Embed Size (px)
Citation preview

Behav. Res & Therap). 1071. Vol 15. pp. l-16 Pergamon Press Prmted m Great Bntam
It is plain from the burgeoning literature on the treatment of nocturnal enuresis by
A CONTROLLED TRIAL OF THE TREATMENT OF NOCTURNAL ENURESIS IN RESIDENTIAL HOMES
FOR CHILDREN
D. JEHU, R. T. T. MORGAN, R. K. TURNER and A. JONES Child Treatment Research Unit, School of Social Work. University of L&ester.
Leicester LEl ?LA, England
(Rrceiced 27 July 1976)
Summary-The present study was undertaken to evaluate the practicability and efficacy of treat- ing enuretic children in residential Children’s Homes by means of the enuresis alarm. A control group design was employed with 19 and 20 subjects in the treatment and control groups tespect- ively. Eighteen of the nmeteen treatment group children achieved initial arrest of enuresis in a mean of 11.9 weeks of treatment (range 5-28 weeks). Over the initial 12-week period, the treatment group showed a statistically significant reduction in mean wetting frequency, both over time and in comparison with the control group. After a follow-up period of at least 20 months. 17 of the 19 children were known to be dry. The results of an independent evaluation are reported, and it is concluded that alarm treatment is as effective and practicable in Children’s Homes as it is in famiiy situations.
the “bell and pad” method (Morgan, 1975; Morgan and Young, 1972; Turner, 1973) that this approach compares very favourably with psychotherapy (Werry and Cohrssen, 1965; De Leon and Mandell, 1966) as well as with drug therapies (McConaghy, 1969). The enuresis alarm has been suc~ssfully used in a variety of settings, including school health clinics (e.g. Young and Morgan, 1972a) and general practice (Mann et al., 1975). A consensus of the published studies indicates an initial success rate for alarm treatment of about 80% within the relatively brief period of approximately 8 to 10 weeks (Morgan and Young, 1972; Turner, 1973). Also, there have been several trials which indicate a definite treatment effect in comparison with control procedures, at least when these extend over a period in excess of one month (Baker, 1969; Collins, 1973; Finlay et al., 1973). Furthermore, while it has been common for the relapse rate to be as much as 30% (Turner, 1973), a simple modification of treatment to include a period of over- learning has been found to reduce this figure substantially (Young and Morgan, 1972b; 1972~; Taylor and Turner, 1975). Finally, it has been established with reasonable confi- dence that the functioning of enuretic children does not deteriorate in other respects once this problem has been treated (Baker, 1969; Sacks et af.. 1974).
The incidence of enuresis is particularly high amongst children in residential homes (Stein and Susser, 1967; Douglas, 1970; Yule and Raynes, 1972) and for this reason there is an urgent need for careful evaluative research of its treatment in this setting (Rutter, 1973). Enuresis is not only socially distressing for the child who lives in residen- tial care, but it also imposes serious restrictions upon plans for fostering or return to parents, for many adults do not easily tolerate children who have failed to gain sphincter control. A good example of this lack of tolerance is provided in the literature on non-accidental injury to children where, next to crying, incontinence has emerged as the second most commonly stated reason for assaults (Kempe and Helfer, 1972). Although the extensive research literature testifies to the efficacy of alarm treatment, al1 but a few of published studies describe its use in natural homes under outpatient supervision, and relatively little is known about the effectiveness, or indeed, the practica- bility. of this form of treatment in the context of residential institutions. There has been only one published report* on its use in residential accommodation (Davidson and Douglass, 1950). and this described the treatment of twenty cases, including adults
*Since writing this paper it has been pointed out that the classic paper by Mowrer and Mowrer (1938) described their use of the bell and pad in a Children’s Home.

2 D. JEHL. R. T. T. MORGAX. R. K. TURE;ER and A. JONES
as well as children, in a hostel setting. It is clear from the high rate of premature termination of treatment (Young and Morgan, 1972a; 1972d) that there are social limi- tations to alarm therapy insofar as it imposes very heavy demands upon those caring for the child during such treatment in natural homes. In institutions, it was envisaged that this form of treatment might be even more difficult to apply because of such factors as the multiplicity of the staff who care for children and the disturbance that a noisy alarm might cause in dormitories. Therefore, a controlled evaluation was under- taken of both the effectiveness and practicability of “bell and pad” treatment when used in Children’s Homes.
