Embed Size (px)
Citation preview

AUGUST 2003, VOL 78, NO 2 Rosentreter - Talboy
A Didactic and Ex eriential
Approach to R ursing Education Janet Rosentreter, RN;
Mary Lynn Talboy, RN
erioperative nursing care is a con- tinuum. From anxious beginnings P through the procedure behind
closed doors to the bustle of awakenings, the perioperative nurse guides a surgical patient’s experience with sensitivity, safety, and evidence-based skills.’ How can postanesthesia care unit (PACU) RNs best be prepared to continue patient advocacy through the perianesthesia period where ”dramatic and life-threat- ening changes can occur rapidly?”’ bus)
Historically, to work in the PAW, nurses were required to have experience, complete six to eight weeks of orienta- tion, obtain advanced cardiac life support certification, and complete a skills labora- tory. In spite of these rigorous require- ments, many nurses believed that more was needed to ensure the success of a nurse learning to work in this specialty
ABSTRACT 0 POSTANESTHESIA CARE UNIT ( P A 0 nut- ing practice -quires indepth underetanding of sedation, analgesia, and anesthetic agents and techniques; physiological and psychological responses to anesthesiq and the vulnerability of patienta subjected to anesthesia.. 0 THIS ARTICLE reviews a pilot program designed to broaden the larowledge base of PACU RNa ’Ifventy-three RNs completed a self-paced module on anesthetic agents befom putidpatiq in an anesthesia and surgical observation phase. The ntuaes then completed evaluations. 0 RESULTS OF THE EVALUATIONS indicated that thie approach to learning was rewarding for the partidpants. AORNIonnaf 78 (August 2003) 274-288.
area. Patient care in the PACU is complex because of anesthetic agents used, surgi- cal procedures performed in the OR, and patients’ health status. This patient care setting lends itself to errors, so patient safety is of the utmost importance. Vigdance and appropriate clinical deci- sion making are essential to positive patient outcomes.
Periuperative nurses have a long and distinguished tradition of promoting patient safety by intervening to mini- mize the risks related to surgical infec- tion and injuty.2(p1m5)
STATEMENT OF THE PROBLEM The PACU education committee at St
Luke’s Regional Medical Center, Boise, Idaho, wanted to fumish nursing staff members with a unique learning experi- ence that uses a didactic and experien- tial approach to enhance their existing knowledge base. The program took place at St Luke’s Regional Medical Center, a tertiary care facility with more than 300 beds. The medical center was recently awarded magnet status through the American Nurses Cre- dentialing Center, a subsidiary of the American Nurses Association. The magnet award recognizes “hospitals that meet quality standards and pro- vide nurses with more responsibilities, autonomy, and opportunities to partici- pate in policy decisi~n.”~ @1764-17ffi3
The need for increased understand- ing of anesthetic agents and their peri- operative administration and effects were recognized after the hospital administered an annual educational needs questionnaire. Administrators believed that minimal exposure to perioperative settings available in
274 AORN JOURNAL

AUGUST 2003, VOL 78, NO 2 Rosentreter - Talboy
most nursing education programs was a contributing factor for a perceived lack of knowledge and experience.
LITERATURE REVIEW The consensus of learning theorists is
that adult learners 0 possess prior knowledge and
experience, 0 are self-directed learners, 0 have the ability to reflect critically,
0 are experiential learners: These adult learning attributes were incorporated in the anesthesia agents module and the intraoperative observa- tion experience developed at St Luke’s.
An extensive review of the literature yielded few current articles that described intraoperative observations and the development of a nursing guide to anesthesia as part of an orien- tation program to the PACU. In dis- cussing skilled clinical knowledge, one group of researchers noted, ”Nursing is not alone in misunderstanding and overlooking the knowledge embedded in skilled performance or experiential learning.”5 (p32) In summary, this study concludes that theoretical and practical domains of knowledge are equally imp~rtant.~
One researcher reviewed a compe- tency-based perianesthesia orientation program that used adult learning prin- ciples and concluded that learners must assume an active role in their learning and thus, be responsible for their own educational process.6 The program reviewed included a PACU reference guide, learning modules, and a clinical practice component provided by pre- ceptors. The outcomes of this orienta- tion appeared to result in more confi- dent nurses who were able to transfer theory into practice.
