groups (Table 3).
Measurements of cortical and corticospinal excitabilitybefore photic stimulation
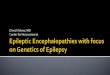
For baseline measurements prior to IPS, ANOVArevealed a difference in RMT among the three groups [F (2,35) ¼ 6.32; p ¼ 0.005]. Post hoc pairwise comparisonsshowed that the main effect was caused by a higher RMT inPPR-positive patients relative to PPR-negative healthy con-trols (p ¼ 0.005) (Fig. 1). There was no significant differ-ence in RMT between PPR-positive and PPR-negativepatients (p ¼ 0.08). Mean MEP amplitudes at rest and theduration of the CSP were comparable between groups(Table 2). MEP amplitudes [F (2, 68) ¼ 69.05; p < 0.001]and the duration of the CSP [F (2, 66) ¼ 118.2; p < 0.001]increased with stimulus intensity. There was no interactionbetween the factors TMS Intensity and Group, showing thatthe effect of stimulus intensity on MEP amplitude and CSPduration was similar among the groups. The strength ofSICI or ICF was also comparable between groups without asignificant main effect of Group in the ANOVA.
Effect of medication on TMS measurementsThe ANOVA, calculated for the three groups controls,
epilepsy patients with and without medication showed asignificant difference among the groups according to theRMT [F (2, 35) ¼ 3.84; p ¼ 0.03]. Post hoc tests showedthat the main effect was caused by different RMTsbetween healthy and epilepsy patients on medication.
Figure 1.
(A) Mean RMT of 12 healthy controls, 13 patients with
photo-sensitivity, and 12 patients without a generalized
photoparoxysmal response (PPR). Mean RMT was
increased in patients with PPR relative to PPR-negative
controls (p ¼ 0.005). (B) Mean RMT of 12 healthy
controls, 17 unmedicated patients, and 8 medicated
patients. Mean RMT was significantly increased in
treated patients in comparison to healthy controls (p¼0.03). The error bar equals one-fold SD.
Epilepsia ILAE
2025
Motor Cortex Excitability in IGE
Epilepsia, 49(12):2022–2029, 2008doi: 10.1111/j.1528-1167.2008.01709.x

The threshold intensity for TMS in the untreated patients(48.82 € 8.45) was higher but not at a significant level(p ¼ 0.16) than in controls (42.3 € 8.4), while the thresh-old intensity in the treated patients (52.75 € 10.35) wassignificantly higher than that in healthy controls (p ¼0.038). There were no differences in MEP amplitude,duration of the CSP, or paired-pulse excitability amongthe three groups. During photic stimulation, only the
group of control subjects showed a shortening of the CSP.Both patients groups demonstrated no change in CSPduration regardless of medication (Fig. 3).
Discussion
We found that patients with generalized epilepsy lackedthe normal changeability of the cortical silent period during
Figure 2.
Mean duration (±SD) of the CSP
elicited with single-pulse TMS
over the left primary motor
hand area at 110%, 130%, and
150% of individual RMT. The
open columns give the mean
CSP without photic stimu-lation.
The filled columns represent the
mean CSP duration during
photic stimulation. (A) Healthy
PPR-negative controls. (B) PPR-
positive patients with IGE. (C)
PPR-negative patients with IGE.
Epilepsia ILAE
Table 2. Mean group values (±SD) of RMT and the amplitudes of MEPs elicited in the relaxed first
dorsal interosseus muscle at 110%, 130%, or 150% above individual RMT
MEP amplitude at MEP amplitude at MEP amplitude at
RMT (%) 110% SI (mV) 130% SI (mV) 150% SI (mV)
Healthy controls without PPR 42.3 ± 8.4 0.17 ± 0.07 0.75 ± 0.37 1.51 ± 0.94
IGE patients without PPR 46.1 ± 7.4 0.28 ± 0.15 0.89 ± 0.73 1.81 ± 1.22
IGE patients with PPR 53.8 ± 9.15 0.23 ± 0.14 1.01 ± 0.88 2.14 ± 1.2
PPR, photoparoxysmal response; IGE, idiopathic generalized epilepsy; SI, stimulus intensity.
