Embed Size (px)
DESCRIPTION
A study conducted by AMCS & the Migrant Resource Centre North West Inc. funded by the Victorian Department of Health, Home and Community Care Program. The primary aim of this study is to accurately capture perceptions of dementia across 10 different cultural groups – the Croatian, Filipino, Indian, Iraqi, Leb anese, Macedonian, Polish, Sri Lankan, Turkish and Vietnamese communities – within the north-western region of Melbourne. They were chosen with direct consultation with the Victorian Department of Health.
Citation preview
A Multicultural Perspective on Dementia: Case Studies and Community Perceptions in the North-western Region of Melbourne
A study conducted byAustralian Multicultural Community Services Inc. & the Migrant Resource Centre North West Inc. for the Department of Health, Victoria
Multicultural perspective publication.indd 1 17/05/2013 11:46:23 AM

This study was funded by the Victorian Department of Health, Home and Community Care Program. It was produced by Zeinab Husssein, Pramod Kumar Vinnakota and George Paris, with the assistance of Anthony Abate and Elizabeth Drozd.
First published in 2013 by:
Australian Multicultural Community Services Inc.Suite 111, 44-56 Hampstead RdMaidstone, Victoria, 3012 Phone: (03) 9689 9170Fax: (03) 9687 [email protected]. No. A0048140C
and
Migrant Resource Centre North West Inc. 45 Main Road, WestSt Albans, Vic. 3021 T: (03) 9367 6044 F: (03) 9367 4344 E: [email protected] W: www.mrcnorthwest.org.auInc. No. A0021391E
The authors, Zeinab Hussein and George Paris, may also be contacted at this address.
The final report was authored by George Paris of the Migrant Resource Centre North West Inc. Editing: Dianne Waite.
The opinions, comments and/or analysis expressed in this document are those of the author or authors and do not necessarily represent the views of the Department of Health, Victoria.
National Library of Australia Cataloguing in Publication data:ISBN: 97809803040-8-4
© This work is copyright and may not be reproduced by any process without the written permission from the publishers, except as permit-ted under the Copyright Act 1068
Multicultural perspective publication.indd 2 17/05/2013 11:46:24 AM

Acknowledgements
A special mention must be made of all members of the Croatian, Fili-pino, Indian, Iraqi, Lebanese, Macedonian, Polish, Sri Lankan, Turkish and Vietnamese communities who participated in the research. Many individuals voluntarily gave up a significant amount of time to share their personal experiences and insights. Without their contribution this study could not have been possible. We would also like to thank most sincerely all of the disability and aged care service providers who contributed their resources and advice during the course of this study.
Multicultural perspective publication.indd 3 17/05/2013 11:46:24 AM
4
Table of Contents
1. Introduction 5
1.1 Background 5
1.2 Study Aims and Objectives 5
1.3 Methodology 7
1.4 Limitations 8
1.5 Community Perspectives on Dementia 8
Croatian 8
Filipino 9
Indian 10
Iraqi 10
Lebanese 11
Macedonian 12
Polish 13
Sri Lankan 14
Turkish 14
Vietnamese 15
2. Case Studies from 10 Culturally Diverse Communities 16
2.1a. Croatian Case Study I 16
2.1b. Croatian Case Study II 17
2.2a. Filipino Case Study I 17
2.2b. Filipino Case Study II 18
2.3a. Indian Case Study I 19
2.3b. Indian Case Study II 20
2.4a. Iraqi Case Study I 21
2.4b. Iraqi Case Study II 22
2.5a. Lebanese Case Study I 23
2.5b. Lebanese Case Study II 24
2.6a. Macedonian Case Study I 25
2.6b. Macedonian Case Study II 26
2.7a. Polish Case Study I 27
2.7b. Polish Case Study II 28
2.8a. Sri Lankan Case Study I 29
2.8b. Sri Lankan Case Study II 30
2.9a. Turkish Case Study I 31
2.9b. Turkish Case Study II 32
2.10a. Vietnamese Case Study I 33
2.10b. Vietnamese Case Study II 34
3. Recommendations 35
4. Conclusion 37
5. Resource Directory 39
6. Appendix 1 – Community Group Questionnaire 41
7. Appendix 2 – Case Study Questionnaire 42
Multicultural perspective publication.indd 4 17/05/2013 11:46:24 AM
5
1. Introduction
1.1 Background
Towards the end of 2011 the Victorian State Government Department of Health held discussions with the Australian Multicultural Community Services (AMCS) and the Migrant Resource Centre North West (MRCNW) about working together to promote the rights and interests of people from culturally and linguistical-ly diverse (CALD) backgrounds. The discussions were guided by the Victorian Government’s Diversity Plan as well as principles within the Active Service Mod-el (ASM). These talks generated a variety of interesting possibilities for future studies and it was jointly agreed that the AMCS and MRCNW, through funding from the Department of Health, would complete a six-month study evaluating the prevalence and perceptions of dementia across 10 different community groups in the north-western region of Melbourne. The AMCS and MRCNW assembled a joint research team and held preliminary talks to scope and formalise the project. A project brief and a memorandum of understanding were prepared before the research team embarked on the collaborative project outlined below.
1.2 Study Aims and Objectives
The primary aim of this study is to accurately capture perceptions of dementia across 10 different cultural groups – the Croatian, Filipino, Indian, Iraqi, Leb-anese, Macedonian, Polish, Sri Lankan, Turkish and Vietnamese communities – within the north-western region of Melbourne. They were chosen with direct consultation with the Victorian Department of Health.
While some previous research had already been carried out with some of the cultural groups studied here, little information is currently available. This study seeks to add further evidence to the small amount of existing literature and re-search about CALD groups and dementia.We would welcome more research, not only in the area of dementia, but also more generally about multicultural communities and health.
Multicultural perspective publication.indd 5 17/05/2013 11:46:24 AM

6
• Multicultural Communities
We predict that different cultures will perceive dementia differently and that mul-ticultural communities will have varied perceptions about dementia. Some may have a sound awareness of many of the issues surrounding dementia, whereas other groups may require more information about what dementia is, what treat-ment and support services are available and the role and challenges of carers. We want to know what the different community perceptions are (if any), why they occur and what can be done to improve our overall knowledge of dementia.
Perception is not just about knowledge, it is also about attitudes, expectations and values, and we want to see how these frame a particular community’s overall perception of dementia. Historically we know that most cultures have in some way harshly stigmatised disability and, unfortunately, this is usually worse with con-ditions relating to mental health. For whatever reason, be it shame, guilt, embar-rassment or denial, many cultures have kept a tight lid on this topic. This has had a negative impact on patients, carers and families. A society that openly embraces and discusses the challenges of psychological health benefits everyone. Further-more, encouraging the sufferer to take control, or at the very least, to be involved in decisions about their own life also promotes better outcomes. Generally we have not promoted personal autonomy and independence for people with poor mental health. Many cultures have also not recognised the enormous difficulties that arise when caring for a chronically ill patient. Carers encounter monumental challenges (day and night), quite often with little or no respite or reward.This study investigated how different cultures perceive the role of the carer and each community’s awareness of the types of support available for carers. It also shows what communities think about counselling, residential care facilities, the role of the family and the influence faith plays.
• Case Studies – Carers
The secondary aim, and the bulk of this current study, was to capture the per-ceptions and experiences from a carer’s perspective. These have been recorded here in the form of case studies. As previously stated, the work of the carer is all too often forgotten and goes unrecognised. This study highlights the plight of carers, their challenges and triumphs in caring for a person with dementia. A total of 20 people (two from each community group mentioned above), each caring for a person with dementia, have been surveyed. We wanted to know their story, including the challenges of caring, coping strategies that may have made their life easier, and general insights about caring for a person with dementia. It is hoped that these 20 case studies will provide useful information, not only to organisa-tions and service providers but also to people in the wider community who may be caring for a loved one and seeking more information about how a person from a similar cultural background lived through the same experience.
• ResourceDirectory
A resource directory details the various support services available in the community.
Multicultural perspective publication.indd 6 17/05/2013 11:46:24 AM
7
1.3 Methodology
The research team was made up of three individuals – two from the MRCNW and one from AMCS. Each organisation focused on five different community groups. The MRCNW surveyed the Croatian, Iraqi, Lebanese, Sri Lankan and Turkish com-munities, and the AMCS surveyed the Filipino, Indian, Macedonian, Polish and Vietnamese communities.
We commenced by designing two separate questionnaires. The first was designed to capture the general community’s overall perceptions and awareness of demen-tia. The second was designed specifically for carers. Consent forms were given to each participant to sign. We explained that all information obtained was confiden-tial and anonymous and used only for the purpose of this study.
Community groups and culturally specific agencies were then contacted and in-formed about the current project. For those who agreed to take part in the study, a time and venue was agreed upon and the questionnaire distributed.The first questionnaire was administered by a member of the research team in a focus group setting such as a Planned Activity Group (PAG) venue, community centre or church hall, with the use of interpreters where necessary. Between seven and 42 people made up the focus groups. Some consultations were done outside ordinary hours as groups did not always meet during work hours. Completing the questionnaires was more difficult for some than for others, especially those with limited English literacy. For these people the responses were written down by the researcher or co-coordinator of the group.
For the case studies the questionnaires were usually completed in the family home. Again, interpreters were used if necessary. A total of 20 people, two from each community group, took part.All consultations with focus groups and case studies occurred between February and June 2012. A sample of both question-naires can be found in Appendix I.
Multicultural perspective publication.indd 7 17/05/2013 11:46:24 AM

