Embed Size (px)
Citation preview

Cancer Genetics and Cytogenetics 131 (2001) 1–12
0165-4608/01/$ – see front matter © 2001 Elsevier Science Inc. All rights reserved.
PII: S0165-4608(01)00483-6
Lead article
A review of the cytogenetics of 58 pediatric brain tumors
P. Roberts
a,
* P.D. Chumas
b
, S. Picton
c
, L. Bridges
d
, J.H. Livingstone
e
, E. Sheridan
f
a
Regional Cytogenetics Unit, St. James’s, Hospital, Beckett Street, Leeds, UK
b
Department of Neurosurgery, Leeds General Infirmary, Beckett Street, Leeds, UK
c
Department of Paediatric Oncology, St. James’s Hospital, Beckett Street, Leeds, UK
d
Department of Neuropathology, Leeds General Infirmary, Beckett Street, Leeds, UK
e
Department of Paediatric Neurology, Leeds General Infirmary, Beckett Street, Leeds, UK
f
Department of Clinical Genetics, St. James’s Hospital, Beckett Street, Leeds, UK
Received 23 March 2001; accepted 6 April 2001
Abstract
We describe the cytogenetic results of 58 pediatric central nervous system (CNS) tumors of vari-able histology, investigated between 1992 and 2000. Successful cytogenetics were obtained for 53patients, with clonal chromosome abnormalities demonstrated in 25. Notable findings included (1)2p abnormality in four primitive neuroectodermal tumors (PNET); (2) 1p loss in four low-gradegliomas and two PNET; (3) telomeric associations in one pilocytic astrocytoma; (4) chromosome 7gain in four astrocytomas and two PNET; (5) 17p loss in four PNET; (6) double minutes in onePNET and three glioblastomas; and (7) chromosome 10 loss in four PNET. Higher grade tumorsdemonstrated greater karyotype complexity. Low-grade tumors showed either minimal simplechromosome changes or a normal karyotype. Chromosome abnormalities were more frequent insupratentorial tumors than their infratentorial counterparts. Our results add weight to the limitedexisting body of cytogenetic documentation for pediatric CNS tumors and provide further evi-dence that 2p loss is a consistent region of chromosome involvement in PNET. We advocate fur-ther studies of CNS tumors, in particular, to evaluate the importance of 2p changes and to com-pare cytogenetic results for supratentorial tumors and their infratentorial counterparts. © 2001
Elsevier Science Inc. All rights reserved.
1. Introduction
The past 20 years have seen a considerable advance inour understanding of the importance of cytogenetic changesin pediatric solid tumors, most notably in small round celltumors. Tumor-specific, pathognomic cytogenetic abnor-malities can assist with diagnosis, as with the t(11;22) trans-location and variants thereof observed in Ewing sarcoma tu-mors [1], and t(1;13) and t(2;13) translocations in alveolarrhabdomyosarcoma [2,3]. Cytogenetic changes also canprovide prognostic information. Perhaps the most strikingexample of this is observed in neuroblastoma. Here, there isan association between 1p loss, 17q gain, and NMYC am-plification in stage IV disease [4], whereas the presence ofnear-triploidy without structural chromosome abnormalityis associated with stage IVS disease for which prognosis ismore favorable [5].
Although central nervous system (CNS) tumors are themost frequently observed pediatric tumors, there is still onlya limited understanding of the underlying cytogeneticchanges. This is partly because few specialist centers re-ceive a sufficient number of cases, and partly because of thetechnical difficulty of successful cell culture. Because mostCNS tumors are of low grade with low mitotic activity, itcan be difficult to grow the cytogenetically abnormal cells,even with reasonably sized biopsies. Cultures therefore aremore likely to fail or to produce a normal karyotype.
Few cytogenetic reviews have helped to clarify the posi-tion [6–11], but clinical and pathological diversity and acorrespondingly diverse cytogenetic picture render interpre-tation of results difficult. It thus has proved difficult to as-sign any clear diagnostic and prognostic implications to cy-togenetic changes in pediatric CNS tumors.
In contrast with pediatric CNS tumors, there is extensivecytogenetic documentation of adult CNS tumors, particu-larly for high-grade disease. Astrocytomas are the best un-derstood, with several consistent cytogenetic changes de-scribed. These include loss of chromosomes 10, 19, or 22,
* Corresponding author. Tel.:
�
44-113-2065419; fax:
�
44-113-2066201.
E-mail address
: [email protected] (P. Roberts).

2
P. Roberts et al. / Cancer Genetics and Cytogenetics 131 (2001) 1–12
gain of chromosome 7, 9p deletion, and double minutes[12–15]. Models of a multistep process illustrate the linksbetween cytogenetic changes and disease stage [16]. How-ever, it is suggested that pediatric CNS tumors have quitedifferent cytogenetic abnormalities to those observed inadults [8]. There are several possible explanations for this.First, there is a difference in location—typically infratento-rial in children and supratentorial in adults. Second, the pre-dominant tumor types differ—most pediatric CNS tumorsare primitive neuroectodermal tumors (PNET) and low-grade pilocytic astrocytomas, whereas high-grade astrocyto-mas predominate in adults. Third, tumor behavior is differ-ent—low grade astrocytomas in adults often progress tohigher grade disease, whereas in children this is unusual.
The cytogenetics of PNET is the best understood of allpediatric CNS tumors, with several recognized, nonrandomchromosome abnormalities. The most frequent of these, ob-served in 30–40% of cases, is loss of 17p, usually throughthe formation of an isochromosome of 17q [17–19]. Severalother chromosome changes have been described by conven-tional cytogenetics [7,8,20]. Additional regions of geneticimbalance also have been demonstrated by microsatelliteanalysis [21] and comparative genomic hybridization(CGH) [22,23], with some studies suggesting genetic differ-ences between infratentorial and supratentorial PNET[24,25]. The overall picture is somewhat equivocal, and therelative contributions of the different genetic changes to dis-ease pathogenesis need further clarification.
Most cytogenetic documentation of pediatric astrocyto-mas is for high-grade disease. Again, the overall picture isunclear. Some studies describe abnormalities in commonwith high-grade adult disease, such as 17p loss, chromo-some 7 gain, and losses of chromosomes 10 and 22 [26],with loss of heterozygosity for chromosome 10 the singlemost frequent genetic change in high-grade pediatric astro-cytomas [27]. Conversely, other studies describe differ-ences compared with adult disease [6,28]. Further data areclearly needed to help establish more conclusively the natureand possible significance of any cytogenetic differences be-tween high-grade astrocytomas in adults and children.
Less is known about the cytogenetics of low-grade pedi-atric astrocytomas. Some reports show no distinct cytoge-netic abnormalities [26] whereas others describe gain ofchromosomes 7 and 8 as important events [29]. Documenta-tion of other pediatric CNS tumors is also scant, althoughsome abnormalities are now well established, such as mono-somy 22 or 22q deletion in malignant rhabdoid tumors [30]and ependymomas [31]. Overall, there is a general correla-tion between karyotype complexity and tumor grade, withlow-grade disease showing a normal karyotype or simplechromosome changes, and malignant disease showing mul-tiple complex chromosome changes.
