Embed Size (px)
Citation preview

Pediatric Case Report
A Novel Colonoscopic Approach for theManagement of a Malone AntegradeContinence Enema Channel, WhichCannot Be Catheterized in the ImmediatePostoperative Period: A Case Report
Konrad M. Szymanski, Alison Keenan, Mark P. Cain, Shamaila Waseem, andMartin KaeferEarly Malone antegrade continence enema (MACE) complications are rare, but can be devastating, particularly if theyinvolve loss of the channel. Management of these complications is not well described. We report on a patient who hadher MACE channel successfully salvaged in the immediate postoperative period using a colonoscopic retrograde wireand catheter placement after failing antegrade percutaneous endoscopic management. To our knowledge, this is the firstreport of a novel, colonoscopic, minimally invasive technique of managing select MACE channels, which cannotbe otherwise recatheterized. We also review the management of postoperative MACE complications. UROLOGY 84:1490e1491, 2014. � 2014 Elsevier Inc.
CASE REPORT
he patient was a 7-year-old girl with myelome-ningocele with neurogenic bladder and bowel Tleading to chronic constipation and fecal soiling.She underwent a split-appendix procedure for appendico-vesicostomy and also a Malone antegrade continenceenema (MACE) procedure. The proximal 4 cm of the insitu split appendix was imbricated in tinea flaps to ensurecontinence. The MACE stoma was spatulated using a V-flap in the right lower quadrant. The patientwas dischargedhome after an uneventful 4-day admission and returned tothe clinic when the 12F-MACE catheter became dislodged8 days after the surgery. We were unable to gently replacethe tube. Fluoroscopy demonstrated contrast in a falsepassage without continuity with the bowel.
Under general anesthesia, we confirmed circumferen-tial mucocutaneous separation and were unable to locatethe lumen of the appendix using an 8.5F Storz cystoscope(Clavien complication classification IIIb).1 The patientwas admitted overnight for the bowel preparation forcolonoscopy the following day. During the colonoscopy,the appendix was successfully cannulated from the cecum
Financial Disclosure: The authors declare that they have no relevant financial interests.From the Division of Pediatric Urology, Riley Hospital for Children at Indiana
University Health, Indianapolis, IN; and the Department of Pediatrics, Section ofPediatric Gastroenterology, Hepatology, and Nutrition, Indiana University School ofMedicine, Indianapolis, INAddress correspondence to: Konrad M. Szymanski, M.D., M.P.H., Division of
Pediatric Urology, Riley Hospital for Children at Indiana University Health, 705 RileyHospital Drive, Suite 4230, Indianapolis, IN 46202. E-mail: [email protected]: July 14, 2014, accepted (with revisions): July 29, 2014
1490 ª 2014 Elsevier Inc.All Rights Reserved
with a 260-cm 0.035-inch guidewire (Fig. 1; Video 1). A10F Mentor catheter was threaded over the wire when itexited the MACE site under direct vision via the co-lonoscope ensuring 7 cm of the catheter rested in theascending colon. The edges of the appendix could not bevisualized even with the catheter in situ. The MACEcatheter was left in situ for 10 weeks postoperatively, andthen antegrade endoscopy was performed. The channelwas noted to be patent but slightly stenotic at the skinlevel. The catheter was left in place for an additional3 weeks. She then began nightly MACE catheterizationwith an indwelling MACE stopper betweencatheterizations.
COMMENTSince its initial description byMalone in 1990,2 theMACEhas offered improved fecal continence and quality of life forcountless patients with neurogenic bowel.3 Although theMACE procedure has been proven to be safe and effectivefor improving fecal continence, it has occasional compli-cations, most commonly related to the stoma.4 Early stomalcomplications are rare but can be devastating especiallywhen the channel is lost. Management of these compli-cations is not well described.We present a novel techniquefor channel salvage in select early severe stomal compli-cations. Long-term outcomes of the technique are notknown, but early reestablishment of a patent tract allowsfor continued MACE in the short term.
