Embed Size (px)
Citation preview

KNEE
A medium to long-term follow-up of ACL reconstructionusing double gracilis and semitendinosus grafts
Andrea Ferretti • Edoardo Monaco •
Silvio Giannetti • Ludovico Caperna •
David Luzon • Fabio Conteduca
Received: 23 July 2009 / Accepted: 17 June 2010 / Published online: 3 July 2010
� Springer-Verlag 2010
Abstract This paper reports the results of our approach to
ACL tears and knee laxity, based on 30 years of experience
in ACL reconstruction with hamstrings and founded on the
following cornerstones: the use of doubled semitendinosus
and gracilis as a free graft; the use of an out-in technique for
femoral drilling and of very strong and stiff fixation devices;
the careful examination and repair or reconstruction of the
lateral compartment in selected patients; and the use of
unaggressive rehabilitation. We prospectively evaluated a
series of 100 consecutive patients who underwent ACL
reconstruction between 2001 and 2002. A clinical and
radiological follow-up was performed at a minimum of
6 years. After 6 years, the International Knee Documenta-
tion Committee score demonstrated good-to-excellent
results (A and B) in 98% of patients. However, arthrometric
results using the KT-1000 demonstrated that 6/80 patients
(7.5%) had [5 mm manual maximum side-to-side differ-
ence. The median Tegner activity score was 5 (range 1–9);
the median Lysholm score was 96 (range 81–100); and the
median subjective IKDC score was 94 (range 66–100). We
reported 6/80 failures as revealed by a 2? or 3? pivot-shift
test result and/or KT-1000 side-to-side difference of more
than 5 mm. The IKDC score revealed excellent results in all
women who underwent extra-articular tenodesis. Radio-
graphic evaluation demonstrated early signs of osteoarthritis
in 9% of patients.
Keywords Anterior cruciate ligament (ACL)
reconstruction � Extra-articular tenodesis � Hamstrings �Tunnel widening
Introduction
Anterior cruciate ligament (ACL) reconstruction is one of the
most frequently performed operations in orthopedic surgery.
Patellar tendon and hamstring tendons are the most com-
monly used graft choice for most surgeons—both options are
reliable and report comparable clinical and functional out-
comes with satisfactory mid- and long-term results in 80% to
more than 90% of patients [4]. The major benefit of using a
hamstring tendon graft is decreased donor-site morbidity, in
particular, there is less anterior knee pain and kneeling dis-
comfort thus resulting in fewer potential damages to the
extensor mechanism (extensor weakness, extension loss)
compared to bone-patellar bone-tendon grafts [4].
Our approach to ACL reconstruction is based on the fol-
lowing cornerstones: the use of doubled semitendinosus and
gracilis tendons dissected as free grafts; the use of very
strong and stiff, quite anatomical, devices implanted using an
out-in technique for femoral drilling; careful examination
and repair or reconstruction of the lateral compartment in
selected patients (severe rotatory laxity with a 3? pivot-shift
test result, revisions, high-risk athletes); and the use of
unaggressive rehabilitation with an extension brace for
2 weeks postoperatively. This initial precaution does not
affect the following steps of the rehabilitation, which
advances quickly with return to competitive sport in about
4–6 months.
The aim of this study was to prospectively evaluate our
present surgical technique to treat ACL tears and knee
laxity at 6 years follow-up in a series of 100 consecutive
A. Ferretti � E. Monaco � S. Giannetti � L. Caperna �D. Luzon � F. Conteduca
Department of Orthopaedics and Traumatology, Kirk Kilgour
Sports Injury Center, II School of Medicine, Sant’Andrea
Hospital, Sapienza University of Rome, Rome, Italy
E. Monaco (&)
Via D. di Buoninsegna 22, 00142 Rome, Italy
e-mail: [email protected]
123
Knee Surg Sports Traumatol Arthrosc (2011) 19:473–478
DOI 10.1007/s00167-010-1206-1

patients, operated by the same senior surgeon (A.F.) just
after the commercial availability of new fixation devices.