8
1.4 Limitations
Undertaking a large study such as this has limitations. Finding 20 carers in a rela-tively short time who were willing to talk about their dementia-caring experience was, at times, challenging and required a great amount of networking and liaising with a wide range of contacts. Some of the communities evaluated here are rela-tively small in number, such as the Lebanese and Iraqi, and sourcing a dementia carer from those who were willing and able to share their story was sometimes difficult.
Another limitation that should be highlighted involves the nature of the groups. They varied in size and in the level of awareness of the issues surrounding de-mentia because some groups were well-informed PAGs, previously exposed to much information about dementia, whereas others were social groups with no focus on HACC services or wellbeing in general. For this reason we do not want to suggest that the perceptions expressed by people in these focus groups reflect or represent the opinions and perceptions of the wider community. This, however, does not undermine the validity of their claims. Indeed, their claims are equally valid and important. We wish to remind readers that the thoughts conveyed by the subjects in this study are purely those from a particular ethno-specific focus group and should be viewed as such.
1.5 Community Perspectives on Dementia
Croatian
The members of Croatian group surveyed in this study were all participants from a PAG for people more than 65 years old. The group was able to demonstrate a sound understanding of many of the issues about dementia, illustrating the effec-tiveness of PAGs in being able to deliver valuable relevant information to partici-pants who would otherwise miss out if they were not part of the group.
Like other groups, forgetfulness was a common symptom mentioned when de-scribing dementia, but people also defined dementia with reference to changes in a person’s behaviour and deterioration in the ability to recognise places, people and objects. Members of this group said dementia sufferers can sometimes be-come aggressive and reproachable towards other family members, wrongly ac-cusing them of misdemeanours.
Stress, poor mental health and social isolation were the three most commonly identified triggers for dementia. People said living a socially isolated life reduces communication with the external world, and this causes the brain to slow down and eventually enter into a ‘sleep-like state’. The group believed that being social-ly and physically active can improve brain activity and avert the onset of demen-tia. It should be highlighted though that social activity and community involvement was deemed to be very important in promoting overall wellbeing for this particular group, more so than physical activity.
Multicultural perspective publication.indd 8 17/05/2013 11:46:24 AM
9
The group thought their local doctor or other specialist health professionals were the best contacts to help people with dementia. It was thought that support for carers can be found with local community centres, PAG coordinators and appoint-ed case managers. However, while this kind of help may be available for carers, the group recognised that caring is a very demanding job and caring for someone with dementia is likely to be highly stressful. This stress not only results from the heavy physical strain and the psychological burden associated with caring but also because the primary carer needs to make difficult decisions which can often conflict with the opinions of other family members. For example, a family disput-ing the decision about when the person with dementia should move into a nursing home. The group believed that carers should access counselling to help them deal with such issues. Also, talking to other people in the wider community about the general challenges of caring was believed to be beneficial in alleviating some of the stress.
This group heralded the good support they continue to receive from their cultural-ly specific community service provider. Here the group is able to get information about dementia in Croatian through staff, DVDs and information sessions deliv-ered by guest speakers from organisations such as Alzheimer’s Australia and Carers Victoria. Consequently, this group feels they are better informed about dementia. Before joining the group, people said they had little knowledge about the condition and even thought it was something that should not be talked about openly and should be hidden from society. The PAG has helped demystify demen-tia for participants and now they claim to feel more comfortable talking about the subject and are more aware of the issues.
Filipino
Dementia within the Filipino community we spoke to is mainly understood as for-getfulness or memory loss acquired by ageing or excessive worrying. Members of this community recognise that a good diet and a positive attitude or outlook to life can reduce the risk of acquiring dementia. Community organisations, govern-ment services and doctors were all highlighted as viable places where carers and people with dementia can get support. In addition, people identified Western med-icine practices as the best option for treatment; in particular, prescription medica-tions, dietary supplements and counselling.
Residential care is perceived to be an inappropriate option because of the lack of privacy and freedom and a poor level of care. Nevertheless, it was conceded that residential care would be accessed for people in their later stages of dementia when it became impossible for family members to provide in-home support.The role of the family in providing care is seen as being extremely significant, and religion also plays a very large role in supporting and comforting people. Some people even believe that having strong faith can help with the treatment of dementia.
Multicultural perspective publication.indd 9 17/05/2013 11:46:24 AM
10
Indian
Of the members of the Indian community surveyed, most described dementia in terms of memory loss and forgetfulness. When asked why people get dementia, responses were varied; however, all were fairly accurate in attributing its onset to poor diet, ageing and stress, with ageing being the risk factor. While spirituality is pertinent in framing the community’s general perceptions about dementia, it was pointed out that there is no connection between lack of faith and dementia. Spir-itual belief offers a sense of meaning and moral duty when caring for someone frail and ill, and provides comfort and emotional strength to help cope with the issues and challenges of dementia.
As far as help is concerned, this group welcomed the use of Western medicine; in particular, general practitioners and physiotherapists. However, traditional reme-dies such as yoga, herbal medicines and breathing exercises were mentioned as important and preferred treatments for dementia.
A good awareness of support for carers was identified, with mention of local com-munity services and social support groups.
Iraqi
The group surveyed was an Iraqi men’s social group that met weekly in the north-ern region of Melbourne and offered a diverse range of responses to many of the questions asked. There was consensus in the group’s description of dementia, defining it as an illness or disease which causes memory loss and forgetfulness. More specifically, some people thought dementia causes short-term memory loss, while others thought it causes long-term memory loss and one person stated that memory loss is intermittent with dementia.
Generally people thought ageing was the main cause of dementia. Some people said stress and anxiety can be contributing factors, and a few disclosed they sim-ply did not know why people get dementia.
When asked about preventative measures, the group responded with different views such as the importance of an active physical and social lifestyle, reading, proper diet, good mental health and plenty of rest. Again, some people in the group could not identify any strategies that could reduce the onset of dementia.
Almost everyone in this group entrusts their local family doctor as the best option for dementia support. Some suggested the government as a good source of assis-tance but did not elaborate. People had different ideas about accessing informa-tion about dementia in Arabic, including Iraqi or Arabic-speaking welfare organi-sations, migrant resource centres, the internet, books, and Allied Health services. A small number did not know where they could find any information in Arabic. The group identified poor English skill levels as a barrier in accessing services. Some people remarked that Australia provides excellent welfare services overall and, while there may be difficulties in accessing this support, they are miniscule com-pared to other countries.
Multicultural perspective publication.indd 10 17/05/2013 11:46:24 AM
11
Many said it is not uncommon for people in their community to think people with dementia are ‘crazy’. Some even believe that dementia is a curse while others said these issues are hidden from public view. However, others thought of de-mentia as a medical condition that can affect anyone. There was widespread acknowledgment that the family plays a pivotal role in supporting the person with dementia. Many said the family should be patient, kind and understanding and should treat them with the same affection and care they would show when caring for a child.
The question of religion sparked divergent views. Some people rejected the influ-ence spirituality can have on their understanding of dementia while others said it provided comfort, meaning and motivation to help.
Lebanese
The group comprised women who demonstrated a reduced level of awareness about dementia. They defined dementia as a mental-health illness similar to de-pression that people can acquire when living isolated and lonely lives. The group thought leading a physically active life can prevent the onset of dementia and some mentioned the benefits of fresh air and travelling overseas as effective pre-ventative measures, but could not identify any treatments.
The family doctor is seen as the first and only place that assists people with de-mentia and their families. People could not suggest any other organisation that provides support. Obtaining information in Arabic about dementia or any other health issue is obtained through an Arabic-speaking family doctor. Unfortunately, there are not a large number of doctors who speak Arabic in Melbourne, so many people travel long distances to access one. The language barrier appears to be a major concern for this community group whose low level of English makes it difficult for them seek and access help. During the focus group, people started discussing how they sometimes felt belittled and insulted because health pro-fessionals would talk to their children instead of to them, assuming they cannot speak any English at all.
The group seemed open to counselling, particularly for carers, and thought it would only be beneficial if the person has the capacity to engage. They thought residential care units are not a good option, but would respect any family’s deci-sion if they chose to access such a facility. But if the family can no longer cope, the group could not see any sense in keeping the person at home.
The group said the Lebanese community’s general attitude about dementia may include some negative stereotyping. Some would think of dementia as ‘the per-son has lost their mind’. This negative stigmatisation can have unfortunate reper-cussions on the family in that they may choose to shelter or hide the person with dementia from the rest of the community.
Multicultural perspective publication.indd 11 17/05/2013 11:46:24 AM
12
Macedonian
The people from a Macedonian background who took part in this study were all members of a senior citizens club in the outer-western region of Melbourne. Most defined dementia simply as forgetfulness and attributed its onset predominantly to ageing, with some also identifying mental health and stress as potential causes of dementia. Comments surrounding poor mental health were sometimes tinged with negative, even pejorative, connotations. People thought an active lifestyle, including regular social interaction and sufficient exercise and relaxation, were key factors that can reduce the onset of dementia. They also suggested their local doctor, psychiatrist and other family members as good support for people with dementia.
For carers, people thought social groups are extremely important in providing a sense of comfort and belonging, as well as an opportunity to socialise. Local doc-tors and telephone help lines were also mentioned. However, people did not know where to find information in their own language; consequently, they would seek information from others in the Macedonian community or from a welfare centre or a Macedonian-speaking health professional.
Health professionals and Western medical intervention were highly regarded in the treatment of dementia by this group, and they also seemed to have a good awareness about supplementary treatments through Allied Health services. It was also acknowledged that a personal commitment towards an active social life and a reduction of stress levels can help in the treatment of dementia. Furthermore, counselling is generally regarded positively in the community in helping both car-ers and people with dementia to cope better with any associated psychological impact.
There is a strong opinion that family members should care for family members with dementia in their own home and consider the option of nursing homes only as a last resort. A close-knit family is thought to be better able to support the per-son with dementia. The role of the daughter was highlighted as extremely import-ant in taking charge of caring responsibilities and household tasks.
Multicultural perspective publication.indd 12 17/05/2013 11:46:24 AM