The aims of this study were to add to the body of existingliterature, evaluate any recurrent abnormalities, comparelow-grade and high-grade disease, compare supratentorialwith infratentorial types, and compare our results with those
already published in the literature. We report the cytoge-netic analysis of a series of 58 pediatric CNS tumors.
2. Materials and methods
Fresh tissue transported in Ham’s F10 culture mediumwas received from 58 pediatric CNS tumors biopsied at theLeeds General Infirmary between 1992 and 2000. This fig-ure represents just over half of the total of pediatric CNS tu-mors referred to Leeds during this period. Those patientsfrom whom biopsies either were not taken or were too smallor unsuitable for cytogenetic study were excluded from thestudy. Once received at the laboratory, biopsies were trans-ferred into fresh Ham’s F10 wash medium and dissociatedwith sterile scissors and forceps. The macerated tissue wasseparated out for suspension and monolayer cultures.
Short-term suspension cultures were established in RPMI1640 medium containing 15% fetal calf serum and supple-mented with glutamine and antibiotics. Cultures were exposedto a final concentration of 20
�
g/ml colcemid for 17 hours andharvested the following day using standard techniques.
Material for monolayer culture was either placed directlyinto Falcon flasks or digested with trypsin/EDTA and typeII collagenase beforehand. Flasks were grown in an opensystem in a 50:50 mixture of Ham’s F10 and RPMI 1640containing 15% fetal calf serum, supplemented with gluta-mine and antibiotics. Cultures were harvested according togrowth and mitotic activity (usually between 3 and 14 days).Less active cultures were exposed to Colcemid for 17 hours,whereas more active cultures were given shorter Colcemidexposure (1–4 hours) at 200
�
g/ml. Harvesting proceededusing standard techniques.
Slides were analyzed by GTL banding. Between 5 and20 metaphases were examined per case, according to avail-ability and karyotype complexity.
3. Results
Successful karyotypes were obtained for 53 of 58 cases.These included 25 astrocytomas, 16 central PNET (includ-ing two pineoblastomas), one peripheral PNET, six ependy-mal tumors, two neuronal and mixed-neuronal tumors, twosubependymal giant cell tumors, and one malignant ter-atoma. Culture failure was attributed to smallness of samplesize in three cases and low mitotic activity in another twocases. Cytogenetic results mostly were obtained from longerterm monolayer cultures (grown for 4–20 days), althoughshorter term (24 hours) suspension cultures from PNET andthe higher grade astrocytomas were often successful. Clonalchromosome changes were observed in 25 (47%) of the 53successes. The results are summarized in Table 1.
3.1. Astrocytomas
In total, 14 infratentorial and 14 supratentorial tumorswere examined. These comprised 19 pilocytic types (nine

P. Roberts et al. / Cancer Genetics and Cytogenetics 131 (2001) 1–12
3
cerebellar, one brain stem, and nine supratentorial, includ-ing three in the optic chiasm), two fibrillary (one cerebellarand one brain stem), two anaplastic (both supratentorial),and five glioblastomas (one cerebellar, one brain stem andthree supratentorial), as outlined in Table 2. Short-term sus-pension cultures were successful for some of the higher
grade tumors, whereas longer term monolayer cultures werenecessary for lower grade tumors. Clonal chromosome ab-normalities were observed in 11 of the 25 successful cases(four of the 10 successful infratentorial types, one of the twosuccessful brain stem types, and six of the 13 successful su-pratentorial types). These included five of the 17 successful
Table 1Cytogenetic results for 58 pediatric brain tumors
Tumor type Total Success Fail Abnormal (%) Normal (%)
Astrocytoma (WHO grade I) 19 17 2 5 (29.4) 11 (70.6)Astrocytoma (WHO grade II) 2 2 0 1 (50) 1 (50)Anaplastic astrocytoma (WHO grade III) 2 2 0 2 (100) 0 (0)Glioblastoma (WHO grade IV) 5 4 1 3 (75) 1 (25)PNET/medulloblastoma 17 16 1 11 (68.7) 5 (31.3)Ependymoma 6 5 1 1 (20) 4 (80)Mixed glial 3 3 0 1 (33.3) 2 (66.7)Subependymal giant cell 2 2 0 0 (0) 2 (100)Teratoma 1 1 0 0 (0) 1 (100)Peripheral PNET 1 1 0 1 (100) 0 (0)Totals 58 53 5 25 (47) 28 (53)
Table 2Cytogenetic results for 28 astrocytic tumors
Case no. Histology Karyotype
Cerebellar tumors (n
�
11)1 PA 114
�
130,dic(2;16),
�
mar,inc2 PA Failed3 PA 46,XY4 PA 45
�
46,XX,del(4)(q12q27),tas(8;21)(p23.3;p13),tas(15;21)(p13;p13),tas(19;21)(q13.4;p13),
�
21[cp14]5 PA 46,XY6 PA 46,XX7 PA 46,XX8 PA 46,XX9 PA 46,XY
10 FIB 54
�
56,XX,
�
1,
�
1,der(1;13)(q10;q10),dic(1;15)(p11;q26.3),
�
5,
�
6,
�
7,
�
9,
�
9,
�
10,
�
11,
�
13[cp3]11
a
GBM 90
�
120,dmin,incBrain stem tumors (n
�
3)12 PA Failed13 FIB 46,XY14
a
GBM 43
�
112,XX,del(1)(q10),
�
10,dic(12;17)(p11;p11),
�
16,
�
17,
�
22,der(22;22)(q10;q10),
�
r,dmin[cp7]Optic chiasm tumors (n
�
3)15 PA 46,XX16 PA 46,XY17 PA 46,XX
Other supratentorial tumors(n
�
11)18 PA 46,XX19 PA 54,XY,
�
1,add(1)(p11),
�
7,
�
8,
�
9,
�
10,
�
12,add(12)(q15),
�
13,
�
20/56,idem,
�
6,
�
9,
�
12,
�
add(12p),
�
17,
�
2120 PA 45,XX,der(1;16)(q10;p10)21 PA 79,XXX,
�
X,
�
5,
�
7,
�
10,
�
12,
�
13,
�
14,
�
15,
�
17,
�
19,
�
20,
�
2222 PA 46,XX23 PA 46,XY24 AA 46,XY,der(17)t(7;17)(q22;q21)25
a
AA 52,XY,
�
2,
�
8,
�
8,
�
10,
�
18,
�
mar26
a
GBM Failed27
a
GBM 50
�
59<2n>,XX,
�
3,add(4)(p15)
�
6,
�
6,add(7)(q11.2),add(7)(q32),
�
9,
�
13,
�
13,
�
15,der(15)t(13;15)(q21;q15),
�
16,add(16)(p13),
�
17,
�
17,add(18)(q12),
�
19,add(19)(p13.3),add(19)(q13.2),
�
20,add(20)(q13.2),
�
5
�
14mar,2
�
6dmin[cp8]28
a
GBM 46,XX
Abbreviations:
PA
�
pilocytic astrocytoma, FIB
�
fibrillary astrocytoma, AA
�
anaplastic astrocytoma, GBM
�
glioblastoma.
a
Died.