Clinical and radiographic results—especially the degree of
degenerative changes and bone tunnel widening—were
specifically evaluated and correlated with the functional
and stability status of the patients.
Materials and methods
Between 2002 and 2003, one hundred consecutive
patients who underwent an ACL reconstruction using a
hamstring tendon autograft were selected for this pro-
spective study and re-evaluated at a minimum of 6 years
postoperatively. Exclusion criteria were severe cartilage
damage (grade 3 or 4 according to the Outerbridge clas-
sification [29]), additional procedures to the cartilage
(autologous chondrocyte transplantation, microfractures,
etc.), open physes and surgery on the involved knee prior
to the injury.
An arthroscopically assisted two-incision technique
using doubled semitendinosus and gracilis tendon auto-
grafts was performed. A cortical fixation to the bone was
achieved on the femur using the SWING BRIDGE device
(Citieffe, Bologna, Italy) and on the tibia using the
EVOLGATE device (Citieffe, Bologna, Italy) [11]. A tight
fit of the graft in the bone tunnel was aimed for in all
patients. Among professional athletes with severe knee
laxity having a 2? or 3? pivot-shift test result, extra-
articular reconstruction was also performed (Coker Arnold
modification of the McIntosh technique [26]).
The postoperative rehabilitation was standardized for all
patients: the involved knee was placed in a full extension
brace for 2 weeks postoperatively with weight-bearing on
crutches as tolerated. Following the 2 weeks, progressive
range-of-motion exercises were encouraged. At 6 weeks
postoperatively, full weight-bearing without crutches and
without brace was permitted. From 2 to 4 months postop-
eratively, a muscle-strengthening program was prescribed
and between 4 and 6 months postoperatively, a gradual
return to specific athletic training was encouraged.
A 6-year follow-up examination was performed by the
same observer (S.G.) who was not involved in the initial
surgery.
The activity level was assessed using the Tegner activity
score [32]. In evaluating the functional status, the Lysholm
score [32] was used, whereas in evaluating the clinical
outcome, the International Knee Documentation Commit-
tee rating system (IKDC) [16] was used.
Patients underwent a standardized bilateral knee exam-
ination. Stability testing was performed using the Lachman
test, the pivot-shift test and the KT-1000 arthrometer
(Medmetric, San Diego, USA).
Weight-bearing comparative radiographs (A-P with
extended knee and lateral view) were obtained and evalu-
ated using Fairbank signs [9], Kellgren scores [21] and the
IKDC grading system [16].
Tunnel enlargement was determined with the method
described by L’Insalata et al. [23]. These measurements
were performed by a single examiner using a digital
calliper and a dedicated digital radiology software
(Centricity Imaging PACS/AW Suite, GE Healthcare IT).
The ratio between this average value and the intraopera-
tively determined tunnel diameter, according to medical
record, was used to assess the tunnel widening.
The Student t-test and analysis of variance (ANOVA)
were used to analyze the data for the patients in this series.
For power analysis, the alpha error was fixed at 5%
(confidence interval 95%) and the level of significance was
P \ 0.05. Statistical evaluation was performed using SPSS
for Microsoft Windows 7.0 (SPSS, Inc., Chicago, IL).
Results
At final follow-up, eight patients (8%) were lost to follow-up
and eighty patients (80%) returned for an evaluation that
included a thorough medical history and physical examina-
tion, a radiographic examination and a KT-1000 arthrometric
test. Eleven patients (11%) were evaluated using only the
rating scales obtained via telephone interview. One patient
was excluded after having suffered a serious accident that
occurred during the follow-up period; eventually, a full
recovery and return to the competitive level achieved before
injury was achieved.
At time of surgery, there were 68 men and 23 women
with a median age of 35 years (range 21–58). The median
follow-up time was 6 years (range 60–65 months).
The mean time between trauma and surgery was 7 days
(min 2, max 14) in the acute patients (25/100 patients) and
4 months (min 2, max 5) in the chronic patients (75/100
patients). A partial medial meniscectomy was performed in
11 patients, a partial lateral meniscectomy in 20 patients
and a partial medial and lateral meniscectomy in 7 patients.
