Embed Size (px)
Citation preview
CASE REPORTHip Pelvis 28(3): 178-181, 2016http://dx.doi.org/10.5371/hp.2016.28.3.178
Copyright ⓒ 2016 by Korean Hip Society178
Print ISSN 2287-3260Online ISSN 2287-3279
The tensor fascia latae and gluteus medius and minimusare known as primary hip abductor muscles. Mainfunctions of these muscles are hip abduction andbalancing the weight of the body and the non-weight-bearing leg during walking1). Abductor deficiency ordysfunction is clinically uncommon. Spontaneousrupture at the greater trochanter is caused by repeatedtrauma such as runners or complication of trochantericbursitis2,3). Other well-known causes are failure of repairof abductor during the total hip replacement and injuryof superior gluteal nerve which innervates hip abductors4).
Regardless of causes, abductor dysfunction may causelimping, positive Trendelenburg sign and pain in nativehip joint. In case of artificial joint, additional importantissue is a joint stability. It may lead to joint instability,recurrent dislocation, finally unsatisfactory results5).
Several treatments were introduced in the literature6-9).In this report, we’d like to introduce easy and reproducibleoperative technique with the use of anterior fiber ofgluteus maximus during the total hip arthroplastyaccompanied with primary abductor deficiency.
CASE REPORT
Sixty four-year-old female presented to our hospital witha history of left hip pain with limping gait. Her hip pain andlimping gait were started about 2 years ago and 5 monthsago, respectively. She had no special trauma history anddiscomfort on her hip joint until two years ago. She had noprior operation history on left hip joint. Body mass indexwas 23.8 kg/m2 and bone mineral density was –0.59.
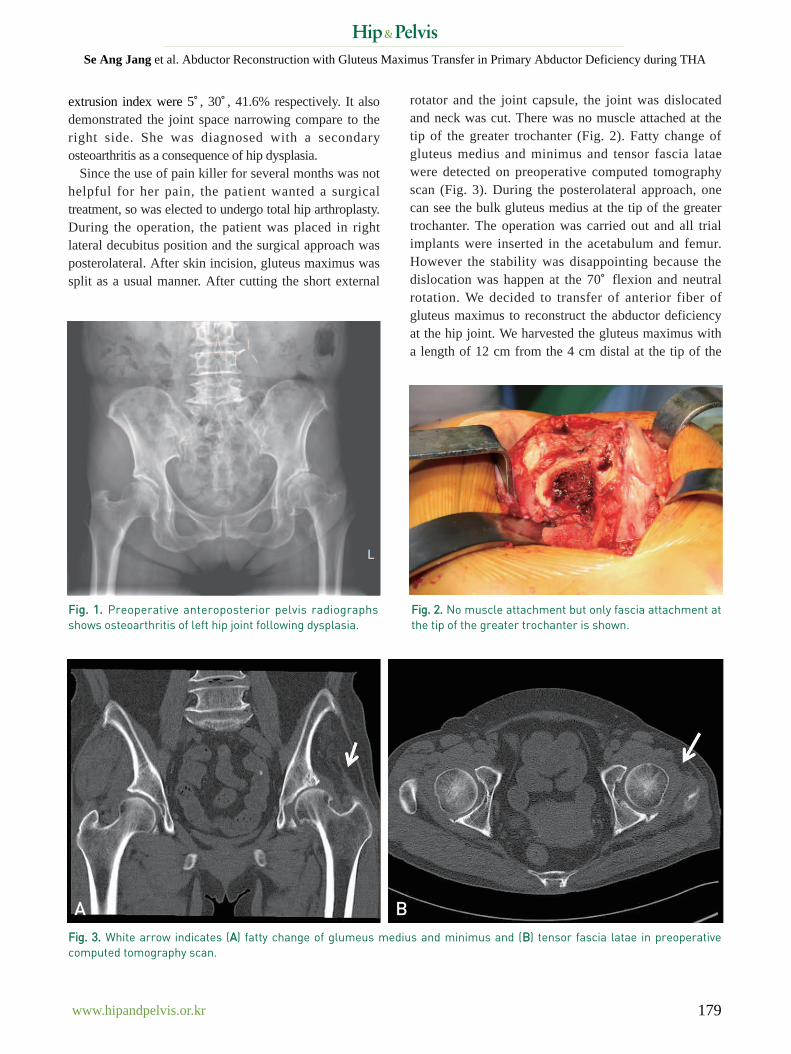
Plain radiographs on pelvis including anteroposterior andfrog leg lateral view were taken initially (Fig. 1). Lateralcenter edge angle, acetabular inclination, and femoral head
Abductor Reconstruction with GluteusMaximus Transfer in Primary Abductor
Deficiency during Total Hip ArthroplastySe Ang Jang, MD, Young Ho Cho, MD, Young Soo Byun, MD, Tae Hoe Gu, MDDepartment of Orthopaedic Surgery, Daegu Fatima Hospital, Daegu, Korea
Abductor deficiency in native hip joint may cause severe limping and pain. It is more serious situation in case ofarthroplasty due to instability and recurrent dislocation. Well-known causes of abductor deficiency are repeatedsurgery, chronic trochanteric bursitis, superior gluteal nerve injury, failure of repair of abductor tendon insertionto the greater trochanter. Author had experienced primary abductor deficiency during total hip replacement andtreated successfully with the transfer of gluteus maximus. We’d like to introduce the operation technique with thereview of literature.
