Embed Size (px)
Citation preview

Aging Clin Exp Res, Vol. 23, No. 4 288
Key words: Anxiety, cardiovascular risk, dizziness, family medicine, geriatric medicine.Correspondence: Carsten Kruschinski, MD, MME, Institute of General Practice, Hannover Medical School, Carl-Neuberg-Str.1,30625 Hannover, Germany.E-mail: [email protected] March 23, 2010; accepted in revised form August 20, 2010.First published ahead of print August 27, 2010 as DOI: 10.3275/7231
A three-group comparison of acute-onset dizzy,long-term dizzy and non-dizzy older patientsin primary care
Aging Clinical and Experimental Research
Carsten Kruschinski1, Julia Sczepanek1, Birgitt Wiese2, Alf Breull1, Ulrike Junius-Walker1
and Eva Hummers-Pradier1
1Institute of General Practice, 2Centre of Biometrics and Medical Informatics, Hannover Medical School,Hannover, Germany
ABSTRACT. Background and aims: The hypothesis ofincreased cardiovascular risk contributing to chronicdizziness has been discussed controversially so far. Weinvestigated older patients suffering from acute (<6months), chronic (≥6 months) or no dizziness, in termsof their cardiovascular risk and other impairments.Methods: A cross-sectional three-group comparison of257 patients (65+) presenting at family medicine surgeriesin Germany was performed. Measures of cardiovascularrisk, including overall scores, scores of quality of life(SF-12), activities of daily living (ADL), depression (GDS),dizziness handicap (DHI) and patients’ needs (DiNA), aswell as comorbidity and medication, were compared inunivariate and multivariate logistic regression analysis.Results: In univariate analysis, systolic and diastolicblood pressure were significantly lower in the dizzinessgroups. The overall cardiovascular risk was not increasedin dizzy patients. Anxiety was strongly associated withdizziness, whereas other associations were of marginal im-portance. In multivariate analysis, age (OR 1.10, 95% CI1.03-1.17), female gender (OR 2.07, 95% CI 1.01-4.26)and anxiety (OR 2.50, 95% CI 1.03-6.05) were associatedwith acute dizziness, whereas only female gender was sig-nificant in chronic dizziness (OR 1.96, 95% CI 1.02-3.75). Comparing all dizzy patients with the non-dizzygroup, lower systolic blood pressure was also signifi-cantly associated with dizziness. Conclusions: Resultsfrom our sample suggest that low systolic blood pressureis more important for dizziness in older patients than in-creased cardiovascular risk. Acute-onset and long-termdizzy patients were comparable in many aspects, whichmakes this classification less clinically important.(Aging Clin Exp Res 2011; 23: 288-295)©2011, Editrice Kurtis
INTRODUCTIONDizziness is one of the most frequent complaints of old-
er patients in primary care. In a recent study in Germany,it ranked in the 6th (male) and 7th (female) positions as thereason for encounter in the 65- to 74-year-olds and in the3rd and 4th positions in the over 75-year-olds (1). Pre-ceding community-based and primary care studies haveshown a very heterogenous picture of the causes of dizzi-ness in old age (2-7) and have led some investigators todefine dizziness as a geriatric syndrome (8, 9), associatedwith anxiety and depression, as well as restrictions in dai-ly life and social activities, impairment in the quality of lifeand reduced self-rated health (2, 7-15). Associations ofdizziness with several cardiovascular conditions such as hy-pertension (including antihypertensive therapy (10) andpolypharmacy (8, 9)), diabetes, angina, myocardial in-farction and stroke have also been described (2, 7-13) butdiscussed controversially so far.
Two qualitative studies revealed reduced blood supplyto the brain due to atherosclerosis as a common conceptto explain dizziness within a group of family physicians(FPs) and their patients (16, 17). The hypothesis thatatherosclerosis is caused by increased cardiovascular riskand is responsible for impairments in blood flow anddizziness makes further investigations to clarify the role ofoverall cardiovascular risk necessary. Therefore, in addi-tion to former studies, we aimed to provide complete car-diovascular risk factor measurements and to use estab-lished risk scores in order to evaluate their contributing rolefor acute-onset dizziness as well as dizziness as a chronicgeriatric syndrome.
In addition, by studying dizzy patients, we were inter-ested in their general handicap, quality of life and other“psychological” aspects, in order to estimate the signifi-

cance of their symptoms and to make them more easilycomparable to other studies. Thirdly, in order to integratepatient-centredness into primary care, we also assessedpatients’ needs in a “dizziness study” for the first time.
METHODSStudy design and recruitment of patientsWe performed a cross-sectional study of patients suf-
fering from chronic dizziness and control patients who hadnot suffered from dizziness so far, in the primary care set-ting (20 FPs’ surgeries). Patients were recruited during twoweeks in each surgery. They were included in the study ifthey were at least 65 years of age; they were excluded ifthey suffered from terminal diseases or dementia, orwere unable to fill in questionnaires. Patients were re-cruited consecutively, i.e., all patients were asked at the re-ception desk whether they had been suffering from a sen-sation of dizziness recurrently for a minimum of 6 months.If this was confirmed, patients were included in the“chronic dizziness” group; otherwise they formed thecontrol group.
