Embed Size (px)
Citation preview
The iournal of Emergency Medune, Vol 4, pp 319-323. 1986 Prlnted In the USA ??CopyrIght 1986 Pergamor Journals Lid
A PATIENT WITH PROLONGED HEADACHE AND LETHARGY
0 Dr John McGill: I received a call from an outside physician regarding a patient he initially saw seven hours prior to calling me. The patient was a 41-year-old obese woman with a history of diabetes who came to his clinic complaining of a frontal head- ache of five days’ duration. She also com- plained of mild anorexia, nausea, and vom- iting. Because of these symptoms, she had not taken her insulin for three days. She had a history of migraine headaches and had been treated successfully in the past with FiorinaP. For her current headache, she had been taking Tylenol@ with some relief. However, because of the persistent nature of her headache, she sought medical attention.
In the clinic, the patient was found to be somnolent, but easily arousable, alert, and oriented when stimulated. Vital signs were normal. The neurologic exam was reported as being nonfocal and her discs were clear. The patient was given half her normal in- sulin dose and sent home. Rethinking the case, however, the physician became more concerned about the patient’s persistent lethargy. Considering the possibility of drug overdose, he sent a nurse to the pa- tient’s home. She found the patient clinical- ly unchanged. There were multiple prescrip- tion medications in the house. The bottles were empty, but the prescription dates were old. The nurse brought the patient back to the clinic where they observed her for a while before finally calling our emer-
gency department. The physician felt there was a manipulative aspect to her presenta- tion, but was concerned about a possible overdose. Because his clinic didn’t have toxicologic screening ability, he wanted to send her to us.
On examination in our emergency de- partment, the patient was a massively obese woman, weighing approximately 300 lbs, sleeping on the cart. Her blood pressure was 1 lo/60 mm Hg; pulse rate, 72 beats per minute; respirations, 18/min; and temper- ature 37.5”C. She was easily arousable, and with stimulation, was alert and oriented. She complained of an intermittent fronto- temporal headache that was not throb- bing and allowed her to sleep comfortably through the night. It was not like her typi- cal migraines. She had achieved moderate relief with Tylenol. She stated that she had not taken an overdose and, though she had a fair amount of stress in her life, she did not feel depressed. She denied neck pain and weakness. The patient related that she had received Vistaril 100 mg IM at the clinic and had taken some Benadryl at home. Her neurologic examination was nonfocal and discs were clear. Reflexes were full and sym- metric. With moderate stimulation and as- sistance, a normal sensori-motor examina- tion was obtained. It was interesting to note that although she knew what we were ask- ing her to do, she seemed apathetic, requir- ing constant prodding to complete the mo- tor exam. The most disturbing aspect of
Emergency Case Records originates from case conferences held at Denver General Hospital’s Department of Emergency Medical Services and is coordinated by Steven
v Silverstein, MD and John McGill, MD.
0736-4679/86 $3.00 + .OO
319
320 Emergency Case Records
her presentation was her degree of lethargy. Because the recent administration of hy- droxyzine pamoate (Vistaril@) and diphen- hydramine (Benadryl@) confused the issue, the patient was observed for several hours in the emergency department and was given ibuprofen (MotrirF’) to relieve her head- ache. Computed tomography (CT) would have been desirable at that time but the scanner was down,
0 Dr Tom Drake: How did the patient describe the onset of the headache?
0 Dr McGill: It came on gradually while she was sitting in a chair. It was not exacer- bated by exertion and was never severe.
Cl A physician: Did she live alone?
0 Dr McGill: No, she lived with family and her son was with her in the ED. I asked him if his mother had been acting normal- ly. He said that she had been sleeping a great deal and, unlike her usual self, wasn’t scolding him when he made noise.
??Dr Markovchickz Did anyone give thought to CO2 retention and check an arterial blood gas?
??Dr McGill: No, that was not considered.
Cl Dr Rosen: The patient probably merited an emergency CT scan. When our scanner is down we have several options. One is to send the patient to one of our affiliated institutions for the scan. The other is to do a carotid angiogram. In this woman’s case, owing to her obesity, I would suggest that it would be much wiser to get her scanned elsewhere. Maury, would she fit in the gantry?
Cl Dr Maurice O’Connor: You bring up a good point. People should be aware that there is a limited space in the scanner. Marked obesity may make a CT scan of the chest, abdomen, or pelvis impossible. They must be able to fit under the gantry.
0 Dr Rosen: One other thing that comes to mind in a patient who has somnolence and an unusual headache is carbon monox- ide poisoning. It might be worth checking a carbon monoxide level.
Cl Dr Markovchick: People with CO poi- soning usually improve after they get up in the morning and out of the bedroom. Their headache goes away, they feel better, and the next morning their symptoms return. That was not this woman’s pattern.