Repair of the medial meniscus was performed in 4 patients.
In 23 of 100 patients, an extra-articular reconstruction was
performed with the above-mentioned technique.
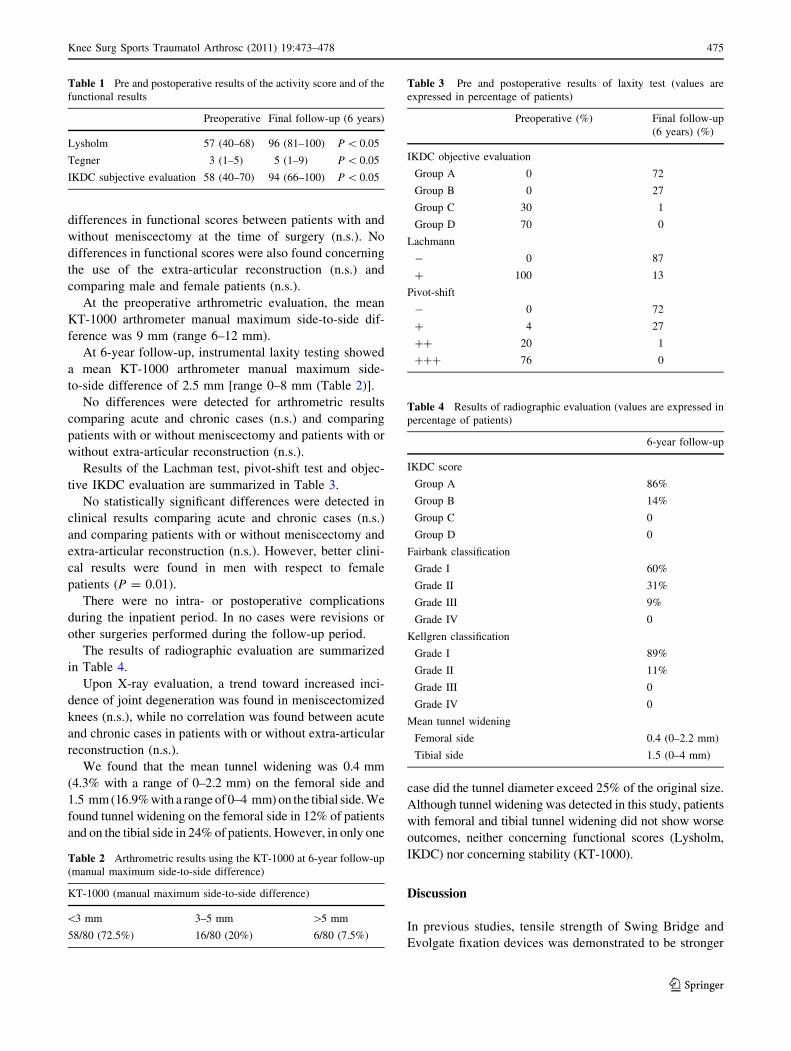
The results of the Tegner score, Lysholm score and
subjective IKDC evaluation are summarized in Table 1.
A statistically significant difference was found com-
paring pre and postoperative functional scores (P = 0.001
for Tegner, Lysholm and IKDC).
No differences were detected for Lysholm and IKDC
activity scores comparing acute and chronic cases (n.s.),
while a significantly better result was found in acute cases
with respect to the Tegner score (P = 0.04). There were no
474 Knee Surg Sports Traumatol Arthrosc (2011) 19:473–478
123
differences in functional scores between patients with and
without meniscectomy at the time of surgery (n.s.). No
differences in functional scores were also found concerning
the use of the extra-articular reconstruction (n.s.) and
comparing male and female patients (n.s.).
At the preoperative arthrometric evaluation, the mean
KT-1000 arthrometer manual maximum side-to-side dif-
ference was 9 mm (range 6–12 mm).
