Embed Size (px)
Citation preview
UNI CEF, 2014
A SYSTEMATIC REVIEW OF PARENTING PROGRAMMES FOR YOUNG CHILDREN IN LOW AND MIDDLE INCOME COUNTRIES
AnextensiveresearchreviewofEarlyChildhoodDevelopment
parentingprogrammes,inlowandmiddle-incomecountries.The
reviewaddressestheknowledgegapandprovidesevidencefor
betterprogrammingforchildrenandfamilies.

ASystematicReviewofParentingProgrammesforYoungChildren
PiaRebelloBritto,PhDUNICEF
L.AngelicaPonguta,PhD,MPHYaleChildStudyCenter
ChinReyes,PhDYaleChildStudyCenter
RomillaKarnati,PhDConsultant,UNICEF
Dateofpublication2015
FrancesAboud,PhD McGillUniversityMarcBornstein,PhD Eunice Kennedy ShriverNational Institute
ofChildHealthandHumanDevelopmentPatriceEngle,PhD CalPolyUniversitySharonLynnKagan,PhD ColumbiaUniversityCostasMeghir,PhD YaleUniversityKylePruett,MD YaleUniversity
Funder:UNICEF
AcknowledgementsAdrian Cerezo,N. ShemrahFallon, SaimaGowani, KatherineLong,Kerrie Proulx,AnjaliRodriguesandAlexandraSoare.

CONTENTS ACRONYMLIST
EXECUTIVESUMMARY 1
Justification 1
Background 1
SummaryofResults 3
DiscussionandSummaryofthe 10
Recommendations 10
ProgrammaticRecommendations: 14
Chapter1:Introduction 15
1.1 Introduction 15
1.2 ParentsandParenting 16
1.3 DatafromtheMultipleIndicatorClusterSurvey 18
1.4 OverviewofParentingProgrammes 19
1.5 Studyobjectivesandresearchquestions 24
1.6Briefdescriptionofchaptersinthepresentreview 25
Chapter2:StudyMethods 27
2.1Literaturesearch 27
2.2Screeningcriteriaforrelevanceandeligibility 31
2.3ScreeningProcedures 33
2.4Dataextraction 36
2.5Studyevaluation 36
2.6PublicationBias 37
Chapter3: Results 39
3.1DescriptiveResults 39
3.2ProgrammeResultsbyChildandParentOutcomes 42
Chapter4:Discussion 95
4.1WhatWorksinParentingProgrammes 96
4.2Knowledgegaps 103
4.3EquitythroughParenting 107
References 108
Appendix1 145

ACRONYMLIST
ACEV-MotherandChildFoundation
ARI-AcuteRespiratoryInfection
CDW-ChildDevelopmentWorker
CONIN-CorporationforChildhoodNutrition
CRC-ConventionsontheRightsoftheChild
DHE-DentalHealthEducation
ECC–EarlyChildhoodCaries
ECD-EarlyChildhoodDevelopment
ENA-EssentialNutritionActions
IMCI-IntegratedManagementforChildhoodIllness
ITI-InternationalTrachomaInitiative
LMIC-Lowandmiddleincomecountries
MDG’s-MillenniumDevelopmentGoals
MICS-MultipleIndicatorClusterSurvey
MOCEP–MotherChildEducation
Programme
MTSP-MediumTermStrategicPlan
PICO–PopulationInterventionComparisonOutcomes
PMTCT–PreventionofMothertoChildTransmission
PROBIT-PromotionofBreastfeedingInterventionTrial
RCT–RandomControlTrials
RUTF-Ready-to-usetherapeuticfoods
SAFE-SurgeryforTrichiasis,FacialCleanlinessandEnvironmentalImprovement
TEEP–TurkeyEarlyEnrichmentProject
UNICEF-UnitedNationsChildren’s Fund
WHO-WorldHealthOrganization
EXECUTIVESUMMARY
1
JUSTIFICATIONTheConventionontheRightsoftheChild(CRC)andamplescientificevidenceacknowledge
thatparentingisoneofthestrongestinfluencesonchildren,particularly,duringtheirearly
childhoodyears.Earlylifeexperiencesformthefoundationforbrainarchitectureand
scientistsnowknowthatamajoringredientinthisbraindevelopmentprocessisthe
interactionbetweenchildrenwiththeirparentsorcaregivers(CenterontheDeveloping
Child,HarvardUniversity,2015). Despitethiswidespreadrecognition,thereareseveralgaps
inourknowledgeofwhatworks,topromotepositiveparentingpractices,particularlyin
vulnerablecontexts.DatastemmingfromtheMultipleIndicatorClusterSurvey(MICS),from
LowandMiddleIncomeCountries(LMIC),suggestthatatbest,only,halfoftheparents
surveyedengageinparentingbehaviorsthatareconsideredpositiveandbeneficialforEarly
ChildhoodDevelopment(ECD).Toaddresstheseprogrammaticandknowledgegapsin
parentingpractices,UNICEFcommissionedasystematicreviewoftheliteraturetoaddress
gapsintheunderstandingofwhatpromoteseffective,sensitiveandresponsivechildrearing
andcaringpracticesthroughECDparentingprogrammesandinterventionsindifferent
national,communityandlocalcontexts. Thepurposeofthissystematicresearchreviewwas
toevaluatetheefficacyofEarlyChildhoodDevelopment(ECD)parentingprogrammesand
examinetheelementsofprogrammingthatmaximizeitsbenefitstoyoungchildrenand
theirfamilies.
BACKGROUND
Whenababyisborn,thebillionsofbraincellsareopentosculptingitselfinresponseto
earlyexperiences.Tofunction,braincellsmustbeorganizedintonetworksthatrequire
trillionsofconnections,whichdependontheinteractionbetweengenesandthe
environment. Thatoptimalenvironmentiscreatedthroughnurturingenvironmentssuch
aspositiveparenting(NationalScientificCouncilontheDevelopingChild,2004).These
2
earlyconnectionsshapebraincircuitsandlaythefoundationforthedevelopmental
outcomelater.Whilegenesprovidetheblueprintfordevelopment,itistheinteraction
withtheenvironmentthatultimatelyshapesit.Theearlyyearsprovideacriticalwindowof
opportunitybutalsopresenttheriskofvulnerabilitywhenneglected.Parents,key
caregiversandfamilieshavetheinfluencingpowertodetermineachild’schancesfor
survivalanddevelopment. Rapidstridesmadebyyoungchildrenacrossalldomainsof
developmentandlearningarefosteredandsupportedthroughparents’practices,
attitudes,knowledgeandresources.Themulti-disciplinaryandtransnationalliteratureon
parentingclearlyindicatesthatparentsareoneofthemostinfluentialfactorsinchildren’s
development(Bornstein,2002;BradleyandCorwyn,2005;Rogoff,2003;Whitingand
Edwards,1998).
Poorparentingcanalterbrainchemistryandarchitectureinwaysthatreversepositive
development,notjustfortheimmediategenerationbutsubsequentgenerationsaswell
(NationalScientificCouncilontheDevelopingChild,2010).Recentworkonadverse
childhoodexperienceshasnotedtheinfluenceofriskfactorsthatcanbemediatedby
contingentandsensitiveparenting(Felitti&Anda,2008).Therefore,competentparenting
asaprotectivefactorinmoderatingriskfactorshasbeenrecognized. Parentingasa
characteristicofprimatesislinkedtotheevolutionofourspeciesandtheintergenerational
transmissionofculture,valuesandtraditions.Undeniably,parentsandkeycaregiverscould
beconsideredtheforemostandstrongestinfluenceonearlychilddevelopment(Shonkoff
&Phillips,2000).However,parentsorcaregivers,andfamiliesoftenneedsupportinbeingabletofulfilltheir
role,especially,iftheyareburdenedbyriskfactors. TheCRCwhilerecognizingthatparents
andkeycaregivershavetheprimaryresponsibilityofrearingchildren,alsorecognizethat
theyrequireassistanceincreatingthoseoptimalenvironmentsforpositivechild
development.AspertheCRC,countriesareobligatedtosupportcaregiversinthisrole
(Hodgkin&Newell,2007).
5
Parentswhoareequippedwiththeknowledgeandskillstheyneedtopromotetheiryoung
child’shealthanddevelopmentareapotentiallypowerfulfactorinmitigatingtherisksof
poverty. Thequestionthenis: whatdoestheempiricalevidencesayabouttheefficacyof
ECDparentingprogrammesinLMIC,apartoftheworldthathasreceivedlittleattentioninthescientific
literature?ThisresearchpaperprovidesanextensiveandrigoroussystematicreviewofECDparenting
programmesconductedinLMIC,addressingtheknowledgegapandprovidingevidencefor
betterprogrammingforchildrenandfamilies.
SUMMARYOFRESULTSThisreportreviewed105studiesofparentingprogrammes.Thesestudieswereoperationally
definedasactivities,programmes,servicesorinterventions,forparents,aimedat
improvingparentinginteraction,behaviors,knowledge,beliefs,attitudesandpractices,
amongstchildrenaged0-8years.Theserecommendationswereintendedtoimprovethe
children’sphysicalhealthbeyondmeresurvival,encouragecognitivedevelopment,and
supporttheirsocialandemotionalwell-being.Thesystematicreviewconsistedofelectronicsearchesof10academicdatabases(including
referencelistsintheindividualstudiesidentified)aswellassearchesofthebroadergrey
literaturebetweentheyears2001-2011.Herein,wedefinegreyliteratureasreportsnot
foundinacademic,peer-reviewed,orpublishedjournals.Intheacademicsearch,multiple
disciplineswereexplored:medicineandglobalhealth,education,psychology,economics
andothersocialsciences.Searcheswereconductedusingbroadheadingsbasedonthe
geographicallocationofthestudy,thetypeofintervention,andthekindofevaluation.In
thegreyliteraturesearch,agencywebsitesweresystematicallyexplored.Keyinformant
solicitationswereconductedtoidentifyunpublishedandagencyevaluationsofECD
parentingprogrammes.StudieswereselectedforanalysisusingthePICOcriteriaaccording
topopulation,intervention,comparison(evaluationtype),andoutcome(Petticrew&
6
Roberts,2006).Inter-rateragreementofthescreeningprocesswas88%(Cohen’sκ=.72),
indicatingsubstantialagreementbetweenthetworeviewers.Wedevisedaqualityscoring
systemandselected105articlesforanalysis(outofapoolof7,086studytitles).Wecoded
articlesaccordingtoprogrammecharacteristicsbasedontheirintensity,deliverymode,
deliveryapproachandcontent,staffing,andtypesofprogramme.Weincludedbothsingle-
generationprogrammesdesignedtodirectlyservecaregiversaswellasmulti-generational
programmesdesignedtoeitherservetheparentandthechildortheentirefamily.Insum,
36countriesin7regionsoftheworldwererepresentedinthissystematicreview,with
29.5%fromlow-incomecountries,33.3%fromlower-middle-incomecountries,and37.1%,
fromupper-middle-incomecountries.
WeclassifiedprogrammaticstrategiesundertwobroadECDprogrammegoals:(i)those
thatpromotednutritionandhealth;and(ii)thosethatpromotedholisticoutcomesbeyond
nutritionandhealthsuchascognitiveandsocio-emotionaldevelopment. Thesegoalswere
classifiedseparatelysincewefoundthatstudiesconductedinSub-SaharanAfricaandSouth
Asiaweremorelikelytoevaluateprogrammesaimedatimprovinghealthandnutrition,
whereasstudiesconductedinCentralandEasternEurope/CommonwealthofIndependent
States,LatinAmericaandtheCaribbeanweremorelikelytoevaluateprogrammesaimedat
improvingnon-health-relatedchilddevelopmentaloutcomes.Belowwesummarizekey
findings,firstintermsofchildoutcomesandthenintermsofparentalpractices.
Child physical wellbeing.Childnutritionandgrowthwereimprovedthroughseveral
typesofparentingprogrammes:micronutrientsupplementationprogrammes,nutrition
education,andothercomprehensivehealthandnutritionprogrammes.Toreducethe
incidenceofearlychildhoodmorbidities,especially,withrespecttodiarrheaeffective
parentingprogrammes,handwashingandbreastfeedingpromotionprogrammeswere
emphasized.Homevisitations,bytrainedparaprofessionals,arethepredominantformat
amongprogrammesthatimprovegrowthorhealthoutcomes.Findingsshowedthatgroup
settingsmustbecombinedwithothermodalitiessuchasindividualcounseling,distribution
ofpamphletsetc.Dosageshouldalsoberelativelyintensive,lastingatleastoneyear.
Programmesthataimedimprovingoralhealthweredidacticandsignificantlylessintensive
althoughpreferably,deliveredbytrainedprofessionals.Intermsofdevelopmentaltiming,
7
theaverageageattimeofinterventionwasprimarilyduringthefirstyearoflifetothe
toddleryears(12-36months).
Child cognitive development.Psychosocialstimulationprogrammes,whichentail
activeengagementbetweenthecaregiverandthechild,areeffectiveinimprovingachild’s
cognitivedevelopment.Theseprogrammesinvolvedtrainedparaprofessionals,givinglive
demonstrationsthatinvolvedchildrenthroughplayactivitiesthatweretailoredaccording
tothechild’sdevelopmentallevelandthefamily’sindividualneeds.Althoughpsychosocial
stimulationprogrammesimprovedcognitiveoutcomeswhentargetingimpoverished
groups,malnourishedchildrenstillperformedwellbelowtheirnon-impoverished
counterparts.Theaverageageofchildrenparticipatingintheinterventionwasaroundone
tothreeyears.Intermsofmodalityanddose,psychosocialprogrammesaredelivered
ideallyasintensivehomevisitingprogrammesorasacombinationofgroupandindividual
sessions.Programmesdeliveredaspartofhomevisitsranbetweenoneandtwoyears,at
weekly,ormonthlyintervals.Thereisalsostrongevidenceforcombiningpsychosocial
stimulationprogrammeswithearlyeducationprogrammes.Thereispreliminaryevidence
thatnutritionalsupplementationalonemaybeinsufficientinimprovingcognitiveoutcomes
inyoungchildren.However,breastfeedingpromotioncouldbeaneffectivestrategyin
improvingcognitiveoutcomes.Thiswasdemonstratedbystudyingtheimpactonlater
cognitivedevelopment,ofchildren6.5yearsofage,fromfamiliesparticipatinginahospital-
basedbreastfeedingpromotionprogramme.
Child socioemotional outcomes. Thefrequencyofevaluationsforthisdevelopmental
domainwasrelativelylow,despitetherecognitionthatpromotingyoungchildren’ssocial
andemotionalwell-beingisessentialinbuildingstronginfrastructureforoptimal
development.Outoftheentireanalysis,onlytwoprogrammesevaluatedthesocioemotional
domain.Participationinbothprogrammesresultedingreaterinterpersonalskillsandself-
esteemandlesseranxietyanddepression.Althoughnoimpactswerefoundfor
externalizingbehaviors(antisocialbehavior,hyperactivity,andoppositionalbehaviors),
participationinaprogramme,duringtheearlyyears,resultedinlowerlikelihoodofbeing
suspendedorexpelledfromschool.
6
Holistic child outcomes.Studiesimplementedinfivecountriesdemonstrated
significantoutcomesinmorethanonechilddevelopmentaldomain.Intervention
approachessreviewedinvolvedpsychosocialstimulation,integratedhealth,nutrition,and
developmentinterventions,andsocialprotectionprogrammes.Theresearchsuggeststhat
effectivestrategiesofimprovingholistichealthanddevelopmentaloutcomesinchildren
couldbeintheformofmulti-sectoralhealthandchilddevelopmentalprogrammesor
intensivepsychosocialstimulationprogrammes.Themulti-sectoralhealthandchild
developmentalprogrammeisefficientandeffectiveinimprovingahostofchildoutcomes.
Theintensivepsychosocialstimulationprogrammeentailsfrequentinteractionswith
caregiversandtheirchildren,lastingbetweenoneandtwoyears.Acrossstudies,itappears
thatdoseisimportantandhiringwell-trainedandsupervisedparaprofessionalswasacost-
effectivesolutiontodeliveringmessagestoparents.Malnourishedchildrenandyounger
agegroupsbenefitedthemostfromtheseprogrammes.Ouranalysisalsosuggeststhat
programmesincludingfathers,inthetraining,isapromisingandunderutilizedstrategy.
Thesefindingsareinagreementwithstudiesfromhigherincomecountriesthat
demonstratedstrongereffectsonbothchildandparentingbehaviorswhenfatherswere
involvedintheprogrammes.
Parenting Outcomes: Physical health-related caregiving. Atotalof20studies
addressedfouroverarchingstrategiestopromotephysicalwellbeingbytargetingparental
outcomesinrelationto(1)healthcareseekingbehaviorsandhygienepractices,(2)oral
healthpractices,(3)nutritioneducation(aloneorintegratedwithotherhealth-related
dimensions),and(4)carepractices.Programmeevaluationsrangedfrommoderatetolarge
(universal)coverage.Mostservicedeliverymodalitiescombinedmorethanoneapproach
withtheexceptionoftwoprogrammesthatutilizedonlyadidacticstrategy. Delivery
settingsalsovaried,withhomeandcommunitybeingthemostcommonformsof
programmedelivery.Datafromtwostudiessuggestthatinterpersonalcommunication,of
contextualizedandtargetedmessages,maypositivelyimpactparentalknowledgeand
specifichealthcareseekingbehaviors.Oneofthecharacteristicsoftheinterventionslikely
tobeassociatedwithpositiveimpactsonparentswasthespecificityofthehealth-related
messages.Interventionsthatusedthelocalworkforcetodeliverkeymessages,suggested
thatparaprofessionalscanimpacthealthknowledgeamongparentsofyoungchildren
bythemselvesorincombinationwithotherprofessionals.Programmescanbemore
effectiveinpromotinghealthybehaviorsiftheyarebuiltonlocalresearchanduse
contextualizeddisseminationchannels.Improvementinoralhealthknowledgecanbe
attainedthrougharangeofinterventiondosesasillustratedbytheintensityrangeofthe
programmes.Interventionsutilizinglocallyavailablefoodsdemonstratedpositiveimpact
inmicronutrientintake(forinstance,vitaminAandretinol).
Theeffectsofparentingprogrammesoncarepracticesviaantenatalprogrammesand
throughacommunity-basedapproachweremixed.Resultsfromoneoftheinterventions
suggestthatmorefrequentexposuretoeducationalmessagesthroughawiderangeof
channelsmayleadtogreaterchangesinmothers’care-seekingbehaviorduringthe
antenatalperiod.Targetedcareandhealthcareseekingpracticeswereimprovedin
responsetopaternalinterventions.However,improvementsinthesepracticesdidnot
translateintodecreaseinchildmortalityrateorchangesinchildweight.Thissuggeststhat
moreresearchisneededtounderstandthemediationofpaternalinvolvementonchild
outcomes.
Parenting Outcomes: Caregiving beyond physical care. Atotalof13studies
demonstratedimpactsoncaregivingbeyondphysicalcareandarecategorizedasfollows:(1)
childprotectionintermsofphysicalsafetyandinjuryprevention,(2)childprotectioninterms
ofabuseandneglect,(3)psychosocialstimulationandsupport,(4)responsivefeedingand
(5)integratedapproaches.Findingsfromevaluationofphysicalabuseprevention
programmessuggestthatgroup-basedprogrammesareeffectiveandusingdemonstrations
throughdidacticapproachesorviatechnologywereeffectivestrategiestodelivermessages.
Findingsfromevaluationofsafetyandpreventionprogrammessuggestthatprofessionals
areeffectivedeliverersofprogrammemessagesconcerningchildsafetyandalsochildabuse.
Itappearsthatevenshort-termprogrammesareeffective,althoughoperationalizationof
safetypracticeshasmostlybeenbasedonself-reports.Infact,onestudydemonstratedthat
theprogrammehadnoimpactonperformance-basedpractice.Responsivefeedingand
integratedprogrammeswere
1Weacknowledgethatresponsivefeedingispartofnutrition-relatedcaregiving,buthere,wefocusonthepsychosocialcomponent. 7
989
also effective programmatic strategies for improving parental practices promoting child
developmentandprotection.Child and Parent Outcomes: Child Developmental Outcomes (Health) and
Associated Parenting Practices.Nineteenstudiesfoundsignificantimpactsonchild
physicalhealthandhealth-relatedcaregivingpractices.Wefoundthreestudiesof
breastfeedingpromotionprogrammesthatimpactedbothchildhealthandparenting
practices.Also,somecommunity-basedhygieneanddiseasepreventionprogrammes
utilizedavailablecommunityresourcestodisseminatehealthandhygieneinformation.
Community-basededucationprogrammesreflectedanimpactinthereductionofthe
incidenceofdisease.Theseresultsmaybesustainedwithahigherfrequencyofexposureto
therelevantmessage.Anotherimportantprogrammaticdimensionarehealth-and-nutrition
educationprogrammes.Ourreviewrevealedthatnutritioneducationprogrammesarelikely
tobemoreeffectiveifprofessionalsdeliverthemessagesintandemwiththehealth
messages.Moreover,nutritioneducationprogrammesthatareintegratedintoexisting
programmesorstructuressuchasnutritionservicesorearlychildhoodservicesaremore
effective.
Wealsorevieweddatafromeightstudiescategorizedundercomprehensivehealthand
nutritionprograms.Afewoftheprogramsreviewedcapitalizedonavailablecommunity
resources,linkingprogramstoexistingpoliciesthroughmultisectoralpartnerships,resulting
inlowerratesofstuntingandbetterparentingpractices. Fromthestudyfindings,therewas
noaddedeffectsforsupplementaryfeedingorfoodfortificationefforts,however,thereis
someevidencethatpreventivenutritionprogramscomparedtorecuperative(i.e.,targeting
malnourishedpopulations)oneshavegreaterimpacts.Impactsonanthropometrywere
strongerforchildrenwhowereexposedtotheprogramwhentheywereyounger(6-23
months).
Child and Parent Outcomes: Child Developmental Outcomes (Non-Health)
and Associated Parenting Practices. Ourreviewofthirteenprogrammeevaluations
revealedthatintensive(atleastweeklyforaperiodofoneyear)psychosocialstimulation
programmesareeffectiveinchangingparentalpracticesandthechild’smental,socialand
9810
emotionaldevelopmentaloutcomes.Buttheyarenoteffectiveinalteringpsychomotor
developmentaloutcomesandanthropometricmeasuresevenwhentheseprogrammesare
integratedintoexistingnutritionprogrammes.Psychosocialstimulationstudiesshowedthat
programmes,whichrequiredirectinteractionwithchildren,aresuccessfulinimproving
children’sinformationprocessingskills,languageskills,andsocialandemotionalwell-being.
Additionally,theyalsoimprovecaregiverpracticesthatpromotechildren’scognitive,social
andemotionaldevelopment.Wediscussthelongitudinalimpactofexemplarprogrammes
anddescribeitsprogrammaticattributes(twoyearduration,deliveredbycertified
paraprofessionals,utilizingmothergroups)inthisreview.
Responsivefeedinginterventionswerealsoassessedfortheirimpactoncognitionand
developmentaloutcomes.Analysisoftheprogrammaticmodelssuggestitisimportantto
includechildreninthesessionactivitiesandfocusonspecificpracticesratherthanmerely
didacticinformationtomaximizeimpact.Integratedhealthanddevelopmentprogrammes
commonlyusedstandardizedmodulessuchasWHO’sCareforDevelopment.Other
programmesutilizedmorecontextualizedcurricula.Home-visitingwasacommonmodality
inthedeliveryofintegratedhealthanddevelopmentprogrammes.Ingeneral,programmes
wereunsuccessfulinimprovingchildren’spsychomotordevelopment,butsuccessfulin
improvingnotonlychildren’scognitiveandsocialandemotionaloutcomes,butalsoin
improvingmothers’knowledgeandpracticeofchildrearing.
Studies with no impact or predominantly mixed findings. Thereviewofcertain
studieshaveshowedeithernoimpactorpredominantlymixedfindingsontheoutcomes
ofinterest:
10
• ChildHealthandParentalHealth-relatedCaregivingOutcomes:Ourreviewof14
programmaticexamplesrevealedthatoverall,parentalpracticesdonotseemto
improve,overall,ifthemodalityisprimarilydidactic:—lecture-stylewithnodirect
interactionswithchildren.Moreover,communityempowermentprogrammeswere
ineffectiveinimprovinghealthoutcomes.Additionalmodalitiesandtheneedto
developsolidconcretetheory-of-changemodels,supportforpaternalinclusionand
communityapproacheslikesuchashomevisitationsmightbenecessary.Intermsof
dosage,lowdosageprogrammes(between1and9sessions)thataredelivered
didacticallywereineffective.
• ChildDevelopmentandParentalChildRearingOutcomes:Thediscussioncomprised:threelongitudinalfollow-upstudies,twochildprotectionprogrammes,
andtwointegratedhealthanddevelopmentprogrammes.Excludingtwoofthe
threefollow-upstudies,theotherswereevaluationswherethedeliveryof
instructionwasprimarilydidactic.Theevidencesuggeststhatbreastfeeding
promotion&psychosocialstimulationprogrammeshavelongtermimpacton
cognitiveoutcomesbutnotonsocialandemotionaldevelopment.Psychosocial
stimulationprogrammesmayhavelong-termimpactonsocialandemotional
outcomeiftheyweretobecombinedwithpreschooleducation.Thefindingsalso
suggestthatthedevelopmentofsocialandemotionalskillsandgeneralwell-being
requiresprogrammestotargettheseskillsdirectlyandovertime,incontextswhere
childrenhavetousethem,suchaspreschoolsettings.
DISCUSSIONANDSUMMARYOFTHE
RECOMMENDATIONSAcrossourreviewoftheliterature,weidentifiedthreekeyprogrammaticareasforexistingECD
parentingprogrammes:Timing of the Programme.Owingtotherapidchangesduringearlychildhood,there
aresensitiveandcriticalwindowsofopportunity,arounddevelopment,thatmustbe
12
accountedforwhendesigningparentingprogrammes.Breastfeedingprogrammesmust
commenceintheveryfirstmomentsofachild’slife. Psychosocialstimulationprogrammes
rangedfromwhenchildrenwereafewmonthsoldto6yearolds.Impactsonanthropometry
werestrongerforchildrenwhowereexposedtotheprogrammewhentheywereyounger.
Programme Dose (duration, frequency, and intensity): Lowdoseprogrammes
acrossduration,frequencyandintensityyieldednon-significantprogrammeimpact.
Durationofaparentingprogrammeislinkedtothetypesofoutcome. Forinstance,inorder
toimproveachild’sphysicalhealth,cognitivedevelopmentandsocialandemotional
development;thereviewsuggeststhat12monthsshouldbetheminimumdurationofa
parentingprogramme.Programmethatlastedover2yearshadamoreconsistentimpact,in
particular,amongstthevulnerableanddisadvantagedpopulations.Simultaneouslyanalysis
alsosuggeststhatshorterdurationprogrammesmayworkforparentlevelresults(for
instanceprogrammesunderoneyeartargetingharshdisciplineandoralhealthpractices).
Moreover,higherfrequencyparentingprogrammesweremoreeffectiveinimprovingparent
andchildoutcomes.Threeimportantobservationsregardingthefrequencyofexposureto
theprogrammeemerged:(i)unlikeduration,effectingparentorchildoutcomesrequiresa
similarhighfrequency;(ii)thefrequencyoftheprogrammedeliverymusttakeinto
considerationthefrequencywithwhichthefamiliesapplythelearntlessons;and(iii)the
frequencyoftheprogrammecanbepacedorphased-inwithmorefrequentexposureinthe
beginning.Intermsofintensity,orhowmuchoftheinterventionisdeliveredineachsession,
datasuggeststhatmoreintensiveapproaches,suchasthosethatincludedirectinteraction
withthechild,areneededtoimprovebothparentingleveloutcomes(e.g.theabilityofthe
caregivertobeemotionallyresponsive)andchildleveloutcomes(e.g.languageabilityofthe
childinresponsetomaternalfeedingpracticeprogrammes).
Programme modality (manner in which the parenting programme was
conducted): Astrongtheoryofchangemustguidetheprogramme’soutcomesthrough
themodalityorthemannerinwhichtheparentingprogrammewasconducted.Ourreview
showedthatchildcognitiveoutcomesweresignificantlyimprovedacrossbothhome-based
modalitiesandcenter-basedprogrammesthatusedgroupsettings.However,active
engagementbetweenthecaregiverandthechildwaskeytoimprovingchildren’scognitive
13
development.Further,programmeoutcomesshouldinfluencethemodality.Forexample,in
thecaseofparentingoutcomestoimprovechildprotection,providingdemonstrationsor
examplesofcontrastingapproachestosafetyareeffectiveininformingparentalpractices.
Consistently,programmesthatusedmorethanonemodalityachievedbetterresultsthan
programmesthatonlyusedonemodality.
Service Provision.Thereareseveralprogrammequalityattributesthatshouldbetaken
intoconsideration. Aprimaryfeatureofqualityistheidentityoftheserviceproviderand
theirabilitytodelivertheprogrammeeffectively. F o r e x amp l e , authorityfiguressuch
asdoctors,nursesandeducatorswereamongthemostsuccessfulserviceprovidersin
improvingparentingoutcomes. Also,trainedlocalfemalecoordinatorswitharelatively
highlevelofeducationwereeffectiveindeliveringtheprogrammeacrosshomeandinthe
groupsettings.Further,community-basedprogrammesthatpromotehealthandnutrition
indicatethatemployinglocalleaders,suchasreligiousleaders,mightbeaviablealternative
strategy.
Knowledge Gaps and Research Priorities.Inreviewingthe105articles,keyfindings
emergedwithimportantimplicationsforprogramming.Here,wediscusstheknowledge
gapsandproposedresearchprioritiesbasedonthereviewoftheliterature:
• Socialprotectionprogrammes,suchascashtransferprogrammes,areanimportant
mechanisminmanycountriestoreachpoorfamilies.Furtherresearchisneededto
addressthefeasibilityofintegratingECDparentingeducationintocashtransfer
programmes.Researchisalsoneededtoassesstheimpactofsuchintegrationon
improvingormediatingtheeffectsofcashtransfersonchildandparentoutcomes.
• Despitethefactthatakeydeterminantofparentingisthecaregiver’swellbeingand
mentalhealth,limitedresearchaddressesthisimportantmediatorbetween
13
programmeandchildoutcomes.Thus,akeyresearchpriorityinvolvesprogrammes
thataccountforthepsychological,emotionalandmentalstateofcaregivers.
• Muchliteratureisbasedonsmall-scaledemonstrationprogrammes.Itiscrucial
toaddresstheimpactofprogrammesatalargerscaleandcharacterizetheir
programmaticattributes.Ingeneralmoreresearchandevidenceisneededonthe
scalingupofECDparentingprogrammes.
• Onlythreestudiesacrosstheentirereviewlookedatfathersasrecipientsof
parentingprogrammes.Itiscrucialtoengagethefathersinprogramme
designandevaluationinkeepingwitharecentreportonpaternalinvolvement.
• Attentiontothesocialandemotionaloutcomesamongstchildrenwere
limited.Studiesexaminingsocialandemotionaldevelopmentwereaminority.
• Itisnecessarytostrengthenformativeresearchinthefield.Littledataisavailable
ontheroleofthe“demand-side”ofparentingprogrammesandwaystointegrate
culturalpreferencestotheprogrammes’designs.
• Metricsforimpactevaluationofparentingprogrammeslargelyrelyonself-report.It
isanimportantresearchprioritytooptimizeinstrumentsforevaluationaswellas
diversifytheinquiryofpotentialprogrammaticimpacts(biologicaloutcomes,
hormonalandstressoutcomesandepigeneticoutcomes).
• ThereisaneedtoconnectECDprogrammeoutcomestocrucialglobalprocesses
(suchaspeacebuilding,socialtransformation,sustainabledevelopment,academic
achievement).Multidisciplinaryand,whenpossible,longitudinalevaluationsare
requiredinLMICstobolsterECDprogramming,advocacyandsustainable
financing.
• Laborlaws,socialassistance,andfamilyleavepoliciesmaybekeymediatorsto
parentingprogrammes(e.g.foodsecurity,timespentathomeafterbirth,maternal
decision-makinginthehome,etc.).Keepingthesestructuralcharacteristicsis
importantinnotonlyunderstandingtheattributesoftheprogrammesthemselves,
butalsoinidentifyingotherentrypointsforadvocacy.
14
PROGRAMMATICRECOMMENDATIONS:
ResultsfromthesystematicreviewofparentingprogrammesinLMICsuggestthe
followingprogrammaticrecommendations:
• Programmaticgoal/sshoulddeterminetheprogrammaticstrategy. Inthecase
ofchildhealthandphysicalwell-being,severaltypesofparentingprogrammessuch
asmicronutrientsupplementation,nutritioneducationandcomprehensivehealth
andnutritionprogrammeswereeffective.Similarly,oralhealthprogrammes
througheducationclassesforparentsandpsychosocialstimulationprogrammesled
byprofessionalsand/ortrainedparaprofessionalswereeffectiveapproaches.
• Themostvulnerablepopulationandyoungeragegroupsbenefitthemostfrom
ECDparentingprogrammes.Amajorityoftheinterventionstargetedthemost
vulnerablepopulation.Malnourishedchildrenandyoungeragegroupsbenefitedthe
mostfromprogrammeslikeintegratedhealthandeducationprogrammes. Basedon
thesefindings,theauthorsrecommendinterventionswithanequityfocus.
• Programmequantityor“dose”(i.e.duration,frequencyandintensity)
influencesprogrammebenefits. Thesefactorsneedtobetakeninto
considerationwhendesigningeffectiveparentingprogrammes.
• Multipleprogrammemodalities(mannerinwhichtheparentingprogramme
wasconducted)–theadoptionofseveralmodalitiessuchasdemonstrations,
practiceandproblemsolvingforprogrammingwasmoreeffectivethanusingonly
onemodality. Thus,theuseofmultiplemodalitiesistherecommendedapproach
toparentingprogrammes.
• Thequalityofserviceprovisionmatterstotheprogramme’ssuccess.
Strengtheningthecapacityofserviceprovidersareassociatedwithsignificant
positiveresultsandrecommendedforprogrammesuccess.
15
CHAPTER1:INTRODUCTION
1.1 INTRODUCTIONParentingapproaches,philosophiesandculturalconstructionsabound,butthereisone
universaltenet:theprimaryfunctionofparentingistofacilitatethesurvival,development
andwell-beingofachild.However,thisfunctionmaynotalwaysbecarriedoutinfull(dueto
anynumberofindividualand/orcontextualfactors),disruptingthemechanismbywhich
positiveparentingpromoteschildren’sabilitytoachievetheirfullpotential.Thequestionis:
whatdoestheempiricalevidencesayabouttheefficacyofearlychildhooddevelopment
(ECD)parentingprogrammesinlowandmiddleincomecountries(LMICs),partsoftheworld
thathavereceivedlessattentioninthescientificliterature?
Thereisagapinourknowledgeonprogrammaticevidenceoneffectiveparenting
programmes.First,muchoftheevidenceonprogrammaticeffectivenessisfromhigh-
incomecountries,wherethesetting,resources,personalcapacitiesandunderstandingsof
programmeimplementationvarygreatlyfromlowandmiddle-incomecountries.Therefore,
thegeneralizabilityofthefindingsislimited.Second,thereistremendousvariationinECD
parentingprogrammefocus,contentandservicedeliverymechanismstherebycreatinga
challengeindelineationofeffectivenessfactors.Third,thereislittlesystematicinformation
onthescalingupofparentingprogrammes,theirsustainabilityandintegrationintoexisting
systemsofservicedeliverytoreachthemostmarginalizedanddisadvantagedpopulations.
Finally,literatureonthedevelopmentofparentingprogrammecurriculaandcontentis
limitedandoftendoesnotinclude“bottom-up”approachesthatcouldpromoteuptakeand
sustainability,giventhatparentingrepresentsthedemandsideandsocialnorms.
UNICEFisinterestedinimprovingthedevelopmentalpotentialofallyoungchildren
throughpromotingevidence-basedparentingpractices.Tothatend,itcommissioneda
systematicreviewoftheliteraturetoaddressgapsintheunderstandingofwhatpromotes
effective,sensitiveandresponsivechildrearingandcaringpracticesthroughECDparenting
programmesandinterventionsindifferentnational,communityandlocalcontexts. This
reportpresentstheresultsofasystematicreviewandidentifieseffectivecharacteristics
andfeaturesofECDparentingprogrammesandpractices.
1.2 PARENTSANDPARENTINGThetermsparentandprimarycaregiverareusedinterchangeablyinthisreport.Theword
parent/caregiverreferstotheindividualorindividualswholookaftertheinfantandyoung
childand/orwhoprovidethebulkofthecareinahomeorfamilycontext.Althoughthis
definitionoftenassumestheparent/caregiveristhebiologicalparent;fosteroradoptive
parents,grandparents,stepparents,eldersiblingorotheradultsproximaltothechild,
mayalsobetheprimarycaregiveriftheyprovideconsistentcaretothechild(Moran,Ghate
andvanderMerwe,2004).Further,someadvocatethetermparentorparentingtodenote
long-termfamilycareandthereforeparentingembodiespastandfutureperspectivesand
deepemotionalinvolvementintherearingandsocializationofayoungchild.Inthese
ways,itisdistinguishablefromthemotivesandactivitiesofpeopleinvolvedinshortterm
orprofessionalcareofchildren(WorldHealthOrganization,2004).Weusethewordparent
orcaregiverinthisreviewbecauseitisagender-neutraltermanditdoesnotexcludenon-
biologicalprogenitors.
Parentingcanbeunderstoodasinteractions,behaviors,emotions,knowledge,attitudes,
beliefsandpracticesassociatedwithchildhealth,development,learning,protectionand
well-being(Yale-AÇEV,20122). Westernmodelsidentifyfivedomainsofparenting:
caregiving,stimulation,supportandresponsiveness,structure,andsocialization(Bradley,
2004),andtheirexpressionisinfluencedbycontextualdifferences.2MotherChildEducationFoundation(ACEV).http://www.acev.org/en/anasayfa
16
17
• Caregivingreferstothebehaviorsandpracticesofcaregivers(mothers,
siblings, fathers, child care providers and those who look after infants and young
children)toprovidefood,healthcare,stimulationandemotionalsupportnecessary
forchildren’shealthysurvival,growthanddevelopment(EngleandLhotska,1999).
• Stimulationpractices are derived from the function of stimulatingneurons
(Shonkoff and Phillips, 2000). Examples include language interaction (e.g. singing,
talking, reading); provision of learning materials and exposure to learning
opportunities (e.g., books, magazines), physical interaction (e.g. sports, playing
games)andparents’behavior,which servesas amodel for children to imitateand
emulate(Brittoetal.,2002).
• Support and responsiveness, with a foundation in early bonding, are
expressedthroughsocialandemotionalrelationships,buildingtrustandattachment
and behavioral interactions such as hugging, holding and loving physical contact
(Bowlby,1988).Responsiveparentingincludespromptresponsetoachild’sbehavior
thatisappropriatetothechild’sneedsanddevelopmentalphase(Esheletal.,2006).
Responsivefeedingpracticeshavebeenpositivelyassociatedwithyoungchildren’s
nutritionstatus(Yousafzaietal.,2013).
• Structureisassociatedwithdiscipline,supervisionandprotectionofthechild
from harm, abuse and neglect (Baumrind, 1996). These parenting interactions are
expressed throughpositivedisciplinarypractices and a safe, secure and consistent
environment.
• Socializationrelatestoparentingthatpromotesthedevelopmentofvalues,
attitudes towards life, and identity; it is often an expression of cultural, social and
religiousmoralsandexpectations(Rogoff,2003).
Although these domains have been conceptualized individually,they are highly
interdependent.Responsive feeding practices involve both caregiving and supportwhile
18
sharedbook reading includesboth stimulationand responsiveness (Britto et al., 2006). In
addition,thereisnotaone-to-onecorrespondencebetweenaparentingdomainandachild
outcomedomain.For example,whenparentsexhibit responsivenesssuch as huggingand
cuddling, they influence their children’s emotionalwellbeing, foster their development of
relationships and shape their biological systems, including nervous and immune system
functioning(McCartneyandPhillips,2006). Nutritionfeedsthebrain,stimulationsparksand
strengthensitsneuralconnections,positivehealthinteractionreducestheimpactofillness
and protection buffers it from the negative impact of stress. The synergy between these
dimensionsunderscorestheimportancenotjustofparentingbutalsoofholistic,committed
parenting.
1.3 DATAFROMTHEMULTIPLEINDICATORCLUSTER
SURVEY(MICS)ONPARENTINGTrendsinparentingfromLMICarebeingcapturedbytheMICS(UNICEF,2009).The
caregivingtrendsarealarming.Forexample,only25%ofsurveyedmotherswithinfants
lessthan6monthsofagereportedexclusivebreastfeedingthepreviousday,withthe
upperlimitat57%.Thismeansthat,atbest,justoverhalfofchildreninthisagerangewere
breastfed(Arabietal.,2012).Similarly,withrespecttostimulation,theMICS3results
indicatethatinthethreedayspriortothesurvey,onanaverage,onlyonequarterof
mothersreadtotheirchild,slightlyoverathirdtoldstoriesandclosetohalf(47%)engaged
incounting,namingandotherlearningactivitieswiththeirchild(BornsteinandPutnick,
2012).However,mothersreportedhigherincidencesofsinging(50%)andplaying(64%)
withtheirchildrenduringthistime.Theresultsinthedomainofstructureareequally
alarming.66%percentofcaregiversreportedthat,inthemonthpriortothesurvey,their
childhadexperiencedpsychologicalaggression;63%reportedtheirchildexperiencedmild
physicaldiscipline,while16%reportedanexperienceofseverephysicaldiscipline.Only18%
ofcaregiversreportedthatnooneinthehouseholdhadusedaviolentformofdisciplinein
thepreviousmonth(LansfordandDeater-Deckard,2012).
19
Inconclusion,theseresultssuggestthatatbest,onlyhalfofparents(interviewedthrough
theMICS)engageinparentingbehaviorsthatareconsideredpositiveandbeneficialfor
ECD(BrittoandUlkuer,2012).
1.4 OVERVIEWOFPARENTINGPROGRAMSParentingsupporthasalwaysexisted(e.g.throughinformalkinshipandfamilynetworks),
butformalrecognitionoftheneedtosupportparentswasestablishedthroughthe
InternationalYearoftheFamilyin1994(UNESCO,1994).Parentingprogrammesare
typicallycategorizedtoinclude‘familysupport’,‘parenteducation’,and‘parenttraining’.
Sometimesthesetermsareusedinterchangeably.However,theydon’talwaysoverlap.For
example,sometimesparenteducationandsupportprogrammesincludenotonlyservices
thathelpparentsintheirrolebutmayalsoincludeotherservicessuchasjobtrainingor
adultliteracywhileparenteducationprogrammes,couldincludeonlyparentingeducation
services.
Supportforparentscomesfromavarietyofsources,oftenbroadlygroupedintoinformal
(fromfamily,friendsandneighbors,arisingfromparents’ownpre-existing‘natural’
networks),semi-formal(oftenprovidedthroughcommunity-basedorganizations,and
generallybythevoluntarysector),andformalsupport(organizedservices,oftenneeds-
based,andprovidedbythestatutorysectoraloneorinpartnershipwiththevoluntary
sector)(Ghate&Hazel,2002).Althoughinformalandsemi-formalsupportisanimportant
modality,inthisreview,onlyformalsupportprogrammeswereconsideredforanalysis.
ThedimensionsacrosswhichprogrammesvarycanbesummarizedintermsofEcological
Locus,DevelopmentalFocusandProgrammeCharacteristicsreviewedinClaveland,
Corter,Pelletier,Colley,Bertrand&Jamieson(2006).
20
TheEcologicalLocusreferstohowaprogrammefitsintothesocialsystemsandcommunity
surroundingthechild(definedbyprogrammelocation,targetpopulation,whothe
participants/staffareandhowtheyinteract).TheDevelopmentalFocusreferstothefact
thatparentprogrammesmayfocusondifferentdevelopmentaldomainsinchildrenand
stagesfromprenataltoinfancytopreschoolandtransitiontoschool(theymayvaryintheir
aimintermsoftheparent’sdevelopment,fromspecificparentingskills,toteachingskills,to
relationship-building,orevenempowerment).Someprogrammesareintendedtoimprove
parents’knowledgeandpracticesrelatedtocaregiving,nutritionandchildhealth(Aboud
andAkhter,2011),whereasothersfocusonearlyeducationandlearning(Kagitçibasietal.,
2001).Therearealsoprogrammescenteredaroundthereductionofharshparentingand
violenceathome(AlHassanandLansford,2011).Somefocusonparentswithchildrenfrom
birthto3yearsold(Hamadanietal.,2006),butothersaredesignedforparentswith
childrenfromthreeyearsandolder(e.g.,Johnsonetal,2012).Typically,programmesthat
focusontheyoungeragegrouphaveahealth,nutritionand/orstimulationfocusandthose
forolderchildrenhaveasocial,learningandeducationfocus.
ProgrammeCharacteristicsincludeintensity(frequencyandduration);deliverymode
(e.g.,face-to-face,group,individual,self-instruction,media),deliveryapproachand
content(e.g.,instructionalandskills-oriented,constructivist,relationship-building,
specificityofcontent,etc.);staffing(e.g.,professional,paraprofessional),andtypesof
programmes(e.g.,familyliteracy,homevisiting,behaviormanagementandsocial
development,center-basedparentchildprogrammes). Programmescanalsobe
differentiatedbythenumberofgenerationsthatarethetargettedbeneficiaries.Single-
generationprogrammesaredesignedtodirectlyservemothers(e.g.breastfeeding
programmes)and/orfathers(Cowanetal.,2007),whilemulti-generationalprogrammes
eitherservetheparentandthechildortheentirefamily(Wasik,2012).Programmesalso
differbasedonsetting:home-based(MotherChildEducationFoundation),clinic-based
(Needleman,1991),community-based(ThompsonandHarutyunyan,2009)andothersa
combinationofdeliverysettings.Programmescanalsobedifferentiatedbythedegreeof
standardizationwithintheircurriculum.Somefollowaverystructuredcurriculumwith
weeklylessonsplansanda