4
P. Roberts et al. / Cancer Genetics and Cytogenetics 131 (2001) 1–12
pilocytic types (two of the eight infratentorial types, andthree of the nine supratentorial types), one of the two fibril-lary types (cerebellar), both of the anaplastic types (supra-tentorial), and three of the four successful glioblastomas(one cerebellar, one brain stem, and one supratentorial).Ploidy ranged from near diploid (typically in pilocytictypes) to near-pentaploid. To date, all of the patients withlow-grade tumors are still alive, whereas all five of the glio-blastomas and one of the anaplastic astrocytomas have died.Although karyotypic complexity was greater in grade IVdisease, and abnormalities were more prevalent amongst su-
pratentorial tumors, there were few consistent chromosomechanges. In general, pilocytic tumors showed no or fewstructural chromosome changes and several chromosomegains. If the pilocytic cases in the optic chiasm are ex-cluded, clonal abnormalities were more frequent in supra-tentorial types (three of six cases) compared with their in-fratentorial counterparts (two of eight cases). Three of thelower grade tumors (two pilocytic and one fibrillary) dem-
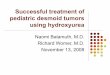
Fig. 1. Cell from case 17: pilocytic astrocytoma showing 1p loss and whole chromosome 1 gain. Karyotype 54,XY,�1,add(1)(p11),�7,�8,�9,�10,�12,add(12)(q15),�13,�20. Arrows denote the add(1p) and the add(12q).
Fig. 2. Partial karyotype of case 4: pilocytic astrocytoma showing telo-meric associations between 8p and 21p and between chromosomes 19qand 19q.
Fig. 3. Polyploid metaphase from case 11: glioblastoma showing multipledouble minutes and multiple chromosome rearrangements.

P. Roberts et al. / Cancer Genetics and Cytogenetics 131 (2001) 1–12
5
Table 3Cytogenetic results for 17 PNET
Case no. Site Karyotype
Infratentorial(n
�
12)29 Cerebellum 46,XY,add(8)(p?),
�
10,add(11)(p13),
�
15,del(15)(q12),?del(17)(p1?),
�
mar1,
�
mar2[cp9]/92,idemx2[6]30 Cerebellum (spinal metastases) Failed31
a
Cerebellum 93,XX,
�
X,
�
Y,
�
Y,
�
2,
�
3,
�
5,
�
8,
�
8,
�
9,
�
9,
�
9,
�10,�10,�11,�11,�13,�13,�15,�17,�17,�17,add(17)(p11)�2,i(17)(q10)�2,�18,�18,�18,�18,�20,�20,�20,�21,�22,�2mar
32a Cerebellum 46,XY33 Cerebellum (with astroglial differentiation) 46,XY34 Cerebellum 46,XX35 Cerebellum 46,XY36a Cerebellum 46,XY,?add(17)(q?)37 Cerebellum (desmoplastic, spinal metastases) 46,XY,der(2)add(2)(p24)add(2)(q33),del(15)(q1q21)38a Cerebellum 46�47,XX,�2,�mar[cp2]/89�92,XX,�add(1)(q?),�2,�add(2)(p?),�6,�6,�7,�7,
�8,�10,�14,�14,�16,�17,�17,�17,�20,� mar1,�mar2,�mar3�2[cp15]39 Cerebellum 46,XX40 Cerebellum 80�86,XYY,add(X)(p22),i(3)(q10)�2,der(7)t(7;11)(q22;q13),i(9)(p10),�11,add(11)
(q23),�14,�14,�16,�17,�20,�22[cp3]Supratentorial(n�5)
41a Cerebral (recurrent with focal glial andneuronal differentiation 46,XX,del(2)(p22.2p23.1),del(5)(q33q35)/46,idem,del(17)(q21.3q21.3)
42a Parietooccipital 56�59,Xc,�X,�1,�1,�1,add(1)(p?),add(1)(q?),�2,del(2)(p24),�7,�8,add(8)(q?),der(9;15)(q10;q10)�2,�11,�13,�18,�20,�20
43 Parietal 69�75,XX,�X,add(1)(q42)�2,�4,�4,add(4)(q3?),�10,�11,del(11)(q2?),�13,�16,�18,�7�13mar,dmin[cp7]
44 Pineal (pineoblastoma) 45,XX,�2245 Pineal (pineoblastoma) 63�82,XXX,�X,�2,�3,�4,�5,�7,�9,�11,�12,�14,�15,�16,�17,�18,�20,
�21,�22[cp6]
aDied.
onstrated relative 1p loss (Fig. 1, case 19). Of particularnote among the abnormal pilocytic types was the presenceof several consistent and random telomeric associations incase 4 (Fig. 2). Chromosome 7 gain was observed in fourastrocytomas (two pilocytic, one fibrillary, and one anaplas-tic). Both of the abnormal anaplastic types showed recur-rence, with relatively simple chromosome changes. All ofthe abnormal glioblastomas contained a complex karyotypewith double minutes (Fig. 3, case 11).
3.2. Central PNET
In total, 17 cases were examined (12 infratentorial andfive supratentorial). Short-term suspension cultures wereused more frequently for this group. A successful karyotypewas obtained for 16 cases, 11 of which demonstrated aclonal chromosome abnormality, the highest of all of thecategories (Table 3). These comprised six of the 10 success-ful cerebellar types (including one desmoplastic variant),and all of the five supratentorial types (including two pineo-blastomas). Ploidy ranged from pseudodiploid (four cases)to near-tetraploidy (three cases). Karyotype complexity var-ied considerably, with six of 11 showing multiple abnormal-ities and five of 11 with relatively few chromosomechanges. To date, two of the supratentorial cases and four of
the infratentorial cases have died. Five of these six caseswere karyotypically abnormal.
Chromosome 10 loss, observed in four cases (three cere-bellar, one supratentorial), was the only consistent numeri-cal chromosome change. Recurrent structural chromosomechanges included (1) rearrangement of 2p22�p24 (Fig. 4,cases 37, 38, 41, and 42), giving 2p loss, in two of the su-pratentorial and two of the cerebellar types; (2) 15q deletionin two cerebellar cases; (3) 1q rearrangement, giving 1qloss, in three cases (two cerebellar, one supratentorial); and(4) 17p loss in two cerebellar types, one of which containedan isochromosome 17q (Fig. 5, case 31). The anticipatedisochromosome 17q (with concomitant 17p loss) thus wasobserved in only one case, although one case showed 17ploss without 17q gain (case 29), whereas two cases (bothalso cerebellar) showed whole chromosome 17 loss (cases38 and 40). Other notable findings included double minutesin one supratentorial case (case 43).