At 6-year follow-up, instrumental laxity testing showed
a mean KT-1000 arthrometer manual maximum side-
to-side difference of 2.5 mm [range 0–8 mm (Table 2)].
No differences were detected for arthrometric results
comparing acute and chronic cases (n.s.) and comparing
patients with or without meniscectomy and patients with or
without extra-articular reconstruction (n.s.).
Results of the Lachman test, pivot-shift test and objec-
tive IKDC evaluation are summarized in Table 3.
No statistically significant differences were detected in
clinical results comparing acute and chronic cases (n.s.)
and comparing patients with or without meniscectomy and
extra-articular reconstruction (n.s.). However, better clini-
cal results were found in men with respect to female
patients (P = 0.01).
There were no intra- or postoperative complications
during the inpatient period. In no cases were revisions or
other surgeries performed during the follow-up period.
The results of radiographic evaluation are summarized
in Table 4.
Upon X-ray evaluation, a trend toward increased inci-
dence of joint degeneration was found in meniscectomized
knees (n.s.), while no correlation was found between acute
and chronic cases in patients with or without extra-articular
reconstruction (n.s.).
We found that the mean tunnel widening was 0.4 mm
(4.3% with a range of 0–2.2 mm) on the femoral side and
1.5 mm (16.9% with a range of 0–4 mm) on the tibial side. We
found tunnel widening on the femoral side in 12% of patients
and on the tibial side in 24% of patients. However, in only one
case did the tunnel diameter exceed 25% of the original size.
Although tunnel widening was detected in this study, patients
with femoral and tibial tunnel widening did not show worse
outcomes, neither concerning functional scores (Lysholm,
IKDC) nor concerning stability (KT-1000).
Discussion
In previous studies, tensile strength of Swing Bridge and
Evolgate fixation devices was demonstrated to be stronger
Table 1 Pre and postoperative results of the activity score and of the
functional results
Preoperative Final follow-up (6 years)
Lysholm 57 (40–68) 96 (81–100) P \ 0.05
Tegner 3 (1–5) 5 (1–9) P \ 0.05
IKDC subjective evaluation 58 (40–70) 94 (66–100) P \ 0.05
Table 2 Arthrometric results using the KT-1000 at 6-year follow-up
(manual maximum side-to-side difference)
KT-1000 (manual maximum side-to-side difference)
\3 mm 3–5 mm [5 mm
58/80 (72.5%) 16/80 (20%) 6/80 (7.5%)
Table 3 Pre and postoperative results of laxity test (values are
expressed in percentage of patients)
Preoperative (%) Final follow-up
(6 years) (%)
IKDC objective evaluation
Group A 0 72
Group B 0 27
Group C 30 1
Group D 70 0
Lachmann
- 0 87
? 100 13
Pivot-shift
- 0 72
? 4 27
?? 20 1
??? 76 0
Table 4 Results of radiographic evaluation (values are expressed in
percentage of patients)
6-year follow-up
IKDC score
Group A 86%
Group B 14%
Group C 0
Group D 0
Fairbank classification
Grade I 60%
Grade II 31%
Grade III 9%
Grade IV 0
Kellgren classification
Grade I 89%
Grade II 11%
Grade III 0
Grade IV 0
Mean tunnel widening
Femoral side 0.4 (0–2.2 mm)
Tibial side 1.5 (0–4 mm)
Knee Surg Sports Traumatol Arthrosc (2011) 19:473–478 475
123
and stiffer compared to other commercially available
devices [10–12, 24].
These technical improvements in fixation devices
allowed us to achieve a very stable knee at final follow-up
with a KT-1000 side-to-side difference of less than 5 mm
in more than 90% of patients. The efficacy of this tech-
nique is validated also by the low incidence of symptoms.
All patients in this series were satisfied with the operation
and no patients complained of pain or instability even
during strenuous sports activities. Moreover, even though
the devices used are both made of a titanium alloy and are
impacted on the cortical bone, no complications such as
ileotibial band friction syndrome and pain on the tibial side
have been reported. Also, in no patient has device removal
been needed.
