Embed Size (px)
Citation preview

Epilepsia, 47(12):2154–2164, 2006Blackwell Publishing, Inc.C© 2006 International League Against Epilepsy
A Survey of Public Awareness, Understanding, and Attitudestoward Epilepsy in Greece
∗Nicholaos Diamantopoulos, ∗Joseph Kaleyias, †Meropi Tzoufi, and ‡Charilaos Kotsalis
∗Department of Pediatric Neurology, Karamandanion Children’s Hospital, Patra, Greece; †Department of Pediatrics, University ofIoannina Hospital, Ioannina, Greece; and ‡Department of Pediatric Neurology, Penteli’s Children’s Hospital, Athens, Greece
Summary: Purpose: To assess familiarity, understanding, andattitude toward epilepsy in Greece and identification of negativepredictive factors.
Methods: A 19-item questionnaire was administered to 750adults. The magnitude of social stigma toward epileptic peoplewith epilepsy was measured with a quantitative scale of socialrejection. Statistical analysis with chi-square and multiple re-gression analysis were used to identify factors associated withnegative attitudes.
Results: Of our respondents 38.8% knew someone withepilepsy and 50.8% had witnessed a seizure. Ninteen percent be-lieved that epilepsy is a type of mental retardation, 15% believedit is a type of insanity, 91.8% considered epilepsy as a brain dis-order while 5.2% considered it as a supernatural phenomenon.Seventy-seven percent considered epilepsy as a curable diseasewhile 57.5% believed that the risk of inheriting it is very high.
Regarding marriage to a patient with epilepsy 45.4% rejectedit while regarding his employment 37.7% were positive, 47.8%were skeptical while 12.8% were against it. The Greek pub-lic’s rejection tendency toward epileptic people was generallylow. Negative predictive factors were older age, low educationallevel, unfamiliarity with epilepsy, and erroneous beliefs aboutepilepsy.
Conclusions: The Greek public is familiar with epilepsy buthas a suboptimal level of appropriate understanding of essentialaspects of the disease. The overall public’s level of rejection to-ward people with epilepsy is low but certain groups of people arehighly rejective. Information campaigns targeting specific pop-ulation subgroups are necessary in Greece in order to improvethe public’s understanding of epilepsy and tolerance towardpeople with epilepsy. Key Words: Epilepsy—Awareness—Knowledge—Attitudes—Greece.
INTRODUCTION
Epilepsy, the falling sickness or sacred disease of pasttimes, is a disease that often carries a heavy social stigma.Although the quality of life of a person with epilepsy isprimarily determined by the duration of the disease andthe extent of seizure control, other nonepileptic parameterssuch as social and psychological factors are also very im-portant. Closely interrelated social factors include socialanxiety, parental anxiety, employment, and social stigma.(Jacoby, 2002; Schachter, 2005).The role of these factorshas been studied by numerous studies and has been thesubject of a book (Baker and Jacoby, 2000).
Stigma is defined as any social attribute that is deeplydiscrediting for an individual and, in the case of epilepsy,it can significantly affect the quality of a patient’s life inmany everyday activities such as going to school, working,driving, creating a family, and obtaining insurance. Thesocial stigma has been classified (Scambler, 1989) as felt
Accepted July 24, 2006.Address correspondence and reprint requests to N. Diamantopoulos,
Department of Pediatric Neurology, Karamandanion Children’s Hospi-tal, Patra, Greece. E-mail: [email protected]
doi:10.1111/j.1528-1167.2006.00891.x
and enacted. Felt stigma is defined as the shame associatedwith being an epileptic and the fear of encountering stigmaby other people while enacted stigma is defined as actualepisodes of discrimination against an epileptic, solely onthe ground of his disease. The stigma associated with anydisorder is determined not only by the actual character-istics of the disorder but also by social stereotypes con-cerning it created by lack of information, misconceptions,and unfounded fears. In the case of epilepsy, stigma seemsto be largely based on the public perception of epilepsyas a disease that can unpredictably cause a violent andfrightening attack on the patient’s mental faculties, thatis incurable, that affects the patient’s personality, and thatmay be transmitted to his offspring. These perceptions,although not entirely or necessarily misconceptions, whenbecome social stereotypes, obviously cause prejudice andrejection toward anyone with epilepsy.
If these problems are to be dealt with, a systematic studyof the public knowledge and attitude toward epilepsy isthe necessary first step. Such studies have been carriedout in many countries throughout the world: UnitedStates (Caveness et al., 1974, Caveness and Gallup, 1980,Kobau and Price, 2003), Germany (Finke, 1980), Finland
2154

SOCIAL ATTITUDES TOWARD EPILEPSY IN GREECE 2155
(Iivanainen et al., 1980), Italy (Canger and Cornaggia,1985), China (Lai et al., 1990), Denmark (Jensen and Dam,1992), Taiwan (Chung et al., 1995), India (Gambhir et al.,1995 Radhakrishnan et al., 2000), Hungary (Mirnics et al.,2001), Czechoslovakia (Novotna and Rector, 2002), NewZealand (Hills and MacKenzie, 2002), Korea (Kim et al.,2003), United Kingdom (Jacoby et al., 2004), and Austria(Spatt et al., 2005). A similar study in Oman (Al Adawiet al., 2001) was restricted to health personnel. The presentstudy is the first of its kind in Greece.
Some of these earlier studies have tried to identify socio-economic variables associated with negative attitudes to-ward people with epilepsy but only two studies (Chunget al., 1995; Spatt et al., 2005) have used methods of mul-tivariate analysis. Our study introduced a novel approachto obtain a quantitative measurement of the public atti-tude toward people with epilepsy and used multivariateanalysis to identify individual predictive variables.
Such studies are performed not just for descriptive pur-poses but with the ultimate hope that their findings willbe helpful in designing information campaigns regardingepilepsy. Some of the earlier studies that have been re-peated over time show positive (more tolerant) changes insocial attitude toward epilepsy. Examples are the USAbetween 1949 and 1979 (Caveness and Gallup, 1980),Hungary between 1994 and 2000 (Mirnics et al., 2001),and the Czech Republic between 1981 and 1998 (Novotnaand Rector, 2002). This trend can be explained by the gen-eral improvements in the educational level, by the easierpropagation of information, and perhaps by sociopoliti-cal changes that have taken place over the past decadesin these countries as well as by specific interventions andcampaigns regarding epilepsy. The exact impact of suchspecific interventions is difficult to evaluate but there islimited evidence that they can be effective (Mirnics et al.,2001; Kim et al., 2003).