3.3. Other tumors
The 13 other tumors examined included seven ependymaltumors, one ganglioglioma, one malignant teratoma, two sub-ependymal giant cell tumors, one peripheral PNET, and onedysembryoplastic neuroepithelial tumor (DNET). Three of

6 P. Roberts et al. / Cancer Genetics and Cytogenetics 131 (2001) 1–12
these patients have died. A successful karyotype was obtainedfor 12 cases (Tables 4 and 5), three of which contained an ab-normal karyotype. A t(11;22) of the type typically observed intumors of the Ewing sarcoma family was found in the periph-eral PNET (Fig. 6, case 53). The patient has since died. Theother abnormal cases included an ependymoma with astro-cytic features (case 51) and an ependymoma with typical his-tology (case 47). The former contained a 1p rearrangement,giving loss of 1p, a feature shared with three of the low-gradeastrocytomas. Case 47 contained a t(X;22)(p22.1;q11) translo-cation (Fig. 7). Normal karyotypes were observed in threecases with ependymomas (one in which the patient has died),the two subependymal giant cell tumors (both with tuberoussclerosis), one DNET , one teratoma (in which the patient hasdied), and one case with ganglioglioma.
3.4. Recurrent chromosome abnormalities common to more than one tumor type
Although there were few cases, there are several recur-rent chromosome abnormalities observed in several types ofCNS tumors. these included (1) chromosome 7 gain (fourastrocytomas, and two central PNET); (2) 1p loss (two cen-tral PNET, three low-grade astrocytomas, and one mixedependymal/astrocytic tumor); (3) 17p loss (four centralPNET and two glioblastomas); and (4) double minutes(three glioblastomas and one central PNET).
4. Discussion
We have performed a cytogenetic study of 58 pediatricCNS tumors and compared our results with those previouslydescribed in the literature [6–11]. Particular attention waspaid to tumor grade and site, most notably whether the tu-mor was infratentorial or supratentorial. Karyotypes wereabnormal in 25 of 53 successful cases, including 11 astrocy-tomas, 11 central PNET, one ependymoma/astrocytoma,one ependymoma, and one peripheral PNET. The abnor-mality rate was highest for the PNET (68.7%) and lowestfor low-grade tumors, although at 29.4% (5 of 17 cases) theabnormality rate for pilocytic astrocytomas was higher thanother published studies. Karyotypic complexity was greateramong high-grade disease, with low-grade tumors typicallyshowing simple chromosome changes or a normal karyo-type. Supratentorial tumors were more likely to demonstratecytogenetic abnormality than their infratentorial counter-parts.
4.1. Astrocytomas
Astrocytomas are the most common pediatric CNS tu-mors. The predominant type is pilocytic astrocytoma (gradeI). These typically are sited in the cerebellar region, occa-sionally in the supratentorial region, and they are rare inadults, in whom high-grade astrocytomas (grades III andIV) are the predominant type. These are less commonly ob-served in children and, in contrast with lower grade tumors,are found most frequently in the supratentorial region, andoccasionally in the brain stem.
Most (19 of 25) of our successfully cultured astrocyto-mas were of low grade (17 pilocytic and two fibrillary).Two cases were in the brain stem and three were in the opticchiasm. Cytogenetic documentation of pediatric low-gradeastrocytomas is scant. Most studies either describe normalkaryotypes or fail to detect any consistent chromosomechanges [26], whereas other studies suggest that trisomy 7and 8 may be frequent events in pilocytic types [29]. Themain cytogenetic problem with low-grade tumors is the lowrate of mitotic activity such that, even if an abnormal cloneis present, it may be difficult to detect this by conventionalcytogenetics. Similarly, it is possible that CGH shows amostly normal profile because the proportions of abnormalcells are too low for detection.
Although most of our low-grade astrocytomas demon-strated a normal karyotype, clonal chromosome changeswere found in five pilocytic types and in one fibrillary type.Five of these were polyploid, with chromosome numberranging from 54 to 130, but with minimal structural abnor-malities. Consistent abnormalities included trisomy 7 (threecases) and 1p loss (three cases). The former thus is consis-tent with the study by White et al. [29] and the review byBhattacharjee et al. [8]. Genomic instability of 1p, usuallyproducing 1p deletion, is a feature of many tumors, and theexistence of several cancer-related genes in this area is sug-gested [32]. Its importance in a wide variety of neoplasias is
Fig. 4. Partial karyotypes from cases 37, 38, 41, and 42: PNET with 2pabnormality. (a) Case 37 with der(2)add(2)(p24)add(2)(q33). (b) Case 38with add(2)(p?). (c) Case 42 with del(2)(p24). (d) Case 41 withdel(2)(p22.2p23.1).

P. Roberts et al. / Cancer Genetics and Cytogenetics 131 (2001) 1–12 7
only recently beginning to unfold, with non-Hodgkin lym-phoma and peripheral PNET being among the latest dis-eases in which 1p involvement has been recognized [33,34].Although 1p deletion is not yet an established finding inCNS tumors, 1p loss of heterozygosity (LOH) has been de-scribed in oligodendrogliomas and mixed gliomas [35].Given our results, it would be interesting to perform LOHand microsatellite studies on other low-grade astrocytomasto assess whether this is another of a growing band of tu-mors in which 1p tumor suppressor genes play a role. Oneof the three cases with 1p loss contained an unbalanced t(1;
16) translocation, producing 16q loss and 1q gain. This hasbeen described in several different tumor types and often isassociated with more advanced disease [32].
Also of particular interest was the pilocytic astrocytomawith a 4q deletion as the sole consistent cytogenetic change,found with numerous telomeric associations (tas). Thesevaried from cell to cell, but mostly involved 15p with 21pand 19q with 21p. Tas is a cytogenetic phenomenon inwhich the telomeres of two chromosomes are associated orjoin with minimal or no loss of genetic material. They arerecognized findings in CNS tumors [7,36–38], and it is sug-gested that tas are preferentially found in low-grade tumors[39]. Given that the absence of telomeres means they cannotbe renewed during cell division, loss of telomeric DNA dur-ing division may result in cells stopping division and couldexplain the low activity of cells in culture. However, it issuggested that tas may be present in a transient stage beforeexpression of telomerase in the progression of many differ-ent tumors [39]. Given this, along with the correlation of te-lomerase expression and high-grade astrocytomas [40], thepresence of tas in low-grade disease should be viewed withcaution.
Comparison of the sites of our low-grade tumors sug-gested differences in the cytogenetic results. The number ofbrain stem (one successful case) and optic chiasm (threecases) tumors were too small for valid comment, although
Fig. 5. Karyogram from case 31: PNET with near-tetraploidy, two copies of an isochromosome 17q and two copies of an unbalanced 17p rearrangement, producing17p loss. Karyotype 93,XX,�X,�Y,�Y,�2,�3,�5,�8,�8,�8,�9,�9,�9,�10,�10,�11,�11,�13,�15,�16,�16,�17,�17,�17,add(17)(p11)x2,i(17)(q10)x2,�18, �18,�20,�20,�20,�21,�21,�21,�22,�8mar. Arrows denote the two copies of the isochromosome 17q (left) and two copies of the add(17p) (right).