The correct positioning of the graft is an important
factor in successful ACL reconstruction. In this series, a
standard tibial guide was used and positioned at 65�degrees with the probe of the guide placed at 7 mm in front
of the PCL. For the femoral tunnel placement, some
authors suggest the use of trans-tibial or anteromedial
portal access. We prefer the out-in technique that allows
the surgeon to orient the femoral tunnel in a more posterior
and anatomical position almost over the top position,
independently from the tibial tunnel position [31]. Con-
sidering the functional results, we believe that using a two-
incision out-in technique is quite safe with just an increased
minimal morbidity or in the case of extra-articular recon-
struction, not increased morbidity because the same second
incision is needed for the lateral plasty.
The first aim of the radiographic study was to determine
tunnel widening. Tunnel widening has been considered as a
major concern in ACL reconstructions with hamstring
tendon grafts [6, 18, 23]. We detected a femoral tunnel
widening in only 12% of patients using a suspension device
such as the Swing Bridge and in 24% of patients at the
tibial side, using an anatomical device such as the
Evolgate, with only one case exceeding 25% of the original
size. Based on these data, we assume that tunnel enlarge-
ment could be limited by using very strong and stiff
devices as previously demonstrated by Iorio et al. in a CT
study [19].
Moreover, many authors hypothesized that aggressive
rehabilitation protocols may be a potential factor for bone
tunnel enlargement, especially in reconstructions per-
formed with hamstring autografts [2, 14, 33]. Although the
use of the devices seem to strongly reduce the micro-
movements of the tendons inside the tunnels, thus pro-
moting Sharpey’s fibers formation, we use an unaggressive
rehabilitation utilizing a full extension brace for 2 weeks
postoperatively in order to better promote the biological
fixation. This rehabilitation protocol does not interfere with
the following steps of the rehabilitation and with the return
to sports activities in 4–6 months postoperatively. The
concept of enhanced integration of the graft into the tunnel
is indirectly confirmed by the fact that a very limited tunnel
enlargement was observed at 6-year follow-up.
However, no correlation was revealed between tunnel
widening and activity level, functional results and KT-1000
results. Therefore, our findings were generally in accor-
dance with literature [2, 5].
The development of osteoarthritis after ACL reconstruc-
tion is reported for all types of reconstructions. Explanations
are difficult (overconstrained grafts, nonanatomical proce-
dures, overuse in stable knees, meniscal lesions and personal
experience of the surgeon). Reports of joint space narrowing
in literature range from 12 to 78% [17].
Nine percent of patients reported grade III degeneration
according to Fairbank signs; only 14% of patients were in
group B according to the Kellgren scores; and all patients
were graded as A or B (normal or nearly normal) using
IKDC. In agreement with previous studies [14], we
detected a trend toward degeneration in patients with
medial meniscectomy (n.s.). No joint degeneration was
observed in chronic patients compared to acute patients nor
in patients without extra-articular reconstruction compared
to those with (n.s.).
Several anatomical and biomechanical studies demon-
strated the strict relationship between ACL and the cap-
sular lateral ligaments in controlling the rotatory stability
of the knee; and that in ACL tears, injuries of these liga-
ments often occur [20, 22]. The degree of involvement of
the lateral capsular ligaments could explain the difference
in rotatory laxity found in ACL tears, currently evaluated
by a pivot-shift ranging from 1? to 3?.