MATERIALS AND METHODS
The study design and the sampleThe study was conducted in January 2003 by cooper-
ation of the Departments of Pediatric Neurology of threeRegional Medical Centers covering three large geograph-ical and administrative areas of Greece: the District ofAttica, in central Greece, including the capital city ofAthens, the District of Achaia, in south west Greece, in-cluding the city of Patra and the District of Ioannina, innorth west Greece, including the city of Ioannina. Thismulticenter design was used to obtain a sample that wouldrepresent large and socioeconomically diverse parts of thecountry in an attempt to approximate a nationwide study.
The questionnaire was administered during a face-to-face interview to randomly selected healthy people vis-iting the three participating medical centers. Epilepsyoutpatient clinics were specifically excluded as potential
sources of interviewees but if one of the other visitors hada relative with epilepsy he was allowed to participate. Inthe case of a whole family visiting the medical center onlyone member was allowed to participate. The only visitorselection criteria were that they should be adults (over20 years old) and that they should be permanent residentsof the district studied. Immigrants into the country musthave been residing in Greece for at least two years andunderstand the language.
Each of the three participating districts contributed 250adults (20 years of age or older) permanently residing inthe district, thus creating a sample of 750 people. TheDistrict of Attica—where the capital city is located—contributed equally to the other two districts because al-though it is a much larger district it represents approxi-mately one-third of Greece’s total population while thetwo other districts represent the remaining two-thirds.Each group of 250 people was stratified according tosex, age (20–39, 40–59, and over 60 years old), area ofresidence (urban: population of more than 10,000, semi-urban: population between 2,000 and 10,000 and rural:population of less than 2,000), educational level (I: illit-erate or only part of primary school, II: graduates of pri-mary school, III: graduates of secondary school, and IV:graduates of university) and marital status. To assure thatthe sample was as much as possible representative of thepopulation under study the proportions of people in eachstratum were predetermined to correspond to the relevantproportions of the Greek 2001 census for each one of thethree participating districts.
Because of a significant influx of economic immigrantsinto Greece over the past 10–15 years (primarily fromAlbania and other countries of the former Eastern block)we thought it appropriate to incorporate a group of im-migrants into the study and therefore the sample was alsostratified according to nationality (Greeks versus immi-grants).
The questionnaireThe questionnaire consisted of 19 questions (see the
Appendix). Eight of them (Q 1, 3, 4, 6, 9, 16, 17, 18) werereplicated, in their original format or slightly modified,from the 1980 USA study of Caveness and Gallup (1980).The other 11 questions were developed after reviewingthe relevant literature and considering the most importantsocial issues relevant to epilepsy. The questionnaire inves-tigated three major issues:
a. Familiarity with epilepsy (Q1–Q4)b. Understanding of epilepsy (Q5–Q11)c. Attitude toward the epileptic person (Q12–Q19).
The answers to the first two groups of questions wereof the “yes or no” format while the questions regardingattitude toward epilepsy allowed for selection betweenthree or four graded answers with the first choice always
Epilepsia, Vol. 47, No. 12, 2006

2156 N. DIAMANTOPOULOS ET AL.
TABLE 1. Demographic data of the sample
I. Attica N (%) II. Achaia N (%) III. Ioannina N (%) Total N (%)250 (100) 250 (100) 250 (100) 750 (100)
Age20–39 yrs 103 (41.2) 101 (40.4) 87 (34.8) 291 (38.8)40–59 yrs 85 (34.0) 79 (31.6) 80 (32.0) 244 (32.5)>60 yrs 62 (24.8) 70 (28.0) 83 (33.2) 215 (28.7)
SexMale 117 (46.8) 125 (48.0) 128 (49.2) 370 (49.3)Female 133 (53.2) 125 (48.0) 122 (43.8) 380 (50.7)
NationalityGreeks 232 (92.8) 233 (93.2) 244 (97.6) 709 (94.5)Immigrants 18 (7.2) 17 (6.8) 6 (2.4) 41 (5.5)
Area of residenceUrban: >10,000 221 (88.4) 147 (58.8) 145 (58.0) 513 (68.4)Semiurban: 2000–10,000 21 (8.4) 66 (26.4) 34 (13.6) 121 (16.1)Rural: <2,000 8 (3.2) 37 (14.8) 71 (28.4) 116 (15.5)
Educationlevel I (illiterate) 25 (10.0) 31 (12.4) 58 (23.2) 114 (15.2)level II (elementary school) 61 (24.4) 68 (27.2) 71 (28.4) 200 (26.7)level III (secondary school) 89 (35.6) 103 (41.2) 78 (31.2) 270 (36.0)level IV (university) 75 (30.0) 48 (19.2) 43 (17.2) 166 (22.1)
Marital statusUnmarried 20 (8.0) 55 (22.0) 40 (16.0) 114 (15.2)Married / divorced 230 (92.0) 195 (78.0) 210 (84.0) 636 (84.8)
Statistical significance (p < 0.01) is indicated in bold.
reflecting minimal rejection toward an epileptic and thelast choice reflecting maximal rejection. This is unlikeearlier studies where a “yes–no” answering format wasused to evaluate attitudes but we preferred graded answersbecause we thought that attitudes and feelings are more ac-curately reported in this way. Points were assigned for eachpossible answer to the attitude-related questions Q13–Q18(1 point for answer 1, 2 points for answer 2, etc.) and byadding them up a number was obtained that reflected theoverall or mean attitude of each interviewee toward epilep-tic people. On this quantitative “scale of Social Rejection”a value of six reflected the least degree of rejection and avalue of 23 the maximum degree of rejection.
The interviewThe interviewers were one of the present authors or
a limited number of trained nurses. Before undertakingthe study all interviewers had repeated meetings to assureuniformity in recruiting interviewees and administeringthe questionnaire. The participants answered the ques-tionnaire without any intervention by the interviewers butthey were allowed to ask for clarifications regarding anyof the questions. Ample time was allowed for comple-tion of the questionnaire and the average time needed was15–20 min.