The Canadian Operating Room Nurses Association envisioned a cur- riculum developed to support the
and
expanded role of the perioperative anesthesia nurse and the perioperative surgical nurse. The perioperative anes- thesia nurse is defined as an
RN with advanced perioperative nursing education and skills . . . lwhol finctions collaboratively with the anesthetist to provide care for the pa tien t undergoing anesthesia during the preoperative, intraoperative, and postoperative phases.7 @*Q
The course content includes advanced didactic courses in pathophysiology and pharmacology as they relate to anesthesia administration, as well as postanesthetic patient The knowledge care management.-
Results from a current study on nurse staffing levels indicates that
inherent in skilled
among surgical patients, performance or experiential a higher portion of care
provided by registered
learning is nurses was associated with lower urinary tract
misunderstood infection, and was asso- ciated with lower rates
and overlooked of failure to rescue. Failure to rescue was
by many people, defined as death from pneumonia, shock, or
venous thrombosis. . . . It is possible that the outcomes for which we found sign? icant associations may be more sensi- tive to the contributions that the skills and education of registered nurses, in particular make to patient care.8 (~1715.1720)
This supports the idea that a strong cor- relation exists between education and better patient outcomes.
AORN JOURNAL 2 7 7

AUGUST 2003, VOL 78, NO 2 Rosentreter - Talboy
Section IV 1 Opiate antaqonists and benzodiazepines As a result of this program, I am able to
7. list three possible side effects after administration of
8. discuss two nursing interventions for resedation after
narcotic or benzodiazepine antagonists. 1 2 3 4
reversal of narcotics or benzodiazepines. 1 2 3 4
- .- Section V General information 9. This offering was helpful to my professional
10.The format of this module was organized to make this
1 1 . X style of learning was a benefit to my personal
1Z.The content of this offering was relative to the program’s
13.Comments and recommendations for future offerings:
development. 1 2 3 4
material easily understood. 1 2 3 4
development. 1 2 3 4
objectives. 1 2 3 4
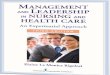
TABLE 1 Evaluation of Self-study Anesthetic Module
Scale: 1 = Strongly disagree 2 = Disagree 3 = Agree 4 = Strongly agree
Section I Inhalation aqents As a result of this program, I am able to
1. discuss three desired effects of inhalation agents.
2. list two nursing considerations when caring for post-
1 2 3 4
anesthesia care unit (PACU) patients who have received inhalation agents. 1 2 3 4
Section II Intravenous anesthetics (ie, sedatives, hypnotics) As a result of this program, I am able to
3. compare the basic actions of the barbiturates and the induction agents (eg, propofol, etomidate, ketamine).
4. formulate a plan of nursing care based on potential postoperative effects from the administration of induction agents/barbiturates. 1 2 3 4
1 2 3 4
Section III Muscle relaxants and neuromuscular blocMnq aqents As a result of this program, I am able to
5. distinguish between the primary pharmacological actions of depolarizing and nondepolarizing muscle relaxants.
6. recognize the potential for cholinergic crisis and recurarization after administration of muscle relaxants.
1 2 3 4
1 2 3 4
PROGRAM DESIGN The pilot program con-
sisted of two parts. The first portion uses a didac- tic learning approach. Initially, a group of four staff RNs developed a self- paced learning module that encompasses the spe- cific anesthetic agents used at St Luke’s Regional Medical Center. The anes- thesia module for St Luke’s PACU nurses con- sists of an extensive glos- sary followed by in-depth discussion of four major anesthetic agent cate- gories, including 0 inhalation agents, 0 intravenous anesthet-
ics (ie, sedatives, hyp- notics),
0 muscle relaxants/ neuromuscular block- ing agents, and
0 opiate antagonists and benzodiazepines? An evaluation (Table
1) and a posttest are included with each mod- ule. Four contact hours are awarded through the Idaho Nurses‘ Asso- ciation upon successful completion. It took the RN educator six months preparation time to com- pile the anesthetic agent module, including ob- taining contact hour approval.