13
Polish
The Polish community members who took part in this study were regular par-ticipants in a Polish-speaking PAG in the north-western region of Melbourne. The group commonly understood dementia symptomatically, mainly defining it as memory loss and forgetfulness. Some people also identified confusion and a general deterioration of cognitive abilities as symptoms thought to be caused by ageing, loneliness, depression and genetic defects. Keeping the body and brain active through activities like regular socialising, reading, physical exercise, healthy eating and regular health checks were all mentioned as important strate-gies for prevention. There were numerous options mentioned where people with dementia can get help, including their local doctor, psychiatrist, specialist clinics, language-specific PAGs and community organisations. Conversely, an awareness of support for carers seemed vague, and people imagined that carers could get help through dementia clinics, community organisations, books and pamphlets. However, when asked about the likely challenges a carer may encounter, people surprisingly gave very descriptive accounts of the ongoing daily challenges a dementia-carer can endure, such as aggressive behaviour, communication diffi-culties and other difficulties with associated psychological illnesses.
Insofar as obtaining information about dementia in Polish, the group said they would usually contact Polish-specific community organisations, Polish-speaking doctors or other people within their Polish community. Some people mentioned that they did not know where to go to find translated information.
In discussions about the treatment of dementia, people identified Western medi-cine as paramount. Counselling was also positively endorsed for both the person with dementia and their carers. Mostly, people said the language barrier causes them the greatest concern. It is difficult for people to communicate with health professionals who do not speak the same language, and often information is lost and not understood. People in this group also perceived a general lack of informa-tion available in the wider community about dementia.
Accessing residential care appears to be dependent upon the health of the indi-vidual with dementia. If the family is living with a person in their later stages of the illness and can no longer cope, then residential care must be taken into consider-ation; however, the exorbitant costs can sometimes make this option impossible for some families. The community’s overall perception of dementia was one of acceptance. That is, people with dementia should be embraced into the community and not be isolated or treated differently. The community also believes that it is important to support one another as this helps alleviate an individual’s personal stress and difficulty.The Polish community is generally very religious, with the majority espousing a Catholic faith, and this played a major role in framing an individual’s attitudes about dementia. Within this group there was a strong belief in miracles and, with that, a sense that divine intervention can turn things around for someone with de-mentia at any time. Notions such as sympathy, acceptance, altruism and solidarity all seem to derive from the community’s faith and strongly influence the communi-ty’s attitudes and actions.
Multicultural perspective publication.indd 13 17/05/2013 11:46:24 AM
14
Sri Lankan
The Sri Lankan community members who contributed to this survey were a mix of PAG participants and social-support-group attendees who meet on a weekly basis in the north-western region of Melbourne. Most people in this group common-ly understood dementia simply as an illness that manifests in memory loss. The causes of dementia could generally not be identified and only a few people iden-tified ageing as a likely cause. Some acknowledged that a physically and mentally active lifestyle can reduce the risk of acquiring dementia, but the majority was not aware of any protective factors.
The community did not appear to have an understanding of any treatment avail-able for dementia and said they would seek advice from their family doctor. Mem-bers of the community could only highlight Commonwealth income streams as the one support available for carers. When asked whether counselling is useful for carers, most agreed and went further to say that counselling was valuable for any mental-health issue.
Knowledge of where to access information about dementia was limited. There was some mention of information being available through local councils and one person mentioned Beyond Blue as a potential source of information. As well peo-ple were not aware of information being available in their own language.
There appears to be differing attitudes towards residential care, with many peo-ple strongly opposed to this concept while others seem to have no problem with it. The same applies to the role of spirituality. For some it helps them to make sense of the world while others made no connection between religion and dementia.
Turkish
The people surveyed in this community group belong to a senior citizens group in the western region of Melbourne that meets on a weekly basis.
The group expressed a vague understanding of dementia, generally thinking it to be a type of sickness that affects memory. Some members of the Turkish commu-nity also identified other symptoms such as repetitious behaviour, problems with speech and an inability to communicate. Age, social isolation, grieving, poor diet and stress were mentioned as likely causes and, in some instances, people be-lieved that dementia can occur to anyone simply because it is a natural part of the ageing process. Overall there were different levels of understanding about the na-ture of dementia across the community, with some claiming to have a solid aware-ness of the condition while others admitted to knowing very little. The majority of the group believed that social participation, an active lifestyle, good diet and regular mental exercises are effective ways to prevent dementia. People identified their local doctor as the best place to seek help and advice.
Multicultural perspective publication.indd 14 17/05/2013 11:46:24 AM
15
Attitudes towards dementia patients and their carers is one of deep sympathy, but very little awareness exists of the support services available for carers. This knowledge seems to be limited to Centrelink payments, with no mention of ser-vices such as respite, counselling or carer-support organisations, Allied Health services, HACC services and so forth.
Centrelink and local doctors also seem to be the most likely places that this com-munity would visit to obtain more information about dementia. There was little mention of Alzheimer’s Australia and people did not know where to access in-formation in their own language. The lack of available information in Turkish was commonly identified as a major difficultly for the community when seeking help.
As far as treatment is concerned, there seemed to be some awareness that med-ication can be helpful, but most people did not know what treatments were avail-able. The local doctor was the person most entrusted to give advice about treat-ment. Counselling was never initially identified as useful for dementia patients and their carers, but when prompted, people had no hesitation in remarking on the benefits. Residential care is a last resort, with families much preferring the person to remain at home as long as possible. Religion did not frame many peo-ple’s thoughts about dementia. Some commented on the benefits of prayer, but in general, religion is seen as something separate to medical conditions.
Vietnamese
The Vietnamese people who took part in this study were all active members of a seniors group that meets weekly in the inner-west region of Melbourne. Most peo-ple defined dementia with reference to obvious symptoms like memory loss and forgetfulness. Poor health and worrying were offered as probable causes by some members, but most stated they did not know what causes dementia. An active lifestyle was thought to protect people from dementia; in particular, social outings with friends as well as activities such as reading, mental exercises and studying. Very few surveyed were aware of any support where people with dementia and their families could get help. Furthermore, people did not know where to access information about dementia and what treatments were available. Counselling was also not understood as an effective tool in supporting people with dementia or their carers. People could not identify any of the challenges that carers are likely to face, but they imagined that caring for someone who repeatedly forgets things must be very demanding and tiring. Support for carers, such as respite and coun-selling, was not identified.
The Vietnamese community has very strong opinions about residential care. Fami-lies will try to do everything possible to keep the person in the family home as long as possible, and will only use the option of residential care in extreme cases.
The community’s overall attitude about dementia is positive. People regularly mentioned that everyone deserves to be respected and accepted, regardless of their situation. Community solidarity was also frequently identified as important when thinking about supporting people with dementia and their families. Spiritual belief does not seem to play a major role in the community’s attitudes to demetia.
Multicultural perspective publication.indd 15 17/05/2013 11:46:24 AM