Statistical analysisDescriptive data are presented as absolute numbers
(N) and percentage (%). The association between the re-sponses and the demographic and all other social variableswas examined with the chi-square test. Odds ratio and 95%confidence intervals were calculated (OR, 95% CI). Mul-tivariate analysis (logistic regression analysis-enter) was
performed in order to identify the independent factors as-sociated with a high degree of rejection. A probabilityvalue of less than 0.01 was considered significant. All sta-tistical analyses were performed with the SPSS statisticalsoftware package (SPSS for Windows, 10, SPSS, Inc.,Chicago).
RESULTS
Out of 803 people invited to participate in the study 53refused and 750 accepted, thus the recruitment rate was93.4%. The demographics of the sample are presented inTable 1. There were some significant differences amongthe three studied districts: a smaller proportion of individ-uals in Attica lived in rural areas compared to both othercenters (an expected finding because Attica harbors thecapital city of Athens), the level of education was lowerin Ioannina compared to both other centers and more peo-ple were married/divorced in Attica compared to the othertwo districts.
Familiarity with epilepsyTable 2 presents the responses to the pivotal question
“Have you ever heard of a disease called epilepsy?” The41 people (5.5%) who answered negatively were excludedfrom the study leaving 709 people as the remaining sam-ple available for further questioning. A negative answerto this question was more likely among the immigrants,those residing in rural areas, and those at the two lowesteducational levels.
Table 3 presents the responses to the three questionsregarding familiarity with epilepsy. Of the 709 people,
Epilepsia, Vol. 47, No. 12, 2006

SOCIAL ATTITUDES TOWARD EPILEPSY IN GREECE 2157
TABLE 2. Answers to Q1 (Have you ever heard of a diseasenamed epilepsy?)
N Yes (%) No (%)
Total sample 750 94.5 5.5Region
Attica 250 96.8 3.2Achaia 250 94.8 5.2Ioannina 250 92.0 8.0
SexMale 370 94.1 5.9Female 380 95.0 5.0
Age20–39 291 97.2 2.840–59 244 95.1 4.9>60 215 90.3 9.7
Nationality:Greeks 709 95.3 4.7Immigrants 41 80.5 19.5
ResidenceUrban 513 97.9 2.1Semiurban 121 95.0 5.0Rural 116 79.5 20.5
EducationLevel I 114 78.1 21.9Level II 200 94 6.0Level III 270 98.9 1.1Level IV 166 99.4 0.6
Marital statusUnmarried 114 14.0 7.0Married / divorced 636 80.2 5.2
Statistical significance (p <0.01) is indicated in bold.
TABLE 3. Answers to questions regarding familiarity with epilepsy
Q2∗ Q3∗ Q4∗
N Yes (%) No (%) N Yes (%) No (%) N Yes (%) No (%)
Total sampleRegion 709 3.4 96.6 704 38.8 61.2 705 50.8 41.2
Attica 241 4.6 95.4 239 34.8 65.2 238 50.6 49.4Achaia 236 1.3 98.7 237 40.9 59.1 238 50.4 49.4Ioannina 229 2.6 97.4 228 42.5 57.5 229 53.5 46.5
SexMale 349 3.1 96.9 347 42.0 58.0 345 56.5 43.5Female 360 3.3 96.7 357 36.1 63.9 360 46.5 53.5
Age20–39 280 3.9 96.1 280 40.7 59.3 280 49.6 50.440–59 233 4.3 95.7 230 39.1 60.9 231 49.5 50.5>60 194 3.0 97.0 194 36.6 63.4 194 55.1 44.9
NationalityGreeks 676 3.5 96.5 672 39.2 60.8 672 51.2 48.8Immigrants 33 9.0 91.0 32 34.4 65.6 33 50.0 50.0
ResidenceUrban 501 4.2 95.8 499 39.8 59.2 498 52.7 47.3Semiurban 116 2.6 97.4 114 38.6 61.4 114 45.6 54.4Rural 92 3.3 96.7 91 37.4 62.6 913 51.6 48.4
EducationLevel I 89 2.2 97.8 88 38.6 61.4 88 50.0 50.0Level II 191 5.8 94.2 189 40.7 59.3 188 52.4 47.6Level III 265 4.1 95.9 264 36.7 63.3 265 48.5 51.5Level IV 164 1.8 98.2 163 41.1 58.9 164 54.6 45.4
Marital statusUnmarried 106 5.6 94.4 104 44.2 55.8 105 48.0 52.0Married / divorced 603 3.5 96.5 598 38.1 61.9 599 51.7 48.3
∗Q2 = Do you have a close relative with epilepsy? Q3 = Do you personally know someone with epilepsy? Q4 = Have you ever witnessed a seizure?
3.4% answered that they had a close relative with epilepsy,38.8% answered that they were personally acquainted withsomeone with epilepsy and 50.8% reported that they hadwitnessed a seizure. These figures represent a signifi-cant degree of familiarity with the disease and its clinicalexpression.
Understanding of epilepsyThe understanding the nature, the cause(s), and the
long-term course of epilepsy were evaluated by a groupof seven questions and the responses are presented inTables 4 and 5. Of the 709 people 18.9% believed thatepilepsy is a type of mental retardation (Q5) and 15.0%believed that it is a type of insanity or madness (Q6). Thesefigures reflect a high degree of misunderstanding of thetrue nature of epilepsy and represent a significant preju-dice toward a person with epilepsy since he or she seemsto be considered by a significant part of the population asinsane or retarded or both by definition. Both of these erro-neous beliefs were significantly more frequent among theless educated (levels I and II), the elderly, and those livingin rural communities (only for mental retardation). Theywere also more frequent among people from the Ioanninadistrict probably reflecting the higher proportion of ruralresidents and the lower educational level in this part of thecountry. Asked (Q7) whether epilepsy is a type of brain
Epilepsia, Vol. 47, No. 12, 2006