21
detailedscriptfortheserviceproviders.Othersarelessformalwithdiscussiontopics
generatedaroundparticipantneedsandinterests.
OuranalysisoftheliteratureprobedfortheEcologicalLocus,DevelopmentalFocus,and
ProgrammeCharacteristicsspecifiedintheprogrammeevaluations.Theoperational
definitionofanECDparentingprogramme,inthisreview,isanactivity,programme,service
orinterventionforparentsaimedatimprovingparentinginteraction,behaviors,knowledge,
beliefs,attitudesandpracticeswithchildren0-8yearsofage,soastoimprovetheirphysical
healthbeyondsurvival,cognitive,socialandemotionalwell-being.
Lately,parentingprogrammeshavebeeninthefocus,andconsequentlythereisagrowing
bodyofrelatedliterature. Inthelate1990s,theWorldHealthOrganization(WHO)review
ofparentingprogrammes,“ACriticalLink”,ledtotheconclusionthatthemosteffective
programmesaretheonesthatinvolveparentsandothercaregiversandfocusonchildren
whoareinthe“criticalwindow”oflifeandwhoaremostat-risk.
Inanextensivereviewofparentingprogrammesinlowandmiddle-income(LMIC)countries,
88UNICEFcountriesindicatedthattheircountryhasa“nationalprogramme”that
promotesgoodparenting(Lansford&Bornstein,2007).Afurtheranalysisof40
programmesin33ofthosecountriesrevealedinterestingdifferencesacrossthetarget
participantsserved,thedescriptionofprogrammecontentandfocus,desiredgoalsand
outcomes,thenatureofservicesprovided,theserviceproviders,andthelocationofwhere
thoseserviceswereprovidedandtheunderlyingtheoryofchange.Thesedimensionsofthe
targetageofchildrenserved(e.g.,infants,preschoolers),methodofservicedelivery(e.g.,
home-based,groups),focusoftheprogramme(e.g.,health,nutrition,cognitive
stimulation,early-education),andactorssponsoringandimplementingtheprogrammes
(e.g.,state,privatesector)havebeenvalidatedthroughareviewofECDprogrammes
implementedinLMIC(Britto,YoshikawaandBoller,2011).Basedonthereviewby
LansfordandBornstein(2007),27ofthereportedprogrammesimpactedmothers,22
impactedfathers,andasmallernumberofreportedprogrammesimpactedchildren,
schoolsandcommunities.Inmostcasestheevidencewasanecdotalandnotscientifically
rigorous.
22
Engleandothers(2011)publishedareviewof11effectivenesstrialsand4scaled-up
parentingprogrammesacrossarangeofdeliverysettings,generationoftarget
beneficiaries,curriculaandkeymessages.Theirreviewreportssubstantialpositive
outcomesforchildren(e.g.cognitive,socialandemotionaldevelopment)andtwoofthe
programmesreportsignificantimprovementinadultparentingknowledgeandthehome
environment.
Theparentingliteraturealsocoversinterventionsthatarenotfocusedonparentingandyet
haveimprovedparentingoutcomes.Forexample,socialprotectionorconditionalcash
transferprogrammesthatcombinecashandparentingserviceshavedemonstrableimpact
onparentingknowledgeandpractice(BerhmanandHoddinott,2005;Macoursetal.,2012).
Adultandfamilyliteracyprogrammeshavealsodemonstratedpositiveimpactonparent
andchildoutcomes(PadakandRasinski,2003).
Therearealsospecificprogrammemodelsthatarebeingimplementedglobally,for
example,CareforChildDevelopment(WHO/UNICEF)andMotherChildEducation
Programme(MOCEP/ACEV).CareforChildDevelopmentpackageisaholisticintervention
thatbringstogethertheessentialevidence-basedcomponentsofparentingbyaimingto
guidetheinteractionbetweenacaregiverandachildinafamilysettingtherebyimproving
thecaregivingskillsofparentsandothercaregivers.Thegoalistostrengthenfamilies’
knowledge,skillsandbeliefstoprovidethebestpossiblecare,stimulationand
environmentfortheirchildren’soptimaldevelopment.Arecentevaluation(conductedin
anexperimentalrandomizedcontrolledtrial)showedthatwithinanyearof
implementation,thechildrenoffamiliesparticipatingintheprogrammehadbetter
cognitivedevelopment,socialrelationships,emotionalbondsandlanguageand
communicationskills.Themotherswerelessdepressedandthefamilyenvironmentwas
morepositiveandstimulating(Petrovic&Yousafzai,2013).Alloftheseimpactsareamong
thestrongestpredictorsoffuturehealth,achievement,andsuccess.Thepremisebehind
theMotherChildEducationProgramme(MOCEP)isthatearlydevelopmentalneedsof
childrenmustbemetandsupportedbytheirimmediateenvironmentandparentsplayan
importantroleas"firsteducators." MOCEPhasbeendevelopedforfamilieswithchildren3
to6yearsofageandisimplementedthrougha25-weekprogrammeconductedbyACEV-

23
trainedgroupleaders,
23
alongwithaweeklycurriculumforthechildthatisimplementedathomebythemothers.
Longitudinalresultsoftheprogrammehavedemonstratedsustainedbenefitsincognitive
development,schoolachievement,schoolattainment,andsocio-emotionaldevelopment
andsocialintegration. Mothersandfamiliesalsobenefitedfromtheprogrammeinterms
ofbetterfamilyrelationsandwomen’sincreasedintra-familystatus(Kagitcibasi,Sunar&
Bekman,2001).BothCareforChildDevelopmentandMOCEParebeingimplementedin
severalcountriesaroundtheworld.
Insummary,earlychildhooddevelopment,definedastheperiodfrombirthuptoeightyears
ofage,isacriticalwindowofopportunityforachild’scognitive,social,emotionaland
physicaldevelopment.Appropriatestimulationandsupportduringearlychildhoodresultin
arangeofsocialandhealthoutcomesinthecourseoflife.Severalpreconditionsmustexist
toensurethatchildrengetthebeststartinlifeandtheopportunitytothrive,including
effective,sensitiveandresponsivecareoftheyoungchildbytheprimarycaregiver,family
andcommunity.Accordingtoanestimatetwohundredmillionorathirdoftheworld’s
youngestchildrendonotachievetheirpotentialduetolackofstimulating,nurturing,safe,
andresponsivecaregiving.Theimportanceofcaregivingcannotbeunderestimatedforearly
childdevelopment(Engleetal.,2007).However,parentsandcaregiversneedtobe
supportedinfulfillingthisrole.Theresultsfromparentingprogrammes,acrosshigh-,middle
andlow-incomecountriesindicatesignificanttrendsinobtainingpositiveresultsfor
parentsandchildren(MOCEP).However,parentingprogrammesexistwithinacomplex
landscapeandrepresentamyriadofdesigns,makingitdifficulttoisolateandcompare
effectivemechanisms. Further,evaluationsoftheseprogrammeshaveusedmixeddesigns
andoftennotrobustevaluationdesigns.Implementingeffective,scaled-upsustainable
parentingprogrammesrequiressystematicguidanceandinformationonwhatprogramme
characteristicspromoteeffective,sensitiveandresponsivechildrearingpractices,witha
specialemphasisonthemostmarginalizedfamiliesandvulnerablechildreninsupportof
UNICEF’sfocusonequity.
24
1.5 STUDYOBJECTIVESANDRESEARCHQUESTIONSTheoverarchingaimofthecurrentstudyistoidentifythemosteffectiveapproachesand
deliverymechanismsofparentingprogrammeswithaspecialfocusonthemost
marginalizedfamiliesandvulnerablechildren.ThisfocusisintandemwithUNICEF’sequity
approachinordertoprovideevidenceforbetterprogramminginaglobalcontext.Giventhe
aimsofthestudy,asystematicreviewmethodologywasconsideredappropriateand
relevant.
Systematicreviewmethodologiesweredevelopedtoovercomethebiasesthatareintrinsic
totraditionalliteraturereviews. Asystematicreviewisanexhaustiveorcomprehensive
reviewofthecurrentpublishedandunpublishedliteratureusingasetofpredetermined
criteriaandprocedures.Systematicreviewsareparticularlyusefulfortopicswherethereisa
vastamountofinformationandmanypublications. Thesystematicreviewmethodology
providesatoolforthesummaryandanalysisoftherespectiveliteraturetoanswerasetof
specificresearchquestions.Asystematicreviewisconsideredaresearchmethod
unlikeatraditionalreviewthatmerelydiscussestheliterature.Asystematicreviewfollowsa
studyprotocoltoanalyzetheliteraturetorespondtospecificresearchquestions(Petticrew
&Roberts,2006).
AccordingtotheCampbellCollaboration(2010),asystematicreviewcouldbeconsideredan
evidence-basedtoolthatusestransparentprocedurestofind,evaluate,andsynthesizethe
resultsofrelevantresearch.Theseproceduresaredesignedinadvance,similartoother
researchdesignstudies,sothatthereviewstudycanbereplicated.Further,theliteratureis
screenedforrelevanceandqualitybasedonasetofpredeterminedcriteriatoreducebias.
ThefollowingcomponentsarerecommendedbytheCampbellCollaborationfora
systematicreviewstudy:(i)anexplicitsearchstrategy;(ii)clearinclusion/exclusioncriteria;
and(iii)systematiccodingandanalysisofincludedstudies.Theaimofthissystematic
review,inparticular,istosynthesizeandanalyzemodelsofECDparentingprogrammesto
discerntheeffectivenessfactorsthatimproveparentingandchild
25
outcomes,withaspecialfocusonthemostmarginalizedfamiliesandvulnerablechildren,
inaglobalcontext.Thestudywasdesignedto:
• Provide an overview of available evaluation-based evidence of parenting
programmes,includingthemostmarginalized;
• Mapoutandcategorizeexistingprogrammesthatimproveparenting(scope,
coverage,deliverychannels,partners),includingachievements,constraintsand
lessonslearned;
• Identifythemosteffectiveapproachesanddeliverymechanisms;
• Improve understanding of the context in which parenting programmes
work/operatemosteffectively;
• Distillessonslearnedandgoodpracticesbyanalyzingwhatworksandwhatdoesnot
work (and why) in various aspects related to planning, management and
implementationofparentinginterventions.
• Identify which programmatic features such as programme dosage, programme
modality,serviceprovision,andtimingcan leadtoa theoryofchangeforeffective
programming.
1.6BRIEFDESCRIPTIONOFCHAPTERSINTHEPRESENT
REVIEWTheoverarchinggoalofthissystematicreviewistosynthesizeextantresearchonearly
childhoodparentingprogrammesinlowandmiddle-incomecountries(LMIC),wherethe
needforsuchprogrammesishighgivengrossimpoverishmentintheseglobalareas.The
reportisdividedintofourmainchapters:
• Chapter1providesthecontextualframeworkforthisreport.Itbeginswithan
introductiontoparentingfollowedbyadefinitionofkeyconcepts,thecurrent
status and overview of parenting programmes, the study objectives and
researchquestions.

26
• Chapter2 elaborateson themethodology used in the systematic review. It
includes the search strategy, inclusion criteria, and protocol for screening
data.
• Chapter 3 presents the systematic review results for LMIC, based on
descriptiveresultsandprogrammaticresults,forchildandparentoutcomes.
• Chapter 4 discusses the key findings of the review of parenting
programmes based on what constitutes effective, sensitive and responsive
childrearingandcaringpracticesthroughECDparentingprogrammes.Italso
discussestheinterventionsaswellastheknowledgegapsandfutureresearch
priorities.

27
CHAPTER2:STUDYMETHODS
2.1LITERATURESEARCHTheliteratureonECDparentingprogrammesisvastandiscoveredinbothacademicand
non-academicresources.Therefore,weconductedasystematicreviewofECDparenting
programmeevaluationsinLMICbeginningwithathree-prongsearchstrategyusingasetof
predefinedconstructs,keywords,anddiscipline-specificvocabulary.First,weconducted
electronicsearchesoftheacademicliterature(namely,peer-reviewedjournalsandreviews
ofreferencelistsinthestudiesidentified)within10databases.Multipledisciplineswere
exploredincludingmedicineandglobalhealth(Medline,EMBASE,CINHAL,GlobalHealth),
psychology(PsycINFO),socialsciences(SSCI,IBSS,andSocialServicesAbstracts),
economics(EconLit),andeducation(ERIC).Searcheswereconductedusingbroadheadings
forgeographicallocationofthestudy,typeofintervention,andtypeofevaluation(Glover
&Odato,personalcommunication).Searchstringswereadaptedtothedifferent
databases,butgenerallythesearchesincluded:(child*orearlychild*orearlyintervention
orearlylearningoryoungchild*orgirlchild*orchildcare)OR(parent*orfather*or
mother*)inconjunctionwithaproximityoperatorfollowedby(guid*ortrain*or
educationorbehav*orprogramme*orinterventionorrelation*)OR(famil*orextended
famil*orcaregiv*orgrandfather*orgrandmother*orgrandparent*orsibling*or
brother*orsister*)AND(programme*orinterv*ortrain*).
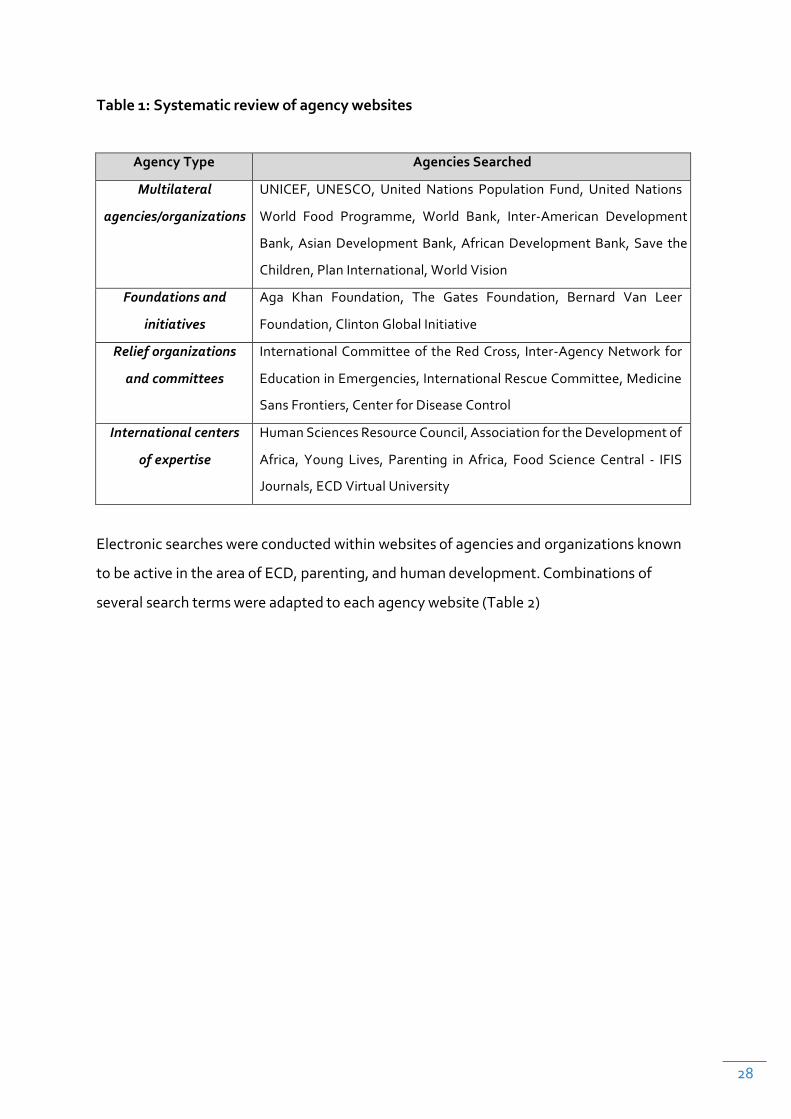
Second,toreducepotentialeffectsofpublicationbias,thebroadergreyliteraturewas
searchedthroughasystematicexplorationofagencywebsites(Table1).
28
Table1:Systematicreviewofagencywebsites
AgencyType AgenciesSearched
Multilateral
agencies/organizations
UNICEF, UNESCO, UnitedNations Population Fund,United Nations
World Food Programme, World Bank, Inter-American Development
Bank,AsianDevelopmentBank,AfricanDevelopmentBank,Save the
Children,PlanInternational,WorldVision
Foundationsand
initiatives
Aga Khan Foundation, The Gates Foundation, Bernard Van Leer
Foundation,ClintonGlobalInitiative
Relieforganizations
andcommittees
InternationalCommitteeof theRedCross, Inter-AgencyNetwork for
EducationinEmergencies,InternationalRescueCommittee,Medicine
SansFrontiers,CenterforDiseaseControl
Internationalcenters
ofexpertise
HumanSciencesResourceCouncil,AssociationfortheDevelopmentof
Africa, Young Lives, Parenting in Africa, Food Science Central - IFIS
Journals,ECDVirtualUniversity
Electronicsearcheswereconductedwithinwebsitesofagenciesandorganizationsknown
tobeactiveintheareaofECD,parenting,andhumandevelopment.Combinationsof
severalsearchtermswereadaptedtoeachagencywebsite(Table2)
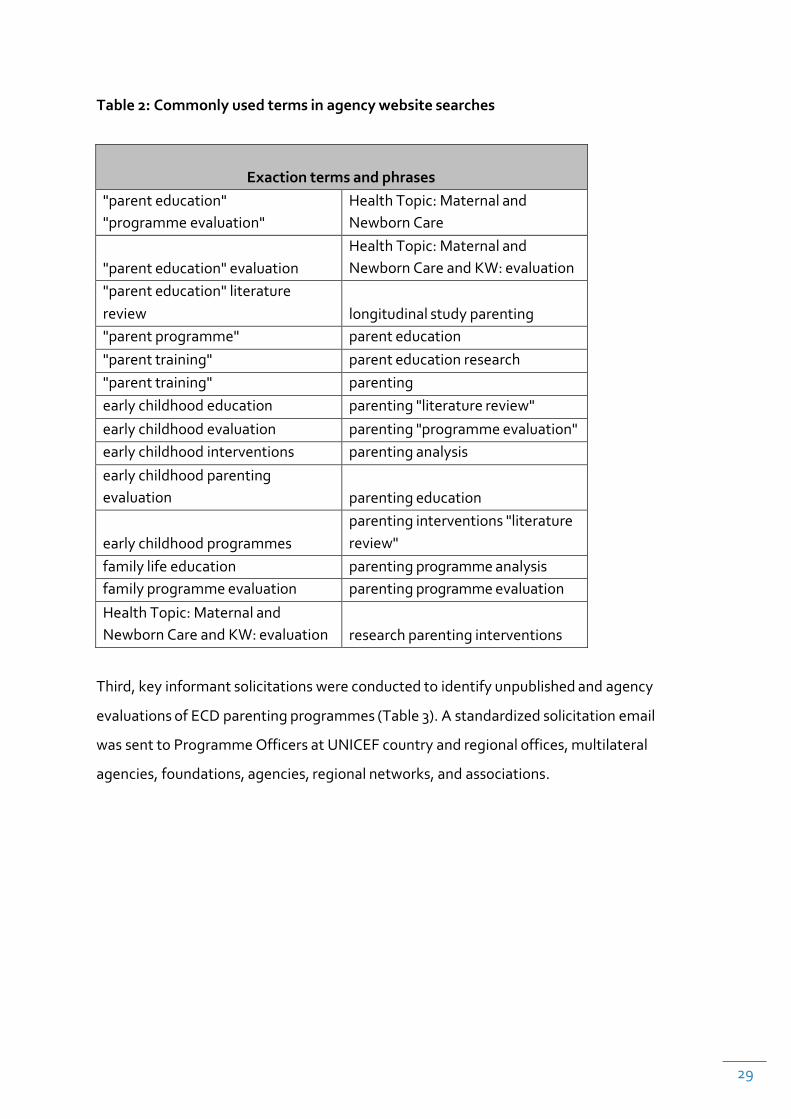
29
Table2:Commonlyusedtermsinagencywebsitesearches
Exactiontermsandphrases"parenteducation""programmeevaluation"
HealthTopic:MaternalandNewbornCare
"parenteducation"evaluation
HealthTopic:MaternalandNewbornCareandKW:evaluation
"parenteducation"literaturereview
longitudinalstudyparenting
"parentprogramme" parenteducation"parenttraining" parenteducationresearch"parenttraining" parentingearlychildhoodeducation parenting"literaturereview"earlychildhoodevaluation parenting"programmeevaluation"earlychildhoodinterventions parentinganalysisearlychildhoodparentingevaluation
parentingeducation
earlychildhoodprogrammes
parentinginterventions"literaturereview"
familylifeeducation parentingprogrammeanalysisfamilyprogrammeevaluation parentingprogrammeevaluationHealthTopic:MaternalandNewbornCareandKW:evaluation
researchparentinginterventions
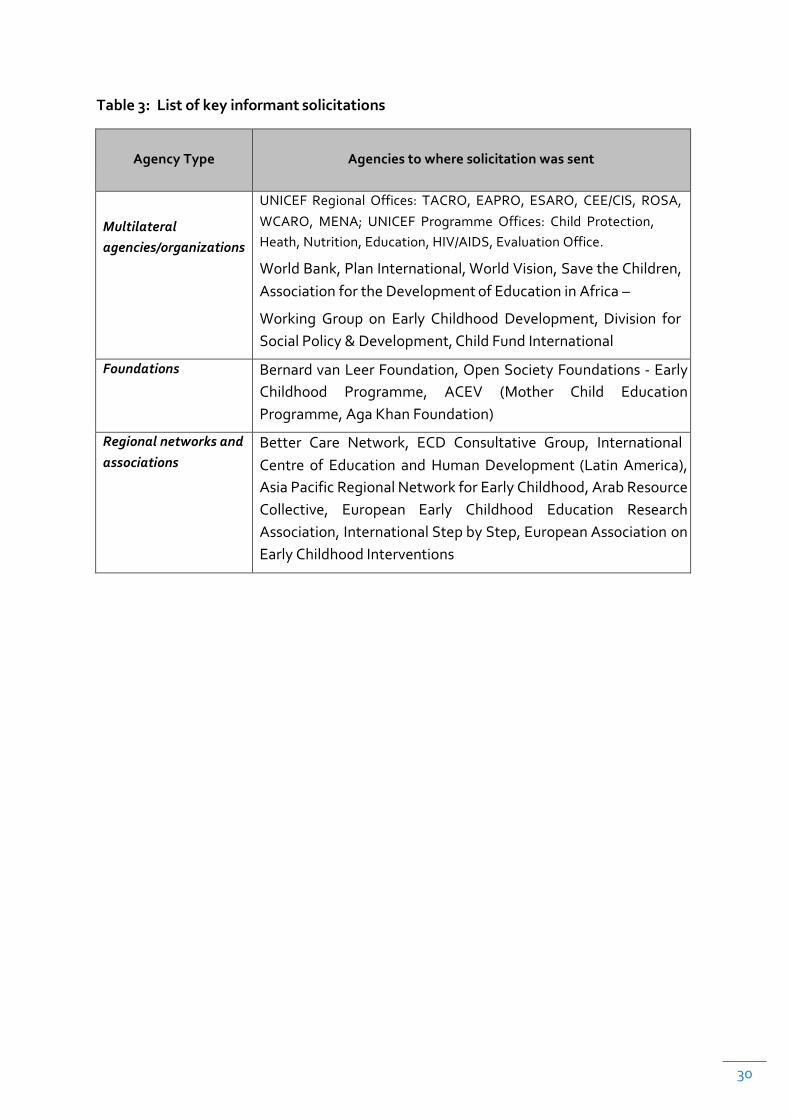
Third,keyinformantsolicitationswereconductedtoidentifyunpublishedandagency
evaluationsofECDparentingprogrammes(Table3).Astandardizedsolicitationemail
wassenttoProgrammeOfficersatUNICEFcountryandregionaloffices,multilateral
agencies,foundations,agencies,regionalnetworks,andassociations.
30
Table3:Listofkeyinformantsolicitations
AgencyType
Agenciestowheresolicitationwassent
Multilateralagencies/organizations
UNICEF Regional Offices: TACRO, EAPRO, ESARO, CEE/CIS, ROSA,WCARO, MENA; UNICEF Programme Offices: Child Protection,Heath,Nutrition,Education,HIV/AIDS,EvaluationOffice.
WorldBank,PlanInternational,WorldVision,SavetheChildren,AssociationfortheDevelopmentofEducationinAfrica–
Working Group on Early Childhood Development,Division forSocialPolicy&Development,ChildFundInternational
Foundations BernardvanLeerFoundation,OpenSocietyFoundations-EarlyChildhood Programme, ACEV (Mother Child EducationProgramme,AgaKhanFoundation)
Regionalnetworksandassociations
BetterCareNetwork,ECDConsultativeGroup, InternationalCentre of Education and HumanDevelopment (LatinAmerica),AsiaPacificRegionalNetworkforEarlyChildhood,ArabResourceCollective, European Early Childhood Education ResearchAssociation,InternationalStepbyStep,EuropeanAssociationonEarlyChildhoodInterventions

31
Figure1summarizesthethreesearchstagesanddatasourcesexploredinthisreview.
Ide
ntif
ica
tion
Includ
ed
Eligibility
Screen
ing
SearchesandkeyinformantconsultationswereperformedduringJuly/August2011.Figure1:SystematicReviewSearchStagesandDataSourcesExplored
Records identified
through academic
database search
(N=7,251)
Recordsidentifiedthroughothersources
(N=49)
Recordsafterduplicatesremoved(N=7,086)
Preliminaryscreeningofabstractsandtitles(N=7,086)
Recordsexcluded(failuretopasspreliminary
screening)( =6,726)
FulltextarticlesassessedforeligibilityusingPICOcriteria
(N=360)
Fulltextarticlesexcluded(failuretopassPICO
criteria)(N=255)
Studiesincluded(N=105)
2.2SCREENINGCRITERIAFORRELEVANCEANDELIGIBILITY
Asapreliminarymethodforscreening,weassessedstudyeligibilitybypublicationdate,
publicationtypeandlanguage.Onlyacademicstudiespublishedafter2001wereincluded
inordertonarrowtheanalysistorecentlypublishedstudies.Documentssuchaseditorials
andnotes,dissertations,letters,caseseries,conferencepapers,andbook
32
chaptersthatemergedfromtheacademicsearcheswereexcluded.Withingreyliterature,
onlyreportspublishedfrom2006onwardsweresearchedandscreenedinordertolimitthe
largevolumeofhitsthatcouldnotbefilteredthroughacentralizeddatabase.Publications
inEnglishandSpanishwereincludedforreview.
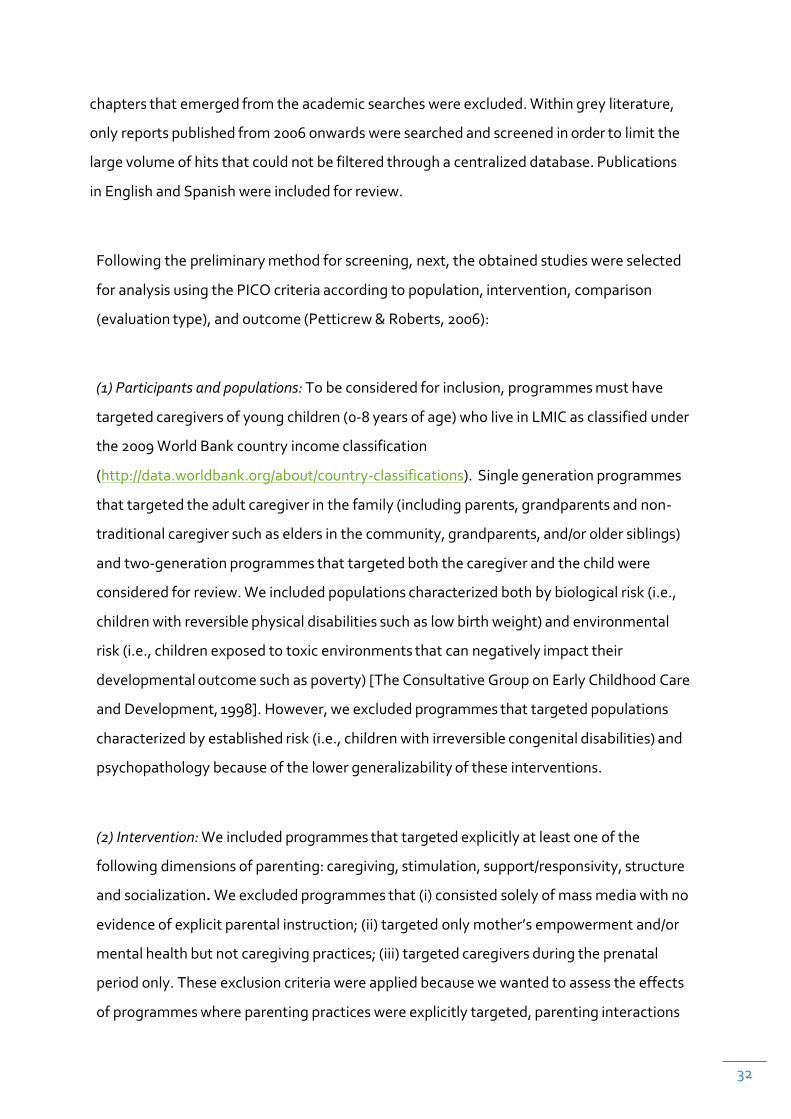
Followingthepreliminarymethodforscreening,next,theobtainedstudieswereselected
foranalysisusingthePICOcriteriaaccordingtopopulation,intervention,comparison
(evaluationtype),andoutcome(Petticrew&Roberts,2006):
(1)Participantsandpopulations:Tobeconsideredforinclusion,programmesmusthave
targetedcaregiversofyoungchildren(0-8yearsofage)wholiveinLMICasclassifiedunder
the2009WorldBankcountryincomeclassification
(http://data.worldbank.org/about/country-classifications). Singlegenerationprogrammes
thattargetedtheadultcaregiverinthefamily(includingparents,grandparentsandnon-
traditionalcaregiversuchaseldersinthecommunity,grandparents,and/oroldersiblings)
andtwo-generationprogrammesthattargetedboththecaregiverandthechildwere
consideredforreview.Weincludedpopulationscharacterizedbothbybiologicalrisk(i.e.,
childrenwithreversiblephysicaldisabilitiessuchaslowbirthweight)andenvironmental
risk(i.e.,childrenexposedtotoxicenvironmentsthatcannegativelyimpacttheir
developmentaloutcomesuchaspoverty)[TheConsultativeGrouponEarlyChildhoodCare
andDevelopment,1998].However,weexcludedprogrammesthattargetedpopulations
characterizedbyestablishedrisk(i.e.,childrenwithirreversiblecongenitaldisabilities)and
psychopathologybecauseofthelowergeneralizabilityoftheseinterventions.
(2)Intervention:Weincludedprogrammesthattargetedexplicitlyatleastoneofthe
followingdimensionsofparenting:caregiving,stimulation,support/responsivity,structure
andsocialization.Weexcludedprogrammesthat(i)consistedsolelyofmassmediawithno
evidenceofexplicitparentalinstruction;(ii)targetedonlymother’sempowermentand/or
mentalhealthbutnotcaregivingpractices;(iii)targetedcaregiversduringtheprenatal
periodonly.Theseexclusioncriteriawereappliedbecausewewantedtoassesstheeffects
ofprogrammeswhereparentingpracticeswereexplicitlytargeted,parentinginteractions

33
couldbeobserved,andsustainedparentingpracticesaimedat.Forinstance,weincluded
parentingsupportprogrammeswithaparentingeducationcomponentasinconditional
cashtransferprogrammesthatrequiredattendanceatparenttrainingworkshops.
(3)Evaluationdesign:ToassessECDprogrammeeffectiveness,first,weincludedimpact
evaluationstudiesfromboththeacademicandgreyliteraturethatcontainedpertinent
statisticaldata.Ameaningfulcomparisongroupmusthavebeenavailable,eitherinthe
formofcontrolgroups(experimentaldesigns),comparisongroups(quasi-experimental
designs),orwithin-groups(pre-post-testdesigns).Inaddition,theevaluationhadto
containatleast100participantsforrobustnessandgeneralizability(Terweeetal.,2012).
(4)Outcomes:Tobeincludedinthereview,theevaluationhadtoassessatleastonechildor
oneparentaloutcome(orboth).Childoutcomesincludedhealthandphysicalwell-being,
cognitivedevelopment,andsocial-emotionaldevelopment.Parentaloutcomesincluded
knowledge,attitudes,practicesbeliefs,andparentalefficacy.Programmesthatevaluated
onlyratesofimmunizationandprevalenceofbreastfeedingwereexcludedbecause
systematicevaluationsoftheseoutcomeshavebeenreviewedelsewhere(Bhuttaetal.,
2010).Moreover,programmesthatevaluatedonlytheeffectsofparentingprogrammeson
childmortalitywereexcludedbecausewewereinterestedinprogrammesthatimproved
otherdimensionsofchilddevelopmentbeyondsurvivalrates.
2.3SCREENINGPROCEDURES
Searchresultsfromacademicdatabasesandhandsearchesofreferencelistswereimported
intoareferencemanagementprogramme(EndnoteX4)whereduplicateswereremoved.
Primaryscreeningofacademicliteratureinvolvedfourreviewersscreening7,086study
titlesandabstractsfromthesearchresults.Outofthescreenedtitlesandabstracts,6,726
studieswereexcludedimmediatelyforfailingtomeetinclusioncriteria(e.g.,notan
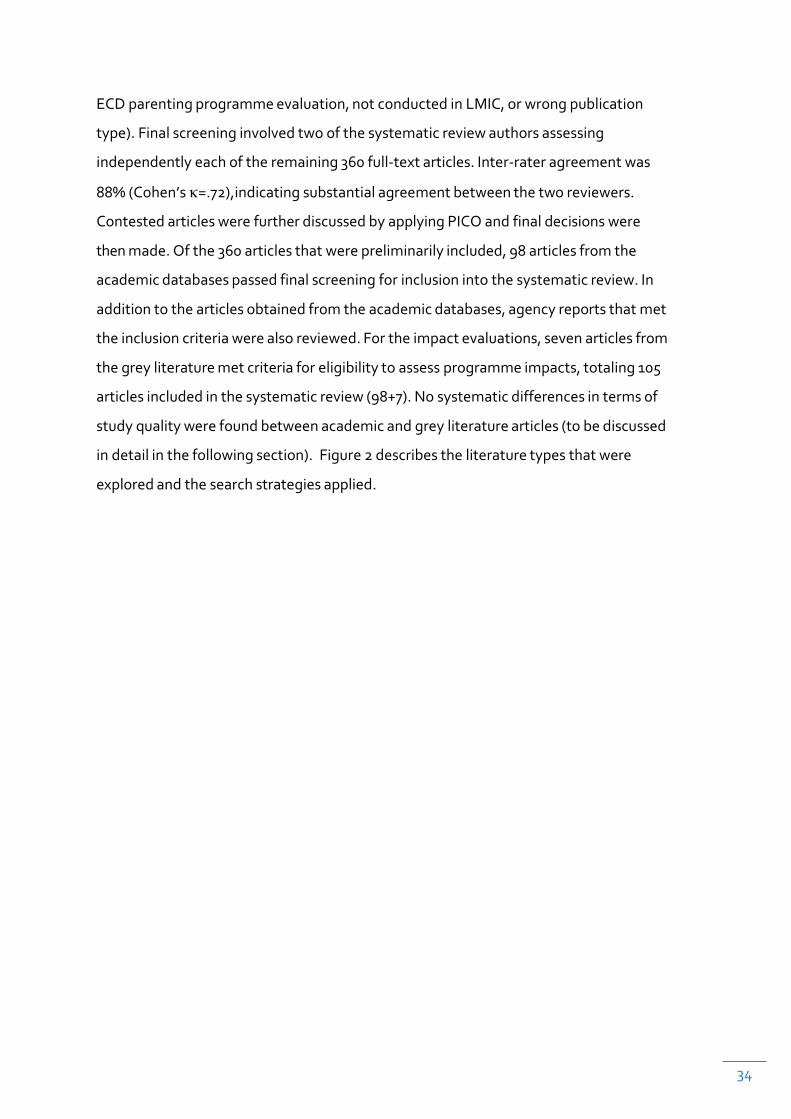
34
ECDparentingprogrammeevaluation,notconductedinLMIC,orwrongpublication
type).Finalscreeninginvolvedtwoofthesystematicreviewauthorsassessing
independentlyeachoftheremaining360full-textarticles.Inter-rateragreementwas
88%(Cohen’sκ=.72),indicatingsubstantialagreementbetweenthetworeviewers.
ContestedarticleswerefurtherdiscussedbyapplyingPICOandfinaldecisionswere
thenmade.Ofthe360articlesthatwerepreliminarilyincluded,98articlesfromthe
academicdatabasespassedfinalscreeningforinclusionintothesystematicreview.In
additiontothearticlesobtainedfromtheacademicdatabases,agencyreportsthatmet
theinclusioncriteriawerealsoreviewed.Fortheimpactevaluations,sevenarticlesfrom
thegreyliteraturemetcriteriaforeligibilitytoassessprogrammeimpacts,totaling105
articlesincludedinthesystematicreview(98+7).Nosystematicdifferencesintermsof
studyqualitywerefoundbetweenacademicandgreyliteraturearticles(tobediscussed
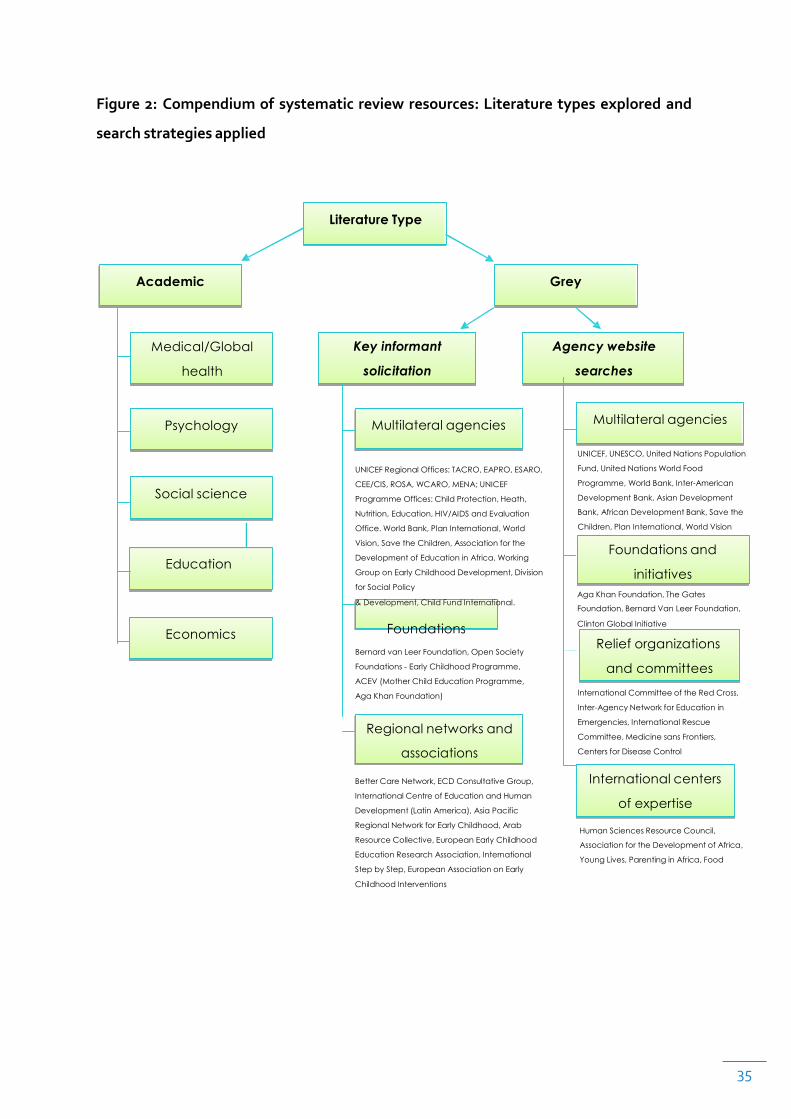
indetailinthefollowingsection).Figure2describestheliteraturetypesthatwere
exploredandthesearchstrategiesapplied.
35
Figure2:Compendiumof systematicreviewresources:Literaturetypesexploredand
searchstrategiesapplied
Literature Type
Academic Grey
Medical/Global
health
Key informant
solicitation
Agency website
searches
Psychology
Multilateral agencies Multilateral agencies
Social science
Education
Economics
UNICEF Regional Offices: TACRO, EAPRO, ESARO,
CEE/CIS, ROSA, WCARO, MENA; UNICEF
Programme Offices: Child Protection, Heath,
Nutrition, Education, HIV/AIDS and Evaluation
Office. World Bank, Plan International, World
Vision, Save the Children, Association for the
Development of Education in Africa. Working
Group on Early Childhood Development, Division
for Social Policy
& Development, Child Fund International.
Foundations
Bernard van Leer Foundation, Open Society
Foundations - Early Childhood Programme,
ACEV (Mother Child Education Programme,
Aga Khan Foundation)
Regional networks and
associations Better Care Network, ECD Consultative Group,
International Centre of Education and Human
Development (Latin America), Asia Pacific
Regional Network for Early Childhood, Arab
Resource Collective, European Early Childhood
Education Research Association, International
Step by Step, European Association on Early
Childhood Interventions
UNICEF, UNESCO, United Nations Population
Fund, United Nations World Food
Programme, World Bank, Inter-American
Development Bank, Asian Development
Bank, African Development Bank, Save the
Children, Plan International, World Vision
Foundations and
initiatives Aga Khan Foundation, The Gates
Foundation, Bernard Van Leer Foundation,
Clinton Global Initiative
Relief organizations
and committees
International Committee of the Red Cross,
Inter-Agency Network for Education in
Emergencies, International Rescue
Committee, Medicine sans Frontiers,
Centers for Disease Control
International centers
of expertise
Human Sciences Resource Council,
Association for the Development of Africa,
Young Lives, Parenting in Africa, Food
36
2.4DATAEXTRACTION
Atotalof105articles(frombothacademicandgreyliterature)wereincludedfordata
extractionandanalysis.Codingsheetswereusedtostandardizedataextraction.Extraction
categoriesincludedtheprogrammeapproach(e.g.,psychosocialstimulation,nutrition
education),deliverysetting(e.g.,primaryhealthcare,communitycenter),deliveryformat
(e.g.,homevisits,grouplectures),programmecomponents(e.g.,useofprint,live
demonstrations,directinteractionswithchild),programmeimplementer(i.e.,professional
orparaprofessional),dosage,evaluationmethod(i.e.,randomornon-random),and
outcomecategories.Wecontactedstudyauthorstofillinmissingdatawheneverpossible.
Tworeaderscoded85%ofthearticlesandattendedweeklymeetingstodiscusscoding
proceduresandchallenges.Theremainingarticleswerecodedbytwooftheauthorsofthis
report,whoalsoreviewedtherestofthecodedarticles.Toensureinter-coderreliability,
15%ofthestudiesweredouble-coded(Cohen’sκ=.76).Discrepancieswerediscussed
duringtheweeklymeetings.Thestudyauthorsdeterminedcodesofcontestedarticles.
2.5STUDYEVALUATIONInthefirstphaseofthesystematicreview,thefirststepinevaluatingeachstudywasto
assessitsquality(i.e.,thestudy’smeritsandpotentialforgeneralizabilityanditsrelevance
toECDprogramminginLMIC).Wedevisedaqualityscoringsystemthatweadaptedfroma
criteriadevisedbyoutsideexperts.(Jadadetal.,1996;Terweeetal.,2012).Ourcriteria
consistedoffivebroadcategories:(1)studydesign(i.e.,participantsrandomlyassignedto
condition;presenceofcontrol/comparisongroup;atleastonepretestandoneposttest;
explicitmentionofdoubleblinding;datacollectorsblindtointervention),(2)sample(i.e.,at
leastthreedescriptionsofthesample;initialequivalencebetweengroupsassessed;
comparison/controlgroupmatchedwithprogrammegroupatbaselinewithrespectto
demographics;comparison/controlgroupmatchedwithprogrammegroupatbaselinewith
respecttooutcomesbeingassessed;sampleattritionbelow20%),(3)programme
implementation(i.e.,useofanestablishedcourseofparentingasevidencedbyauthors’