16
2. Case Studies from 10 Culturally Diverse Communities
2.1a. Croatian Case Study I
“Vladko” is 84 and until recently was the primary carer for his wife who is 82 years old. They have four children who no longer live in the family home. Vladko’s wife has been living with dementia for nine years and he was the sole carer during this time; however, he has received a lot of support from his family. Vladko’s wife’s condition recently worsened, and the family made the difficult decision for her to move into permanent residential care as his ability to provide the necessary level of care decreased significantly.
When Vladko’s wife was living at home, the family did not access many HACC ser-vices. They felt they were quite capable of providing better care in the home than that provided by external services. Vladko said he currently receives four hours of home help every fortnight from the local council.
The most difficult thing that Vladko experienced while caring for his wife was witnessing the gradual decline in her ability to recognise family members. Vladko visits his wife every day and assists with feeding and tries to spend as much time as he can with her during the day. He commented on the importance of being pa-tient and spending as much time as possible someone with dementia. He believes both of these strategies have helped him provide better care for his wife. Recently a Croatian-speaking volunteer has started visiting his wife once a week to provide some social support and Vladko feels this has been very positive.
Vladko regularly attends a Croatian-speaking PAG with the Australian Croatian Community Services. He says this provides him with links to other people from his community and practical information about health and general wellbeing. Vlad-ko spoke highly of staff from this organisation and said they had made referrals, booked appointments and given him a lot of information about dementia. Vladko also commented that his local doctor had been extremely supportive.
Vladko said he has grown to be more compassionate and is a lot more understand-ing, not only about issues relating to dementia but also in his outlook on life and relationships.
Multicultural perspective publication.indd 16 17/05/2013 11:46:24 AM

17
2.1b. Croatian Case Study II
“Fay” is 76 and visits and cares for an 84-year-old family friend currently living in a residential care unit in the outer north-western region of Melbourne. Fay has been providing this support for the last four years.
She said her friend has no family in Australia and few friends of her own. Her husband died after they were married for only two years; they had no children and she chose not to remarry.
Fay began to notice changes in her friend’s behaviour and detected she was be-coming easily confused and disoriented. She also started to swear and become abusive, which was highly uncharacteristic, and would later be ashamed and tear-fully apologise for behaving this way. Fay found this change in her friend’s per-sonality extremely difficult to cope with and thought she was losing a very close friend. She claimed her belief in God and active prayer allowed her to manage this change better.
Fay completed an Alzheimer’s Australia workshop designed specifically for volun-teers who are working with people with dementia and found this to be highly valu-able. She said her knowledge of dementia significantly increased and she was able to help her friend in a more meaningful way.
Fay said she believes that love and family support are vital to protect people from getting dementia. For Fay a life of continual social isolation is a major risk factor for dementia and her friend is an unfortunate example that points to this supposi-tion.
2.2a. Filipino Case Study I
“Mary” is 25 years old and cares for her grandmother who is currently receiving a few hours of respite support each week from her local council. Mary finds this extremely valuable as it gives her a much-needed break from her caring responsi-bilities.
Prior to her grandmother’s diagnosis, Mary had no knowledge of dementia. However, once she commenced caring, she underwent a radical change as she witnessed the effects of dementia first-hand. Mary said she struggled initially to come to terms with her grandmother’s ‘strange’ behaviour. She felt her grand-mother was becoming a different person and this worried her enormously. Mary enrolled in an aged care/disability education course to help deal with this change. This increased her knowledge of the aged and disability service sector as well as her knowledge of dementia. More importantly, upon completion of this course, Mary gained a greater awareness and confidence in caring for her grand-mother and highly recommended similar courses for other carers.Mary’s overall perception about health services for her grandmother is general-ly very good and she could not suggest any way things could be improved. Her opinions about residential services are that she would only like her grandmother to consider this option when Mary is away for more than two consecutive days.
Multicultural perspective publication.indd 17 17/05/2013 11:46:24 AM
18
2.2b. Filipino Case Study II
“Ellie” is 37 and is caring for her grandmother. She expressed a deep affection for her grandmother but found caring for her to be highly stressful and difficult.
One of the most demanding things she had to cope with was her grandmother’s constant mood swings, which made it almost impossible for Ellie to plan and or-ganise her day and to implement a routine. She also mentioned the difficulties in communicating. Having to explain things repeatedly was frustrating and often she did not know whether her grandmother comprehended anything she said.
Friends have been a great support to Ellie and doctors were valuable in provid-ing her with general information about dementia and making referrals. Support through Allied Health services and other service providers was also very positive. Ellie also completed a Certificate III in Aged Care to gain a deeper understanding of dementia so she could be better equipped to care for her grandmother. She said this was very useful and empowering.
Ellie said her grandmother accessed a variety of support services through wel-fare organisations including Allied Health services, HACC services and aged care services; however, she imagined that it might be difficult for people who require interpreters as much of the information discussed from various service providers can be technically complex.
She said her family is extremely close and enjoy caring. They would feel they were abandoning their grandmother if she went to a residential care unit, which should only be a last resort. The home help support of 3.5 hours per week delivers an excellent service that improves her mother’s quality of life in her own home.
Ellie said it is important for carers to be compassionate, patient and understand-ing. She also recommended education in aged care for carers. Ellie praised and promoted the services of Carers Victoria and Alzheimer’s Australia. She feels there are not enough respite and counselling services made available to families.
Multicultural perspective publication.indd 18 17/05/2013 11:46:24 AM