2158 N. DIAMANTOPOULOS ET AL.
TABLE 4. Answers to questions regarding understanding of epilepsy
Q5∗ Q6∗ Q7∗ Q8∗ Q10∗ Q11∗
N Yes No N Yes No N Yes No N Yes No N Never Often N Small High,rarely usually moder. very high
% % % % % % % % % % % %
Total sample 560 18.9 81.1 574 15.0 75.0 552 91.8 8.2 612 5.2 94.8 497 77.5 22.5 520 42.5 57.5Region
Attica 209 6.7 93.3 205 7.8 92.2 203 90.6 9.4 223 1.8 98.2 176 74.4 25.6 171 50.9 49.1Achaia 188 29.2 70.8 195 13.8 86.2 176 92.0 8.0 199 4.5 95.5 168 83.3 16.7 182 29.7 70.3Ioannina 163 22.7 77.3 174 24.7 75.3 173 93.0 7.0 190 10.0 90.0 153 74.5 25.5 167 47.9 52.1
SexMale 281 18.5 81.5 288 14.6 85.4 271 92.9 7.1 306 3.9 96.1 234 76.5 23.5 250 45.2 54.8Female 279 19.3 80.7 286 15.4 84.6 281 91.1 8.9 306 6.5 93.5 263 78.3 21.7 270 40.0 60.0
Age:20–39 225 12.4 87.6 237 8.0 92.0 226 88.9 11.1 259 2.3 97.7 187 71.1 28.9 195 51.8 48.240–59 192 16.1 83.9 192 13.0 87.0. 188 94.7 5.3 203 5.9 94.1 175 74.8 25.2 175 43.4 56.6> 60 143 32.9 67.1 145 28.9 71.1 138 92.7 7.3 150 9.3 91.7 135 89.6 10.4 150 29.3 70.7
NationalityGreeks 540 18.5 81.5 553 14.8 85.2 529 91.9 8.1 587 4.6 95.4 475 77.7 22.3 498 42.6 57.4Immigrants 20 30.0 70.0 21 19.4 80.6 23 91.3 8.7 25 20.0 80.0 22 72.7 27.3 22 40.9 59.1
ResidenceUrban 405 15.3 84.7 405 13.3 86.7 400 92.7 7.3 441 3.6 96.4 352 76.7 23.3 365 42.5 57.5Semiurban 92 31.5 68.5 98 18.4 81.6 95 89.5 10.5 101 9.9 90.1 90 81.1 18.9 88 40.9 59.1Rural 63 23.8 76.2 71 19.7 80.3 57 89.5 10.5 70 8.6 91.4 55 76.4 23.6 67 44.8 55.2
EducationLevel I 50 44.0 56.0 53 45.3 54.7 53 88.7 11.3 61 22.9 77.1 59 91.5 8.5 69 34.8 65.2Level II 138 34.0 66.0 145 23.4 76.6 142 91.5 8.5 145 8.3 91.7 139 91.4 8.6 144 31.2 68.8Level III 219 13.7 86.3 224 10.7 89.3 212 92.4 7.6 244 0.8 99.2 187 73.3 26.7 188 44.7 55.3Level IV 153 4.6 95.4 152 2.6 97.4 145 92.4 7.6 162 2.5 97.5 112 59.8 40.2 119 57.1 42.9
Marital statusUnmarried 87 11 76 88 11.4 88.6 87 91.9 8.1 97 5.1 94.9 68 72.0 28.0 73 45.2 54.8Married / divorced 471 95 376 484 15.7 84.3 463 92.0 8.0 514 5.2 94.8 429 78.5 21.5 447 41.8 58.2
∗ Q5 = Is epilepsy a type of mental retardation? Q 6 = Is epilepsy a type of insanity or madness? Q7 = Is epilepsy a type of brain disorder ormalfunction? Q8 = Is epilepsy caused by supernatural phenomena? Q10 = Can epilepsy be radically cured? Q11 = What is the risk of an epilepticperson transmitting his disease to his offspring?
Noncommitting answers have been omitted, therefore N’s for each question vary. Statistical significance (p < 0.01) is indicated in bold.
disorder or malfunction 91.8% of the sample correctly an-swered “yes” but asked (Q8) whether epilepsy is causedby supernatural phenomena 5.2% also answered “yes.”This later response was more frequent among the elderly,the immigrants, and the undereducated (22.9%). This re-sponse was also more frequent in the Ioannina districtprobably for the same reasons mentioned before.
Attempting to get the feeling of the public about thelong-term prognosis of epilepsy they were asked (Q10)whether a person with epilepsy could be cured (definedto the interviewee as being seizure free without any medi-cation). An affirmative answer was given by 77.5% whilethe rest believed the contrary. The negative answer was,once again, more frequent among the elderly, the under-educated, and the residents of the Ioannina district. Q11inquired about the risk of transmitting the disease to one’soffspring. Assuming that “small” and “moderate” are thecorrect answers, 42.5% answered correctly while 57.5%answered that the risk is “high” or “very high.” Undere-ducated people were much more likely to give “wrong”answers. This finding reflects a deeply rooted public opin-ion that epilepsy is usually a hereditary disease.
Finally, question Q9 specifically inquired about the po-tential cause(s) of epilepsy and the results are presented
in Table 5. In order of decreasing frequency epilepsy wascorrectly identified as a nervous system disorder, a heredi-tary disorder, a congenital abnormality, and incorrectly asa psychological or mental problem or as a blood disorder.Of note is the fact that 30% of the people were not able toselect any of the potential causes and answered “ I do notknow” or “some other problem” indicating a high degreeof uncertainty about this matter.
Attitude toward epilepsy and a person with epilepsyThe responses to the group of six questions probing
the attitudes toward a person with epilepsy are presentedin Table 6. For the purposes of this study a person withepilepsy was defined as “a person who occasionally has
TABLE 5. Answers to Q9 (What is the cause of epilepsy?)(multiple answers permitted)
1. A Nervous system disorder 472 (66.6%)2. A congenital abnormality 224 (31.6%)3. A mental or psychological disorder 94 (31.6%)4. A hereditary disease 305 (43.0%)5. A blood disease 31 (4.4%)6. Some other problem 117 (16.5%)7. I do not know 96 (13.5%)
Epilepsia, Vol. 47, No. 12, 2006

SOCIAL ATTITUDES TOWARD EPILEPSY IN GREECE 2159
TABLE 6. Answers to questions regarding attitude toward epilepsy (consider as epileptic a person who occasionally has seizures butis otherwise normal)
Q13. How you would react if you learned that someone you Q14. Would you like to associate with him/her in social situations ?know has epilepsy? 1. I would easily do it 531 (74.9%)
1. I would treat him as before 541 (76.3%)2. I would feel a little awkward and afraid and I would
rather avoid him63 (8.9%) 2. I would be a little hesitant about it 103 (14.5%)
3. I would feel very awkward and afraid and I would stopcontacting him
46 (6.5%) 3. I would be very hesitant about it 35 (4.9%)
4. I do not know or wish to answer 49 (6.9%) 4. I would not do it 29 (4.1%)
Q15. Could you become a close friend with Q16. Would you agree to marry (yourself or your children) with him/herhim/her ? provided this person is otherwise acceptable?