37
reportofacurriculumortrainingmanual;assessedfidelitytointervention;trainingof
parenttrainersdescribed),(4)outcomemeasures(i.e.,usedstandardizedorobjective
measuresofatleastoneoftheoutcomevariablesofinterest;post-interventionscores
testedmorethanonce;effectsizesreported),and(5)culturalresponsivity(musthave
checkedatleastoneofthefollowing:materialstranslatedintolocallanguage;
programmepractices/materialsconsistentwith—oradaptedtofitwith—localcontext,
culture,orreligion;programmeownershipgiventolocalcommunity).Codersassigned0
and1foreachitem(total17items),wherehigherscoresmeanthigherqualityratings. We
calculatedpercentagestomakeupthequalityscoreforeachstudy(M=59.12%,
SD=16.45).Nosignificantdifferenceinqualityscoringpercentageswerefoundbetween
studiesderivedfromacademicdatabases(M=59.50,SD=16.74,range=14.29-9412)and
greyliterature(M=53.73,SD=11.13,range=38.46-68.67),t(103)=0.90,ns.Thesecondstepinevaluatingfindingsineachstudywastodetermineiftheprogrammehad
a significant impact. We set the significance level at p<.05 to remain consistent as few
studies consideredp<.10as significant.Whenevera study reported significantdifferences
between study participants and non-study participants (i.e., normal populationwhowere
not in the studycomparisongroup),weusedavailabledata fromthearticle todetermine
statistical significance between programme participants and their corresponding
control/comparisonparticipants.
2.6PUBLICATIONBIASGiventhenatureofourstudy,itishighlyprobablethatevaluationsofECDparenting
programmesinLMICwereconductedbutneverpublishedinpeer-reviewedjournals.We
addressedthisissueusingthreestrategies.First,asmentionedpreviously,weincluded
studiesobtainedfromthegreyliteratureiftheymetourstandardsforinclusion.This
approachcastsawidernetofstudiesthatmayotherwisenothavebeenfoundusing
traditionalacademicsearchstrategies.Second,weincludedstudiespublishedinSpanishto
expandthenumberofhits.GiventhatECDprogrammingisgrowingrapidlyinLatinAmerica
(Vegas
38
andSantibáñez2010),includingstudiespublishedonlyinSpanishlessensthebiasin
reportingresultspublishedonlyinEnglish.Finally,weincludedinourresultsasectionon
studiesthatshowedeithernosignificantimpactorpredominantlymixedfindingsonthe
outcomesofinterest.Altogether,thesestrategies,albeitimperfect,increasethe
generalizabilityofourfindings.
39
CHAPTER3:RESULTSThe105articlesreviewedinthisstudyprovidearangeofresultswithimplicationsfor
improvingtheeffectivenessofECDProgrammesandareaswherewehaveknowledgegaps
thatneedtobeaddressedbyfutureresearch. Resultsarepresentedintwosections.First,
weprovideadescriptiveoverviewofthestudieswithinformationongeographicregionof
theworld,wheretheProgrammesarebeingimplemented,andcommonProgrammefoci
andmodalities. Inthesecondpartofthischapter,wediscusstheresultsbyoutcome
domainswheresignificantdifferenceswerefound.
3.1DESCRIPTIVERESULTSThissectionpresentsresultsofourfindings.Thirty-sixcountriesinsevenregionsofthe
worldwererepresentedinthissystematicreview:with29.5%fromlow-income,33.3%from
lower-middle-income,and37.1%,fromupper-middle-incomecountries,respectively.About
athird(31.1%)ofthestudieswereconductedinLatinAmericaandtheCaribbean
(Argentina,Belize,Brazil,Haiti,Jamaica,Mexico,Nicaragua,Paraguay,Peru,andSt.Lucia),
followedbyoveraquarter(25.7%)inSouthAsia(Bangladesh,India,Nepal,andPakistan),
11.4%inEasternandSouthernAfrica(Ethiopia,Madagascar,Malawi,SouthAfrica,
Swaziland,Uganda)9.5%inCentralandEasternEurope(Armenia,Belarus,Turkey),8.6%in
EastAsiaandthePacific(China,Philippines,Thailand,Vietnam),7.6%inSub-SaharanAfrica
(BurkinaFaso,Gambia,Niger,Nigeria,Senegal),and5.7%intheMiddleEastandNorth
Africa(Egypt,Iran,Jordan,Syria).
40
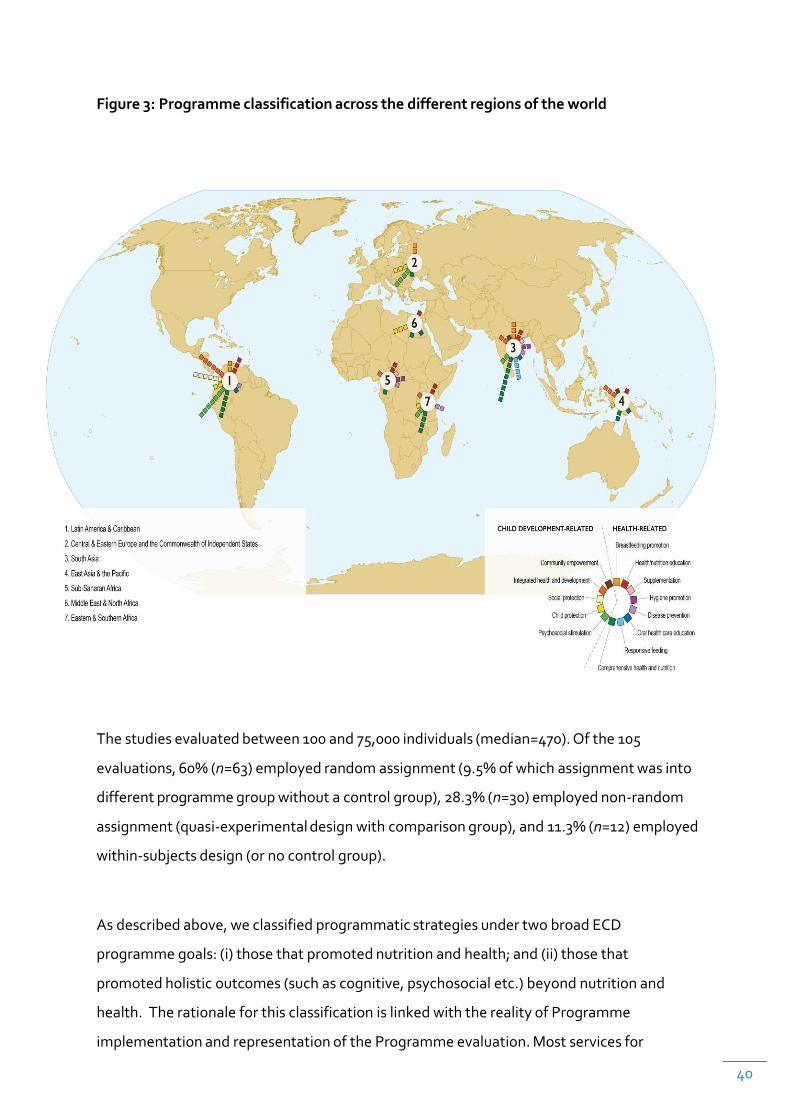
Figure3:Programmeclassificationacrossthedifferentregionsoftheworld
Thestudiesevaluatedbetween100and75,000individuals(median=470).Ofthe105
evaluations,60%(n=63)employedrandomassignment(9.5%ofwhichassignmentwasinto
differentprogrammegroupwithoutacontrolgroup),28.3%(n=30)employednon-random
assignment(quasi-experimentaldesignwithcomparisongroup),and11.3%(n=12)employed
within-subjectsdesign(ornocontrolgroup).
Asdescribedabove,weclassifiedprogrammaticstrategiesundertwobroadECD
programmegoals:(i)thosethatpromotednutritionandhealth;and(ii)thosethat
promotedholisticoutcomes(suchascognitive,psychosocialetc.)beyondnutritionand
health. TherationaleforthisclassificationislinkedwiththerealityofProgramme
implementationandrepresentationoftheProgrammeevaluation.Mostservicesfor

41
familieswithchildrenunder3
41
yearsofageareimplementedbythehealthsector.TheseProgrammestendtofocuson
healthrelatedoutcomes. Second,theliteratureonECDparentingwasbroadlydividedinto
ProgrammesthataddressedhealthandnutritionneedsandProgrammesthataddressed
otherdomainsofdevelopment. Thereforethisclassificationrepresentsthedistributionof
Programmefocusnotedintheliterature.
ECDparentingprogrammesthataimedtopromotenutritionandhealth(56.2%)consisted
ofbreastfeedingpromotion,health/nutritioneducation,micronutrientsupplementation,
hygienepromotion,diseaseprevention,oralhealthcareeducation,responsivefeeding,and
comprehensivehealthandnutrition.Comprehensivehealthandnutritionprogrammeswere
acombinationofanyofthementionedapproachesthataimtoimprovenutritionand
health.Theseprogrammesmayincludegrowthmonitoring,foodfortification,andhealth
education,forexampletheIntegratedManagementofChildhoodIllnesses,anintegrated
approachtochildhealththatfocusesonthewell-beingofthewholechildwithaprimarily
healthdrivenfocus.
Inadditiontoprogrammesthataimtopromotenutritionandhealth,otherprogrammes
aimedtopromotedomainsofchilddevelopmentotherthanhealth(43.8%).Theseincluded
psychosocialstimulation,childprotection,socialprotection(asinconditionalcashtransfer
programmes).InthiscategorywealsoincludedProgrammesthatintegratedhealthwith
development,i.e.,programmesthatcombinedhealthaimswithnon-healthchild
developmentalaims.
Certainregionsoftheworldstressedoneprogrammaticaimovertheother,χ2(6)=19.39,
p=.004(seeFigure3).StudiesconductedinSub-SaharanAfrica(87.5%)andSouthAsia
(81.5%)—regionswherefoodinsecurityandmalnutritionarepredominant—weremorelikely
toevaluateprogrammesaimedatimprovinghealthandnutrition,whereasstudies
conductedinCentralandEasternEurope/CommonwealthofIndependentStates(70.0%)
andLatinAmericaandtheCaribbean(63.6%)weremorelikelytoevaluateprogrammes
aimedatimprovingnon-health-relatedchilddevelopmentaloutcomes.
42
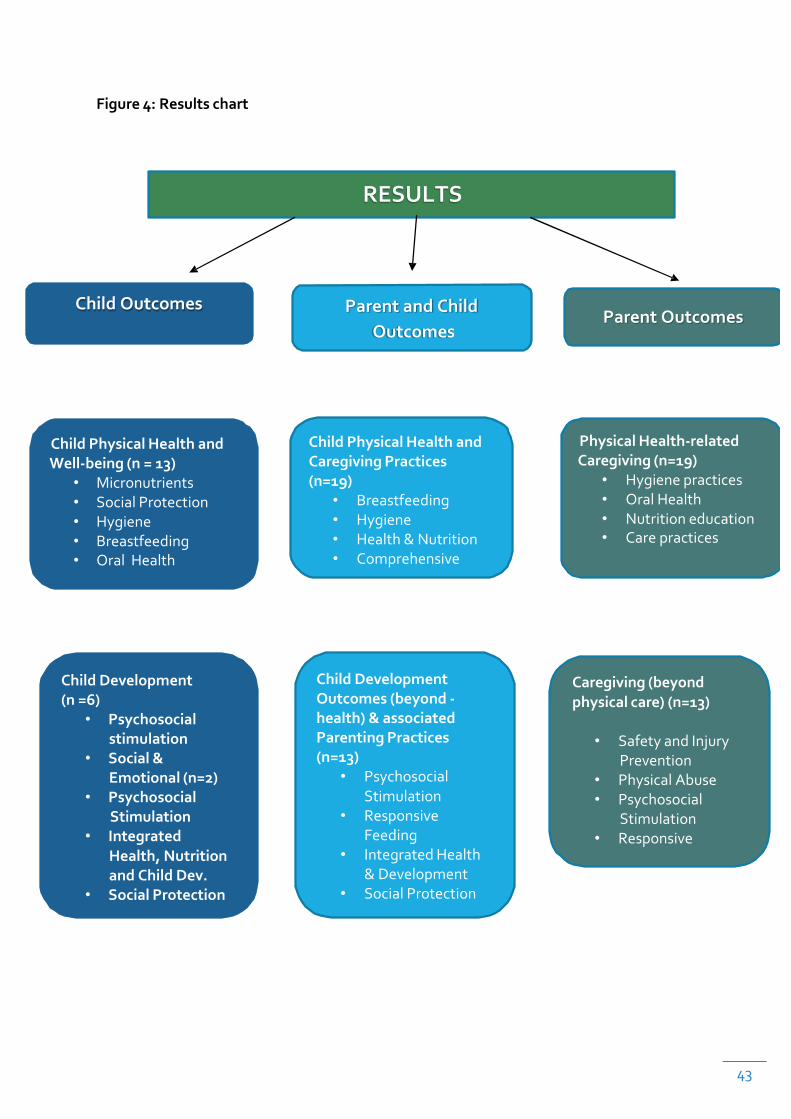
3.2PROGRAMRESULTSBYCHILDANDPARENTOUTCOMESWenowpresentresultsbyoutcomedomains:(1)childoutcomes(physicalwell-being,
cognitivedevelopment,socialandemotionaldevelopment,holisticdevelopment),(2)
parentoutcomes(knowledge,attitudes,andpracticesrelatedtohealth-relatedcaregiving,
caregivingbeyondphysicalcare,andacombinationofhealth-andnon-health-related
caregiving),and(3)bothchildandparentoutcomes(i.e.,comprehensiveoutcomes).(Figure
4).Programmaticdetailssuchasapproach,deliveryformatandsetting,dosage,and
implementerarediscussed.Thefinalsectionwillpresentresultsofevaluationsthatfound
noimpactorpredominantlymixedfindings.
Wearepresentingresultsseparatelyforsinglegenerationoutcomesandtwo-generation
outcomesbecausethetheoryofchangeunderlyingthesemodelsdiffer.Programmesthat
focusonsinglegenerationoutcomesmayormaynotemployafamilyfocusedecological
approach,asdiscussedinchapter1.Furthermore,theroleofparentsinmediatingchange
inchildoutcomes,isvieweddifferentlywhenonlychildrenarethefocusoftheintervention
comparedtowhenbothparentsandchildrenarethefocusoftheintervention.Finally,the
modality,doseandaimofProgrammesthattargetchildorparentoutcomesareoften
differentfromthoseprogrammesthataimtoimpactboththechildandtheparent.
43
Figure4:Resultschart
RESULTS
ChildOutcomes ParentandChildOutcomes
ParentOutcomes
ChildPhysicalHealthandWell-being(n=13)
• Micronutrients• SocialProtection• Hygiene• Breastfeeding• Oral Health
ChildPhysicalHealthandCaregivingPractices(n=19)
• Breastfeeding• Hygiene• Health&Nutrition• Comprehensive
PhysicalHealth-relatedCaregiving(n=19)
• Hygienepractices• OralHealth• Nutritioneducation• Carepractices
ChildDevelopment(n=6)
• Psychosocialstimulation
• Social&Emotional(n=2)
• PsychosocialStimulation
• IntegratedHealth,NutritionandChildDev.
• SocialProtection
ChildDevelopmentOutcomes(beyond-health)&associatedParentingPractices(n=13)
• PsychosocialStimulation
• ResponsiveFeeding
• IntegratedHealth&Development
• SocialProtection
Caregiving(beyondphysicalcare)(n=13)
• SafetyandInjuryPrevention
• PhysicalAbuse• Psychosocial
Stimulation• Responsive
44
3.2.1CHILDOUTCOMES
Childoutcomesarecategorizedintermsofthefollowingdomains:physicalwell-being(i.e.,
growth/anthropometry,morbidity,oralhealth);cognitivedevelopment(i.e.,information-
processingability,psychomotordevelopment,languagedevelopment,andacademic
achievementandperformance);socialandemotionaldevelopment(i.e.,internalizing
problems,externalizingproblems,andsocialadjustment);andholisticoutcomes(i.e.,a
combinationofoutcomesacrosstwoormoredomains).Twenty-sevenstudieswere
includedinthissection.
3.2.1.1 Child Physical Well-Being (n=13)
Inthissection,wepresentananalyticalsummaryofECDparentingprogrammesthataim
toimprovechildphysicalwell-being(SeeTable4inAppendix1).Thestudiesevaluated
between241and2,764children(median=906),spanningacrossninecountries:fourfrom
India,twofromPakistan,andoneeachfromBrazil,Iran,Malawi,Mexico,Niger,South
Africa,andVietnam.Thefollowingprogrammaticapproacheswereused:(1)micronutrient
supplementation,(2)hygienepromotion,(3)breastfeedingpromotion,(4)comprehensive
healthandnutrition,(5)oralhealthcareeducation,and(6)socialprotection.
Micronutrient Supplementation Parentalpracticesthatpromotemicronutrientintake
duringtheearlyyearsarecrucialforappropriategrowthandadequatephysical,motor,and
cognitivedevelopment.Micronutrientdeficienciesresultingfrommalnutritionmayleadto
irreversibleeffectsonbraindevelopmentandotherfunctionaloutcomes(Lozoff,Beardet
al.2006).Commonandrelatedanthropometricmeasurestoassessdelaysingrowth
trajectoriesincludestunting(height-for-agez<2),wasting(weight-for-heightz<2),and
underweight(weight-for-agez<2)(Cogill,2003).Stuntinginearlylifeisassociatedwith
impairedhealth,educationalperformance,cognitivedevelopment,andschool
achievement(DeweyandBegum,2011).Wastingoftenreflectsshort-termmalnutrition
45
(Richard,Blacketal.2012).Underweightisastrongpredictorofmortalityamongchildren
underfiveyearsofage(UNICEF2007).Oneothermeasureinassessingnutritional
developmentandstatusofdevelopingchildrenislineargrowthretardation,whichindicates
long-termexposuretonutritionaldeprivation(Allen1994).Amongthestudiesreviewed,micronutrientfortification/supplementationprogrammes
improvedgrowthandanthropometricmeasuresofchildren(Bhandari,Bahletal.2001;
Gaboulaud,Dan-Bouzouaetal.2007).Onelarge-scaletherapeuticrehabilitationprogramme
inNigersoughttoreduceseveremalnutritioninchildrenaged6-59months(Gaboulaud,
Dan-Bouzouaetal.2007).Inthisstudy,ready-to-usetherapeuticfoods(RUTF)were
distributedinhouseholds,weekly,whereparentswereinstructedtoprovidethreedaily
mealsandtwoadditionalpacketsoftheRUTF.Mealpreparationdemonstrationswere
organizedformothersatfollow-uphomevisitsforthoseassignedtothehomevisiting
group.InIndia,assignmenteithertothesupplementationgroupornutritionaleducation
groupresultedingreaterweightgainineitherinterventionrelativetothecontrolgroups
(Bhandari,Bahletal.2001).Bothprogrammeswereimplementedduringthetoddleryears
(between12-36months),onaverage,andbothprogrammesemployedprimarilydidactic
instructiontoincreaseweightgain.Dosagevariedacrossbothstudies.
Social Protection Socialprotectionprogrammessuchasconditionalcashtransfershave
beenshowntoimprovegrowthandanthropometry.Theparentingeducationcomponent
ofsuchprogrammeswaslessexplicitalthoughitwasincludedintheprogrammatic
strategy.Conditionalcashtransferprogrammesprovidemonetaryaidtofamiliesundera
contractorsetofconditions(Lindert,2005).Theconditionalcashtransferprogrammein
MexicocalledPROGRESAtargetedruralareasandwasexpandedtourbanareasundera
newname,Oportunidades(Levy,2006).Itincludedthedistributionofmicronutrient
fortifiedfoodwithhealthservicesandcashtransfertools(Rivera,Sotres-Alvarezetal.
2004).Fromanequityperspective,thePROGRESAevaluationisimportantbecausethe
nutritionalcomponentoftheprogrammeisintendedforlow-incomehouseholdsin
underprivilegedcommunitiesofSouthCentralMexico.Inourreviewoftheacademic
literature,evaluationoftheMexicanprogrammeappearedastheonlymodelof
conditionalcashtransfersthattargetednutritional

46
practicesandthatprovidedparentingeducationforcaregiversofyoungchildren.The
evaluationoftheprogrammedemonstratedthatchildrenwhowereeligibleforandenrolled
intheprogrammehadanimprovedgrowthadvantage.Inparticular,theevaluationfound
thattheeffectonheightwasstrongerininfantsyoungerthan6monthsatbaselinewholived
inthepooresthouseholds.Theparentingeducationcomponentconsistedofmandatory
sessionsonpre-andpostnatalcareaswellasnutritionandhealtheducationinadditionto
mandatoryimmunizationandwell-babycareandgrowthmonitoringsessions.
Hygiene Promotion Intermsofmorbidity,prevalenceofdiarrhealdiseaseisoften
includedasaprimaryoutcomeofinterest.Diarrhealdiseaseisasignificanthealthburden
causinganestimated1.3milliondeathseachyearinchildrenyoungerthanfiveyearsofage
(Black,Cousensetal.2010).Long-termeffectsofdiarrheaincludedecreasedphysical
fitness,delayedschoolentry,andpoorschoolperformance(Guerrant,Koseketal.2002).
Althoughcausesofinfectiousdiarrheavary,inLMICs,pathogentransmissionoccurs
primarilythroughcontactwithcontaminatedwater,viruses,andbacteria,oftenleadingto
fluidloss,dehydration,andmalnutrition(Santosham,Chandranetal.2010;Alkizim,
Mathekaetal.2011).Interventionsthatpreventthetransferofpathogens(i.e.,hygiene
promotionsuchashand-washing),increaseimmunity(i.e.,breastfeedingpromotion),and
promotethetimelyuseoftreatments(i.e.,oralrehydrationtherapy,zincsupplementation)
arecriticaltoreducingmorbidityandmortalityassociatedwithdiarrhealdiseasesamong
newborns,infants,andyoungchildren(BajaitandThawani,2011;Lamberti,Walkeretal.
2011).InPakistan,thehandwashingpromotioninterventionconsistedofthreecomponents:
demonstrations,discussionsbeforeandduringtheintervention,andpostersasrewardsfor
householdsusingsoap(Luby,Agboatwallaetal.2004).Resultsfavoredtheintervention
groups(familiessuppliedwitheitherregularorantibacterialsoap)overthecontrolgroup
withrespecttoreductionintheprevalenceandseverityofdiarrhea.Nodifferenceswere
notedwitheitherinterventiongroup,suggestingthatpromotingtheuseofeitherregular
orantibacterialsoapisaneffectivestrategyinreducingdiarrhealdiseaseinyoungchildren.
47
Breastfeeding Promotion and Comprehensive Health and Nutrition Ourfindings
revealedthatotherthanhygienepromotionprogrammes,breastfeedingpromotion
programmeshavebeenshowntolowertheratesofdiarrhea(Bhandari,Bahletal.2003)and
otherneonatalorearlychildhoodmorbidities(Sripaipan,Schroederetal.2002;Bang,
Baituleetal.2005).Moreover,breastfeedingpromotionprogrammeshavebeenfoundtobe
effectiveinimprovinganthropometricmeasureswhenbreastfeedingpromotionis
combinedwithotherinterventionapproachessuchascaregiversupport(leRoux,leRouxet
al.2010)orotherformsofcomprehensivehealthapproaches(Sripaipan,Schroederetal.
2002;Saleemi,Zamanetal.2004;Bang,Baituleetal.2005;Bang,Bangetal.2005;
Kalimbira,MacDonaldetal.2010).Forinstance,thePhilaniinterventioninSouthAfrica
stressedtheroleofrespectfulandcaringrelationshipsbetweenMentorMothersand
caregiversinadditiontoprovidinghome-basedcounseling(leRoux,leRouxetal.2010).
Indeed,thedynamic,rapport,andpersonalconnectionbetweencaregiversandprogramme
providersarekeyingredientstoprogrammaticsuccess(Forry,Moodieetal.2011).
Elsewhere,onelarge-scalehome-basedneonatalcareprogrammeinIndiaprovidesservices
topregnantwomenwhoreceivehealtheducationonthermalcare,preventionand
managementofinfections,managementofneonatalsepsis,andhealth-seekingbehaviors
inadditiontobreastfeeding(Bang,Baituleetal.2005;Bang,Bangetal.2005).Among
breastfeedingpromotionprogrammes,theprimarydeliveryformatwashomevisitsand
programmedosewasgenerallyintensive,lastingatleastuptooneyear.InIndia,local
villageworkersbelongingtotheIntegratedChildDevelopmentServicesscheme,thelargest
multi-sectoralmaternalandchildhealthandnutritionprogrammeintheworld(Kapil2002),
auxiliarynursemidwiveswhoranimmunizationclinics,andotherhealthcareproviders
(IMCI-trained)visitedmotherswithlowliteracylevels,monthly,foroneyear;thiswas
supplementedwithmonthlyneighborhoodmeetingstoreinforcethebreastfeeding
messagesledbycommunityrepresentatives(Bhandari,Bahletal.2003).InPakistan,
monthlyhomevisitslastedupto2years(Saleemi,Zamanetal.2004).Acrossthesestudies,
trainedparaprofessionalsdeliveredtheintervention.
Oral Health Care Education hasnotbeenamajorareaofinquiryintheearlychildhood
literatureinLMICeventhoughitisakeycomponentofoverallphysicalwell-being.Inthis
review,
48
twostudiesthatexaminedoralhealthoutcomesinyoungchildrenwereconductedinIran
(Mohebbi,Virtanenetal.2009)andBrazil(PereiraandFreire2004).Whereasboth
programmesfoundimprovementsintheincidenceofdentalcaries,programmemodalities
differed.IntheIranstudy,thestrategyincludedeitherdeliveryofpamphletswith
informationonfeedinghabits,sugarintake,bacteriatransmission,andoralhygiene
(“pamphletgroup”),and/orthreebi-monthlyphonecallsdeliveredduringa6-monthperiod
remindingparentsoftheoralhealthinstructionsdeliveredbyclinicstaff(“pamphlet+
reminder”).Whilethepamphlet+remindergrouphadfewerchildrenwithdentalcaries
thanthecontrolgroup,thepamphlet-onlygroupdidnotdifferwiththecontrolgroup,
signifyingthefrivolityofhandingoutpamphletsinimprovingoralhealthoutcomes.Inthe
Brazilstudy,parentsattendedthreeweeklysessionsonoralhealtheducationdeliveredby
traineddentistsandhygienists,whichresultedinadecreaseinthenumberofchildren
classifiedunderthehighcariesriskgroup.Whatwascommonbetweenthetwostudieswas
theywerebothdelivereddidacticallytoindividualparentsandwereoflowdose(three
sessionsorremindercalls).
Summary Amongstudiesthatreportedsignificantchildphysicalwell-beingoutcomes,our
findingsrevealedthatchildnutritionandgrowthareimprovedthroughseveraltypesof
parentingprogrammes:micronutrientsupplementationprogrammes,nutritioneducation,
andcomprehensivehealthandnutritionprogrammes.Toreducetheincidencesofearly
childhoodmorbiditiesespeciallydiarrhea,effectiveparentingprogrammesincludedhand
washingandbreastfeedingpromotionprogrammes.Homevisitationbytrained
paraprofessionalswasthepredominantformatamongprogrammesthatimprovegrowthor
healthoutcomes(non-oralhealth).
Moreover,findingsshowedthatgroupsettingsmustbecombinedwithothermodalitiesto
bemosteffective.Dosageshouldalsoberelativelyintensive,lastingatleastoneyearona
monthlybasis.Thesefindingssuggestthatbyhavingparentsexposedtomultiple
modalitiesforalongperiodoftime,themessageofappropriateandadequatenutrition
getsreinforced.Bycontrast,programmesthataimedtoimproveoralhealthcouldbe
didacticandsignificantlylessintensivealthoughpreferablydeliveredbytrained
professionals.In
49
termsofdevelopmentaltiming,theaverageageattimeofinterventionwasprimarily
duringthefirstyearoflifetothetoddleryears(12-36months).
Asexpected,amajorityoftheinterventionstargetedthemostvulnerablepopulations.
Programmeslikeconditionalcashtransferstargetthemostvulnerableandaretherefore
potentiallyeffectivemechanismstodeliverparentingeducationtothesepopulations.
FurtherresearchisneededtoaddressthefeasibilityofintegratingexplicitECDparenting
educationintoconditionalcashtransferprogrammesandassesstheirimpactsonimproving
ormediatingtheeffectsofcashtransfersonoutcomes.Theimpactsofthisapproachon
otheroutcomedomainsarereportedinothersectionsofthisreview.3.2.1.2 Child Cognitive Development (n=6)
Sixstudiesemergedthatshowedsignificantimpactsoncognitivedevelopment.Thesample
sizesrangedbetween103and13,889children(median=139)infivecountries:twofrom
JamaicaandoneeachfromBelarus,Brazil,SouthAfrica,andTurkey. Thesettingsinwhich
theprogrammestookplacewerehome-based,primaryhealthcaresettings,andhome-and
community-basedsettings,whichincludedhomevisitsoracombinationofhomevisitsand
groupsessions.
Psychosocial Stimulation Exceptforonestudy,theprimaryprogrammaticapproachwas
psychosocialstimulation(SeeTable4inAppendix1).Inthisapproach,primarycaregivers
aretaughttheimportanceofarangeofbehaviorsandskillsnecessarytosupportchildren’s
non-health-relateddevelopmentaloutcomes.Theseincludelearningtheimportanceof,and
usingskillsthat,promotepositiveparent-childinteractionswithchildren,providingpositive
attentionandresponsivenesstodevelopmentalmilestonesandcues,encouragingchildren’s
autonomyandexplorationoftheirenvironment,andpromotingattachment(Engleand
Lhotska,1999).Inlowresourcesettings,suchasthoseincludedinthisreview,psychosocial
stimulationactivitieswereintegratedintoafamily’sdailyroutineandcapitalizedontheuse
ofrecyclablematerialstocreatetoysforyoungchildren.
50
Two examples of psychosocial stimulation programmes that combined home visits with
groupsessionswereconductedinTurkey(Bekman,Koçetal.2004)andinBrazil(Eickmann,
Limaetal.2003),theonlynon-RCTstudiesunderthecognitivedevelopmentcategory.
TheTurkishstudycombinedasummerpreschoolprogrammewithaparentingeducation
programmeformothers.Thetopicscoveredwerebroad,addressingtheholisticneedsof
youngchildren.Theparentingeducationprogrammelasted12weeks.Mothersmetonce
aweekfor2.5hoursandwereexpectedtoengageinpracticessuchasstory-tellingand
creativeactivitieswiththeirchildren,aswellasreinforcelessonschildrenlearnedintheir
preschool.Thepreschoolteachersalsoconductedhomevisitstoprovidefeedback.
InBrazil,onecommunity-basedinterventionwithahomevisitationcomponentconsisted
ofaninitialhomevisit,three3-hourworkshopsthatalsoprovidedrefreshmentsand
transportation,and10reinforcementhomevisits(totalof14contactswhenchildrenwere
betweenages13and17months).ResultsoftheTurkishandBrazilianstudiesshowed
impactsonschoolreadinessandlanguageskills(Bekman,Koçetal.2004)andmentaland
psychomotorskills(Eickmann,Limaetal.2003).
Otherprogrammescombinedpsychosocialstimulationwithnutritionsupplementation.
Twofollow-upRCTsinJamaicatestedtheefficacyofnutritionalsupplementationand
psychosocialstimulation(separatelyorcombined)inimpactingcognitiveoutcomesin
malnourishedpopulations(Gardner,Powelletal.2005;Walker,Changetal.2005).Both
studiesshowedthatsupplementationwaseffectiveinimprovingchildren’scognitive
outcomesonlywhenitwascombinedwithpsychosocialstimulation;thatis,nutritional
supplementationalonewasineffectiveinimprovingcognitivedevelopment.
Thetrainingandcredentialsoftheprogrammeprovidersweremostlytrained
paraprofessionals,althoughtwostudiesemployedprofessionals(e.g.,BrazilandSouth
Africa).IntheBrazilianpsychosocialstimulationstudy,occupationaltherapistswith
specializationsinchilddevelopmentdeliveredtheworkshopswhereastrained
paraprofessionalsperformedthehomevisits(Eickmann,Limaetal.2003).InSouthAfrica,
51
theprogrammeemployedatrainedphysiotherapisttodelivertheprogrammetolow-
incomefamilieswithyoungchildren,agesbelow2.5years,infectedwithHIV(Potterton,
Stewartetal.2010).Inthatstudy,overa12-monthperiod,thehomestimulationcurriculum
wasupdatedeverythreemonthstomatchwiththechild’sdevelopmentallevel.Although
thestudyrevealedgreaterchangeinprogrammechildren’smentaldevelopment(measured
usingBayleyScalesofInfantDevelopment—2ndedition)thancontrolchildren,the
programmechildren’smentaldevelopmentwasstillsignificantlydelayedcomparedtothe
normalpopulation.Moreover,theprogrammehadnoimpactonchildren’santhropometry.
Apartfrompsychosocialstimulationasaprogrammaticapproachinimprovingcognitive
outcomes,onestudyexaminedthelong-termimpactofabreastfeedingpromotion
programmeoncognitivedevelopment.ThisstudywasknownasthePromotionof
BreastfeedingInterventionTrial(PROBIT)interventioninBelarus,whichisthelargest
lactation-relatedRCTintheworldtodate(Kramer,Aboudetal.2008).Pediatriciansfrom
eachofthePROBIThospitalsandpolyclinicsreceivedan18-hourlactationmanagement
trainingcourse.Midwives,nurses,andphysiciansprovidedbreastfeedingsupportto
programmemothersduringlabor,delivery,thepostpartumhospitalstay,andduringvisits
tothepolyclinics.Atotalof17,046womenwithhealthyinfantswereenrolledand13,889
werefollowedupwhenchildrenwere6.5yearsofage.ResultsshowedthatPROBITchildren
scoredhigherthancontrolchildreninbothstandardizedtestsofintelligenceandteacher
ratingsofreadingandwritingperformance.
Summary Psychosocialstimulationprogrammes,whichentailactiveengagement
betweenthecaregiverandthechild,wereeffectiveinimprovingchildren’scognitive
development.Theseprogrammesinvolvedlivedemonstrationswithchildrenthroughplay
activitiesthataretailoredaccordingtothechild’sdevelopmentallevelandthefamily’s
individualneeds.Trainedparaprofessionalswereeffectiveprogrammeimplementers.
Althoughpsychosocialstimulationprogrammeswereeffectiveinimprovingcognitive
outcomeswhentargetingimpoverishedgroups,malnourishedchildrenstillperformedwell
belowtheirnon-impoverishedcounterparts.Theaverageageofinterventionwasaround
thetoddleryears.
52
Intermsofdose,psychosocialprogrammesaredeliveredideallyasintensivehomevisiting
programmesorasacombinationofgroupandindividualsessions.Programmesdelivered
aspartofhomevisitsranbetweenoneandtwoyearsatweeklyormonthlyintervals.
Programmesthatwereofshorterdurationcombinedearlyeducationwiththeparenting
programme,asinthesummerpreschoolprogrammeinterventioninTurkey(Bekman,Koç
etal.2004).Ofnote,noneofthestudiesreviewedofferedgroupsessionssolely.Basedon
onecommunity-basedprogrammeinBrazil,whenofferinggroupsessions(inadditionto
homevisits),itisrecommendedthattransportationandrefreshmentsareprovided.
Providingconvenientservices—suchaschildcareserviceswhileparentsareinattendance,
ortransportationservicesforruralfamilies—aswellasofferingprogrammesatconvenient
locations(e.g.,office,preschool,communitycenters)andtimes(includingeveningsand
weekendswhenthereisademand)areknowntoincreaseparticipationrates(Moran,
Ghateetal.2004).
Thereisalsostrongevidenceforcombiningpsychosocialstimulationprogrammeswith
earlyeducationprogrammesasdemonstratedintheTurkishstudy(Bekman,Koçetal.
2004).Thisisvalidatedinresearchemergingfromnon-LMICsuggestingthatmulti-
componentprogrammes—thoseinvolvingtrainingofchildren,teachers,andparents—are
effectiveinpromotingschoolreadinessskills(Moran,Ghateetal.2004,Reese,Sparksetal.
2010).Schoolreadiness,whichgenerallyreferstoayoungchild’scapacitytobereadyfor
bothlearningandperformingintheclassroom,includesfivedimensions:(i)physicalwell-
beingandmotordevelopment,(ii)socialandemotionaldevelopment,(iii)approachesto
learning(e.g.,enthusiasm,curiosity,taskpersistence),(iv)languagedevelopment,and(v)
cognitionandgeneralknowledge(Kagan,Mooreetal.1995).Theseskillsareimportant
precursorstolifelongsuccess.
Thereispreliminaryevidencethatnutritionalsupplementationalonemaybeinsufficientin
improvingcognitiveoutcomesinyoungchildrenasdemonstratedbythelongtermfollow
upoftheJamaicastudies.However,breastfeedingpromotioncouldbeaneffectivestrategy
inimprovingcognitiveoutcomes.Giventhatbreastfeedingpromotionhasalong-term
impactonchildren’sfullscaleIQandlanguagedevelopment,thissuggeststhat
53
breastfeedingpromotionistheearliestexplicitformofECDparentinginterventionthatis
effectiveinimpactingchildren’scognition,notjusttheirphysicalwell-being.3.2.1.3 Child Social and Emotional Development (n=2)
Youngchildren’ssocialandemotionalcompetence,inadditiontotraditionalintellectual
capacities,hasbeenshowntobeessentialnotonlyforsuccessinacademicsbutalsofor
successinadultlife(Brackett,Riversetal.2011,Durlak,Weissbergetal.2011).Promoting
youngchildren’shealthysocialandemotionalwell-beingisthereforeessentialinsetting
thestageforoptimaldevelopment.
Twoevaluations,TheRovingCaregiversProgrammeinSt.Lucia(Janssens,Rosembergetal.
2009),andthe17-yearfollowupoftheJamaicanpsychosocialstimulation+
supplementationstudymentionedpreviously(Walker,Changetal.2006)makeupthis
sectionofthereview.Bothprogrammeswereintensive.TheRovingCaregivers
Programme,whichwasbothahomevisitingandgroup-basedprogrammetargeted
vulnerablefamilieswithchildrenages0-3andconsistedoftwiceweeklyvisitations
lasting45minutespersessioninadditiontomonthlyparentingmeetings.The
Jamaicanstudyconsistedofweekly1-hourhomevisitsfortwoyears.Participationin
bothprogrammesresultedingreaterinterpersonalskillsandself-esteemandlesser
anxietyanddepression.Althoughnoimpactswerefoundforexternalizingbehaviors
(antisocialbehavior,hyperactivity,andoppositionalbehaviors),participationin
programmeduringtheearlyyearsresultedinlowerlikelihoodofbeingsuspendedor
expelledfromschool.
AlthoughonlytwostudiesfoundsignificantimpactofECDparentingprogrammeson
children’ssocialandemotionaldevelopment(SeeTable4inAppendix1).),thisdoesnot
meanthattheseweretheonlytwostudiesthatexaminedthisoutcomedomain.Inthenext
section,weexamineholisticoutcomes,whichpertaintostudiesthatfoundECDprogramme
impactsacrossmultipledevelopmentaldomains,includingsocialandemotional
development.
54
3.2.1.4 Holistic Outcomes (n=6) Sixstudies,implementedinfivecountries(twoeachinJamaicaandMexico,andoneeachin
thePhilippinesandVietnam),consistedofsignificantoutcomesinmorethanonechild
developmentaloutcomedomain,suchashealth,socialandemotional(SeeTable4in
Appendix1).Thenumberofchildrenevaluatedrangedbetween140and7,922
(median=1,019).Allbutoneofthesixstudiesemployedrandomassignment(fourRCTsand
tworandomassignmentwithnocontrolgroup).Interventionapproachesinvolved
psychosocialstimulation,integratedhealth,nutrition,anddevelopmentinterventions,and
socialprotectionprogrammes.
Psychosocial Stimulation OnesuchpsychosocialstimulationprogrammeinJamaica
(twostudies)wasderivedfromWHO’sProgrammefortheEnrichmentofInteractions
betweenMothersandChildren,whichtargetedlowbirthweightchildrenbetween9-24
monthsofage(Gardner,Walkeretal.2003,Walker,Changetal.2010).Trainedfemale
paraprofessionalsconductedeightweeklyhomevisits(1hour/visit)toplayandtalkwith
childrenandteachmothershowtoengagetheirchildrenthroughtalking,singing,and
showingaffection.Duringthesecondphase,from7-24months,thetrained
paraprofessionalsconducted30-minuteweeklyhomevisits. Attheendofthe8-week
period,interventioninfantsexhibitedmoremeans-endproblem-solvingbehaviors(as
measuredbyaPiagetianproblem-solvingtaskwhereinfantsuncoveredahiddentoyor
retrievedadistanttoy)andwereratedhigherincooperationandhappinessbytrained
observerscomparedtocontrolinfants(Gardner,Walkeretal.2003).Inthesix-yearfollow-
upofthatstudy,interventionchildrenscoredhigherinmentalacuity(performance
subscaleoftheWPPSIandCorsiblockdesign)andlowerintotalbehavioraldifficultiesthan
controlchildren;however,nolong-termimpactswerefoundforthefullandverbalscalesof
theWPPSI,thePPVT,attentionalcapacity,andreadingachievement(Walker,Changetal.
2010).Thesefindingsdemonstratethatintensivepsychosocialstimulationprogrammeshave
long-termimpactsonchildren’scognitiveandsocialandemotionaloutcomes.