19
2.3a. Indian Case Study I
“Dilraj” is 51 and has cared for his father for several years. When his father was first diagnosed with dementia, Dilraj recalled that the family received very little support from service providers and family members. As a result he felt stressed with the volume of work and responsibility required to care for his father alone. The family did not seek any support through services such HACC, claiming that this was a foreign concept.
Dilraj said his father’s short-term memory loss caused serious problems with caring as he would often forget things such as basic instructions, events and activities already performed during the day. Dilraj remarked that, with constant repetition and reminders, his father’s performance of ordinary daily tasks and recollection of events improved. He also said he found communicating with his father more effective when he framed his dialogue in the form of a story. Speaking in this descriptive narrative seemed to improve his ability to perform tasks inde-pendently and recollect important events. But as his father’s condition worsened, Dilraj found it increasingly difficult to cope on his own. The family eventually made the decision for Dilraj’s mother to withdraw from her education studies so she could focus on caring for him full-time.
Dilraj believes more information about dementia would have made his experience easier. He said there are not enough resources or information, particularly for carers. However, Dilraj said he has no difficulty engaging with health care provid-ers and has always found them approachable.
Residential services are not feasible because it is too expensive. Furthermore, Dil-raj believes the quality of care provided in these facilities can never approximate that provided by family members in the home. His father’s difficulty with English makes this decision even more unpalatable.
Multicultural perspective publication.indd 19 17/05/2013 11:46:24 AM
20
2.3b. Indian Case Study II
“Harmeet” is 45 and cares for her mother. During the initial stages of her mother’s dementia, the entire family received good emotional support. A nurse would fre-quently visit, as well as a physiotherapist and a social worker.
Harmeet said the biggest challenge she faced when first caring for her mother was coming to terms with the daily tasks, which she found physically demanding and emotionally draining. Her mother has significantly reduced mobility, and for Harmeet, heavy physical handling has caused muscular problems.
Harmeet remarked on the difficulties of communicating with her mother whose skills in this area have deteriorated. By trying to anticipate her mother’s needs, Harmeet said she can plan the day and be better organised. She also mentioned the importance of non-verbal communication. Being able to read her mother’s body language and facial expressions is very useful. Modifications to her moth-er’s diet and monitoring her sugar levels, as recommended by a nutritionist, have helped to prevent further complications and her mother’s mood has improved.
Harmeet said she is still very happy with the overall support she and her mother received from different health services. She believes good support structures exist but would like to see families given a greater say in the referral process from the hospital. Harmeet voiced her concerns about the long waiting periods for a range of support services. The family has chosen not to receive personal care and domestic assistance through HACC services for a variety of reasons, includ-ing cultural ones. The family is not accustomed to having strangers assisting with domestic and caring responsibilities. They see this as their own responsibility and believe their mother’s restricted communication and mobility would complicate things further.
Harmeet said looking after her mother has given her an insight into the symptoms of dementia and the daily challenges carers endure. She found her own research into dementia extremely valuable and it gave her a better understanding of her mother’s condition. She would like to see better education programs made avail-able, in particular to immediate family members, but also the wider community. Harmeet also believes that dementia-screening tests should be made mandatory at a certain age.
Multicultural perspective publication.indd 20 17/05/2013 11:46:25 AM
21
2.4a. Iraqi Case Study I
“Sabeen” is 57 and cares for her mother-in-law who is 84 years old. Sabeen’s family began to notice worrying signs with her mother-in-law’s behaviour before she was diagnosed in 2001. She would accuse Sabeen of stealing her clothes and giving them to her extended family. In time her behaviour worsened. She stopped listening and following instructions and would suddenly storm out into the street. On one occasion she was almost hit by a passing vehicle. She would also eat tis-sues, wash her hands inside the toilet and play with her own excrement.
Sabeen said she attended information sessions and a dementia forum held by an Arabic welfare organisation. These provided her with some basic yet important ideas about dementia and how to deal with different situations. Now she tries to calm her mother-in-law when she becomes aggressive and often agrees with her to avoid further upsets.
The family call upon an occasional respite service only on special occasions like weddings and funerals. They have also installed a manoeuvrable barrier near the toilet to prevent Sabeen’s mother-in-law engaging in inappropriate behaviour.
Sabeen said she would like more support, especially respite, so she can have more time to herself. When asked about occasional or permanent residential care, Sabeen said the family would be highly unlikely to consider this option, particular-ly after their first trial when her mother-in-law lived in a residential care facility for three months and the family quickly noticed her health deteriorate. Sabeen said her mother-in-law appeared heavily sedated and stopped eating, speaking and moving. The family then decided to bring her home and vowed never to return to a similar facility.
Sabeen summarised by saying that she would like more respite in the family home so she can have time to run essential household errands. She also commented that she had learnt a lot more about dementia by closely caring for someone with the condition.
Multicultural perspective publication.indd 21 17/05/2013 11:46:25 AM
22
2.4b. Iraqi Case Study II
“Leyla” is 43 and cares for her sister who is 61 years old. Leyla lives in her own home with her daughter and her sister sleeps over several times a week.
Leyla said her sister was originally diagnosed with dementia in 2009 in Syria. She explained that her sister’s son was killed in 2006 in the Iraq War and this, she feels, triggered the onset of dementia. The family arrived in Australia in early 2010 and received counselling support from a service that helps survivors of torture and trauma.
Leyla pointed out that her sister’s behaviour has radically changed and she seems to be an entirely different person. She had become very confused, disorganised and messy. Leyla felt hurt to see her sister in this state and said she coped by talking to people in her community and gained strength through her religious be-liefs.
Leyla encouraged her sister to engage an English tutor, believing that if she kept her mind busy then her sister’s health was less likely to deteriorate. The tutor was provided by the same service that helps survivors of torture and trauma and pro-vides home tutorials. This organisation also provided valuable and practical infor-mation sessions about dementia for all the family.
Leyla linked in with an Arabic-specific support service that organises excursions and camps for families, among other things, which were very well received by the family as their only form of social activity.
Leyla explained she has health problems herself, including a hearing impairment that requires surgery and she suffers from severe back pain. While that impacts on her ability to provide adequate care, she says she is more than happy to contin-ue helping as much as she can.
Leyla recently toured a residential care unit and her impressions became more favourable. However, the family would still only consider this option as a last re-sort. Leyla said if her own health continued to decline, then she would consider residential care for her sister.
The family presently receive no HACC services. Leyla would certainly like to ac-cess respite and is interested in home help. She finished by saying she was under enormous pressure and needs more help to care for her sister.
Multicultural perspective publication.indd 22 17/05/2013 11:46:25 AM
23
2.5a. Lebanese Case Study I
“Mariam” is 19 and is the primary carer for her mother who is 38 years old. Her mother was diagnosed with vascular dementia in 2010 after suffering a stroke. Mariam lives at home with her mother and father and six siblings. She is the sec-ond-eldest child.
Mariam began by describing some of the strange behavioural changes her mother started to display, like wandering aimlessly around the house, excessive eating habits and chain-smoking. They would find her mother often asking neighbours for extra cigarettes when she would run out. Mariam also mentioned that her mother expresses child-like behaviours and frequently becomes aggressive for no appar-ent reason. At night they have often found her attempting to go outside and on one occasion Mariam stated they discovered that her mother had cut off all of her youngest daughter’s hair. Before being diagnosed, Mariam’s mother was a re-served and quiet person and would never engage in these behaviours.
While these behavioural changes have caused frustration within the family, shar-ing some of the caring duties has helped. During the day, Mariam’s father also tries to assist with as much of the responsibilities as possible. Mariam has had to stop her TAFE course to concentrate on supporting her mother. While this has stalled her career development, it has been necessary to provide her mother with quality support in the family home.
Mariam said carers need to be patient and simply to get on with it, despite the monumental challenges. Unfortunately, Mariam’s mother has rejected any support from HACC services such as home help and respite, making it more difficult for Mariam to focus on her own life.
Multicultural perspective publication.indd 23 17/05/2013 11:46:25 AM
24
2.5b. Lebanese Case Study II
“Greta” is 47 and cares for her mother-in-law who is 84 years old and recently diagnosed with dementia. Greta’s father also had dementia but is now deceased. This prior experience better equipped her to care for her mother-in-law. Greta has never received training or information about dementia except for a Lebanese health program broadcast on a multicultural radio station. Greta lives at home with her husband, mother-in-law and her three children.
Greta takes her mother-in-law to all her appointments and helps to remind her about taking her medication, but receives no recognition. Greta also said her mother-in-law has developed strange and confronting behaviours such as openly talking about sex. It is highly unusual for a woman from her cultural background and age to be unashamedly discussing these topics and, when this occurs, other people feel very awkward. Greta’s mother-in-law now distrusts others and only trusts Greta. The children are frustrated with their grandmother and do not ex-press the same level of sympathy and patience.
Greta claimed her mother-in-law is in denial about her dementia. Consequently, she often stubbornly refuses to take her medication and this usually leads to argu-ments. Complicating matters further is the fact that her mother-in-law has several other serious health concerns including diabetes, hypertension and recent knee surgery.
Greta remarked that she internalises a lot of the stress that comes with caring for an ill person and does not want to reveal her true feelings to her mother-in-law or the rest of her family. Taking some personal time-out whenever she can is import-ant for her own wellbeing and this is the only strategy she employs to help her cope. Currently the family receives no HACC services or other type of support, al-though Greta said she would like more help, such as respite, home help and coun-selling. The family is very reluctant about accessing residential care, particularly because that had been an unpleasant experience for Greta’s father.
Multicultural perspective publication.indd 24 17/05/2013 11:46:25 AM
25
2.6a. Macedonian Case Study I
“Suzie” is 52 and has cared for her mother, aged 82, who recently moved into a permanent residential care facility in the northern region of Melbourne. Suzie remarked she was more fortunate than other carers as she already had a profes-sional background in aged care and was able to draw upon this to support her mother.
When Suzie’s mother was initially diagnosed with dementia, the family was sup-ported by their local doctor. He gave them basic information about dementia and spoke about potential referrals. Suzie also commented that the financial support through Centrelink Carer Payment and Carer Allowance was extremely important as she had no other source of income after leaving work to care for her mother.
Throughout that period Suzie said one of hardest things was that her own priori-ties and social life were always of lesser importance than her mother’s interests. Often her mother’s unpredictable behaviour would interfere with her own plans. Suzie also found maintaining her mother’s personal hygiene, the daily bathing, toileting and dressing, both physically and emotionally stressful.
Suzie implemented different methods to make her role more manageable. She would take her mother on long drives and visit parks and gardens. These outings seemed to relax her mother and made her feel happy, leading to a decrease in anti-social behaviours.
Suzie’s experience with support services was generally good. She found the staff to be friendly and informative. She does not have a negative view of residential care. When deciding upon a facility for her mother, the family looked at a range of factors including the reputation of the facility, friendliness of staff, cleanliness and whether there were any Macedonian-speaking staff and/or residents. Suzie wished that she could still care for her mother, but her condition and financial constraints meant this was not possible. Previously Suzie’s mother received home help through her local council for two hours every fortnight.
Suzie said she could not blame her mother for some of her anti-social behaviour, such as her kleptomania because that is part of the condition. She also comment-ed on the importance of finding strategies that suit both the carer and the person with dementia.
Suzie overall feels she successfully fulfilled the role of primary carer to the best of her ability. She recommended carers should keep a close watch on their own wellbeing as they are likely to suffer some health setbacks if they are not vigilant.
Multicultural perspective publication.indd 25 17/05/2013 11:46:25 AM

