Embed Size (px)
Citation preview
Abdominal approach for Rectal prolapse
Leung Yu WingTKOH
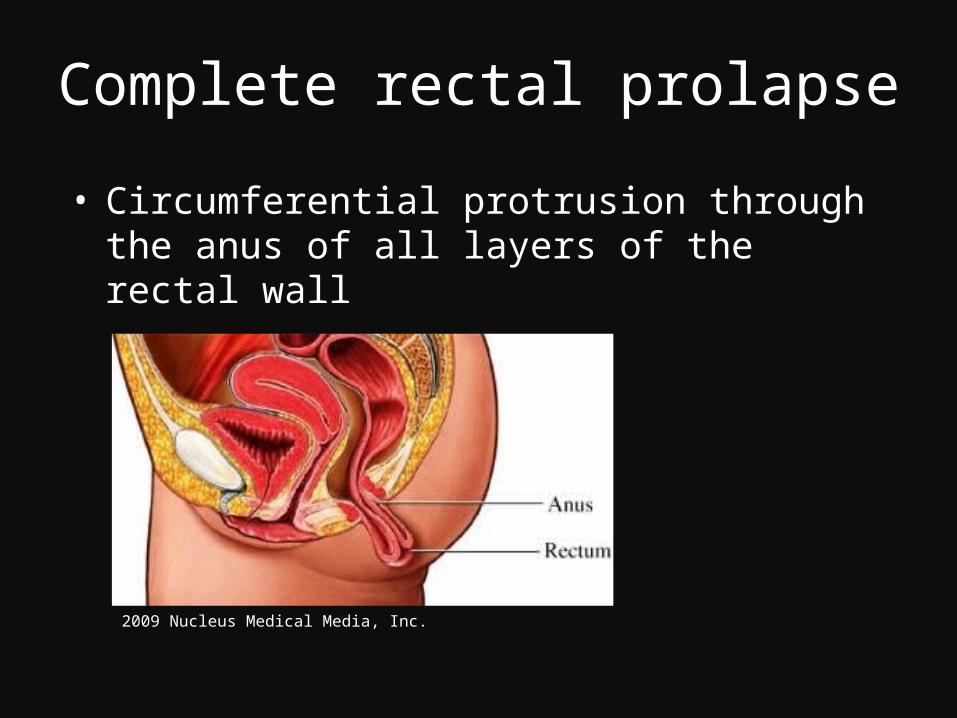
Complete rectal prolapse
• Circumferential protrusion through the anus of all layers of the rectal wall
2009 Nucleus Medical Media, Inc.
Epidemiology
• True incidence unknown• Annual incidence in Finland quoted to be
2.5/100, 000• Male to female 1:6• More common in the elderly
Kairaluoma MV, Kellokumpu IH. Epidemiologic aspects of complete rectal prolapse. Scand J Surg. 2005;94(3):207-10
Predisposing factors
• Chronic constipation• Multiple vaginal delivery• Previous surgery, e.g. hysterectomy• Connective tissue disorder
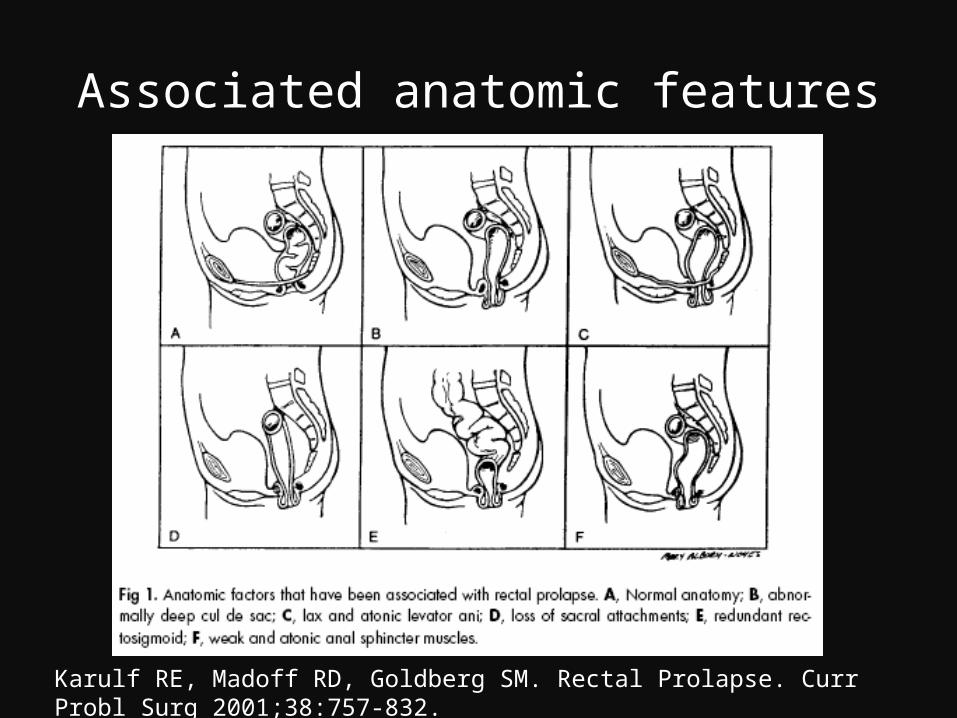
Associated anatomic features
Karulf RE, Madoff RD, Goldberg SM. Rectal Prolapse. Curr Probl Surg 2001;38:757-832.
Symptoms
• Protruding rectum• Faecal incontinence 50-75% • Constipation 25-50% • Pain variable• Ulceration 10-25%• Bleeding• Incarceration, gangrene rare
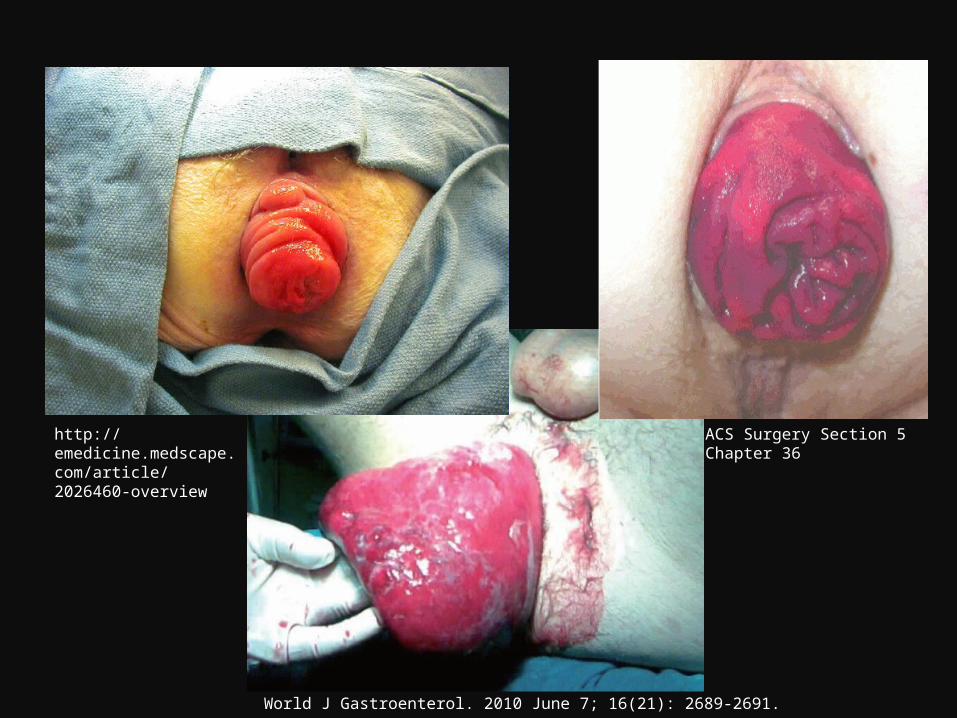
World J Gastroenterol. 2010 June 7; 16(21): 2689-2691.