55
Integrated Health, Nutrition, and Child Development programmeshavelikewise
beensuccessfulinimpactingchildren’sholisticdevelopment.Inlinewiththenotionofthe
wholechildapproach,integratedprogrammesareusuallymulti-sectoralprogrammesthat
aimtodeliverabroadersetofECD-relatedservicestofamilieswithyoungchildren.
TwostudieswereconductedinSoutheastAsiaandtargetedthemostdisadvantaged
communities.Thelarge-scalePhilippineECDprogrammedeliveredacombinationof
center-based(e.g.,daycarecenters,preschools,healthcenters)andhome-based(family
daycareprogrammesandhomevisitsbyhealthworkers)services(Armecin,Behrmanetal.
2006).Tolinkthecenter-andhome-basedservices,childdevelopmentworkers(CDWs)
complementedtherolesofmidwivesandhealthworkersinprovidingfoodandnutritional
supplementsandmonitoringchildren’shealthstatus.CDWsalsoprovidedcommunity-
basedparentingeducationaboutECD.Programmechildrenperformedbetterthannon-
programmechildrenincognitiveskills,grossandfinemotorskills,expressiveandreceptive
language,andsocialandemotionalskills.Amongtwo-andthree-year-oldsexposedtothe
programme,Z-scoreswereone-halfto1.8ofastandarddeviationhigherformotorand
languagedevelopment(Armecin,Behrmanetal.2006).Moreover,therewerelower
proportionsofanemiaandlowerratesofwastinginprogrammeareasthaninnon-
programmeareas.Positiveprogrammeimpactsvariedbyage,butweremorepronounced
forchildrenyoungerthanagefour.
InruralVietnamwheretherewasahighprevalenceofstunting,SavetheChildrenJapan
implementedamulti-sectoralinterventionfortwoyears(Watanabe,Floresetal.2005).The
interventionhadtwocomponents.Thenutritioncomponentincludedbi-monthlygrowth
monitoringforallchildrenandninesessionsofa12-daynutritioneducationrehabilitation
programmeconductedeverymonthtargetingseverelymalnourishedchildren.TheECD
componentprovidedmaterialsupportandteachertrainingonchild-centeredpedagogy.
Thisalsoincludedestablishingsmalllocallibrariesforparentsandpromotedplayareasin
homes.Furthermore,whatisuniqueaboutthisinterventionisthatittargetedfathers
explicitlyinadditiontotargetingmothers.TheECDcomponentprovidedsupportforparents
throughaone-daytrainingsessionforfathersandmothersseparatelyeverymonth
56
onvarioustopicsonchildcareanddevelopment.Resultsrevealedthatbothprogrammatic
componentsresultedindecreasesinstunting,butresultsfavoredtheECDcomponent+
nutritioncomponentgroupindecreasingseverestuntingoverthenutritioncomponent
onlygroup.Moreover,comparedtothenutrition-onlygroup,theECDcomponent+
nutritioncomponentgroupperformedhigherinstandardizedtestscoreswheremore
pronounceddifferenceswerefoundforstuntedchildren.Thesefindingssuggestthatan
integratedapproachtochilddevelopmentyieldseffectsonthewholechildandthathigh-
riskchildrenbenefitthemost,promotingequity.Moreover,dosagefindingssuggestthat
nutritionprogrammesareinsufficientinimpactingmoreholisticoutcomes.
Social Protection theMexicanOportunidadesmentionedpreviouslyhasbeenthemodel
conditionalcashtransferprogrammeinLatinAmerica.Inthenextsetofevaluationsthat
werefive-(Fernald,Gertleretal.2008)and10-year(Fernald,Gertleretal.2009)follow-up
studiesofOportunidades,dose-responseanalysescomparingearly(familiesenrolled
immediatelyintoprogramme)andlate(familiesenrolled18monthslater)enrollment
favoredearlyenrollmentacrossphysical,cognitive,andsocialandemotional
developmentaloutcomes(Fernald,Gertleretal.2008;Fernald,Gertleretal.2009).Inthe
10-yearfollow-up,however,greaterprogrammedosedidnotsustainitsadvantagein
height-for-agezscores,bodymassindex,andcognitiveandverbalassessments(Fernald,
Gertleretal.2009).
Summary Holisticprogrammingbegetsholisticoutcomes.Ideallyinterventionsshould
takeonawholechildapproach.Theresearchsummarizedinthissectionsuggeststhat
effectiveapproachestoimprovingholistichealthanddevelopmentaloutcomesinchildren
couldbeintheformofmulti-sectoralhealthandchilddevelopmentalprogrammes(asinthe
examplesofscale-uporlarge-scaleprogrammesinMexico,thePhilippines,andVietnam)or
intensivepsychosocialstimulationprogrammes.Theformerapproachisefficientand
effectiveinimprovingahostofchildoutcomes.Thelatterentailsfrequentinteractionswith
caregiversandtheirchildren,lastingbetweenoneandtwoyears.Acrossstudies,itappears
thatdoseisimportant.Forexample,intheMexicanOportunidadescashtransfer
programme,participatingintheprogrammeforanadditional18monthswasadvantageous
intermsofimprovingchildoutcomes.Hiringwell-trainedparaprofessionalswasacost-

57
effective
57
solutiontodeliveringmessagestoparents.Malnourishedchildrenandyoungeragegroups
benefitedthemostfromtheseprogrammes.Thissuggeststhatcaregiversmaybeutilizing
themoneytheyreceivetoenrolltheirchildreninbetterqualitycarethroughgrowth
monitoring,wellbabyvisits,andparticipationinparentinginterventions,whichweresome
oftheconditionsforenrollmentinOportunidades.Futureevaluationsshouldexamine
parentalactivitiesafterprogrammeenrollment.
AsevidencedintheVietnamstudy,includingfathersinthetrainingsisapromisingand
underutilizedstrategy(Barker,Bartlettetal.2004,UnitedNationsDepartmentof
EconomicandSocialAffairs2011).Indeed,findingsfromhigherincomecountries
demonstratedstrongereffectsonbothchildandparentingbehaviorswhenfatherswere
involvedintheprogramme(Lundahl,Tollefsonetal.2008).ConductingECDparenting
programmesthattargetfathersexplicitlyaresuggestedforfutureresearch.
3.2.2PARENTOUTCOMES
Thissectionsummarizes33studiesthatshowedsignificantimpactsonresultsforparenting
onlyintheareasofparentingattitudes,beliefs,andpractices.Thesectionisdividedinto
thefollowingbroadcategories:(1)caregivingpertainingtopromotingchildren’sphysical
healthandnutritionalstatusand(2)caregivingbeyondphysicalcare.
3.2.2.1 Physical Health-Related Caregiving (n=19)
Earlychildhoodparentingprogrammesthatevaluatedcaregivingknowledge,attitudes
andpracticestoimprovephysicalhealthappeartobewidelyimplemented.Herein,we
definephysicalhealth-relatedpracticesasthosethathavebeenshowntoreducedisease
prevalenceandpromotegrowthandphysicalwellbeingamongyoungchildren.Atotalof
20studiesaddressedfouroverarchingstrategiestopromotephysicalwellbeingby
targetingparentaloutcomesinrelationto(1)healthcareseekingbehaviorsandhygiene
practices,(2)oralhealth,(3)nutritioneducation(aloneorintegratedwithotherhealth-
relateddimensions),and(4)carepractices.Programmeevaluationsrangedfrom
moderate
58
(n=129)tolarge(universal)coverage.Mostevaluations(20%)wereconductedinIndia.
African(Belize,Nigeria,SouthAfrica,Burkina,Malawi),Asian(China),SouthAsian(Nepal),
SouthEastAsian(Bangladesh,Thailand),andLatinAmericanandtheCaribbean(Haiti,
Brazil)regionswerealsorepresentedintheprogrammeevaluationsreviewed.
Theoverviewofprogrammesindicatedthatparaprofessionalsandacombinationofservice
deliverymodalitiesarecommonlyusedwhenpromotingphysicalchildhealthand
caregiving.Themajority(65%)ofinterventionsweredeliveredbyparaprofessionalssuchas
localcommunitymembersandcommunityhealthworkers.Professionalsdelivered20%of
theinterventionsand10%ofthereportsdidnotspecifytheserviceproviderswhodelivered
theintervention.Mostservicedeliverymodalitiescombinedmorethanoneapproach(e.g.,
useofprintmaterials,modeling,discussion,activeinstructionorteaching,mediaand
communityevents)withtheexceptionoftwoprogrammesthatonlyutilizedalecture
strategy. Deliverysettingsalsovaried,withcommunitybased(35%)andhomeand
community(30%)beingthemostcommonformsofprogrammedelivery.Mosttrials(40%)
usedrandomassignment,followedbynon-randomassignment(35%).Qualityofthe
programmeevaluations,asrevealedbyourqualityscoring,variedconsiderably(cumulative
scoresrangedfrom29.4to82.35).Thesectionsbelowsummarizethefindingsofthe
programmeevaluationstoassesswhatprogrammecharacteristicsareassociatedwith
positiveparentaloutcomeswithaspecialemphasisoncommonlyreportedapproachesto
culturalresponsivityintheprogrammaticdesign.
Healthcare seeking behaviors and hygiene practices Studiesinvestigatedthe
effectsofECDparentingprogrammesonhealthcareseekingbehaviorsandhygiene
practicesassociatedwithmalaria,diseaseandacuterespiratoryinfectionmanagement
(Cropleyetal.,2004;Okeke,2009;Holloway,etal.,2009;Mohanetal.2004;Curtis,et.al,
2001;andLuby,etal.,2010).ThekeycharacteristicsofthesetrialsaredisplayedinTable4
inAppendix1.
59
BelizeandCropleyetal(2004)examinedtheeffectofhealtheducationinterventions
deliveredbyparaprofessionalsonmothers’treatment-seekingbehaviorsfortheirchildren’s
malariafevers.Interpersonalchannels(e.g.voluntarycollaboratorsandvectorcontrolteam
personnel)contextualizedanddisseminatedthemessagesalongwithvisualmaterialsof
classicmalariasymptomsandrecommendedactions(e.g.displayedpamphletsandposters).
Post-interventionsurveysrevealedthatinterpersonalcommunicationimprovedsome
proxiesofhealthcareseekingbehaviorsintheinterventionbutnotinthecontrolgroups
(e.g.seekingmalariatreatmentwithin48hoursofthefirstrecognitionoffever).Knowledge
ofmalariacauses,symptomsandtreatmentalsoimprovedinresponsetotheintervention.
Thestudywasunabletoprovideevidencethatthevisualmaterialspositivelyinfluenced
treatment-seekingbehaviors.Educationandcommunicationmaterials,whichincluded
postersdepictingachildwithmildandseveremalariawithalistoftheclinicalsymptoms,
wereusedinNigeriatoimproveknowledgeofcauses,andcareformoderateandsevere
malaria(Okeke2009).Theinterventionwasacombinationofmassmedia,community-
basedactivities,andtrainingactivitiesbyleadersofwomengroups.18monthsafterthe
intervention,therewasasignificantincreaseintheknowledgeofsymptomsofmildand
severemalariaandtargetedhealthcareseekingpractices.
NepalandHollawayetal(2009)evaluatedtheimpactofamulti-modalinterventioninthe
treatmentofacuterespiratoryinfection.Messagestargetedknowledgeonsymptoms
indicativeofillnessandcorrespondingtreatmentprocedures.Professionalsand
paraprofessionalsdeliveredsmallandlargegroupactivitiesandone-to-onecounseling
sessions.ResultsvariedaccordingtoseverityofAcuteRespiratoryInfection(ARI)and
outcomeofinterest.Forinstance,attendanceathealthpostsincreasedforsevereARIand
fellinchildrenwithmildARI.Althoughthestudyprovidesimplementationstrategiesthat
utilizelocalservicedeliveryinfrastructureindifficultcircumstances,furtherresearchis
neededtoassesstheimpactofdisseminationstrategiesthatonlyusevisualmaterialsand
addresssymptomsofdifferingseveritieslikeARI.
AparentingeducationprogrammewasconductedinruralIndiatoassessiftrainingdoctors
incounseling,communicationandclinicalskillsusingthe(IMCI)approachimprovedcare
60
seekingbehaviorsinfamiliesofsickchildren(Mohanetal.,2004).Theobjectiveofthe
counselingsessionswasprimarilytoteachmothersofchildrenunder-5yearsofagetoseek
promptcareuponpresentationofdangersigns.Comparedwithcontrolsites,mothers’
acknowledgementoftheneedtoseektimelyandappropriatecareincreased,buttherewas
nosignificantdifferenceincareseekingbehaviors.Theauthors’hypothesizedchangesin
behaviormayrequireprolongedexposuretotheeducationalmessages.
Hygienepracticesweretargetedtoreducetheriskofdiarrhealdiseasesandfood-borne
illnesses.InBurkinaFaso(Curtisetal.,2001)andBangladesh(Lubyetal.,2010),
programmestargetingbehaviorsassociatedwithhygieneandhandwashingpractices
wereevaluated.Bothprogrammesutilizedacommunity-basedapproach.InBurkina,a
combinationofmonthlyhouse-to-housevisits,weeklyplay,discussiongroupsin
communityhealthcenters,andradiospotstargetedstoolmanagementpractices.In
Bangladesh,fieldworkersintroducedsoaporsanitizerandwereinstructedtowashhands
afterseveralexposures.Instructionwascomplementedwithpositivereinforcementby
encouragingparentsinthecompoundtosupporteachothertoimprovehandhygiene,
andbyplacingpostedrecognitionstickersinhouseholdsthatusedmostsoap/sanitizer.
TheBangladeshinterventiontookintoaccountlocalcustoms(e.g.sanitizeruseddidnot
containalcoholbecausemanyMuslimsinBangladesharereluctanttouseproductsthat
containalcohol).After3-yearsofimplementingtheprogrammeinBurkinaFaso,the
evaluationrevealedgreatestimprovementsin2outofthe4targetbehaviors(hand-
washingwithsoapaftercleaningachild’sbottomandtheproportionofmotherswho
washedtheirhandswithsoapafterusingthelatrine).InBangladesh,theevaluation
showedthatwaterlesshandsanitizerwasreadilyadoptedbythecommunityandreduced
handcontamination.However,itdidnotimprovethefrequencyofhandwashing
comparedwithsoap.
Oral Health TwoprogrammeevaluationsinIndia(Nairetal.,2009)andThailand
(Vachirarojpisan,Shinada,&Kawaguchi,2005)assessedtheeffectofeducation
interventionsinparentaloralhealthknowledgeorpractices.InThailand,astudytestedthe
effectsofactiveinvolvementusingaparticipatorydentalhealtheducation(participatory-
DHEprogramme)comparedtoanationalteachingDHEprogramme.Intheparticipatory

61
DHEgroup,atrainedmoderatordeliveredsmall-groupsessionsonceamonthduringa3-
month
61
participatorydentalhealthprogramme.ThenationalDHEprogrammeconsistedofdidactic
teachingaboutearlychildhoodcaries(ECC)preventionmethodsandprovidingfree
toothbrushes.TheparticipatorycomponentoftheDHEprogrammewasassociatedwith
improvedoralhealthpracticessuchasparentsbrushingchildren’steethandusingtheright
amountoffluoridetoothpaste.However,therewerenodifferencesintheincidenceof
cavitiesbetweenparticipatoryandnon-participatoryDHEprogrammegroups. InIndia,
publichealthnursesandcommunityhealthworkersfacilitatedoralhealthclasseswith
mothersduringgroupmeetings.Audiovisualaids,modules,charts,postersandbrochuresin
theregionallanguagewereutilized.Resultsrevealedastatisticallysignificantimprovement
inknowledgeregardingoralhygienehabits,importanceofmilkteeth,causesofdental
diseases,preventionofdentaldiseases,andtreatmentofsomedentalconditions.
Nutrition education Nutritioneducationinterventionsencompassawidevarietyof
approaches,includingcounselingaboutchildfeedingaloneorincombinationwithfood
supplementation,fortificationofcomplementaryfoods,andfoodpreparationtechniquesto
maximizenutrientquality.InSouthAfrica(Faber,Venter&Benade,2002)andBurkinaFaso
(Nanaetal.,2006),nutritioneducationinterventionswereevaluatedtotesttheirimpacton
vitaminAintakeandserumretinolconcentrationinchildren.Bothinterventionsused
contextualizedapproachesandtestedtheimpactoflocallyavailablefoodsorutilizinghome
gardenswithproducewithhighvitamin-Acontent.InSouthAfrica,demonstrationgardens
werecombinedwithacommunity-basedgrowth-monitoringprogramme.Oneyearafter
theintervention(whichincluded12trainingsessionsinthedemonstrationgardengiven
duringmonthlygrowthmonitoringsessions),vitaminAintakewashigheramongboth
interventionandcontrolgroups.However,theincreasewasgreaterinchildrenfromthe
interventiongroup.Theauthorshypothesizedthatcontrolgroupeffectscouldbeexplained
byanincreasedawarenessinthecommunitythatresultedfromthevisibilityofproject
gardensanddemonstrationsaswellasthenutritioneducationprogramme.InBurkinaFaso,
theprogrammeevaluationassessedtheeffectivenessofabehaviorchangeapproach
throughpromotionalactivities,withorwithoutfinancialsupport,inimprovingvitaminA
intakeandserumretinolconcentrationthroughconsumptionoflocally-availablefoods
(mangoandliver).Overall,theresultsindicatedthatbothvitaminAintakeandserum
62
retinolconcentrationimprovedsignificantlybetweenthebeginningandtheendofthe
interventionregardlessofthepresenceoffinancialsupport.Intheabsenceofatruecontrol
group,itwasdifficulttofullyattributethisimprovementtotheintervention.
Nutritioneducationprogrammesdelivered,atleastinpart,byhealthserviceprovidersand
thattargetedparentalhealthknowledgeandhealth-seekingpracticeswerealsoevaluated.
Threestudiesassessedtheimpactofintegratingnutritionandchildcareeducationin
center,hospital,andcommunityhealthcenters.Theoutcomesassessedwereparental
knowledgeandpracticesand,insomecases,childhealthindicatorsandanthropometry.In
Bangladesh,levelsofchildhoodmalnutritionwerecomparedbetweenareaswherethe
IntegratedNutritionProjecthadbeenoperationalforover5yearsincommunitynutrition
centreswithmatchednon-projectareas(Hossain,Duffield&Taylor,2005).Duringmonthly
growthmonitoringandpromotionvisits,caregiversofchildren0-23monthsofage,
receivedcounselingonhealth,familyplanning,breastfeeding,caringpractices,personal
hygieneandtheuseofiodizedsalt.Self-reportednutritionalknowledgeamongmothersin
theinterventiongroupwassignificantlyhigherascomparedtothecontrolgroup,although
nosignificantimpactwasobservedinreducingmoderateandsevereunderweightof
children.However,theevaluationdidnotcontrolformalnutritionratesatthebeginningof
thetrial.InBrazil,physiciansweretrainedwithanIMCI-derivednutritioncounseling
protocolandretentionofmessageswasexamined(Pelto,etal.,2004).Theintervention
usedlocallyappropriatemessages,toolsforassessingindividualproblems,andcounseling
skillsofserviceproviders.Motherswhoreceivedadvicefromtrainedprovidershad
significantlyhigherratesofrecallingthemessagesonspecificfoodsandfeedingpractices
aswellasrecommendationsonfoodpreparationcomparedtothosewhodidnotreceive
advice.Theproportionofthemessagesrecalledonbreast-feedingdidnotdiffer
significantlybetweentheinterventionandcontrolgroups.Furthermore,resultsfroma
studyinMadagascarsuggestedthatimplementingtheEssentialNutritionActions(ENA)
operationalframeworkandBehaviorChangeCommunicationmayleadtosignificant
improvementsinsomechildfeedingandnutritionalpractices(breastfeedinginitiationand
continuationrates,feedingratesamongchildren6-23months,rateofmaternaliron-folic
acidandvitaminAsupplementationduringtheperinatalperiod)(Guyonetal.,2009).The
providersand
63
communityhealthworkersusedcounselingcards,newsprint,andchildhealthbooklets.
Recommendationsandnutritionmessageswereharmonizedwithvarioushealth
programmes(e.g.IMCI)andcomplementedwithmassmediaandothercommunity-based
activities.Noimprovementswerereportedinincreasingfoodintakeduringchildillnessor
pregnancy.
Programmeevaluationswerealsoconductedtoassesstheeffectivenessofpromoting
breastfeedingandfeedingpracticesthroughavailablehealth-deliverychannels.InIndia,a
trialevaluatedtheeffectsofdeliveringexclusivebreastfeedingandcomplementaryfeeding
practicesbytrainedhealthandnutritionworkers(Bhandarietal.,2005).Counseling
opportunitiesincludedvisitstophysicians,homevisits,andimmunizationandweighing
sessions.Anincreaseinthenumberofchannelsthroughwhichcaregiverswerecounseled
waspositivelyassociatedwithexclusivebreastfeedingprevalenceandconsumptionof
certaincomplementaryfoodsamongdifferentchildageranges.Additionally,intervention
areas,comparedwiththecontrolgroup,hadhighercoverageforvitaminAandironfolicacid
supplementation.AparticipatorynutritioneducationprogrammeinMalawiwas
implementedtointroduceavarietyofpracticesforimprovingcomplementaryfeedingHotz
&Gibson(2005).Workshops,demonstrations,andwrittenmaterialsweredevelopedand
communityHealthCommitteemembersandlocalMinistryofHealthSurveillance
Assistantsdeliveredthelocallyadaptedlessonsforcomplementaryfeedingpractices.The
studyindicatedthatthroughnutritioneducation,participatingmotherswereabletouse
existingfoodresourcestoimprovecomplementaryfeedingpracticesandthiswas
associatedwithenhancedadequacyofenergyandintakeofseveralmicronutrientsinthe
complementarydietsoftheirchildren.
InChina,townshiphospitaldoctorsweretrainedonchildnutrition,breastfeeding,
complementaryfeeding,andcounselingskills(Zhang,Shi,Chen,Wang&Wang,2009).
Participantsintheinterventiongrouphadsignificantlyhigherscoresthanparticipantsin
thecontrolgroupinknowledge,attitudes,self-efficacy,intention,normbeliefs,aswellas
feedingbehaviors.Thestudyfoundtheintervention,mothers’knowledge,intentionand
subjectivenormofvillagersindependentlypredictedmaternalfeedingbehaviorsafterthe
intervention.Theauthorsconcludedthattomotivatecaretakerstoadoptoptimalfeeding
64
behaviors,itwascriticaltoprovidethemwithnecessaryknowledge,information,skills,and
asupportiveenvironment.
Care practices:Estimatessuggestthatupto1/3ofneonatalmortalitycouldbe
preventedthroughhighaccessofpreventativefamilyandcommunitynewborncare
(Darmstadtetal.,2005).
Interventionstargetingcare-seekingbehaviorsimpactnotonlysurvivalbutalsophysical
outcomesanddecreaseinmorbiditiesthatcanaffectchildhealthanddevelopment.In
India,acombinationofmonthlycommunitymeetingsfromthe2ndto3rdtrimester,
antenatalhomevisits,andneonatalvisitswereimplementedtopreventhypothermiaand
modifypracticesandreducingneonatalmorbiditiesandmortalities(Kumaretal.,2008).
Twointerventions(apackageofessentialnewborncarewithorwithoutanindicatordevice
forhypothermia)weretestedagainstacontrolgroupwhoreceivedroutineservices.The
interventionwasassociatedwithimprovementsinprenatal(e.g.birthpreparedness)and
post-natal(e.g.thermal,umbilical,andskincare,andhygienicdeliveryandbreastfeeding)
carepractices.Care-seekingbehaviordidnotdifferbetweentheinterventionandcontrol
groups.Theprogrammewasassociatedwithasignificantreductioninchildmortality.
Socioculturalcontextualizationandacommunity-baseddesigntargetedtowardshigh-risk
newborn-carepractices,weresomeofthecharacteristicstowhichimpactsofthe
interventionwereattributed.
Acommunity-basedprogrammetargetedfathersthroughfather’sclubsinHaiti(Sloand,
Astone&Gebrian,2010).TheFather’sClubinHaiticonsistedofregularmeetingsamong
fatherstodiscusstheirinvolvementinchildcare.Theyalsoattendedhealtheducation
sessionswithinputfromthenurseorvillagehealthagentwhereseveralpractices(e.g.
exclusivebreastfeedingfor6months,immunizingchildren,andprovidingadequatefluids
andseekingappropriatehealthcarewhenthechildissick)werediscussed.Fathers’
knowledge,skills,andperformanceinearlychildhoodcareweretargeted.Thepresenceof
afathers’clubwasassociatedwithincreasedvaccinationstatus,growthmonitoring,and

65
vitaminAsupplementation.However,childmortalityratesandchildweightdidnotdiffer
beforeandaftertheinitiationoffather’sclubsinthevillages.Summary:Datafromtwostudiessuggestinterpersonalcommunicationofcontextualized
andtargetedmessagesmaypositivelyimpactparentalknowledgeandspecifichealthcare
seekingbehaviors.Oneofthecharacteristicsoftheinterventions,likelytobeassociated
withpositiveimpacts,wasspecificityofthehealth-relatedmessages.Interventionsthat
usedthelocalworkforcetodeliverkeymessages,suggestedthatparaprofessionalscan
impacthealthknowledgeamongparentsofyoungchildrenaloneorincombinationwith
professionals.Furtherresearchisneededtoassesstheimpactofvisualmaterialsalonein
healthcareseekingknowledgeandbehaviors.Ourreviewoftwoparentingprogrammes
targetinghygienepracticessuggeststhatprogrammescanbemoreeffectiveinpromoting
healthybehaviorsiftheyarebuiltonlocalresearchandusecontextualizeddissemination
channels.InBangladesh,(Lubyet.al.2010),thelarge-scale3-yearprogrammesuggested
thattheinterventionshouldbedeliveredrepeatedlyandforanextendedtimetoleadto
measurableimpactsatapopulationlevel.Furthermore,theBangladeshprogramme
suggeststhatuseofnewitems(likewaterlesshandsanitizers)toimprovehandwashing
practicesmaybemoreeffectiveinsettingswherewaterandsoapareunavailable.
Therefore,tomaximizetheimpactoftheintervention,designingeffectiveprogrammatic
strategiesshouldtakeintoaccountexistingpracticesandpreferences.
Theoralhealthprogrammeevaluationsindicatedthatoralhealthknowledgecanbe
strengthenedthrougheducationclassesledbyprofessionalsand/ortrained
paraprofessionals.Improvementinoralhealthknowledgecanbeattainedthrougharange
ofinterventiondoses,asillustratedbytherangeintheintensityoftheprogrammes.
Althoughaparticipatoryapproachtooralhealtheducationledtoimprovedoralhealth
practices,itdidnotcontributetoareductioninchildcaries.Furtherresearchisneededto
assesstheimpactofknowledgechangeonsustainedoralhealthpracticesandonoutcomes
foryoungchildren,andtheaddedvalueofactiveinvolvementinimprovingchildoralhealth
duringearlychildhood.
66
Withthenutritionaleducationprogrammes,vitaminAandretinolintakewereassessedto
testtheimpactofprogrammestargetedtocontextualizedfoodharvestingandpreparation
bycaregiversofyoungchildren.Resultswereinconclusiveinregardstotheimpactthat
gardeningactivitiesandfinancialsupporthavebeyondparentaleducationalone.However,
thetwocommunity-basedactivitiesevaluatedshowedmodesteffectsonvitaminAintake
suggestingthatbehavioralchangecanbeinstilledthroughcontextualizedapproachesthat
involvelocally-availablefoods.Resultsoninterventionsthatcombinednutritionaland
healthcareseekingeducationinhealthsettingsshowedthatself-reportednutritional
knowledge,messagerecallofsomefeedingpractices,andimprovementsinsomenutritional
practicescanbeimprovedviatrainedprofessionals.However,inBangladeshalthough
mothersinprojectareasreportedbettercaringpracticesthanmothersinthenon-project
areas,theimprovementsinself-reportedpracticeswerenotassociatedwiththenutritional
statusofchildren.Promotionofbreastfeedingandcomplementaryfeedingpractices
throughavailablehealth-deliverychannelsweresuccessfulinIndia,MalawiandChinawhere
existinghealthcarechannelswereusedtodelivermessagesandcounseling.InChina,
mediatorsofprogrammeeffectivenessincludedparticipantintentionandcontext.
Theeffectofparentingprogrammesoncarepracticesviaantenatalprogrammesand
throughacommunity-basedapproachweremixed.InIndia,althoughtherewasno
differenceincare-seekingbehaviorsbetweenthecontrolandexperimentalarms,the
interventionwasassociatedwithasignificantreductioninchildmortality.Thestudyresults
suggestthatmorefrequentexposuretoeducationalmessagesthroughawiderrangeof
channelsmayleadtogreaterchangesinmothers’care-seekingbehaviorsthanwe
observed.However,prenatalandneonatalcarepracticeswereimprovedinresponsetothe
interventionsuggestingthatsomepracticescanbemodifiedusingtheimplemented
strategies.Conversely,inHaitisometargetedcareandhealthcareseekingpracticeswere
improvedinresponsetoFathers’Clubs.Improvementsonthosepracticesdidnottranslate
todecreasesinchildmortalityrateorchangesinchildweight.Furtherinvestigationis
neededtoassesshowpaternaleducationandimprovedpracticestranslateintofavorable
childdevelopmentandhealthoutcomes.
3.2.2.2 Caregiving Beyond Physical Care (n=13) Theprogrammeapproachesemployedinthe13studiesthatdemonstratedimpactson
caregivingbeyondphysicalcarearecategorizedasfollows:(1)childprotectionintermsof
safetyandinjuryprevention,(2)childprotectionintermsofphysicalabuse,(3)psychosocial
stimulationandresponsiveness,(4)responsivefeeding3andintegratedhealthand
developmentapproaches.Programmeswereimplementedin11countries,almosthalfof
whichwereintheMiddleEast:threeinTurkey,andoneeachinBangladesh,Brazil,Egypt,
Mexico,Iran,SouthAfrica,Pakistan,Jordan,Thailand,andUganda.Thenumberofparents
evaluatedrangedbetween126and2,250(median=337).Theevaluationswerecomprisedof
sevenRCTs,threequasi-experimentswithcomparisongroups,andthreewithnocontrol
groups.Eightofthestudiesemployedprofessionals(Ertem,Atayetal.2006;Farahat,
Farahatetal.2009;Issler,Marosticaetal.2009;Oveisi,Ardabilietal.2010;
Sawasdipanich,Srisuphanetal.2010;Özyazıcıoğlu,Polatetal.2011)oracombination
ofprofessionalsandparaprofessionals(Mock,Arreola-Risaetal.2003;AlHassanand
Lansford2011)todelivertheprogramme.Thechild’sageatinterventionwasprimarily
duringthetoddlerandpreschoolyears.
Child Protection: Safety and Injury Prevention Amongparentsofinfantsandyoung
children,safetyisoneofthemostsalientconcerns.InLMIC,accidentalinjuriesarethe
causeofdeathanddisabilityamongmillionsofchildreneachyear,withratesestimatedto
beatleastfivetimeshigherthanthoseinnon-LMIC(Bartlett2002).Fourstudiesexamined
childprotectionintermsofphysicalsafetyandinjurypreventionthataimedtoincrease
parentalknowledgeaboutpesticidehazards(Farahat,Farahatetal.2009)andparental
practicesconcerningsafety(Mock,Arreola-Risaetal.2003;Issler,Marosticaetal.2009;
Özyazıcıoğlu,Polatetal.2011).Inallfourstudies,professionalsoracombinationof
professionalsandparaprofessionalsdeliveredtheprogramme.Moreover,allthese
programmesdeliveredservicestotheparentsingroups.Itappearsthereforethatgroup
modalityisacommonapproachtoparentingprogrammesthatareaimedatpromoting
childsafety.
3Weacknowledgethatresponsivefeedingispartofcaregiving,buthere,wefocusonthepsychosocialcomponent.
67
68
Concerningprotectionagainstpesticidehazards,parentsofpreschoolchildreninone
farmingcommunityinEgyptreceived15healtheducationsessionsonpesticidehazards
(Farahat,Farahatetal.2009).Parentswereassignedrandomlytooneoftwoconditions:
eithertheylistenedtostudyinvestigatorslectureortheyviewedavideotapeonhazards
andsafeuseofpesticides.Althoughthevideogroupscoredhigherthanthelecturegroup
onatestofpesticideknowledge,neithergroupdifferedonatestofpesticidepractice,
whichsuggeststhattheapproachusedwaseffectiveinimprovingknowledgebutnot
practice.
Concerningparentalpracticesaroundsafety,threestudiesfoundsignificantimpacts.All
threeprogrammesuseddidacticapproachesorlivedemonstrationswithindividualized
counseling.InBrazil,interventionmothersreceivedindividualizedinstructionprovidedby
hospitalstaffandmedicalstudentsinadditiontobeinginstructedusingdemonstrations
withababydollmodelonhowtopositioninfantswhenasleeptoreducetheincidenceof
SuddenInfantDeathSyndrome(Issler,Marosticaetal.2009).InTurkey,study
investigatorsconducted60-minutegroupsessionsonsuitablefirst-aidandtreatmentsfor
burns,lacerations,fractures,andpoisoninginadditiontohandingoutinformationon
availablecommunityresourcesformotherstocontact(Özyazıcıoğlu,Polatetal.2011).
Bothstudiesshowedthatprovidingdemonstrationsorexamplesofcontrastingapproaches
tosafetyareeffectiveininformingparentalpracticesofsafety.InMexico,oneprogrammeusedavarietyofapproachesinadditiontolivedemonstrations
andindividualizedcounseling(Mock,Arreola-Risaetal.2003).Theprogrammewasbased
onbothanestablishedprogramme(TheInjuryPreventionProgramme)andalocally
developedone(PalKai,or“healthychild).Thestudysites,whichwerecontingentuponthe
safetyneedsofeachsocioeconomicstratum(SES)group,wereprivateclinicsthatcharged
lowfees,andpubliclysubsidizedforupper-,middle-,andlow-SESgroups,respectively.Inall
clinics,thebasicprogrammemodelconsistedofelementsofinjurypreventioncounseling
deliveredbynursesandtrainedhealthcareworkersaspartofoverallhealthpromotion.
Counselingwasupgradedaspartofthisintervention.ForupperandmiddleSESgroups,the
upgrading
69
involvedlecturesanddemonstrationslastingsixhoursandutilizingaudio-visualmaterials
fromseveralsources.Inaddition,themiddleSESgroupreceivedclinic-basedcounseling
thatlasted15-20minutes,whereasthelowerSESgroupreceived30-minutehomevisitsby
trainednursesandhealthpromoters.Resultsrevealedthatwithrespecttousingcaution,all
threeSESgroupsdemonstratedimprovementspre-andpost-intervention. Howeverfor
otherdimensions(activitiesthatrequiredtheuseofsafety-relateddevices),theresults
weremixed.Thenon-randomizationofthedesign,thelackofdetailsregardingselection
criteria,andthelackofgeneralizabilityacrossSESgroupslimittheinterpretationofresults.Child Protection: Physical Abuse Althoughtheprevalenceofchildabusevariesacross
LMIC(LansfordandDeater-Deckard2012),thepercentageofchildrenexperiencing
psychologicalabuse,moderatephysicalabuse,andseverephysicalabuseishigherin
Africancountries(medianrates=83%,64%,and43%,respectively)thaninotherregions
(medianrates=56%,46%,and9%,respectively)(Akmatov2011).Oursystematicsearch
yieldedfourstudiesinfourcountries,threeofwhichwereMiddleEasterncountries.None
wereconductedinAfricancountries.Allprogrammesweregroup-basedexceptforone
group-basedprogrammewithahomevisitingcomponent.
Threeofthefourprogrammesweregroup-based,allfromtheMiddleEast(Koçak2004,
Oveisi,Ardabilietal.2010,AlHassanandLansford2011).InIran,Oveisi(2010)exploredthe
viabilityofusingprimaryhealthcaresettingsasvenuesforpreventiveinterventionsfor
childphysicalandemotionalabuse.Inthefirsttrainingsession,traineddoctorseducated
parentsinparentalskillbuildingincludingdiscussionsoncommonparentingmistakes.In
thesecondsession,mothersrole-playedandwatchedvideoclips.Bothsessionslastedfor
twohoursintwosuccessiveweeks.Resultsshoweddeclinesinparentalreportsof
instancesofabuseaswellasindysfunctionalformsofparenting.
The other two group-based programmes targeted fathers (Koçak 2004) in addition to
mothers(AlHassanandLansford2011).TheprogrammeswereimplementedinTurkeyand
Jordan. The Father Support Programme in Turkey targeted low-income immigrantswho
werefathers
70
(Koçak2004).Theprogrammewasa13-weekgroup-basedintervention(2.5hours/week)
thatwaslimitedto15fathers.Thesessionsweredesignedtopromotesocializationamong
fathersbysharingtheirproblemsandexperienceswitheachother.Bytheendofthe
programme,fatherattitudesbecamelesstraditionalandlessauthoritarianandtheyused
moreopenformsofcommunicationwiththeirfamilies.Theotherprogrammethat
targetedexplicitlyfathers(inadditiontomothers)wastheBetterParentingProgrammein
Jordanthatwasbroughtaboutbyanationalparentingstudy(AlHassanandLansford
2011).Thisprogrammehasbeenbroughttoscale,withmorethan200centersnationwide
implementingtheprogramme.Onedistinguishingfeatureoftheprogrammeisitsflexible
approachtotraining.Sessionscouldbeimplementedonceaweekforonemonthorthree
tofourconsecutivedays,ortwiceaweekfortwoweeks.Althoughonly6%offathers
participatedintheevaluation,resultsshowedsmallbutpositiveeffectsonknowledgeof
childneglect,spendingtimewithchild,anduseofexplanationsinthecourseofdiscipline.
Noimpactwasfoundonknowledgeofchildabuseandexpressionsofcontentment.Finally,oneprogrammecombinedgroupeducationwithhomevisiting.Thisprogramme
aimedtochangeparentalcognitiveprocessesregardingchildrearingamongThaiparents
(Sawasdipanich,Srisuphanetal.2010).Thegroupeducationcomponentusedvarious
programmecomponents:groupdiscussions,valuessharing,scenarioanalysisofvideotaped
presentations,andhomeworkusingabooklettoevaluatethecontentofthegroupsessions
andrecordtheirbehaviorsathomewithrespecttodealingwiththeirchildren’sbehaviors.
Thehomevisitswereusedtoidentifyparentalchallengesaswellastoproblem-solveand
increaseparentalefficacy. Resultsshowedprogrammeimpactsonparentalattitudes
towardchildrearingbutnotonpotentialforchildphysicalabuse.
Psychosocial Stimulation and Responsiveness Threestudiesfoundsignificant
impactsoncaregivers’abilitytoprovidestimulationandemotionalsupport(Ertem,Atayet
al.2006;Cooper,Tomlinsonetal.2009;Rahman,Iqbaletal.2009).InTurkey,an
adaptationoftheIMCICareforDevelopmentprogrammewasimplementedtoenhance
caregivers’playandcommunicationwiththeirtoddlers(Ertem,Atayetal.2006).During
theclinicvisit,trainedpediatriciansdeliveredtheintervention,whichconsistedof
71
strategiesforlisteningandobservingpositiveinteractions,usingspecificpraiseand
positivereinforcement,andprovidingthecaregiverwithideasonplayandhomemadetoys
forage-appropriatestimulation.Thislastedapproximately30minutes.Resultsofthe
evaluationshowedimpactsonavailabilityofstimulationopportunitiesbutnotoncaregiver
responsiveness,suggestingthatmoreintensiveapproaches(e.g.,directinteractionwith
child)areneededtoimprovecaregivers’abilitytobeemotionallyresponsive.
Thenexttwostudiesaimedtoimprovematernalsensitivityandresponsiveness,both
adaptedtofitlocalcontext.TheLearningThroughPlayprogramme,whichhasbeen
introducedin10countriesincludingIndia,hasbeenadaptedinruralPakistan(Rahman,
Iqbaletal.2009).Theprogrammehadaflexibleformat,allowingforbothindividualand
groupbasedformats.Theindividual-basedformatwasdeliveredinparents’homesbylocal
villagehealthworkerswhoknewthemotherswell.Thegroup-basedformatconsistedofa
one-weekworkshopthatwasintegratedintoroutinepre-andpostnatalvisits,orspread
overthefirst3yearsofthechild’slife.Theprogrammerequiredminimalamountsof
literacy.
TheotherstudywasSouthAfrica’sadaptationofBritain’sSocialBabyprogramme,which
aimedtoimprovematernalsensitivityandresponsivenesstowardtheirinfantsfollowing
WHO’sprinciplesofpsychosocialstimulation(Cooper,Tomlinsonetal.2009).Inthat
programme,trainedfemalecommunityworkersvisitedhomesconsideredhighriskfor
parentingproblemstoprovideparentingsupportandguidance.Theinterventiongroup
wasvisitedforatotalof16sessions(endingat5monthspostpartum).Consistentwith
resultsfoundinmoredevelopedcountries,theprogrammesfoundimpactsoncaregiving
knowledge(Rahman,Iqbaletal.2009)andonthequalityofmother-infantrelationships
(Cooper,Tomlinsonetal.2009).Bothstudies,however,wereunsuccessfulinalleviating
maternaldepression.Bothprogrammesemployedtrainedparaprofessionals,suggesting
thataddressingmaternaldepressionmayrequiremorehighlytrainedprofessionals.
Alternatively,treatingmaternaldepressionmayrequiremoretargetedprogrammesaimed
specificallyatthisissue.Recommendationstotreatmaternaldepressiongivenitssizeable
impactnotonlyonmaternalmentalhealthbutalsoonchilddevelopmentincludeinvolving
policymakers,researchers,andprogrammeproviders(Knitzer,Thebergeetal.2008).
72
Responsive Feeding and Integrated Health and Development Approaches
Twostudiesfoundsignificantimpactsonparentalcaregivingrelatedtobothhealth-and
non-healthpractices.OnestudyinBangladeshusedaresponsivefeedingapproach(Aboud,
Shafiqueetal.2009)andtheotherinUgandawasanintegratedhealthanddevelopment
programme(Britto,Engleetal.2007).
Intheresponsivefeedingapproach,thecaregiverfeedsthechildinresponsetothechild’s
cuesandpsychomotorabilitiestoensurethatthechildisfedwhenhungryandalsosatisfied
withthefeedingsituation(EngleandLhotska1999).IntheBangladeshstudy,programme
mothersreceived12sessionsonchilddevelopmentandrearinginadditiontosixweekly
sessionsonresponsivefeeding(Aboud,Shafiqueetal.2009).Althoughnoprogramme
impactswerefoundforweightgain,programmemothersbecamemoreresponsiveand
morehygienicthancontrolmothers.Theauthorsofthestudy(Aboud,Shafiqueetal.
2009)concludedthatforweightgainmorenutritionalinputisrequiredmainlyinareasof
highfoodinsecurity.
IntheUgandastudy,childhealthdayswereheldeverysixmonthscombinedwithan
educationalcampaignonhealth-seekingbehaviors,breastfeedingandcomplementary
feedingintheformofradiobroadcasts,posters,andotherlocalmedia(Britto,Engleetal.
2007).Moreover,familyandcommunitycapacitieswerestrengthenedviajobskillstraining
andcommunitygrantsandincentives.Thisprogrammehappenedforaperiodoftwoyears.
In addition to improvements in attitudes toward learning support for children,
improvementswith practices relating to physical care and school readiness skill building
werefound.
Summary Findingsfromevaluationsofsafetyandpreventionprogrammessuggestthat
professionalsareeffectivedeliverersofprogrammemessagesconcerningchildsafety.
Findingsfromnon-LMICsupportthisbyshowingthatauthorityfigures—doctors,nurses,
educators,forexample—aresuccessfulatincreasingparentingknowledge(Moran,Ghate
etal.2004).Commonstrategiestodeliveringmessagesincludedemonstrationsusing
didacticapproachesorusingtechnology.Groupsettingsmaybeeffectiveinincreasing

73
knowledgebutnotactualpractice.Itappearsthatevenshort-termprogrammesare
effective,althoughoperationalizationofsafetypracticeshavemostlybeenbasedonself-
reports.Infact,onestudydemonstratedthattheprogrammehadnoimpacton
performance-basedpractice(Farahat,Farahatetal.2009).Innon-LMIC,ECDparenting
programmesthataimtoimprovesafetyaremosteffectivewhentheycatertofamilieswith
childrenlessthanthreeyearsofage,andprovidecasemanagementservicesandparent-
childactivities(Kendrick,Barlowetal.2007).
Moreover,findingsfromevaluationsofphysicalabusepreventionprogrammessuggestthat
group-basedprogrammesareeffectiveinpreventingchildabuse.Althoughimpactswere
foundforparentalknowledge,attitudes,andpractices,onlyonestudyoperationalizedchild
abuseintermsofactualcommitmentofabuse.Itisimportanttodistinguishbetween
potentialforandactualabuse.Indeed,onesystematicreviewof298publicationsconducted
inprimarilynon-LMICrevealedfourtypesofprogrammesconsideredtobepromising
approachestopreventactualchildabuseasopposedtopotentialtocommitabuse(Mikton
andButchart2009).Theseprogrammesareideally:(i)earlychildhoodhomevisitation
programmeswheretrainedpersonnelvisitparentsandtheirchildrenintheirhomesto
providesupport,education,andinformationtopreventchildmaltreatment;(ii)center-
basedparenteducationprogrammesdeliveredingroupsthataimtopreventchild
maltreatmentbyimprovingparents’childrearingskills,increasingECDknowledge,and
encouragingtheuseofappropriatebehaviormanagementstrategies;(iii)programmesthat
includeabusiveheadtrauma(ShakenBabySyndrome)prevention;and(iv)multi-sectoral
programmesthatincludeservicessuchasfamilysupport,preschooleducation,andchild
care.Lesssuccessfultypesofprogrammesinclude:(i)childsexabuseprevention
programmesintheformofuniversalprogrammesdeliveredinschoolsthatteacheschildren
aboutbodyownershipandhowtodetectabusivesituations;(ii)media-basedinterventions
intheformofmediacampaignstoraisepublicawareness;and(iii)supportgroupsthat
aimedtostrengthenparents’socialnetworks.Moreover,thatreviewnotedthathome
visitationandparenteducationprogrammeswerebotheffectivenotjustinpreventing
actualabusebutalsoinreducingriskfactorsassociatedwithit(MiktonandButchart2009).
GiventhatratesofabusearehigherinAfricancountries(Akmatov,2011),noneofthe
studieswereconducted