These participants were compared with a third groupof patients, presenting at their FPs’ offices (21; differentfrom the above) because of acute-onset dizziness as themain reason for encounter (lasting for less than 6 monthsand being a first encounter). FPs asked for their partici-pation, with consecutive recruitment intended over a pe-riod of one year. These patients underwent follow-up at4 weeks and 6 months, the results of which have beenpublished elsewhere (18).
Patients in all three study groups gave their informedconsent. The study was approved by the Ethical Com-mittee of Hannover Medical School (no. 4291) and fol-lowed the ethical rules for human experimentation statedin the Declaration of Helsinki.
Measurements and instrumentsPatients in each group were assessed by a question-
naire containing sociodemographic characteristics, smok-ing behavior, incidence of falls, and type of dizziness (if ap-plicable). Dizziness was classified according to Drach-man and Hart (19), i.e., as vertigo, fainting, unsteadiness,and “other”, such as a feeling of lightheadedness.
A battery of instruments was used to investigate the fol-lowing associations with the symptom of dizziness: SF-12(quality of life (20)), Geriatric Depression Scale (GDS(21)), Activities of Daily Living (ADL (22)), DizzinessHandicap Inventory (DHI (23)) and Dizziness Needs As-sessment (DiNA (24)). Some of the scores were slightlymodified and culturally adapted according to the specificcircumstances in Germany. The scores of the instru-ments as used in our study were interpreted as follows:- SF-12 (51 points or more: “no disability”; 30 or less:
“severe disability”),- GDS (less than 6 points: “no depression”; 6 or more and
less than 11: “mild to moderate depression”; 11 ormore: “severe depression”),
- DHI/modified (maximum score, i.e., highest handicap:88 points [physical: 16, functional: 36, emotional: 36]),
- ADL/modified (maximum score, i.e., lowest handicap:42 points [instrumental (iADL): 22, ADL: 16, conti-nence: 4]).
The DiNA consists of six-point Likert scale items, “1”representing low and “6” high values, respectively. Theanxiety and worry items (dichotomous response: yes/no)correspond to an established screening instrument for anx-iety and phobia (25): “In the past four weeks, have youbeen compromised by anxiety or a feeling of being emo-tionally out of balance (2nd item: compromised by worry)?”
In addition, during or close to the actual encounter (i.e.,time-point of inclusion), the following measures weretaken: height, weight, systolic and diastolic blood pressure,cholesterol (total, HDL) and HbA1c (if diabetic). If morethan one value had been documented, means were cal-culated. We used established and validated scores, the Ger-man ARRIBA (26) and the modified Framingham scoreaccording to Anderson (27) (used here without consider-ation of ECG changes for hypertrophy of the heart) to cal-culate overall cardiovascular 10-year risk (defined as car-diovascular incidence such as myocardial infarction orstroke). The Framingham score relies on the diagnosis ofdiabetes as being “present”, whereas ARRIBA includesHbA1c values in diabetic patients. ARRIBA also con-siders manifest atherosclerosis defined as coronary heartdisease, TIA/stroke or claudicatio and, in these cases, au-tomatically defines the risk as 50%.
Each FP was interviewed (acute group) or asked to pro-vide all diagnoses and actual medication prescribed foreach patient (chronic and control groups). Due to thesedifferent procedures, the number of most of the diagnoseswas higher in the acute group, as diagnoses had been ac-tively requested according to a complete list of all im-portant groups of diagnoses. The FPs who recruited thechronic and control patients sent the patient-related di-agnoses by mail or fax, without having “checked” if allpossible diagnoses had been taken into account.
If necessary, patients, FPs or practice nurses werecontacted by phone to provide missing data. Taking theabove-mentioned instruments together (SF-12, GDS,DHI, ADL), only n=285/16,260 single final answerscould not be completed (1.75%). As exemplified weight-ed scores did not result in obvious differences, we reliedon rough scores for further statistical analysis.
Statistical analysisDescriptive statistics were presented as mean values or
absolute and relative frequencies. For two-group com-parisons, the independent two-tailed Student’s t-test wasused for means and the chi-square test for proportions. Tocompare three groups (acute and chronic dizziness, con-
C. Kruschinski, J. Sczepanek, B. Wiese et al.
289 Aging Clin Exp Res, Vol. 23, No. 4
trols), variance analysis (one-way ANOVA) was per-formed. Otherwise, for categorical variables, the chi-square test was applied.
For multivariate analysis, logistic regression was per-formed with acute dizziness, chronic dizziness or bothcombined (acute or chronic dizziness) as well as vertigo asthe binary outcomes, including relevant indicators of car-diovascular risk, psychological impact, age and gender ascovariates. The covariates (except age, blood pressure andGDS scores) were coded into dichotomous factors (gen-der; polypharmacy, defined as 5 or more drugs; anxiety)or factors with a maximum of three categories (number ofantihypertensive drugs [0, 1, 2 or more]). For each vari-able, the odds ratio (OR) is presented, including 95% con-fidence intervals (CI).
p-values of less than 0.05 were considered statisti-cally significant. All data were analysed with PASW statis-tics software, version 17.0 (SPSS Inc., Chicago, IL).