http://emedicine.medscape.com/article/2026460-overview
ACS Surgery Section 5 Chapter 36
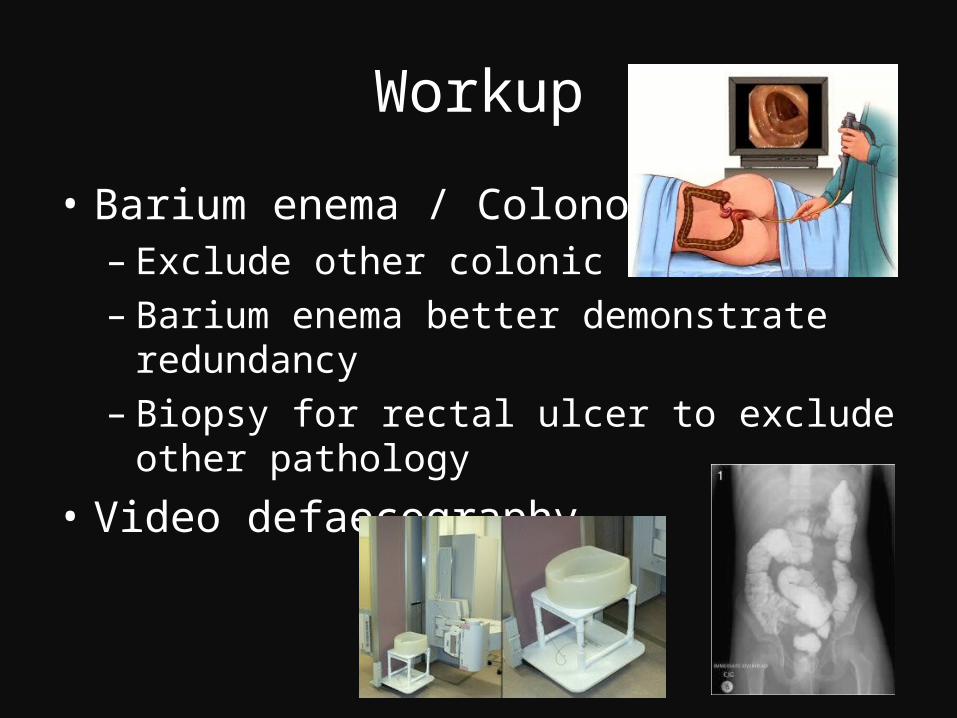
Workup
• Barium enema / Colonoscopy– Exclude other colonic lesions– Barium enema better demonstrate redundancy– Biopsy for rectal ulcer to exclude other pathology
• Video defaecography
Workup
• Anorectal manometry– Decrease in resting pressure in internal sphincter– Absence of anorectal inhibitory reflex
• Sitz marker study– Measure colonic transit to determine need for
colonic resection
• Pudendal nerve terminal motor latency (PNTML)– Neurologic injury / dysfunction
Management
• Fibre and stool softener may alleviate constipation
• Surgery is the mainstay for treatment
• No study directly compare surgical and conservative management
Tou S, Brown SR, Malik AI, Nelson RL. Surgery for complete rectal prolapse in adults. Cochrane Database Syst Rev. 2008: CD001758.
Management
• A number of procedures have been described
• Perineal approach for elderly frail patients
• Abdominal approach for fit patients
Brown AJ, Anderson JH, McKee RF, Finlay IG. Strategy for selection of type of operation for rectal prolapse based on clinical criteria. Dis Colon Rectum 2004; 47: 103–107Deen KI, Grant E, Billingham C, Keighley MRB. Abdominal resection rectopexy with pelvic floor repair versus perianal rectosigmoidectomy and pelvic floor repair for full-thickness rectal prolapse. British Journal of Surgery 1994;81(2):302–4.
Management
• Abdominal approach– division of lateral ligament vs no division– suture vs prosthesis for rectopexy– rectopexy vs resection + rectopexy– open vs laparoscopic
Division of lateral ligament
• 18 patients had posterior rectopexy, of whom 10 had division of lateral ligament
• No recurrence• No significant difference detected in
constipation score
Mollen RM, Kuijpers JH, van Hoek F. Effect of rectal mobilisation and lateral sphincter division on colonic and anorectal function. Diseases of the Colon and Rectum 2000;43:1283–7.
Division of lateral ligament• A prospective randomized study of rectopexy
with (n=14) or without (n=12) division of lateral ligaments
• Recurrence in the group with division vs without 0% vs 33%
• In the division group, constipation increased from 21.4% to 71.4% (pre-op to post-op)
Speakman CTM, Madden MV, Nicholls RJ, Kamm MA. Lateral ligament division during rectopexy causes constipation but prevents recurrence: results of a prospective randomized study. British Journal of Surgery 1991;78(12):1431–3.
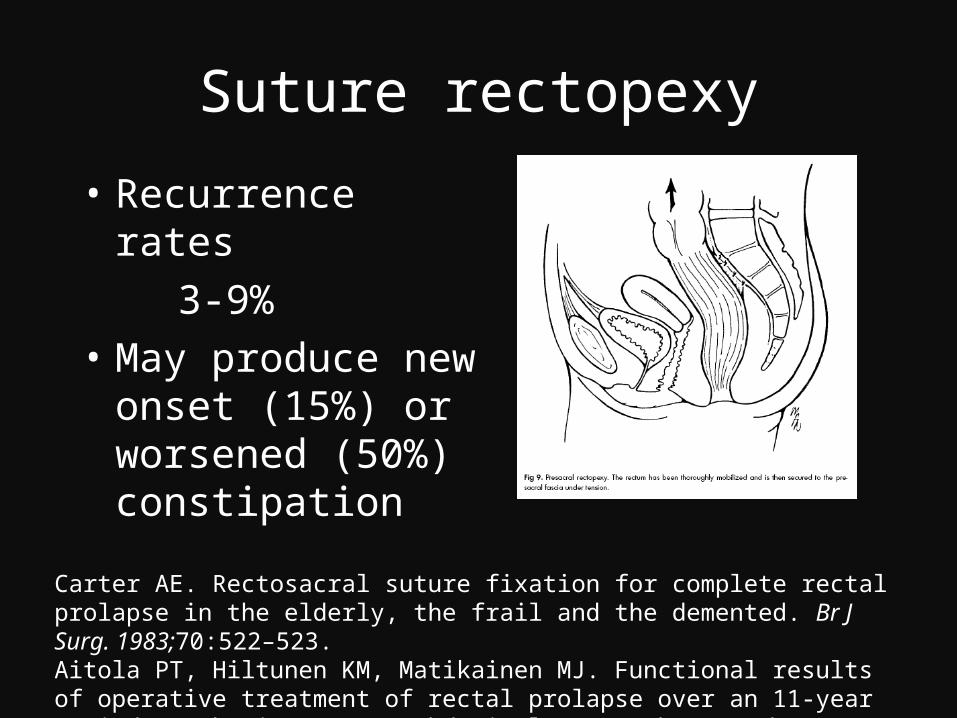
Suture rectopexy
• Recurrence rates 3-9%• May produce new
onset (15%) or worsened (50%) constipation
Carter AE. Rectosacral suture fixation for complete rectal prolapse in the elderly, the frail and the demented. Br J Surg. 1983;70:522–523.Aitola PT, Hiltunen KM, Matikainen MJ. Functional results of operative treatment of rectal prolapse over an 11-year period: emphasis on transabdominal approach. Dis Colon Rectum. 1999;42:655– 660.