74
intheAfricancontinentwithinthepastdecade,suggestingthatnotenoughchild
protectionprogrammesarebeingevaluatedinhighriskregions.
Insummary,acrossstudiesthatshowedsignificantimpactsoncaregivingthatpromoted
childdevelopment(non-health),thefindingssuggestthatprofessionalswereregardedas
individualswithauthorityandexpertiseandwereeffectiveinincreasingparental
knowledgeaboutchildprotection.Group-basedprogrammesappearedtobeeffectivein
impactingknowledgeaboutchildprotection,althoughitsimpactonactualasopposedto
self-reportedabuseremainsinconclusive.Singledoseprogrammeswereinsufficientin
improvingparentalemotionalresponsiveness.Combininghomevisitingwithgroup
sessionsappearedtobepromisingeveniftheyweredeliveredbytrainedparaprofessionals.
Responsivefeedingandintegratedprogrammeswerealsoeffectiveprogrammatic
strategiesforimprovingparentalpracticespromotingchilddevelopmentandprotection.
3.2.3COMPREHENSIVE(BOTHCHILDANDPARENT)OUTCOMES
Parentingprogrammesgenerallyaimtochangeparentalknowledge,attitudes,and
practicesthatwould,inturn,improvechildoutcomes.Notallparentingprogrammes
evaluatebothparentandchildoutcomesandfindimpactsonboth.Inthissection,studies
thatshowedsignificantimpactsonbothparentandchildoutcomes(i.e.,comprehensive
outcomes)arepresented.Here,comprehensiveoutcomesareorganizedaccordingto(1)
childphysicalhealthandhealth-relatedcaregivingpracticesand(2)childdevelopmental
outcomesandassociatedparentingpractices.3.2.3.1 Child Physical Health and Health-Related Caregiving Practices (n=19)
Nineteenstudies,halfofwhichwereRCTs,foundsignificantimpactsonchildphysical
healthandhealth-relatedcaregivingpractices.Thestudiesevaluatedbetween121and
6,144child-caregiverpairs(median=744)across9countries:Bangladesh,Brazil,Egypt,
Ethiopia,Haiti,India,Peru,Senegal,andUganda.Theprogrammaticapproachesusedwere
75
intheformofbreastfeedingpromotion,hygieneanddiseaseprevention,nutrition
education,andcomprehensivehealthandnutritionprogrammes.
Breastfeeding Promotion programmesinLMIChavebeenshowntoeffectivelyinform
newmothersofbreastfeeding’sbenefitsandtoincreasethechancesofactually
breastfeeding(Imdad,Yakoobetal.2011).Indeed,studieshaveshownthatknowledgeof
breastfeedingbenefitsareassociatedwithconfidenceinbreastfeedingandactuallactation
duration(Chezem,Friesenetal.2006),whichareimportantinensuringneonatalhealth.
Inourreview,wefoundthreestudiesofbreastfeedingpromotionprogrammesthatfound
impactsonbothchildhealthandparentingpractices.OnewasconductedinIndia
(Bhandari,Mazumderetal.2004)andtwowereconductedinBrazil(Cardoso,Vicenteet
al.2008,Vitolo,Bortolinietal.2008).InIndia,the12-and18-monthfollow-upofa
breastfeedingpromotionprogrammementionedinprevioussections(Bhandari,Bahletal.
2003;Bhandari,Mazumderetal.2005)showedsmallgainsinheight,withgreatergains
foundinboysthaningirls(Bhandari,Mazumderetal.2004).Thisstudyalsofound
programmeeffectsonparentalhealthpractices(SeeTable4inAppendix1).InBrazil,one
programmewasbasedonWHOguidelinesthatwasdeliveredinthehomesetting(Vitolo,
Bortolinietal.2008)andtheotherwasbasedonasystematicreviewofstrategies
appropriatetoaprimaryhealthcaresettingthateffectivelyincreasesthedurationof
breastfeeding(Cardoso,Vicenteetal.2008).Bothprogrammesshowedlowerratesof
respiratorymorbidity(butonlyfor<4monthsofageinCardosoetal.(2008))andmore
appropriatehealth-relatedcaregivingpractices.IntheCardosoetal.(2008)study,
reductionsindiarrheawerefoundbutonlyforthe4-12monthsagegroup,nottheyounger
group.Thisstudyisalsotobeinterpretedcautiously,givenitslowqualityscore(23%).
Hygiene and Disease Prevention Thenextsetofstudieswasacommunity-based
hygieneanddiseasepreventionprogrammeconductedinEthiopia(Cumberland,Edwards
etal.2008;Edwards,Harding-Eschetal.2008).Theseprogrammesutilizedavailable
communityresourcestodisseminatehealthinformation.InEthiopia,theprogrammewas
knownasthe
76
InternationalTrachomaInitiative(ITI),whichwasderivedfromtheSurgery,Antibiotics,
FacialCleanlinessandEnvironmentalImprovement(SAFE)strategyanddisseminatedin
randomlyselectedcommunitiesthroughmassdrugadministration,information,education
andcommunicationmaterials,andcommunityvideobroadcasts(Cumberland,Edwardset
al.2008;Edwards,Harding-Eschetal.2008).Post-interventiondataindicatedthatITIled
toareductioninoddsofactivetrachomaamongyoungchildrenlivinginprogrammeareas
andincreasesinparentalknowledgeofeyediseasepreventionbutnotinreportedor
observedhygienepractices(Cumberland,Edwardsetal.2008).Thethree-yearfollow-up
showedloweroddsofinfectioninolderchildren(6-9yearsold)thaninyoungerchildren,and
inchildrenwhoreceivedtwoorthreedosesratherthanone(Edwards,Harding-Eschetal.
2008).Thereisevidenceofimprovementinsanitarypracticessurroundingwaterusageand
thepresenceofflypopulationsinthefollow-upstudy.
Health and Nutrition Education Sixstudiesevaluatedhealthandnutritioneducation
programmes. Except for one study (Santos, Victora et al. 2001), five evaluated
programmes that targeted malnourished populations (Ghoneim, Hassan et al. 2004;
Kilaru,Griffithsetal.2005;Penny,Creed-Kanashiroetal.2005;Roy,Fuchsetal.2005;
Waters,Pennyetal.2006).ExceptforKilaruandothers(2005),professionalsandexperts
(Santos, Victora et al.2001; Ghoneim, Hassan et al. 2004) or a combination of
professionalsandparaprofessionals(Penny,Creed-Kanashiroetal.2005;Roy,Fuchset
al. 2005; Waters, Penny et al. 2006) delivered the health messages. For example, in
Bangladesh,doctors received20-hour training innutritioncounselingfollowingthe IMCI
feeding guidelines (Santos, Victora et al. 2001). Maternal recall of dietary
recommendationsand useof recommendedfoods and feedingpracticeswerehigher in
the programme group than in the control group, although gains in anthropometry
(weight-for-ageandweight-for-height)werefoundonlyfortheoldestagegroup(between
12and18months).
Infoodinsecureregions,theprogrammeswereviewedutilizedlocalresourcestoeducate
caregivers.InIndia,forexample,locallytrainedcounselorsprovidedmonthlynutrition
educationtocaregiverswithchildrenbetweenfiveand11monthsofage(Kilaru,Griffithset
al.2005).Thecounselingmessagesfocusedonthepreparationandtheuseof
77
developmentallyappropriatelocalfoodsandthepreparationofthesefoodsaswellas
feedingadvice.Thecounselorsweretrainedtobesensitiveofhouseholdconstraints(e.g.,
limitedfinancialresources,availablehouseholdfood,decision-makingcapacityand
privilegewithinthefamilystructure).TheIndianprogrammeresultedingreaterweight
velocityandgreaterdietarydiversity.
Deliverysettingsalsovariedforhealthandnutritionprogrammesreviewed.InPeru,the
extenttowhichlocalcommunitiescouldserveasdeliverysettingsfornutritioneducation
programmestobeintegratedwithexistingnutritionserviceswastested(Penny,Creed-
Kanashiroetal.2005;Waters,Pennyetal.2006).Localfieldworkersvisitedfamilies
duringcrucialstagesofdevelopmenttoassessnutrition,feedingpractices,andgrowth:
afterbirthandat3,4,6,8,9,12,15,and18monthsofage.Reductionsinstuntingand
increasesinage-specificfeedingknowledgeandhealth-seekingbehaviorswerereported.
Thus,thehealthcentersimprovedtheirqualityandcoverageoftheirnutritioneducation
throughlocalfieldworkers(Penny,Creed-Kanashiroetal.2005).
Inadditiontocommunity-basedsettings,theutilizationofdaycarecentersasdelivery
settingsofnutritioneducationprogrammeswastestedinEgypt(Ghoneim,Hassanet
al.2004).Theprogrammeconsistedofestablishingkitchensinthecentersand
providingtwomealsperday.Inaddition,parentsreceived12healtheducationsessions
fromuniversitystaffonfeedingpracticesandfeedingschedules.Improvementsin
maternalnutritionknowledgeandinanthropometricmeasuresanddecreasesinthe
percentageofanemicchildrenwereobservedpost-intervention.ThePeruvianand
Egyptianstudieshighlighttheimportanceofintegratinghealthandnutritioneducation
programmesintoexistingstructures.
InBangladesh,theamountofparentinginstructionneededtoimpactchangewas
examinedbyRoyandcolleagues(2005). Moderatelymalnourishedmotherswererandomly
assignedtooneofthefollowingnutritioneducationconditions:(1)twiceaweekforthree
months,(2)twiceaweekforthreemonthsinadditiontosupplementaryfeedingforsix
daysaweek,and(3)twiceamonthnutritioneducationaspartofstandardroutineservice
oftheBangladeshIntegratedNutritionProject(thecontrolcondition).Nodifferences
78
betweenthetwointerventiongroupswerefoundintermsofchildanthropometry,
morbidity,andparentalfeedingpractices,butbothinterventionswerefavoredoverthe
controlcondition.Thisstudyshowedthatadditionalsupplementaryfeedinghadno
additiveimpactonearlychildhoodhealthwhencombinedwithhealtheducation.This
finding,however,shouldbeinterpretedwithcaution,asunintendedimpactswerereported
(e.g.,higherratesofdiarrheaandfebrileepisodesininterventiongroupsthanincontrol
group).
Nutritioneducationprogrammesaremoreeffectivewhenprofessionalsdeliverthe
healthmessages.Parentsmayinterprethealthcareprofessionalsasexpertsinthefield
andarethereforemoreamenabletodidacticinstruction.Nutritioneducation
programmesthatareintegratedintoexistingprogrammesorstructuressuchasnutrition
services(Penny,Creed-Kanashiroetal.2005;Waters,Pennyetal.2006)orearly
childhoodservices(Ghoneim,Hassanetal.2004)aremoreeffective.
Comprehensive Health and Nutrition Programmes Eightstudieswerecategorized
undercomprehensivehealthandnutritionprogrammes.Theprogrammingmodalities
werecommunity-basedprogrammes(Alderman2007,Dubowitz,Levinsonetal.2007;
Roy,Jollyetal.2007;Alderman,Ndiayeetal.2009,Arifeen,Hoqueetal.2009)and
homevisits(Ruel,Menonetal.2008;Donegan,Maluccioetal.2010;Feldens,Giugliani
etal.2010).
Fivestudieswerecommunity-basedprogrammesthatpromotedhealth,growth,and
nutrition.TwostudieswereconductedinBangladesh.OnetestedtheefficacyoftheIMCI
strategyinchildhoodmortalityandnutrition(Arifeen,Hoqueetal.2009)andtheotherone
wasacomprehensivehealthandnutritioneducationprogrammethattargetedmothersof
moderatelymalnourishedchildrenaged6-9months(Roy,Jollyetal.2007).IntheIMCI
study,allthreecomponentsoftheIMCIstrategy(i.e.,health-workertraining,health-
systemsimprovements,andfamilyandcommunityactivities)wereimplemented.Village
practitionersdeliveredinformationonmanagementofsickchildren,avoidanceofharmful
treatmentpractices,andreferralofseverelyillchildren.Thestudyalsotrainedand
79
supportedMuslimimamsidentifiedintheprogrammeareastoconveycrucialmessages
duringsermons.Moreover,atheaterscriptaddressingIMCImessageswasdevelopedand
twocommunitytheatergroupsweretrainedandsupportedtoundertakeopen-airtheater
showsintheIMCIareavillagesonceeveryeighttoninemonthstocommunicatekey
messages.Caregiversinprogrammeareasweremorelikelythanthoseincontrolareasto
utilizeavailablecommunityresources(e.g.,counseledbyvillagehealthworkers,attended
meetingsonmaternalandchildhealth).Therewasalsoevidenceoflowerprevalenceof
stuntingandwastinginprogrammeareasthanincontrolareas.
IntheotherstudyinBangladesh,theprogrammegroupreceivedweeklynutritioneducation
inadditiontostandardcareforthefirstthreemonthsandthenonceeverytwoweeksfor
thenextthreemonthswhereasthecontrolgroupreceivedregularservicesfromthe
BangladeshIntegratedNutritionProject.Mothersintheprogrammegrouphadbetter
feedingpracticesthanmothersinthecontrolgroup.Moreover,childrenintheprogramme
grouphadlowerratesofstunting,werelessunderweight,andhadgreaterweightgainthan
childreninthecontrolgroup.Thenutritionprogrammesreviewedthereforewereeffectivein
improvingbothanthropometricmeasuresandmaternalcaregivingpractices.
Thenextsetofcommunity-basedhealthandnutritionProgrammeswereimplementedin
Uganda,Senegal,andIndia.TheUgandaandSenegalprogrammes,whichcapitalizedon
thesupportofparishactivitiesandanationalmultisectoralcoordinatingbody,respectively,
weresuccessfulinimpactingratesofbeingunderweightandparentalcaregivingbehaviors
(Alderman2007;Alderman,Ndiayeetal.2009).ThegoaloftheDularprogrammeinIndia
wastocapitalizeanddevelopcommunityresourcesatthegrassrootsleveltoimprove
nutritionalpracticesanddecreasemalnutrition.Activitiesincludedtheestablishmentofa
community-basedtrackingsystemofthehealthstatusofwomenandchildrenamongother
growthandnutritionactivities.IntheevaluationoftheDularprogramme,the
interventionwasdividedintothree:onereceivingtheregularDularprogramme(regularhealth
andnutritionactivities,trainingandadvocacy,distributionofeducationmaterials),one
receivingtheintensiveDularprogramme(regularprogrammewiththeadditionof
trainingandassignmentoflocalresourcepersons,monitoring,andfollow-upactivity),
andonenon-

80
Dulargroup(receivingregularhealthandnutritionactivities)(Dubowitz,Levinsonetal.
2007).Eitherregularorintensiveprogrammeswerefavoredoverthenon-Dularinterms
ofparentalhealthandnutritionpracticesandratesofbeingunderweight.Rateof
immunizationwashigherintheregularDulargroupthanbothintensiveDularandnon-
Dulargroups.
OneinterventioninBrazilcombinedoralhealthpromotionwithTenStepsforHealthy
Feeding,whichwasapartnershipbetweenWHOandtheBrazilianNationalHealthPolicy
(Feldens,Giuglianietal.2010).TheotherinterventionwasconductedinHaiti(Ruel,
Menonetal.2008;Donegan,Maluccioetal.2010).IntheBrazilianstudy,12university-
levelnutritionstudentswhowereextensivelytraineddelivered30-minutemonthlyhome
visitsuptosixmonthsandthenbi-monthlyhomevisitsforthenextsixmonths.Although
theprogrammedidnotimpactconsumptionoffruitsandvegetables,significantimpacts
favoringtheinterventionwerefoundforfewercariesandcaregiversgivinglowerdensityof
sugarinfoods(Feldens,Giuglianietal.2010). TheevaluationoftheHaitianprogramme
involved13-14homevisitsfornewborninfantsandseverelyundernourishedchildrenin
additiontootherprogrammeactivities(foodassistance,nutritioncounselingprovidedat
rallypostsandmothers’clubs,vaccination,vitaminAsupplementation,oralrehydration
salts,anddrugsthatattackparasites)(Ruel,Menonetal.2008;Donegan,Maluccioetal.
2010).Fortheevaluation,twoversionsoftheprogrammewereimplemented.The
preventiveprogrammetargetedallchildren(6-23monthsold)whereastherecuperative
programmetargetedunderweightchildren(6-59monthsold).Comparedtothecomparison
group,caregiversfromeitherprogrammeversionsweremorelikelytotaketheirchildrento
rallypostsforhealtheducation,growthmonitoringandgettingfullvaccinationsfortheir
children.Moreover,childrenassignedtothepreventive(universal)programmehadlower
incidencesofstunting,wasting,andbeingunderweightthanchildreninthecomparison
group;therewasnodifferencebetweenchildrenassignedtotherecuperativeprogramme
andthoseassignedtothecomparisongroup.Theeffectsonanthropometricmeasureswere
strongerforyoungerchildren(i.e.,thoseexposedtotheprogrammeduringtheages6-23
months).Theyprovidehelpfulguidanceontheleveloftrainingofserviceprovidersand
programmedose.
81
Summary Thissectionreviewedstudiesthatexaminedandshowedimpactsonbothchild
andparentingoutcomesrelatedtophysicalwell-being.Acommonstrategyusedinthe
programmesreviewedcapitalizedonavailablecommunityresourcesandcommunityevents
todelivertheprogramme.Placesofworshipservedasprogrammedeliverysettingsinsome
cases.Further,linkingprogrammestoexistingpoliciesprovidesanillustrationofhowtotest
theefficacyofpolicyimplementation.Multisectoralpartnershipshavebeennotedasthekey
ingredienttoprogrammaticsuccess.Noadditiveeffectswerefoundforsupplementary
feedingorfoodfortificationefforts.Thereissomeevidencethatpreventivenutrition
programmes(i.e.,targetingentirepopulations)asopposedtorecuperative(i.e.,targeting
malnourishedpopulations)oneshavegreaterimpacts.Intermsofdevelopmentaltiming,
impactsonanthropometrywerestrongerforchildrenwhowereexposedtotheprogramme
whentheywereyounger.3.2.3.2 Child Developmental Outcomes (Non-Health) and Associated
Parenting Practices (n=13) Thirteenstudiesconductedineightcountries--Bangladesh,China,India,Jamaica,Mexico,
Nicaragua,Paraguay,andTurkey—evaluatedbetween100and4,465child-caregiverpairs
(median=202)andfoundsignificantimpactsonbothchildandparentoutcomesconcerning
non-health-relatedoutcomes.EightwereRCTs.Over¾oftheprogrammesmentionedwere
deliveredbyparaprofessionals.Successfulprogrammaticapproachestoimpactingchild
developmentaloutcomesandassociatedparentingpracticeswereintheformof
psychosocialstimulationprogrammes,integratedhealthanddevelopmentprogrammes,
andsocialprotectionprogrammes.
Psychosocial Stimulation Studiesthatexaminedpsychosocialstimulationprogrammes
wereconductedinIndia(SharmaandNagar2009),Turkey(Kagitcibasi,Sunaretal.2001),
Jamaica(Walker,Changetal.2004),andMexico(Solis-CamaraandRomero2002).These
studieshaveshownthatpsychosocialstimulationprogrammes,whichrequiredirect
interactionswithchildren,aresuccessfulnotonlyinimprovingchildren’sinformation
processingskills,languageskills,andsocialandemotionalwell-being,butalsoinimproving
82
caregiverpracticesthatpromotechildren’scognitiveandsocialandemotional
development.Itappearsthatparaprofessionalsareaseffectiveparenttrainersas
professionalsgiventhattheprogrammesreviewedusedeitheroneortheother.
ThelongitudinalimpactofonemodelpsychosocialstimulationprogrammeinTurkey
hasreceivedinternationalattention.TheTurkishEarlyEnrichmentProject(TEEP)was
designedtotrainmotherstodeveloptheirchildren’scognitiveabilitiesandimproveparent-
childinteractions(Kagitcibasi,Sunaretal.2001;Kagitcibasi,Sunaretal.2009).Two
hundredeightymothersandtheirpreschool-agedchildren,whobelongedtothree
categoriesofearlychildcareenvironments(i.e.,educationalnurseryschool,custodialday
care,andhomecare)participatedinthestudy.Childreninthehomecaregroupwere
randomlyassignedtoreceivetheprogrammeornot.Theprogrammeconsistedofa
cognitivecomponentandamotherenrichmentcomponent.Thecognitivecomponent
consistedof60bi-weeklyguidedgroupdiscussionsovertwoyears.Trainedlocalfemale
coordinators,withrelativelyhighlevelsofeducation,deliveredthesessionsbothinthe
homeandinthegroupsettings.Bothrole-playinganddirectinstructionwereusedtoteach
mothershowtointeractwiththeirchildren.Mothersworkedwiththeirchildren15-20
minutesaday. Themotherenrichmentprogrammeconsistedof30bi-weeklyguidedgroup
discussionsthatlastedforonehour.Thetopicsforthediscussionsincludednutrition,child
development,parent-childinteractions,andparentalwell-being.Thediscussionscateredto
mothers’everydayexperiences.Resultsofthefour-year,follow-upevaluationshowedthat
mothersintheprogrammeweremorelikelytobeinvolvedincognitivestimulationactivities
thanthosewhowerenotintheprogramme.Inaddition,thechildreninthemother
programmescoredhigherinanalyticability,andtheprogrammehadsustainedeffectsin
schoolattainment,vocabularyscores,favorableattitudestowardschool,andfamilyand
socialadjustmentattheseven-year,follow-upstudy(Kagitcibasi,Sunaretal.2001).
Findingshighlighttheimportanceofthehomeenvironmentasasupportmechanismto
earlychildhoodeducation.
Thestudiesreviewedheresuggestthatintensiveprogrammesaresuccessfulinimpacting
childandparentoutcomes.
83
Responsive Feeding: TheInternationalCentreforDiarrhealDiseasesResearchin
Bangladeshexaminedtheimpactsofaresponsivestimulationandfeedinginterventionon
childnutritionanddevelopmentaloutcomesaswellascaregivingpractices(Aboud2007;
Aboud,Mooreetal.2008;AboudandAkhter2011).Inthefirststudythatusedapost-test
onlydesign,trainedlocalfemalepeereducatorsimpartedinformationtogroupsofmothers
onacomprehensivesetoftopics(e.g.,healthandsanitation,cognitiveandlanguage
development)overanaverageof16sessionsforoneyear(Aboud2007).Inadditionto
improvementsinchildren’sweight-for-heightzscores,improvementsinbothknowledge
andactualpracticesthatpromotechilddevelopmentwerefound.However,no
improvementinlanguagecomprehensionwasfound.Thisfindingsuggeststheneedto
includechildreninthesessionactivitiesandfocusonspecificpracticesratherthan
information.AsubsequentRCTthatincludedchildrenandfocusedonresponsive
interactionsfoundlanguagedifferences(AboudandAkhter2011). Inthatstudy,control
mothersreceived13informationalsessionsonhealthandnutrition.Inadditiontowhat
controlmothersreceived,interventionmothersreceived6weekly90-minutegroup
sessionsonfeedingandstimulationdeliveredbylocalpeereducators.Theprogramme
taughtparentsabouthygiene(e.g.,howtowashtheirchild’shandsbeforeeating)and
promotedhealthandnutritionstrategies(e.g.,dietarydiversity,allowingforself-feeding).
Verbalresponsivenesswasalsostressed,aswerecopingwithrefusals.Oneadditional
interventiongroupreceivedalso6monthsoffoodpowderfortifiedwithmineralsand
vitamins.Resultsoftheimpactevaluationshowedthattheinterventiongrouphadmore
stimulatinghomeenvironmentsandmother-childresponsivetalkingthanthecontrol
group.Moreover,interventionchildrenhadhigherscoresthancontrolchildrenonlanguage
development,mouthfulseaten,andhandwashing.Foodfortificationcontributedonlyto
weightgainbutnotlanguagedevelopment.Insummary,theresponsivefeedingapproach,
ifimplementedatleastbetween16and18sessions,areeffectiveinimprovingweightand
maternalfeedingpractices(Aboud2007,Aboud,Mooreetal.2008);languageabilityis
morelikelytobeimprovediftheprogrammeinvolveschildrendirectly(AboudandAkhter
2011).
Integrated Health and Development Programmes Theevaluationsof
integratedhealthanddevelopmentprogrammes,wereconductedinChina(Jin,Sun
etal.2007),
84
Bangladesh(Hamadani,Hudaetal.2006),Jamaica(Powell,Baker-Henninghametal.
2004),andParaguay(Peairson,Austinetal.2008).Allprogrammesweredeliveredby
localcommunityhealthworkerswhoweremostlywell-trainedexceptforoneprogramme
thatemployedvolunteerswithminimaltrainingandsupervision(Peairson,Austinetal.
2008).Onlyoneevaluationemployednon-randomassignment(Peairson,Austinetal.
2008).
TheChinastudywasbasedonWHO’sCareforDevelopmentprogramme,whichoffered
anintegratedpackageconsistingofpsychosocialstimulationinadditiontotheIMCI
healthandnutritionpackage(Jin,Sunetal.2007).Trainedhealthprofessionals
counseledcaregiversforatotaloftwocounselingsessionsthatcontainedage-specific
messagesonhowcaregiverscouldengagetheirchildrenbothinplayandineveryday
communication.Theprogrammehadnodiscernibleimpactonpsychomotor
development,buttheprogrammeimpactedchildren’slanguageandadaptiveandsocial
behaviorsaswellasmothers’knowledgeofchildrearing.
TheBangladeshandJamaicastudiesincludedahomevisitingcomponent.Bothstudies
integratedearlystimulationintoeitheranexistingnationalnutritionprogramme
(Hamadani,Hudaetal.2006)orintoprimaryhealthcaresettings(Powell,Baker-
Henninghametal.2004).Bothprogrammestargetedmalnourishedpopulations.Although
bothprogrammeswereunsuccessfulinimprovingchildren’spsychomotordevelopment,
bothweresuccessfulinimprovingnotonlychildren’scognitiveandsocialandemotional
outcomes,butalsoinimprovingmothers’knowledgeandpracticeofchildrearing.Both
programmesalsowereintensiveintermsofdosage.TheBangladeshprogramme
consistedofweeklygroupmeetingsfor10monthsfollowedbybi-weeklymeetingsfor2
months,andbi-weeklyhomevisitsfor8months,followedbyweeklyhomevisitsfor4
months.TheJamaicanprogrammeconsistedof30-minutesweeklyhomevisitsforone
year.Bothprogrammesinvolveddirectinteractionwiththechild.TheBangladesh
curriculum,whichoriginatedinJamaica,wasadaptedtotheculturebyincluding
traditionalgamesandsongsandbyproducinglow-costpicturebookssuitablefor
Bangladeshichildrenandtheirmothers.Thecurriculumstressedthe
importanceofparent-childinteractionsandprovideddevelopmentallyappropriate
85
activitiesforthechild.Parentswereeducatedontheimportanceofpraisingandgiving
85
positivefeedback,engaginginconversationwithchildren,anddiscouragingpunishment,
amongothers.
TheotherintegratedprogrammewasthePastoraldelNiño,inParaguay,whichhasbeenan
ongoinglow-costprogrammesince1995thatcaterstochildren0-5yearsofage(Peairson,
Austinetal.2008).Minimallytrainedandsupervisedvolunteersmeetwithfamiliesin
chapelsorcommunitycentersonceamonthtoengageparentsinadiscussionaboutchild
health,nutrition,safety,anddevelopment.Volunteersalsoconducthomevisitsaswellas
accompanypregnantwomentohealthpostsforprenatalcheckups.Althoughno
programmeeffectswerefoundforstuntingandunderweight,theprogrammehadimpacts
onotherchilddevelopmentaloutcomesandparentalcaregivingandchildrearingpractices
(SeeTable4inAppendix1).Thelowqualityscoreratingofthestudy,however,warrants
cautionintheinterpretationoffindings.
Social Protection TwoevaluationsofNicaraguanconditionalcashtransferprogrammes
havebeenshowntoeffectivelyimpactholisticdevelopmentandparentingoutcomes.
(MaluccioandFlores2004,Macours,Schadyetal.2008). TheReddeProtecciónSocialwas
modeledaftertheMexicanPROGRESAprogramme,andtheAtenciónaCrisispilot
programmewasmodeledafterReddeProtección.Forbothprogrammes,duringenrollment
andpaydays,programmestaffrepeatedlystressedtheimportanceofvarieddiets,health,
andeducationtocaregivers.Thisformofcommunicationwasmeanttoinstructparents
wheretoinvesttheirmoneyandwhattoconsume(Macours,Schadyetal.2012).Toremain
eligibleintheprogramme,caregiverswererequiredtotaketheirpreschool-agedchildrenfor
regularvisitstohealthcentersforgrowthmonitoring,vaccination,andreceiptoffood
supplements.ThedifferencebetweenReddeProtecciónandtheAtenciónaCrisispilot
programmewasthelatter’srelianceonpublichealthinfrastructureincontrasttoRedde
Protección‘srelianceonprivatehealthproviders.TheevaluationofbothprogrammeswerebasedonclusteredRCTs.ResultsoftheRedde
Protecciónrevealedthatparentsinprogrammeareasweremorelikelythanparentsinnon-
86
programmeareastotaketheirchildrenages0-3tohealthcontrolcentersandfeedtheir
childrenwithmorevarieddiets(MaluccioandFlores,2004).Theeffectswerestronger
amongthepoorandextremepoorbutnotfornon-poorpopulations.Furthermore,the
increasedvarietyinhouseholddietandincreaseduseofpreventivehealthcareservicesfor
childrenwereaccompaniedbyanimprovementinthenutritionalstatusofbeneficiary
childrenunderage5.Theneteffectwasadeclineinthenumberofstuntedchildren.
Despiteimprovementsinthedistributionofironsupplementstothesesamechildren,
however,ReddeProtecciónSocialwasunabletoimprovehemoglobinlevelsorlowerrates
ofanemia(MaluccioandFlores,2004).
FortheevaluationofAtenciónaCrisis,parentswereassignedrandomlyintooneoffour
conditions:(1)aconditionalcashtransfercontingentuponchildren’sprimaryschooland
healthserviceattendance(CCTonly),(2)aconditionalcashtransferplusascholarshipthat
allowedoneofthehouseholdmemberstochooseamonganumberofvocationaltraining
coursesofferedinthemunicipalheadquarters(CCT+training),(3)aconditionalcash
transferplusaproductiveinvestmentgrantaimedtoencouragingbeneficiariestostarta
smallnon-agriculturalactivity(CCT+investment),or(4)controlcondition(Macours,
Schadyetal.2008). Ninemonthsafterprogrammereceipt,effectsforthethree
programmepackagesweresimilarthroughout.Impactsfavoringanyoftheprogramme
groupsoverthecontrolgroupwerenotedforvocabulary,memory,psychomotorskills,and
social-personalskills(Macours,Schadyetal.2008).Theseweredomainswherechildren
hadparticularlylargedelays,andwheresocioeconomicgradientsweresteeper.Caregiver
practicesalsochanged,whichmayaccountforimpactsfoundinchildren’sdevelopment.
Overallfoodexpendituresincreasedamongprogrammehouseholds,andexpenditureson
nutrient-richfoodsuchasanimalproteins,fruitandvegetablesincreasedmorethan
proportionally.Moreover,programmecaregiversweremorelikelythancontrolcaregivers
totaketheirchildrenforgrowthcheck-upstoreceivecareandnutritionservices.
Furthermore,earlystimulationactivitiessuchasreadingtothechildweregreaterin
programmehouseholdsthanincontrolhouseholds.Althoughprogrammechildrenhad
lowerratesofstuntingthancontrolchildren,noeffectswerefoundforratesof
underweight(under5months)andcaregiverreportofproblembehaviors.

87
Summary Findingsareconsistentwithresultsfromprevioussections.Thatis,intensive(at
leastweeklyforoneyear)psychosocialstimulationprogrammesareeffectiveinchanging
parentalpracticesandchildmentalandsocialandemotionaldevelopmentaloutcomesbut
noteffectiveinchangingpsychomotordevelopmentaloutcomesandanthropometric
measuresevenwhentheseprogrammesareintegratedintoexistingnutritionprogrammes.
Psychosocialstimulationprogrammescombinedwithformalearlyeducationyieldedrobust
longitudinaleffectsasevidencedintheTurkishdemonstrations.Thefindingsalsostressthe
importanceofincludingchildrenintheprogrammeasevidencedintheresponsivefeeding
programmesimplementedinBangladesh.Thesefindingsareconsistentwiththosefrom
non-LMIC,whichrevealedthatstrategiesassociatedwithimprovingbothchildandparent
outcomesincluded:(i)trainingparentshowtointeractpositivelywiththeirchildrenona
dailybasis(real-lifeeverydayscenarios)and(ii)livemodeling(practicingnewlylearned
skillswiththeirownchild)vs.role-playingwithapeerortrainer(Kaminski,Valleetal.
2008).Inadditiontopsychosocialstimulationprogrammes,socialprotectionprogrammesinthe
formofconditionalcashtransferprogrammesappeartobepromisinginspiteofthe
inexplicitparentaltraininginvolved.Indeed,findingsfromwelfaredemonstration
programmesintheUSyieldsimilarresults.Duncanandothers(2011)pooleddatafromfour
studiesthatevaluatedRCTsofeightwelfareandantipovertyprogrammes(closeto
N=20,000).Likeconditionalcashtransferprogrammes,noneoftheprogrammesevaluated
weredesignedtoaffectchildoutcomesdirectlynorweretheydesignedtotargetparenting
outcomes.Resultsrevealedthatthepreschoolperiodwasespeciallyvulnerabletoincome
fluctuations.Specifically,a$1,000increaseinannualincomesustainedforatleasttwoyears
resultedina6%SDincreaseinachievementtestscores.ThisfindingintheUSsuggeststhat
thesmallbutsignificanteffectsizeoftheprogrammesmaybecomelargerifthewelfare
programmestargetedexplicitlyparentingandchildoutcomes.Thepathwaysbywhichincreasesinincomeleadtobetterparentandchildoutcomescanbe
explainedbydatadrawnfromthePanelStudyofIncomeDynamics(Yeung,Linveretal.
2002).Here,Yeungandothers(2002)demonstratedthattherearetwopathwaysbywhich

88
incomeislinkedtooutcomes. Thefirstpathwayisthroughtheimpactofincreasedincome
onincreasedaccesstostimulatingenvironments—forexample,increaseduseofcenter-
basedservicesforearlyeducationandcare—which,inturn,impactschildren’scognitive
development.Thesecondpathwayisthroughtheimpactofincreasedincomeonmaternal
emotionalwell-being—forexample,reductionsinmaternalstress—which,inturn,impacts
children’ssocialandemotionalwell-being.Althoughtheeffectsofincomesupplementsare
generallypositive,onestudyfoundthatthiswasonlytrueforparentswhowere“hard-to-
employ”butnotforparentswhowere“hardest-to-employ”(Yoshikawa,Magnusonetal.
2003).Ofnote,althoughcashtransfersappeartobeeffectivetoacertainextent,theyare
insufficientinreducingthedetrimentalimpactsofpovertyonyoungchildren;aligningsuch
strategieswithhealth,education,andotherECDservicesisanimportantstep(Aber,
Bierstekeretal.2013).3.2.4STUDIESWITHNOIMPACTORPREDOMINANTLYMIXEDFINDINGS
The14studiesreviewedinthissectionshowedeithernoimpactorpredominantlymixed
findingsontheoutcomesofinterest.Halfofthestudiesreviewedwereintheareaofhealth
andtheotherhalfwereintheareaofchilddevelopment(non-health),includingassociated
parentingoutcomes.
3.2.4.1 Child Health and Parental Health-related Caregiving Outcomes (n=7)
Sevenstudieswiththefollowingprogrammaticapproachesmakeupthissection:(1)
hygienepromotioninNiger(Abdou,Munozetal.2010),(2)nutritioneducationinChina
(Strand,Pengetal.2002)andSenegal(Gartner,Kamelietal.2007),(3)
comprehensivehealthandnutritionwithcaregiversupportcomponentinSyria
(Bashour,Kharoufetal.2008),(4)communityempowermentviapositivedeviance
approachinVietnam(Schroeder,Pachetal.2002)andviaparticipatorylearningin
India(Tripathy,Nairetal.2010),and(4)socialprotectionintheformofconditional
cashtransfersinMexico(BehrmanandHoddinott2005).Sixofthesevenstudieswere
RCTs.Onlyonestudyusedhomevisiting.Thecommonthreadacrossthese
programmeswasthattheyweremostly
90
delivereddidacticallybyparaprofessionals.Therewas,however,considerablevariation
acrossprogrammesintermsofprogrammaticdesignandstrategies.
Twocommunityempowermentprogrammesdifferedintheirdesign.Oneprogrammein
Vietnamwasdesignedasacommunity-basednutritionprogrammeusingthehearthmodel
andthepositivedevianceapproach(Schroeder,Pachetal.2002).Inthisstrategy,
communitymembersidentifypoorfamilieswithwell-nourishedchildrenanddocumenttheir
caregivingbehaviors—feedingpractices,caring,andhealth-seekingbehaviors(Marshand
Schroeder2002).Programmersthendesigntheinterventionbasedontheadoptionofthese
behaviors.Theotherprogrammewasdesignedasaparticipatorylearningprogrammein
women’sgroupsinIndia(Tripathy,Nairetal.2010).Inthisprogramme,healthcommittees
wereformedinbothprogrammeandcontrolareas,allowingforcommunitymembersto
expresstheiropinionsoflocalhealthservices.Inprogrammebutnotincontrolareas,local
womenfacilitated20monthlygroupmeetings.Findingsrevealednoimpacton
anthropometricmeasuresfortheVietnamprogrammebutrevealedthatprogramme
childrenlessthan15monthsandprogrammechildrenwhoweremoremalnourished
deterioratedsignificantlylessthanthecontrolgroup(Schroeder,Pachetal.2002).Forthe
Indianprogramme,significantimpactwasfoundonlyoninfantmortalityrates,whichwas
notanoutcomeunderinvestigationinthisreview(Tripathy,Nairetal.2010).No
programmeeffectswerefoundformaternaldepression,illnessindicators,andcare-seeking
behaviors.Thefindingsfrombothprogrammessuggestthatcommunityempowerment
programmesinandofthemselvesmaynotbeaseffectiveinimprovingchildphysicalwell-
beingandmaternalcaregivingbehaviorsbeyondchildhoodsurvival.Otherprogramming
modalities,suchashomevisitsmayhavetobecombinedwiththisprogrammaticapproach
toyieldmorepositiveprogrammeimpacts.Anothersetofstudiesconsistedofrelativelylow-doseprogrammes(between1and9
sessions)andmayhaveaccountedforthelackofprogrammeeffectiveness.Thesewere
implementedinNiger(Abdou,Munozetal.2010),inChina(Strand,Pengetal.2002),andin
Syria(Bashour,Kharoufetal.2008).ThehygienepromotionprogrammeinNigerconsisted
ofonetotwovillagemeetings(betweenoneandtwohourspermeeting)facilitatedby
villagehealthworkerstrainedonthespreadoftrachomaandstrategiestopreventits
91
transmission.Atleastonehandpumpwellwithpotablewaterwasalsoconstructedineach
programmevillage.ThericketspreventionprogrammeinChinaconsistedofdoctors
examiningchildrenforatotalofnineexamsandinstructingcaregiversonbasicnutritionand
vitaminDandcalciumsupplementation.InSyria,wherepostpartumcareisratherignored,
Bashourandcolleagues(2008)testedtheefficacyofhomevisitingbyregisteredmidwives.
Firsttimemotherswererandomlyassignedintooneofthreeconditions:(1)fourhomevisits
(1st,3rd,7thdayafterdelivery+4thweekafterdelivery),(2)onehomevisit,or(3)nohome
visits.
Homevisitationactivitiesincludedphysicalexaminations,educatingmothersonpostnatal
care,andprovidingemotionalsupport.Acrossallthementionedlow-dosagestudies,no
impactsontheoutcomesofinterestweredetected(SeeTable4inAppendix1).
FinallytwostudiesconductedinSenegalandMexicofoundnooverallimpactsbutimpacts
werefoundbasedonsub-groupanalyses.Bothstudiesgarneredlowqualityscores(<50%).
TheprogrammeinSenegalyieldedasignificantimpactondietarydiversitybutonlyforthe
oldestagegroup(24-35monthsofage)(Gartner,Kamelietal.2007).Moreover,the
evaluationalsoyieldedcounterintuitivefindings,favoringthecontrolgroup. Forinstance,
thecontrolgrouphadhigherratesofimmunizationagainstmeasles,butonlyforthe
youngestagegroup(6-11monthsofage),andgreaterratesofdeclineinwastingandbeing
underweightthantheprogrammegroup.TheprogrammeinMexicowastheevaluationof
theconditionalcashtransferprogramme,PROGRESA,onchildheight(Behrmanand
Hoddinott2005).Resultsoftheintent-to-treatanalysesshowednoimpactonheight;
however,afteremployingchildfixed-effectsestimatesthataccountedforunobserved
heterogeneitycorrelatedwithaccesstonutritionsupplements,theprogrammeaccounted
foranincreaseofaboutonesixthinchesperyear.Notethatintheprevioussection,
PROGRESA’seffectonheightwasstrongeramongtheyoungestinfantsatbaselinewho
livedinthepooresthouseholds(Rivera,Sotres-Alvarezetal.2004).
Summary Overall,appropriateparentalpracticesdonotseemtoimproveifthemodalityis
primarilydidactic—lecture-stylewithnodirectinteractionswithchildren,resultinginmaking
changesinchilddevelopmentlesslikely.Moreover,communityempowermentprogrammes
asevidencedintheVietnampositivedevianceapproachtocommunitynutrition

91
andintheIndianparticipatorylearningprogrammeamongwomen’sgroupswereineffective
inimprovinghealthandnutritionoutcomesbeyondsurvivalrateswhenimplemented
throughonlyonemodality. Additionalmodalitiesmaybenecessarysuchashome
visitationstocomplementtheseprogrammes.Intermsofdosage,lowdosageprogrammes
(between1and9sessions)thataredelivereddidacticallyareineffective.Evenhome
visitation,ifitconsistsofamaximumof4sessions,isineffectiveinimpactinginfanthealth
andhealthpracticesoffirsttimemothers.Finally,manyofthestudiesreviewedhaveshown
impactsonsub-groupsbyage,gender,oractualuptake.
3.2.4.2 Child Development and Parental Child Rearing Outcomes (n=7)
Thediscussioniscomprisedofthreelongitudinalfollow-upstudies,twochildprotection
programmes,andtwointegratedhealthanddevelopmentprogrammes.Exceptfortwo
ofthethreefollow-upstudies,therestwereevaluationsdeliveryofinstructionwas
primarilydidactic.
Longitudinal Follow-Up Evaluations.Threelongitudinalfollow-upevaluationsofa
breastfeedingpromotionprogrammeinBelarus(Kramer,Fombonneetal.2008),a
psychosocialstimulationprogrammeinJamaica(Chang,Walkeretal.2002),andanearly
careandstimulationprogrammeinTurkey(Kagitcibasi,Sunaretal.2009)makeupthis
section.ThestudyinBelaruswasthe6.5-yearfollow-upofthePROBITbreastfeeding
promotionprogramme(Kramer,Fombonneetal.2008);thestudyinJamaicawasthe
eight-yearfollowupof9-24montholdstuntedchildrenwhowereassignedrandomlyto
receiveeithernointervention,supplementationonly,stimulationonly,oracombinationof
stimulationandsupplementation(Chang,Walkeretal.2002);andthestudyinTurkeywas
the22-yearfollowupstudyofTEEP(Kagitcibasi,Sunaretal.2009).Thesethreestudies
examinedwhethertherewereanysustainedprogrammeimpactsonprimarilybehavioral
adjustmentoutcomes.Inthefollow-upofPROBIT,noevidenceoflong-termintervention
effectsonchildbehavioralproblemsormaternaladjustmentwasfound(Kramer,
Fombonneetal.2008).Inthefollow-upofJamaicaninfantswhowerenowbetween11-12
yearsofage,nodifferencesamongthefourconditionsweredetectedinimpactingparental
orteacher
92
ratingsofbehaviorandstandardizedtestsofacademicachievement(Chang,Walkeretal.
2002).Inthe22-yearfollow-upofTEEPchildren,nomaineffectsoneducationaloutcomes
orsocialadjustmentweredetected(Kagitcibasi,Sunaretal.2009).Child Protection Programmes. Twostudiesexaminedchildprotectionoutcomes.They
wereverydifferentintermsofstudygoals.Thefirststudyexaminedtheefficacyof
integratingpostnatalvisitsintoSwaziland’spreventionofmother-to-childtransmission
(PMTCT)programme—aformofpreventiveinterventionforHIV-positivewomen(Mazia,
Narayananetal.2009).Healthworkersvisitedhomestwicewithinoneweekofdeliveryto
delivercounselingmessagesonbasicpreventivecare,identificationofdangersigns,and
appropriatecare-seekingbehaviors.Theprogrammehadnoimpactonmothers’recallof
informationonbasiccareanddangersigns.Giventhatthemodeloftrainingwasatrain-
the-trainermodelandthat43%ofthestaffwereleftuntrainedduetoconflictingactivities,
thisstudyunderscorestheimportanceofensuringthatthesecondleveloftraineesreceive
adequatetraining.
Thesecondstudyexaminedtheeffectsofprolongedswaddling,acommontraditionin
Mongolia,onchilddevelopment(Manaseki-Holland,Spieretal.2010).Thehypothesis
ofthesecondstudywas,infact,toacceptthenullhypothesis—thatis,toprovethat
swaddlinghasnodeleteriouseffectsonchilddevelopment.Programmemotherswere
instructedtofollowatraditionalMongolianpatternofswaddling.Thepatternofswaddling
forthefirsttwomonthsweremoreintensive,butby7months,swaddlingwasrestrictedto
timeswheninfantswereasleep.Compliancewasmonitoredviahomevisitsanddiaries.
Resultsdemonstratedthatnosignificantdifferencesbetweenprogrammeandcontrol
infantswerefoundinstandardizedtestsofmentalandpsychomotorskills.Swaddling
infantsthroughoutinfancy,therefore,hadnodetrimentaleffectsonchildren’s
development.
Integrated Health and Development Programmes Twointegratedhealthand
developmentprogrammeswereunsuccessful:theCONIN(CorporationforChildhood
Nutrition)programmeinArgentinaandtheParentalEducationProgrammeinthe
Gambia.The
93
CONINstudyinArgentinawasaretrospectivequasi-experimentalstudyofchildrenages5-
17exposedtotheCONINunder-nutritionpreventioncenters(from1996-2005)andthose
whowerenotexposedtotheprogramme(Ortiz-Andrellucchi,Peña-Quintanaetal.2009).
Thestudytestedtheeffectsoftheprogrammeonahostofanthropometricmeasuresand
childdevelopmentaloutcomes.TheGambianstudywasaquasi-experimentalevaluationof
theParentalEducationProgrammeattheendofafour-yearperiod(Sidibeh2008).
Althoughbothprogrammesweresimilarintheirgoalofpromotingnutritionand
psychosocialsupportandstimulation,theyalsodifferedinafewways.
First,thetargetofinterventiondifferedforbothprogrammes.TheCONINprogramme
targetedmotherswhereastheParentalEducationProgrammetargetedparentsandother
caregivers(includingsiblings)aswellascommunityleadersandcivilservantsfrom
differentsocialsectors.Second,programmaticstrategiesdifferedalsoforboth
programmes.TheCONINprogrammeconsistedofnutritionworkshopsthatincluded
communitygardenswiththeaimofteachingparentshowtopreparenutritiousfoodsas
wellasofhomevisitswiththeaimofprovidingsupportandeducationontheimportance
ofstimulationandattachmentrelationships.Ontheotherhand,theParentalEducation
ProgrammeintheGambiaemployedatwo-prongedapproach:(1)acomprehensive
communicationstrategywithkeymessagesonnutrition,health,waterandsanitation,and
childdevelopmentandprotection;and(2)thedevelopmentofacomprehensiveparental
education(“train-the-trainer”)manualthatservedasaguidefortrainingnon-literate
communityvolunteers.Communityvolunteersthenconductedtheprogrammeinthe
formoffocusgroupdiscussions.Differentmaterialsweregeneratedtodisseminate
programme’scontent(i.e.songsweredevelopedthateducatedparentsonthe
relationshipbetweenearlylearningandtoys).Attheendoftheprogrammeperiod,nosignificantdifferenceswerefoundbetween
programmeandcomparisongroups(Sidibeh2008;Ortiz-Andrellucchi,Peña-Quintanaet
al.2009).Moreover,countertohypotheses,thenon-CONINchildrenhadlowerratesof
visualimpairmentandhigherlevelsofschoolachievementthanCONINchildren(Ortiz-
Andrellucchi,Peña-Quintanaetal.2009).Thenon-significantfindingsofbothstudies
maybeattributedtotheirlowqualityscoreratings(<50%)andtothefactthattheywere
94
primarilydidacticwithnomentionofdirectinteractionswithchildren.Programdosage
informationcouldnotbedeterminedineitherprogramme.Summary Thestudiesreviewedhereshowedthatbreastfeedingpromotion&psychosocial
stimulationprogrammeshavelongtermimpactsoncognitiveoutcomesbutnotonsocial
andemotionaldevelopment.Breastfeedingpromotionprogrammeshavebeenshownto
benefitextendedbreastfeeding,childhealthandgrowth,andmentaldevelopment,butnot
tomoredistaloutcomessuchaschildsocialandemotionaladjustmentandmaternalwell-
being.Psychosocialstimulationprogrammesmayhavelongtermimpactsonsocialand
emotionaloutcomesiftheyaretobecombinedwithpreschooleducationasseeninthe
TEEPstudy.Asahomevisitationprogrammeinitself,psychosocialstimulation
programmesmaynotbeaseffectiveinimprovingchildren’ssocialandemotional
developmentinthelongrun.Thisfindingsuggeststhatthedevelopmentofsocialand
emotionalskillsandwell-beingrequiresprogrammestotargettheseskillsdirectlyandover
timeincontextswherechildrenhavetousethem,e.g.preschoolProgrammesintheTEEP
model.Evidencefromsocialandemotionallearningprogrammessuggestthatteaching
theseskillsrequirebothqualitydeliveryandpositiveattitudesofimplementersto
effectivelyimpactchildren’ssocialandemotionalskills(Reyes,Brackett,Rivers,
Elbertson,&Salovey,2012).Intermsofevaluationdesign,quasi-experimentalstudieswithlowqualityscoresmaynot
havebeeneffectiveinfindingarepresentativecontrolgrouptomatchtheintervention
group.Finally,inevaluatingourfindings,onemusttakeintoconsiderationthedistinction
betweenimmediateprogrammeimpactsandlong-termfollow-upimpacts,andthe
distinctionbetweenpilotsandscaledupprogrammes.