Development of the observational component was the second step. A formal written proposal was presented to the director of surgical servic- es, the manager of the
278 AORN JOURNAL

AUGUST 2003, VOL 78, NO 2 Rosentreter - Talbdy
~~~~~ ~~ ~
TABLE 2 Sample Intraoperative Anesthesia
Observation Program Proposal purpose To provide postanesthesia care unit (PACU) nurses with the opportunity to follow a variety of patients through perioperative or endoscopic procedures. This intraoperative observational opportu- nity, in combination with completion of a didactic anesthetic module, will enhance PACU nurses’ understanding of anesthetic agents, thus improving nurses’ ability to care for postoperative patients.
T i e frame Each nurse will be allowed four hours observation time allowing preference for choice of type of surgery within time and scheduling constraints, when possible.
of Program Specify time frame
Preceptors Anesthesia care providers
Observations 0 American society of Anesthesiologists (ASA) classification 0 Preanesthesia evaluation related to proposed surgery 0 Sequence of anesthetic administration 0 Transition to PACU 0 Overview of postoperative course
Objectives 0 Define the use of the ASA classification system as it relates to the assigned patient. 0 List two indications for choice of anesthetic (ie, general, monitored anesthesia care, regional). 0 Describe the sequence of anesthetic events used to include preoperative medications, airway man-
0 List any untoward effects of agents used and requited management. 0 Summarize patient’s postoperative course, including pain and nausea management, length of stay,
Program coordinator: Specify name
Surgical services: Preoperative holding area: Postanesthesia care unit: Endoscopy unit: Minimally invasive care unit Department of anesthesia: Department of surgery:
Submitted by Specify names
agement, muscle relaxants, inhalation agents, IV therapy, narcotics, and reversal agents.
and any complications as obtained from chart review or patient care nurse interview.
Appwed by
PACU/preoperative holding area (POHA) and the chairs of the depart- ments of anesthesia and surgery (Table 2). Written approval was granted. Preparing the observational component required approximately two months and included developing the observa- tional guidelines (Table 3), intraopera-
tive observation worksheet, and evalua- tion form for the intraoperative observa- tion experience and obtaining approval.
Project coordinators worked with the scheduling committee to provide each RN trainee four hours observational time. Most RNs were able to observe two procedures during this four-hour time
AORN JOURNAL 2 79

AUGUST 2003, VOL 78, NO 2 Rosentreter - Talboy
TABLE 3 0 bsewational G uideli nes
Intraoperative observation 4xperiencc 1. You are scheduled for your intraoperative
observation experience for 4 hours on
End-py obeexvatim experience 1. You are scheduled for your endoscopy
observation experience for 4 hours on
2. Arrive in the preoperative holding area (POHA) 30 minutes before the start of the procedure you have selected to observe. This allows you enough time to identify the pre- operative nurse, anesthesia care provider, and circulating nurse and collect data about your patient. This information is located on the surgical schedule at the POHA desk.
3. Don surgical hair covering and a mask and accompany your patient into the OR with the circulating nurse and anesthesia care provider. The anesthesia care pmvider or cir- culating nurse will show you where to stand (ie, sterile vs unsterile areas) to best observe the patient being induced under anesthesia and ask questions.
4. Introduce yourself to the surgeon when timing is appropriate.
5. Accompany the patient to the postanesthesia care unit (PACU), listen to report, and finish your paperwork (ie, not to recover the patient).
6. Put your completed observation sheet and evaluation into the appropriate mailbox.
7. You may have time in the 4-hour period to observe a second procedure; if not, please take a break and then let your partner start his or her Chour observation.