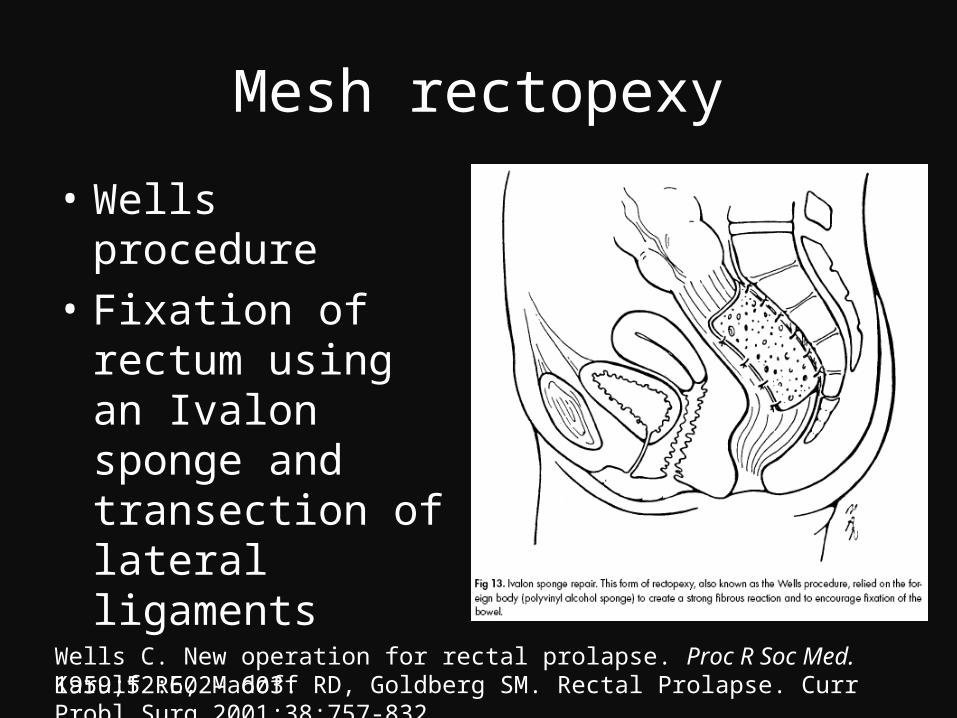
Mesh rectopexy
• Wells procedure • Fixation of rectum
using an Ivalon sponge and transection of lateral ligaments
Wells C. New operation for rectal prolapse. Proc R Soc Med. 1959;52:602– 603.Karulf RE, Madoff RD, Goldberg SM. Rectal Prolapse. Curr Probl Surg 2001;38:757-832.
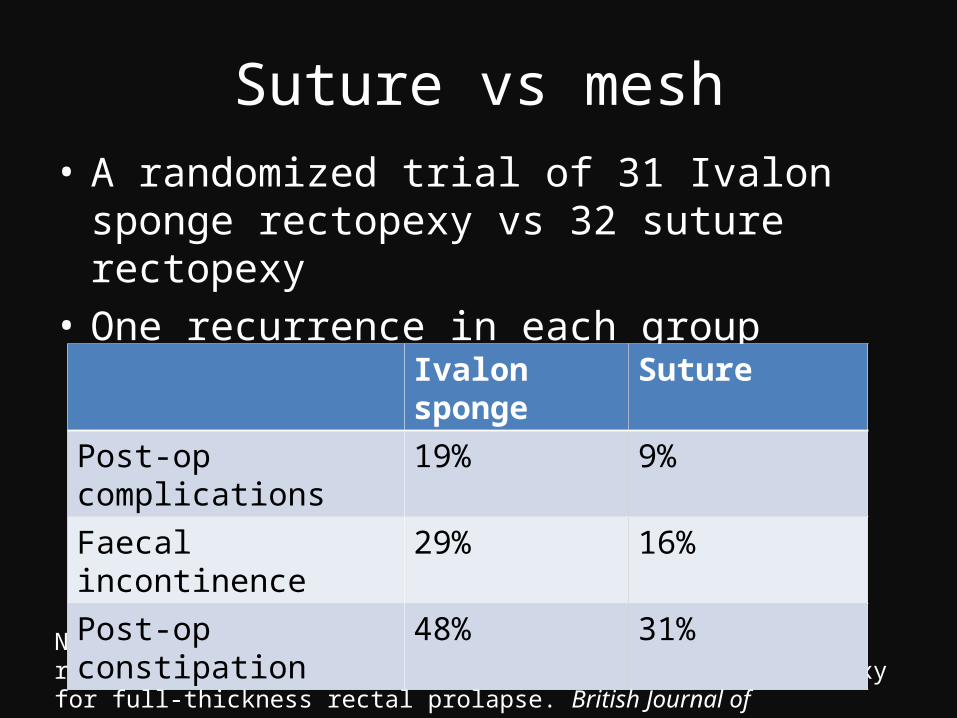
Suture vs mesh• A randomized trial of 31 Ivalon sponge rectopexy
vs 32 suture rectopexy• One recurrence in each group
Novell JR, Osborne MJ, Winslet MC, Lewis AA. Prospective randomized trial of Ivalon sponge versus sutured rectopexy for full-thickness rectal prolapse. British Journal of Surgery1994;81(6):904–6.
Ivalon sponge SuturePost-op complications 19% 9%
Faecal incontinence 29% 16%Post-op constipation 48% 31%
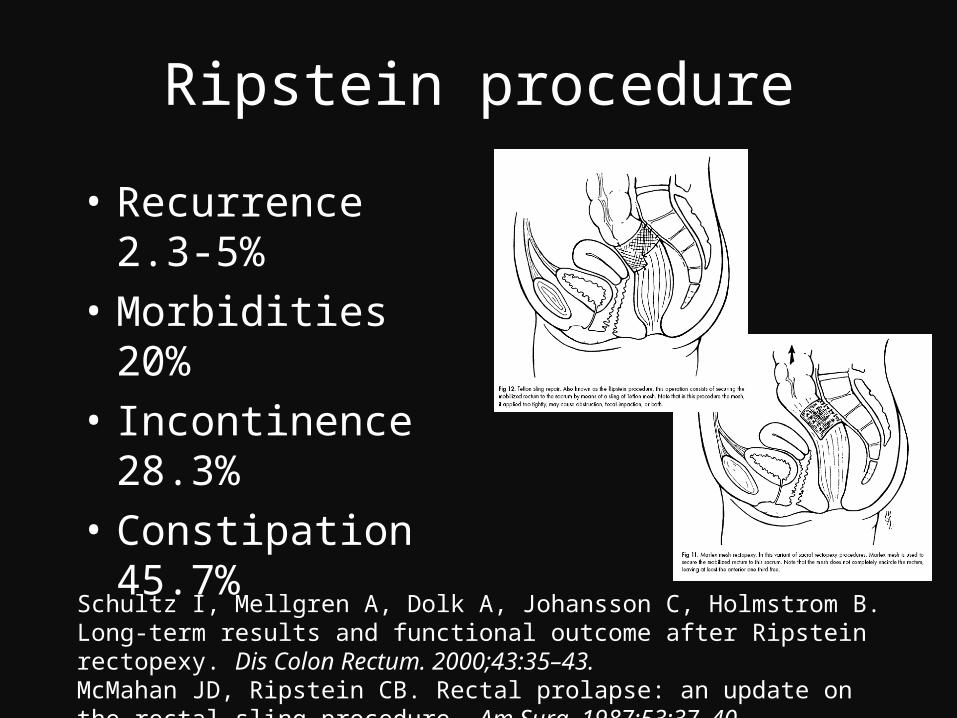
Ripstein procedure
• Recurrence 2.3-5%• Morbidities 20%• Incontinence 28.3%• Constipation 45.7%
Schultz I, Mellgren A, Dolk A, Johansson C, Holmstrom B. Long-term results and functional outcome after Ripstein rectopexy. Dis Colon Rectum. 2000;43:35–43.McMahan JD, Ripstein CB. Rectal prolapse: an update on the rectal sling procedure. Am Surg. 1987;53:37–40.