METHOD
Design
Children suffering from nocturnal enuresis were identified by a survey of all the Children’s Homes operated under the auspices of the City of Birmingham Social Services Department. These clients were then allocated at random to one of two groups: (a) a potential treatment group, who would receive treatment immediately after a 28-day baseline period; or (b) a potential control group. for whom houseparents were to be requested to keep a record of wetting incidence for a period of 4 months (after which the investigators undertook to treat all these children outside the trial wherever this was considered still desirable at the conclusion of the control period). Within this research design it was possible to compare the response of treated children, first with untreated controls, and secondly with their own baseline, pretreatment records of the frequency of enuresis.
Selection and allocation of subjects
The survey identified 101 children who were enuretic according to the following cri- teria: (i) age four years or over; (ii) wetting frequency of at least four nights in the initial 28 day period; (iii) if of school age, attending normal rather than special school; (iv) not previously treated by the alarm method within one year; (v) having no gross physical handicap. Some children were then excluded from the study since treatment was impractical (e.g. children who spent only school holidays and/or weekends in the Home). These exclusions reduced the total group of potential cases to 93 children who were then allocated at random to the potential treatment or control group, comprising 47 and 46 cases respectively.
In each of these cases, the child’s general medical practitioner was asked to complete a brief questionnaire about any known physical factors of possible relevance to the enuresis, a mid-stream specimen of urine was sent for pathological investigation, and the child was only included in the trial if known to be free from infection and to have no relevant organic pathology.
In the potential treatment group the decision to proceed with the “bell and pad” procedure was subject to the following additional criteria: (i) the child’s houseparent and social worker accepted the offer of treatment and there was no objection from the senior social worker who supervised the residential home; (ii) the child was in agreement with treatment; (iii) there were no clinical grounds that contraindicated treat- ment; (iv) the child’s GP did not object to treatment; (v) no other child in the same establishment was under treatment by the alarm method (it was felt to be unreasonable to expect residential child care staff to cope with more than one such treatment at a time).
Out of the 93 potential subjects identified in the survey, 61 were excluded from the investigation for any of several reasons (see Table 1). It was therefore necessary to supplement this original sample by a second, but smaller survey of children who had entered the city’s establishments since the time of the original survey. The children who were identified in the second survey were then randomly allocated to the two groups until a complement of 20 cases had been reached in each group. However,

The treatment of nocturnal enuresis
Table 1. Reasons for the exclusion of identified cases
Potential treatment
group
Potential control group Total
Dry or very infrequently wet Discharged from care or home on trial Placed at residential special school Under treatment for enuresis elsewhere Treatment not practicable Tranferred to Children’s Home outside dept. Treatment not desired by housemother Current alarm treatment of another child in same
establishment Alarm treatment within previous year
(child therefore recently relapsed) Child considered to be retarded Child absconded Child fostered Treatment not desired by social worker Chitd considered to be grossly disturbed:
treatment inapprop~ate Child encopretic Relevant physical abnormality Child being treated by Imipramine for depression
6 8
9 4 4 3
2 2
0
0 2 0 0
0
2 0
0 1 0 0
15 12 5 4 4
2 2 2
32 29 61
one child had to be excluded from the treatment group when she was found to have a urinary tract infection and it was not possible to replace this child; consequently, the treatment group comprised only 19, as opposed to the expected 20 children.
Treatment procedure
The procedure followed is fully described in a manual (Morgan, 1975) that is available from the Child Treatment Research Unit (CTRU). It began after the completion of a 28-day baseline period, the houseparents having already been asked to discontinue any existing management procedures (e.g. lifting, fluid restriction) when they started to keep the baseline record. The Eastleigh MOH 7 enuresis alarm was used to rouse the child ~manufactur~ by N. H. Eastwood & Co., London). This equipment conforms to the Department of Health and Social Security safety s~ifications (Ministry of Health, 1968). It comprises a buzzer box which is triggered (at the onset of urination) by means of a pair of metal gauze detector pads of the sandwich type. The alarm buzzer can be set at any one of 3 intensity levels. In addition, there is a small light which is illuminated at the same time. Staff were asked to make sure that the child got up and went to the toilet after each alarm triggering; they were also asked to help remake the bed and reset the alarm if this was considered practical.
Although changes in procedure were made in the light of experience with each case, treatment usually continued until fourteen consecutive dry nights had been recorded. At this stage overlearning was introduced whenever practicable: the child was requested to increase fluid intake just before bedtime (usually between 1 and 2 pints), but to continue using the alarm. Thereafter, treatment continued until the child had been dry for another period of fourteen consecutive nights. The results of two studies indicated that there is a marked reduction in rates of relapse following overlearning (Young and Morgan, 1972b; 1972c), and this was the reason why this modification to the alarm treatment was used.