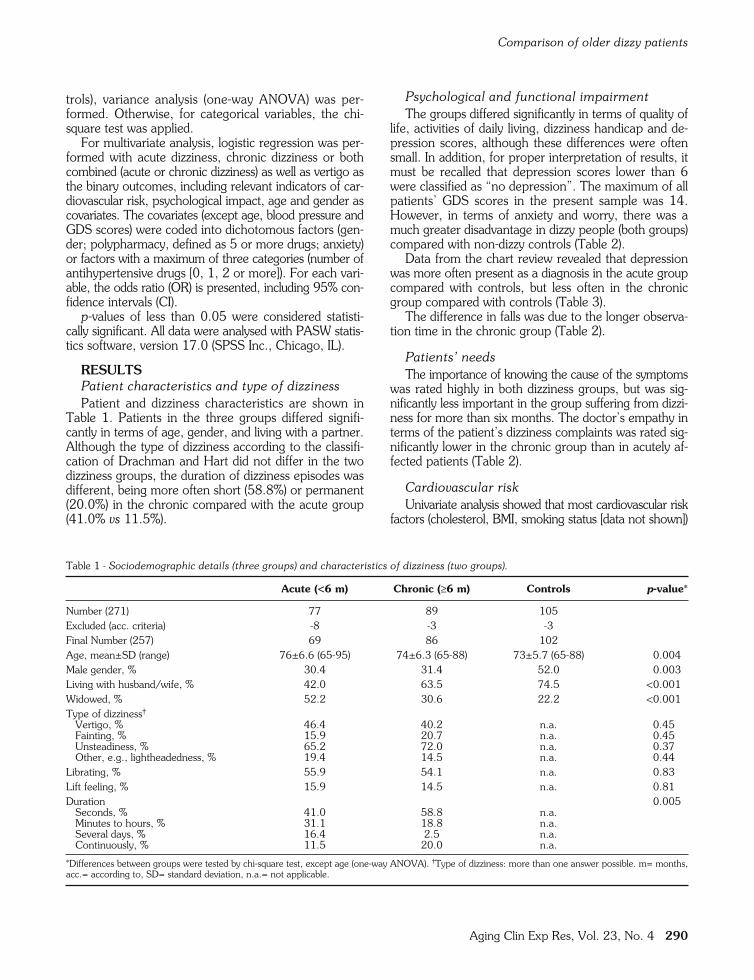
RESULTSPatient characteristics and type of dizzinessPatient and dizziness characteristics are shown in
Table 1. Patients in the three groups differed signifi-cantly in terms of age, gender, and living with a partner.Although the type of dizziness according to the classifi-cation of Drachman and Hart did not differ in the twodizziness groups, the duration of dizziness episodes wasdifferent, being more often short (58.8%) or permanent(20.0%) in the chronic compared with the acute group(41.0% vs 11.5%).
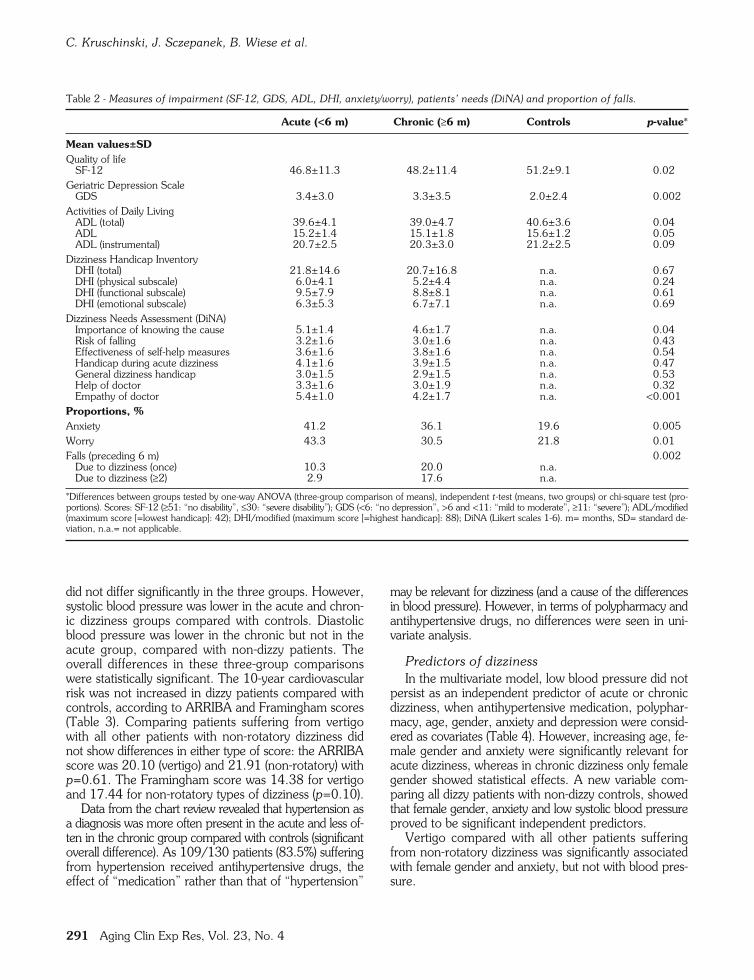
Psychological and functional impairmentThe groups differed significantly in terms of quality of
life, activities of daily living, dizziness handicap and de-pression scores, although these differences were oftensmall. In addition, for proper interpretation of results, itmust be recalled that depression scores lower than 6were classified as “no depression”. The maximum of allpatients’ GDS scores in the present sample was 14.However, in terms of anxiety and worry, there was amuch greater disadvantage in dizzy people (both groups)compared with non-dizzy controls (Table 2).