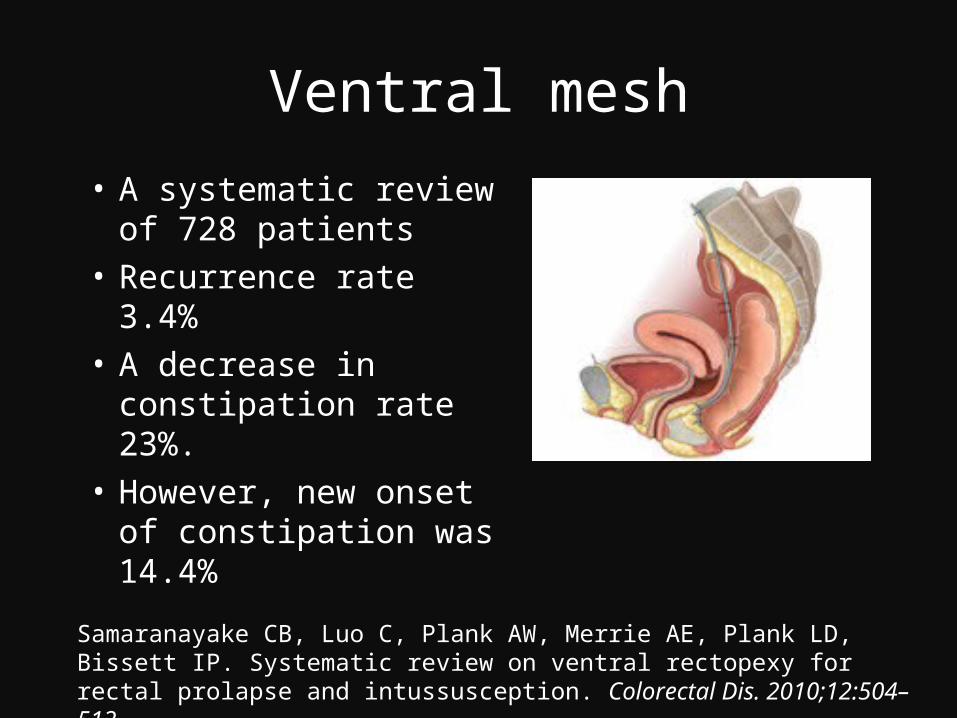
Ventral mesh
• A systematic review of 728 patients
• Recurrence rate 3.4%• A decrease in
constipation rate 23%. • However, new onset
of constipation was 14.4%
Samaranayake CB, Luo C, Plank AW, Merrie AE, Plank LD, Bissett IP. Systematic review on ventral rectopexy for rectal prolapse and intussusception. Colorectal Dis. 2010;12:504–512.
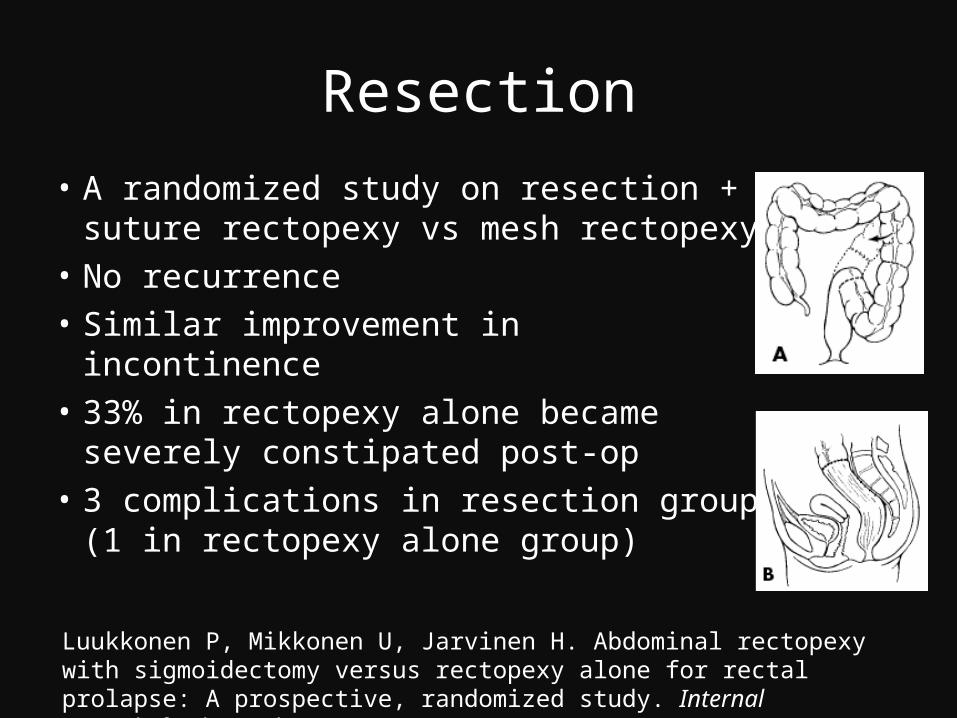
Resection
• A randomized study on resection + suture rectopexy vs mesh rectopexy
• No recurrence• Similar improvement in incontinence• 33% in rectopexy alone became
severely constipated post-op• 3 complications in resection group (1
in rectopexy alone group)Luukkonen P, Mikkonen U, Jarvinen H. Abdominal rectopexy with sigmoidectomy versus rectopexy alone for rectal prolapse: A prospective, randomized study. InternalJournal of Colorectal Disease 1992;7(4):219–22.
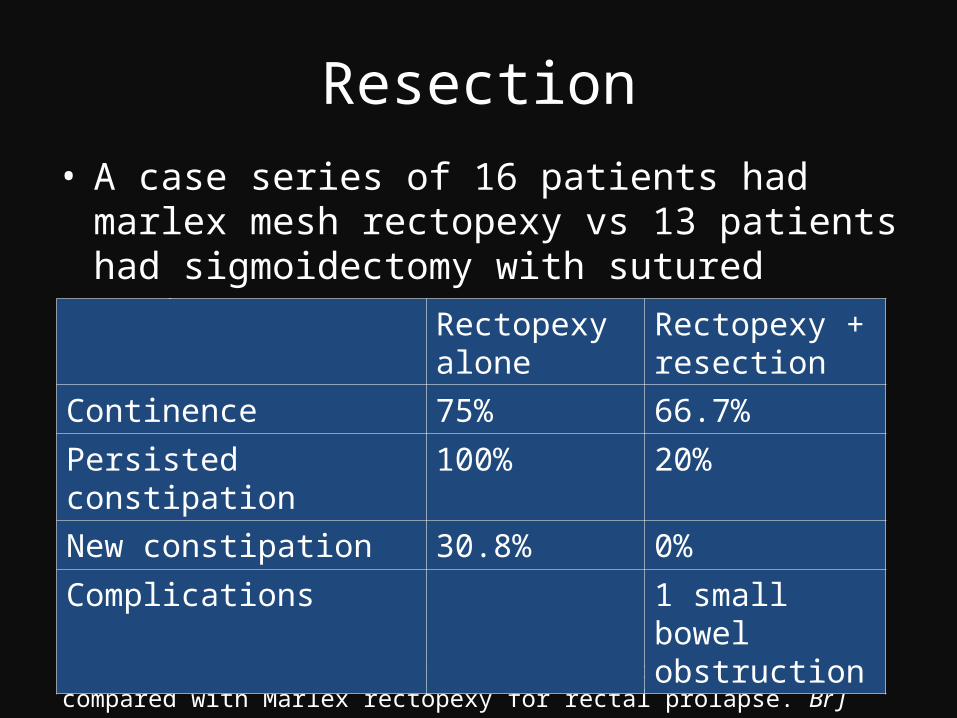
Resection• A case series of 16 patients had marlex mesh
rectopexy vs 13 patients had sigmoidectomy with sutured rectopexy
Sayfan J, Pinho M, Alexander-Williams J, Keighley MR. Sutured posterior abdominal rectopexy with sigmoidectomy compared with Marlex rectopexy for rectal prolapse. Br J Surg. 1990;77:143–145.