Key Words: Hip, Abductor deficiency, Reconstruction, Gluteus maximus
Submitted: May 31, 2016 1st revision: July 12, 2016Final acceptance: July 15, 2016Address reprint request toYoung Ho Cho, MDDepartment of Orthopaedic Surgery, Daegu Fatima Hospital, 99Ayangro, Dong-gu, Daegu 41199, KoreaTEL: +82-53-940-7324 FAX: +82-53-954-7417E-mail: [email protected]
This is an Open Access article distributed under the terms of the CreativeCommons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use,distribution, and reproduction in any medium, provided the original work isproperly cited.
www.hipandpelvis.or.kr 179
Se Ang Jang et al. Abductor Reconstruction with Gluteus Maximus Transfer in Primary Abductor Deficiency during THA
extrusion index were 5。, 30。, 41.6% respectively. It alsodemonstrated the joint space narrowing compare to theright side. She was diagnosed with a secondaryosteoarthritis as a consequence of hip dysplasia.
Since the use of pain killer for several months was nothelpful for her pain, the patient wanted a surgicaltreatment, so was elected to undergo total hip arthroplasty.During the operation, the patient was placed in rightlateral decubitus position and the surgical approach wasposterolateral. After skin incision, gluteus maximus wassplit as a usual manner. After cutting the short external
rotator and the joint capsule, the joint was dislocatedand neck was cut. There was no muscle attached at thetip of the greater trochanter (Fig. 2). Fatty change ofgluteus medius and minimus and tensor fascia lataewere detected on preoperative computed tomographyscan (Fig. 3). During the posterolateral approach, onecan see the bulk gluteus medius at the tip of the greatertrochanter. The operation was carried out and all trialimplants were inserted in the acetabulum and femur.However the stability was disappointing because thedislocation was happen at the 70。flexion and neutralrotation. We decided to transfer of anterior fiber ofgluteus maximus to reconstruct the abductor deficiencyat the hip joint. We harvested the gluteus maximus witha length of 12 cm from the 4 cm distal at the tip of the
FFiigg.. 11.. Preoperative anteroposterior pelvis radiographsshows osteoarthritis of left hip joint following dysplasia.
FFiigg.. 33.. White arrow indicates (AA) fatty change of glumeus medius and minimus and (BB) tensor fascia latae in preoperativecomputed tomography scan.
FFiigg.. 22.. No muscle attachment but only fascia attachment atthe tip of the greater trochanter is shown.