2. Arrive in POHA 15 minutes before the pm- cedure you have selected to observe. This allows you enough time to identify the pre- operative nurse, anesthesia care provider, and endoscopy nurse and collect data about your patient. This information is located on the surgical schedule at the POHA desk. Notify the charge nurse that you are going to observe an endoscopy procedure.
3. Accompany your patient into the endoscopy room with the endoscopy nurse and anesthesia care provider. The anesthesia care provider or circulating nurse will show you where to stand (ie, sterile vs unsterile areas) to best observe the patient being induced under anesthesia and ask questions.
4. Introduce yourself to the gastroenterologist or surgeon when timing is appropriate.
5. After the procedure is completed, accompa- ny the patient to the P A W and complete your paperwork.
6. Put your completed observation sheet and evaluation into the appropriate mailbox.
7. You may have time in the Chow period to observe a second procedure; if not, please take a break and then let your partner start his or her &hour observation.
block. Written guidelines were estab- lished, describing the procedure to be fol- lowed for the intraoperative observation experience. The RN participants were instructed to arrive in POHA 30 minutes before the start of the selected case. This allowed time to idenbfy the mentoring POHA RN and meet with the assigned circulating nurse and certified RN anes- thetist (CRNA). Informed consent was obtained from the surgeon and patient to allow the participant to be present and observe the surgical procedure. The RNs were encouraged to complete the anes- thesia agent module before the intraoper-
ative experience. All surgical procedures were observed in the OR suites at the main campus of St Luke’s Regional Medical Center. The RN participant fol- lowed the patient with the circulating nurse and the CRNA into the OR suite. The circulating nurse or CRNA indicated where the RN participant should stand to best observe induction and the surgical procedure, ask questions, and maintain a sterile surgical environment. Participants completed an observation worksheet (Table 4) and evaluation tool (Table 5) at the end of their experience. The work- sheet summarized basic data, such as the
280 AORN JOURNAL

AUGUST 2003, VOL 78, NO 2 Rosentreter - Talboy
I
TABU 4 Intraoperative Anesthesia Obsewation Worksheet 1. Observer: 2. Date: 3. Start time: 4. Type of surgery: 5. Patient information:
0 Age: 0 Gender: 0 herican society of Anesthesiologists classification
(selectone): 1 2 3 4 5 E Reason:
6. Preoperative laboratory test and examination results:
7. Anesthetic type and reason, if known:
8. !3equence of intraoperative medications administered: 0 Antibiotics 0 Antiemetics 0 Anti-inflammatories 0 Emergence 0 Induction and point of intubation 0 Inhalation agents 0 Iv anesthetics (eg, pentothal) 0 Localanesthetics 0 Musclerelaxants 0 Narcotics 0 Preoperative medication 0 Reversalagents
0 Preoperative 0 Induction 0 Emergence
0 Endotrachealtube 0 Laryngeal airway mask 0 Mask 0 Other
9. Name of medications and brief description of action:
10. Type of airway management (select one):
11. Postoperative course and medications:
1Z.Obtaining information from the patient’s medical chart or via a patient or nurse inteMew, summarize patient’s postoperative
0 pain and nausea management, 0 lengthofstayand 0 any complications.
course, including
American society of Anesthesiologists patient classification, the sequence of medication administered and the phar- macological actions, and postoperative course. The worksheet did not disclose patient identity. The RN participants were encouraged to ask relevant ques- tions about intubation, extubation, and
the sequence of anesthetic agents delivered relative to the time frame of the surgical procedure. The intraoperative observa- tion experience for the 23 participants was sched- uled during a five-month period.