Rectopexy alone
Rectopexy + resection
Continence 75% 66.7%
Persisted constipation 100% 20%
New constipation 30.8% 0%
Complications 1 small bowel obstruction
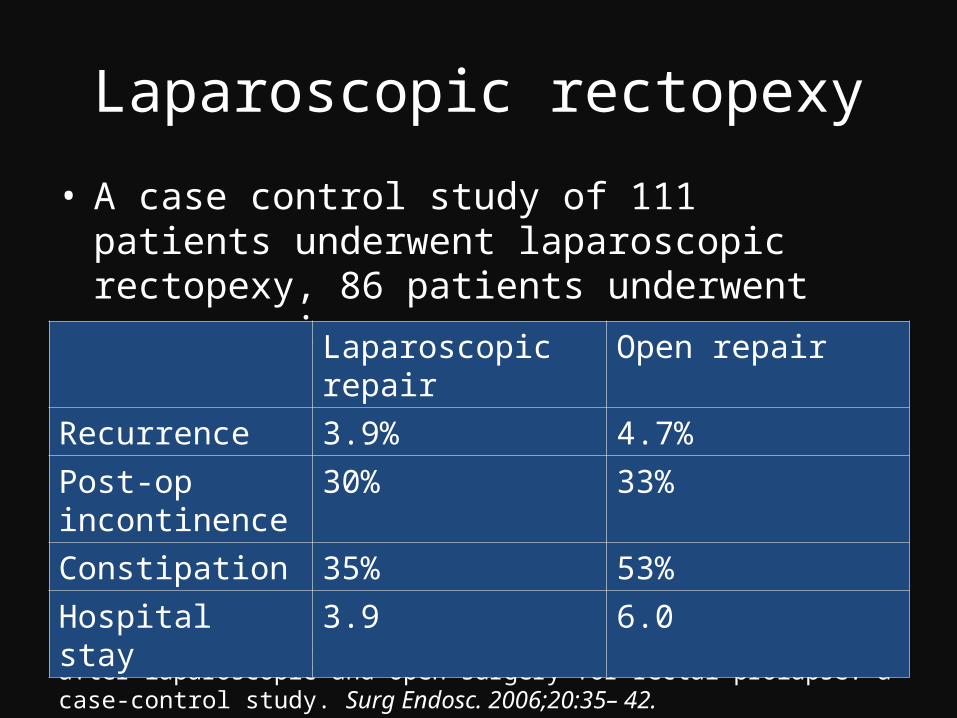
Laparoscopic rectopexy
• A case control study of 111 patients underwent laparoscopic rectopexy, 86 patients underwent open repair
Kariv Y, Delaney CP, Casillas S, et al. Long-term outcome after laparoscopic and open surgery for rectal prolapse: a case-control study. Surg Endosc. 2006;20:35– 42.
Laparoscopic repair Open repair
Recurrence 3.9% 4.7%Post-op incontinence
30% 33%
Constipation 35% 53%Hospital stay 3.9 6.0
Laparoscopic rectopexy
• 40 patients randomized to laparoscopic vs open group
• Laparoscopy group:– less pain and narcotic requirement– better mobility– shorter hospital stay– Estimated saving of 357 pounds
per patientSalkeld G, Bagia M, Solomon M. Economic impact of laparoscopic versus open abdominal rectopexy. British Journal of Surgery 2004;91(9):1188–91.Solomon MJ, Young CJ, Eyers AA, Roberts RA. Randomized clinical trial of laparoscopic versus open abdominal rectopexy for rectal prolapse. British Journal of Surgery 2002;89(1):35–9.

Robotic
Moorthy K, Kudchadkar R, et al. Robotic assisted rectopexy. Am J Surg. 2004;187:88 –92.
Robotic
• 14 robot assisted laparoscopic rectopexy vs 19 conventional laparoscopic rectopexy
• Similar conversion rates 3-5%• Similar constipation, continence• Mean operating time 39min longer• Costs US$745.09 higher
Heemskerk J, de Hoog DE, van Gemert WG, Baeten CG, Greve JW, Bouvy ND. Robot-assisted vs conventional laparoscopic rectopexy for rectal prolapse: a comparative study on costs and time. Dis Colon Rectum. 2007;50:1825–1830..
Conclusion
• Abdominal approach– Division of lateral ligament vs no division
• Division of lateral ligament may have less recurrence, but more constipation
– Suture vs prosthesis for rectopexy• Prosthesis may have more complications, more
constipation
Conclusion
• Abdominal approach– Rectopexy vs resection + rectopexy
• With resection, there is less constipation, but slightly more complications
– Open vs laparoscopic• Laparoscopic approach has comparable results• Laparoscopic approach decreases hospital stay
and costs
PROSPER trial
• 293 patients from 2/2001 to 4/2008 were randomised between – (a) abdominal and perineal and – (b) suture vs resection rectopexy for those receiving
abdominal procedure or – (c) Altemeier’s vs Delorme’s for those receiving
perineal procedures• Primary outcome were defaecatory performance
and QOL, secondary outcome were operative mortality / morbidity and recurrence
http://www.birmingham.ac.uk/research/activity/mds/trials/bctu/trials/coloproctology/prosper/index.aspx
Q&A


Workup
• In 26 patients of rectal prolapse, EMG and pudendal nerve terminal motor latency were performed before Ripstein rectopexy
• Anal continence was improved, but was not predicted by pre-op EMG / PNTML
Schultz I, Mellgren A, Nilsson BY, Dolk A, Holmstrom B. Preoperative electrophysiologic assessment cannot predict continence after rectopexy. Dis Colon Rectum. 1998;41:1392–1398.
Workup
• 45 patients underwent anal manometry and PNTML before rectal prolapse repair
• Pre-op squeeze pressure >60mmHg vs lower Better post-op fecal continence 10% vs 54%
• PNTML was not predictive of post-op continence
Glasgow SC, Birnbaum EH, Kodner IJ, Fleshman JW, Dietz DW. Preoperative Anal Manometry Predicts Continence After Perineal Proctectomy for Rectal Prolapse. Dis Colon Rectum. 2006;49:1052-1058.
Division of lateral ligament
• 20 patients randomized, 11 underwent marlex rectopexy with division of lateral ligament, 9 patients without.
• Continence improved in both groups, post-op symptoms improved significantly in those without division compared with those with division.
Selvaggi F, Scotto di Carlo E, Silvestri L, Festa L, Piegari V. Surgical treatment of rectal prolapse: a randomised study (Abstract). British Journal of Surgery 1993;80:S89.
No rectopexy vs rectopexy
• Multicentre randomized controlled trial of 251 patients
• 116 no rectopexy compared with 136 rectopexy, sigmoidectomy added if constipation
• No sig difference in complication• Significant difference in 5 year recurrence
8.6% vs 1.5%Karas JR, Uranues S, Altomare DF, et al. No rectopexy versus rectopexy following rectal mobilization for full-thickness rectal prolapse: a randomized controlled trial. Dis Colon Rectum. 2011 Jan;54(1):29-34
Alternative mesh materials• 2 trials comparing polyglycolic acid mesh (n=37) vs
polyglactin (n=30) / polypropylene (n=17) mesh• 1 recurrence in polyglycolic acid mesh• Residual incontinence
– 20% for polyglycolic acid mesh – 35% for polyglactin mesh
Winde G, Reers B, Nottberg H, Berns T, Meyer J, Bunte H. Clinical and functional results of abdominal rectopexy with absorbable mesh-graft for treatment of complete rectalprolapse. European Journal of Surgery 1993;59(5):301–5.Galili Y, Rabau M. Comparison of polyglycolic acid and polypropylene mesh for rectopexy in the treatment of rectal prolapse. European Journal of Surgery 1997;163(6):445–8.
