Embed Size (px)
Citation preview

Opportunities, Threats Face NPs AsCongress Deals with Deficits
Dave Mason, Mason Consulting, LLC
A A
N P
FOR
As springtime temperatures start to warm, battlesin Washington over restraining the growth of federalspending are heating up, too. From expiring taxcuts to across-the-board spending reductions to raisingthe limit on the national debt, it seems that PresidentBarack Obama and congressional leaders have beentrying to avoid one “fiscal cliff” after another formonths. A key aspect of these efforts to get the federalbudget under control is reforming mandatoryspending programs such as Social Security, Medicare,and Medicaid. Efforts to restructure these programsare obviously laced with political perils, meaning thatRepublicans and Democrats have only a few monthsto reach some agreement before the politics of the2014 mid-term congressional election starts toemphasize areas of partisan differences rather thanbipartisan accord.
Modernizing Medicare and Medicaid will beessential to the nation’s long-term fiscal stability, butrecent efforts provide ample evidence that reachingagreement on how to improve the programs will beextremely difficult. House Republicans proposeda budget for fiscal year 2013 a year ago that includedrepealing large parts of the Affordable Care Act(such as the Prevention and Public Health Fund),converting Medicare into a defined benefit voucherprogram, and turning Medicaid and the SupplementalNutritional Assistance Program, formerly known asfood stamps, into block-grant programs to states. Thatplan drew strong partisan opposition and eventuallydied in the Senate, which was unable to reachagreement and pass its own 2013 budget. The Senatealso ignored a budget reconciliation bill passed bythe House last May that would have replaced the
automatic “sequestration” of discretionary fundingwith deeper cuts in health programs. Critics arguedthat the House targets for Medicare and Medicaidsavings were so high that structural changes under-cutting eligibility and benefits would be inevitable.
Medicare and Medicaid reforms could clearly havea significant impact on nurse practitioners. Steepreductions in federal spending could result in greaterfinancial burden on states, coupled with fewer federalrules defining payment and practice requirements forproviders. Such a shift could be harmful or beneficialfor nurse practitioners depending on the law in thestates where they practice, but it would clearly makestate-level policy debates even more important eespecially as states debate establishing and operatinghealth insurance exchanges and expanding eligibilityfor Medicaid coverage. Efforts to achieve moreefficient patient care through better coordinationcould mean shifting from traditional fee-for-servicepayments to bundled payments for episodes of careor expansions of medical and health homes andaccountable care structures. Changes such as theseshould favor greater use of nurse practitioners recog-nized to provide care at the top of their licenses e butwill they? Or will arcane perceptions of medicalpractice result in extended barriers to recognizing thecare that NPs and other advanced practice registerednurses are capable of providing?
It isn’t clear if 2013 will be the year that federalpolicy makers come to grips with reforming healthcare entitlement programs. But it is critical that theirdebate include recognition of the modern practicesand capabilities of nurse practitioners as part of thesolution to controlling health care spending.
A17
UM
A18
A A
N P
FO
RU
M
State of the StatesTay Kopanos, DNP, NP, Vice President of Health Policy/State Government Affairs
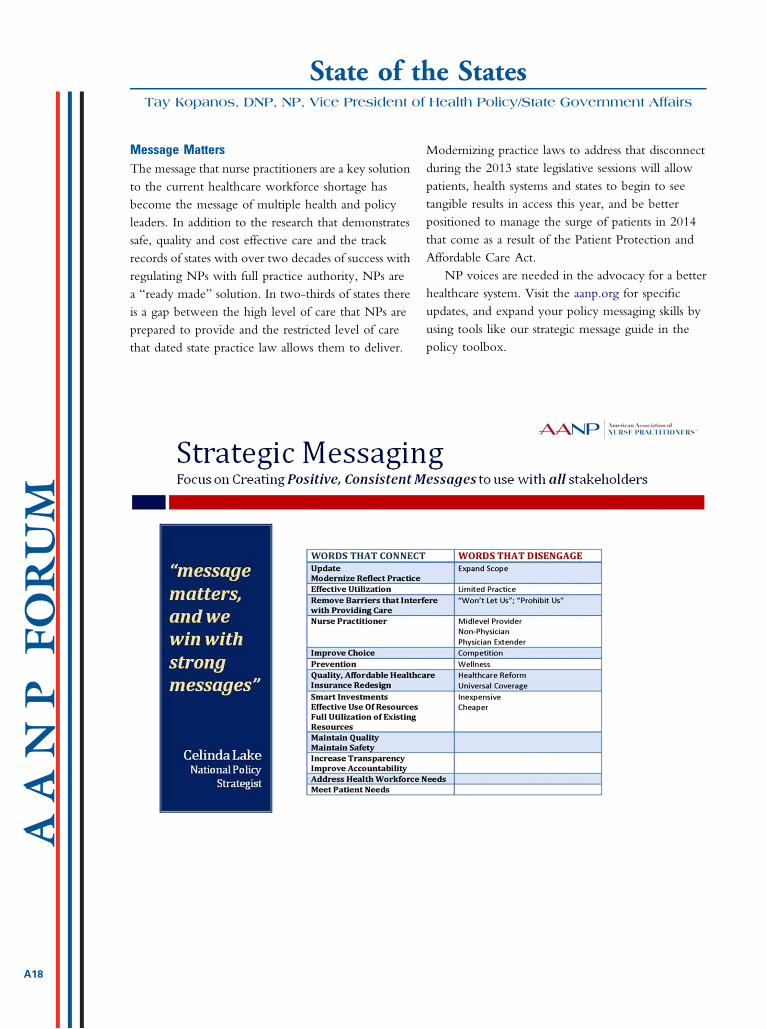
Message MattersThe message that nurse practitioners are a key solutionto the current healthcare workforce shortage hasbecome the message of multiple health and policyleaders. In addition to the research that demonstratessafe, quality and cost effective care and the trackrecords of states with over two decades of success withregulating NPs with full practice authority, NPs area “ready made” solution. In two-thirds of states thereis a gap between the high level of care that NPs areprepared to provide and the restricted level of carethat dated state practice law allows them to deliver.