26
2.6b. Macedonian Case Study II
“Anna” is 44 and has cared for her mother, who is 82, for approximately five years before she moved into residential care. Anna said when her mother was first diag-nosed with dementia the family could not afford the services available at the time. She acknowledged they did not have a great deal of information about dementia or know where to seek assistance.
Anna recalled that the most demanding aspect of caring for her mother was dealing with her aggressive behaviour. Often she would refuse to take her medica-tion, get dressed or attend appointments. Soon arguments would develop and this would escalate her mother’s agitation.
Anna resorted to using more effective methods of communication and became a lot more patient. If her mother became frustrated, Anna would try to distract her or change the subject temporarily and her mother would calm down. She said she still had to adopt a firm approach; otherwise, her mother would simply not fulfil daily tasks like feeding or taking her medication.
When asked about her mother’s experience in residential care, Anna was full of praise. She was impressed with the number of staff and the high quality of care. But she was disappointed with the treatment her mother received in hospital, say-ing staff lacked expertise in supporting dementia patients and the hospital was severely understaffed.
Prior to entering permanent residential care, Anna said the family did not receive any HACC services. The main reason for this was cultural as the family was not accustomed to strangers providing home help.
Anna said it is important to talk to people who can offer sound advice. Her disad-vantage was not having any prior knowledge of dementia and, although she tried to read up on the topic, it was better to talk to health professionals. Anna also mentioned the importance of financial planning. There are large costs involved in caring for a person with dementia and Centrelink payments are meagre. Anna admitted that she mistakenly did not access any support services and encour-aged others to access as many as possible; otherwise, the burden can threaten the carer’s own health.
Multicultural perspective publication.indd 26 17/05/2013 11:46:25 AM
27
2.7a. Polish Case Study I
“Tekla” is 50 and cares for her father who is aged 90. Tekla praised the financial support offered by Centrelink and the readily available information, in both En-glish and Polish, about dementia and various kinds of assistance. She mentioned the support received from specific Polish community services and said respite is a vital service that gives her a much-needed break.
One of Tekla’s daily challenges was dealing with aggressive behaviour. She said some of the personal-care work was very demanding and strenuous, and added that bathing and toileting can be stressful.
Tekla accessed counselling in the past to help her implement coping strategies and claims some were highly beneficial. She highlighted the importance of main-taining personal interests or having some respite and time to oneself. Tekla also believes that openly talking about her feelings as a carer to family, friends and her doctor has helped her cope better.
Accessing healthcare professionals has never been difficult for Tekla. In her expe-rience they have always been very supportive and she could not think of any way things could be improved.
Tekla said residential care would not be suitable for the person she is caring for as he is prone to accidents and personal injury. His frequent aggressive behaviour would make life difficult for everyone in the nursing home. However, Tekla would consider residential care as a last resort only after heavily scrutinising the merits of the facility, such as client/staff ratios and quality of care. Tekla said she has learned a lot about dementia since her family member was diagnosed. She firmly believes that each person with dementia should be treated on an individual basis and there is no universal approach. Tekla also said caring requires a lot of pa-tience, often the carer needs to explain things repeatedly and implement innova-tive strategies that work for all concerned.
Tekla believes it is important to engage the person with activities that stimulate brain activity and to use appropriate human touch and show emotional support and sympathy. Another useful technique is to try to anticipate and predict the pa-tient’s intentions.
Tekla highlighted the importance of encouraging the person with dementia to make as many decisions as possible and to help them find the reasons for their actions.
Multicultural perspective publication.indd 27 17/05/2013 11:46:25 AM
28
2.7b. Polish Case Study II
“Aleksandra ” is approximately 45 and has been caring for her mother, aged 86, for the last eight years. Aleksandra’s mother was diagnosed with vascular demen-tia in 2004.
Aleksandra highlighted the good support she received from a variety of organi-sations such as the Royal District Nursing Service, HACC services, Polish com-munity organisations and case management services. When her mother was first diagnosed, Aleksandra said she was not aware of the different support services available and did not receive much support. Later Aleksandra and her mother accessed more services and she became quite satisfied with them. Unfortunately, Aleksandra does not receive much help from other members of her family and this impacts on her own wellbeing and stress levels.
Aleksandra remarked she no longer has time to do things for herself, such as shopping or socialising, and is frustrated because she finds it almost impossible to communicate meaningfully with her mother. She says her mother is childlike and has great difficulty with speech, so she cannot engage in conversations.
Aleksandra was forced to leave work to care for her mother as other family mem-bers were reluctant to offer their support. She is the sole-carer and takes her mother to appointments with doctors, psychologists and other specialists. If she had continued working, Aleksandra’s mother would not have been cared for ap-propriately or have been able to remain in the family home.
Aleksandra believes residential nursing homes are understaffed and lack the time and patience required to support a person with dementia. She says people who live in these homes are usually unnecessarily heavily sedated. Only if her mother is in danger of harming herself or other people in the home, would she consider this option. A variety of HACC services has been accessed by Aleksandra’s moth-er in her home, and when Aleksandra was away for a few days, HACC provided increased support for her mother.
Aleksandra feels she now has a solid understanding of dementia. Her mother’s diagnosis motivated her to learn more about the condition. She believes the wider community has very little awareness of dementia and would like to see more edu-cation campaigns. She understands the need of family support groups and would like to see more made available. Aleksandra suggested that dementia education for families should be mandated once a loved one is diagnosed.
Multicultural perspective publication.indd 28 17/05/2013 11:46:25 AM

29
2.8a. Sri Lankan Case Study I
“Vithiya” is 67 and cares for her husband who is 75 years old. He was diagnosed with dementia five years ago. Eleven years ago he suffered a heart attack and, just before being diagnosed with dementia, he suffered a stroke. Vithiya’s daughter still lives in the family home and sometimes helps her mother with caring respon-sibilities.
Vithiya said feeding time causes her the most difficulty. She has to assist her hus-band to put food into his mouth and constantly remind him to finish his food. He also needs to be reminded about many other things throughout the day.
Every Thursday morning Vithiya’s husband is collected by an attendant carer and transported to a local respite facility, where he spends half the day. This gives Vithiya almost four hours to do things for herself. While respite is an excellent re-source, it is only very brief, so Vithiya has had to rely on other mechanisms to help her cope. Every second Saturday Vithiya visits her local temple of worship and has also joined a Sinhalese social group where she is the secretary. She says this gives her an outlet and an opportunity to focus on something else. Participating in these additional activities, however, means she is extremely busy and terribly tired. She acknowledges the activities would not be possible if her daughter was not available to act as the secondary carer.
When seeking professional advice about her husband, Vithiya always contacts her family doctor. She also said through her local council they receive fortnightly home help and a maintenance man comes every month to mow the lawns. Vithiya is very satisfied with these services and could not think of any way in which HACC services could be improved for her or her husband.
When asked about residential care, Vithiya said certainly she would consider this option, providing it was financially viable. Currently the family is heavily burdened with bills and mortgage repayments and could not afford residential care.
Multicultural perspective publication.indd 29 17/05/2013 11:46:25 AM
30
2.8b. Sri Lankan Case Study II
“Hirruni” is 63 and cares for her mother who is 94 years old. Hirruni lives at home with her husband and mother. Her mother was diagnosed by their family doctor approximately five years ago. Since then her condition has significantly deteriorat-ed after having a stoke three months ago. Hirruni said she noticed major changes and it was difficult to know if these were attributable to stroke or dementia. Hir-runi’s mother now requires a lot of support to walk independently. Her speech has become incoherent and her memory skills have declined sharply. She is fright-ened of the dark and wants the light left on during the night and she wanders around the house.
The local council provides 4.5 hours of respite every week, giving Hirruni a well-earned break, albeit brief. Occasionally Hirruni’s close friend looks after her mother when Hirruni needs to step out, so does her husband, who always offers his support. Hirruni said she used to enjoy going to her local Buddhist temple with her mother where a nurse was available to help if necessary, but since the stroke her mother is entirely housebound and Hirruni needs to stay at home with her. This has caused Hirruni a considerable amount of distress as she cannot imagine herself being able to cope without more time to herself. She has real fears of suf-fering a mental illness if this situation continues and is desperate for more respite hours.
Recently Hirruni’s mother experienced two weeks of respite care in a residential care unit. The family decided against further residential respite because Hirruni felt she was abandoning her mother. Also, Hirruni imagined her mother would be lonely in the residential unit or even come to resent her for making the decision. If Hirruni’s mother’s condition changes, the family may reconsider this option.
Hirruni lamented the fact that there is no known cure for dementia. She is deeply saddened to see her mother suffering and is frustrated that she cannot do much to improve her health.
Multicultural perspective publication.indd 30 17/05/2013 11:46:25 AM
31
2.9a. Turkish Case Study I
“Bahar” is 78 and is caring for her husband who is 83 year old. He was diagnosed with dementia eight years ago. Bahar said her husband would perform many du-ties around the house, but since his condition worsened, he has become incapa-ble of doing many of these chores. This forced Bahar to learn new skills such as driving, gardening and basic maintenance.
Bahar said her husband was first diagnosed with dementia by their family doctor after the family started to notice changes in his behaviour. After the diagnosis, her husband applied for and received a Community Aged Care Package with the as-sistance of a community migrant-service provider which offered a range of sup-port which Bahar was pleased about.
Having recently started receiving counselling herself, Bahar said she would have needed it sooner had it not been for the good support of family and friends. This service provides an invaluable opportunity to talk to someone privately about her difficulties. However, in the beginning, she was reluctant to access counselling as well as other service support. Although doctor encouraged her initially, she re-fused, mainly due to cultural reasons. Bahar said in her culture there is the expec-tation that family members, especially the wife, looks after those who are unwell; seeking external support can be considered shameful. But as her husband’s con-dition declined, Bahar was forced to look beyond these cultural constraints and accept outside help. She lamented how difficult the last decade has been, dealing with the emotional and psychological impact.
Bahar’s opinion about residential care was very firm. She said she has been mar-ried for 48 years and cannot conceive living apart now. HACC services have cer-tainly played a major role in improving her husband’s quality of life at home.
Bahar said her awareness of dementia has grown significantly. Before her hus-band’s diagnosis, Bahar and the rest of her family knew very little about the con-dition. Now she knows it is an illness and not merely something people get when they age.
Multicultural perspective publication.indd 31 17/05/2013 11:46:25 AM
32
2.9b. Turkish Case Study II
Najat is 54 and cares for her father who is 92 and has recently been diagnosed with dementia. Najat lives with her father and gets caring assistance from her three sisters. When her father was first diagnosed, Najat received no support as a carer. She had no engagement with support services, other than her family doc-tor, and knew very little about the different types of support available.
When describing the challenges faced in caring for her father, Najat made repeat-ed reference to his forgetfulness and memory loss. She is frustrated that she has to constantly remind him about appointments and where he placed his belong-ings, when to eat meals and so forth.
Najat wished there was more information available about how to best care for a person with dementia. She wants to learn more so she can improve the way she cares for her father.
Currently the family does not receive any external support such as HACC ser-vices, mainly because Najat’s father has four daughters who all help him in a vari-ety of ways such as cooking, cleaning, shopping and any personal care he cannot manage for himself. For the same reason, Najat’s father has not considered res-idential care and is unlikely to in the future. A strong family support network will ensure Najat’s father never needs to leave the family home.
Najat said she has very little knowledge about dementia as her father has only recently been diagnosed. In time she feels she will begin to understand the con-dition a lot more. She would, however, like to see her Turkish social club deliver information sessions about dementia and thinks this is a good way for her to learn.
Multicultural perspective publication.indd 32 17/05/2013 11:46:25 AM
33
2.10a. Vietnamese Case Study I
“Khoa” is 45 and until recently cared his father who is 79 years old. Khoa’s father has suffered from dementia for approximately five years and now lives in perma-nent residential care. Khoa has returned to full-time work.
Khoa mentioned he found Centrelink Carer Payment and Carer Allowance import-ant financial support and it would have been impossible for him to care for his father without these supplements.
Khoa knew very little about dementia initially and this made his experience of car-ing for his father a lot more stressful. After gaining experience as a care provider, Khoa said people with dementia should not be questioned or challenged; instead, carers ought to accept the person’s behaviour as a symptom of the disease and to try and work around it.
Khoa found maintaining a written record of important daily events concerning his father to be very useful, especially when talking to health professionals. This helped him understanding dementia better and led to positive changes in his fa-ther’s health care, such as trying different medications and treatments.Khoa believes people with dementia should be encouraged to pursue hobbies and to remain as physically and socially active as possible. He tries to spend a lot of quality time with his father and frequently takes him out to Vietnamese restau-rants, as this was something his father enjoyed.
Khoa was critical of his experiences with health professionals. He found waiting times too long. He also suggested that health professionals do not spend enough time counselling their patients and families about dementia. He would like to see a checklist of symptoms developed and made available to families to help them detect dementia early on.
Khoa’s father’s condition had declined and the family could no longer care for him at home. While this was not an easy decision, the family, including Khoa’s father, seem very satisfied with this arrangement. Unfortunately, Khoa was not aware of HACC services while his father was living at home so the family never accessed any HACC assistance at all.
Khoa expressed the importance for carers to look after their own wellbeing. He said family support is paramount, but when the person’s condition declines, resi-dential services can be sought to lift the burden. He said carers should sometimes ignore comments from friends and family as they may not be aware of the intri-cacies of the situation. Only the primary carer understands the overall picture in what is a very tough situation.
Multicultural perspective publication.indd 33 17/05/2013 11:46:25 AM
34
2.10b. Vietnamese Case Study II
“Huong” is 60 and has been caring for her 84-year-old mother for the last seven years.
When Huong started caring she immediately received Centrelink assistance through Carer Payment and Carer Allowance. Her family doctor was also a good source of information and support, providing detailed explanations about the diagnosis, symptoms and dementia in general. Huong also appreciated the ex-tensive support received from family and friends. They would visit frequently and would always offer help.
Huong said her mother’s memory loss became a problem for everyone in the fam-ily. She would constantly misplace things and would then accuse innocent family members of stealing these items. Then she would behave aggressively towards them while they became distressed about being falsely accused.Huong discovered that introducing more structure and organisation into her mother’s life helped everyone cope better with her memory loss problems. Huong created an ‘order of things’ in the household, arranging items thematically, chronologically or by priority, and found her mother’s recall improved. She also discovered that giving her mother emotional support, especially when confused, helped a great deal.
In time Huong’s mother’s condition deteriorated. Eventually the family made the decision to move her into a permanent residential care unit. Huong’s mother has been living there for two years and is very happy with the service and has a high opinion of the quality of care provided. Huong believes her mother is in the best possible environment, with qualified staff who are better skilled to look after her health.
Before she moved to a nursing home, Huong’s mother accessed a range of HACC services three times per week from the Australian Vietnamese Women’s Associ-ation. These included home help, personal care, help with shopping and social support. These were all highly appreciated and delivered in a culturally sensitive manner.
Huong said she believes carers should always try to remain calm and patient. Sometimes it is easy to get angry, but this is counterproductive. Instead, Huong highlighted the benefits of expressing sympathy and compassion towards the patient, communicating with them as frequently as possible.
Multicultural perspective publication.indd 34 17/05/2013 11:46:25 AM