2026
S. Groppa et al.
Epilepsia, 49(12):2022–2029, 2008doi: 10.1111/j.1528-1167.2008.01709.x

IPS. Confirming previous studies (Entezari-Taher & Dean,2000), healthy controls without a PPR showed a shorteningof the CSP during IPS. In contrast, IPS failed to shorten theCSP in PPR-positive and PPR-negative patients with gener-alized epilepsy. The duration of the CSP reflects the excit-ability of intracortical GABAergic circuits, presumablymediated by GABAB receptors (Ziemann et al., 1996; Sieb-ner et al., 1998). In PPR-negative healthy individuals, photicstimulation attenuates the excitability of GABAergic inhibi-tory circuits in the motor cortex as indexed by a shorter dura-tion of the CSP. Photic stimulation failed to reduce the CSPin IGE patients, indicating that the excitability level of corti-cal circuits mediating long-lasting inhibition is maintainedthroughout the period of photic stimulation. Critically, thisabnormal response pattern was present in both, treated and
untreated patients, indicating that antiepileptic medicationdid not account for the attenuated suppression of the CSPduring IPS.
In our recent study, the duration of the CSP remainedunchanged during IPS in asymptomatic individuals inwhom EEG had shown a PPR with propagation (Siniatch-kin et al., 2007). Here we show that IPS also failed toshorten the CSP in PPR-positive and PPR-negativeindividuals with generalized epilepsy and PPR.
Together, these studies demonstrate that healthy indi-viduals with PPR but without IGE, as well as patients withIGE but without PPR, lack a normal response of the CSPto IPS. Hence, the presence of PPR or IGE alone is suffi-cient to block the normal response pattern of inhibitorycircuits in the motor cortex. PPR and IGE are differententities, yet they share a common feature. Both conditionsshow an abnormal tendency to develop hypersynchro-nized neuronal activity throughout the brain. The failureto shorten the CSP with IPS in both conditions indicatesan altered control of cortical excitability by sensory(visual) input that may be linked to the abnormal tendencytowards hypersynchronization.
We can only speculate whether the failure of IPS toreduce the CSP duration bears some pathophysiologicalsignificance. It is unlikely that the failure of IPS toshape intracortical inhibition constitutes a pathogenicfactor leading to IGE. If this were the case, this corticalresponse pattern should not be present in healthyindividuals with PPR. Alternatively, it may represent aprotective mechanism to counteract an excessiveincrease in cortical excitability during IPS. For instance,a persistence of intracortical inhibition during IPS maycounteract an excessive build-up of excitatory neuronalactivity in the cortex. The fact that the failure of IPS toshorten the CSP was equally present in healthyindividuals with generalized PPR does not exclude acompensatory mechanism. It just shows that compensa-tion may not always be sufficiently effective to preventthe occurrence of seizures. However, we cannot excludethe possibility that the failure to reduce the CSP withIPS is just a nonspecific electrophysiological trait with-out a causal link to network synchronization.
Table 3. Mean group values (±SD) of SICI at an ISI of 2 ms and ICF at an ISI of 15 ms
SICI at an ISI of 2 ms ICF at an ISI of 15 ms Unconditioned MEP (mV)
Healthy controls without PPR
without IPS 0.45 ± 0.30 1.45 ± 0.50 0.91 ± 0.71
during IPS 0.42 ± 0.19 1.49 ± 0.58 0.81 ± 0.47
IGE patients without PPR
without IPS 0.50 ± 0.19 1.44 ± 0.41 0.92 ± 0.66
during IPS 0.54 ± 0.28 1.54 ± 0.32 0.94 ± 0.84
IGE patients with PPR
without IPS 0.52 ± 0.35 1.37 ± 0.47 0.92 ± 0.68
during IPS 0.55 ± 0.35 1.28 ± 0.43 0.95 ± 0.67
PPR, photoparoxysmal response; IGE, idiopathic generalized epilepsy.