Recently, several authors have reconsidered the role of
lateral tears and reconstructions in rotatory instabilities and
often perform extra-articular reconstructions in association
with the intra-articular reconstructions [1, 25, 27]. The role
and effectiveness of a lateral extra-articular procedure
performed in association with ACL reconstruction has not
been defined [30]. While some authors have expressed
belief that postoperative stability cannot be improved by
any additional procedure [3], others have reported better
results when an extra-articular iliotibial band tenodesis was
performed in association with an intra-articular ACL
reconstruction, especially if a semitendinosus and gracilis
graft was used [15, 34]. In vitro analysis performed by
Engebretsen et al. [8] has shown that the extra-articular
plasty, when used in combination with intra-articular
reconstruction, reduces the stress to the graft by approxi-
mately 43%. Moreover, some biomechanical in vitro
studies [26, 28] demonstrate that the extra-articular
reconstruction reduces the internal rotation of the tibia with
less risk of pivoting. More recently, the role of the extra-
articular reconstruction in reducing the internal rotation of
476 Knee Surg Sports Traumatol Arthrosc (2011) 19:473–478
123

the tibia has also been demonstrated in vivo with computer-
assisted surgery [28].
A modified MacIntosh lateral tenodesis [26] was used to
treat severe chronic rotatory laxity (3? pivot-shift test) in 23
patients committed to professional sports activities; at fol-
low-up, all of these patients were graded as normal or nearly
normal, with and without evidence of degenerative changes
when compared to patients treated with an intra-articular
reconstruction alone. Moreover, considering as biome-
chanical reconstruction failure a 2? or 3? pivot-shift test
and/or a KT-1000 side-to-side difference of more than
5 mm, we observed 6 cases of failure (3 men and 3 women).
All of these 6 patients were operated without the extra-
articular tenodesis. The highly satisfactory results obtained
in this series show that, from a clinical point of view, a
combination of intra and extra-articular procedures for ACL
reconstruction is a valid option and seems to confirm the
role of the procedure to restore rotator stability of the knee
also at long-term follow-up, especially in severe rotatory
instabilities.
In the last few years, the use of an accelerated rehabil-
itation program after ACL reconstruction has become
widely accepted. However, it is well known that secure
tendon-to-bone healing requires at least 12 weeks. There-
fore, accelerated rehabilitation and the related micromotion
of the graft in the tunnels could compromise the bone-
tendon interface, resulting in poor biological fixation
[7, 33]. When hamstring grafts are used, even when strong
and stiff fixation devices are utilized, we believe that a
slower rehabilitation program such as the one employed in
the present study should be suggested. However, despite
the initial unaggressive regimen used in this series, almost
all patients, 77 of 92 (83.7%) could return to their
pre-operative sport level and activity within 6 months
postoperatively.
The limitation of this study is that there is no control
group. However, the strength is in reporting clinical,
functional and radiological results at a long-term follow-up
for a series of 100 consecutive patients operated by the
same senior surgeon.
An 8% loss to follow-up allows a representative
outcome evaluation. Clinical evaluation revealed good-
to-excellent subjective results at IKDC in 79/80 patients
(group A and B) with a stable knee joint and a side-to-side
difference at KT-1000 of less than 5 mm in 74/80 patients
(92.5%).
In agreement with previously published studies, we
found worst objective results at IKDC evaluation
(P = 0.01) and a trend toward worst arthrometric results
(n.s.) in women. However, the IKDC score revealed
excellent results (group A) in all women who underwent
extra-articular tenodesis.
Conclusion
In conclusion, we still consider the hamstrings an excellent
graft for ACL reconstruction. However, in light of the
findings shown in this paper, we introduced a new har-
vesting technique for the semitendinosus [13], preserving
as much of its distal insertion as possible, thus preventing
internal rotation strength deficit and extending indication
for the lateral tenodesis to the moderate rotator laxity
(pivot-shift 2?), especially in women.
References
1. Aglietti P, Buzzi R, D’Andria S, Zaccherotti G (1992) Long-term
study of anterior cruciate ligament reconstruction for chronic
instability using the central one-third patellar tendon and a lateral
extraarticular tenodesis. Am J Sports Med 20:38–45
2. Asik M, Sen C, Tuncay I, Erdil M, Avci C, Taser OF (2007) The
mid- to long-term results of the anterior cruciate ligament
reconstruction with hamstring tendons using Transfix technique.