Data from the chart review revealed that depressionwas more often present as a diagnosis in the acute groupcompared with controls, but less often in the chronicgroup compared with controls (Table 3).
The difference in falls was due to the longer observa-tion time in the chronic group (Table 2).
Patients’ needsThe importance of knowing the cause of the symptoms
was rated highly in both dizziness groups, but was sig-nificantly less important in the group suffering from dizzi-ness for more than six months. The doctor’s empathy interms of the patient’s dizziness complaints was rated sig-nificantly lower in the chronic group than in acutely af-fected patients (Table 2).
Cardiovascular riskUnivariate analysis showed that most cardiovascular risk
factors (cholesterol, BMI, smoking status [data not shown])
Comparison of older dizzy patients
Aging Clin Exp Res, Vol. 23, No. 4 290
Acute (<6 m) Chronic (≥6 m) Controls p-value*
Number (271) 77 89 105Excluded (acc. criteria) -8 -3 -3Final Number (257) 69 86 102Age, mean±SD (range) 76±6.6 (65-95) 74±6.3 (65-88) 73±5.7 (65-88) 0.004Male gender, % 30.4 31.4 52.0 0.003Living with husband/wife, % 42.0 63.5 74.5 <0.001Widowed, % 52.2 30.6 22.2 <0.001Type of dizziness†
Vertigo, % 46.4 40.2 n.a. 0.45Fainting, % 15.9 20.7 n.a. 0.45Unsteadiness, % 65.2 72.0 n.a. 0.37Other, e.g., lightheadedness, % 19.4 14.5 n.a. 0.44
Librating, % 55.9 54.1 n.a. 0.83Lift feeling, % 15.9 14.5 n.a. 0.81Duration 0.005
Seconds, % 41.0 58.8 n.a.Minutes to hours, % 31.1 18.8 n.a.Several days, % 16.4 2.5 n.a.Continuously, % 11.5 20.0 n.a.
*Differences between groups were tested by chi-square test, except age (one-way ANOVA). †Type of dizziness: more than one answer possible. m= months,acc.= according to, SD= standard deviation, n.a.= not applicable.
Table 1 - Sociodemographic details (three groups) and characteristics of dizziness (two groups).
did not differ significantly in the three groups. However,systolic blood pressure was lower in the acute and chron-ic dizziness groups compared with controls. Diastolicblood pressure was lower in the chronic but not in theacute group, compared with non-dizzy patients. Theoverall differences in these three-group comparisonswere statistically significant. The 10-year cardiovascularrisk was not increased in dizzy patients compared withcontrols, according to ARRIBA and Framingham scores(Table 3). Comparing patients suffering from vertigowith all other patients with non-rotatory dizziness didnot show differences in either type of score: the ARRIBAscore was 20.10 (vertigo) and 21.91 (non-rotatory) withp=0.61. The Framingham score was 14.38 for vertigoand 17.44 for non-rotatory types of dizziness (p=0.10).
Data from the chart review revealed that hypertension asa diagnosis was more often present in the acute and less of-ten in the chronic group compared with controls (significantoverall difference). As 109/130 patients (83.5%) sufferingfrom hypertension received antihypertensive drugs, theeffect of “medication” rather than that of “hypertension”
may be relevant for dizziness (and a cause of the differencesin blood pressure). However, in terms of polypharmacy andantihypertensive drugs, no differences were seen in uni-variate analysis.
Predictors of dizzinessIn the multivariate model, low blood pressure did not
persist as an independent predictor of acute or chronicdizziness, when antihypertensive medication, polyphar-macy, age, gender, anxiety and depression were consid-ered as covariates (Table 4). However, increasing age, fe-male gender and anxiety were significantly relevant foracute dizziness, whereas in chronic dizziness only femalegender showed statistical effects. A new variable com-paring all dizzy patients with non-dizzy controls, showedthat female gender, anxiety and low systolic blood pressureproved to be significant independent predictors.
Vertigo compared with all other patients sufferingfrom non-rotatory dizziness was significantly associatedwith female gender and anxiety, but not with blood pres-sure.