A B
www.hipandpelvis.or.kr180
Hip Pelvis 28(3): 178-181, 2016
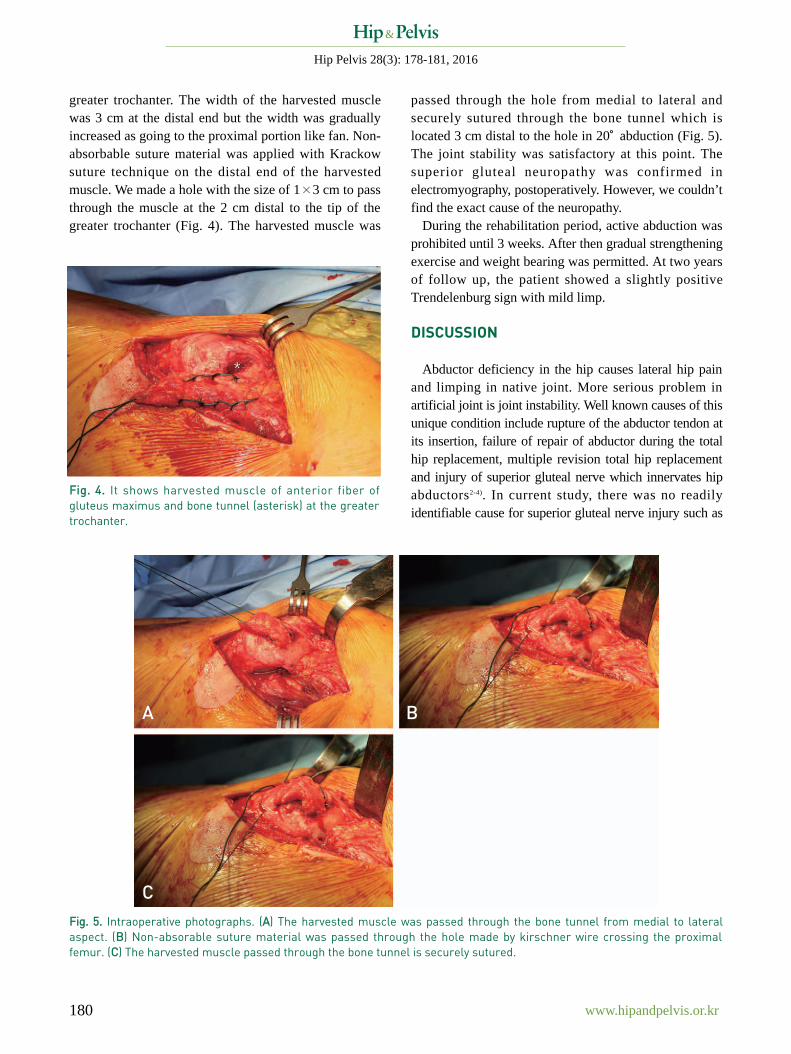
greater trochanter. The width of the harvested musclewas 3 cm at the distal end but the width was graduallyincreased as going to the proximal portion like fan. Non-absorbable suture material was applied with Krackowsuture technique on the distal end of the harvestedmuscle. We made a hole with the size of 1×3 cm to passthrough the muscle at the 2 cm distal to the tip of thegreater trochanter (Fig. 4). The harvested muscle was
passed through the hole from medial to lateral andsecurely sutured through the bone tunnel which islocated 3 cm distal to the hole in 20。abduction (Fig. 5).The joint stability was satisfactory at this point. Thesuperior gluteal neuropathy was confirmed inelectromyography, postoperatively. However, we couldn’tfind the exact cause of the neuropathy.
During the rehabilitation period, active abduction wasprohibited until 3 weeks. After then gradual strengtheningexercise and weight bearing was permitted. At two yearsof follow up, the patient showed a slightly positiveTrendelenburg sign with mild limp.
DISCUSSION
Abductor deficiency in the hip causes lateral hip painand limping in native joint. More serious problem inartificial joint is joint instability. Well known causes of thisunique condition include rupture of the abductor tendon atits insertion, failure of repair of abductor during the totalhip replacement, multiple revision total hip replacementand injury of superior gluteal nerve which innervates hipabductors2-4). In current study, there was no readilyidentifiable cause for superior gluteal nerve injury such as
FFiigg.. 44.. It shows harvested muscle of anterior fiber ofgluteus maximus and bone tunnel (asterisk) at the greatertrochanter.
FFiigg.. 55.. Intraoperative photographs. (AA) The harvested muscle was passed through the bone tunnel from medial to lateralaspect. (BB) Non-absorable suture material was passed through the hole made by kirschner wire crossing the proximalfemur. (CC) The harvested muscle passed through the bone tunnel is securely sutured.
A
C
B

www.hipandpelvis.or.kr 181
Se Ang Jang et al. Abductor Reconstruction with Gluteus Maximus Transfer in Primary Abductor Deficiency during THA
trauma, injection around hip joint, prior surgical history.Several techniques were introduced in the literatures6-9).
Fehm et al.6) reported the results of repair of a deficientabductor mechanism with achilles tendon allograft.However this technique was used in irreparable abductortendon at their insertion site. Kohl et al.7) introducedvastus lateralis muscle shift technique and had showedthe satisfactory result. As they mentioned in the article,however, their technique is complex, demanding, relativelyhigh complication rate and not easily applicable bymany surgeons.