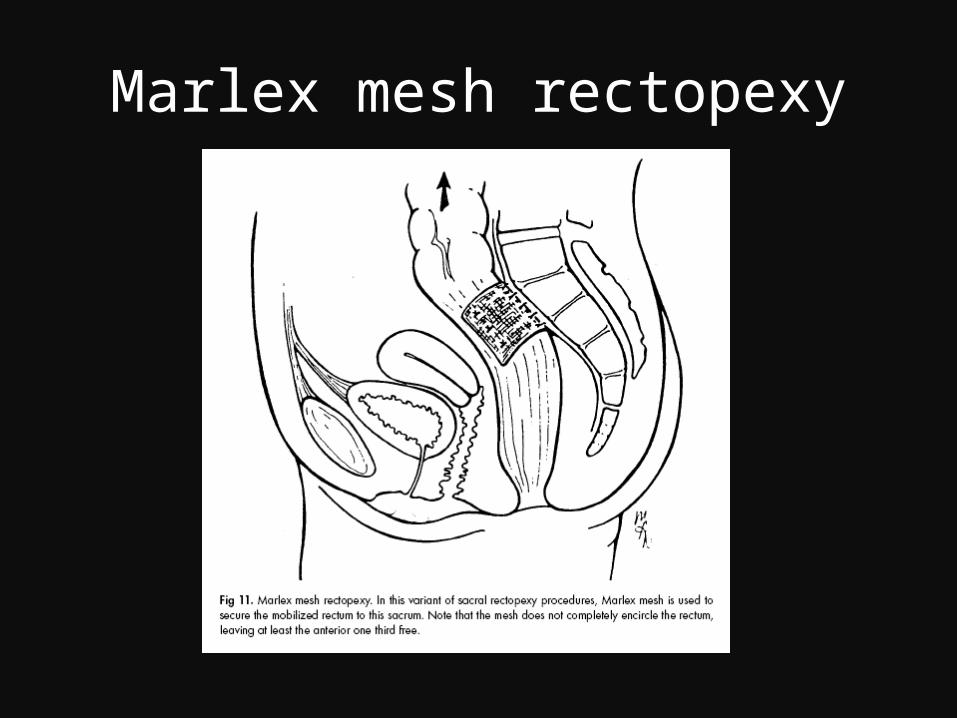
Marlex mesh rectopexy
Resection
• 18 patients randomized to rectopexy alone or with sigmoidectomy
• 77.8% in rectopexy alone group, 22.2% in sigmoidectomy group complained of severe constipation
Mckee RF, Lauder JC, Poon FW, Aitchison MA, Finlay IG. A prospective randomized study of abdominal rectopexy with and without sigmoidectomy in rectal prolapse. Surgery, Gynecology and Obstretics 1992;174(2):145–8.
Resection
• 12 patients with no preexisting constipation had laparoscopic rectopexy without resection
• No complications• No recurrence• Only 1 patient previously had irritable bowel
syndrome developed significant constipation
Hsu A, Brand MI, Saclarides TJ. Laparoscopic rectopexy without resection: a worthwhile treatment for rectal prolapse in patients without prior constipation. Am Surg. 2007;73:858–861.
Laparoscopic rectopexy
• Retrospective study of 13 by open technique and 8 by laparoscopic approach
• Incontinence sig. improved in both groups
• Post-op stay was shorter in laparoscopic group
Boccasanta P, Rosati R, Venturi M, Montorsi M, Cioffi U, De Simone M, et al.Comparison of laparoscopic rectopexy with open technique in the treatment of complete rectal prolapse: clinical and functional results. Surgical Laparoscopy and Endoscopy 1998;8(6):460–5.
Laparoscopic rectopexy
• A case series of 109 patients had laparoscopic ventral rectopexy for rectal prolapse
• Conversion 3.7%• Recurrence 3.7%• No mortality, minor morbidity 7%• Mean hospital stay 5.14 days
D’Hoore A, Penninckx F. Laparoscopic ventral recto(colpo)pexy for rectal prolapse: surgical technique and outcome for 109 patients. Surg Endosc. 2006;20:1919 –1923.DHoore A, Cadoni R, Penninckx F (2004) Long-term outcome of laparoscopic ventral rectopexy for total rectal prolapse. Br J Surg 91: 1500–1505
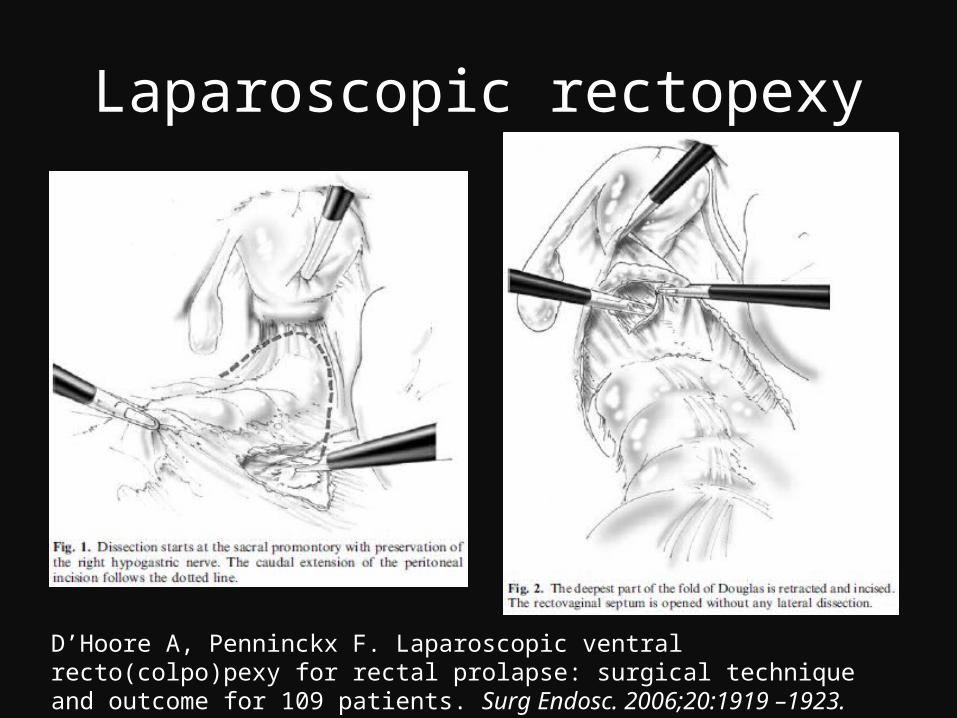
Laparoscopic rectopexy
D’Hoore A, Penninckx F. Laparoscopic ventral recto(colpo)pexy for rectal prolapse: surgical technique and outcome for 109 patients. Surg Endosc. 2006;20:1919 –1923.
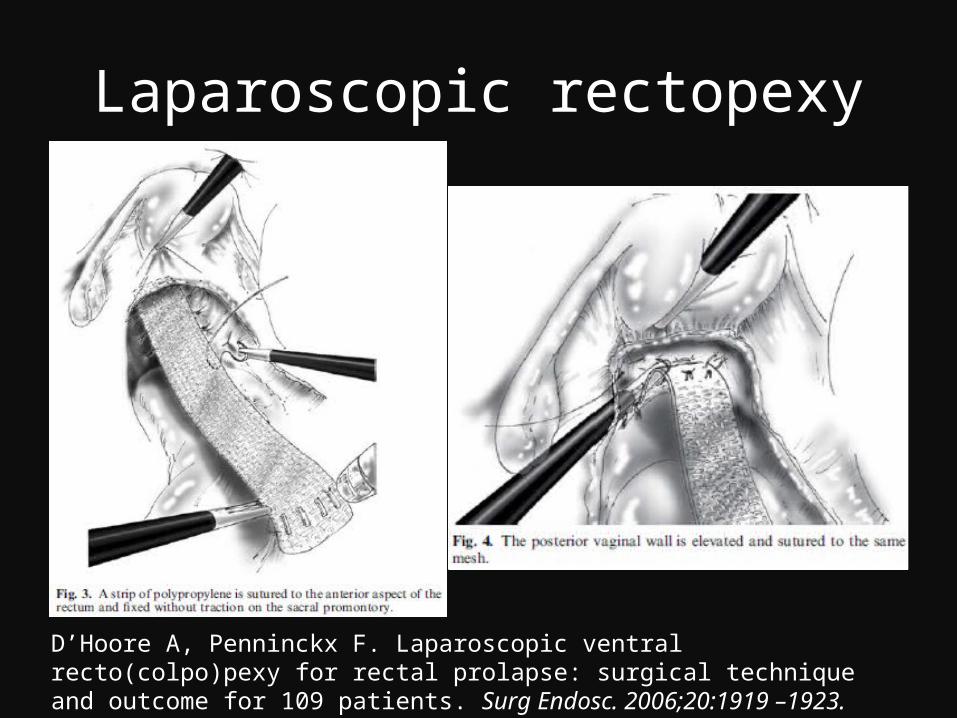
Laparoscopic rectopexy
D’Hoore A, Penninckx F. Laparoscopic ventral recto(colpo)pexy for rectal prolapse: surgical technique and outcome for 109 patients. Surg Endosc. 2006;20:1919 –1923.