Table 4Cytogenetic results for seven ependymal tumors
Caseno. Site Histology Karyotype
46 Cerebralhemisphere
Malignant 46,XY
47 Posterior fossa Typical 46Y,t(X;22)(p22.1;q11)
48 Posterior fossa Malignant (recurrent) 46,XY49 Posterior fossa Typical 46,XX50a Posterior fossa Malignant (recurrent) Failed51 Posterior fossa Mixed ependymoma/astrocytoma 46,XY,
add(1)(p12)52 Posterior fossa Typical 46,XY
aDied.

8 P. Roberts et al. / Cancer Genetics and Cytogenetics 131 (2001) 1–12
all four showed a normal karyotype. If these are excluded,perhaps the most noteworthy observation of our low-gradeastrocytomas is the higher abnormality rate in the supraten-torial types (three of six cases) compared with infratentorialtypes (two of eight cases). Given that 5% of pilocytic tu-mors have a reduced survival rate, follow-up of these casesis important to determine if any link can be made betweencytogenetic abnormality and prognosis. At present, becauseall of our cases with low-grade astrocytomas are still alive,it is important to monitor the patients to determine whethercytogenetic abnormality at diagnosis has any bearing onsurvival, especially for supratentorial tumors in which prog-nosis is generally poorer. Could cytogenetic change help todiscriminate between good and poorer prognosis?
High-grade astrocytomas are less prevalent in children thanin adults. The outcome is poor whatever the age of the patient.In adults, they may be either de novo or arise from a prior low-grade tumor. They are the best characterized cytogeneticallyof all adult CNS tumors. Commonly described abnormalitiesinclude trisomy 7, monosomy 10, monosomy 22, sex chromo-some loss, 9p deletion, and double minutes (usually amplifica-tion of epidermal growth factor receptor [EGFR]) [12–15].Genetic differences between de novo glioblastomas and ma-lignant change in a previously low-grade glioma have beendescribed, most notably the loss of heterozygosity of 17p andlack of EGFR amplification in the latter type [28]. Whereaskaryotypes are often complex and it can be difficult to charac-terize some of the abnormalities, it recently has proved possi-
Table 5Cytogenetic results for six other tumors
Case no. Site Histology Karyotype
Peripheral PNET (n�1)53a
Suprasellar Underlying teratoma 51,XX,add(2)(q3?),�5,�8,t(11;22)(q24;q12),�12,�18,�18
Ganglioglioma (n�1)54 Left temporal Mixed astrocytes and ganglion cells 46,XY
Teratoma (n�1)55a Left cerebral Malignant (recurrent) 46,XX
Subependymal giant cell astrocytoma(n�2)
56 Anterior left lateral ventricle
Typical (with focus of malignantprogression)
46,XX (known tuberous sclerosis)
57 Right paraventricular Typical 46,XX (known tuberous sclerosis)DNET (n � 1) 58 Right temporal lobe Mixed glial cells and neurone 46,XY
aDied.
Fig. 6. Cell from case 53: peripheral PNET with t(11;22) translocation. Karyotype 51,XX,add(2)(q3?),�5,�8,t(11;22)(q24;q12),�12,�18,�18. Arrowsdenote the add(2) and the t(11;22).

P. Roberts et al. / Cancer Genetics and Cytogenetics 131 (2001) 1–12 9
ble to link certain cytogenetic changes, particularly mono-somy 10, to a poorer prognosis [27].
The genetics of high-grade pediatric astrocytomas is lesswell understood. They are usually de novo with no priorlow-grade disease. It is suggested that they follow differentgenetic pathways to high-grade adult astrocytomas [28], assupported by the observation that double minutes andmonosomy 10 are frequent events in adults but not in chil-dren [6].
Our data included two anaplastic astrocytomas and fiveglioblastomas. Both of the anaplastic types showed simpleclonal chromosome changes in keeping with the results ex-pected for lower grade tumors. Interestingly, one of theseshowed an unbalanced t(7;17) giving loss of 17q and gain of7q as the sole chromosome changes. This case was a recur-rent tumor, thought to have progressed from a previouslylow-grade disease. The other anaplastic case showed simpletrisomies (with none of the recognized changes of adult dis-ease), and the patient has since died. All of our five glio-blastoma cases have died. Highly complex abnormal karyo-types were produced for three of these, two of which alsodemonstrated multiple double minutes. Although our num-bers of malignant cases are too low for assessing any recur-rent changes, it was clear that karyotype complexity is fargreater in glioblastomas than in lower grades of astrocytoma.
The only abnormality consistently seen across differentgrades of astrocytomas was chromosome 7 gain, usually as atrisomy, seen in two pilocytic, one fibrillary and one anaplas-
tic astrocytoma. Amplification of the genes EGFR, PDGF,and PDGFR that are all located on 7p has been described inastrocytoma [16]. Given the suggestion that at least EGFR isnot amplified in a subgroup of pediatric astrocytomas [28],further study of these genes would be interesting.
4.2. PNET
The most common malignant pediatric brain tumors arePNET, accounting for 20% of all cases. They are most fre-quently infratentorial, arising from the cerebellar hemi-spheres or vermis and commonly are referred to as medullo-blastomas. They are found less frequently at supratentorialsites, either in the pineal region where they are referred to aspineoblastomas or in the cerebral hemispheres. Up to 20%of medulloblastomas are desmoplastic, of nodular architec-ture and with a neuronal or glial phenotype. Prognosis de-pends on age, with younger children fairing less well, aswell as on size, dissemination, and extent of surgical resec-tion. “Good risk” patients have a 60–70% overall 5-yearsurvival rate, whereas “poor risk” patients have only a 35%5-year survival rate. Supratentorial location is less favorablethan infratentorial.
We examined 17 patients with PNET: 12 medulloblasto-mas and five supratentorial types (including two pineoblas-tomas). The abnormality rate at 68.7% was the highest of allof the groups of tumors studied, reflecting the malignant na-ture of this disease. Clonal chromosome changes were ob-served in six of 11 successful medulloblastomas and all of
Fig. 7. Cell from case 47: ependymoma with typical histology and t(X;22) translocation (arrow). Karyotype 46,Y,t(X;22)(p22.1;q11).

10 P. Roberts et al. / Cancer Genetics and Cytogenetics 131 (2001) 1–12
the five supratentorial types. The cytogenetics of PNET isperhaps the best described of all pediatric CNS tumors. Themost frequent abnormality is loss of 17p, usually as an iso-chromosome of 17q, observed in 30% of cases [17–19],with a common chromosomal region of disruption sug-gested at 17p11.2 [41]. Several other chromosome changesalso have been described, including gain of chromosome 7,loss of chromosomes 8 and 22, 9q deletion, 1q gain, struc-tural rearrangements of chromosomes 7 and 11, and doubleminutes [7,8,20]. Recent CGH studies have added otherchromosome regions to this list, including gains of 4p, 5p,5q, 7q, 8q, and 11q and losses of 8p, 9q, 10q, 3, 11, 16q, andX [22–25,42].