1. I would easily do it 459 (64.7%) 1. I would easily agree 64 (9%)2. I would be a little hesitant about it 126 (17.8%) 2. I would be a little hesitant about it 162 (22.8%)3. I would be very hesitant about it 55 (7.8%) 3. I would be very hesitant about it 149 (21%)4. I would avoid it 58 (8.2%) 4. I would avoid it 332 (45.4%)
Q17. Would you hire him/her in your own business provided Q18. Would you agree your children to play and have as a friend anotherhe-she had the skills or qualifications for it ? child with epilepsy?
1. I would hire him 267 (37.7%) 1. I would easily agree with it 462 (65.2%)2. I would hire him under certain circumstances 253 (35.7%) 2. I would be a little hesitant about it 134 (18.9%)3. I would be very hesitant to hire him 86 (12.1%) 3. I would be very hesitant about it 46 (6.5%)4. I would not hire him 91 (12.8%) 4. I would avoid it 56 (7.9%)
seizures but is otherwise normal” and this definition wasexplained to the interviewees prior to answering thesequestions. As mentioned in the Methods section the an-swer choices to each question reflected a progressively in-creasing degree of rejection toward an epileptic person.
Asked how they would react to the announcement thatsomeone they knew is suffering from epilepsy, the ma-jority (76.3%) reported a neutral type of reaction andonly 6.5% reported feelings of awkwardness or fear anda desire to stop associating with this person. In concertwith this positive attitude 74.9% reported that they wouldeasily socially associate with an epileptic and 64.7%that they would easily become close friends with a per-son with epilepsy. The majority also reported that theywould have no (65.2%) or only a slight (18.9%) objec-tion to their children playing and becoming friends witha child with epilepsy while only 6.5% felt very hesitantabout it.
When however the area of investigation shifted to muchmore personal issues the responses changed significantly.Asked whether they would agree to marriage with some-one with epilepsy only 9% reported no objection while43.8% were hesitant about it, and 45.4% clearly rejectedthe idea. Asked if they would hire a person with epilepsyin their own business 37.7% gave an affirmative answer,47.8% were more or less skeptical about it, and 12.8%
TABLE 7. Answers to questions regarding personal stance toward epilepsy
Q12. If you had epilepsy how easily would you talk about it with Q19. If a person close to you was to have a disease whichother people ? one would you “prefer” it to be?
1. I would keep it as a secret from everybody 76 (10.7%) Rank of order1. Epilepsy 102 (14.3%) 4 th
2. I would talk about it only with close friends 357 (50.4%) 2. Diabetes 194 (27.4%) 2 nd3. I would freely talk about it with everyone 177 (25%) 3. A chronic respiratory problem 221 (31.2%) 1 st4. I do not know or wish to answer 99 (14%) 4. A chronic cardiac problem 126 (17.8%) 3 nd
5. A psychiatric problem 6 (0.8%) 5 th
flatly rejected the idea. Regarding this last question itshould be noted that in our study the phrasing was differedcompared to all other earlier studies where the exact phras-ing was “Do you think that people with epilepsy shouldor should not be employed in jobs like other people?”Ours was a much more direct type of question that mayhave influenced the response since it is a different matterto agree in principle with the employment rights of a per-son with epilepsy than to decide to employ him in yourown business. We thought that our type of questioning wasmore likely to elicit responses closer to real life.
Table 7 presents the answers to two questions (Q12 andQ19) investigating the overall attitude toward epilepsy as adisease. Asked if they themselves suffered from epilepsyhow easily they would talk about it with other people,10.7% report that they would maintain absolute secrecyabout their disease, 50.4% would confine it only to closefriends, and 25% reported that they would openly talkabout it. The options of total secrecy/confinement to closefriends were associated with female, age over 60 and na-tionality “immigrant.” Asked what type of disease (amongfive chronic diseases: epilepsy, diabetes, respiratory prob-lems, cardiac problems, and psychiatric problems) wouldbe “preferable” for a relative of theirs the respondersranked epilepsy 4th in terms of tendency to avoid it. Onlypsychiatric problems ranked worse than epilepsy. This is a
Epilepsia, Vol. 47, No. 12, 2006

2160 N. DIAMANTOPOULOS ET AL.
0
20
40
60
80
100
120
140
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23
Social rejection score
N
6 = no rejection 14 = moderate rejection 23 = maximum rejection
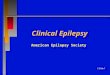
FIG. 1. Distribution of social rejection scores toward people with epilepsy.
clear indication of the fearful nature of epilepsy in people’sminds.
Population characteristics involved in the socialrejection of a person with epilepsy
Based on the answers to the six questions regarding theirattitude toward people with epilepsy (Table 6) a quan-titative estimation of the overall rejection tendency wasdeveloped as explained in the “Methods” section. Thenumber of people who had responded to all six ques-tions and were available to statistical analysis was 698.The distribution of the scores was not normal (Fig. 1)with the curve skewed to the left and the median valuewas 9.0 (25th and 75th percentiles: 8.0 and 12.0). Almost80% of the respondents had a score below 14, definedas a moderate degree of rejection, indicating a very lowlevel of rejection of a person with epilepsy by the Greekpublic. Univariate statistical analysis with chi-square re-vealed that the tendency to reject was heavily influencedby a number of factors shown in Table 8: low educationallevel, older age, not being personally acquainted with an
TABLE 8. Factors associated with a high degree of rejection∗ toward people with epilepsy
Factor N (%) OR (95% CI) p-value
Education Level Low (I and II) 80/274 (29%) 3.0 (2.14–4.26) <0.0001High (III and IV) 41/424 (9.6%)
Age >60 y.o. 62/193 (32%) 2.1 (1.36–3.28) <0.001<60 y.o 59/505 (11.6%)
Knowing someone with epilepsy No 95/430 (22%) 2.64 (1.65–4.20) <0.0001Yes 26/268 (9.7%)
Belief that epilepsy is a type of mental retardation Yes 37/106 (35%) 3.9 (2.56–5.80) <0.0001No 40/448 (9%)
Belief that epilepsy is a type of madness Yes 26/85 (30.5%) 3.07 (2.03–4.67) <0.0001No 48/483 (10%)
∗A score higher than 13 on the scale of social rejection (see the Results section).
epileptic patient, and the erroneous beliefs that epilepsyis a form of mental retardation or madness. Marital sta-tus, contrary to our expectations, was of no significance.Immigrants compared to native Greeks had a twofoldincrease in their rejection tendency but the differencewas not statistically significant (OR: 1.97, CI 0.85–4.58,p = 0.1).