An anatomic study1) showed the gluteus medius iscomposed of three distinct parts making up the fan shape.The posterior part of this muscle and gluteus minimus runalmost parallel to the neck of the femur. The fibers ofmiddle and anterior part run vertically. Distal attachmentsof these two muscles are the anterosuperior margin of thegreater trochanter not the lateral aspect. In this study, also,the authors postulated that the gluteus medius andminimus function primarily as hip stabilizers and pelvicrotators, rather than hip abductors. In other words, thehorizontal fibers work as hip stabilizer and the verticalfiber is pelvic rotator. The primary function of hipabduction would then be achieved via the tensor fasciaelatae muscle. According to this study, the joint stabilitycan be achieved by transfer of the anterior fiber of gluteusmaximus which have a running route similar to horizontalfibers of gluteus medius and gluteus minimus. If thefunction of the tensor fascia latae is normal, transfer ofthis muscle isn’t necessary.
Whiteside8,9) introduced two techniques for thereconstruction of deficient abductor of the hip. One istransfer of anterior fiber of gluteus maximus and theother is combined transfer of gluteus maximus andtensor fascia latae. The concept of Whiteside’s techniquesis similar with our technique; however, the differencesare as follow. The first one is distal fixation method. Wemade a hole to pass the harvested muscle from inside tooutside. We thought this method would reconstruct thegluteus medius and minimus simultaneously and maystabilize the femoral head in the acetabulum moreeffectively due to its closer location from the joint. Thesecond one is posterior capsule enforcement withposterior fiber of gluteus maximus. Theoretically, itwould be better than no soft tissue envelop in terms ofpreventing dislocation. But we can’t make sure theeffectiveness in the artificial joint. Because many hipsurgeons experiences that dislocation doesn’t happen in
the artificial joint without posterior capsule. So, wethought this additional procedure make the operationdifficult. The correct position of the implant, reconstructionof the deficient abductor and patient education are thecornerstone to prevent the dislocation. The third one iscombined transfer of tensor fascia latae. However, it’simpossible to transfer this muscle because combineddeficiency with gluteus medius due to superior glutealneuropathy.
There are several limitations in this study. First, weexperienced only one case. Second, follow-up period isalso short. Third, there is no comparative group.
Despite these several limitations, we think currenttechnique is one of the useful treatment methods to gainjoint stability and abductor function in the abductordeficient hip joint.
CONFLICT OF INTEREST
The authors declare that there is no potential conflictof interest relevant to this article.
REFERENCES
01.Gottschalk F, Kourosh S, Leveau B. The functional anatomyof tensor fasciae latae and gluteus medius and minimus. JAnat. 1989;166:179-89.
02.Davies H, Zhaeetan S, Tavakkolizadeh A, Janes G. Surgicalrepair of chronic tears of the hip abductor mechanism. HipInt. 2009;19:372-6.
03.Bird PA, Oakley SP, Shnier R, Kirkham BW. Prospectiveevaluation of magnetic resonance imaging and physicalexamination findings in patients with greater trochantericpain syndrome. Arthritis Rheum. 2001;44:2138-45.
04.Baker AS, Bitounis VC. Abductor function after total hipreplacement. An electromyographic and clinical review. JBone Joint Surg Br. 1989;71:47-50.
05.Daly PJ, Morrey BF. Operative correction of an unstabletotal hip arthroplasty. J Bone Joint Surg Am. 1992;74:1334-43.
06.Fehm MN, Huddleston JI, Burke DW, Geller JA, MalchauH. Repair of a deficient abductor mechanism with Achillestendon allograft after total hip replacement. J Bone JointSurg Am. 2010;92:2305-11.
07.Kohl S, Evangelopoulos DS, Siebenrock KA, Beck M. Hipabductor defect repair by means of a vastus lateralismuscle shift. J Arthroplasty. 2012;27:625-9.
08.Whiteside LA. Surgical technique: Transfer of the anteriorportion of the gluteus maximus muscle for abductor deficiencyof the hip. Clin Orthop Relat Res. 2012;470:503-10.
09.Whiteside LA. Surgical technique: Gluteus maximus andtensor fascia lata transfer for primary deficiency of theabductors of the hip. Clin Orthop Relat Res. 2014;472:645-53.