96
CHAPTER4:DISCUSSIONThereistremendousdiversityaroundtheworldinparentingapproaches,philosophiesand
culturalconstructions.Howevertherearealsoafewuniversalpropertiesandcharacteristics
inparentingpractices,primaryamongwhichisthefunctionofparentingtonurturethe
survival,developmentandwellbeingofthechild. Thisfunctionisatriskformorethan1/3
oftheworld’syoungestchildrenasnotedbylackofstimulating,responsiveandsafe
parentingpracticesduetoanynumberofindividualand/orcontextualfactors. Parents,
especiallythemostvulnerableones,needtobesupportedintheirroleandabilitytocarry
outthefunctionofparenting. Thereforeparentingsupport,educationandtraining
programmesneedourattentiontoimplementeffectiveservicestohelpparentsand
families.
TheaimofthissystematicreviewhasbeentosynthesizetherecentmodelsofECD
parentingprogrammes,evaluatetheireffectivenessandidentifyprogramme
characteristicsthatcouldbescaleduptopromoteeffective,sensitiveandresponsivechild
rearingandcaringpractices,withaspecialfocusonthemostmarginalizedfamiliesand
vulnerablechildreninsupportofUNICEF’sequityapproach,inaglobalcontext. One
hundredandfivearticleswerereviewedcoveringECDparentingprogrammesfromLMIC
witharangeinfocifromhealth,nutrition,socialprotection,psychosocialsupportandearly
learningtoprogrammemodalities,deliverymechanisms,dose,andimpactonimproving
childandparentoutcomes.
Ingeneral,mostreportedprogrammesthatmetourinclusioncriteriashowedsignificant
resultsinimprovingchildand/orparentingoutcomes.ECDparentingprogrammesthat
aimedtopromotenutritionandhealth(56.2%)andprogrammesaimedtopromote
domainsofchilddevelopmentotherthanhealth(43.8%),ofthetotalnumberof
programmesthatmettheeligibilitycriteriaforthecurrentstudy.Thissuggeststhat
parentingprogrammesaremakingadifferenceinthelivesofchildrenandfamilies.Inthis
chapterwepresentourreviewandanalysesoftheresultsthatemergedfromeffective

97
practiceswiththeintentionofinformingimplementation.Wefocusonthecharacteristicsof
effectiveECDparentingprogrammeswiththeobjectiveofmakingrecommendationsforthe
nextgenerationofprogramming. Thecharacteristicsarepresentedinthreesections:what
weknowworks,knowledgegaps,andaddressingvulnerablefamilies.
4.1WHATWORKSINPARENTINGPROGRAMS
Acrossthereviewofthe105articles,weidentified3areasthatareimportanttoconsiderin
designing and implementing effective parenting programmes: programme dose;
programmequalityandprogrammetimingwithrespecttotheageofthechild.
4.1.1ProgrammeDose
Dosagehasbeenidentifiedasimportantforprogrammeeffectiveness.Howeverthereis
stillalackofconsensusinthedefinitionandmeasurementofdosage.Statedsimply,doseis
theamountoftheprogrammethatisdelivered(Wasik,Mattera,Lloyd,&Boller,2013).
Followingtheacceptedconceptualizationofinterventiondose,wereviewthethree
components:duration,frequency,andintensity.
Lowdoseprogrammesacrossduration,frequencyandintensityyieldednon-significant
programmeimpacts. Forexample,therelativelylow-doseprogrammes(between1and9
sessions)forhygienepromotioninNiger(Abdou,Munozetal.,2010),ricketsprevention
inChina(Strand,Pengetal.,2002),andpostpartumcareinSyria(Bashour,Kharoufetal.,
2008)hadnoimpactonchildorparentoutcomes.Thelowdose,inpart,mayhave
accountedforthelackofprogrammeeffectiveness,makingitanimportantcomponent
toconsiderinprogramming.
Duration isthelengthofthefullprogrammefromstarttofinish.Acrossthestudies,
tremendousvariationwasnotedinthelengthoftheparentingprogrammes. Ananalysis
of

97
theresultsrevealsthattheoptimallengthofaparentingprogrammeislinkedtothetypes
ofresultsitisabletoimpact.
Forimprovingchildleveloutcomes,indomainsofphysicalhealth,cognitivedevelopment
andsocialandemotionaldevelopment,thereviewsuggeststhat12monthsisthe
minimumdurationofaparentingprogramme.However,forprogrammesthatwere
implementedovera2-yearperiod,moreconsistentimpactwasnoted,inparticularfor
vulnerableanddisadvantagedpopulations. Forexample,theprogrammedurationofan
effectiveparentingprogrammeimplementedbySavetheChildrenJapaninruralVietnam,
wheretherewasahighprevalenceofstunting,wastwoyears(Watanabe,Floresetal.,
2005).ThecashtransferinterventioninMexico,Opportunidades,childreninfamilieswho
enrolledearlyorhadan18monthleadcomparedtochildreninthefamilieswhoenrolled
laterdidbetteronarangeofholisticchildoutcomes(Fernald,Gertleretal.,2009).With
respecttocognitivedevelopment,theTurkishEnrichmentProgramme,TEEP(Kagitcibasi,
Sunaretal.,2001),consistedof60bi-weeklyguidedgroupdiscussionsovertwoyears.
TheseexamplesillustratethattherecommendedECDparentingprogrammedurationis24
monthstoimpactchilddevelopmentaloutcomes.Forotheroutcomessuchasoralhealth,it
appearsthatlowdoseswillsuffice(e.g.,Mohebbietal.,2009;Pereira&Freire,2004).
Wealsocoveredprogrammesthatonlyreportedonparentleveloutcomes. Itappearsthat
shorterdurationprogrammesmightworkforparentlevelresults.Forexample,
programmestoreduceharshdisciplinelastonlyseveralmonthswhilethosetargetingto
changechildoutcomestook1to2years.Howeversuchacomparisonshouldbetreated
withcaution,sincechildoutcomesweremeasuredinareasofhealthanddevelopment
whileparentingoutcomesaremeasuredinadifferentdomain,suchasdiscipline.Also,the
latterisoftenmeasuredintermsofchangeinknowledgebutnotwithrespecttochangein
behavior.Regardless,itappearsthatreviewedprogrammesthataimtochangeparenting
knowledgecouldbeshorterindurationcomparedtoprogrammesthataimtoimprove
resultsforchildren.
99
The second component of dose is frequency orhowoftentheprogrammeis
delivered. Ascanbeexpectedhigherfrequencyparentingprogrammesweremoreeffective
inimprovingparentandchildoutcomes. Thelongitudinalresultsfromparenting
programmesarederivedprimarilyfromTEEPinTurkeyandthepsychosocialandnutrition
interventioninJamaicaindicatethattheprogrammefrequencyneedstobeatleastoncea
week.TheRovingCaregiversprogrammeinJamaicawasdeliveredtwiceperweek,aneven
higherfrequency.
Therearethreenotablepointswithrespecttoparentingprogrammefrequency. First,unlike
duration,impactingparentorchildoutcomesrequiresahighfrequency. Second,the
frequencyoftheprogrammedeliveryneedstobematchedwiththefrequencyofthe
parentsimplementingintheirdailylifewhattheyhavelearned. IntheTEEPmodel,for
example,mothersworkedwiththeirchildren15-20minutesaday. T h e frequencyof
parentingprogrammesneedtohaveafollowupathomefortheparentstodowithchildren
almostdaily.Third,thefrequencyoftheprogrammecanbepaced.Forexamplethe
integratedearlystimulationandnutritionprogramme(Hamadani,Hudaetal.,2006)for
malnourishedpopulationsvariedprogrammefrequencyoverthecourseofimplementation.
Theprogrammeconsistedofweeklygroupmeetingsfor10monthsfollowedbybi-weekly
meetingsfor2months,andbi-weeklyhomevisitsfor8months,followedbyweeklyhome
visitsfor4months.Theprogrammewaseffectiveinimprovingparentingpracticesandchild
outcomes.
Intensity isthethirdcomponentofdoseandhasbeendefinedasthestrengthofan
interventionorhowmuchoftheinterventionisdeliveredwithineachsession.Withrespect
tointensity,weexamineseveralcharacteristics.
First,thetimeallottedforeachsessionisanindicatorofintensity. Amongststudiesthat
reportedthetimeofeachsession,theyappearedtohavelastedfor45to60minutes. For
example,intheJamaicaintervention,eachhomevisitwas1hourlong.
Second,withrespecttointensityitisimportanttounderstandwhoisinvolvedinthe
100
session,suchastheparentonlyortheparentandthechild. Resultsfromthereview
suggestthatmoreintensiveapproaches,e.g.,directinteractionwithchild,areneededto
improveparentingleveloutcomes,forexample,caregivers’abilitytobeemotionally
responsive(Ertem,etal.,2006).Inthecaseoftheresponsivefeedingprogrammein
Bangladesh,resultsindicatedimprovementinchildweightandmaternalfeeding
practicesbutnotincognitiveandlanguagedevelopment,whentheprogrammetargeted
onlyparents.Howeverwhentheprogrammeinvolvedchildren,theirlanguageabilitywas
improvedsignificantly(AboudandAkhter,2011).Therefore,involvingchildreninthe
sessionscouldbeanapproachtoincreasingtheprogrammeintensity.
4.1.2ProgrammeModality
Programmemodalityreferstothemodeormannerinwhichtheparenting
programmewasconducted.
Fromthereviewofstudies,wefoundthatmodalityofaprogrammeisakeydeterminantin
thetheoryofchange.Modalityofaprogrammeinfluencesthetheoryofchangeand
consequentlytheprogrammeoutcome/s.Forexample,childcognitiveoutcomeswere
significantlyimprovedacrossbothhome-basedmodalitiesandcenter-basedprogrammes
thatusedgroupsettings.Howeveritwasthepsychosocialstimulationaspectofthe
programmes,whichentailsactiveengagementbetweenthecaregiverandthechildthatwas
effectiveinimprovingchildren’scognitivedevelopment.Therefore,ifthetheoryofchangeis
usedastheguidingfactorthentheprogrammemodality(inthiscase,groupsettingsand
psychosocialstimulation)canbeselectedaccordingly.
Besidesthetheoryofchange,thedesiredoutcomesoftheprogrammeshouldinfluence
themodality.Forexample,inthecaseofimprovingchildprotection,evidencefrom
programmesinBrazilandTurkeyshowedthatprovidingdemonstrationsorexamplesof
contrastingapproachestosafetyareeffectiveininformingparentalpracticesofsafety.
(Issler,Marosticaetal.2009);(Özyazıcıoğlu,Polatetal.2011).Groupmodalitieswerea
morecommonapproachtoparentingprogrammesthatareaimedatpromotingchild
protection
100
throughreducingharshdiscipline.However,inthecaseofpromotingbreastfeeding
practicesandhealthoutcomes,homevisitswerefoundtobeeffectivemodalities.
Therefore,decisionsregardingtheprogrammemodalityneedstobeguidedbytheaimsof
theprogramme.
Furthermore,thenumberofmodalitiesalsoprovidesanindicationofprogrammestrength
orintensity. Acrossthereviewedstudies,aconsistentresultwasthatprogrammesthat
usedmorethanonemodalityachievedbetterresultsthanprogrammesthatonlyusedone
modality.Forexample,thestudiesthatimprovedchildphysicalhealthoutcomesshowed
thatgroupsettingsmustbecombinedwithothermodalities.Thesefindingssuggestthat
byhavingparentsexposedtomultiplemodalitiesforalongperiodoftime,themessageof
appropriateandadequatenutritiongetsreinforced.Thereforecombinghomevisitswith
groupsessionsismoreeffectivethanonlyhomevisitsoronlygroupsessions(Engle,etal.,
2011).However,combiningprogrammemodalitiesisnotanadhocarrangementofservices.
Rather,thereneedstobecriteriathatguidetheapproach.Modalitiesneedtobebridged.
Forexample,inthePhilippines(Armecin,Behrmanetal.2006),thecenter-andhome-
basedserviceswerelinkedbytheCDWswhocomplementedtherolesofmidwivesand
healthworkersinprovidingfoodandnutritionalsupplementsandmonitoringchildren’s
healthstatus.CDWsalsoprovidedcommunity-basedparentingeducationaboutECD.In
providingthisbridge,theprogrammewasabletomaximizethestrengthorintensityofthe
dosetoachieveimpactonparentandchildoutcomes.
4.1.3ServiceProvision
Thethirdelementofwhatworkswithparentingprogrammesisensuringhighquality
programmes. Oneofthemainfeaturesofqualityasgleanedthroughthereviewisthe
serviceproviderandtheirabilitytodeliverandmaintaintheprogrammeeffectively.
101
Authorityfigures,suchasdoctors,nurses,educators,forexamplewereamongthemost
successfulserviceprovidersinimprovingparentingoutcomes. Forexample,asignificant
increaseinparentingknowledgewasassociatedwithprofessionalserviceproviders(Moran,
Ghateetal.2004).Nutritioneducationprogrammesweremoreeffectivewhenthe
professionalsdeliveredthehealthmessages.Thereasonwhyauthorityfiguresmightbe
effectiveisbecauseparentsmayinterprethealthcareprofessionalsasexpertsinthefield
andarethereforemoreamenabletolisteningtothemandfollowingtheirguidance.
However,therealityofthesituationwithrespecttoECDprogrammesisthatthevast
majorityoftheprogrammesaredeliveredbycommunityworkersorparaprofessionals.The
fieldasawholeisfarfromhavingaprofessionalworkforce.Thereforeinourreview,wealso
examinedcommunity-basedapproachestoidentifyeffectivefactorsassociatedwith
servicesdeliveredbynon-professionalsorserviceproviderswithlimitedtraining.
Trainedlocalfemalecoordinatorswithrelativelyhighlevelsofeducationwerealsoeffective
indeliveringtheprogrammeacrosshomeandinthegroupsettings.Theseserviceproviders
thoughneedfairlyintensivetrainingnotonlyintheprogrammeapproachbutalsointerms
oftechniques.Forexample,bothlivemodelinganddirectinstructionhavebeenusedwith
successtoteachmothershowtointeractwiththeirchildren.Thesearetechniquesinwhich
serviceprovidersneedtobetrained.Thesefindingsareconsistentwiththosefromnon-
LMIC,whichrevealedthatstrategiesassociatedwithimprovingbothchildandparent
outcomesincluded:(i)trainingparentshowtointeractpositivelywiththeirchildrenona
dailybasis(real-lifeeverydayscenarios)and(ii)livemodeling(practicingnewlylearnedskills
withtheirownchild)vs.role-playingwithapeerortrainer(Kaminski,Valleetal.
2008).Thecommunity-basedprogrammesthatpromotehealthandnutritionindicatethat
employinglocalleaders,e.g.,theImamsinBangladeshandcommunitytheatreactorswith
scriptwrittenforthelocalcommunitymightbealternativestrategiestoconsider(Arifeenet
al.,2009). Acommonstrategyusedintheprogrammesreviewedcapitalizedonavailable
communityresourcestodelivertheprogramme.ForexampletheDularmodelinIndia
102
capitalizedanddevelopedcommunityresourcesatthegrassrootsleveltoimprove
nutritionalpracticesanddecreasemalnutrition(Dubowitz,Levinsonetal.2007).
Insummary,oneofthemainissuesofprogrammequalityappeartobelinkedwiththe
abilityoftheserviceproviderandcurrentlythevastmajorityofECDparenting
programmesusecommunityworkersorparaprofessionalstodeliverservices.The
strategiesforimprovingprogrammequalityarestillunclear,thoughstrengtheningthe
capacityoftheserviceproviders,usingprofessionalsandlocalleadershavebeen
associatedwithsignificantpositiveresults.
4.1.4TimingofProgramme
Giventhattheearlyyearsareatimeofextraordinarilyrapidgrowthandchange,parents’
interestinissuesofchilddevelopmentiscloselylinkedtotheageofthechildandthestage
oftheirdevelopment.Certaintypesofnutritionalprogrammesaremoreappropriatefor
certainagegroupsofchildren. Furthermore,giventhatchilddevelopmenthassensitive
windowsitisimportanttomaximizetheinfluenceofparentingbydesigningprogrammes
thatareageappropriate.
Ingeneral,acrossthestudiesreviewed,therewasnoclearsetofresultswithrespectto
programmetimingandageofthechild.Howeverafewillustrativeexamplesdoprovide
guidanceforprogrammedesign.Oneoftheclearestexamplesfortimingofaparenting
interventionarebreastfeedingprogrammesbecausetheyhavetocommenceinthefirst
momentsofachild’slife.Resultsfrombreastfeedingprogrammesdidshowresultsfor
improvedhealthpracticesformothersandforinfantsintermsoflong-termbenefitsfor
theircognitivedevelopmentandphysicalhealth. Thepsychosocialstimulation
programmesrangedfromwhenchildrenwereafewmonthsoldtoalmost6yearsofage.
Thereforediscerningtheappropriatetimingtocommenceapsychosocialinterventionis
challengingbasedonthisreview. Finally,intermsofdevelopmentaltiming,impactson
anthropometrywerestrongerforchildrenwhowereexposedtotheprogrammewhen
theywereyoungerasseenin
103
thenutritionandhealthprogrammefromHaiti(Ruel,Menonetal.2008,Donegan,
Maluccioetal.2010).
4.2KNOWLEDGEGAPS
ThereviewhasbeenincrediblyinformativeinunderstandingwhatworksforECDparenting
programmestoimproveparentandchildoutcomes. Howevertherearestillseveralareas
thatneedfurtherresearchandexamination,ifwearetotrulyimprovetheeffectivenessof
programmes.
4.2.1Socialprotectionprogrammesandparenting
Oneofthelargestinfluencesonparentingistheavailabilityofresourcesthatallowparents
toprovidefortheirchildreninthebestpossiblemanner.Low-incomefamiliesandthose
livinginpovertyareoftenatriskforpoorerdevelopmentaloutcomesandthereforein
greaterneedofparentinginterventions. Socialprotectionprogrammes,suchascash
transferprogrammesareemergingasoneofthemostimportantmeanstoreachpoor
families.Parentingprogrammestargetthemostvulnerablepopulations.Thereforecash
transferprogrammesarepotentiallyeffectivemechanismstodeliverparentingeducationto
thesepopulations.TheresearchfromMexicoandNicaraguasuggeststhatsucha
combinationmaybeverybeneficialforthefamiliesbecausenotonlydoesitprovidethe
financialresourcesthattheparentsneedtoraisetheirfamilybutalsotheinformationand
skillstousethosefundsandparenttheirchildren. Furtherresearchisneededtoaddressthe
feasibilityofintegratingexplicitlyECDparentingeducationintocashtransferprogrammes
andassesstheirimpactsonimprovingormediatingtheeffectsofcashtransferson
outcomes.Theimpactsofthisapproachonotheroutcomedomainsarereportedinother
sectionsofthisreview.
104
4.2.2MaternalmentalhealthOneofthesignificantinfluencesonparentingismaternalmentalhealth. However,fewto
noneofthestudiesexplicitlyaddressedthisimportantmediatorbetweenprogrammesand
childoutcomes(Shawetal.,2009).Althoughweexcludedstudiesofprogrammesspecifically
targetingwomendiagnosedwithdepressionandotherhealthproblems;twoofthestudies
wefoundconsideredmaternaldepressionasanareatoaddressthroughtheirparenting
programmes.Bothprogrammes,however,wereunsuccessfulinalleviatingmaternal
depression(Cooperetal.,2009;Rahmanetal.,2009).Bothprogrammesemployedtrained
paraprofessionals,suggestingthataddressingmaternaldepressionmayrequiremorehighly
trainedprofessionals.Alternatively,treatingmaternaldepressionmayrequiremore
targetedprogrammesaimedspecificallyatthisissue.Thisisanareaforfurtherworkand
inquiry.
4.2.3ScalingUpofECDParentingProgrammes
Mostofthestudiesincludedinthereviewwerebasedonsmall-scaledemonstration
programmes.Therewereahandfulofstudiesthatwerebasedonscaledupprogrammes.In
thestudies,ingeneraltherewaslittleinformationonscale-up. Afewexampleswere
presentedthatwedrawontopresentasetofconclusions. First,linkingprogrammesto
existingpoliciesprovidedamechanismtoenhancepolicyimplementation.Multisectoral
partnershipshavebeennotedasthekeyingredienttoprogrammaticsuccess.Theworkfrom
UgandanandSenegaleseprogrammes,whichcapitalizedonthesupportofparishactivities
andanationalmultisectoralcoordinatingbody,respectively,weresuccessfulinimpacting
ratesofbeingunderweightandparentalcaregivingbehaviors(Alderman2007;Alderman,
Ndiayeetal.2009).Nutritioneducationprogrammesthatareintegratedintoexisting
programmesorstructuressuchasnutritionservices(Penny,Creed-Kanashiroetal.
2005;Waters,Pennyetal.2006)orearlychildhoodservices(Ghoneim,Hassanetal.2004)
aremoreeffective.Howeversuchexampleswerefewandfarbetween.
105
Scalingupatthecommunitylevelwasalsoexploredinthereview. Theresultssuggestthat
communityempowermentprogrammesinandofthemselvesmaynotbeaseffectivein
improvingchildphysicalwell-beingandmaternalcaregivingbehaviorsbeyondchildhood
survival.Otherprogrammingmodalities,suchashomevisitsmayhavetobecombined
withthisprogrammaticapproachtoyieldmorepositiveprogrammeimpacts(Schroeder,Pach
etal.2002;Tripathy,Nairetal.2010).Ingeneralmoreresearchandevidenceisneededintheimplementationscienceofscalingup
ECDParentingprogrammes.4.2.4RoleofFathersintheParentingProcess
Fathersingeneralareunder-studiedinECDparentingprogrammes(Barker,Bartlettetal.
2004,UnitedNationsDepartmentofEconomicandSocialAffairs2011).Threestudies
acrosstheentirereviewlookedatfathersasrecipientsofparentingprogrammes.(Koçak
2004)(AlHassanandLansford2011).Twoofthethreewereondiscipline.Theresultsclearly
indicateamuchgreaterneedtoincludefathersinparentinginterventions,notmerelyas
maternalsupportbutasfactorsinfluencingchildoutcomes.
4.2.5NextGenerationIssuesforECDParenting
Effectiveparentingprogrammesrequireabalancebetweensupplyofservicesanddemand
forservices. Parentingisademandsideissue.But,acrossourreview,noworkhadbeen
completedonthedemandsideofparentingprogrammes.
Afewstudiesexaminedincreasinguptakeoftheprogrammes.Forexamplethe
community-basedprogrammeinBrazil,whenofferinggroupsessions(inadditionto
homevisits),recommendedthattransportationandrefreshmentsshouldbeprovided.
Otherrecommendationsincludedprovidingconvenientservice,suchaschildcareservices
while
106
parentsareinattendance,ortransportationservicesforruralfamilies—aswellasoffering
programmesatconvenientlocations(e.g.,office,preschool,communitycenters)andtimes
(includingeveningsandweekendswhenthereisademand)wereexaminedasfactorsthat
increaseparticipationrates(Moran,Ghateetal.2004).HoweverdemandforECDparenting
programmeswasnotstudiedconsistently.
Alsotheattentiontochildsocialandemotionaloutcomeswaslimited.Inordertoimprove
holisticoutcomesforchildren,parentingprogrammeshavetomovebeyondphysicalhealth
andcognition.Althoughsomestudiesdidexaminesocialandemotionaldevelopment,they
wereinaminority.
4.2.6ComprehensiveandContextualMeasures
Regardingmetricsandstudydesigns,thesystematicreviewalsorevealedthatmeasuresto
assesstheimpactofprogrammesontheattitudes,practicesandbehaviorsofparents
consistprimarilyofself-reports,whichpresentrisksofreportingbiases.Furthermore,there
isvirtuallynopresenceofimpactevaluationsthataddressbiophysiologicalimpactsof
programmesatthechildlevel.Mostphysicaleffectsaddressanthropometricindicatorsbut
ignoreimportantdimensionssuchasbiomarkersofstressandattachment.Longitudinal
studiesofECDparentingprogrammesarelacking,inparticularonoutcomeslinkedwith
long-termhealth,prosocialbehaviors,adultproductivity,andothersustainableimpacts
associatedwithsocialtransformation.Lastly,programmeevaluationsoftendonotcontrol
formacro-levelcovariates(e.g.accesstoservices,presenceorabsenceof
conflict/displacement,environmentaldeterminants,etc.),providinganincompletepicture
ofthecontextofthechild.

107
4.3EQUITYTHROUGHPARENTING
Mostparentingprogrammesaddressvulnerablefamiliesandclearresultswerenotedfor
improvingequityinchildoutcomes. Forexample,malnourishedchildrenandyoungerage
groupsbenefitedthemostfromtheseprogrammes(Watanabe,Floresetal.2005).
Howevertheprogrammesalsohadtobeofahigherquality.Malnourishedpopulations
benefitedfromservicesthatinvolvedprofessionalsandexperts(Santos,Victoraetal.2001;
Ghoneim,Hassanetal.2004)oracombinationofprofessionalsandparaprofessionals
(Penny,Creed-Kanashiroetal.2005;Roy,Fuchsetal.2005;Waters,Pennyetal.2006).
Sincethesituationofvulnerablepopulationsismorecomplexthereisagreaterneedfor
proficiencyintheimplementationprocess.Forexample,inBangladesh,doctorsreceived20-
hourtraininginnutritioncounselingfollowingtheIMCIfeedingguidelines(Santos,Victora
etal.2001)resultinginbettermaternalrecallofdietaryrecommendationsandmaternal
reporteduseofrecommendedfoodsandfeedingpractices.Althoughpsychosocial
stimulationprogrammeswereeffectiveinimprovingcognitiveoutcomeswhentargeting
impoverishedgroups,malnourishedchildrenstillperformedwellbelowtheirnon-
impoverishedcounterparts.

REFERENCESAbdou,A.,etal.(2010)."Howmuchisnotenough?AcommunityrandomizedtrialofaWaterandHealthEducationProgrammeforTrachomaandOcularC.trachomatisinfectioninNiger."TropicalMedicine&InternationalHealth15(1):98-104.
Aber,L.,etal.(2013).Socialprotectionandwelfaresystems.Implicationsforearlychildhooddevelopment.Handbookofearlychildhooddevelopmentresearchanditsimpactonglobalpolicy.
Aboud,F.E.(2007)."EvaluationofanearlychildhoodparentingProgrammeinruralBangladesh."JournalofHealth,Population&Nutrition25(1):3-13
*4Aboud,F.E.andS.Akhter(2011)."Acluster-randomizedevaluationofaresponsivestimulationandfeedinginterventioninBangladesh."Pediatrics127(5):e1191-e1197.
OBJECTIVES:Thegoalofthisstudywastodetermineifaresponsivestimulationandfeedinginterventionimproveddevelopmentalandnutritionaloutcomescomparedwitharegularinformation-basedparentingprogramme.Thehypothesiswasthatmothersintheinterventionwouldexhibitbetterparentingskillsandchildrenwouldexhibitbetterdevelopmentalandnutritionaloutcomesthancontrols.METHODS:Acluster-randomizedfieldtrialwasconductedwith302childrenaged8to20monthsandtheirmothersinruralBangladeshwhowererandomlyassignedaccordingtovillageto1of3groups.Thecontrolmothersreceived12informationalsessionsonhealthandnutrition.Theinterventiongroupsreceivedanadditional6sessionsdeliveredbypeereducatorswhoincludedmodelingandcoachedpracticeinself-feedingandverbalresponsivenesswiththechildduringplay.Asecondinterventiongroupreceived,alongwiththesessions,6monthsofafoodpowderfortifiedwithmineralsandvitamins.DevelopmentaloutcomesincludedtheHomeObservationforMeasurementoftheEnvironment(HOME)Inventory,mother-childresponsivetalk,andlanguagedevelopment.Nutritionaloutcomesincludedweight,height,self-feeding,andmouthfulseaten.Weusedanalysisofcovariancetocomparethe3groupsattheposttestandatfollow-up,covaryingthepretestlevelsandconfounders.RESULTS:Atfollow-up,responsivestimulation-feedinggroupshadbetterHOMEinventoryscores,responsivetalking,language,mouthfulseaten,andhand-washing.Micronutrientfortificationresultedinmoreweightgain.CONCLUSIONS:Abriefbehavior-changeprogrammethatfocusedonmodelingandpracticeinstimulationandfeedingwas
*Note:Annotatedreferencesareapartofthesystematicreview.
108

109
foundtobenefitchildren'snutritionandlanguagedevelopment.Micronutrientsbenefitedchildren'sweightbutnotlength.Aboud,F.E.,etal.(2008)."Effectivenessofacommunity-basedresponsivefeedingProgrammeinruralBangladesh:aclusterrandomizedfieldtrial."Maternal&ChildNutrition4(4):275-286.
Aboud,F.E.,etal.(2009)."Aresponsivefeedinginterventionincreaseschildren'sself-feedingandmaternalresponsivenessbutnotweightgain."TheJournalofNutrition139(9):1738-1743.
Akmatov,M.K.(2011)."Childabusein28developingandtransitionalcountries—resultsfromtheMultipleIndicatorClusterSurveys."InternationalJournalofEpidemiology40(1):219-227.
AlHassan,S.M.andJ.E.Lansford(2011)."EvaluationofthebetterparentingProgrammeinJordan."EarlyChildDevelopmentandCare181(5):587-598.
Alderman,H.(2007)."Improvingnutritionthroughcommunitygrowthpromotion:LongitudinalstudyofthenutritionandearlychilddevelopmentprogrammeinUganda."WorldDevelopment35(8):1376-1389.
Alderman,H.,etal.(2009)."EffectivenessofaCommunity-basedinterventiontoimprovenutritioninyoungchildreninSenegal:adifferenceindifferenceanalysis."PublicHealthNutrition12(05):667-673.
Alkizim,F.,etal.(2011)."Childhooddiarrhoea:Failingconventionalmeasures,whatnext?"PanAfricanMedicalJournal8(1).
Allen,L.H.(1994)."Nutritionalinfluencesonlineargrowth:Ageneralreview."EuropeanJournalofClinicalNutrition48(1):75-89.
Anda,R.F.,Felitti,V.J.,Bremner,J.D.,Walker,J.D.,Whitfield,C.,Perry,B.D.,Dube,S.R.,&Giles,W.H.(2006).“Theenduringeffectsofabuseandrelatedadverseexperiencesinchildhood.”EuropeanArchivesofPsychiatryandClinicalNeuroscience,256,174-186.
Arabi,M.,Frongillo,E.A.,Avula,R.andMangasaryan,N.(2012),“InfantandYoungChildFeedinginDevelopingCountries.”ChildDevelopment,83:32–45.
110
Arifeen,S.E.,etal.(2009)."EffectoftheIntegratedManagementofChildhoodIllnessstrategyonchildhoodmortalityandnutritioninaruralareainBangladesh:aclusterrandomisedtrial."TheLancet374(9687):393-403.
Armecin,G.,etal.(2006).Earlychildhooddevelopmentthroughanintegratedprogramme:EvidencefromthePhilippines.WorldBankPolicyResearchWorkingPaper3922.Washington,DC,TheWorldBank.
Bajait,C.andV.Thawani(2011)."Roleofzincinpediatricdiarrhea."Indianjournalofpharmacology43(3):232.
Bang,A.T.,etal.(2005)."LowBirthWeightandPretermNeonates:CantheybeManagedatHomebyMotherandaTrainedVillageHealthWorker?"JournalofPerinatology25(S1):S72.
Bang,A.T.,etal.(2005)."ReducedIncidenceofNeonatalMorbidities:EffectofHome-BasedNeonatalCareinRuralGadchiroli,India."JournalofPerinatology25(S1):S51.
Barker,G.,etal.(2004).Supportingfathers:ContributionsfromtheInternationalFatherhoodSummit2003.TheHague,Netherlands,BernardVanLeerFoundation.
Bartlett,S.N.(2002)."Theproblemofchildren’sinjuriesinlow-incomecountries:Areview."HealthPolicyandPlanning17(1):1-13.
Bashour,H.N.,etal.(2008)."Effectofpostnatalhomevisitsonmaternal/infantoutcomesinsyria:Arandomizedcontrolledtrial."PublicHealthNursing25(2):115-125.
Baumrind,D.(1996)“TheDisciplineControversyRevisited”.FamilyRelations,45(4):405-414.
Behrman,J.R.andJ.Hoddinott(2005)."Programmeevaluationwithunobservedheterogeneityandselectiveimplementation:TheMexicanPROGRESAimpactonchildnutrition."OxfordBulletinofEconomicsandStatistics67(4):547-569.
Bekman,S.,etal.(2004).AmodelofearlyinterventioninSouth-eastTurkey:Apilotimplementionofthe"SummerPreschool.Researchreport.Turkey,MotherChildEducationFoundation.

111
Bhandari,N.,etal.(2003)."Effectofcommunity-basedpromotionofexclusivebreastfeedingondiarrhoealillnessandgrowth:aclusterrandomisedcontrolledtrial."TheLancet361(9367):1418-1423.
*Bhandari,N.,Bahl,R.,Nayyar,B.,Khokhar,P.,Rohde,J.E.,Bhan,M.K.(2001)."Foodsupplementationwithencouragementtofeedittoinfantsfrom4to12monthsofagehasasmallimpactonweightgain."TheJournalofNutrition131(7):1946-1951.
Itisunclearwhetherasubstantialdeclineinmalnutritionamonginfantsindevelopingcountriescanbeachievedbyincreasingfoodavailabilityandnutritioncounselingwithoutconcurrentmorbidity-reducinginterventions.Thestudywasdesignedtodeterminewhetherprovisionofgenerousamountsofamicronutrient-fortifiedfoodsupplementsupportedbycounselingornutritionalcounselingalonewouldsignificantlyimprovephysicalgrowthbetween4and12monthsofage.Inacontrolledtrial,418infants4monthsofagewereindividuallyrandomizedtooneofthefourgroupsandfolloweduntil12monthsofage.Thefirstgroupreceivedamilk-basedcerealandnutritionalcounseling;thesecondgroupmonthlynutritionalcounselingalone.Tocontrolfortheeffectoftwice-weeklyhomevisitsformorbidityascertainment,similarvisitsweremadeinoneofthecontrolgroups(visitationgroup);thefourthgroupreceivednointervention.Themedianenergyintakefromnonbreastmilksourceswashigherinthefoodsupplementationgroupthaninthevisitationgroupby1212kJat26wk(P<0.001),1739kJat38wk(P<0.001)and2257kJat52wk(P<0.001).Thefoodsupplementationinfantsgained250g(95%confidenceinterval:20–480g)moreweightthandidthevisitationgroup.Thedifferenceinthemeanincrementinlengthduringthestudywas0.4cm(95%confidenceinterval:−0.1–0.9cm).Thenutritionalcounselinggrouphadhigherenergyintakesrangingfrom280to752kJatdifferentages(P<0.05atallages)butnosignificantbenefitonweightandlengthincrements.Methodstoenhancetheimpactoftheseinterventionsneedtobeidentified.
Bhandari,N.,etal.(2005)."Useofmultipleopportunitiesforimprovingfeedingpracticesinunder-twoswithinchildhealthProgrammes."HealthPolicyandPlanning20(5):328-336.
*Bhandari,N.,etal.(2004)."AneducationalinterventiontopromoteappropriatecomplementaryfeedingpracticesandphysicalgrowthininfantsandyoungchildreninruralHaryana,India."TheJournalofNutrition134(9):2342-2348.
Complementaryfeedingpracticesareofteninadequateindevelopingcountries,resultinginasignificantnutritionaldeclinebetween6and18monthsofage.Weassessedtheeffectivenessofaneducationalinterventiontopromoteadequatecomplementaryfeedingpracticesthatwouldbefeasibletosustainwithexistingresources.Thestudywasaclusterrandomizedcontrolledtrialincommunitiesinthe
112
stateofHaryanainIndia.Wedevelopedtheinterventionthroughformativeresearch.Eightcommunitieswerepairmatchedontheirbaselinecharacteristics;oneofeachpairwasrandomlyassignedtoreceivetheinterventionandtheothernospecificfeedingintervention.Healthandnutritionworkersintheinterventioncommunitiesweretrainedtocounselonlocallydevelopedfeedingrecommendations.Newbornswereenrolledinallofthecommunities(552intheinterventionand473inthecontrol)andfollowedupevery3monthstotheageof18months.Themainoutcomemeasureswereweightsandlengthsat6,9,12,and18monthsandcomplementaryfeedingpracticesat9and18months.Allanalyseswerebyintenttotreat.Intheoverallanalyses,therewasasmallbutsignificanteffectonlengthgainintheinterventiongroup(differenceinmeans0.32cm,95%CI,0.03,0.61).Theeffectwasgreaterinthesubgroupofmaleinfants(differenceinmeanlengthgain0.51cm,95%CI0.03,0.98).Weightgainwasnotaffected.Energyintakesfromcomplementaryfoodsoverallweresignificantlyhigherintheinterventiongroupchildrenat9months(mean±SD:1556±1109vs.1025±866kJ;P<0.001)and18months(3807±1527vs.2577±1058kJ;P<0.001).Improvingcomplementaryfeedingpracticesthroughexistingservicesisfeasiblebuttheeffectonphysicalgrowthislimited.Factorsthatlimitphysicalgrowthinsuchsettingsmustbebetterunderstoodtoplanmoreeffectivenutritionprogrammes.
Bhutta,Z.Aet.al,(2010).“Countdownto2015decadereport(2000-10):takingstockofmaternal,newborn,andchildsurvival”.TheLancet.375(9730):2032-2044.
Black,R.E.,etal.(2010)."Global,regional,andnationalcausesofchildmortalityin2008:Asystematicanalysis."Lancet375(9730):1969-1987.
Bornstein,M.H,(2002).“HandbookofParentingVolume4SocialConditionsandAppliedParenting”.PsychologyPress.
Bornstein,M.H.andD.L.Putnick.(2012).“CognitiveandSocioemotionalCaregivinginDevelopingCountries”.ChildDevelopment.83(1):46-61.
Bowlby,J(1988).“ASecureBase:Parent-ChildAttachmentandHealthyHumanDevelopment”.BasicBooks.
Brackett,M.A.,etal.(2011)."Emotionalintelligence:Implicationsforpersonal,social,academic,andworkplacesuccess."SocialandPersonalityPsychologyCompass5(1):88-103.
Bradley,R.H.(2004).“Chaos,culture,andcovariancestructures:Adynamicsystemsviewofchildren'sexperiencesathome.”Parenting,4(2-3):243-257.