C. Kruschinski, J. Sczepanek, B. Wiese et al.
291 Aging Clin Exp Res, Vol. 23, No. 4
Acute (<6 m) Chronic (≥6 m) Controls p-value*
Mean values±SDQuality of life
SF-12 46.8±11.3 48.2±11.4 51.2±9.1 0.02Geriatric Depression Scale
GDS 3.4±3.0 3.3±3.5 2.0±2.4 0.002Activities of Daily Living
ADL (total) 39.6±4.1 39.0±4.7 40.6±3.6 0.04ADL 15.2±1.4 15.1±1.8 15.6±1.2 0.05ADL (instrumental) 20.7±2.5 20.3±3.0 21.2±2.5 0.09
Dizziness Handicap InventoryDHI (total) 21.8±14.6 20.7±16.8 n.a. 0.67DHI (physical subscale) 6.0±4.1 5.2±4.4 n.a. 0.24DHI (functional subscale) 9.5±7.9 8.8±8.1 n.a. 0.61DHI (emotional subscale) 6.3±5.3 6.7±7.1 n.a. 0.69
Dizziness Needs Assessment (DiNA)Importance of knowing the cause 5.1±1.4 4.6±1.7 n.a. 0.04Risk of falling 3.2±1.6 3.0±1.6 n.a. 0.43Effectiveness of self-help measures 3.6±1.6 3.8±1.6 n.a. 0.54Handicap during acute dizziness 4.1±1.6 3.9±1.5 n.a. 0.47General dizziness handicap 3.0±1.5 2.9±1.5 n.a. 0.53Help of doctor 3.3±1.6 3.0±1.9 n.a. 0.32Empathy of doctor 5.4±1.0 4.2±1.7 n.a. <0.001
Proportions, %Anxiety 41.2 36.1 19.6 0.005Worry 43.3 30.5 21.8 0.01Falls (preceding 6 m) 0.002
Due to dizziness (once) 10.3 20.0 n.a.Due to dizziness (≥2) 2.9 17.6 n.a.
*Differences between groups tested by one-way ANOVA (three-group comparison of means), independent t-test (means, two groups) or chi-square test (pro-portions). Scores: SF-12 (≥51: “no disability”, ≤30: “severe disability”); GDS (<6: “no depression”, >6 and <11: “mild to moderate”, ≥11: “severe”); ADL/modified(maximum score [=lowest handicap]: 42); DHI/modified (maximum score [=highest handicap]: 88); DiNA (Likert scales 1-6). m= months, SD= standard de-viation, n.a.= not applicable.
Table 2 - Measures of impairment (SF-12, GDS, ADL, DHI, anxiety/worry), patients’ needs (DiNA) and proportion of falls.

than six months, whereas only 5% reported dizzinesslasting less than one month.
We therefore examined both acute-onset and chroni-cally affected patients, to learn more about their differ-ences. Differences were seen in the duration of dizzinessattacks, and the higher percentage of shorter episodes inthe chronic group may indicate the higher frequency ofbenign paroxysmal positional vertigo, which has been de-scribed as a frequent cause of dizziness in old age (30).However, in our study, the underlying causes of dizzinesswere not investigated further. Many other differencesbetween acutely and chronically affected patients in oursample may be interpreted as “slight” and of minor clin-ical importance such as the overall low depression scores.In some other studies, depression occurred more fre-quently, and quality of life has been shown to be muchmore affected by dizziness (11, 12). This may reflectdifferent sampling strategies, as the recruitment of ourchronic group, for example, was based on a relatively low“threshold”. It is of interest that, in our study, the patients’need to know the cause of the symptom and the ratingsof their doctor’s empathy was relatively high in both
DISCUSSIONIn the present study, the two groups of acutely and
chronically affected dizzy patients differed only slightlyin many of the parameters examined. The overall car-diovascular risk and established risk factors such ascholesterol were not able to explain differences be-tween dizzy and non-dizzy control patients. Instead, lowsystolic blood pressure was significantly associatedwith dizziness. Some variables from former studieswere also verified as associated factors, i.e., increasingage, female gender and anxiety. For the first time, weintegrated patients’ needs and found that the wish toknow the causes of the illness was rated as very im-portant.