PROGRAM EVALUATION According to the Stan-
dards of Perianesthesia Nursing Practice, 2002 edition,
professional behaviors inherent in perianesthe- sia practice are the acquisition and applica- tion ofu specialized body of knowledge and skills, accountability and re- sponsibility, communi- cation, autonomy, and collaborative rela tion- ships with others. lo (p5)
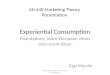
A vital part of this knowledge base is a strong comprehension of anesthetic agents and their delivery. Evalua- tions of the perceived benefits of this program were derived from the subjective evaluation forms filled out by the RN participants (n = 23) (Table 6). Analysis of the evaluation’s auantita tive
portion of the module (ie, qu’estions 1-8) indicate overall satisfaction. The aggre- gate data derived from the questions pertaining to knowledge enhancement (ie, questions 9-12) indicated that 98.1% of the respondents agreed or strongly agreed that the learning objectives had been achieved. These results strongly
282 AORN JOURNAL

AUGUST 2003, VOL 78, NO 2 Rosentreter - Talboy
suggest that the partici- pants perceived a greater understanding of anes- thetic agents and their actions. A majority of respondents (99.1%) per- ceived that an improved comprehension of anes- thetic agents would posi- tively affect their nursing care in the PACU.
Results from observa- tional evaluations (n = 23) (ie, questions 1-4) indi- cate that 94.5% of the respondents perceived an improved knowledge base, and 95.7% of the participants supported the statement (ie, ques- tion 5) that this experi- ence resulted in a better understanding of the postoperative nursing care required by patients (Table 7). Personal com- ments from this evalua- tion include “I enjoyed mv OR experience. The
TABLE 5 Evaluation of Intraoperative Observation
Scale: 1 = Strongly disagree 2 = Disagree 3 = Agree 4 = Strongly agree
As a result of this program, I am able to:
1. Define the use of the American Society of Anesthesio- logists’ classification system for a variety of patients.
2. List two indications for anesthetic selections in selected
1 2 3 4
patients. 1 2 3 4
3. Describe the sequence of anesthetic agents used in selected patients. 1 2 3 4
4. List two possible untoward effects of medications used and management of these complications. 1 2 3 4
5. Develop a better understanding of postoperative patient care. 1 2 3 4
This style of learning was a benefit to my professional development. 1 2 3 4
Recommendations for f u h offerings:
comments:
OR staff A d the surgeon were very good at explaining things to me and accommodating me” and ”. . . much appreciation for CRNAs and OR nurses for their patience and explanations of procedures while they worked.” An additional benefit of the intraoperative observation experience was that the RN participants were able to observe the circulating nurse in the patient’s contin- uum of physical and emotional care.
Anecdotally, two participants verbal- ly expressed anxiety and apprehension about their upcoming intraoperative observation experiences. One nurse described a previous fainting episode during her rotation in the OR as a stu- dent nurse. After discussing her previ- ous experience, this nurse did proceed and had a successful and rewarding
observational experience. A second nurse indicated that she preferred to observe conscious sedation in the endoscopy suite in lieu of an intraoper- ative experience, and this request was honored. A third nurse noted in her postobservational evaluation that she did not feel this intraoperative observa- tion experience was of value to her; however, she believed that the anesthet- ic agent component was informative.
RECOMMENDATIONS FOR EDUCATION AND CLINICAL PRACTICE
This pilot program provided a secure, self-directed learning environment based on adult learning and mentoring princi- ples. Using cognitive learning by com- pleting the anesthetics module to pre- pare for the intraoperative experience
AORN JOURNAL 285

AUGUST 2003, VOL 78, NO 2 Rosentreter - Talboy
_ _ - - - -- -
TABLE 6 Self-study Anesthetic Agents Module Evaluation Results
Strongly As a result of this program, I am able to disagree
1. discuss three desired effects of inhalation agents;
2. list two nursing considerations when caring for postanesthesia care unit patients who have received inhalation agents;
3. compare the basic actions of the barbiturates and induction agents (eg, propofol, etomidate, ketamine);
4. formulate a plan of nursing care based on potential postoperative effects from the ad- ministration of induction agents/barbiturates;
5. distinguish between the primary pharmaco- logical actions of depolarizing and nondepolarizing muscle relaxants;
6. recognize the potential for cholinergic crisis and tion after administration of muscle relaxants;
7. list three possible side effects after administra- tion of narcotic or benzodiazepine antagonists;
8. discuss two nursing interventions for resedation after reversal of narcotics or benzodiazepenes.
This offering was helpful to my professional development.
The format of this module was organized to make this material easily understood.