There was no criterion of failure in the present study. In all cases treatment continued either until the cessation of the bedwetting or. as in one case, therapy had to be discon- tinued for practical reasons.
At the start of treatment all children in the sample were living in residential Children’s Homes. However. in several cases children were moved subsequently, either to different

4 D. JEHL. R. T. T. MORGAL R. K. TURNER and A. JONES
residential establishments, or to their own natural homes. and therapy continued in the new placement. Where children went home for weekends there was no attempt to continue treatment in the natural home as this was usually considered to be impracti- cal; thus in six cases the treatment was concentrated mainly on weekdaays. This is clearly a practical difficulty that arises when therapy takes place amongst children in residential care, but who have some contact with the outside world. Those most directly
involved with treatment were the residential staff of each Children’s Home. although in a number of cases the children themselves became responsible for conducting their own therapy. The assessment and regular supervision of each case was carried out by one of the CTRU therapists who visited or telephoned each Home, normally at about weekly intervals.
Control procedure
The assessment of all children in the control group was identical to that of cases who had been allocated to treatment. Houseparents were requested to keep a record of wet and dry nights for at least three months and, if possible, for an additional month. The houseparents were not asked to change their usual way of managing the enuresis; thus, they continued to lift some children, while in other cases the child remained on a restricted fluid intake. This was because it was considered unreasonable to ask houseparents to stop all other attempts to manage the enuresis; furthermore
it provided a more realistic control procedure insofar as treatment was then being compared with the normal way of handling enuresis in a Children’s Home. After the 3 or 4 months of control recording all children were offered treatment if this was still considered desirable; to this extent, the control procedure also took into account any improvement that might have occurred due to the effects of assessment, monitoring and expecting treatment.
Follow up procedure
Eighteen of the original 19 children were discharged as soon as they had achieved the initial criterion of being dry overnight for a period of two weeks, usually after a period of overlearning. Follow up was then by telephone enquiry to the Home, initially at monthly intervals, and later after periods of three months. At the time of discharge the staff had been invited to contact the therapist should they be concerned about any recurrence of bedwetting.
Six months after discharge from treatment the therapist visted the Home where he interviewed the staff and saw the child. A report was obtained from the school. and in some cases the natural parents were seen.
Independent ecaluatiorl
The independent assessor (AJ) visited each Home and discussed the treatment with all who were concerned in the present care of the child, in one case this being the natural mother in the child’s own home. In some cases, where children had moved to other Homes, or had returned to their natural home, the assessor visited the staff of the Home where treatment was originally conducted. The interview was semi-struc- tured insofar as the assessor and staff completed and commented on a number of ratings which described both the present state of the child’s enuresis and several aspects of treatment.
In 16 of the 18 cases it was possible to interview the staff who had been caring for the child during treatment, and in 12 of these 16 the children were still in the same Home and in the care of the same staff. In one case where the staff were not available, only the child was interviewed, and in another case the interview was with a member of staff who had indirect knowledge of the child’s treatment. The period of time from the end of treatment to the date of interview ranged from 7 months to 18 months. The interviews took from 45 to 75 min, depending on whether the child was seen as well as staff.