113
Bradley,R.H.andR.F.Corwvn,(2005).“CaringforChildrenAroundtheWorld:AviewofHOME”.InternationalJournalofBehavioralDevelopment29(6):468-478.
113
Britto,P.R.,Fuligni,A.S.,&Brooks-Gunn,J.(2002).“Reading,rhymes,androutines:Americanparentsandtheiryoungchildren.ChildrearinginAmerica:Challengesfacingparentswithyoungchildren.”CambridgeUniversityPress.
Britto,P.R.,Brooks-Gunn,J.,&Griffin,T.(2006).StoryReadersandStoryTellers:StylisticDifferencesinLowIncome,Young,African-AmericanMothers'ReadingStyles.ReadingResearchQuarterly.41,68-89.
Britto,P.R.,Engle,P.L.,&Alderman,H.(2007)."Earlyinterventionandcaregiving:EvidencefromtheUgandaNutritionandEarlyChildDevelopmentprogramme."ChildHealthandEducation1(2):112-133.
Britto,P.R.,Yoshikawa,H.,&Boller,K.(2011).Qualityofearlychildhooddevelopmentprogrammesinglobalcontexts:Rationaleforinvestment,conceptualframeworkandimplicationsforequity.SocialPolicyReport.Vol.25,No.2.
Britto,P.R.andN.Ulkuer,(2012).“ChildDevelopmentinDevelopingCountries:ChildRightsandPolicyImplications.”ChildDevelopment83(1):92-103.
CampbellCollaboration(2010). RetrievedNovember20,2014fromhttp://www.campbellcollaboration.org
Cardoso,L.O.,etal.(2008)."TheimpactofimplementationoftheBreastfeedingFriendlyPrimaryCareInitiativeontheprevalenceratesofbreastfeedingandcausesofconsultationsatabasichealthcarecenter."JornaldePediatria84(2):147-153.
*Chang,S.M.,etal.(2002)."Earlychildhoodstuntingandlaterbehaviorandschoolachievement."JournalofChildPsychology&Psychiatry&AlliedDisciplines43(6):775-783.
BACKGROUND:Stuntinginearlychildhoodiscommonindevelopingcountriesandisassociatedwithpoorercognitionandschoolachievementinlaterchildhood.Theeffectofstuntingonchildren’sbehaviorsisnotaswellestablishedandisexaminedhere.METHOD:Childrenwhowerestuntedatage9to24monthsandhadtakenpartina2–yearinterventionProgrammeofpsychosocialstimulationwithorwithoutnutritionalsupplementationwerereexaminedatage11–12yearsandcomparedwithnonstuntedchildrenfromthesameneighbourhoods.TheirschoolandhomebehaviorswereassessedusingtheRutterTeacherandParentScalesandschoolachievementwasmeasuredusingtheWideRangeAchievementTest(WRAT)andtheSuffolkReadingScales.RESULTS:Nosignificantinterventioneffectswerefoundamongthestuntedgroups.Thusdatafromthefourinterventiongroupswereaggregatedforsubsequentanalyses,comparingall116stuntedchildrenwith80non–stuntedchildren.Controllingforsocialbackgroundvariables,thestunted

114
grouphadmoreconductdifficulties(p<.05)asratedbytheirparents.Theyalsohadsignificantlylowerscoresinarithmetic,spelling,wordreadingandreadingcomprehensionthanthenon–stuntedchildren(allp<.001).Conductdifficultiesand
114
hyperactivitywererelatedtopoorerschoolachievement.Controllingforthechildren’sIQ,thestuntedchildren’sarithmeticscoresremainedsignificantlylowerthanthoseofthenon–stuntedchildren,butreadingandspellingscoreswerenotdifferent.Conclusions:Previouslystuntedchildrenhadmoreconductdifficultiesathome,regardlessoftheirsocialbackground,thannon–stuntedchildren.Theireducationalattainmentwasalsopoorerthannon–stuntedchildrenandtheseresultsaresuggestiveofaspecificarithmeticdifficulty.Childrenwithbehaviorproblemsperformedlesswellatschool.[ABSTRACTFROMAUTHOR]
CopyrightofJournalofChildPsychology&Psychiatry&AlliedDisciplinesisthepropertyofWiley-Blackwellanditscontentmaynotbecopiedoremailedtomultiplesitesorpostedtoalistservwithoutthecopyrightholder'sexpresswrittenpermission.However,usersmayprint,download,oremailarticlesforindividualuse.Thisabstractmaybeabridged.Nowarrantyisgivenabouttheaccuracyofthecopy.Usersshouldrefertotheoriginalpublishedversionofthematerialforthefullabstract.(CopyrightappliestoallAbstracts.)
Chezem,J.C.,etal.(2006)."Breastfeedingknowledge,breastfeedingconfidence,andinfantfeedingplans:Effectsonactualfeedingpractices."JournalofObstetric,Gynecologic,&NeonatalNursing32(1):40-47.
Claveland,G.,Corter,C.,Pelletier,J.,Colley,S.,Bertrand,J.,Jamieson,J.(2006).AReviewoftheStateoftheFieldofEarlyChildhoodLearningandDevelopmentinChildCare,Kindergarten,andFamilySupportProgrammes.FromtheAtkinsonCentreforSocietyandChildDevelopment.
Cogill,B.(2003).Anthropometricindicatorsmeasurementguide.Washington,DC,FoodandNutritionalTechnicalAssistanceProject,AcademyforEducationalDevelopment.
Cooper,P.J.,etal.(2009)."Improvingqualityofmother-infantrelationshipandinfantattachmentinsocioeconomicallydeprivedcommunityinSouthAfrica:Randomisedcontrolledtrial."BritishMedicalJournal338:1-8.
Cowan,C.P,Cowan,P.A.,Pruett,M.K.,&Pruett,K.(2007).“AnApproachtoPreventingCoparentingConflictinDivorceinLow-incomeFamilies:StrengtheningCoupleRelationshipsandFosteringFather’sInvolvement.”FamilyProcess,46(1):109-121.
Cropley,L.(2004).“Theeffectsofhealtheducationinterventionsonchildmalariatreatment-seekingpracticesamongmothersinruralrefugeevillagesinBelize,CentralAmerica”.HealthPromotionInternational.19(4):445-452
*Cumberland,P.,etal.(2008)."TheimpactofcommunityleveltreatmentandpreventativeinterventionsontrachomaprevalenceinruralEthiopia."InternationalJournalof

115
Epidemiology37(3):549-558.

115
BACKGROUND:TheInternationalTrachomaInitiative(ITI)trachomacontrolProgrammebasedontheSAFEstrategy(Surgery,Antibiotics,FacialcleanlinessandEnvironmentalimprovement)wasimplementedin2002intworuralEthiopianzones,withmassdeliveryofazithromycinstartingin2003.WeevaluatetheimpactofcombinedantibioticandhealtheducationalinterventionsonactivetrachomaandChlamydiatrachomatisdetectedfromocularswabs,inchildrenaged3–9years.METHOD:Three-yearfollow-upcross-sectionalsurveywascarriedoutin40ruralEthiopiancommunitiestoevaluatetheProgramme.Householdswererandomlyselectedandallchildrenwereinvitedforeyeexaminationforactivetrachoma.In2005,eyeswabsweretakenforPolymeraseChainReaction(PCR)detectionofocularC.trachomatisDNA.Adultknowledgeandbehaviorrelatedtotrachomawereassessed.RESULTS:Communitysummarizedmeanprevalence,overall,was35.6%(SD=17.6)foractivetrachoma,34.0%(18.7)fortrachomatousinflammation,follicular(TF)aloneand4.3%(5.3)forPCRpositivityforC.trachomatis.Afteradjustment,oddsofactivetrachomawerereducedincommunitiesreceivingantibioticsandoneortwoeducationalinterventioncomponents(OR=0.35,95%CI:0.13–0.89orOR=0.31,0.11–0.89,respectively).TheoddsofbeingPCRpositivewerelowerintheseinterventionarms,comparedwithcontrol(OR=0.20,0.06–0.62andOR=0.07,0.02–0.30,respectively).Knowledgeoftreatmentandpreventativemethodswerereportedwithmuchhigherfrequency,comparedwithbaseline.CONCLUSIONS:TrachomaremainsapublichealthprobleminEthiopia.Antibioticadministrationremainsthemosteffectiveinterventionbutcommunity-basedhealtheducationprogrammescanimpact,toadditionallyreduceprevalenceofC.trachomatis.
Curtis,V.etal.(2001).EvidenceofbehaviorchangefollowingahygienepromotionProgrammeinBurkinaFaso.BulletinoftheWorldHealthOrganization,79(6):518–527.
DarmstadtG.L,BhuttaZ.A.,CousensS.,AdamT.,WalkerN.,deBernisL.(2005).Evidence-based,cost-effectiveinterventions:howmanynewbornbabiescanwesave?Lancet2005;365:977–88.
Dewey,K.G.andK.Begum(2011)."Long-termconsequencesofstuntinginearlylife."Maternal&ChildNutrition7(s3):5-18.
*Donegan,S.,etal.(2010)."Twofood-assistedmaternalandchildhealthnutritionprogrammeshelpedmitigatetheimpactofeconomichardshiponchildstuntinginHaiti."TheJournalofNutrition140(6):1139-1145.
Rigorousevaluationsoffood-assistedmaternalandchildhealthandnutritionprogrammesarestymiedbytheethicsofrandomizingrecipientstoacontroltreatment.Usingnonexperimentalmatchingmethods,weevaluatedtheeffectof2
116
suchprogrammesonchildlineargrowthinHaiti.The2well-implementedprogrammesofferedthesameservices(foodassistance,behaviorchangecommunication,andpreventivehealthservices)topregnantandlactatingwomenandyoungchildren.Theydifferedinthatone(thepreventiveprogramme)usedblankettargetingofallchildren6–23months,whereastheother(therecuperativeprogramme)targetedunderweight(weight-for-ageZscore<−2)children6–59months,astraditionallydone.Weestimatedprogrammeeffectsonheight-for-ageZscores(HAZ)andstunting(HAZ<−2)bycomparingoutcomesofchildreninprogrammeareaswithmatchedchildrenfromcomparablepopulationsintheHaitiDemographicandHealthSurvey.Children12–41mointhepreventiveandrecuperativeprogrammeareashadlowerprevalenceofstuntingthanthoseinthematchedcontrolgroup[16percentagepoints(pp)lowerinpreventiveand11ppinrecuperative].Childreninthe2programmeareasalsoweremorelikelythanthoseinthematchedcontrolgrouptobebreast-fedupto24months(25pphigherinpreventive,22inrecuperative)andchildren12monthsandolderweremorelikelytohavereceivedtherecommendedfullscheduleofvaccinations(32pphigherinpreventive,31inrecuperative).Bothprogrammesimprovedtargetedbehaviorsandprotectedchildgrowthinatimeofdeterioratingeconomiccircumstances.
Dubowitz,T.,etal.(2007)."IntensifyingeffortstoreducechildmalnutritioninIndia:AnevaluationoftheDularprogrammeinJharkhand,India."FoodNutrtionBulletin28(3):266-273.
Duncan,G.J.,etal.(2011)."Doesmoneyreallymatter?Estimatingimpactsoffamilyincomeonyoungchildren'sachievementwithdatafromrandom-assignmentexperiments."DevelopmentalPsychology47(5):1263.
*Durlak,J.A.,etal.(2011)."Theimpactofenhancingstudents'socialandemotionallearning:Ameta-analysisofschool-baseduniversalinterventions."ChildDevelopment82(1):405-432.
Thisarticlepresentsfindingsfromameta-analysisof213school-based,universalsocialandemotionallearning(SEL)programmesinvolving270,034kindergartenthroughhighschoolstudents.Comparedtocontrols,SELparticipantsdemonstratedsignificantlyimprovedsocialandemotionalskills,attitudes,behavior,andacademicperformancethatreflectedan11-percentile-pointgaininachievement.SchoolteachingstaffsuccessfullyconductedSELprogrammes.Theuseof4recommendedpracticesfordevelopingskillsandthepresenceofimplementationproblemsmoderatedprogrammeoutcomes.ThefindingsaddtothegrowingempiricalevidenceregardingthepositiveimpactofSELprogrammes.Policymakers,educators,andthepubliccancontributetohealthydevelopmentof
117
childrenbysupportingtheincorporationofevidence-basedSELprogrammingintostandardeducationalpractice.[ABSTRACTFROMAUTHOR]
CopyrightofChildDevelopmentisthepropertyofWiley-Blackwellanditscontentmaynotbecopiedoremailedtomultiplesitesorpostedtoalistservwithoutthecopyrightholder'sexpresswrittenpermission.However,usersmayprint,download,oremailarticlesforindividualuse.Thisabstractmaybeabridged.Nowarrantyisgivenabouttheaccuracyofthecopy.Usersshouldrefertotheoriginalpublishedversionofthematerialforthefullabstract.(CopyrightappliestoallAbstracts.)
Edwards,T.,etal.(2008)."RiskfactorsforactivetrachomaandChlamydiatrachomatisinfectioninruralEthiopiaaftermasstreatmentwithazithromycin."TropicalMedicine&InternationalHealth13(4):556-565.
Eickmann,S.H.,etal.(2003)."Improvedcognitiveandmotordevelopmentinacommunity-basedinterventionofpsychosocialstimulationinnortheastBrazil."DevelopmentalMedicine&ChildNeurology45(8):536-541.
Engle,P.L.andL.Lhotska(1999)."Theroleofcareinprogrammaticactionsfornutrition:DesigningProgrammesinvolvingcare."FOODANDNUTRITIONBULLETIN-UNITEDNATIONSUNIVERSITY-20(1):121-135.
Engle,P.L.,Black,M.M.,Behrman,J.R.,CabraldeMello,M.,Gertler,P.J.,Kapiri,L.,Martorell,R.,&Young,M.E,andtheInternationalChildDevelopmentSteeringGroup.(2007)Strategiestoavoidthelossofdevelopmentalpotentialinmorethan200millionchildreninthedevelopingworld.Lancet,369,229-242.
Engle,P.L,Fernald,L.C.H.,Alderman,H.,Behrman,J.,O’Gara,C.,Yousafzai,A.,CabraldeMello,M.,Hidrobo,M.,Ulkuer,N.,Ertem,I.,Iltus,S.,andtheGlobalDevelopmentSteeringgroup(2011).Strategiesforreducinginequalitiesandimprovingdevelopmentaloutcomesforyoungchildreninlow-incomeandmiddle-incomecountries.TheLancet,37,1339-1353.
*Ertem,I.O.,etal.(2006)."Promotingchilddevelopmentatsick-childvisits:Acontrolledtrial."Pediatrics118(1):e124-e131.
OBJECTIVE.Indevelopingcountries,thehealthcaresystemoftenistheonlyexistinginfrastructurethatcanreachyoungchildren,andhealthcareencountersmaybetheonlyopportunityforprofessionalstohaveapositiveinfluenceonchilddevelopment.ToaddressthediscrepancybetweenWesternanddevelopingcountriesrelatedtotheinformationthatisavailableforcaregiversonhowtosupporttheirchild'sdevelopment,theWorldHealthOrganizationDepartmentofChildandAdolescentHealthandDevelopmentandUnitedNationsInternational
118
Children'sEducationFundhavedevelopedtheCareforDevelopmentIntervention.
118
TheCareforDevelopmentInterventionaimsduringacutehealthvisitstoenhancecaregivers'playandcommunicationwiththeirchildren.Forfacilitationofitsdeliveryworldwide,theCareforDevelopmentInterventionwasdevelopedasanadditionalmoduleoftheIntegratedManagementofChildhoodIllnesstrainingcourse.ThepurposeofthisstudywastodeterminetheefficacyandthesafetyoftheCareforDevelopmentInterventionwhenimplementedduringayoungchild'svisitforacuteminorillness.METHODS.Thestudydesignisasequentiallyconductedcontrolledtrial,withthecomparisonarmcompletedfirst,CareforDevelopmentInterventiontrainingprovidedforthecliniciansnext,followedbytheinterventionarm.AtthePediatricDepartmentofAnkaraUniversitySchoolofMedicine,2pediatricianswhowereblindedtothestudyaimsandhypothesesbeforeCareforDevelopmentInterventiontrainingprovidedstandardhealthcaretothecomparisongroup;theythenreceivedCareforDevelopmentInterventiontrainingandprovidedstandardhealthcareplustheCareforDevelopmentInterventiontotheinterventiongroup.Compliancewithtreatmentandtheoutcomeofillnessweredeterminedbyafollow-upexaminationintheclinic1weeklater.Onemonthaftertheclinicvisits,anadaptedHomeObservationforMeasurementoftheEnvironmentwasadministeredinthehomesbyresearcherswhowereblindedtostudyaimsandhypotheses.RESULTS.Childrenwhowereaged≤24monthsandattendedtheclinicwithminorornoillnesseswererecruitedforthestudy:113inthecomparisongroupand120intheinterventiongroup.Atthe1-monthhomevisit,significantlymorefamilieshadoptimalHomeObservationforMeasurementoftheEnvironmentscores(17.5%vs6.2%),morehomemadetoyswereobserved(42.5%vs10.6%),andmorecaregiversreportedreadingtotheirchildren(20.0%vs3.5%)intheinterventionthaninthecomparisongroup.ThreeindependentpredictorsofoptimalHomeObservationforMeasurementoftheEnvironmentscoreemergedfromthelogisticregressionanalysis:beingintheinterventiongroup,childages>6months,andmaternaleducationgreaterthansecondaryschool.Compliancewithmedicaltreatmentandillnessoutcomeswerenotsignificantlydifferentbetweenthe2groups.CONCLUSIONS.TheCareforDevelopmentInterventionisaneffectivemethodofsupportingcaregivers'effortstoprovideamorestimulatingenvironmentfortheirchildrenandcanbeusedbyhealthcareprofessionalsduringvisitsforacuteminorillness.
Eshel,N.,etal.(2006).“Responsiveparenting:interventionsandoutcomes.”BulletinoftheWorldHealthOrganization,84(12):991-998.
Eyberg,S.M.,etal.(2008)."Evidence-basedpsychosocialtreatmentsforchildrenandadolescentswithdisruptivebehavior."JournalofClinicalChild&AdolescentPsychology37(1):215-237.

119
Farahat,T.M.,etal.(2009)."Evaluationofaneducationalinterventionforfarmingfamiliestoprotecttheirchildrenfrompesticideexposure."EasternMediterraneanHealthJournal15(1):47-56.
Faber,M.,Venter,S.L.,&Benadé,A.J.S.(2002).IncreasedvitaminAintakeinchildrenaged2-5yearsthroughtargetedhome-gardensinaruralSouthAfricancommunity.PublicHealthNutrition,5(1),11-16.
Feldens,C.A.,etal.(2010)."Long-termeffectivenessofanutritionalprogrammeinreducingearlychildhoodcaries:arandomizedtrial."CommunityDentistryandOralEpidemiology38(4):324-332.
FelittiVJ,AndaRF.TheRelationshipofAdverseChildhoodExperiencestoAdultHealth,Well-being,SocialFunction,andHealthcare. ChapterinLaniusR,VermettenE.TheHiddenEpidemic:TheImpactofEarlyLifeTraumaonHealthandDisease. CambridgeUniversityPress.2008.
Fernald,L.C.H.,etal.(2008)."RoleofcashinconditionalcashtransferProgrammesforchildhealth,growth,anddevelopment:ananalysisofMexico'sOportunidades."Lancet371(9615):828-837.
Fernald,L.C.H.,etal.(2009)."10-yeareffectofOportunidades,Mexico'sconditionalcashtransferProgramme,onchildgrowth,cognition,language,andbehavior:Alongitudinalfollow-upstudy."TheLancet374(9706):1997-2005.
Forry,N.D.,etal.(2011).Family-providerrelationships:Amultidisciplinaryreviewofhighqualitypracticesandassociationswithfamily,child,andprovideroutcomes.IssueBriefOPRE2011-26a.Washington,DC,OfficeofPlanning,ResearchandEvaluation,AdministrationforChildrenandFamilies,U.S.DepartmentofHealthandHumanServices.
*Gaboulaud,V.,etal.(2007)."CouldNutritionalRehabilitationatHomeComplementorReplaceCentre-BasedTherapeuticFeedingProgrammesforSevereMalnutrition?"JournalofTropicalPediatrics53(1):49-51.
TomeasurethesuccessrateofthreedifferentstrategiesusedinMédecinsSansFrontièreslarge-scaletherapeuticnutritionalrehabilitationProgrammeinNiger,weanalysedthreecohortsofseverelymalnourishedpatientsintermsofdailyweightgain,lengthofstay,recovery,casefatalityanddefaulting.Atotalof1937childrenaged6–59monthswerefollowedprospectivelyfrom15August2002to21October2003.Forthethreecohorts,660childrenweremaintainedinthetherapeutic
120
feedingcentre(TFC)duringtheentiretreatment,937childrenwereinitiallytreatedattheTFCandcompletedtreatmentathomeand340childrenwereexclusivelytreatedathome.Forallcohorts,averagetimeintheProgrammeandaverageweightgainmettheinternationalstandards(30–40days,>8 g/kg/day).Defaultrateswere28.1,16.8and5.6%forTFConly,TFCplushome-basedandhome-basedalonestrategies,respectively.TheoverallcasefatalityratefortheentireProgrammewas6.8%.Casefatalityrateswere18.9%forTFConlyand1.7%forhome-basedalone.Nodeathswererecordedinchildrentransferredtorehabilitationathome.Thisstudysuggeststhatsatisfactoryresultsforthetreatmentofseveremalnutritioncanbeachievedusingacombinationofhomeandhospital-basedstrategies.
Gardner,J.M.,etal.(2003)."Arandomizedcontrolledtrialofahome-visitinginterventiononcognitionandbehaviorintermlowbirthweightinfants."TheJournalofPediatrics143(5):634-639.
*Gardner,J.M.M.,etal.(2005)."Zincsupplementationandpsychosocialstimulation:effectsonthedevelopmentofundernourishedJamaicanchildren."TheAmericanJournalofClinicalNutrition82(2):399-405.
BACKGROUND:Undernourishedchildrenhavepoorlevelsofdevelopmentthatbenefitfromstimulation.Zincdeficiencyisprevalentinundernourishedchildrenandmaycontributetotheirpoordevelopment.Objective:Weassessedtheeffectsofzincsupplementationandpsychosocialstimulationgiventogetherorseparatelyonthepsychomotordevelopmentofundernourishedchildren.DESIGN:Thiswasarandomizedcontrolledtrialwith4groups:stimulationalone,zincsupplementationalone,bothinterventions,andcontrol(routinecareonly).Subjectswere114childrenaged9–30monthsandbelow–1.5zscoresoftheNationalCenterforHealthStatisticsweight-for-agereferenceswhowererecruitedfrom18healthclinics.Clinicswererandomlyassignedtoreceivestimulationornot;individualchildrenwererandomlyassignedtoreceivezincorplacebo.Thestimulationprogrammecomprisedweeklyhomevisitsduringwhichplaywasdemonstratedandmaternal-childinteractionswereencouraged.Thesupplementationwas10mgZnassulfatedailyorplacebo.Development(assessedbyuseoftheGriffithsMentalDevelopmentScales),length,andweightweremeasuredatbaselineand6molater.Weeklymorbidityhistoriesweretaken.RESULTS:Significantinteractionswerefoundbetweenzincsupplementationandstimulation.Zincbenefitedthedevelopmentalquotientonlyinchildrenwhoreceivedstimulation,andbenefitsfromzinctohandandeyecoordinationweregreaterinstimulatedchildren.Zincsupplementationaloneimprovedhandandeyecoordination,andstimulationalonebenefitedthedevelopmentalquotient,hearingandspeech,andperformance.Zincsupplementationalsoreduceddiarrhealmorbiditybutdidnotsignificantlyimprove
121
growth.CONCLUSION:Zincsupplementationbenefitsdevelopmentinundernourishedchildren,andthebenefitsareenhancedifstimulationisalsoprovided.
Gartner,A.,etal.(2007)."HasthefirstimplementationphaseoftheCommunityNutritionProjectinurbanSenegalhadanimpact?"Nutrition23(3):219-228.
Ghate,D.,Hazel,N.(2002).Parentinginpoorenvironments:Stress,supportandcoping.London:JessicaKingsleyPublications.
Ghoneim,E.,etal.(2004)."AninterventionProgrammeforimprovingthenutritionalstatusofchildrenaged2-5yearsinAlexandria."EastMediterrHealthJ10(6):828-843.
Guerrant,R.L.,etal.(2002)."Magnitudeandimpactofdiarrhealdiseases."ArchivesofMedicalResearch33(4):351-355.
Guyon,A.B.,Quinn,V.J.,Hainsworth,M.,Ravonimanantsoa,P.,Ravelojoana,V.,
Rambeloson,Z.,&Martin,L.(2009).Implementinganintegratednutritionpackageatlargescalein
Madagascar:theEssentialNutritionActionsframework.Food&NutritionBulletin,30(3),233-244.
*Hamadani,J.D.,HudaS.N.,Khatun,F.&Grantham-McGregorS.M.(2006)."PsychosocialstimulationimprovesthedevelopmentofundernourishedchildreninruralBangladesh."TheJournalofNutrition136(10):2645-2652.
Undernutritioninearlychildhoodisassociatedwithpoormentaldevelopmentandaffects45%ofchildreninBangladesh.Althoughlimitedevidenceshowsthatpsychosocialstimulationcanreducethedeficits,nosuchinterventionshavebeenreportedfromBangladesh.TheBangladeshIntegratedNutritionProgramme(BINP)hasprovidednutritionsupplementationtoundernourishedchildrenthroughcommunitynutritioncenters(CNCs).Weaddedpsychosocialstimulationtothetreatmentofundernourishedchildreninarandomizedcontrolledtrialtoassesstheeffectsonchildren'sdevelopmentandgrowthandmothers'knowledge.TwentyCNCswererandomlyassignedtointerventionorcontrolgroupswith107childrenineachgroup.Wealsostudied107nonintervenedbetter-nourishedchildrenfromthesamevillages.Pre-andpostinterventionmeasurementsincludedchildren'sheight,weight,developmentassessedonBayleyScales,behaviorratingsduringthetest,andaquestionnaireonmothers'knowledgeofchildrearing.Theinterventioncomprisedhomevisitsandgroupmeetingswithmothersandchildrenfor12mo.Interventionbenefitedchildren'smentaldevelopment(4.6±2.0,P=0.02),vocalization(0.48±0.23,P=0.04),cooperation(0.45±0.16,P=0.005),response-

122
to-examiner(0.50±0.15,P=0.001),emotionaltone(0.33±0.15,P=0.03),andmothers'knowledge(3.5±0.49,P<0.001).Attheend,undernourishedcontrolshad
122
poorermental(–4.6±2.0,P=0.02)andmotor(–6.6±2.2,P=0.003)development,weremoreinhibited(–0.35±0.16,P=0.03),fussier(–0.57±0.16,P<0.001),lesscooperative(–0.48±0.17,P=0.005),andlessvocal(–0.76±0.23,P=0.001)thanbetter-nourishedchildren.Intervenedchildrenscoredloweronlyinmotordevelopment(–4.4±2.3,P=0.049).Neithergroupofundernourishedchildrenimprovedinnutritionalstatus,indicatingthattreatmenthadnoeffect.Inconclusion,addingchilddevelopmentactivitiestotheBINPimprovedchildren'sdevelopmentandbehaviorandtheirmothers'knowledge;however,thelackofimprovementingrowthneedstobeexaminedfurther.
Hodgkin,R.andP.Newell(2007).“ImplementationhandbookfortheConventionontheRightsofaChild.”Geneva,Switzerland:UnitedNationsChildren’sFund.
HollowayK.A.,KarkeeS.B,,TamangA,, GurungY.B,,KafleK.K.,PradhanR,&ReevesB.C.(2009)CommunityinterventiontopromoterationaltreatmentofacuterespiratoryinfectioninruralNepal.TropicalMedicineandInternationalHealth,14:101–110
Hossain,S.M.M.,Duffield,A.,&Taylor,A.(2005).AnevaluationoftheimpactofaUS$60millionnutritionProgrammeinBangladesh.HealthPolicyandPlanning,20(1),35-40.doi:10.1093/heapol/czi004
Hotz,C.,&Gibson,R.S.(2004).Participatorynutritioneducationandadoptionofnew
feedingpracticesareassociatedwithimprovedadequacyofcomplementarydietsamongruralMalawianchildren:apilotstudy.Europeanjournalofclinicalnutrition,59(2),226-237.
Imdad,A.,etal.(2011)."Effectofbreastfeedingpromotioninterventionsonbreastfeedingrates,withspecialfocusondevelopingcountries."BMCPublicHealth11(Suppl3):S24.
Issler,R.M.S.,etal.(2009)."Infantsleepposition:ArandomizedclinicaltrialofaneducationalinterventioninthematernitywardinPortoAlegre,Brazil."Birth36(2):115-121.
Jaded,A.R.etal,(1996).“Assessingthequalityofreportsofrandomizedclinicaltrials:Isblindingnecessary?.ControlledClinicalTrials.17(1):1-12.
Janssens,W.,etal.(2009).Theimpactofahome-visitngearlychildhoodinterventionintheCaribbeanoncognitiveandsocioemotionalchilddevelopment.Amsterdam,AmsterdamInstituteforInternationalDevelopment.
*Jin,X.,etal.(2007).""CareforDevelopment"interventioninruralChina:Aprospectivefollow-upstudy."JournalofDevelopmental&BehavioralPediatrics28(3):213-218

123
210.1097/dbp.1090b1013e31802d31410b.
123
OBJECTIVE:TheaimofthisstudywastotesttheefficacyandappropriatenessoftheWorldHealthOrganization'sCareforDevelopment(CFD)counselingmaterials,whichformpartoftheIntegratedManagementofChildhoodIllness(IMCI)strategy.TheCFDmaterialsarebasedontheMother'sCard,whichcontainedage-specificmessagesonhowcaregiverscanbetterplayandcommunicatewithachild.METHOD:Weenrolled100familieswithachildofyoungerthan2yearsofagefromsevenrandomlyselectedvillagesinanimpoverishedruralcountyinAnhuiProvince,China.Twocounselingsessions,usingtheCFDMother'sCard,wereprovidedto50familiesrandomlyselectedfromamongthestudyparticipants.AllchildrenwereassessedwithGesellDevelopmentalSchedulesbeforecounselingandafter6months.Aquestionnaireonfamilysituationandknowledge,attitudes,andpracticesregardingchilddevelopmentwasalsoadministeredatthestartandconclusionofthestudy.RESULTS:Atbaselineassessment,bothcontrolandinterventiongroupswereequal,withaveragedevelopmentalscoreslessthanthenationalnorms.Childreninfamilieswhoreceivedcounselinghadsignificantlyhigherdevelopmentquotientscoresincognitive,social,andlinguisticdomains.Questionnairedataonchildrearingsuggestedthatresponsiveandrichinteractionsandconsistentcaregiverscorrelatedwithhigherscores.TheCFDMother'sCardwasfoundtobefeasibleandhelpfulinthosefamilieswhoreceivedcounseling.CONCLUSION:ThereisurgentneedforfurtherworkonpromotionofchilddevelopmentinruralChina.TheWorldHealthOrganization'sCFDapproachandMother'sCardisfeasibleandeffectiveandshouldbeexpandedinuse,especiallywithinthenationalIMCIprogramme.(C)2007LippincottWilliams&Wilkins,Inc.
Kagan,S.L.,etal.(1995).Reconsideringchildren’searlydevelopmentandlearning:Towardscommonviewsandvocabulary.Washington,DC,NationalEducationalGoalsPanel.
Kagitcibasi,C.,Sunar,D.,&Bekman,S.(2001)."Long-termeffectsofearlyintervention:Turkishlow-incomemothersandchildren."JournalofAppliedDevelopmentalPsychology22(4):333-361.
Kagitçibasi,C.,Sunar,D.,Bekman,S.,Baydar,N.,&Cemalcilar,Z.(2009)."Continuingeffectsofearlyenrichmentinadultlife:TheTurkishEarlyEnrichmentProject22yearslater."JournalofAppliedDevelopmentalPsychology30(6):764-779.
*Kalimbira,A.A.,etal.(2010)."Theimpactofanintegratedcommunity-basedmicronutrientandhealthProgrammeonstuntinginMalawianpreschoolchildren."PublicHealthNutrition13(05):720-729.
124
OBJECTIVE:Toassesstheimpactofthe1996–2005integratedcommunity-basedmicronutrientandhealth(MICAH)Programmeonlineargrowthretardation(stunting)inMalawianpreschoolchildrenlivinginruralareas.DesignProspectivestudyofthreelarge-scalecross-sectionalsurveysconductedin1996,2000and2004inMICAHandComparisonpopulations.SETTING:RuralareasinMalawi.SUBJECTS:Preschoolchildren(6·0–59·9months)fromrandomlyselectedhouseholds(474fromthe1996baselinesurvey;1264from2000MICAHareas;1500from2000Comparisonareas;1959from2004MICAHareas;and1008from2004Comparisonareas),whorespondedtoahouseholdquestionnaire,wereweighedandmeasuredusingstandardprotocols.RESULTS:Atthebaselinein1996,theprevalenceofstunting(60·2%)wasveryhigh.By2000,theprevalenceofstuntinghaddeclinedto50·6%and56·0%(χ2=7·8,P=0·005)inMICAHandComparisonareas,respectively.In2004,theprevalenceofstuntingdidnotdiffersignificantlybetweenMICAHandComparisonareas(43·0%v.45·1%;χ2=1·11,P=0·3).Severestuntingaffected34·7%ofchildrenatbaseline,whichdeclinedto15·8%and17·1%(χ2=0·86,P=0·4)inMICAHandComparisonareas,respectively,by2004.Regionalvariationsexisted,withproportionatelyfewerchildrenfromtheNorthernregionbeingstuntedcomparedtotheirCentralandSouthernregioncounterparts.CONCLUSION:Giventhelengthofimplementation,wide-scalecoverageandpositiveimpactonchildgrowthinPhaseI(1996–2000),theMICAHProgrammeisapotentialmodelforcombatinglineargrowthretardationinruralareasinMalawi,althoughthecatch-upimprovementinComparisonareasduringPhaseII(2000–2004)cannotbeadequatelyexplained.
*Kaminski,J.W.,etal.(2008)."Ameta-analyticreviewofcomponentsassociatedwithparenttrainingprogrammeeffectiveness."JournalofAbnormalChildPsychology:AnofficialpublicationoftheInternationalSocietyforResearchinChildandAdolescentPsychopathology36(4):567-589.
Thiscomponentanalysisusedmeta-analytictechniquestosynthesizetheresultsof77publishedevaluationsofparenttrainingprogrammes(i.e.,programmesthatincludedtheactiveacquisitionofparentingskills)toenhancebehaviorandadjustmentinchildrenaged0-7.Characteristicsofprogrammecontentanddeliverymethodwereusedtopredicteffectsizesonmeasuresofparentingbehaviorsandchildren'sexternalizingbehavior.Aftercontrollingfordifferencesattributabletoresearchdesign,programmecomponentsconsistentlyassociatedwithlargereffectsincludedincreasingpositiveparent-childinteractionsandemotionalcommunicationskills,teachingparentstousetimeoutandtheimportanceofparentingconsistency,andrequiringparentstopracticenewskillswiththeirchildrenduringparenttrainingsessions.Programmecomponentsconsistentlyassociatedwithsmallereffectsincludedteachingparentsproblemsolving;teachingparentstopromotechildren'scognitive,academic,orsocialskills;andprovidingother,additionalservices.Theresultshave
125
implicationsforselectionandstrengtheningofexistingparenttrainingprogrammes.(PsycINFODatabaseRecord(c)2010APA,allrightsreserved)(journalabstract)
*Kapil,U.(2002)."Integratedchilddevelopmentservices(ICDS)scheme:AprogrammeforholisticdevelopmentofchildreninIndia."IndianJournalofPediatrics69(7):597-601.
TheIntegratedChildDevelopmentServices(ICDS)schemeisthelargestprogrammeforpromotionofmaternalandchildhealthandnutritionnotonlyinIndiabutinthewholeworld.Theschemewaslaunchedin1975inpursuanceoftheNationalPolicyforChildren.Theschemehasexpandedinthelasttwenty-sevenyearsform33projectsto5171blocks.ICDSisamulti-sectoralprogrammeandinvolvesseveralgovernmentdepartments.Theprogrammeservicesarecoordinatedatthevillage,block,district,stateandcentralgovernmentlevels.TheprimaryresponsibilityfortheimplementationoftheprogrammelieswiththeDepartmentofWomen&ChildDevelopmentattheCentreandnodaldepartmentatthestates,whichmaybeSocialWelfare,RuralDevelopment,TribalWelfareorHealthDepartmentoranindependentDepartment.Thebeneficiariesarechildrenbelow6years,pregnantandlactatingwomenandwomenintheagegroupof15to44yrs.ThebeneficiariesofICDSaretoalargeextentidenticalwiththoseundertheMaternalandChildHealthProgramme.Theprogrammeprovidesanintegratedapproachforconvergingallthebasicservicesforimprovedchildcare,earlystimulationandlearning,healthandnutrition,waterandenvironmentalsanitationaimedattheyoungchildren,expectantandlactatingmothers,otherwomenandadolescentgirlsinacommunity.ICDSprogrammeisthereflectionoftheGovernmentofIndiatoeffectivelyimprovethenutritionandhealthstatusofunderprivilegedsectionofthepopulationthroughdirectinterventionmechanism.Theprogrammecovers27.6millionbeneficiarieswithsupplementarynutrition.Theprogrammeservicesandbeneficiarieshasessentiallyremainedthesamesince1975.Recentlyareviewoftheschemewasheld,sponsoredbyGovernmentofIndia,whichsuggestedmodificationsinthehealthandnutritioncomponentofICDSschemetoimprovetheprogrammeimplementationandefficiency
*Kendrick,D.,etal.(2007)."Parentinginterventionsforthepreventionofunintentionalinjuriesinchildhood."CochraneDatabaseofSystematicReviews(4).
BACKGROUNDParenteducationandtrainingProgrammescanimprovematernalpsychosocialhealth,childbehavioralproblemsandparentingpractices.Thisreviewassessestheeffectsofparentinginterventionsforreducingchildinjury.ObjectivesToassesstheeffectsofparentinginterventionsforpreventingunintentionalinjuryaswellasincreasingpossessionanduseofsafetyequipmentandparentalsafetypractices.SEARCHSTRATEGYWesearchedCENTRAL,MEDLINE,EMBASE,BiologicalAbstracts,PsychINFO,Sociofile,SocialScienceCitationIndex,CINAHL,
126
DissertationAbstracts,ERIC,DARE,ASSIA,WebofScience,SIGLEandZETOC.WealsohandsearchedabstractsfromtheWorldConferencesonInjuryPrevention&ControlandthejournalInjuryPrevention.ThesearcheswereconductedinMay2005.SelectioncriteriaWeincludedrandomisedcontrolledtrials(RCTs),non-randomisedcontrolledtrials(non-RCTs)andcontrolledbeforeandafterstudies(CBAs),whichevaluatedparentinginterventionsadministeredtoparentsofchildrenaged18yearsandunder,andreportedoutcomedataoninjuries(unintentionalorunspecifiedintent),andpossessionanduseofsafetyequipmentorsafetypractices.Parentinginterventionsweredefinedasthosewithaspecifiedprotocol,manualorcurriculumaimedatchangingknowledge,attitudesorskillscoveringarangeofparentingtopics.DATACOLLECTIONANDANALYSISStudieswereselected,datawereextractedandqualityappraisedindependentlybytwoauthors.Pooledrelativerisks(RR)wereestimatedusingrandomeffectmodels.MainresultsFifteenstudieswereincludedinthereview:11RCTs(oneincludedaCBAwithinthesamestudy),onenon-RCT,onestudycontainedbothrandomisedandnon-randomisedarmsandtwoCBAs.Twoprovidedsolelyeducationalinterventions.Thirteenprovidedinterventionscomprisingparentingeducationandothersupportservices;11ofwhichwerehomevisitingProgrammesandtwoofwhichwerepaediatricpractice-basedinterventions.Thirteenstudiesrecruitedfamiliesatriskofadversechildhealthoutcomes.NineRCTswereincludedintheprimarymeta-analysis,whichindicatedthatinterventionfamilieshadasignificantlylowerriskofinjury(RR0.82,95%CI0.71to0.95).Severalstudiesfoundfewerhomehazards,ahomeenvironmentmoreconducivetochildsafety,oragreaternumberofsafetypracticesininterventionfamilies.AUTHORS'CONCLUSIONSParentinginterventions,mostcommonlyprovidedwithinthehomeusingmulti-facetedinterventionsmaybeeffectiveinreducingchildinjury.Theevidencerelatesmainlytointerventionsprovidedtofamiliesatriskofadversechildhealthoutcomes.Furtherresearchisrequiredtoexploremechanismsbywhichtheseinterventionsreduceinjury,thefeaturesofparentinginterventionsthatarenecessaryorsufficienttoreduceinjuryandthegeneralisabilitytodifferentpopulationgroups.
Kilaru,A.,etal.(2005)."Community-basednutritioneducationforimprovinginfantgrowthinruralKarnataka."Indianpediatrics42(5):425.
Knitzer,J.,etal.(2008).Reducingmaternaldepressionanditsimpactonyoungchildren:Towardaresponsiveearlychildhoodpolicyframework.NewYorkCity,NationalCenterforChildreninPoverty,MailmanSchoolofPublicHealth,ColumbiaUniversity.
Koçak,A.(2004).EvaluationreportoftheFatherSupportProgramme.Turkey,MotherChildEducationFoundation.
127
*Kramer,M.S.,etal.(2008)."Breastfeedingandchildcognitivedevelopment:newevidencefromalargerandomizedtrial."ArchivesofGeneralPsychiatry65(5):578-584.
CONTEXT The evidence that breastfeeding improves cognitive development isbasedalmostentirelyonobservationalstudiesandisthuspronetoconfoundingbysubtle behavioral differences in the breastfeeding mother's behavior or herinteractionwiththeinfant.OBJECTIVEToassesswhetherprolongedandexclusivebreastfeedingimproveschildren'scognitiveabilityatage6.5years.DesignCluster-randomized trial,withenrollmentfromJune17, 1996, toDecember31, 1997,andfollow-upfromDecember21,2002,toApril27,2005.SettingThirty-oneBelarussianmaternity hospitals and their affiliated polyclinics. Participants A total of 17 046healthybreastfeedinginfantswereenrolled,ofwhom13889(81.5%)werefollowedupatage6.5years.InterventionBreastfeedingpromotioninterventionmodeledontheBaby-FriendlyHospitalInitiativebytheWorldHealthOrganizationandUNICEF.MainOutcomeMeasuresSubtestandIQscoresontheWechslerAbbreviatedScalesofIntelligence,andteacherevaluationsofacademicperformanceinreading,writing,mathematics,andothersubjects.RESULTSTheexperimentalinterventionledtoalargeincreaseinexclusivebreastfeedingatage3months(43.3%fortheexperimentalgroupvs6.4%forthecontrolgroup;P<.001)andasignificantlyhigherprevalenceofanybreastfeedingatallagesuptoandincluding12months.TheexperimentalgrouphadhighermeansonalloftheWechslerAbbreviatedScalesofIntelligencemeasures,withcluster-adjustedmeandifferences(95%confidenceintervals)of+7.5(+0.8to+14.3)forverbalIQ,+2.9(-3.3to+9.1)forperformanceIQ,and+5.9(-1.0to+12.8)forfull-scaleIQ.Teachers'academicratingsweresignificantlyhigherintheexperimentalgroupforbothreadingandwriting.CONCLUSIONTheseresults,basedonthelargestrandomizedtrialeverconductedintheareaofhumanlactation,providestrongevidencethatprolongedandexclusivebreastfeedingimproveschildren'scognitivedevelopment.TrialRegistrationisrctn.orgIdentifier:ISRCTN37687716
*Kramer,M.S.,etal.(2008)."Effectsofprolongedandexclusivebreastfeedingonchildbehaviorandmaternaladjustment:Evidencefromalarge,randomizedtrial."Pediatrics121(3):e435-e440.
OBJECTIVE.Theobjectiveofthisstudywastoassessthelong-termeffectsofbreastfeedingonchildbehaviorandmaternaladjustment.METHODS.WefollowedupchildrenwhowereinthePromotionofBreastfeedingInterventionTrial,acluster-randomizedtrialofabreastfeedingpromotioninterventionbasedontheWorldHealthOrganization/UnitedNationsChildren'sFundBaby-FriendlyHospitalInitiative.Atotalof17046healthy,breastfeedingmother–infantpairswereenrolledfrom31Belarussianmaternityhospitalsandaffiliatedpolyclinics;13889(81.5%)

128
werefollowedupat6.5years.MothersandteacherscompletedtheStrengthsandDifficultiesQuestionnaireandsupplementalquestionsbearingoninternalizingandexternalizingbehavioralproblems.Mothersalsorespondedtoquestionsconcerningtheirrelationshipstotheirpartnerandchildandtheirbreastfeedingofsubsequentlybornchildren.RESULTS.Theexperimentalinterventionledtoalargeincreaseinexclusivebreastfeedingat3months(43.3%vs6.4%)andasignificantlyhigherprevalenceofanybreastfeedingatallagesuptoandincluding12months.NosignificanttreatmenteffectswereobservedoneitherthemotherortheteacherStrengthsandDifficultiesQuestionnaireratingsoftotaldifficulties,emotionalsymptoms,conductproblems,hyperactivity,peerproblems,orprosocialbehaviororonthesupplementalbehavioralquestions.Wefoundnoevidenceoftreatmenteffectsontheparent'smarriageoronthemother'ssatisfactionwithherrelationshipswithherpartnerorchild,buttheexperimentalinterventionsignificantlyincreasedthedurationofanybreastfeeding,andmothersintheexperimentalgroupwerenearlytwiceaslikelytobreastfeedexclusivelythenext-bornchildforatleast3months.CONCLUSIONS.Onthebasisofthelargestrandomizedtrialeverconductedintheareaofhumanlactation,wefoundnoevidenceofrisksorbenefitsofprolongedandexclusivebreastfeedingforchildandmaternalbehavior.Breastfeedingpromotiondoes,however,favorablyaffectbreastfeedingofthesubsequentchild.
Kumar,V.,Mohanty,S.,Kumar,A.,Misra,R.P.,Santosham,M.,Awasthi,S.,...&Darmstadt,G.L.(2008).Effectofcommunity-basedbehaviorchangemanagementonneonatalmortalityinShivgarh,UttarPradesh,India:acluster-randomisedcontrolledtrial.TheLancet,372(9644),
1151-1162.Lamberti,L.M.,etal.(2011)."Breastfeedingandtheriskfordiarrheamorbidityandmortality."BMCPublicHealth11(Suppl3):S15.
Lansford,J.E.andK.Deater-Deckard(2012)."Childrearingdisciplineandviolenceindevelopingcountries."ChildDevelopment83(1):62-75.
Lansford,J.E.,&Bornstein,M.H.(2007).Reviewofparentingprogrammesindevelopingcountries.NewYork:UNICEF.
leRoux,I.,etal.(2010)."HomevisitsbyneighborhoodMentorMothersprovidetimelyrecoveryfromchildhoodmalnutritioninSouthAfrica:resultsfromarandomizedcontrolledtrial."NutritionJournal9(1):1-10.
129
Levy,S.(2006).Progressagainstpoverty:SustainingMexico'sProgresa-Oportunidadesprogramme.Washington,DC,BrookingsInstitutePress.
Lindert,K.(2005).ReducingpovertyandinequalityinLatinAmerica:Thepromiseofconditionalcashtransfers.Washington,DC,TheWorldBank.
Lozoff,B.,Beard,J.,Connor,J.,Felt,B.,Georgieff,M.&Schallert,T.(2006)."Long-lastingneuralandbehavioraleffectsofirondeficiencyininfancy."NutritionReviews64:S34-S43.
*Luby,S.P.,etal.(2004)."Effectofintensivehandwashingpromotiononchildhooddiarrheainhigh-riskcommunitiesinpakistan:Arandomizedcontrolledtrial."JAMA:TheJournaloftheAmericanMedicalAssociation291(21):2547-2554.
CONTEXT Washinghandswithsoappreventsdiarrhea,butchildrenatthehighestriskofdeathfromdiarrheaareyoungerthan1year,tooyoungtowashtheirownhands.Previousstudieslackedsufficientpowertoassesstheimpactofhouseholdhandwashingondiarrheaininfants.OBJECTIVE Toevaluatetheeffectofpromotinghouseholdhandwashingwithsoapamongchildrenatthehighestriskofdeathfromdiarrhea.Design,Setting,andParticipantsAclusterrandomizedcontrolledtrialof36low-incomeneighborhoodsinurbansquattersettlementsinKarachi,Pakistan.FieldworkersvisitedparticipatinghouseholdsatleastweeklyfromApril15,2002,toApril5,2003.Eligiblehouseholdslocatedinthestudyareahadatleast2childrenyoungerthan15years,atleast1ofwhomwasyoungerthan5years.INTERVENTIONSWeeklyvisitsin25neighborhoodstopromotehandwashingwithsoapafterdefecationandbeforepreparingfood,eating,andfeedingachild.Withininterventionneighborhoods,300households(1523children)receivedaregularsupplyofantibacterialsoapand300households(1640children)receivedplainsoap.Elevenneighborhoods(306householdsand1528children)comprisedthecontrolgroup.MAINOUTCOMEMEASURE Incidencedensityofdiarrheaamongchildren,definedasthenumberofdiarrhealepisodesper100person-weeksofobservation.RESULTSChildrenyoungerthan15yearslivinginhouseholdsthatreceivedhandwashingpromotionandplainsoaphada53%lowerincidenceofdiarrhea(95%confidenceinterval[CI],–65%to–41%)comparedwithchildrenlivingincontrolneighborhoods.Infantslivinginhouseholdsthatreceivedhandwashingpromotionandplainsoaphad39%fewerdayswithdiarrhea(95%CI,–61%to–16%)vsinfantslivingincontrolneighborhoods.Severelymalnourishedchildren(weightforagezscore,<–3.0)youngerthan5yearslivinginhouseholdsthatreceivedhandwashingpromotionandplainsoaphad42%fewerdayswithdiarrhea(95%CI,–69%to–16%)vsseverelymalnourishedchildreninthecontrolgroup.Similarreductionsindiarrheawereobservedamongchildrenlivinginhouseholdsreceivingantibacterialsoap.CONCLUSION Inasettinginwhichdiarrheaisaleadingcauseof