In former publications, most authors examined pa-tients with either acute or chronic dizziness. However, def-initions of “chronic” varied between two months (28)and five years (29) and seemed to be based on pragmat-ic reasons rather than validated concepts. One-third ofpeople over 65 suffered from dizziness in a population-based questionnaire study in Scotland (10). Eighty percentof patients reported having had such symptoms for more
Comparison of older dizzy patients
Aging Clin Exp Res, Vol. 23, No. 4 292
Acute (<6 m) Chronic (≥6 m) Controls p-value*
Cardiovascular risk, meansBody height, cm, mean±SD n.i. 164.2±9.0 168.9±8.4 <0.001Body weight, kg, mean±SD n.i. 76.2±14.9 78.1±14.5 0.38Body mass index, kg/m2, mean±SD n.i. 28.23±4.91 27.27±4.19 0.16Systolic blood pressure, mmHg, mean±SD 135.2±13.2 132.7±17.1 139.9±15.8 0.007Diastolic blood pressure, mmHg, mean±SD 79.9±7.7 76.3±8.0 80.0±8.3 0.003Cholesterol (total), mg/dL, mean±SD 211.1±44.1 212.1±41.5 214.4±41.3 0.88Cholesterol (HDL), mg/dL, mean±SD 63.7±18.6 62.1±17.7 61.4±17.5 0.77HbA1c (diabetic patients), %, mean±SD 6.2±1.3 6.2±0.8 6.5±1.2 0.41
ARRIBA score†, %, 10-y risk ±SD 23.5±19.1 20.0±16.4 23.2±16.5 0.44Framingham score, %, 10-y risk ±SD 13.2±5.03 17.2±6.31 17.9±6.4 0.038Diagnoses‡, %
Hypertension 74.6 54.5 60.5 0.047Coronary heart disease 27.9 14.0 14.9 0.046Heart valve disease 7.4 5.8 3.0 0.42Heart failure 13.2 10.5 9.9 0.78Arrhythmia 16.2 19.8 9.9 0.16TIA 2.9 2.4 3.0 0.96Stroke 4.4 3.5 4.0 0.96
Neurological disorder 25.4 8.6 7.6 0.003Polyneuropathy 7.4 2.9 1.3 0.13Migraine 7.4 2.9 3.8 0.41
Psychological disorder 38.8 17.1 15.2 0.001Depression 26.5 2.9 6.3 <0.001Phobia 8.8 1.4 0.0 0.006
MedicationNo. of drugs (acc. doctor), mean±SD 4.4±3.1 4.9±3.6 4.0±2.7 0.15No. of antihypertensive drugs, mean±SD 1.2±1.3 1.4±1.2 1.3±1.2 0.65
*Differences between the groups tested by one-way ANOVA (three groups, mean values), independent t-test (two groups, mean values) or chi-square test (pro-portions). †Scores based on lower patient numbers, due to age limitations and several missing values: calculation of ARRIBA limited to patients <83 and Fram-ingham score to patients <74 years of age. Total numbers for cardiovascular risk scores: 182 (ARRIBA) and 100 (Framingham). ‡Different methods of dataretrieval: each diagnosis was actively explored in acute group. m= months, SD= standard deviation, n.i.= not investigated, y= years, acc.= according to.
Table 3 - Cardiovascular risk, diagnoses and medication.

groups. This was comparable to one of our other studies(24) and has implications for counselling patients in sucha way that causes are clearly explained, in order to preventmisunderstandings and “wrong” expectations.
Our study is one of others investigating associations ofcardiovascular comorbidity and a spectrum of other fac-tors within the complex entity of dizziness in old age (2,7-13). However, in the past, factors not consistently at-tributed to the problem of dizziness, e.g., diabetes (history-based, without HbA1c having been measured) were eitherconsidered relevant (9) or not identified as being associated(2, 11). We therefore aimed at integrating all factors in acardiovascular risk score by providing measurements in ad-dition to using reported diagnoses, and considered that thiswas suitable in order to examine the concept ofatherosclerosis causing “circulation” problems (16) or a“central vascular disease” (2). However, no such associ-
ation could be found when comparing patients with dif-ferent durations of dizziness or different types of dizziness(vertigo or non-rotatory), although vertigo was clearlyassociated with stroke in an earlier study (31). One ex-planation for this discrepancy may be seen in the fact thatscreening questions for types of dizziness and answerswere culturally different.
Our results of low (systolic) blood pressure contradictsome other studies, although values have often been re-ported to be slightly lower in dizzy groups comparedwith controls (8, 11). A fall in blood pressure caused bypostural changes also often causes symptoms in dizzycompared with non-dizzy patients (2, 9) and one study im-pressively demonstrated that lower blood pressure valuesas such were more frequently related to feelings of faint-ing and dizziness (32). A pre-existing diagnosis of car-diovascular disease and hypertension has recently been de-