Figure 3.
Mean duration (±SD) of the CSP elicited with single-
pulse TMS over the left primary motor hand area at
110%, 130%, and 150% of individual RMT. The open
columns give the mean CSP without photic stimulation.
The filled columns represent the mean CSP duration
during photic stimulation. The right part of the panel
gives the mean data of the 17 patients who were free of
medication. The left part of the panel shows the mean
data of the eight patients who were on medication at
the time of the study.
Epilepsia ILAE
2027
Motor Cortex Excitability in IGE
Epilepsia, 49(12):2022–2029, 2008doi: 10.1111/j.1528-1167.2008.01709.x

Because we did not record EEG during our experiment,we have no information regarding which of the participantsdeveloped a PPR during the CSP measurements. Therefore,the question of whether or how the occurrence of PPRacutely changes the CSP modulation during IPS remains tobe addressed in future studies that combine TMS and EEG.
In the present study, the duration of the CSP was normalin IGE patients when no visual stimulation was applied.Photic stimulation was necessary to disclose an abnormalchangeability of excitability in the cortical circuits medi-ating the CSP. Previous TMS studies of the duration of theCSP without simultaneous photic stimulation reportedvariable results. While some studies showed a prolonga-tion of the CSP in drug-naive patients with generalizedepilepsy (Macdonell et al., 2001; Manganotti et al., 2001),other studies found a normal duration of the CSP inpatients with generalized seizures (Delvaux et al., 2001).A recent study examined the CSP in 35 drug-naivepatients with IGE, using three different stimulus intensi-ties (Badawy et al., 2007). Confirming our results, nochange in CSP duration was evident at any of the threeintensities of stimulation relative to healthy controls. Dif-ferences in the patient groups studied may account for theinconsistencies across studies (Ertas et al., 2000).
In PPR-positive epileptic patients, the RMT was higherthan in healthy PPR-negative individuals. Post hoc analy-sis revealed that only patients who were on antiepilepticmedication showed an increase in RMT. Therefore, weattribute the increase in RMT to antiepileptic medicationrather than to PPR itself. This finding is in accordancewith previous studies showing that treatment with valpro-ate consistently increases the RMT, presumably by block-ing sodium and calcium channels (Reutens et al., 1993;Nezu et al., 1997). Of note, this difference in RMT amonggroups did not determine the cortical response of thecircuits mediating the CSP to photic stimulation.
Other measures of cortical excitability such as theunconditioned MEP amplitude and paired-pulse excitabil-ity (i.e., SICI at 2 ms and ICF at 15 ms) showed no differ-ences among groups when measured during IPS orwithout photic stimulation. In the present study, assess-ment of SICI and ICF was limited as we only used a singleISI and stimulus intensity. It has been shown in healthysubjects that the relative amount of SICI and ICF variesdepending on the ISI between the conditioning and teststimulus and the intensity of the conditioning pulse (Ilicet al., 2002). A more extensive exploration of paired-pulseexcitability using different ISIs and stimulus intensitiesmight have revealed subtle changes in SICI during IPS. Itshould also be noted that previous studies of SICI inpatients with epilepsy reported inconsistent results(Tassinari et al., 2003; Valentin et al., 2008). Someauthors found a reduction in ICI and ICF in patients withIGE (Reutens et al., 1993; Nezu et al., 1997; Macdonellet al., 2001; Manganotti et al., 2001), yet a study on 18
untreated IGE patients failed to show changes in SICI andICF (Delvaux et al., 2001). Elapsed time from last seizure,used medication as well as the clinical heterogeneity ofinvestigated groups may explain these discrepancies.