130
childdeath,improvementinhandwashinginthehouseholdreducedtheincidence
ofdiarrheaamongchildrenathighriskofdeathfromdiarrhea.
Luby,S.P.,Kadir,M.A.,Sharker,Y.,Yeasmin,F.,Unicomb,L.,Islam,M.S.(2010.“ACommunityrandomizedcontrolledtrialpromotingwaterlesshandsanitizerandhandwashingwithsoap,Dhaka,Bangladesh”.TropicalMedicineandInternationalHealth.15(12):1508-1516
*Lundahl,B.,etal.(2006)."Ameta-analysisofparenttraining:Moderatorsandfollow-upeffects."ClinicalPsychologyReview26(1):86-104.
Ameta-analysisof63peer-reviewedstudiesevaluatedtheabilityofparenttrainingprogrammestomodifydisruptivechildbehaviorsandparentalbehaviorandperceptions.Thisanalysisextendspreviousworkbydirectlycomparingbehavioralandnonbehavioralprogrammes,evaluatingfollow-upeffects,isolatingdependentvariablesexpresslytargetedbyparenttraining,andexaminingmoderators.Effectsimmediatelyfollowingtreatmentforbehavioralandnonbehavioralprogrammesweresmalltomoderate.Fornonbehavioralprogrammes,insufficientstudiesprecludedexaminingfollow-upeffects.Forbehavioralprogrammes,follow-upeffectsweresmallinmagnitude.Parenttrainingwasleasteffectiveforeconomicallydisadvantagedfamilies;importantly,suchfamiliesbenefitedsignificantlymorefromindividuallydeliveredparenttrainingcomparedtogroupdelivery.Includingchildrenintheirowntherapy,separatefromparenttraining,didnotenhanceoutcomes.(PsycINFODatabaseRecord(c)2010APA,allrightsreserved)(journalabstract)
*Lundahl,B.W.,etal.(2008)."Ameta-analysisoffatherinvolvementinparenttraining."ResearchonSocialWorkPractice18(2):97-106.
OBJECTIVE:Investigate(a)whetherincludingfathersinparenttrainingenhancesoutcomesand(b)whethermothersandfathersbenefitequallyfromparenttraining.METHOD:Usingtraditionalmeta-analysismethodology,26studiesthatcouldanswertheresearchquestionswereidentifiedandmeta-analyzed.Results:Studiesthatincludedfathers,comparedwiththosethatdidnot,reportedsignificantlymorepositivechangesinchildren'sbehavioranddesirableparentingpractices,butnotinperceptionstowardparenting.Comparedwithmothers,fathersreportedfewerdesirablegainsfromparenttraining.CONCLUSIONS:Fathersshouldnotbeexcludedfromparenttrainingandshouldbeencouragedtoattend.Furtherresearchshouldseektounderstandhowparent-trainingprogrammesmightbettermeettheneedsoffathers.
131
Macours,K.,etal.(2008).Cashtransfers,behavioralchanges,andcognitivedevelopmentinearlychildhood.Evidencefromarandomizedexperiment.PolicyResearchWorking
Paper4759.Washington,DC,TheWorldBank.*Macours,K.,etal.(2012)."Cashtransfers,behavioralchanges,andcognitivedevelopmentinearlychildhood:Evidencefromarandomizedexperiment."AmericanEconomicJournal:AppliedEconomics4(2):247-273.
Cashtransferprogrammeshavebecomeextremelypopularinthedevelopingworld.Alargeliteratureanalyzestheireffectsonschooling,healthandnutrition,butrelativelylittleisknownaboutpossibleimpactsonchilddevelopment.Thispaperanalyzestheimpactofacashtransferprogrammeonearlychildhoodcognitivedevelopment.Childreninhouseholdsrandomlyassignedtoreceivebenefitshadsignificantlyhigherlevelsofdevelopmentninemonthsaftertheprogrammebegan.Thereisnofade-outofprogrammeeffectstwoyearsaftertheprogrammeended.Additionalrandomvariationshowsthattheseimpactsareunlikelytoresultfromthecashcomponentoftheprogrammealone.
Maluccio,J.A.andR.Flores(2004).Impactevaluationofaconditionalcashtransferprogramme:TheNicaraguanReddeProtecciónSocial.FCNDDiscussionPaperNo.184.Washington,DC,FoodConsumptionandNutritionDivision,InternationalFoodPolicyResearchInstitute.
*Manaseki-Holland,S.,etal.(2010)."Effectsoftraditionalswaddlingondevelopment:Arandomizedcontrolledtrial."Pediatrics126(6):e1485-e1492.
OBJECTIVE:Evidenceoftheeffectsoftight,prolongedbindingofinfantsondevelopmentisinconclusiveandbasedonsmallethnographicstudies.ThenullhypothesiswasthatMongolianinfantsnotswaddledorswaddledtightlyinatraditionalsetting(to>7monthsofage)donothavesignificantlydifferentscoresfortheBayleyScalesofInfantDevelopment,SecondEdition(BSID-II).PATIENTSANDMETHODS:Inarandomizedcontrolledtrial,1279healthynewbornsinUlaanbaatar,Mongolia,wereallocatedatbirthtotraditionalswaddlingornonswaddling.Thefamiliesreceived7monthsofhomevisitstocollectdataandmonitorcompliance.At11to17monthsofage,theBSID-IIwasadministeredto1100children.RESULTS:Nosignificantbetween-groupdifferenceswerefoundinmeanscaledmentalandpsychomotordevelopmentalscores.Theunadjustedmeandifferencebetweenthegroupswas−0.69(95%confidenceinterval[CI]:−2.59to1.19)forpsychomotorand−0.42(95%CI:−1.68to0.84)formentalscoresinfavoroftheswaddlinggroup.Asubgroupanalysisofthecompliantsampleproducedsimilarresults.BSID-II–scaledpsychomotorandmentalscoreswere99.98(95%CI:99.03–100.92)and105.52(95%CI:104.89–106.14),respectively.Backgroundcharacteristicswerebalancedacross
132
thegroups.CONCLUSIONS:IntheMongoliancontext,prolongedswaddlinginthefirstyearoflifedidnothaveanysignificantimpactonchildren'searlymentalor
psychomotordevelopment.Additionalstudiesinothersettingsneedtoconfirmthisfinding.TheMongolianinfantsinthistrialhadscaledBSID-IImentalandpsychomotorscorescomparabletoUnitedStatesnorms.
Marsh,D.R.andD.G.Schroeder(2002)."Thepositivedevianceapproachtoimprovehealthoutcomes:Experienceandevidencefromthefield."Food&NutritionBulletin23(4):3-6.
Mazia,G.,etal.(2009)."IntegratingqualitypostnatalcareintoPMTCTinSwaziland."GlobalPublicHealth4(3):253-270.
McCartney,K.,&Phillips,D.A.(Eds.)(2006).HandbookofEarlyChildhoodDevelopment.Oxford:BlackwellPublishing.
MeaneyM.(2010).Epigeneticsandthebiologicaldefinitionofgenexenvironmentinteractions.ChildDevelopment,81(1),41–79.
*Mikton,C.andA.Butchart(2009)."Childmaltreatmentprevention:Asystematicreviewofreviews."BulletinoftheWorldHealthOrganization87(5):353-361.
OBJECTIVE:Tosynthesizerecentevidencefromsystematicandcomprehensivereviewsontheeffectivenessofuniversalandselectivechildmaltreatmentpreventioninterventions,evaluatethemethodologicalqualityofthereviewsandoutcomeevaluationstudiestheyarebasedon,andmapthegeographicaldistributionoftheevidence.METHODS:Asystematicreviewofreviewswasconducted.Thequalityofthesystematicreviewswasevaluatedwithatoolfortheassessmentofmultiplesystematicreviews(AMSTAR),andthequalityoftheoutcomeevaluationswasassessedusingindicatorsofinternalvalidityandoftheconstructvalidityofoutcomemeasures.FINDINGS:Thereviewfocusedonsevenmaintypesofinterventions:homevisiting,parenteducation,childsexabuseprevention,abusiveheadtraumaprevention,multi-componentinterventions,media-basedinterventions,andsupportandmutualaidgroups.Fouroftheseven-home-visiting,parenteducation,abusiveheadtraumapreventionandmulti-componentinterventions-showpromiseinpreventingactualchildmaltreatment.Threeofthem-homevisiting,parenteducationandchildsexualabuseprevention-appeareffectiveinreducingriskfactorsforchildmaltreatment,althoughtheseconclusionsaretentativeduetothemethodologicalshortcomingsofthereviewsandoutcomeevaluationstudiestheydrawon.Ananalysisofthegeographicaldistributionoftheevidenceshowsthatoutcomeevaluationsofchildmaltreatmentpreventioninterventionsareexceedinglyrareinlow-andmiddle-incomecountries
133
andmakeuponly0.6%ofthetotalevidencebase.CONCLUSION:Evidenceforthe
effectivenessoffourofthesevenmaintypesofinterventionsforpreventingchildmaltreatmentispromising,althoughitisweakenedbymethodologicalproblemsandpaucityofoutcomeevaluationsfromlow-andmiddle-incomecountries.CopyrightCO2009WorldHealthOrganization
*Mock,C.,etal.(2003)."InjurypreventioncounsellingtoimprovesafetypracticesbyparentsinMexico."BulletinoftheWorldHealthOrganization81(8):591-598.
OBJECTIVES:ToevaluatetheeffectivenessofeducationalcounsellingProgrammesaimedatincreasingparents'practiceofchildhoodsafetyinMonterrey,Mexico,andtoprovideinformationaimedathelpingtoimprovetheeffectivenessoffutureeffortsinthisfield.METHODS:ThreedifferentcounsellingProgrammesweredesignedtomeettheneedsoftheupper,middleandlowersocioeconomicstrata.Evaluationinvolvedtheuseofbaselinequestionnairesonparents'existingsafety-relatedpracticesforinterventionandcontrolgroupsandtheadministrationofcorrespondingquestionnairesaftertheProgrammeshadbeencarriedout.FINDINGS:Datawereobtainedon1124childrenbeforecounsellingtookplaceandon625afterithadbeengiven.Overallsafetyscores(%saferesponses)increasedfrom54%and65%fortheloweranduppersocioeconomicstrata,respectively,beforecounsellingto62%and73%aftercounselling(P<0.001forallgroups).Improvementsoccurredbothforactivitiesthatrequiredcautionandforactivitiesthatrequiredtheuseofsafety-relateddevices(e.g.helmets,carseats).However,scoresfortheuseofsuchdevicesremainedsuboptimalevenaftercounsellingandtherewerewidediscrepanciesbetweenthesocioeconomicstrata.Thepost-counsellingscoresfortheuseofsafety-relateddeviceswere55%,38%and19%fortheupper,middleandlowersocioeconomicstrata,respectively.CONCLUSIONS:Briefeducationalinterventionstargetingparents'practiceofchildhoodsafetyimprovedsafebehaviors.Increasedattentionshouldbegiventospecificsafety-relateddevicesandtothesafetyofpedestrians.Educationaleffortsshouldbecombinedwithotherstrategiesforinjuryprevention,suchastheuseoflegislationandtheimprovementofenvironmentalconditions.Copyright©2003WorldHealthOrganization.
MohanP., Iyengar,S.D.,Martines,J,,Cousens,S,,Sen,K.(2004). Impactofcounsellingoncare-seekingbehaviorinfamilieswithsickchildren:clusterrandomizedtrialinruralIndia.BMJPublishingGroupLimited.329(7460):266.
Moran,P.,Ghate,D.,andvanderMerwe,A.(2004).WhatWorksinParentingSupport?AReviewoftheInternationalEvidence.ResearchReportRR57420014,PolicyResearchBureau.
134
Mohebbi,S.Z.,etal.(2009)."Aclusterrandomisedtrialofeffectivenessofeducationalinterventioninprimaryhealthcareonearlychildhoodcaries."CariesResearch43(2):110-118.329(7460):266.
Moran,P.,Ghate,D.,andvanderMerwe,A.(2004).Whatworksinparentingsupport?Aninternationalreviewofliterature.London,DepartmentforEducationandSkills.
Nair,M.,Renjit,M.,Siju,K.,Leena,M.,George,B.,&Kumar,G.S.(2009).Effectivenessofacommunityoralhealthawarenessprogramme.Indianpediatrics,46,s86.
Nana,C.,Brouwer,I.,Zagré,N.,Kok,F.,&Traoré,A.(2006).Impactofpromotionofmango
andliverassourcesofvitaminAforyoungchildren:apilotstudyinBurkinaFaso.PublicHealthNutrition,9(06),808-813.doi:doi:10.1079/PHN2005911
NationalScientificCouncilontheDevelopingChild(2004).YoungChildrenDevelopinanEnvironmentofRelationships:WorkingPaperNo.1.RetrievedJuly21,2014fromwww.developingchild.harvard.edu
NationalScientificCouncilontheDevelopingChild(2010).EarlyExperiencesCanAlterGeneExpressionandAffectLong-TermDevelopment:WorkingPaperNo.10.RetrievedJuly21,2014fromwww.developingchild.harvard.edu
Needleman,J.,(1991).“HandbookofEarlyChildhoodIntervention”.JournalofDevelopmental&BehavioralPediatrics,12(4):275-280.
Nixon,R.D.V.(2002)."Treatmentofbehaviorproblemsinpreschoolers:Areviewofparenttrainingprogrammes."ClinicalPsychologyReview22(4):525-546.
Ogilvie,D.,Fayter,D.,Petticrew,M.,Sowden,A.,Thomas,S.&Whitehead,M.(2008)."Theharvestplot:Amethodforsynthesisingevidenceaboutthedifferentialeffectsofinterventions."BMCmedicalresearchmethodology8(1):8.Okeke,T.A.,&Uzochukwu,B.SC.(2009).Improvingchildhoodmalariatreatmentandreferralpracticesbytrainingpatentmedicinevendorsinruralsouth-eastNigeria.MalariaJournal,8,260.
Ortiz-Andrellucchi,A.,etal.(2009)."Facingmalnutritionandpoverty:EvaluatingtheCONINexperience."NutritionReviews67:S47-S55.
135
Oveisi,S.,etal.(2010)."Primarypreventionofparent-childconflictandabuseinIranianmothers:Arandomized-controlledtrial."Childabuse&neglect34(3):206.
Özyazıcıoğlu,N.,etal.(2011)."Theeffectoftrainingprogrammesontraditionalapproachesthatmothersuseinemergencies."JournalofEmergencyNursing37(1):79-85.
Padak,N.andT.Rasinski(2003).“FamilyLiteracyProgrammes:WhoBenefits?”OhioLiteracyResourceCenter.KentStateUniversity.
Panter-Brick,C.,Burgess,A.,Eggerman,M.,McAllister,F.,Pruett,K.,&Leckman,J.F.(inpress).Recommendationsforagamechangeinparentinginterventionsbasedonasystematicreviewoftheglobalevidence.JournalofChildPsychologyandPsychiatry.
Peairson,S.,etal.(2008)."CognitivedevelopmentandhomeenvironmentofruralParaguayaninfantsandtoddlersparticipatinginPastoraldelNiño,anearlychilddevelopmentprogramme."JournalofResearchinChildhoodEducation22(4):343-362.
Pelto,G.H.,Santos,I.,Gonçalves,H.,Victora,C.,Martines,J.,&Habicht,J.P.(2004).Nutritioncounselingtrainingchangesphysicianbehaviorandimprovescaregiverknowledgeacquisition.TheJournalofnutrition,134(2),357-362.
Penny,M.E.,etal.(2005)."Effectivenessofaneducationalinterventiondeliveredthroughthehealthservicestoimprovenutritioninyoungchildren:acluster-randomisedcontrolledtrial."TheLancet365(9474):1863-1872.
Pereira,M.B.B.andM.d.C.M.Freire(2004)."AninfantoralhealthProgrammeinGoiânia-GO,Brazil:resultsafter3yearsofestablishment."BrazilianOralResearch18(1):12-17.
Petrovic,O.&Yousafzai,A.K.(2013). PromotingCareforChildDevelopmentinCommunityHealthServices. ASummaryofthePakistanEarlyChildDevelopmentScale-up(PEDS)Trial. UNICEFReport. RetrievedonJuly23,2014fromhttp://www.unicef.org/earlychildhood/files/3_PEDS_Trial_Summary_Report.pdf
Petticrew,M.&Roberts,H.(2006).SystematicReviewsintheSocialSciences. APracticalGuide. BlackwellPublishing.
Potterton,J.,etal.(2010)."TheeffectofabasichomestimulationProgrammeonthedevelopmentofyoungchildreninfectedwithHIV."DevelopmentalMedicine&Child

136
Neurology52(6):547-551.

136
Powell,C.,etal.(2004)."FeasibilityofintegratingearlystimulationintoprimarycareforundernourishedJamaicanchildren:Clusterrandomisedcontrolledtrial."BritishMedicalJournal329(7457):89.
Rahman,A.,etal.(2009)."Clusterrandomizedtrialofaparent-basedinterventiontosupportearlydevelopmentofchildreninalow-incomecountry."Child:Care,HealthandDevelopment35(1):56-62.
*Reese,E.,etal.(2010)."Areviewofparentinterventionsforpreschoolchildren’slanguageandemergentliteracy."JournalofEarlyChildhoodLiteracy10(1):97-117.
Itiswellknownthatchildren’slanguagedevelopmentlaysthefoundationfortheirliteracydevelopment,thoughitisdifficultforpreschoolteachersalonetoconsistentlyengageintheindividualinteractionsnecessarytoboostchildren’slanguageskills.Giventhatparentsaretheirchildren’sfirstteachers,itisimperativetoconsiderhowparentscanhelpimprovetheirchildren’slanguageandemergentliteracydevelopmentpriortoformalschooling.Thisarticlereviewsparent-trainingstudiesofchildren’slanguageandliteracyinthreecontexts:parent—childbook-reading;parent—childconversations;andparent—childwriting.Parenttrainingineachofthesecontextshasthecapacitytoimprovechildren’slanguageandliteracy,withtheeffectsbeingspecifictothetargetedskill.Allthreecontextsarepotentiallyvaluablesitesfortrainingparentstohelptheirchildren’slanguageandliteracy.Inconclusion,parentsareanundertappedresourceforimprovingchildren’slanguageandliteracy.
Reyes,M.R.,etal.(2012)."Theinteractioneffectsofprogrammetraining,dosage,andimplementationqualityontargetedstudentoutcomesforTheRulerApproachtoSocialandEmotionalLearning."SchoolPsychologyReview41(1):82-99.
Richard,S.A.,Black,R.E.,&Checkley,W.(2012)."Revisitingtherelationshipofweightandheightinearlychildhood."AdvancesinNutrition:AnInternationalReviewJournal3(2):250-254.
Richter,L.(2004).“Theimportanceofcaregiver-childinteractionsforthesurvivalandhealthydevelopmentofyoungchildren.”Areview.
*Rivera,J.A.,etal.(2004)."ImpactoftheMexicanprogrammeforeducation,health,andnutrition(PROGRESA)onratesofgrowthandanemiaininfantsandyoungchildren:A

137
randomizedeffectivenessstudy."JAMA:TheJournaloftheAmericanMedicalAssociation291(21):2563-2570.
CONTEXT Malnutritioncausesdeathandimpairedhealthinmillionsofchildren.Existinginterventionsareeffectiveundercontrolledconditions;however,littleinformationisavailableontheireffectivenessinlarge-scaleprogrammes.ObjectiveTodocumenttheshort-termnutritionalimpactofalarge-scale,incentive-baseddevelopmentprogrammeinMexico(Progresa),whichincludedanutritionalcomponent.DESIGN,SETTING,ANDPARTICIPANTS:Arandomizedeffectivenessstudyof347communitiesrandomlyassignedtoimmediateincorporationtotheprogrammein1998(interventiongroup;n=205)ortoincorporationin1999(crossoverinterventiongroup;n=142).Arandomsampleofchildreninthosecommunitieswassurveyedatbaselineandat1and2yearsafterward.Participantswerefromlow-incomehouseholdsinpoorruralcommunitiesin6centralMexicanstates.Children(N=650)12monthsofageoryounger(n=373interventiongroup;n=277crossoverinterventiongroup)wereincludedintheanalyses.INTERVENTIONChildrenandpregnantandlactatingwomeninparticipatinghouseholdsreceivedfortifiednutritionsupplements,andthefamiliesreceivednutritioneducation,healthcare,andcashtransfers.MAINOUTCOMEMEASURES Two-yearheightincrementsandanemiaratesasmeasuredbybloodhemoglobinlevelsinparticipatingchildren.RESULTS Progresawasassociatedwithbettergrowthinheightamongthepoorestandyoungerinfants.Age-andlength-adjustedheightwasgreaterby1.1cm(26.4cmintheinterventiongroupvs25.3cminthecrossoverinterventiongroup)amonginfantsyoungerthan6monthsatbaselineandwholivedinthepooresthouseholds.After1year,meanhemoglobinvalueswerehigherintheinterventiongroup(11.12g/dL;95%confidenceinterval[CI],10.9-11.3g/dL)thaninthecrossoverinterventiongroup(10.75g/dL;95%CI,10.5-11.0g/dL)whohadnotyetreceivedthebenefitsoftheintervention(P=.01).Therewerenodifferencesinhemoglobinlevelsbetweenthe2groupsatyear2afterbothgroupswerereceivingtheintervention.Theage-adjustedrateofanemia(hemoglobinlevel<11g/dL)in1999washigherinthecrossoverinterventiongroupthanintheinterventiongroup(54.9%vs44.3%;P=.03),whereasin2000thedifferencewasnotsignificant(23.0%vs25.8%,respectively;P=.40).CONCLUSION Progresa,alarge-scale,incentive-baseddevelopmentprogrammewithanutritionalintervention,isassociatedwithbettergrowthandlowerratesofanemiainlow-income,ruralinfantsandchildreninMexico.
Rogoff,B.(2003).Theculturalnatureofhumandevelopment.NewYork:OxfordUniversityPress.
Roy,S.K.,etal.(2005)."Intensivenutritioneducationwithorwithoutsupplementaryfeedingimprovesthenutritionalstatusofmoderately-malnourishedchildreninBangladesh."
138
Roy,S.K.,etal.(2007)."PreventionofmalnutritionamongyoungchildreninruralBangladeshbyafood-health-careeducationalintervention:Arandomized,controlledtrial."Food&NutritionBulletin28(4):375-383.
Ruel,M.T.,etal.(2008)."Age-basedpreventivetargetingoffoodassistanceandbehaviorchangeandcommunicationforreductionofchildhoodundernutritioninHaiti:Aclusterrandomisedtrial."TheLancet371(9612):588-595.
*Saleemi,M.A.,etal.(2004)."FeedingPatterns,DiarrhoealIllnessandLinearGrowthin0–24-Month-oldChildren."JournalofTropicalPediatrics50(3):164-169.
Theaimwastostudytheimpactofsimplehealthcareinterventionsin0–24-month-oldchildrenlivinginruralcommunitiesoutsideLahore,Pakistan.Newbornsbelongingtofourbirthcohortswerefollowedmonthlyfrom0–24monthsofagelivinginruralcommunities.Threecohortswerefromthesamevillage:CohortA(1984–1987),n=485;CohortB(1990–1992),n=544;andCohortC(1995–1997),n=518.Afourth,CohortD,wasfromneighbouringvillages(1995–1997),n=444.FindingsfromCohortAformedthebasisofahealthcareProgramme,includingpromotionofoptimalbreastfeedingpractices,adviceonoralrehydrationtherapy,andcontinuedfeedingduringdiarrhoea.Theoutcomemeasuresstudiedweretimeofinitiationofbreastfeeding,feedingofprelacteals,exclusivebreastfeeding,diarrhoealillnesses,andpostnatallineargrowth.Themediantimeofinitiationofbreastfeedingdecreasedfrom47to3handexclusivebreastfeedingincreasedfrom5percentinCohortAtomorethan80percentinthesubsequentcohorts,at1monthofage.Noprelactealsweregivento34percentofnewbornsinlatercohortscomparedwith100percentinCohortA.Diarrhoealillnessesduringthefirst6monthshadreducedsignificantly.Postnatallineargrowthimprovedbyabout3cminthelatercohorts.Appropriatechangesinbreastfeedingpracticesthroughintegratedandfocusedhealthcare,especiallyantenatally,canreducediarrhoealillnesses,andsustainandimprovelineargrowthinyoungchildren.
*Santos,I.,etal.(2001)."NutritioncounselingincreasesweightgainamongBrazilianchildren."TheJournalofNutrition131(11):2866-2873.
Toassesstheimpactonchildgrowthofthenutrition-counselingcomponentoftheIntegratedManagementofChildhoodIllnesses(IMCI)strategy,arandomizedtrialwasimplemented.All28governmenthealthcentersinaSouthernBrazilcitywerepairedaccordingtobaselinenutritionalindicators.Onecenterfromeachpairwasrandomlyselectedanditsdoctorsreceived20-htraininginnutritioncounseling.Thirty-threedoctorswereincludedand12–13patients<18monthsofagefromeachdoctorwererecruited.Thestudyincludedtestingtheknowledgeofdoctors,
139
observingconsultationsandvisitingthechildrenathome8,45and180daysaftertheinitialconsultation.Maternalknowledge,practicesandadherencetonutritionalrecommendationswereassessed,andanthropometricmeasurementsweretaken.Day-longdietaryintakewasevaluatedonasubsampleofchildren.Doctorsintheinterventiongrouphadbetterknowledgeofchildnutritionandimprovedassessmentandcounselingpractices.Maternalrecallofrecommendationswashigherintheinterventionthaninthecontrolgroup,aswassatisfactionwiththeconsultation.Reporteduseofrecommendedfoodswasalsoincreased.Dailyfatintakewashigherintheinterventionthaninthecontrolgroup;meandailyintakesofenergyandzincalsotendedtoimprove.Children12monthsofageorolderhadimprovedweightgainandapositivebutnonsignificantimprovementinlength.Nutrition-counselingtrainingimproveddoctors’performances,maternalpracticesandthedietsandweightgainofchildren.Therandomizeddesignwithblindoutcomeevaluationstronglysupportsacausallink.Theseresultsshouldbereplicatedinothersettings.
Santosham,M.,etal.(2010)."Progressandbarriersforthecontrolofdiarrhoealdisease."TheLancet376(9734):63-67.
Sawasdipanich,N.,etal.(2010)."EffectsofacognitiveadjustmentprogrammeforThaiparents."Nursing&healthsciences12(3):306-313.
*Schroeder,D.G.,etal.(2002)."Anintegratedchildnutritioninterventionimprovedgrowthofyounger,moremalnourishedchildreninnorthernVietNam."FoodandNutritionBulletin23(Supplement2):50-58.
Integratednutritionprogrammesarewidelyusedtopreventand/orreversechildhoodmalnutrition,butrarelyrigorouslyevaluated.TheimpactofsuchaprogrammeonthephysicalgrowthofyoungruralVietnamesechildrenwasmeasured.WerandomizedsixcommunestoreceiveanintegratednutritionprogrammeimplementedbySavetheChildren.Wematchedsixcommunestoserveascontrols.Oursampleconsistedof238children(<I>n</I>=119pergroup)whowere5to30monthsoldonentry.BetweenDecember1999andDecember2000,wemeasuredweightandheightmonthlyforsixmonthsandagainatmonth12.Principleoutcomeswereweight-for-ageZscore(WAZ),height-for-ageZscore(HAZ),andweight-for-heightZscore(WHZ),andthechangesamongthesemeasures.Asexpected,anthropometricindicatorsrelativetointernationalreferencesworsenedasthechildrenaged.Overall,childrenintheinterventioncommuneswhowereexposedtotheintegratednutritionprogrammedidnotshowstatisticallysignificantbettergrowththancomparisonchildren.Interventionchildrenwhowereyounger(15monthsorless)andmoremalnourished(lessthan−2Z)atbaseline,however,deteriorated
140
significantlylessthantheircomparablecounterparts.Betweenbaselineandmonthfour,forexample,interventionchildrenwhoweremalnourishedandlessthan15monthsoldatentrylostonaverage0.05WAZwhilesimilarcomparisonchildrenlost0.25WAZ(<I>p</I>=.02).Lackofoverallimpactongrowthmaybeduetoalowerthanexpectedprevalenceofmalnutritionatbaselineand/ordewormingofcomparisonchildren.Targetingnutritioninterventionsatveryyoungchildrenwillhavethemaximumimpactongrowth.
Sharma,S.andS.Nagar(2009)."InfluenceofhomeenvironmentofpsychomotordevelopmentofinfantsinKangraDistrictofHimachalPradesh."JournalofSocialSciences21(3):225-229.
Shaw,D.S.,Connell,A.,Dishion,T.J.,Wilson,M.N.,&Gardner,F.(2009).Improvementsinmaternaldepressionasamediatorofinterventioneffectsonearlychildhoodproblembehavior.Developmentandpsychopathology,21(02),417-439.
Shonkoff,JackP.andPhillips,DeborahA.,(eds.),(2000)FromNeuronstoNeighborhoods:TheScienceofEarlyChildhoodDevelopmen.Washington,NationalAcademyPress.
Sidibeh,L.(2008)EvaluationoftheparentaleducationProgrammeatLRR,CRR&URR,TheGambia.
Sloand,E.,Astone,N.M.,&Gebrian,B.(2010).Theimpactoffathers’clubsonchildhealthinruralHaiti.FieldActionReport,100(2),201-204.
Solis-Camara,P.andM.D.Romero(2002)."Effectsofaparentingprogrammeformothersandfathersofyoungchildren:Theimportanceofparents'schooling"RevistaLatinoamericanadePsicologia34(3):203-215.
*Sripaipan,T.,etal.(2002)."EffectofanintegratednutritionprogrammeonchildmorbidityduetorespiratoryinfectionanddiarrheainnorthernVietNam."Food&NutritionBulletin23(Supplement2):67-74.
Infectiousdiseaseandpoordietarethetwoproximalcausesofmalnutritioninchildren.Duringthe1990s,integratednutritionprogrammesimplementedbySavetheChildren(SC)inVietnamreducedseverechildmalnutrition,butithasnotbeenclearifthisimpactwasdueprimarilytoimproveddietorreduceddisease.Theaimofthisstudywastodeterminewhetheracommunity-based,integratednutritionprogrammeinVietnamreducedchildmorbidityduetodiarrheaoracuterespiratoryinfections.Children5to25monthsoldwererandomlyselectedfromrandomlyassignedinterventionandcomparisoncommunes.Caregiversofchildrenfromtheinterventionandcomparisongroups(<I>n</I>=119pergroup)wereinterviewedabouttheirchild'smorbidityatprogrammebaselineandatstudymonths2,4,6,and
141
12.Multiplelogisticregressionandgeneralestimatingequations(GEE)wereusedtoevaluatetheeffectoftheinterventionontheoccurrenceofanydiarrheaandrespiratoryillnessintheprecedingtwoweeks.Respiratoryillness,mainlyupperrespiratoryillness,wasmorecommonthandiarrhealdiseaseatbaseline(54%vs.6%,respectively).Duringfollow-up,childrenintheinterventioncommuneshadapproximatelyhalftherespiratoryillnessexperiencedbythoseincomparisoncommunes(AOR=0.5;<I>p</I>=.001).Diarrhealdiseasewasalsolowerintheinterventiongroup,althoughdifferenceswerenotstatisticallysignificant.WeconcludethatSC'sintegratednutritionprogrammewasassociatedwithreducedupperrespiratoryillness,perhapsduetoimprovedhygienepracticesand/orimprovedmicronutrientintakes.
Stokes,T.F.andD.M.Baer(1977)."Animplicittechnologyofgeneralization."Journalofappliedbehavioranalysis10(2):349.
Strand,M.A.,etal.(2002)."Preventingricketsinlocallyappropriateways:AcasereportfromNorthChina."InternationalQuarterlyofCommunityHealthEducation21(4):297-322.
Terwee,C.B.et.al(2012). Qualitycriteriawereproposedformeasurementpropertiesofhealthstatusquestionnaires.JournalofClinicalEpidemiology,60(1):34-42.
*Thomas,R.andM.Zimmer-Gembeck(2007)."BehavioraloutcomesofParent-ChildInteractionTherapyandTripleP—positiveparentingprogramme:Areviewandmeta-analysis."JournalofAbnormalChildPsychology35(3):475-495.
Weconductedareviewandmeta-analysesof24studiestoevaluateandcomparetheoutcomesoftwowidelydisseminatedparentinginterventions—Parent-ChildInteractionTherapyandTripleP-PositiveParentingProgramme.Participantsinallstudieswerecaregiversand3-to12-year-oldchildren.Ingeneral,ouranalysesrevealedpositiveeffectsofbothinterventions,buteffectsvarieddependingoninterventionlength,components,andsourceofoutcomedata.Bothinterventionsreducedparent-reportedchildbehaviorandparentingproblems.TheeffectsizesforPCITwerelargewhenoutcomesofchildandparentbehaviorswereassessedwithparent-report,withtheexclusionofAbbreviatedPCIT,whichhadmoderateeffectsizes.AllformsofTriplePhadmoderatetolargeeffectswhenoutcomeswereparent-reportedchildbehaviorsandparenting,withtheexceptionofMediaTripleP,whichhadsmalleffects.PCITandanenhancedversionofTriplePwereassociatedwithimprovementsinobservedchildbehaviors.ThesefindingsprovideinformationabouttherelativeefficacyoftwoprogrammesthathavereceivedsubstantialfundingintheUSAandAustralia,andfindingsshouldassistinmakingdecisionsaboutallocationsoffundinganddisseminationoftheseparentinginterventionsinthefuture.
142
Thompson,M.E.andT.L.Harutyunyan(2009).“Impactofacommunity-basedintegratedmanagementofchildhoodillness(IMCI)ProgrammeinGegharkunik,Armenia”.HealthPolicyandPlanning,24(2):101-107.
Tripathy,P.,etal.(2010)."Effectofaparticipatoryinterventionwithwomen'sgroupsonbirthoutcomesandmaternaldepressioninJharkhandandOrissa,India:acluster-randomisedcontrolledtrial."TheLancet375(9721):1182-1192.
UNESCO(1994). InternationalYearoftheFamily. FinalReport. RetrievedonJuly22,2014fromhttp://unesdoc.unesco.org/images/0009/000999/099959eb.pdf
UNICEF(2007).Progressforchildren:AWorldFitforChildrenstatisticalreview.NewYork,Author.
UNICEF(2009). EvaluationofUNICEFMultipleIndicatorClusterSurveyRound3(MICS3).FinalReport. RetrievedonJuly22,2014fromhttp://www.unicef.org/evaldatabase/files/MICS.pdf
UnitedNationsDepartmentofEconomicandSocialAffairs(2011).Meninfamiliesandfamilypolicyinachangingworld.NewYork,UnitedNations.
Vachirarojpisan,T.,K.Shinada,&Y.Kawaguchi,(2005).“TheprocessandoutcomeofaProgrammeforpreventingearlychildhoodcariesinThailand”.CommunityDentalHealth.22(4):235-259.
Vegas,E.andL.Santibáñez(2010).ThepromiseofearlychildhooddevelopmentinLatinAmericaandtheCaribbean.WashingtonDC,WorldBankPublications.
Vitolo,M.R.,etal.(2008)."Effectivenessofanutritionprogrammeinreducingsymptomsofrespiratorymorbidityinchildren:Arandomizedfieldtrial."Preventivemedicine47(4):384-388.
*Walker,S.P.,etal.(2004)."Psychosocialinterventionimprovesthedevelopmentoftermlow-birth-weightinfants."TheJournalofNutrition134(6):1417-1423.
Itisestimatedthat11%ofbirthsindevelopingcountiesaretermlow-birth-weight(LBW);however,thereislimitedinformationonthedevelopmentoftheseinfants.OurobjectivesweretodeterminetheeffectofpsychosocialinterventiononthedevelopmentofLBWinfantsandtocomparetermLBWandnormal-birth-weight(NBW)infants.TermLBW(n=140)andNBWinfants(n=94)wereenrolledfromthemainmaternityhospitalinKingston,Jamaica.TheLBWinfantswererandomly

143
assignedtocontrolorinterventioncomprisingweeklyhomevisitsfrombirthto8wkandfrom7to24moofage.Developmentwasassessedat15and24mowiththeGriffithsScales.Theinterventionbenefitedtheinfants’developmentalquotient(DQ,P<0.05)andperformancesubscaleat15mo(P<0.02),thehandandeye(P<

143
0.05)andperformancesubscales(P<0.02)at24mo,andhomeenvironmentat12mo.Theeffectoftheinterventionondevelopmentwasmediatedinpartbytheimprovementinthehomeenvironment.ThecontrolLBWinfantshadsignificantlylowerscoresthantheNBWinDQandseveralsubscales,whereastherewerenosignificantdifferencesbetweentheNBWandtheLBWinfantsafterintervention.Inconclusion,termLBWwasassociatedwithdevelopmentaldelays,whichwerereducedwithpsychosocialintervention.
Walker,S.P.,etal.(2005)."Effectsofearlychildhoodpsychosocialstimulationandnutritionalsupplementationoncognitionandeducationingrowth-stuntedJamaicanchildren:Prospectivecohortstudy."TheLancet366(9499):1804-1807.
Walker,S.P.,etal.(2006)."Effectsofpsychosocialstimulationanddietarysupplementationinearlychildhoodonpsychosocialfunctioninginlateadolescence:Follow-upofrandomisedcontrolledtrial."BMJ333(7566):472.
Walker,S.P.,etal.(2010)."Theeffectofpsychosocialstimulationoncognitionandbehaviorat6yearsinacohortofterm,low-birthweightJamaicanchildren."DevelopmentalMedicine&ChildNeurology52(7):e148-e154.
Wasik,B.A.&Iannone-Campbell,C.(2012/January2013).DevelopingVocabularyThroughPurposeful,StrategicConversations.TheReadingTeacher,66(4),321–332.
*Watanabe,K.,etal.(2005)."EarlychildhooddevelopmentinterventionsandcognitivedevelopmentofyoungchildreninruralVietnam."TheJournalofNutrition135(8):1918-1925.
Littleisknownaboutthelong-termbenefitsofinterventionsthataimtopromoteearlychildhooddevelopmentprogrammes.Thegoalofthisresearchwastodeterminewhetheranearlychildhooddevelopmentinterventionaddedtoanutritioninterventionduringpreschoolageshadlastingeffectsonthecognitivedevelopmentofschool-agechildrenincommunesofThanhHoaprovinceinruralVietnam.Thestudyfocusedonatotalof313childrenaged6.5–8.5y(grades1and2inprimaryschool)in2communesthatwereexposedtonutritioninterventionornutritionandearlychildhooddevelopment(ECD)interventionfrom1999to2003.Measurementsofheightandcognitivetestscores(Raven’sProgressiveMatricesTest)werecollectedfromthechildren;householdcharacteristicsweredeterminedbyinterviewswithmothers.Longitudinalanalysiswasperformedbyintegratingthedatawiththatcollectedfromthesamechildreninpastsurveys.SignificanteffectsoftheECDinterventioncomparedwiththenutritioninterventionweredetected.ThebeneficialeffectofECDinterventiononthecognitivetestscoreswaslargeforthemostnutritionallychallengedchildrenwhoseheight-for-ageZ-scoresdeclined

144
orremainedinthestuntedrange.Thefindingshelpprovideusefulinsightsintothe
144
developmentofaneffectiveintegratedmodelofECDandnutritioninterventionforchildreninruralVietnam.
*Waters,H.R.,etal.(2006)."Thecost-effectivenessofachildnutritioneducationProgrammeinPeru."HealthPolicyandPlanning21(4):257-264.
Thisarticlereportsimpactandcostresultsfromahealthfacility-basednutritioneducationProgrammetargetingchildrenlessthan2yearsofageinTrujillo,Peru.KeyelementsoftheProgrammeincludedparticipativecomplementaryfeedingdemonstrations,growthmonitoringsessionsandanaccreditationprocess.Datawerecollectedfromsixinterventionandsixcontrolhealthfacilitiestomeasureutilizationandcostsassociatedwiththeintervention.Tocalculatetheunitcostsofservices,thesecostsareallocatedusingactivity-basedcosting.Tomeasuretheeffectsoftheintervention,338childrenwerefollowedthroughhouseholdsurveysatregularintervalsfrombirthuntiltheageof18months.Theinterventionhadaclearpositiveimpactbothontheuseofnutrition-relatedservicesandonchildren'sgrowthoutcomes.Childrenintheinterventionareasmade17.6visitstohealthfacilitiesinthefirst18monthsoflife,comparedwith14.1visitsforchildreninthecontrolareas(P<0.001).Thispatternholdstrueforallsocioeconomicgroups.Theinterventionprevented11.1casesofstuntingper100children.Inmultivariatelogisticregressionanalysis,childrenintheinterventionwere0.33timesaslikelytobestuntedasthecontrols(P=0.002).Themarginalcostoftheintervention–includingexternalcosts,training,healtheducationmaterialsandextratravelandequipment–isUS$6.12perchildreachedandUS$55.16percaseofstuntingprevented.TheestimatedmarginalcostoftheinterventionperdeathavertedisUS$1952.
Whiting,B.B.,&Edwards,C.P.(1988).Childrenofdifferentworlds:Theformationofsocialbehavior.Cambridge,MA:HarvardUniversityPress.
WorldHealthOrganization(2004).Theimportanceofcaregiver-childinteractionsforthesurvivalandhealthydevelopmentofyoungchildren;DepartmentofChildandAdolescentHealthandDevelopment.
Yeung,W.J.,etal.(2002)."HowMoneyMattersforYoungChildren'sDevelopment:ParentalInvestmentandFamilyProcesses."ChildDevelopment73(6):1861-1879.
Yoshikawa,H.,etal.(2003)."Effectsofearnings-supplementpoliciesonadulteconomicandmiddle-childhoodoutcomesdifferforthe“hardesttoemploy”."ChildDevelopment74(5):1500-1521.
Yousafzaietal.(2013).“AnnualResearchReview:ImprovedNutrition-Apathwaytoresilience”.JournalofChildPsychologyandPsychiatry,54(4):367-377.














![University of Edinburgh · Web view[Systematic review: 2 tables; 3 figures; 1 Supplementary Table] Mellow Parenting: systematic review and meta-analysis of an intervention . to promote](https://img.dokumen.tips/doc/110x75/600f204a0016be77f129f626/university-of-edinburgh-web-view-systematic-review-2-tables-3-figures-1-supplementary.jpg)