??Dr McGill: No, she was somnolent throughout. This was documented during her clinical stay.
0 Dr Markovchick: So you decided to let her metabolize her Vistaril@ and Benadryl@ and see if her mental status improved?
Cl Dr McGill: Yes. Another readily avail- able diagnostic modality is lumbar punc- ture (LP), especially if one was suspecting subarachnoid hemorrhage or infection. However, my primary concern was a possi- ble mass lesion. In this setting, I felt that an LP was contraindicated.
??Dr Gerald Gordon: Were the findings of her fundoscopic examination normal?
0 Dr McGill: Yes.
0 Dr Adam Cwinn: Did she have any head tenderness?
Cl Dr McGill: No; no facial or scalp tenderness.
Cl Dr Rosen: Was she hungry?
0 Dr McGill: No, she complained of nau- sea and intermittent vomiting. These are significant additions to her symptom com- plex of lethargy and headache. We often admit this type of patient to our ED ob- servation unit overnight, get a neurology consultation, and wait for the CT scan to become functional the next day. However,
Prolonged Headache and Lethargy 321
on this occasion, the CT scanner required 0 Dr Gruber: Let’s discuss what happened a part from out-of-town. Because of the next. Neurology evaluated the patient and potential delay, I obtained a neurology agreed that her exam was nonfocal. She consultation and advised admission. Re- was admitted to the neurology service with garding the decision on whether or not an the diagnosis of unexplained lethargy. A emergent CT was needed, I felt that be- CT scan was planned once the scanner be- cause the patient’s condition had remained came operational. The patient was admit- stable over the past several days and she ted to a ward bed and got some pain relief was nonfocal, she could be followed clini- with oral analgesics. At 9:00 the following cally until the CT scanner was running the evening, the CT scan was obtained. What next day. did it show Maury?
I? Dr Markovchick: Before the advent of CT scan, if you suspected a subarachnoid hemorrhage and the patient was not herniat- ing, you performed an LP. This would be difficult in a 300-lb woman.
Cl Dr McGill: If you’re thinking subarach- noid bleed (SAH), you’re right. However, although it was considered, with SAH and her degree of lethargy, one would normal- ly expect a history of sudden onset of severe headache rather than a well-localized mild headache of five days’ duration.
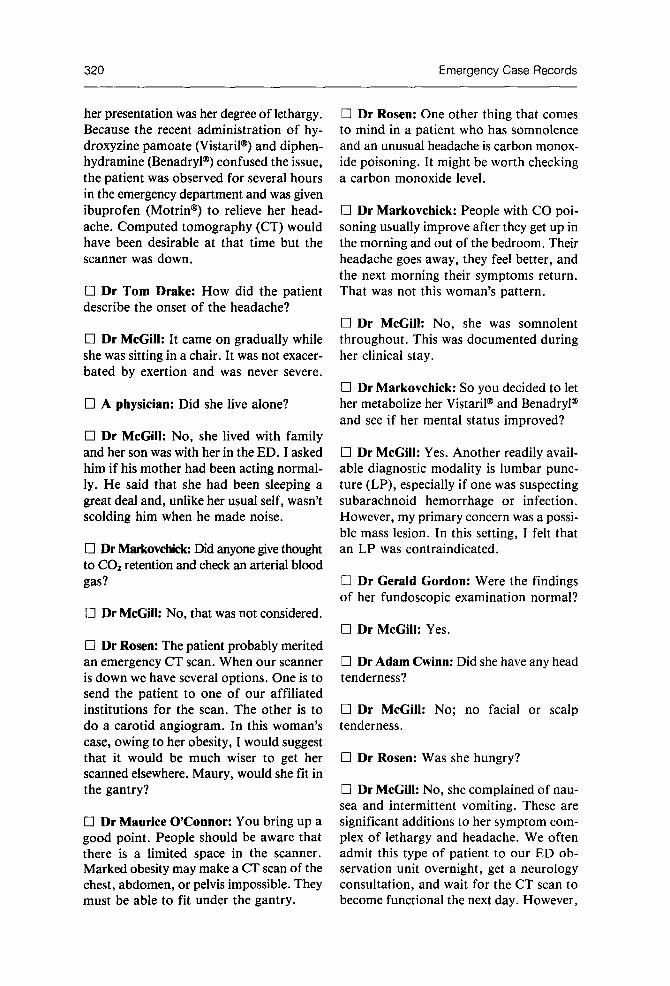
0 Dr O’Connor: I’d like to direct your at- tention to the scan in the right tempopa- rietal area (Fig 1). This is a noncontrast study and you can see increased density in this area. There is about a 7-mm mass ef- fect with shift. The neuroradiologists felt this was typical of a venous infarct. There are few other things that look like this with the increased attenuation on the noncon- trast study, edema, shift, and effacement of the folds as you go superiorly.