This style of learning was a benefit to my p e r ~ o ~ l development.
The content of this offering was relative to the program’s objectives.
o.oo/o
0.0%
0.0%
o.oO/o
0.070
0.0%
om0
0.0%
0.0%
0.0%
o.oo/o
o.o”/o
Disagree
0.0%
0.0%
0.0%
o.o”/o
o.oo/o
4.3%
4.3%
4.5%
o.o”/o
0.0%
0.0%
0.070
Agree
43.5%
34.8%
60.9o/u
56.5%
60.9%
39.1%
26.1%
18.2%
26.1 ‘10
56.5%
47.8%
34.8%
Strongly agree
56.5%
65.2%
39.1%
43.5%
34.8%
56.5%
69.6%
77.3%
73.9010
43.5%
52.2%
65.2%
Twenty-three people responded to questions 1 through 4 and 6 through 8. Only 22 people responded to question 5, so it does not total to 100%.
awarded the nurse a meaningful and thought-provoking experience. To determine the efficacies of these learn- ing tools, a pretest could be adminis- tered before participation in this pro- gram to measure changes in specific knowledge. Suggestions for improving the mentor/CRNA process include
~~
direct selection of the CRNAs most interested in teaching participants. Using the primary coordinating CRNA for communication and scheduling was an integral part of the planning process. Sensitivity to the needs of RNs who choose not to observe is essential in planning an intraoperative observation.
286 AORN JOURNAL

AUGUST 2003, VOL 78, NO 2 Rosentreter - Talboy
_._ ~ __ ~ ~~
TABLE 7 Intraoperative Observation Evaluation Results (n = 23)
Strongly Strongly As a result of this program, 1 am able to disagree Disagree Agree agree
1. Define the use of the American society of Anesthesiologists' classification system for a variety of patients. 0.0'%1 4.5% 50.0% 45.5"/0
2. List two indications for anesthetic selections in selected patients. 0.0Y" 4.3% 52.5"/0 43.5%
3. Describe the sequence of anesthetic agents used in selected patients. O.oY0 4.3% 56.5% 39.1'/0
4. List two possible untoward effects of medications used and management of these complications. 0.O0/" 8.7"/0 52.2% 39.1%
5. Develop a better understandmg of postoperative patient care. 0.0% 4.3Y" 43.5% 52.2Yo
This style of learning was a benefit to my professional development. 0.0% 4.3% 30.4% 65.2%
An alternative experience can be planned for these individuals. Seren- dipitously, it was identified that partic- ipants should eat breakfast before their intraoperative observation experience.
The positive responses from this learning experience have prompted POHA nursing educators to request an expansion of this program to include their staff members. By following the steps delineated in this article, this pro- gram easily could be replicated in a variety of hospital settings.
RECOMMENDATIONS FOR RESEARCH A tool linking nursing competency
and patient satisfaction in perianesthe- sia units could be developed. This tool could be comprised of a pretest and the- ory-based posttest, skill laboratory assessment to measure progression in nursing behaviors and a self-evaluation and preceptor evaluation. Patient satis- faction could be measured through a questionnaire or interview.
SUMMARY The survey results evaluating this
pilot program strongly suggest the PACU RN participants enjoyed this learning experience and found it to be
helpful in their nursing practice. In gen- eral, participants agreed that this didac- tic and experiential program enhanced the unique knowledge base required of PACU RNs. This experience also allowed PACU RNs a greater apprecia- tion of the professional and compassion- ate behaviors practiced by perioperative nurses. Most importantly, this experien- tial and didactic approach integrates the intrinsic art of nursing with the intellect of bedside nursing care. *:*
Janet Rosentreter, RN, BSN, is a staff nurse in the medical imaging and PACU departments, St Luke's Regional Medical Center, Boise, Idaho.
Mary Lynn Tdboy, RN, MSN, is a staff nurse in the PACU, St Luke's Regional Medical Center, Boise, Idaho.