These factors are apparently interrelated and thereforethey were entered into a logistic regression model to iden-tify primary variables associated with a high degree ofrejection (rejection score > 13). The multivariate analysisrevealed that the following factors are independent pre-dictors of a high degree of rejection: (a) low educationlevel (p = 0.003), (b) not acquainted with someone withepilepsy (p = 0.005), and (c) belief that epilepsy is a typeof mental retardation (p = 0.001).
DISCUSSION
Our study investigated familiarity, understanding, andattitude toward epilepsy in Greece. It follows a series of
Epilepsia, Vol. 47, No. 12, 2006

SOCIAL ATTITUDES TOWARD EPILEPSY IN GREECE 2161
TABLE 9. Comparison of studies of public opinion about epilepsy in different countries (% of positive responses)
USA Germany Italy Denmark Hungary China Taiwan N.Zealand India Austria GreeceCaveness Finke Canger Jensen Mirnics Lai Chung Hills Czechia Gambhir Spatt present
1974 1980 1985 1992 1994 2000 1990 1995 2002 2002 1995 2005 study
I have heard of epilepsy 95 90 73 97 88 89 93 87 95 94 92 89 94I Know someone with
epilepsy63 61 60 51 41 77 60 73 – 77 40 39
I have witnessed aseizure
59 ? 52 50 36 37 72 56 67 – 55 36 51
Ignorance about thecause of epilepsy∗
39 16 27 44 45 40 34 32 – 29 13
Epilepsy is a curabledisease
37 – 37 – – – – – – 22
Epilepsy is a type ofinsanity
3 21 8 15 17 16 7 1 29 15 11 15
Objection to childrenassociating withan epileptic child
6 21 11 7 19 16 57 18 2 13 43 11 14
Objection to marriage toan epileptic
18 – – 53 41 87 72 5 – 21 15 66
Agreement to regularemployment of anepileptic ∗∗
79 70 70 93 45 62 35 49 69 74 – 84 73
∗ % of people who answered “I do not know” to a question regarding the cause(s) of epilepsy.∗∗The exact phrasing of this question in the Greek study was slightly different from the other studies (see the Results section).
similar earlier studies performed in 14 other countries. Allthese studies have used generally similar methods of in-vestigation and are therefore comparable but also sharesome common methodological problems. The representa-tive strength of the population sample investigated in eachstudy varies significantly both in terms of covering thewhole or only parts of a given country and the method-ologies used to collect a sample accurately reflecting thedemographic characteristics of each country. Ideally, toobtain a sample accurately representing a country onewould need to extend the study all over the country incooperation with a professional type of Gallup agency butin our case such a task was beyond our financial abilities.Attempting to minimize the sampling bias of our studywe investigated three different country districts, with dif-ferent geographical and demographic characteristics, andtook pains to ascertain that our sample was representativeof each district according to the latest Greek census. Wethink that our results are not very far from representingthe total population because Greece is culturally a ratherhomogeneous country. This situation has been recentlychanging because of an increasing influx of economic im-migrants entering the country comprising, according to re-cent data, 10% of the country’s workforce. We addressedthis social change, also observed in most countries of theformer Western block, by incorporating a number of im-migrants in our sample. This proved very useful since thesocial attitudes of the immigrants turned out to be differentcompared to those of native Greeks.
Another major methodological issue is the type(s) ofquestionnaires used in these studies. A core of eight ques-tions that were originally used by Caveness in the USA
studies (Caveness et al., 1974 and Caveness and Gallup,1980) are traditionally replicated with no or minor vari-ations in all subsequent studies. To this common core ofquestions each study adds no, a few, or many questions. Inour study we have added 11 questions that we deemed ap-propriate. It must be stressed however that neither the orig-inal questions of Caveness nor any other questions usedin the subsequent studies have ever been validated or stan-dardized. This is an important limitation, especially whensocial attitudes are in question, and one we strongly feelshould be addressed by future studies. Perhaps a unifiedprotocol, allowing for variations between important ethnicand cultural variations, could be the answer to this prob-lem as has also been suggested by Lim and Pan (2005).With all the above-mentioned limitations in mind, Table 9presents and compares the results of our study to earlierstudies. Naturally only items that were common are in-cluded in this comparison. Only percentages of affirma-tive answers are presented because negative responses and“no answers” have been handled differently in each study.
Ninety-four percent of our sample “has heard” ofepilepsy, a figure comparable to the other studies (73–95%). The chance of not being familiar with epilepsy atall was higher among older people, the less well educated,and the residents of rural areas, a finding also observedin many of the other studies. Personal acquaintance witha person with epilepsy was reported by 39% of the par-ticipants in our study, the lowest figure among the otherstudies (40–77%). The percentage of people in our studythat have witnessed a seizure was 51%, a figure in themiddle of the range (36–72%). The differences among thevarious nations in these two measures of familiarity with
Epilepsia, Vol. 47, No. 12, 2006

2162 N. DIAMANTOPOULOS ET AL.
epilepsy are difficult to interpret given that the incidenceof epilepsy is similar across all countries.
Regarding the cause(s) of epilepsy all studies providea set of possible answers as well as the choice “I do notknow” indicating total ignorance of the cause of epilepsy.Only 13% of our sample elected this choice (the lowestfigures among all studies), a finding indicative of a ratherwell-informed Greek public. Regarding however the accu-racy of knowledge on the cause of epilepsy, although themajority of our sample responded correctly, 31% considerepilepsy as a mental or psychological problem. Of course,interpretation of these results is difficult since differenti-ation between “neurological” and “mental or psycholog-ical” problems may not be very clear in many people’sminds.
All studies, including our own, have attempted to mea-sure the public’s attitude toward a person with epilepsy.Comparison of specific attitudes (allowing children toplay with a child with epilepsy, marrying to a personwith epilepsy, and employment rights of someone withepilepsy) in our study to the other studies is difficult sincethe range of responses in these studies is extremely wide.