Our studies revealed a more diverse pattern, with a widevariety of different chromosome changes in our 11 abnor-mal cases. Six of these showed a complex karyotypewhereas the other five cases showed either multiple numeri-cal chromosome changes or a low number of structural rear-rangements. Perhaps the most striking finding of our resultswas the four cases (two supratentorial and two infratento-rial) with rearrangement of chromosome arm 2p, leading torelative 2p loss. Loss of 2p21�p24 has been demonstratedby conventional cytogenetics in few medulloblastomas andhigh-grade astrocytomas [7], and by microsatellite analysis[21], suggesting this could be an important region in the de-velopment and progression of some malignant tumors. In-terestingly, two of our cases with 2p loss also demonstratedglial differentiation. The MYCN gene maps to 2p24, and itis possible that it may be one of several important genes lostin our four cases. This is in marked contrast with the fewcases of PNET described with amplification of MYCN [43–46]. Further investigation of this region is warranted, partic-ularly because it was the sole abnormality in one case andalso because it was observed in both infratentorial and su-pratentorial types.
We also observed some of the more established findingsfor PNETs, including gain of chromosome 7 (two cases),17p loss (two cases as structural changes and two cases asmonosomy 17), 1q rearrangement (three cases), and doubleminutes (one case). It was interesting to note the higher ab-normality rate (five of five) among supratentorial typescompared with infratentorial cases (six of 10). It is sug-gested that there are genetic differences between infratento-rial and supratentorial types [24,25]. In particular Russo etal. [25] suggested 17q gain (and presumably 17p loss) maybe restricted to the former, with other changes such as lossof 14q and 19q more a feature of the latter. Further geneticstudies comparing infratentorial and supratentorial types areclearly warranted. Although the numbers in our study arelow, we also note that all four of our cases with chromo-some 17 loss were infratentorial. All of the other recurrentabnormalities (i.e., three or more cases) were found in bothtypes. These included 1q rearrangement and chromosome10 loss (observed in four cases). Rearrangement of 1q is arecognized finding in many tumors, usually in the form of1q gain, and it is observed frequently in PNET [8]. Mono-
somy 10 is not a frequent finding in PNET. Microsatelliteanalysis suggests loss of part of 10q, with retention of 10pand distal 10q, and is observed in a subset of PNET andglioblastomas [10]. Note that all of our cases with chromo-some 10 imbalance demonstrated whole chromosome 10loss. Given the involvement of the gene PNET (at 10q23) inastrocytomas, it would be interesting to establish if thisplays a similar role in PNET [28].
4.3. Ependymomas
Ependymomas are the third most common pediatric CNStumors, accounting for 6–12% of the total. They arise fromthe precursors of cells that line the ventricles and are foundmostly in the posterior fossa. Most cases show benign histo-logical features, and those remaining are anaplastic. Themost common chromosome abnormalities described inthese tumors are deletions of 6q and 22q [31,47]. Three ofour ependymomas showed a normal karyotype; one casewith mixed ependymoma/astrocytoma histology containedloss of 1p as the sole chromosome abnormality, a findingalso described elsewhere [48], and one with “typical” histol-ogy contained a t(X;22) translocation. This appears to havedisrupted 22q11, the site of a putative tumor suppressorgene [48]. Loss of heterozygosity studies in this case wouldbe of particular interest. Monosomy 22 or 22q abnormalityis the most common abnormality in pediatric and adultependymoma, observed in approximately one third of allkaryotypically abnormal cases [31].
4.4. Subependymal giant cell astrocytomas withtuberous sclerosis
These are rare, benign tumors typically found in the lat-eral ventricles and characteristically associated with tuber-ous sclerosis. The only documented cytogenetic study oftwo cases of this tumor in individuals with tuberous sclero-sis demonstrated a 22q deletion [49]. Our two cases bothshowed a normal karyotype with no evidence of chromo-some 22 abnormality.
4.5. Other tumors
The four other tumors in our study included one gan-glioglioma, one DNET, one malignant teratoma, and oneperipheral PNET.
Gangliogliomas are low-grade gliomas consisting of amixed population of neoplastic ganglion cells and astro-cytes and account for 5% of pediatric CNS tumors. They areclinically benign and typically found in the medial temporallobe, and they can occasionally undergo malignant transfor-mation. There are very few cytogenetic reports. Most showa normal karyotype. Those with clonal changes typicallyshow few simple abnormalities, although no consistentchanges have been identified yet [6,8]. Our single caseshowed a normal karyotype.
A DNET is a low-grade, mixed neuronal and glial tumorwith good prognosis that rarely undergoes malignant trans-

P. Roberts et al. / Cancer Genetics and Cytogenetics 131 (2001) 1–12 11
formation. There is no documented cytogenetic change spe-cific to this tumor type. Our patient with a DNET in theright temporal lobe demonstrated a normal karyotype, inkeeping with most other low-grade tumors.
Primary intracranial germ cell tumors are rare, account-ing for 5% of the total. They usually present in the suprasel-lar or pineal regions and are thought to arise in the brain af-ter improper migration of primordial cells during embryonicdevelopment. Cytogenetic studies of testicular germ cell tu-mors describe isochromosome 12p as a common abnormal-ity [50]. Cytogenetic documentation of intracranial terato-mas is scant. Of the six published cases to date, only onecontained an isochromosome 12p [51]. Our case was lo-cated in the left cerebral hemisphere and demonstrated amalignant histology. Cytogenetic analysis revealed a nor-mal karyotype.
Peripheral PNET is a soft tissue tumor with a neural phe-notype. The tumor rarely metastasizes to the brain and isdistinguished cytogenetically from central PNET by thepresence of a t(11;22) translocation or variants thereof, ob-served in up to 90% of cases [52]. This has not been de-scribed in central PNET. Our case of peripheral PNET pre-sented in the suprasellar region and, at diagnosis, appearedhistologically very similar to a malignant teratoma. Aftersubtotal resection, the tumor rapidly regrew after which itappeared much more undifferentiated than it had previ-ously. Cytogenetics of the diagnostic biopsy showed theclassic t(11;22), along with gains of chromosomes 5, 8, 12,and 18. Trisomy of chromosomes 8 and 12 are frequent sec-ondary cytogenetic changes in peripheral PNET [53].
5. Conclusions
Several conclusions can be drawn from our findings:
1. High-grade tumors are more likely to demonstrate anabnormal karyotype than low-grade tumors.
2. Karyotypic complexity is greatest for high-grade tu-mors. Karyotypically abnormal low-grade tumors typ-ically demonstrate numerical chromosome changes.
3. Supratentorial tumors more frequently contain chro-mosome abnormalities than infratentorial counterparts.
4. The most frequently observed cytogenetic change inlow-grade astrocytomas was loss of 1p.
5. Gain of chromosome 7 was the most frequent abnor-mality in astrocytomas.
6. Most PNET contain a chromosome abnormality.Monosomy 10 and 2p deletions were the most fre-quent changes.
7. Cytogenetic changes were less prevalent in ependy-momas and the other types of tumors.
8. The t(11;22) was observed in the case of peripheralPNET but not in any of the central PNET.
Our results thus concur with other published studies. Werecommend close follow-up of cases of pilocytic astrocy-toma with chromosome abnormalities to assess any possible
prognostic impact. In particular, comparison between infra-tentorial and supratentorial cases with cytogenetic abnor-mality would be interesting. We also suggest a new area ofchromosome loss at 2p22�p24 in PNET and recommendfurther study of this region to characterize the abnormalitymore fully at the molecular level.