At the time of MACE procedure, we typically leave anindwelling 10-12F Mentor catheter in place for 3-6 weeks.
http://dx.doi.org/10.1016/j.urology.2014.07.0470090-4295/14

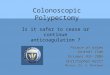
Figure 1. Colonoscopic view of the Malone antegrade continence enema channel (A) without a wire, (B) cannulated with awire, and (C) a catheter. (Color version available online.)
This is based on channel size and surgeon preference. Tapwater flushes of MACE are started with the return of bowelfunction and titrated according our institutional protocol.Patients who do not have adequate fecal continence orrelief of constipation after 6 months of MACE use arestarted on a stepwise program of increasing flush volumesadditives as we have previously reported.5 A MACE stop-per is used between the MACE catheterizations to preventstomal stenosis in the first 6 months.
We present a novel, colonoscopic, minimally invasiveapproach in the management of an MACE channelinadvertently decannulated in the immediate post-operative period, which could not be catheterizedpercutaneously. Tube dislodgement in the immediatepostoperative period is relatively rare, and the cathetercan typically be gently replaced at the bedside or endo-scopically. Given the inability to cannulate the MACEpercutaneously, the channel could have been managedconservatively. Subsequently, the MACE site would healby secondary intention and the tip of the appendix scardown, with a possible delayed MACE revision to bringthe appendix to the skin. This approach would mostlikely entail another laparotomy, a difficult dissection anda possible loss of appendix conduit. Placing a catheteracross the MACE to ensure lumen continuity does notpreclude a need for the future stomal revision due tocircumferential scarring, but it may avoid a subfascialrevision. In addition to the use of an MACE stopper, anL-stent may at least delay the need for a stomal revision.6
Alternatively, an indwelling Chait tube may ensure long-term access.
The use of colonoscopy in the management of 3 ste-notic MACE channels, which were difficult to catheterizehas been described by Farrugia et al,7 but the authors onlyused the colonoscope as a light source to guide thecystoscope into the MACE lumen for a subsequent wireplacement via the cystoscope. We have used a similarapproach successfully in the case of a 19-year-old femalepatient with spinal cord injury and an in situ appendix
UROLOGY 84 (6), 2014
MACE and Monti ileovesicostomy procedures. Shedeveloped a false passage and difficulty in catheterizingher MACE. She underwent catheterization via thecystoscope under colonoscopic guidance 6 weeks aftersurgery. Unfortunately, 18 months later, she required aChait tube placement due to persistent catheterizationdifficulties. The technique described in this report allowsfor a cannulation of a channel completely separated andinaccessible from the skin.
Acknowledging our limited experience and short-termfollow-up with this technique, we feel that this novelapproach can be successfully used in salvaging an MACEchannel in select patients in the immediate postoperativeperiod.
References
1. Dindo D, Demartines N, Clavien PA. Classification of surgicalcomplications: a new proposal with evaluation in a cohort of 6336patients and results of a survey. Ann Surg. 2004;240:205-213.
2. Malone PS, Ransley PG, Kiely EM. Preliminary report: the antegradecontinence enema. Lancet. 1990;336:1217-1218.
3. Yerkes EB, Cain MP, King S, et al. The Malone antegrade conti-nence enema procedure: quality of life and family perspective. J Urol.2003;169:320-323.
4. VanderBrink BA, Cain MP, Kaefer M, et al. Outcomes followingMalone antegrade continence enema and their surgical revisions.J Pediatr Surg. 2013;48:2134-2139.
5. Bani-Hani AH, Cain MP, King S, Rink RC. Tap water irrigation andadditives to optimize success with the Malone antegrade continenceenema: the Indiana University algorithm. J Urol. 2008;180:1757-1760; discussion 1760.
6. Mickelson JJ, Yerkes EB, Meyer T, et al. L stent for stomal stenosis incatheterizable channels. J Urol. 2009;182:1786-1791.
7. Farrugia MK, Melville D, Boddy SA. Coming face to face with thestenotic MACE-combined Maceoscopy and colonoscopy (therendez-vous procedure): a preliminary report. J Pediatr Surg. 2007;42:685-687.
Supplementary data associated with this articlecan be found, in the online version, at http://dx.doi.org/10.1016/j.urology.2014.07.047.
1491