Cl Dr Gordon: How old was this process?
Figure 1. CT scan demonstrating a venous infarct in the right frontotemporal area.
322 Emergency Case Records
0 Dr O’Connor: Perhaps several days.
0 A physician: You say this is a venous in- farct, but isn’t that the density of a bleed?
??Dr O’Connor: Yes, hemorrhage pooled in the area; an infarct with bleeding.
0 Dr Gruber: Following the abnormal CT scan results, the neurology resident reexamined the patient and found a subtle left arm drift and a left homonymous hemianopsia.
0 Neurology resident: Prior to her CT scan, the patient’s old records were helpful in determining whether or not she was be- ing manipulative. Her last hospital admis- sion was 4 years ago, she had no ED visits, and few clinic visits. This history made us take her more seriously.
0 Dr Gruber: The exact cause of the in- farct was unclear and the patient under- went carotid angiography.
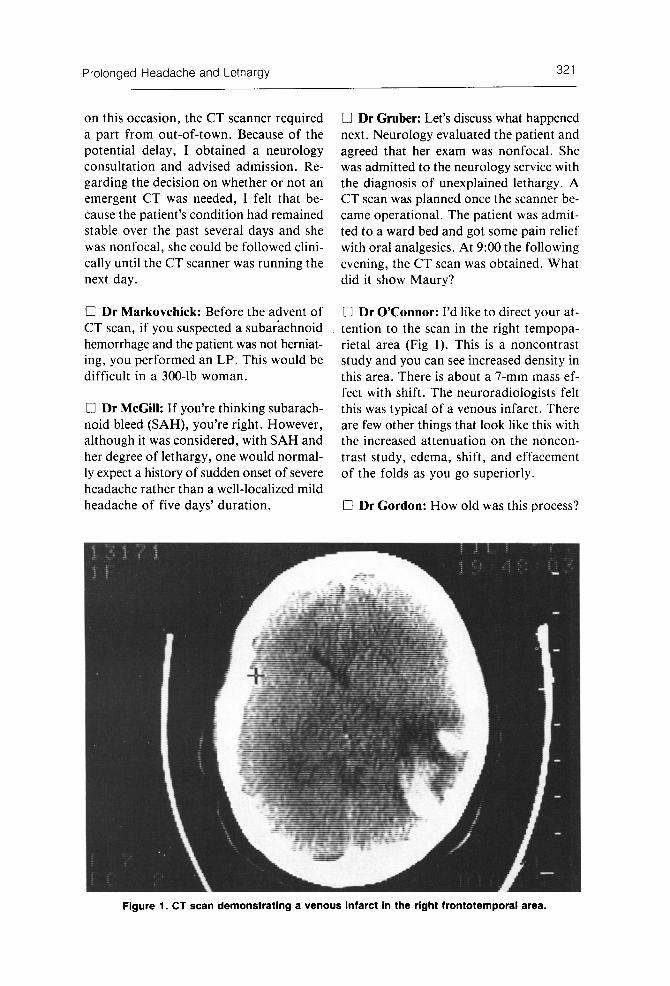
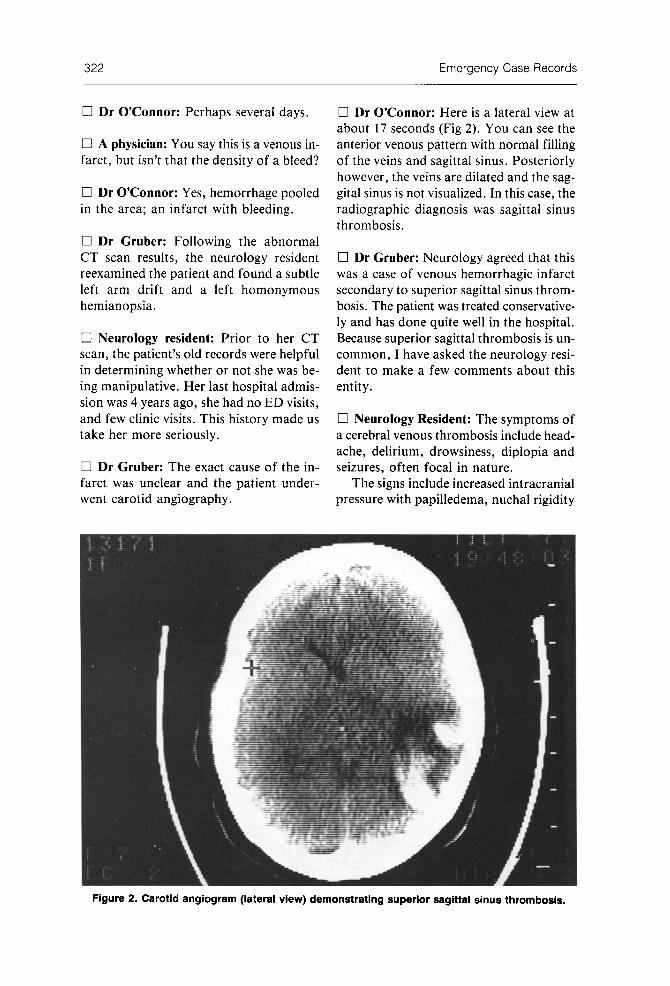
0 Dr O’Connor: Here is a lateral view at about 17 seconds (Fig 2). You can see the anterior venous pattern with normal filling of the veins and sagittal sinus. Posteriorly however, the veins are dilated and the sag- gital sinus is not visualized. In this case, the radiographic diagnosis was sagittal sinus thrombosis.