Our conventional cytogenetics study thus has provided auseful genome-wide overview of a diverse range of pediat-ric CNS tumors. We would anticipate future studies to in-corporate a combined approach using conventional cytoge-netics and some of the other new genetic technologies.These could include fluorescence in situ hybridization usingregion-specific probes on interphase cells, CGH studies onfresh and paraffin-embedded material, microarray and mic-rosatellite studies (to assess smaller genetic imbalances),loss of heterozygosity studies, and polymerase chain reac-tion. Such a combined approach on a large cohort of cases islikely to be the way forward in our attempts to further un-ravel the genetic complexities of this group of tumors.
References
[1] de Alva E, Gerald WL. Molecular biology of the Ewing’s sarcoma/prim-itive neuroectodermal tumour family. J Clin Oncol 2000;18:204–13.
[2] Davis RJ, D’Cruz CM, Lovell MA, Biegel JA, Barr FG. Fusion ofPAX7 to FKHR by the variant t(1;13)(p36;q14) translocation in alve-olar rhabdomyosarcoma. Cancer Res 1994;54:2869–72.
[3] Shapiro DN, Sublett JE, Li B, Downing JR, Naeve CW. Fusion ofPAX3 to a member of the forkhead family of transcription factors inhuman alveolar rhabdomyosarcoma. Cancer Res 1993;53:5108–12.
[4] Lastowska M, Cotterill S, Pearson ADJ, Roberts P, McGuckin A,Lewis IJ, Bown N. Gain of chromosome arm 17q predicts unfavourableoutcome in neuroblastoma patients. Eur J Cancer 1997;33:1627–33.
[5] Look AT, Hayes FA, Shuster JJ, Douglass EC, Castleberry RP, Bow-man LC, Smith EI, Brodeur GM. Clinical relevance of tumour cellploidy and N-myc gene amplification in childhood neuroblastoma: aPaediatric Oncology Group study. J Clin Oncol 1991;9:581–91.
[6] Neumann E, Kalousek DK, Norman MG, Steinbock P, Cochrane DD,Goddard K. Cytogenetic analysis of 109 paediatric central nervoussystem tumours. Cancer Genet Cytogenet 1993;71:40–9.
[7] Bigner SH, McLendon RE, Fuchs H, McKeever PE, Friedman HS.Chromosomal characteristics of childhood brain tumours. CancerGenet Cytogenet 1997;97:125–34.
[8] Bhattacharjee MB, Armstrong DD, Vogel H, Cooley LD. Cytoge-netic analysis of 120 primary pediatric brain tumours. Cancer GenetCytogenet 1997;97:39–53.
[9] Fuji Y, Hongo T, Hayashi Y. Chromosome analysis of brain tumoursin childhood. Genes Chromosom Cancer 1994;11:205–15.
[10] Agamanolis DP, Malone JM. Chromosomal abnormalities in 47 pedi-atric brain tumours. Cancer Genet Cytogenet 1995;81:125–34.
[11] Sainati L, Bolcato S, Montaldi A, Celli P, Stella M, Leszl A, SilvestroL, Perilongo G, Cordero di Montezemolo L, Basso G. Cytogeneticsof pediatric central nervous system tumours. Cancer Genet Cytogenet1996;91:13–27.
[12] Bigner SH, Mark J, Burger PC, Mahaley MS, Bullard DE, MuhlbaierLH, Bigner DD. Specific chromosomal abnormalities in malignanthuman gliomas. Cancer Res 1988;48:405–11.
[13] Jenkins RB, Kimmel DW, Moertel CA, Schultz CG, ScheithauerBW, Kelly PJ, Dewald GW. A cytogenetic study of 53 human glio-mas. Cancer Genet Cytogenet 1989;39:253–79.
[14] Thiel G, Losanova T, Kintzel D, Nisch G, Martin H, Vorpahl K, Wit-kowski R. Karyotypes in 90 human gliomas. Cancer Genet Cytogenet1992;58:109–20.

12 P. Roberts et al. / Cancer Genetics and Cytogenetics 131 (2001) 1–12
[15] Weber GR, Sommer C, Albert FK, Kiessling M, Cremer T. Clinicallydistinct subgroups of glioblastoma multiforme studied by compara-tive genomic hybridisation. Lab Invest 1986;74:108–19.
[16] Sehgal A. Molecular changes during the genesis of human gliomas.Semin Surg Oncol 1998;14:3–12.
[17] Mertens F, Johansson B, Mitelman F. Isochromosomes in neoplasia.Genes Chromosom Cancer 1994;10:221–30.
[18] Biegel JA, Rorke LB, Packer RJ, Sutton LN, Schut L, Bonner K, Eman-uel BS. Isochromosome 17q in primitive neuroectodermal tumours ofthe central nervous system. Genes Chromosom Cancer 1989;1:139–47.
[19] Biegel JA, Rorke LB, Janss AJ, Sutton LN, Parmiter AH. Isochromo-some 17q demonstrated by interphase fluorescence in situ hybridisa-tion in primitive neuroectodermal tumours of the central nervous sys-tem. Genes Chromosom Cancer 1995;14:85–96.
[20] Heim S, Mitelman F, editors. Tumours of the central nervous system.In: Cancer cytogenetics: chromosomal and molecular genetic aberra-tions of tumour cells. 2nd ed. New York: Wiley-Liss, 1995 pp. 432–54.
[21] Blaeker A, Rasheed BKA, McLendon RE, Friedman HS, Batra SK,Fuchs HE, Bigner SH. Microsatellite analysis of childhood brain tu-mours. Genes Chromosom Cancer 1996;15:54–63.
[22] Reardon DA, Michalkiewicz E, Boyett JM, Sublett JE, Entrekin RE,Ragsdale ST, Valentine MB, Behm FG, Heideman RL, Kun LE, Sha-piro DN, Look TA. Extensive genomic abnormalities in childhoodmedulloblastoma by comparative genomic hybridisation. Cancer Res1997;57:4042–7.
[23] Avet-Loiseau H, Venaut A-M, Terrier-Lacombe M-J, Lellouch-Tubi-ana A, Zerah M, Vassal G. Comparative genomic hybridisation de-tects many recurrent imbalances in central nervous system primitiveneuroectodermal tumours in children. Br J Cancer 1999;79:1843–7.
[24] Nicholson JC, Ross FM, Kohler JA, Ellison DW. Comparative ge-nomic hybridisation and histological variation in primitive neuroecto-dermal tumours. Br J Cancer 1999;80:1322–31.
[25] Russo C, Pellarin M, Tingby O, Bollen AW, Lamborn KR, Moha-patra G, Collins VP, Feuerstein BG. Comparative genomic hybridisa-tion in patients with supratentorial and infratentorial primitive neuro-ectodermal tumours. Cancer 1999;86:331–9.
[26] Schrock E, Blume C, Meffert M-C, du Manoir S, Bersch W,Kiessling M, Lazanowa T, Thiel G, Witkowski R, Ried T, Cremer T.Recurrent gain of chromosome arm 7q in low-grade astrocytic tu-mours studied by comparative genomic hybridisation. Genes Chro-mosom Cancer 1996;15:199–205.