The treatment of nocturnal enuresis 5
Sex and age DESCRIPTION OF SUBJECTS
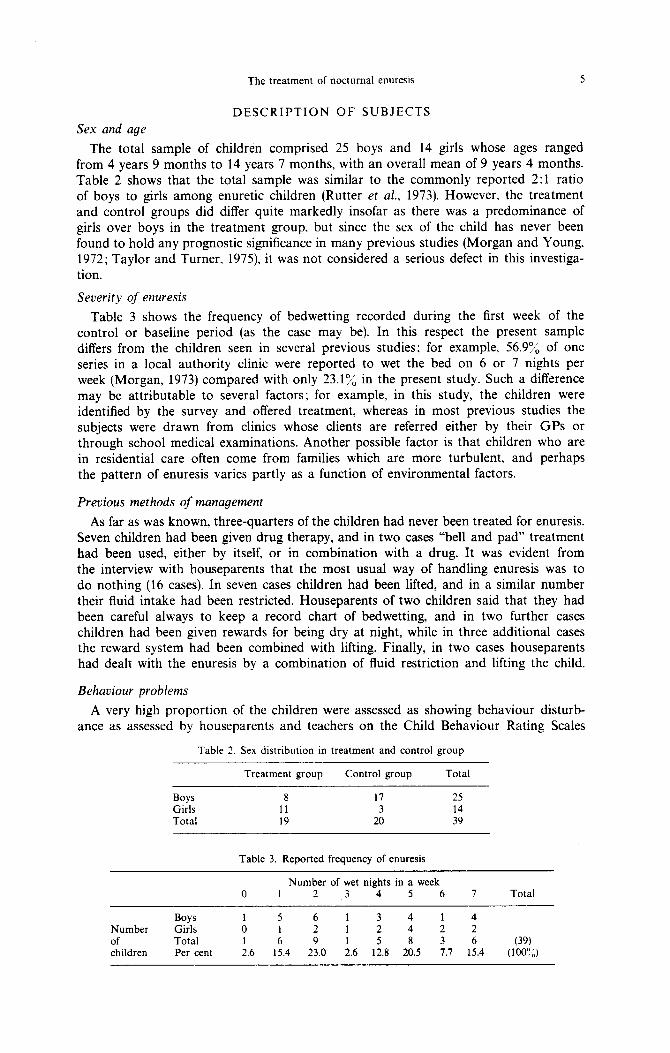
The total sample of children comprised 25 boys and 14 girls whose ages ranged from 4 years 9 months to 14 years 7 months, with an overall mean of 9 years 4 months. Table 2 shows that the total sample was similar to the commonly reported 2:l ratio of boys to girls among enuretic children (Rutter et al., 1973). However, the treatment and control groups did differ quite markedly insofar as there was a predominance of girls over boys in the treatment group, but since the sex of the child has never been found to hold any prognostic significance in many previous studies (Morgan and Young, 1972; Taylor and Turner, 1975) it was not considered a serious defect in this investiga- tion.
Severity of enuresis
Table 3 shows the frequency of bedwetting recorded during the first week of the control or baseline period (as the case may be). In this respect the present sample differs from the children seen in several previous studies; for example, 56.97; of one series in a local authority clinic were reported to wet the bed on 6 or 7 nights per week (Morgan, 1973) compared with only 23.1 “/, in the present study. Such a difference may be attributable to several factors; for example, in this study, the children were identified by the survey and offered treatment, whereas in most previous studies the subjects were drawn from clinics whose clients are referred either by their GPs or through school medical examinations. Another possible factor is that children who are in residential care often come from families which are more turbulent, and perhaps the pattern of enuresis varies partly as a function of environmental factors.
Previous methods of management
As far as was known, three-quarters of the children had never been treated for enuresis. Seven children had been given drug therapy, and in two cases “bell and pad” treatment had been used, either by itself, or in combination with a drug. It was evident from the interview with houseparents that the most usual way of handling enuresis was to do nothing (16 cases). In seven cases children had been lifted, and in a similar number their fluid intake had been restricted. Houseparents of two children said that they had been careful always to keep a record chart of bedwetting, and in two further cases children had been given rewards for being dry at night, while in three additional cases the reward system had been combined with lifting. Finally, in two cases houseparents had dealt with the enuresis by a combination of fluid restriction and lifting the child.
Behaviour problems
A very high proportion of the children were assessed as showing behaviour disturb- ance as assessed by houseparents and teachers on the Child Behaviour Rating Scales
Table 2. Sex distribution in treatment and control group
Treatment group Control group Total
Boys 8 17 25 Girls I1 3 14 Total 19 20 39
Table 3. Reported frequency of enuresis
0 Number of wet nights in a week
1 2 ,3 4 5 6 7 Total
Boys 1 5 6 1 3 4 1 4 Number Girls 0 1 2 1 2 4 2 2 of Total 1 6 9 1 5 8 3 6 (39) children Per cent 2.6 15.4 23.0 2.6 12.8 20.5 7.7 15.4 (100’:“)
6 D. JEHL-. R. T. T. MORGAN. R. K. TURNER and A. JONES
Table 4. Proportions of children showing deviant* scores on Child Behaviour Rating Scale: comparison with prevtous samples