0 Dr Gruber: Neurology agreed that this was a case of venous hemorrhagic infarct secondary to superior sagittal sinus throm- bosis. The patient was treated conservative- ly and has done quite well in the hospital. Because superior sagittal thrombosis is un- common, I have asked the neurology resi- dent to make a few comments about this entity.
0 Neurology Resident: The symptoms of a cerebral venous thrombosis include head- ache, delirium, drowsiness, diplopia and seizures, often focal in nature.
The signs include increased intracranial pressure with papilledema, nuchal rigidity
Figure 2. Carotid angiogram (lateral view) demonstrating superior sagittal sinus thrombosis.

Prolonged Headache and Lethargy 323
and focal neurologic signs, most often hemi- paresis or a hemisensory loss. Patients gen- erally appear somewhat restless, confused, and obtunded. The most common primary sites of superior sagittal sinus thrombosis are the cavernous sinus and lateral sinus. In the superior sagittal sinus, blood flows anterior to posterior and drains the larger cerebral veins from both hemispheres.
The causes of superior sagittal sinus thrombosis are either infective or noninfec- tive. Infective thromboses result from in- fection in the nasal cavity, extensions from the lateral or cavernous sinuses, from epi- dural or subdural infections, or as exten- sions of osteomyelitis. Although cavernous sinus and lateral sinus thromboses are al- most always infective in nature, this is not the case with superior sagittal sinus throm- boses. A significant percentage of them have noninfective etiologies.
The noninfective causes include terminal disease, marasmus, cyanotic congenital heart disease, hypercoagulability, including sickle cell disease and polycythemia (pri- mary or secondary) antithrombin III defi- ciency, protein C deficiency, and other hy- percoagulative states. Trauma and tumor have also been found to be predisposing factors. Other cases appear to be purely idiopathic.
When the patient initially presents, focal neurologic signs and symptoms may be en- tirely absent, as they were in this case. Sometimes, symptoms of increased intra- cranial pressure, including headache, nau- sea and vomiting, and blurred vision, are the presenting complaints. In other patients, generalized lethargy may be the only pre-
senting sign. As the clot extends into larger cerebral veins, focal signs and symptoms develop as a result of hemorrhage into both grey and white matter. The definitive diag- nosis is made by carotid angiography.
Cl A physician: Could we return to the question of performing a lumbar puncture in this patient? Is it safe to do an LP if the neurologic exam is nonfocal? Maybe this is not the case.
0 Dr Rosen: I don’t think that it would have made any difference in this woman.
0 Dr McGill: I would maintain that an LP in this patient is relatively contraindi- cated. Infection was very low on the dif- ferential. If you feel that an immediate diagnosis is necessary, transferring the pa- tient to obtain the CT scan would be more advisable than doing an LP in someone with this presentation.
0 Dr Rosen: In this case, the real key is persistent lethargy. We didn’t know wheth- er it was caused by the Vistaril@ and the Benadryl@ or whether it was part of her clinical syndrome. Once we got that clari- fied, I think this patient definitiely needed a CT scan. The timing of it may have had some significance. In this case it didn’t change our management. We found a le- sion that would not have responded to ear- ly therapy or surgical intervention. This might not have been the case. I think we tend not to push to get the diagnostic pro- cedure when it is inconvenient to do so.
REFERENCES
I. Hesselbrock R, Sawaya R, Tomsick T: Superior 2. Imai WK, Everhart FR, Sanders JM: Cerebral ve- sagittal sinus thrombosis after closed head injury. nous sinus thrombosis. Report of a case and review Neurosurgery 1985; 16:825-828. of the literature. Pediafrics 1982; 70:965-970.





