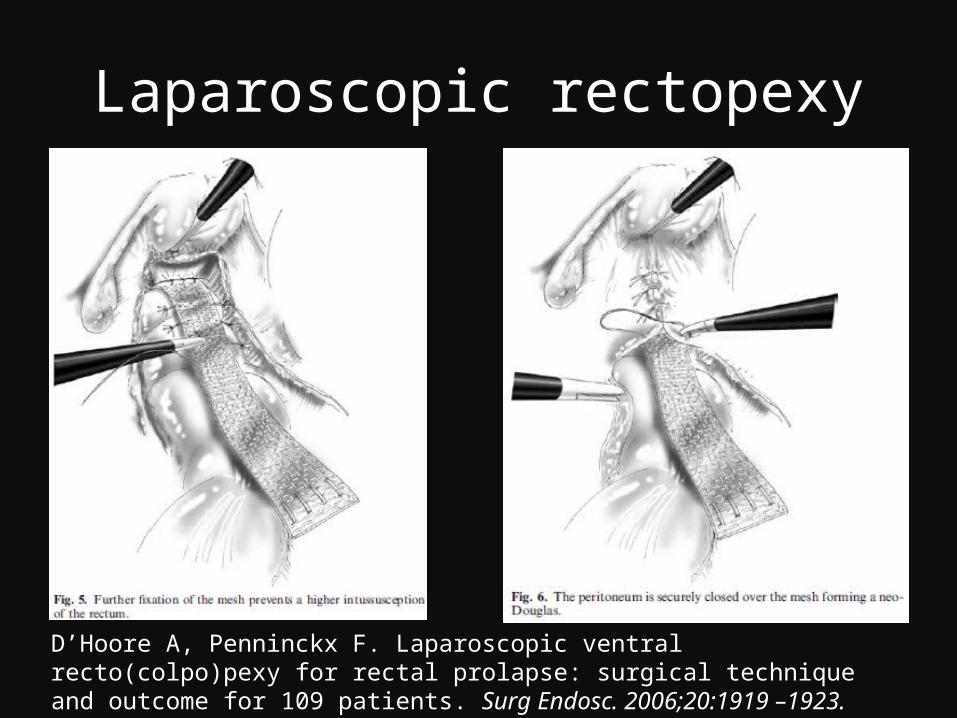
Laparoscopic rectopexy
D’Hoore A, Penninckx F. Laparoscopic ventral recto(colpo)pexy for rectal prolapse: surgical technique and outcome for 109 patients. Surg Endosc. 2006;20:1919 –1923.
Anterior resection• In a review of 113 patients• Operative morbidity 29%, including 3
anastomotic leakage• Recurrence rate at 2, 5, 10 years were 3%, 6%,
12%• Also a low pelvic anastomosis in those with
borderline continence may cause complete loss of control
Cirocco WC, Brown AC. Anterior resection for the treatment of rectal prolapse: a 20-year experience. Am Surg. 1993;59:265–269.Schlinkert RT, Beart RW Jr, Wolff BG, Pemberton JH. Anterior resection for complete rectal prolapse. Dis Colon Rectum. 1985;28:409–412.
Robotic
• 2 mesh rectopexy, 4 sutured rectopexy + sigmoidectomy were performed
• No mortality• 1 conversion• 1 rectal tear with temporary
colostomy• No recurrence
Ayav A, Bresler L, Hubert J, Brunaud L, Boissel P. Robotic-assisted pelvic organ prolapse surgery. Surg Endosc. 2005;19:1200–1203.