Editor's note: The authors would like to thank Sherry Boyer, RN, BSN, department director; Reuben Dyck, RN, MSN, clinical instructor; Dessa Lagerstrom, EdD, pro- gram development coordinator; Lisa Baratcart, supervisor Anderson Center; Cathy Mayes, administrative assistant; and the anesthesia, surgical, PACU, and perioperative nursing staff members at St
AORN JOURNAL 287

Lukes Regional Medical Center, Boise, Idaho, for their encouragement and assis- tance with the project.
NOTES 1. J C Rothrock, ”Foundations for practice,” in Alexander’s Care of the Patient in Surgery, 12th ed, J C Rothrock, ed (St Louis: Mosby,
2. S C Beyea, “Nurses making a difference one life at a time,“ AORN Journal75 (May 2002) 1005. 3. R Steinbrook, ”Nursing in the crossfire,” The New England Journal of Medicine 346 (May 30,2002) 1764-1765. 4. J C Reid, ”Adult learning, An online education sourcebook,” National Library of Medicine, http://collab.nlm.nih.gov/tutorial spublicationsandmaterials/sourcebookhadultlear ning.htm1 (accessed 26 June2003). 5. P Benner, J Wrubel, ”Skilled clinical knowledge: The value of perceptual aware- ness, Part 2,” Journal of Nursing
I ~ c , 2003) 1-16.
Administration 12 (June 1982) 28-33. 6. A T Speers, L Ziolkowski, “Preparing for the future: Perianesthesia orientation,” Journal of Perianesthesia Nursing 11 (June
7. “Blueprint for: Curricula development for the role of the perioperative nurse anes- thesia (PNA) and surgery (PNS),” Canadian Operating Room Nursing Journal 14 (December 1996) 16-20. 8. J Needleman et al, “Nurse staffing levels and the uality of care in hospitals,” The New EnJand Journal of Medicine 346 (May 30,2002) 1715. 9. J Rosentreter, M L Talbo L Thomason, Anesthesia Module for St Lu&s Postanesthesia Care Unit Nurses (Boise, Idaho: St Luke’s Regional Medical Center, 2000). 10. American society of Perianesthesia Nurses, Standards of Perianesthesia Nursing Practice, 2000 edition (Cherry Hills, NJ: American society of Perianesthesia Nurses, 2000) 5.
1996) 133-142.
~
Report Shows Disparities in Facilities‘ Donation Rates report from the Office of Inspector General
A ( O I G ) h as revealed that the rate of consent for organ donation varies widely among transplant cen- ters a t the national, regional, and local levels, according to a June 2, 2003, news release from OIG. The report was undertaken to provide data for OIG‘s efforts to raise awareness about the impor- tance of organ donation. Documenting the variation among centers w i l l help identify centers that have the potential to increase the number of donors, a step toward narrowing the gap between the need for and availability of organs for transplantation. The report includes an analysis of 190 transplant centers and 51 organ procurement organizations nationwide from August 2001 to November 2002.
Consent rate i s defined as the number of patients for whom consent to donate organs was given as a percentage of all patients at the facility who were medically eligible to donate organs. Eighteen of the transplant centers were found t o have a consent rate below 30%. Had these 18 cen- ters been able to obtain consent a t the average
rate (ie, 54%) of the other 172 centers studied, they would have obtained approximately 450 more organs for transplantation.
ters with low consent rates are located i n urban areas. Data also reveal that hospitals with a larger number of transplantation programs and procedures experience slightly higher consent rates. The study does not explain the differences i n consent rates; however, it identifies areas in which the opportuni- ty to increase organ donations exists.
More than 80,000 Americans currently are awaiting organ transplants. I n 2002, fewer than 25,000 people received transplants, and 6,400 people died while waiting for organs to become available.
Among the report‘s findings are that many cen-
Wide Variation Among Transplant Centers in Procuring Organ Donors (news release, Washington, DC: Ofice of Inspector General, June 2, 2003) http://oig. hhs.gov/pub lications/docs/press/2003/060203release.pdf (accessed 2 June 2003).
288 AORN JOURNAL