35
3. Recommendations
This study has sought to build on the present research on dementia. The narrative information, it is anticipated, could be used to provide the basis for further work in CALD communities and on issues related to dementia. While a range of statistics and research exists, this material is not necessarily exhaustive; a study of this nature could be used to confirm or contrast existing data on the subject. There is much work to be done to further empower CALD communities on this issue and all stakeholders have a role to play. It is not necessarily a case of increasing resourc-es – although this may be a cause for consideration – rather, part of the answer may also lie in better utilising existing capacity. Community organisations, for example, need to continue working together. Matters associated with taboo and misunderstanding within communities need to be addressed. Individuals ought to be empowered, and service providers should be assisted to enhance their cross-cultural understanding. As a practical means of assisting this process and as direct evidence based on the research contained within this report, the follow-ing recommendations are put forward for discussion and consideration. 1. As with the broader community, greater awareness of dementia is required across ethnic communities. Initiatives that include public-service announcements in the media should be considered. The capacity of ethnic radio and newspapers remains an effective mechanism for communicating with migrant groups.
2. The development of culturally sensitive respite options should be encouraged or expanded wherever possible.
3. The welfare of carers is important. Linking them to available counselling options is a key mechanism for supporting their mental health. Part of the approach should include information strategies that challenge any taboos about the appro-priateness of counselling services.
4. Initiatives undertaken in partnership with Commonwealth agencies should contin-ue to be encouraged. Information relating to the carers benefits available through Centrelink, for example, should be promoted wherever possible. While a sample of participants in this study had an awareness of such benefits, it is unknown if those with limited community linkages experience the same access.
5. There are many stories of good service provision and care, and these should be acknowledged and celebrated. There is a role for peak bodies and HACC ser-vices, such as the Ethnic Communities Council of Victoria, to acknowledge both service providers and individual carers. This can be viewed as a means of promot-ing best practice. In relation to carers, individual achievements could be viewed as a source of inspiration for others.
Multicultural perspective publication.indd 35 17/05/2013 11:46:25 AM
36
6. The importance of ethno-specific support groups is evident in many of the cas-es cited in this report. It therefore follows that they should be supported in every manner possible. There should be a particular emphasis on the establishment of groups that have little or no linkages to HACC social support services. There also needs to be an emphasis on assisting isolated individuals who are socially dislo-cated on an acute scale.
7. General practitioners present a key pathway for disseminating information to car-ers and patients on support services. The availability of translated material would assist with the provision of information on advocacy services and support groups.
8. Every effort should be made to enhance access to HACC services across all com-munities. The narratives in this study demonstrate that those with migrant back-grounds do not necessarily possess strong social networks. Some of the respon-dents had no understanding of social welfare programs beyond Centrelink.
Multicultural perspective publication.indd 36 17/05/2013 11:46:25 AM
37
4. Conclusion
The principal aim of this study was to capture the perceptions of dementia among 10 diverse communities within the north-western region of Melbourne. Before making any concluding remarks, we wish to remind readers that the people who participated in this study may not necessarily represent the views of the whole community group from which they originate. As with most research studies, sam-ple sizes are usually limited in number, therefore, they can never capture the entire nature of the wider group, thus making generalisations difficult. Neverthe-less, the people we spoke to were all representatives of their ethnic groups, and all expressed their honest opinions and perceptions about dementia. Their voices are essential in informing us about the nature and issues of dementia. They are, in effect, providing another piece of the puzzle.
Community Groups
It appears that different groups have very different perceptions and levels of understanding about dementia. We also found this difference was often not attrib-utable to cultural factors but to levels of education and prior awareness of de-mentia. For example, participants within PAGs who regularly met and discussed topics about health and wellbeing seemed to demonstrate a higher level of aware-ness about dementia in general. They were able to speak more insightfully about its nature, the challenges for carers, available treatments, protective mechanisms and so forth. They were also more likely to perceive dementia as an illness rather than something that occurs as a result of the normal process of ageing. However, we noticed that even individuals within PAGs had different levels of understanding of dementia. While PAGs and social groups were generally good at elevating the community’s overall knowledge of dementia, people with no access to a PAG-type environment or access to information about dementia had a significantly lower level of awareness.
The majority of people we spoke to defined dementia in terms of the most com-mon symptoms: memory loss and forgetfulness. Most struggled to define demen-tia more broadly than this and many could not identify any of the probable causes of dementia. It appears that most people could benefit from more education about dementia, especially those not within PAGs. People within PAGs could also benefit from further dementia education. We recommend that this group would benefit substantially from further education.
The main barriers that impede increased knowledge of dementia seem to be poor English skill levels and not knowing where to find information. This appears to be allied to low levels of confidence in accessing information and asking questions. A person who struggles with English is unlikely to respond to a printed pamphlet about dementia. Equally it is unlikely that she or he would speak to a health pro-fessional until someone in the family is diagnosed. In this context the notion of information being available on the internet may also produce negligible benefits.
Multicultural perspective publication.indd 37 17/05/2013 11:46:25 AM