Knee Surg Sports Traumatol Arthrosc 15:965–972
3. Barrett GR, Noojin FK, Hartzog CW, Nash CR (2002) Recon-
struction of the anterior cruciate ligament in females: a compar-
ison of hamstring versus patellar tendon autograft. Arthroscopy
18:46–54
4. Bunchner M, Schmeer T, Schmitt H (2007) Anterior cruciate
ligament reconstruction with quadrupled semitendinosus ten-
don—minimum 6 year clinical and radiological follow-up. Knee
14:321–327
5. Cinar BM, Akpinar S, Hersekli MA, Uysal M, Cesur N,
Pourbagher A, Derincek A (2009) The effects of two different
fixation methods on femoral bone tunnel enlargement and clinical
results in anterior cruciate ligament reconstruction with ham-
string tendon graft. Acta Orthop Traumatol Turc 43:515–521
6. Clatworthy MG, Annear P, Bulow J-U, Bartlett RJ (1999) Tunnel
widening in anterior cruciate ligament reconstruction: a pro-
spective evaluation of hamstring and patella tendon graft. Knee
Surg Sports Traumatol Arthrosc 7:138–145
7. Draganich LF, Reider B, Ling M, Samuelson M (1990) An in
vitro study of an intraarticular and extraarticular reconstruction in
the anterior cruciate ligament deficient knee. Am J Sports Med
18:262–266
8. Engebretsen L, Lew WD, Lewis JL, Hunter RE (1990) The effect
of an iliotibial tenodesis on intraarticular graft forces and knee
joint motion. Am J Sports Med 18:169–176
9. Fairbank TJ (1948) Knee joint changes after meniscectomy.
J Bone Joint Surg 30B:664–670
10. Ferretti A, Conteduca F, La Bianca L, Monaco E, De Carli A
(2005) Evolgate fixation of doubled flexor graft in ACL recon-
struction: biomechanical evaluation with cyclic loading. Am
J Sports Med 33:574–582
11. Ferretti A, Conteduca F, Morelli F, Ticca L, Monaco E (2003)
The Evolgate: a method to improve the pullout strength of
interference screws in tibial fixation of anterior cruciate ligament
reconstruction with doubled gracilis and semitendinosus tendons.
Arthroscopy 19:936–940
12. Ferretti A, Monaco E, Labianca L, D’Angelo F, De Carli A,
Conteduca F (2006) How four and twelve weeks of implantation
affect the strength and stiffness of a tendon graft securely fixed in
a bone tunnel: a study of Evolgate fixation in an extra-articular
model bovine model. J Orthop Traumatol 7:136–141
Knee Surg Sports Traumatol Arthrosc (2011) 19:473–478 477
123
13. Ferretti A, Vadala A, De Carli A, Argento G, Conteduca F,
Severini G (2008) Minimizing internal rotation strength deficit
after use of semitendinosus for anterior cruciate ligament
reconstruction: a modified harvesting technique. Arthroscopy
24:786–795
14. Giron F, Aglietti P, Cuomo P, Mondanelli N, Ciardullo A (2005)
Anterior cruciate ligament reconstruction with double-looped
semitendinosus and gracilis tendon graft directly fixed to cortical
bone: 5-year results. Knee Surg Sports Traumatol Arthrosc
13:81–91
15. Goertzen M, Schulitz KP (1993) Comparison of combined extra-
and intra-articular stabilization versus isolated arthroscopic
semitendinosus repair after rupture of the anterior cruciate liga-
ment. Sportverletz Sportschaden 7:7–12
16. Hefti F, Muller W, Jakob RP, Staubli HU (1993) Evaluation of
knee ligament injuries with the IKDC form. Knee Surg Sports
Traumatol Arthrosc 1:226–234
17. Hertel P, Behrend H, Cierpinski T, Musahl V, Widjaja G (2005)
ACL reconstruction using bone-patellar tendon-bone press-fit
fixation: 10-year clinical results. Knee Surg Sports Traumatol
Arthrosc 13:248–255