Our study has used a novel approach in estimatingthe degree of social rejection. Besides examining the re-sponses to individual questions we introduced a quantita-tive measurement of the overall social attitude by the use ofthe social rejection scale. We feel that this approach allowsfor a much better evaluation of the overall public attitudeand permits a more reliable means of defining social para-meters related to rejection. The overall social attitude ofthe Greek public as measured by this scale seems to bevery tolerant toward people with epilepsy. These positiveobservations are in accordance with another study that in-vestigated knowledge and attitude toward children withepilepsy among primary and secondary school teachers inGreece (Kaleyias et al., 2005). These results however mustbe interpreted with reasonable caution because of the in-herent problem in all studies of this type, namely, the prob-lem of the potential tendency of some people to answerquestions reflecting their social attitudes in a “sociallydesirable” or “politically correct” manner that does notalways represent their most sincere thoughts (Hills andMacKenzie, 2002; Spatt et al., 2005). A not unexpectedfinding was that tolerance toward a person with epilepsywas significantly lower when very personal issues such asmarriage and offering employment were involved.
In our study a number of factors were associated witha higher tendency to reject an epileptic patient and theycould be organized into three groups:
a. Older age (> 60 years old) and a low educationalstatus.
b. Unfamiliarity with epilepsy (not having observed aseizure and not being acquainted with an epilepticperson)
c. The erroneous notions that epilepsy is a form ofmental retardation or a type of mental (psychiatric)disturbance.
Many of these factors however are apparently interre-lated: being older is usually associated with a lower ed-ucational status (because of the different socioeconomiccharacteristics of the previous generations) and this in turnmay influence the level of appropriate knowledge aboutepilepsy. Among these factors, multivariate analysis iden-tified low educational level, not being acquainted withsomeone with epilepsy and believing that epilepsy is a kindof mental retardation as independent negative predictivefactors.
Most of these findings were not unexpected since theyhave also been observed in some of the earlier studies(Caveness et al. 1980, Jensen and Dam, 1992, Chung et al.,1995; Novotna and Rector, 2002, Hills and Mackenzie,2002; Spatt et al., 2005). However only two of these stud-ies have used multivariate statistics to identify independentnegative predictive factors: the Taiwanese study (Chunget al., 1995) identified male, older age, and lower level ofemployment while the Austrian study (Spatt et al., 2005)identified male, low socioeconomic background, havinglittle theoretical knowledge about epilepsy, misconceptionof epilepsy as a form of insanity, and no personal acquain-tance with someone with epilepsy. Our findings are veryclose to the above findings, especially those of the Austrianstudy. Most of the negative predictive factors identified inthese studies not only represent the results of careful sta-tistical analyses but also stand to reason: a higher level ofeducation is traditionally thought to increase tolerance to-ward social minorities or people with special needs. Alsobeing familiar with a disorder naturally increases the levelof tolerance toward it, as we are usually fearful of thingsthat we do not know or understand. Finally, having im-portant misconceptions about epilepsy (believing that aperson with epilepsy is by definition mentally retarded orpsychiatrically disturbed or both) naturally leads to prej-udice and rejection.
Immigrants to Greece were a group with a strong ten-dency to reject the epileptics although the difference didnot reach statistical significance. The educational statusof the immigrant people in our study was not known butis very likely to be low, explaining perhaps their negativeattitude. This finding also emphasizes the need to encom-pass, often difficult to reach, minority groups in any studyof social attitudes.
We also used another approach to look at how “stigma-tized” epilepsy is in the minds of our respondents: 61%stated that if they were epileptics they would confine their“secret” only to close friends if at all. The fearful na-ture of epilepsy is also supported by the observation thatamong a group of five serious medical problems, epilepsyranks very high in an increasing order of seriousness. Both
Epilepsia, Vol. 47, No. 12, 2006

SOCIAL ATTITUDES TOWARD EPILEPSY IN GREECE 2163
these observations point toward a rather high degree of feltstigma (what I think the others will think about me). It alsopoints to a contradiction between how tolerant the Greekpublic seems to be when epilepsy concerns “others” incontrast to when it concerns “us.”
In conclusion, the Greek public seems to be relativelywell acquainted and informed about epilepsy and verytolerant toward people suffering from epilepsy. Howeversignificant gaps in essential knowledge or misconceptionsabout epilepsy exist, especially among people of older ageand of a lower educational level. The same groups of peo-ple are those with the highest level of rejection toward peo-ple with epilepsy. These results clearly indicate the needfor information campaigns regarding epilepsy in Greece,a project that has not been undertaken so far by any publicor scientific authority. Groups of people with a high levelof prejudice toward epilepsy should be specific targets ofsuch a campaign.
REFERENCES
Al-Adawi S, Al-Ismaily S, Martin R, Al-Naamani A, Al-Riyamy K, Al-Maskari M, Al-Hussaini A. (2001) Psychosocial aspects of epilepsyin Oman: attitude of health personnel. Epilepsia 42:1476–1481.
Baker GA, Jacoby A. (eds). (2000) Quality of life in epilepsy: beyondseizure counts in assessment and treatment. Harwood Academic Co,Reading, UK.
Canger R, Cornaggia C. (1985) Public attitudes toward epilepsy in Italy:results of a survey and comparison with U.S.A. and West Germandata. Epilepsia 26:221–226.
Caveness WF, Meritt HH, Gallup GH Jr. (1974) A survey of publicattitudes toward epilepsy in 1974 with an indication of trends overthe past thirty years. Epilepsia 15:523–536.
Caveness WF, Gallup GH Jr. (1980) A survey of public attitudes towardepilepsy in 1979 with an indication of trends over the past thirtyyears. Epilepsia 21:509–18.
Chung MY, Chang YC, Lai YH, Lai CW. (1995) Survey of public aware-ness, understanding, and attitudes toward epilepsy in Taiwan. Epilep-sia 36:488–493.
Finke M. (1980) Public attitudes toward epilepsy in the Federal Republicof Germany: trends over the past thirty years. Epilepsia 21:201.
Gambhir SK, Kumar V, Singhi PD, Goel RC. (1995) Public awareness,understanding and attitudes toward epilepsy. The Indian Journal ofMedical Research 102:34–38.
Hills MD, MacKenzie HC. (2002) New Zealand community attitudestoward people with epilepsy. Epilepsia 43:1583–1589.
Iivanainen M, Uutela A, Vilkkumaa I. (1980) Public awareness and at-titudes toward epilepsy in Finland. Epilepsia 21: 413–423.
Jacoby A. (2002) Stigma, epilepsy and quality of life. Epilepsy Behavior3(suppl 2):10–20.