38
Case Studies
We found that people living or caring for someone with dementia had a very high level of awareness and a much deeper understanding about dementia. Carers were able to describe graphically many of the difficulties they endured on a daily basis, including dealing with challenging behaviours, physical handling and the psychological stress associated with caring for a person full-time. Many carers stated that, since adopting their caring responsibilities, they had little or no time to pursue their own interests. If carers wanted to maintain their social connec-tions and hobbies, a great deal of planning and preparation was required and, even then, plans could change suddenly because of the unpredictable nature of caring.
Many carers found innovative and useful strategies that helped them and their families cope better with difficult situations. Different families used different tech-niques and each needs to work out what works best for them.
Multicultural perspective publication.indd 38 17/05/2013 11:46:25 AM
39
5. Resource Directory
Alzheimer’s Australia Vic94–108 Riversdale Road Hawthorn, Vic. 3122T: (03) 9815 7800F: (03) 9815 7801 W: www.fightdementia.org.auE: [email protected]
Australian Croatian Community Services40 Pickett StreetFootscray, Vic. 3011T: (03) 9686 5811www.accs.asn.au
Australian Multicultural Community ServicesLevel 1, 44–56 Hampstead RdMaidstone, Vic. 3012T: (03) 9689 9170F: (03) 9687 7446 W: www.amcservices.org.au
Cyprus Senior Citizens Turkish Group Errington Community Centre 1 Princess Street,St Albans, Vic. 3021T: (03) 9363 8177
Department of HealthNorth and West Metropolitan Region145 Smith StreetFitzroy, Vic. 3065T: 1300 360 408W: www.health.vic.gov.au
Filipino Community Council of Victoria IncPhilippine Australia Multi-Purpose Centre98 Cowper StreetFootscray, Vic. 3011T: (03) 9687 9011F: (03) 9687 9120E: [email protected]
Hammurabi Cultural Society Inc. / Tuesday Gathering GroupMeadow Heights Community Centre15–29 Buchan StreetMeadow Heights, Vic. 3048T: 0422 335 063
Multicultural perspective publication.indd 39 17/05/2013 11:46:25 AM
40
ISIS Primary Care1 Andrea Street St Albans, Vic. 3021T: 03 9296 1200F: 03 9366 2086W: www.isispc.com.au
Macedonian Senior Citizens GroupHobsons Bay City Council115 Civic ParadePO Box 21Altona, Vic. 3018T: (03) 9932 1000F: (03) 9332 1039
Migrant Resource Centre North West Inc45 Main Road WestSt Albans, Vic. 3021T: (03) 9367 6044F: (03) 9367 4344W: www.mrcnorthwest.org.au
North Cyprus Turkish Seniors Group547 Ballarat RoadSunshine, Vic. 3020T: (03) 9449 9176
Northern Region Indian Seniors Association of Victoria18A Bent StreetNorthcote, Vic. 3070T: (03) 9486 8103
Victorian Arabic Social Services (VASS)C1, 1–13 The GatewayBroadmeadows, Vic. 3047T: (03) 9359 2861F: (03) 9359 2899E: [email protected]: www.vass.org.au
Vietnamese Welfare Resource Centre58 Holland Court PO Box 55Flemington, Vic. 3031T: (03) 9376 2033F: (03) 9376 4687E: [email protected]
Multicultural perspective publication.indd 40 17/05/2013 11:46:25 AM
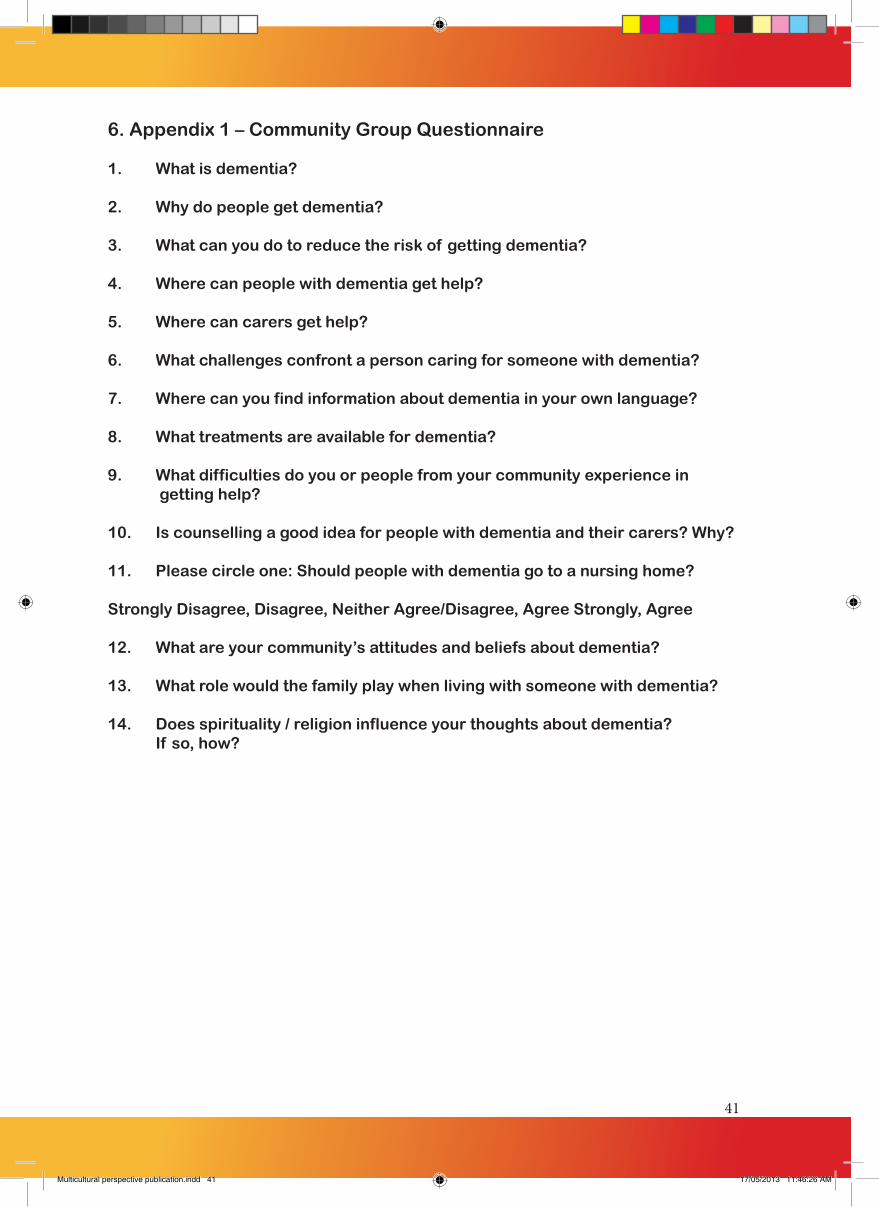
41
6. Appendix 1 – Community Group Questionnaire
1. What is dementia?
2. Why do people get dementia?
3. What can you do to reduce the risk of getting dementia?
4. Where can people with dementia get help?
5. Where can carers get help?
6. What challenges confront a person caring for someone with dementia?
7. Where can you find information about dementia in your own language?
8. What treatments are available for dementia?
9. What difficulties do you or people from your community experience in getting help?
10. Is counselling a good idea for people with dementia and their carers? Why?
11. Please circle one: Should people with dementia go to a nursing home? Strongly Disagree, Disagree, Neither Agree/Disagree, Agree Strongly, Agree
12. What are your community’s attitudes and beliefs about dementia?
13. What role would the family play when living with someone with dementia?
14. Does spirituality / religion influence your thoughts about dementia? If so, how?
Multicultural perspective publication.indd 41 17/05/2013 11:46:26 AM

42
7. Appendix 2 – Case Study Questionnaire
1. What kind of support did you and your family receive when your family member was diagnosed with dementia? 2. Can you describe some of the most difficult challenges you have experi enced when caring for a person with dementia?
3. What strategies helped you overcome these challenges?
4. Can you explain your experiences in dealing with health care services in relation to dementia?
5. Can you suggest anything that could have made it easier?
6. What are your impressions about residential nursing homes and did you consider them as an option?
7. Have you received any in-home support?
8. Do you think your perceptions and knowledge about dementia have changed since your loved one was diagnosed?
9. Anything else you would like to suggest or share about your experiences in caring for a person with dementia.
Multicultural perspective publication.indd 42 17/05/2013 11:46:26 AM

Multicultural perspective publication.indd 43 17/05/2013 11:46:26 AM

Multicultural perspective publication.indd 44 17/05/2013 11:46:26 AM















![Future Doctors' Perceptions about Incorporating Nutrition ...€¦ · oporosis, dementia, nutritional anemias, gall bladder disease, and several forms of cancer [1]. A recent report](https://img.dokumen.tips/doc/110x75/5f55fca06261315bdc7f6085/future-doctors-perceptions-about-incorporating-nutrition-oporosis-dementia.jpg)