In summary, we found that IGE is associated with anabnormal sensory-motor interaction between photic inputand the excitability of intracortical circuits in the M1HAND
that generate the CSP. This abnormality was independentof medication and occurred in IGE patients with and with-out photosensitivity. The failure to shorten the duration ofthe CSP with IPS was associated with a ‘‘normal’’ restinglevel of cortical excitability of the circuits mediating theCSP. This interpretation is corroborated by our previousstudy (Sinatchkin et al., 2007). In that study, there were nodifferences in RMT between PPR-positive and PPR-nega-tive healthy subjects, yet only PPR-negative, and notPPR-positive individuals, showed a reduction in CSP.Obviously, the sensitivity of TMS in detecting abnormalpatterns of motor-cortical excitability in humans criticallydepends on the functional state of the stimulated neuronalcircuits.
Acknowledgments
The authors thank the patients and their families for the time and effortthey dedicated to this research. The research of S.G. was supported byFriedrich-Ebert Foundation, Bonn, Germany.
Conflict of interest: We confirm that we have read the Journal’s positionon issues involved in ethical publication and affirm that this report is con-sistent with those guidelines. The authors have no conflicts of interest todeclare.
References
Badawy RAB, Curatolo JM, Newton M, Berkovic SF, Macdonell RAL.(2007) Changes in cortical excitability differentiate generalized andfocal epilepsy. Ann Neurol 61:324–331.
Chiappa KH, Hill RA, Huang-Hellinger F, Jenkins BG. (1999) Photosen-sitive epilepsy studied by functional magnetic resonance imaging andmagnetic resonance spectroscopy. Epilepsia 40(Suppl 4):3–7.
Curr� A, Modugno N, Inghilleri M, Manfredi M, Hallett M, Berardelli A.(2002) Transcranial magnetic stimulation techniques in clinicalinvestigation. Neurology 59:1851–1859.
Delvaux V, Alagona G, Gerard P, De Pasqua V, Delwaide PJ, Maertensde Noordhout A. (2001) Reduced excitability of the motor cortex inuntreated patients with de novo idiopathic ‘‘grand mal’’ seizures.J Neurol Neurosurg Psychiatry 71:772–776.
Entezari-Taher M, Dean AC. (2000) Alteration of motor cortex excitabil-ity in response to intermittent photic stimulation. Clin Neurophysiol111:1809–1812.
Epilepsia Commission on Classification and Terminology of the Interna-tional League Against Epilepsy. (1989) Proposal for revised classifi-cation of epilepsies and epileptic syndromes. Commission onClassification and Terminology of the International League AgainstEpilepsy. Epilepsia 30:389–399.
Ertas NK, Gul G, Altunhalka A, Kirbas D. (2000) Cortical silent periodfollowing transcranial magnetic stimulation in epileptic patients. Epi-leptic Disord 2:137–140.
Ferlazzo E, Zifkin BG, Andermann E, Andermann F. (2005) Cortical triggersin generalized reflex seizures and epilepsies. Brain 128:700–710.
Gregory RP, Oates T, Merry RT. (1993) Electroencephalogram epilepti-form abnormalities in candidates for aircrew training. Electroencep-halogr Clin Neurophysiol 86:75–77.
2028
S. Groppa et al.
Epilepsia, 49(12):2022–2029, 2008doi: 10.1111/j.1528-1167.2008.01709.x

Ilic TV, Meintzschel F, Cleff U, Ruge D, Kessler KR, Ziemann U. (2002)Short-interval paired-pulse inhibition and facilitation of human motorcortex: the dimension of stimulus intensity. J Physiol 545:153–167.
Kobayashi M, Pascual-Leone A. (2003) Transcranial magnetic stimula-tion in neurology. Lancet Neurol 2:145–156.
Kujirai T, Caramia MD, Rothwell JC, Day BL, Thompson PD, Ferbert A,Wroe S, Asselman P, Marsden CD. (1993) Corticocortical inhibitionin human motor cortex. J Physiol 471:501–519.
Lloyd KG, Scatton B, Voltz C, Bryere P, Valin A, Naquet R. (1986) Cere-brospinal fluid amino acid and monoamine metabolite levels of Papiopapio: correlation with photosensitivity. Brain Res 363:390–394.