18. Horer J, Moller HD, Fu FH (1998) Bone enlargement after
anterior cruciate ligament reconstruction: fact or fiction? Knee
Surg Sports Traumatol Arthrosc 6:231–240
19. Iorio R, Vadala A, Argento G, Di Sanzo V, Ferretti A (2007)
Bone tunnel enlargement after ACL reconstruction using autol-
ogous hamstring tendons: a CT study. Int Orthop 31:49–55
20. Jonsson H, Riklund-Ahlstrom K, Lind J (2004) Positive pivot
shift after ACL reconstruction predicts later osteoarthrosis. Acta
Orthop Scand 75:594–599
21. Kellgren JH, Lawrence JS (1957) Radiological assessment of
osteo-arthrosis. Ann Rheum Dis 16:494–502
22. Kessler MA, Behrend H, Henz S, Stutz G, Rukavina A, Kuster
MS (2008) Function, osteoarthritis and activity after ACL-
rupture: 11 year follow-up results of conservative versus recon-
structive treatment. Knee Surg Sports Traumatol Arthrosc
16:442–448
23. L’Insalata JC, Klatt B, Fu FH et al (1997) Tunnel expansion
following anterior cruciate ligament reconstruction: a comparison
of hamstring and patellar tendon autografts. Knee Surg Sports
Traumatol Arthrosc 5:234–238
24. Labianca L, Monaco E, Speranza A, Camillieri G, Ferretti A
(2006) A biomechanical evaluation of six femur-graft-tibia com-
plex in ACL reconstruction. J Orthop Traumatol 7:131–135
25. Lerat JL, Chotel F, Besse JL et al (1998) The results after
10–16 years of the treatment of chronic anterior laxity of the knee
using reconstruction of the anterior cruciate ligament with a
patellar tendon graft combined with an external extra-articular
reconstruction. Rev Chir Orthop Reparatrice Appar Mot
84:712–727
26. MacIntosh DL, Darby JA (1976) Lateral substitution recon-
struction. In: Proceedings of the Canadian Orthopaedic Associ-
ation. J Bone Joint Surg Br 58:142
27. Marcacci M, Zaffagnini S, Giordano G, Iacono F, Presti ML
(2009) Anterior cruciate ligament reconstruction associated with
extra-articular tenodesis: a prospective clinical and radiographic
evaluation with 10–13-year follow-up. Am J Sports Med 37:707–
714
28. Monaco E, Labianca L, Conteduca F, De Carli A, Ferretti A
(2007) Double bundle or single bundle plus extraarticular teno-
desis in ACL reconstruction? A CAOS study. Knee Surg Sports
Traumatol Arthrosc 15:1168–1174
29. Outerbridge RE (1961) The etiology of chondromalacia patellae.
J Bone Joint Surg 43-B:752–757
30. Pearl AJ, Bergfeld JA (eds) (1992) Extraarticular reconstruction
in the anterior cruciate ligament deficient knee. Human Kinetics,
Champaign
31. Sommer CH, Friederich NF, Muller W (2000) Improperly placed
anterior cruciate ligament grafts: correlation between radiological
parameters and clinical results. Knee Surg Sports Traumatol
Arthrosc 8:207–213
32. Tegner Y, Lysholm J (1985) Rating systems in evaluation of knee
ligament injuries. Clin Orthop Relat Res 198:43–48
33. Vadala A, Iorio R, De Carli A, Argento G, Di Sanzo V,
Conteduca F, Ferretti A (2007) The effect of accelerated, brace
free, rehabilitation on bone tunnel enlargement after ACL
reconstruction using hamstring tendons: a CT study. Knee Surg
Sports Traumatol Arthrosc 15:365–371
34. Zaffagnini F, Marcacci M, Lo Presti M et al (2006) Prospective
and randomized evaluation of ACL reconstruction with three
techniques: a clinical and radiographic evaluation at 5 year fol-
low-up. Knee Surg Sports Traumatol Arthrosc 14:1060–1069
478 Knee Surg Sports Traumatol Arthrosc (2011) 19:473–478
123





