C. Kruschinski, J. Sczepanek, B. Wiese et al.
293 Aging Clin Exp Res, Vol. 23, No. 4
Odds ratio 95% CI 95% CI p-value*(lower) (upper)
Acute dizzinessAge 1.10 1.03 1.17 0.002Female gender 2.07 1.01 4.26 0.047Systolic blood pressure 0.97 0.94 1.00 0.06Diastolic blood pressure 1.04 0.98 1.09 0.18Antihypertensive drug (1) 0.99 0.42 2.33 0.98Antihypertensive drugs (≥2) 0.66 0.22 1.95 0.45Polypharmacy 1.48 0.62 3.53 0.38Anxiety 2.50 1.03 6.05 0.04Depression (GDS Score) 1.05 0.91 1.22 0.50
Chronic dizzinessAge 1.02 0.96 1.07 0.54Female gender 1.96 1.02 3.75 0.04Systolic blood pressure 0.98 0.96 1.00 0.10Diastolic blood pressure 0.97 0.93 1.02 0.20Antihypertensive drug (1) 1.21 0.56 2.60 0.64Antihypertensive drugs (≥2) 1.15 0.46 2.90 0.77Polypharmacy 0.87 0.41 1.86 0.72Anxiety 2.10 0.92 4.75 0.08Depression (GDS Score) 1.08 0.95 1.23 0.24
Combined acute and chronicAge 1.05 1.00 1.10 0.05Female gender 1.97 1.13 3.42 0.02Systolic blood pressure 0.98 0.96 1.00 0.03Diastolic blood pressure 1.00 0.96 1.04 0.91Antihypertensive drug (1) 1.11 0.56 2.18 0.77Antihypertensive drugs (≥2) 0.87 0.38 1.99 0.74Polypharmacy 1.08 0.55 2.10 0.83Anxiety 2.20 1.10 4.43 0.03Depression (GDS Score) 1.98 0.96 1.21 0.20
VertigoFemale gender 2.61 1.18 5.77 0.02Systolic blood pressure 1.00 0.97 1.03 0.93Diastolic blood pressure 1.03 0.97 1.09 0.34Antihypertensive drug (1) 1.42 0.59 3.40 0.43Antihypertensive drugs (≥2) 1.94 0.66 5.69 0.23Polypharmacy 1.16 0.50 2.71 0.73Anxiety 2.67 1.15 6.18 0.02Depression (GDS Score) 0.89 0.78 1.01 0.07
n
Table 4 - Logistic regression, including relevant indicators of cardiovascular risk, medication, anxiety screening, depression scores, ageand gender for acute, chronic dizziness and combined acute and chronic dizziness as well as vertigo as binary outcomes.

scribed to be associated with dizziness in a representativesecondary data analysis (7). As cardiovascular risk, towhich hypertension would contribute, was not increasedin our dizzy vs control groups, the concept of low systolicblood pressure may be a more plausible explanationthan atherosclerosis. In addition, multivariate analysisshowed that antihypertensive medication was not inde-pendently associated with dizziness.
Limitations of our study are given by the fact that co-diagnoses were documented in different ways in theacute and chronic/control groups. The differences musttherefore be interpreted with caution, and these vari-ables were not included in multivariate analysis. Cardio-vascular measurements were not standardized either,e.g., the procedure of taking blood pressure values.However, blood pressure measurements - even whenstandardised - are also known to vary during the day. Lab-oratory measurements of cholesterol and HbA1c may beconsidered more reliable, although their values, for in-stance, depend on medication.
As regards external validity (representativeness), itmust be noted that consecutive recruitment had beenintended in all three groups. However, we cannot becompletely sure that some patients were “missed” bydoctors (acute group) or nurses at the reception desk(chronic group, control group). In addition, patients whorefused participation were not analysed separately. Thestrengths of this study are that, for the first time, real andcomplete measurements for calculating cardiovascularrisk profiles were taken, and that we did not rely solely ondiagnoses taken from patients’ history.
CONCLUSIONSOur results show that the concept of general
atherosclerosis as causing “circulation” problems seemsless appropriate to describe dizziness in old age than a sin-gle cardiovascular factor (i.e., low blood pressure) and oth-er well described associated factors such as increasing age,female gender and anxiety. Nor does it seem adequate todistinguish between acute and chronic dizzy patients inmany of the aspects examined. However, our study con-firms the concept of a geriatric syndrome, in which notonly a broad spectrum of psychosocial factors such as anx-iety but also patients’ perspectives should be taken into ac-count simultaneously. For future research, more prospec-tive studies investigating causative roles instead of asso-ciations would be of value, and meta-analyses of existingheterogeneous study results in large numbers of patientswould be helpful, for proper interpretation of data.
ACKNOWLEDGEMENTSThe authors thank all participating patients and their family physi-
cians. The study was funded by the German Federal Ministry of Edu-cation and Research (grant no. 01GK0611). Conflict of interest: Theauthors declare that they have no competing interest.
Comparison of older dizzy patients
Aging Clin Exp Res, Vol. 23, No. 4 294
REFERENCES1. Kühlein T, Laux G, Gutscher A, Szecsenyi J. Kontinuierliche
Morbiditätsregistrierung in der Hausarztpraxis - vomBeratungsanlass zum Beratungsergebnis. München: Urban &Vogel, 2008.
2. Colledge NR, Barr-Hamilton RM, Lewis SJ, Sellar RJ, Wilson JA.Evaluation of investigations to diagnose the cause of dizziness inelderly people: a community based controlled study. BMJ 1996;313: 788-92.
3. Neuhauser HK, Radtke A, von Brevern M, Lezius F, Feldmann M,Lempert T. Burden of dizziness and vertigo in the community.Arch Intern Med 2008; 168: 2118-24.
4. Lawson J, Fitzgerald J, Birchall J, Aldren CP, Kenny RA.Diagnosis of geriatric patients with severe dizziness. J Am GeriatrSoc 1999; 47: 12-7.
5. Katsarkas A. Dizziness in aging: the clinical experience. Geriatrics2008; 63: 18-20.
6. Sloane PD, Coeytaux RR, Beck RS, Dallara J. Dizziness: state ofthe science. Ann Intern Med 2001; 134: 823-32.
7. Maarsingh OR, Dros J, Schellevis FG, van Weert HC, Bindels PJ,Horst HE. Dizziness reported by elderly patients in family practice:prevalence, incidence, and clinical characteristics. BMC FamPract 2010; 11: 2.