Jacoby A, Gorry J, Gamble C, Baker GA. (2004) Public knowledge,private grief: a study of public attitudes to epilepsy in the UnitedKingdom and implications for stigma. Epilepsia 45:1405–1415.
Lim SH, Pan A. (2005) Knowledge, attitudes and perceptions of epilepsyin Asia: toward a uniform study protocol. Epilepsia 46(suppl 1):48–49.
Jensen R, Dam M. (1992) Public attitudes toward epilepsy in Denmark.Epilepsia 33:459–463.
Kaleyias J, Tzoufi M, Kotsalis C, Papavasiliou A, Diamantopoulos N.(2005) Knowledge and attitude of the Greek educational communitytoward epilepsy and the epileptic student. Epilepsy Behavior 6:179–186.
Kim MK, Kim IK, Kim BC, Cho KH, Kim SJ, Moon JD. (2003) Posi-tive trends of public attitudes toward epilepsy after public educationcampaign among rural Korean residents. Journal of Korean MedicalScience 18:248–254.
Kobau R, Price P. (2003) Knowledge of epilepsy and familiarity with thisdisorder in the U.S. population: results from the 2002 HealthStylesSurvey. Epilepsia 44:1449–1454.
Lai CW, Huang XS, Lai YH, Zhang ZQ, Liu GJ, Yang MZ. (1990) Surveyof public awareness, understanding, and attitudes toward epilepsy inHenan province, China. Epilepsia 31:182–187.
Mirnics Z, Czikora G, Zavecz T, Halasz P. (2001) Changes in publicattitudes toward epilepsy in Hungary: results of surveys conductedin 1994 and 2000. Epilepsia 42: 86–93.
Novotna I, Rektor I. (2002) The trend in public attitudes in the CzechRepublic towards persons with epilepsy. European Journal of Neu-rology 9:535–540.
Radhakrishnan K, Pandian JD, Santhoshkumar T, Thomas SV, DeethaTD, Sarma PS, Jayachandran D, Mohamed E. (2000) Prevalence,knowledge, attitude, and practice of epilepsy in Kerala, South India.Epilepsia 41:1027–1035.
Scambler G. (1989) Epilepsy. Tavistock, London.Schachter SC. (2005) Improving quality of life beyond seizure control.
Epileptic Disorders 7(suppl 1):S34–S38.Spatt J, Bauer G, Baumgartner C, Feucht M, Graf M, Mamoli B,
Trinka E. (2005) Austrian Section of the International LeagueAgainst Epilepsy. Predictors for negative attitudes toward subjectswith epilepsy: a representative survey in the general public in Aus-tria.Epilepsia 46:736–742.
Appendix: The Questionnaire
Q1. Have you ever heard of a disease calledEpilepsy ?
a. Yesb. Noc. Don’t Know or wish to answer
Q2. Do you have a close relative with Epilepsy ?
a. Yesb. Noc. Don’t Know or wish to answer
Q3. Do you personally know someone with Epilepsy ?
a. Yesb. Noc. Don’t Know or wish to answer
Q4. Have you ever seen a seizure ?
a. Yesb. Noc. Don’t Know or wish to answer
Q5. Do you think Epilepsy is a type of Mental Retarda-tion ?
a. Yesb. Noc. Don’t Know or wish to answer
Q6. Do you think Epilepsy is a type of insanity or mad-ness ?
a. Yesb. Noc. Don’t Know or wish to answer
Epilepsia, Vol. 47, No. 12, 2006

2164 N. DIAMANTOPOULOS ET AL.
Q7. Do you think Epilepsy is a type of brain disorderor malfunction ?
a. Yesb. Noc. Don’t Know or wish to answer
Q8. Do you think Epilepsy is caused by supernaturalphenomena such as evil spirits, the Devil, the moon cycleetc ?
a. Yesb. Noc. Don’t Know or wish to answer
Q9. What do you think is the cause (s ) of Epilepsy ?(you may choose more than one answer ).
1. A Nervous System disorder2. A congenital abnormality3. A mental or psychological disorder4. A hereditary disease5. A blood disease6. Some other problem7. I do not Know or wish to answer
Q10. Do you know if an epileptic can be radically cured(i.e. to be seizure free without taking any medications ).
1. Never2. Rarely3. Often4. Usually5. I do not Know or wish to answer
Q11. An epileptic person (man or woman ) has children.What do you think is the risk of his children having thesame problem ?
1. The risk is relatively small2. The risk is moderate3. The risk is high4. The risk is very high5. I do not Know or wish to answer
Before answering the following questions please con-sider, for the purpose of this questionnaire, an epilepticas a person who occasionally has a seizure but is oth-erwise normal.
Q12. If yourself had Epilepsy how easily would youtalk about it with other people ?
1. I would keep it as a secret from every body.2. I would talk about it only to people very close to
me.3. I would talk about it freely with anyone.4. I do not Know or wish to answer
Q13. How you would react if you learnt that someoneyou know has Epilepsy?
1. I would treat him as before.2. I would feel a little awkward and afraid and I would
rather avoid him.3. I would feel very awkward and afraid and I would
stop contacting him.4. I do not Know or wish to answer
Q14. Would you like to associate with him / her in socialsituations ?
1. I would easily do it.2. I would be a little hesitant about it.3. I would be very hesitant about it4. I would avoid it.
Q15. Could you become a close friend with him/ her ?
1. I would easily do it.2. I would be a little hesitant about it.3. I would be very hesitant about it.4. I wouldn’t do it.
Q16. Would you agree to marry (yourself or your chil-dren ) with him/her provided this person is otherwise ac-ceptable ?
1. I would easily agree.2. I would be a little hesitant about it.3. I would be very hesitant about it4. I would avoid it.
Q17. Would you hire him in your own business providedhe had the skills or qualifications for it ?
1. I would hire him2. I would hire him under certain circumstances3. I would be very hesitant to hire him4. I wouldn’t hire him.
Q18. Would you agree your children to play and haveas a friend another child with Epilepsy ?
1. I would easily agree with it.2. I would be a little hesitant about it.3. I would be very hesitant about it4. I would avoid it.
Q19. If a person close to you was to have a diseasewhich one would you “prefer” it to be ?
1. Epilepsy2. Diabetes3. A chronic respiratory problem4. A chronic cardiac problem5. A psychiatric problem
Epilepsia, Vol. 47, No. 12, 2006