Robotic
• 6 cases of robotic assisted rectopexy
• No conversion• No mortality or major
complications• No recurrence• No reports of constipation• Mean operative time 127minMoorthy K, Kudchadkar R, et al. Robotic assisted rectopexy. Am J Surg. 2004;187:88 –92.
Quality of life
• 54 patients underwent laparoscopic rectopexy• No mortality, morbidity 5.5%• 7.4% recurrence• 20.3% constipation• Continence improved in 72.4%• QOL rated satisfactory in 96%
Auguste T, Dubreuil A, Bost R, Bonaz B, Faucheron JL. Technical and functional results after laparoscopic rectopexy to the promontory for complete rectal prolapse. Prospective study in 54 consecutive patients. Gastroenterol Clin Biol. 2006 May;30(5):659-63.
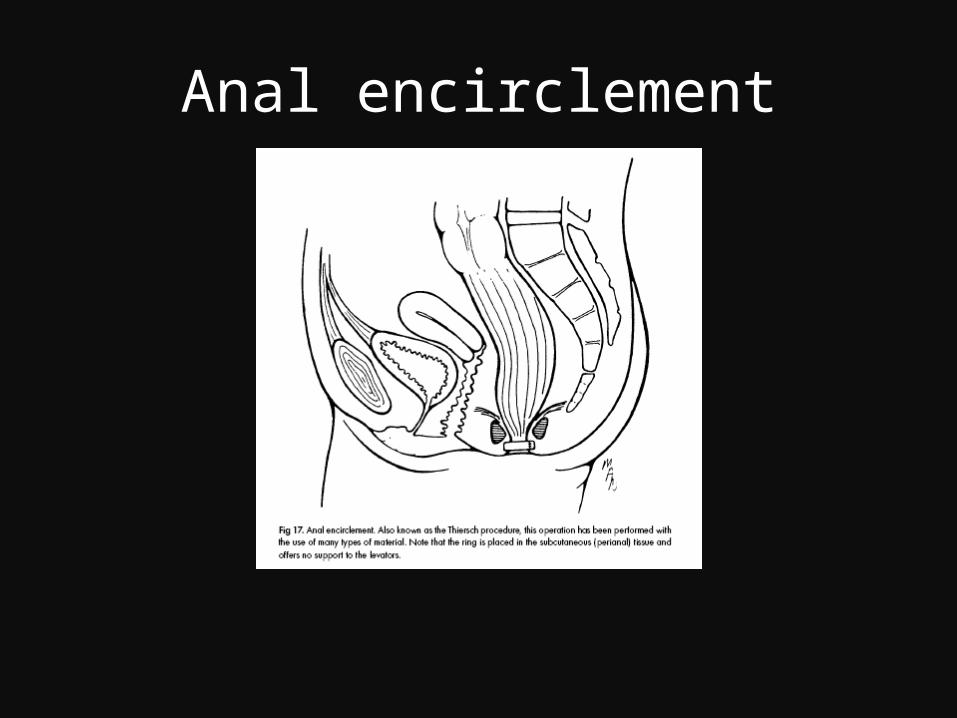
Anal encirclement
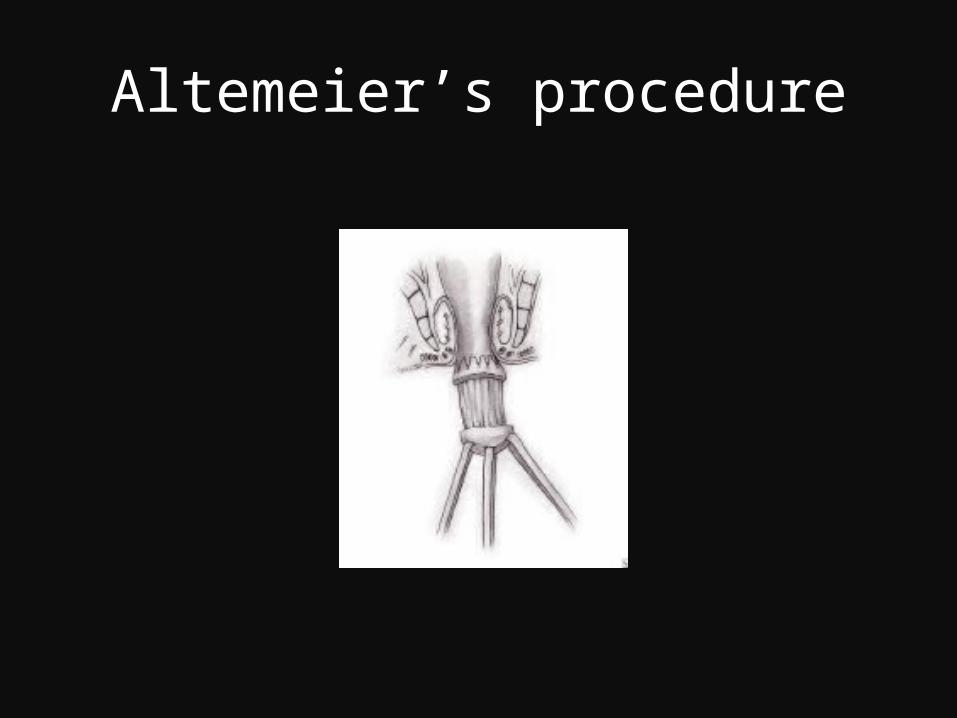
Altemeier’s procedure
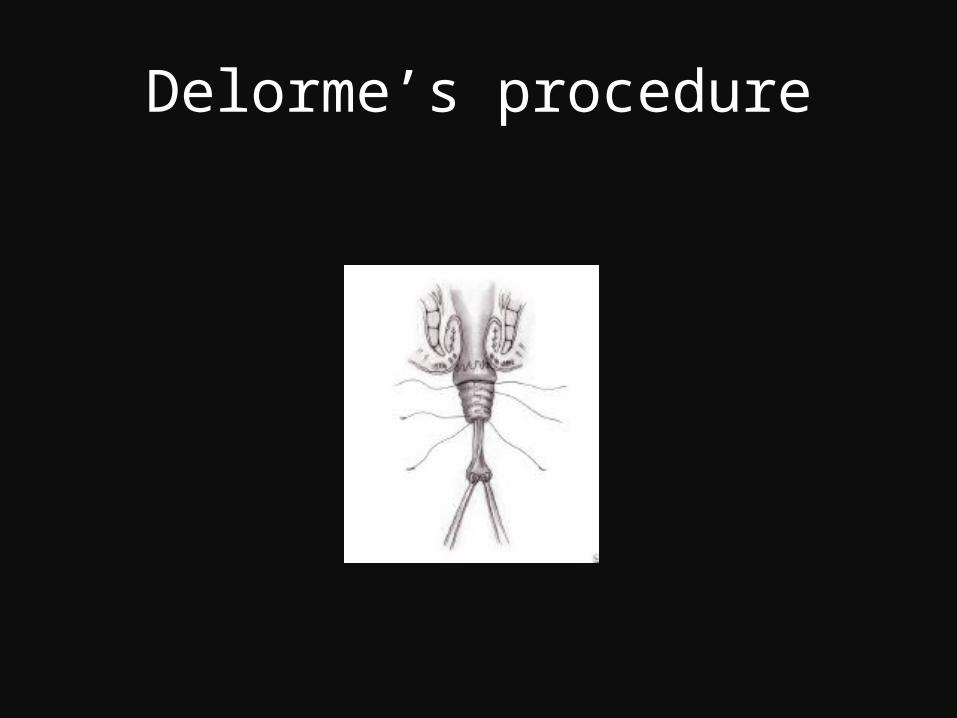
Delorme’s procedure
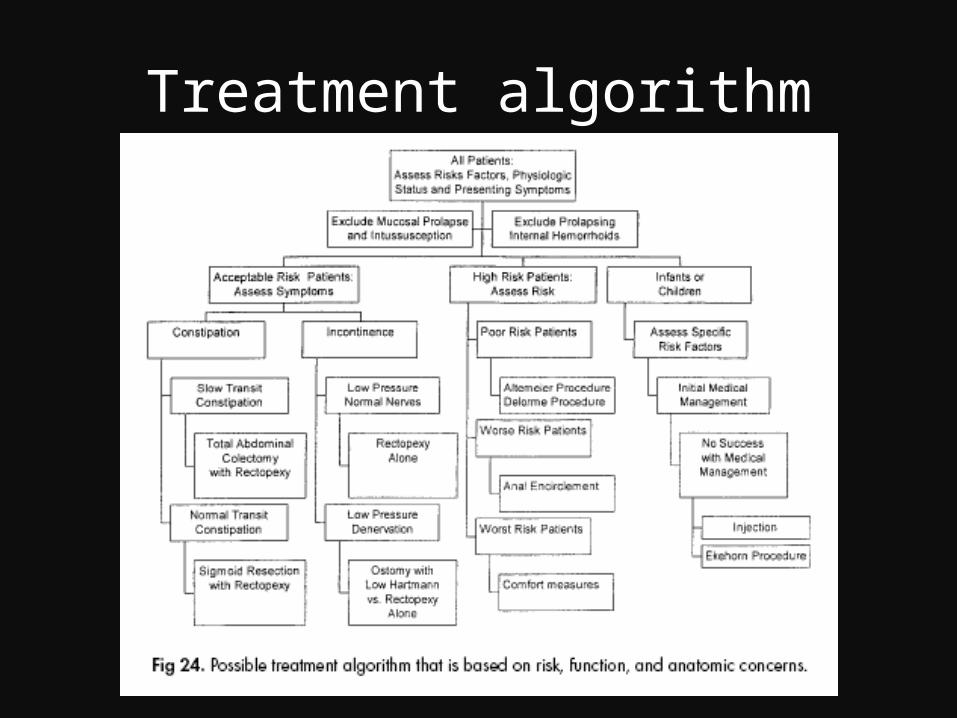
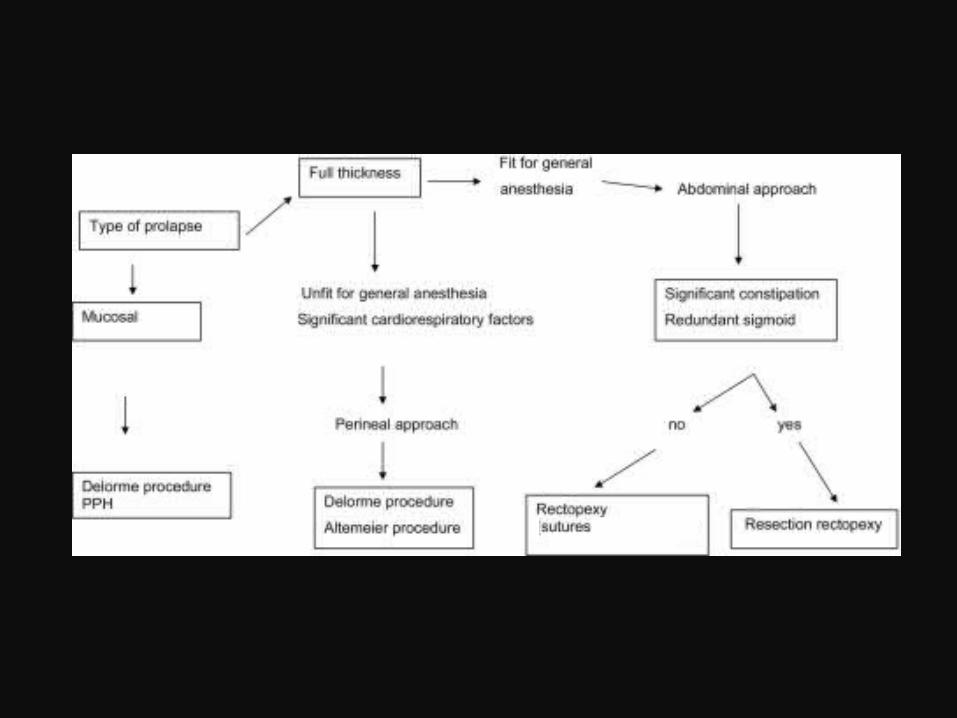
Treatment algorithm





