8. Tinetti ME, Williams CS, Gill TM. Dizziness among older adults: apossible geriatric syndrome. Ann Intern Med 2000; 132: 337-44.
9. Kao AC, Nanda A, Williams CS, Tinetti ME. Validation of dizzi-ness as a possible geriatric syndrome. J Am Geriatr Soc 2001;49: 72-5.
10. Colledge NR, Wilson JR, Macintyre CCA, MacLennan WJ. Theprevalence and characteristics of dizziness in an elderly commu-nity. Age Ageing 1994; 7: 1-8.
11. Tinetti ME, Williams CS, Gill TM. Health, functional, and psy-chological outcomes among older persons with chronic dizziness.J Am Geriatr Soc 2000; 48: 417-21.
12. Grimby A, Rosenhall U. Health-related quality of life and dizzinessin old age. Gerontology 1995; 41: 286-98.
13. Sloane PD. Dizziness in primary care: results from the NationalAmbulatory Medical Care Survey. J Fam Pract 1989; 29: 33-8.
14. Gopinath B, McMahon CM, Rochtchina E, Mitchell P. Dizzinessand vertigo in an older population: the Blue Mountains prospec-tive cross-sectional study. Clin Otolaryngol 2009; 34: 552-6.
15. Hsu L-C, Hu H-H, Wong W-J, Wang S-J, Luk Y-O, Chern C-M.Quality of life in elderly patients with dizziness: analysis of theShort-Form Health Survey in 197 patients. Acta Otolaryngol2005; 125: 55-9.
16. Kruschinski C, Schweizer S, Hummers-Pradier E, Theile G. “Avery broad field“: concepts of general practitioners for dizzi-ness. Z Allg Med 2009; 85: 377-82.
17. Kruschinski C, Theile G, Dreier S, Hummers-Pradier E. Thepriorities of elderly dizzy patients suffering from dizziness: aqualitative study. Eur J Gen Pract 2010; 16: 6-11.
18. Sczepanek J, Wiese B, Hummers-Pradier E, Kruschinski C.Newly diagnosed incident dizziness of older patients: a follow-upstudy in primary care. BMC Fam Pract 2011; 12: 58.
19. Drachman DA, Hart CW. An approach to the dizzy patient.Neurology 1972; 22: 323-34.
20. Ware JE, Kosinski M, Keller SD. A 12-Item Short-Form HealthSurvey: construction of scales and preliminary tests of reliabilityand validity. Med Care 1996; 34: 220-33.
21. Shiekh JI, Yesavage JA. Geriatric Depression Scale (GDS): recentevidence and development of a shorter version. In Brink T (Ed)

Clinical Gerontology: A Guide to Assessment and Intervention.New York: Howarth Press, 1986: 165-73.
22. Fillenbaum GG. Screening the elderly. A brief instrumental ac-tivities of daily living measure. J Am Geriatr Soc 1985; 33:698-706.
23. Jacobsen GP, Newman CW. The development of the DizzinessHandicap Inventory. Arch Otolaryngol Head Neck Surg 1990;116: 424-7.
24. Kruschinski C, Klaassen A, Breull A, Broll A, Hummers-PradierE. Priorities of elderly dizzy patients in general practice: findingsand psychometric properties of the “Dizziness Needs Assessment”(DiNA). Z Gerontol Geriatr 2010; 43: 317-23.
25. Spitzer RL, Williams, JB, Kroenke K et al. Utility of a new pro-cedure for diagnosing mental disorders in primary care. ThePRIME-MD 1000 study. JAMA 1994; 272: 1749-56.
26. Krones T, Keller H, Sönnichsen A et al. Absolute cardiovasculardisease risk and shared decision making in primary care: a ran-domized controlled trial. Ann Fam Med 2008; 6: 218-27.
27. Anderson KM, Wilson PW, Odell PM, Kannel WB. An updatedcoronary risk profile. A statement for health professionals.Circulation 1991; 83: 356-62.
28. Yardley L, Donovan-Hall M, Smith HE, Walsh BM, Mullee M,Bronstein AM. Effectiveness of primary care-based vestibularrehabilitation for chronic dizziness. Ann Intern Med 2004; 141:598-605.
29. Nazareth I. Dizziness. In Jones R, Britten N, Culpepper L et al(Eds) Oxford Textbook of Primary Medical Care. New York:Oxford University Press, 2005: Vol. 2, 1058-63.
30. Hansson EE, Mansson N-O, Hakansson A. Benign paroxysmalpositional vertigo among elderly patients in primary care.Gerontology 2005; 51: 386-9.
31. Grimley Evans J. Transient neurological dysfunction and risk ofstroke in an elderly English population: the different significance ofvertigo and non-rotatory dizziness. Age Ageing 1990; 19: 43-9.
32. Wessely S, Nickson J, Cox B. Symptoms of low blood pressure:a population study. BMJ 1990; 301: 362-5.
C. Kruschinski, J. Sczepanek, B. Wiese et al.
295 Aging Clin Exp Res, Vol. 23, No. 4