[27] Balesaria S, Brock C, Bower M, Clark J, Nicholson SK, Lewis P, deSanctis S, Evans H, Peterson D, Mendoza N, Glaser MG, NewlandsES, Fisher RA. Loss of chromosome 10 is an independent prognosticfactor in high-grade gliomas. Br J Cancer 1999;81:1371–7.
[28] Cheng Y, Ho-Keung NG, Zhang S-F, Pang JS-F, Zheng J, Poon W-S.Genetic alterations in pediatric high grade astrocytomas. Hum Pathol1999;30:1284–90.
[29] White FV, Anthony DC, Yunis EJ, Tarbell NJ, Scott RM, SchofieldDE. Nonrandom chromosomal gains in pilocytic astrocytomas ofchildhood. Hum Pathol 1995;26:979–86.
[30] Biegel JA, Zhou J-Y, Rorke LB, Stenstrom C, Wainwright LM,Fogelgren B. Germ-line and acquired mutations of INI1 in atypicalteratoid and rhabdoid tumors. Cancer Res 1999;59:74–9.
[31] Mazewski C, Soukup S, Ballard E, Gotwals B, Lampkin B. Karyo-type studies in 18 ependymomas with literature review of 107 cases.Cancer Genet Cytogenet 1999;13:1–8.
[32] Schwab M, Praml C, Amler LC. Genomic instability in 1p and humanmalignancies. Genes Chromosom Cancer 1996;16:211–29.
[33] Dave BJ, Hess MM, Pickering DL, Zaleski DH, Pfiefer AL, Weisen-burger DD, Armitage JO, Sanger WG. Rearrangements of chromo-some band 1p36 in non-Hodgkin’s lymphoma. Clin Cancer Res 1999;5:1401–9.
[34] Hattiger CM, Rumpler S, Strehl S, Ambros IM, Zoubek A, PotshgerU, Gadner H, Ambros PF. Prognostic impact of deletions of 1p36 andnumerical aberrations in Ewing tumours. Genes Chromosom Cancer1999;24:243–54.
[35] Mrózek K, Bloomfield CD. Der(16)t(1;16) is a secondary chromo-some aberration in at least 18 different types of human cancer. GenesChromosom Cancer 1998;23:78–80.
[36] Sawyer JR, Swanson CM, Roloson GJ, Longee DC, Chadduck WM.Cytogenetic findings in a case of pediatric glioblastoma. CancerGenet Cytogenet 1992;64:75–9.
[37] Sawyer JR, Sammartino G, Husain M, Lewis JM, Anderson B, BoopFA. Ring chromosome 12 resulting from nonrandom telomeric asso-ciations with the short arm of chromosome 15 in a cerebellar astrocy-toma. Genes Chromosom Cancer 1993;8:69–73.
[38] Harrison KJ, Neumann E, Kalousek DK, Norman MG, Masui S, Har-rison K. Astrocytoma with a unique telomere association. CancerGenet Cytogenet 1994;76:33–5.
[39] de Lange T. Telomere dynamics and genomic instability in human can-cer. In: Telomeres. EH Blackburn, CW Grieder, editors. Cold SpringHarbor, NY: Cold Spring Harbor Laboratory Press, 1995, pp. 265–93.
[40] Langford MA, Piatyszek MA, Xu RS, Schold SCJ, Shay J. Telom-erase activity in human brain tumours. Lancet 1995;346:1267–8.
[41] Scheurlen WG, Seranski P, Mincheva A, Kuhl J, Sorensen N, KraussJ, Lichter P, Poustka A, Wilgenbus KK. High-resolution deletionmapping of chromosome arm 17p in childhood primitive neuroecto-dermal tumours reveals a common chromosomal disruption withinthe Smith-Magenis region, an unstable region in chromosome band17p11.2. Genes Chromosom Cancer 1997;18:50–8.
[42] Schutz BR, Scheurlen W, Krauss J, du Manoir S, Joos S, Bentz M,Lichter P. Mapping of chromosomal gains and losses in primitiveneuroectodermal tumours by comparative genomic hybridisation.Genes Chromosom Cancer 1996;16:196–203.
[43] Rouah E, Wilson DR, Armstrong DL, Darlington GJ. N-myc amplifi-cation and neuronal differentiation in human primitive neuroectoder-mal tumours of the central nervous system. Cancer Res 1989;49:1797–801.
[44] Wasson JC, Saylors III LS, Zeltzer P, Friedman HS, Bigner SH,Burger PC, Bigner DD, Look AT, Douglas EC, Brodeur GM. Onco-gene amplification in paediatric brain tumours. Cancer Res 1990;50:2987–90.
[45] Badiali M, Pession A, Basso G, Andreini L, Rigobello L, Galassi E,Giangaspero F. N-myc and c-myc oncogene amplification inmedulloblastoma: evidence of particularly aggressive behaviour of atumour with c-myc amplification. Tumori 1995;77:118–21.
[46] Fuller GN, Bigner SH. Amplified cellular oncogenes in neoplasms ofthe central nervous system. Mutat Res 1992;276:299–306.
[47] Reardon DA, Entrekin RE, Sublett J, Ragsdale S, Li H, Boyett J,Kepner JL, Look AT. Chromosome arm 6q loss is the most commonrecurrent autosomal alteration detected in primary paediatric ependy-moma. Genes Chromosom Cancer 1999;24:230–7.
[48] Hulsebos TJM, Oskam NT, Bijleveld EH, Westerweld A, HermsenMA, van den Ouweland AMW, Hamel BC, Tijssen CC. Evidence foran ependymoma tumour suppressor gene in chromosome region22pter-22q11.2. Br J Cancer 1999;81:1150–4.
[49] Debiec-Rychter M, Jesionek-Kupnicka D, Zakrewski K, Liberski PP.Cytogenetic changes in two cases of subependymal giant-cell astro-cytoma. Cancer Genet Cytogenet 1999;109:29–33.
[50] Atkin NB, Baker MC. i(12p): specific chromosomal marker in semi-noma and malignant teratoma of the testis? Cancer Genet Cytogenet1983;10:199–204.
[51] De Bruin TWA, Slater RM, Defferrari R, Geurts van Kessel A, Suij-kerbuijk RF, Jansen G, de Jong B, Oosterhuis JW. Isochromosome12p-positive pineal germ cell tumour. Cancer Res 1994;54:1542–4.
[52] Delattre O, Zucman J, Plougastel B, Desmaze C, Melot T, Peter M,Kovar H, Joubert I, de Jong P, Rouleau G, Aurias A, Thomas G. Genefusion with an ETS DNA-binding domain caused by chromosometranslocation in human tumours. Nature 1992;359:162–5.
[53] Maurici D, Perez-Atayde A, Grier HE, Baldinin N, Serra M, FletcherJA. Frequency and implications of chromosome 8 and 12 gains inEwing’s sarcoma. Cancer Genet Cytogenet 1998;100:106–10.