Macdonell RA, King MA, Newton MR, Curatolo JM, Reutens DC,Berkovic SF. (2001) Prolonged cortical silent period after transcra-nial magnetic stimulation in generalized epilepsy. Neurology57:706–708.
Manganotti P, Tamburin S, Zanette G, Fiaschi A. (2001) Hyperexcitablecortical responses in progressive myoclonic epilepsy: a TMS study.Neurology 57:1793–1799.
Menini CS-BC. (1998) The photosensitive epilepsy of the baboon. In B.G. Zifkin (ed) Reflex epilepsies and reflex seizures: advances in neu-rology. vol. 75. Lippincott-Raven Press, Philadelphia, pp. 286–297.
Nezu A, Kimura S, Uehara S, Kobayashi T, Tanaka M, Saito K. (1997)Magnetic stimulation of motor cortex in children: maturity of corti-cospinal pathway and problem of clinical application. Brain Dev19:176–180.
Orth M, Rothwell JC. (2004) The cortical silent period: intrinsic variabil-ity and relation to the waveform of the transcranial magnetic stimula-tion pulse. Clin Neurophysiol 115:1076–1082.
Reutens DC, Berkovic SF, Macdonell RA, Bladin PF. (1993) Magneticstimulation of the brain in generalized epilepsy: reversal of corticalhyperexcitability by anticonvulsants. Ann Neurol 34:351–355.
Rossini PM, Barker AT, Berardelli A, Caramia MD, Caruso G, CraccoRQ, Dimitrijevic MR, Hallett M, Katayama Y, L�cking CH et al.
(1994) Non-invasive electrical and magnetic stimulation of the brain,spinal cord and roots: basic principles and procedures for routine clin-ical application. Report of an IFCN committee. ElectroencephalogrClin Neurophysiol 91:79–92.
Shiraishi H, Fujiwara T, Inoue Y, Yagi K. (2001) Photosensitivity in rela-tion to epileptic syndromes: asurvey from an epilepsy center in Japan.Epilepsia 42:393–397.
Siebner HR, Dressnandt J, Auer C, Conrad B. (1998) Continuous intra-thecal baclofen infusions induced a marked increase of the transcra-nially evoked silent period in a patient with generalized dystonia.Muscle Nerve 21:1209–1212.
Siniatchkin M, Groppa S, Jerosch B, Muhle H, Kurth C, Shepherd AJ,Siebner H, Stephani U. (2007) Spreading photoparoxysmal EEGresponse is associated with an abnormal cortical excitability pattern.Brain 130:78–87.
Tassinari CA, Cincotta M, Zaccara G, Michelucci R. (2003) Trans-cranial magnetic stimulation and epilepsy. Clin Neurophysiol114:777–798.
Trojaborg W. (1992) EEG abnormalities in 5,893 jet pilot applicants reg-istered in a 20-year period. Clin Electroencephalogr 23:72–78.
Valentin A, Arunachalam R, Mesquita-Rodrigues A, Garcia Seoane JJ,Richardson MP, Mills KR, Alarcon G. (2008) Late EEG responsestriggered by transcranial magnetic stimulation (TMS) in the evalua-tion of focal epilepsy. Epilepsia 49:470–480.
Waltz S, Christen HJ, Doose H. (1992) The different patterns of thephotoparoxysmal response—a genetic study. ElectroencephalogrClin Neurophysiol 83:138–145.
Werhahn KJ, Kunesch E, Noachtar S, Benecke R, Classen J. (1999) Dif-ferential effects on motorcortical inhibition induced by blockade ofGABA uptake in humans. J Physiol 517(Pt 2):591–597.
Ziemann U, Lonnecker S, Steinhoff BJ, Paulus W. (1996) The effect oflorazepam on the motor cortical excitability in man. Exp Brain Res109:127–135.
2029
Motor Cortex Excitability in IGE
Epilepsia, 49(12):2022–2029, 2008doi: 10.1111/j.1528-1167.2008.01709.x