Modernizing practice laws to address that disconnectduring the 2013 state legislative sessions will allowpatients, health systems and states to begin to seetangible results in access this year, and be betterpositioned to manage the surge of patients in 2014that come as a result of the Patient Protection andAffordable Care Act.
NP voices are needed in the advocacy for a betterhealthcare system. Visit the aanp.org for specificupdates, and expand your policy messaging skills byusing tools like our strategic message guide in thepolicy toolbox.
Registration Brochure NowAvailable Online for the 2013
National ConferenceThe 28th National Conference will be held June 19-23,2013, at The Venetian, The Palazzo, and Sands Expo andConvention Center, Las Vegas, Nevada.
The 2013 AANP National Conference RegistrationBrochure is available at http://www.aanp.org. Featuringan additional day of workshops on Tuesday, June 18,the conference includes approximately 350 concurrentsessions and 40 skill-enhancing workshops with up to 42contact hours of continuing education. Register early forthe best selection of workshops and sessions! Workshopshave limited seating and fill quickly.
Upon completion of registration and payment, yourreceipt will contain a link to AANP Housing and theAccess Code required to make reservations at theconference hotel, The Venetian and The Palazzo. AANP
has arranged for a specialconference rate of $159 perstandard suite, plus taxes andresort fee. This rate will behonored for reservations thatoccur any nights, June 15-25,2013, based on availabilitywith some restrictions.
If you have questions orneed assistance, please [email protected] or call
(512) 442-4262, ext. 5238.Join us at the 2013 AANP National Conference
as we continue to shape the future and celebratethe past!
AANP Announces UpdatedMembership Categories for 2013
The American Association of Nurse Practitioners(AANP) is pleased to share our updated membershipcategories for 2013. Two categories have beenrenamed. The membership categories for 2013 are:� NP (formerly Full) - $125� Associate - $125� Career Starter - $95
� Post Master’s Student (formerly Recognized NPStudent) - $95
� Student - $55� Retired - $55
AANP appreciates your continued support as weexpand our efforts to raise awareness of the valuable roleof the nurse practitioner. We look forward to workingwith you in 2013!
A19
A A
N P
FOR
UM
AANP Urges FDA to ReconsiderHydrocodone Reclassification
Arguing that federal and state authorities already have toolsto prevent abuse of prescription pain medication, AANPurged Food and Drug Administration (FDA) Commis-sioner Margaret Hamburg, MD, to consider the harmfulconsequences of an advisory committee’s recommendationto reclassify medications containing hydrocodone fromSchedule III to Schedule II controlled substances.
In comments submitted on February 1, AANP Presi-dent Angela Golden, DNP, FNP-C, FAANP, pointed outthat several states limit or prohibit NPs from prescribing
Schedule II drugs. “We are deeply concerned that theadvisory committee’s recommendation will have theunintended consequence of denying appropriate andeffective treatment to patients with a legitimate clinicalneed during a critical time in the healing process,” she said.“If all forms of hydrocodone medication were reclassifiedto Schedule II, NPs in the affected states would no longerbe able tomake these treatments available to their patients.”The FDA is expected to review the advisory committee’srecommendation later this year.
American Heart MonthFebruary was American Heart Month, and AANP haspartnered with Million Hearts� to encourage nursepractitioners to help prevent 1 million heart attacks andstrokes over 5 years. In support of this initiative, AANPFellows helped raise awareness about heart disease, thenumber 1 killer of women, on National Wear Red Day�(February 1) during the FAANPWinter Meeting in Dallas.For more information and resources on Million Hearts�,visit aanp.org. Please email [email protected] to shareinformation about or photos of your American HeartMonth events.
Workforce Issues Raise Concernson Capitol Hill
With the health reform law’s deadline to expand insur-ance coverage rapidly approaching, Congress is exploringstrategies to increase and expand the workforce of primarycare providers. At a Senate Health Education Labor andPensions subcommittee hearing on primary care work-force on January 29, Sen Bernie Sanders (I-VT) releaseda report that called for expanding community healthcenters, increasing opportunities for primary careeducation and residencies in community settings ratherthan teaching hospitals, increasing scholarship and loanrepayment opportunities, and expanding the role ofnurse practitioners and physician assistants to boost theprimary care workforce. Sanders argued that Medicaremedical residency funding should be changed to
promote training of primary care physicians, but medicalschool representatives responded that attempts to influ-ence specialty choice through GME payments havefailed.
AANP and other nursing organizations continueto work with members of the House and Senate onpolicies and legislation to increase and improve federalsupport for workforce development, including thegraduate nurse education demonstration created inthe Affordable Care Act, and to eliminate barriers infederal statutes and regulations that prevent nursepractitioners from filling gaps in primary care forwomen, children, and families, particularly in ruralor underserved areas.
A20
A A
N P
FO
RU
M





