A2 (parent) scale Boys Giris
B? (teacher) scale Boys Girls
Present sample (n = 39) Isle of Wight study
(Rutter et al.. 1970) Children in care
(Yule and Raynes, 1972)
68.0”” 57.1”,, 42.9O,, 35.1”,,
8.06”, 5.56”, 10.04”,, 5.05””
29.79”,, 23.910,, 38.83”,, 36.96”,,
* $9 on Teacher (B2) Scale and 3 13 on Parent (AZ) Scale
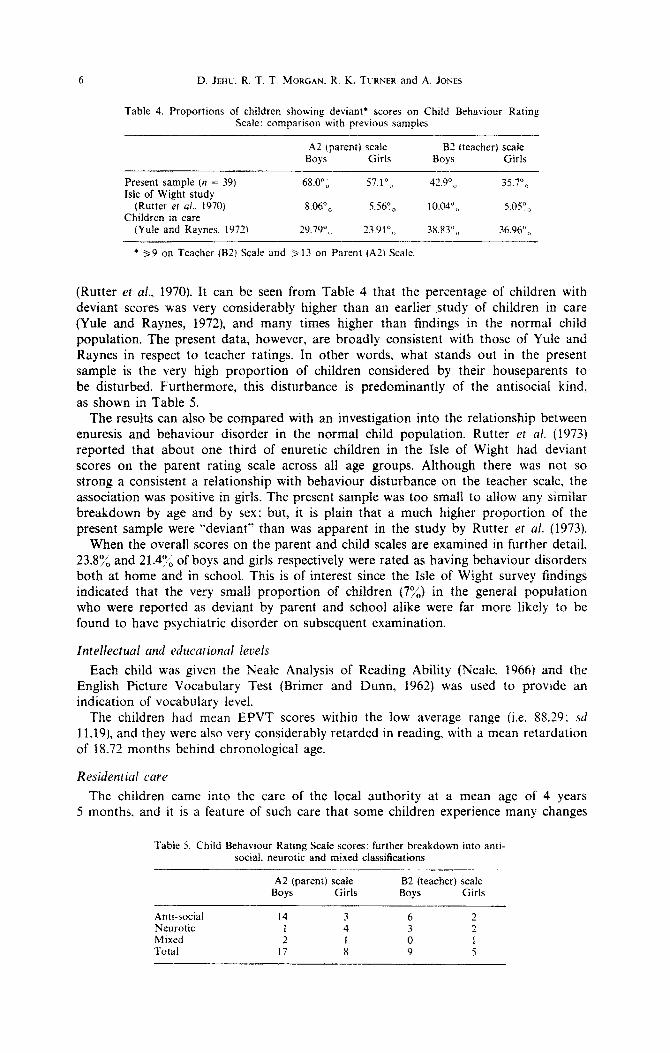
(Rutter et al., 1970). It can be seen from Table 4 that the percentage of children with deviant scores was very considerably higher than an earlier study of children in care (Yule and Raynes, 1972), and many times higher than findings in the normal child population, The present data, however, are broadly consistent with those of Yule and Raynes in respect to teacher ratings. In other words, what stands out in the present sample is the very high proportion of children considered by their houseparents to be disturbed. Furthermore, this disturbance is predominantly of the antisocial kind, as shown in Table 5.
The results can also be compared with an investigation into the relationship between enuresis and behaviour disorder in the normal child population. Rutter er al. (1973) reported that about one third of enuretic children in the Isle of Wight had deviant scores on the parent rating scale across all age groups. Although there was not so strong a consistent a relationship with behaviour disturbance on the teacher scale, the association was positive in girls. The present sample was too small to allow any similar breakdown by age and by sex: but, it is plain that a much higher proportion of the present sample were “deviant” than was apparent in the study by Rutter et ul. (1973).
When the overall scores on the parent and child scales are examined in further detail, 23.8% and 21.474 of boys and girls respectively were rated as having behaviour disorders both at home and in school. This is of interest since the Isle of Wight survey findings indicated that the very small proportion of children (7%) in the general population who were reported as deviant by parent and school alike were far more likely to be found to have psychiatric disorder on subsequent examination.
Intellectual and educational levels
Each child was given the Neale Analysis of Reading Ability (Neale. 1966) and the English Picture Vocabulary Test (Brimer and Dunn, 1962) was used to provide an indication of vocabulary level.
The children had mean EPVT scores within the low average range (i.e. 88.29; sd 11.19), and they were also very considerably retarded in reading, with a mean retardation of 18.72 months behind chronological age.
The children came into the care of the local authority at a mean age of 4 years 5 months. and it is a feature of such care that some children experience many changes
Table 5. Child Behaviour Rating Scale scores: further breakdown into antt- social. neurotic and mixed classifications
A2 (parent) scale Boys Girls
B2 (teacher) scale Boys Girls
Anti-social 14 3 6 2 Neurotic 1 4 3 2 Mixed 2 t 0 1 Total 17 a 9 5

The treatment of nocturnal enuresis 7
and breaks, so that there is limited continuity in their relationships with the adults who look after them. The present sample was no exception. The median number of changes of placement that these children had experienced was two occasions; however, the range was very large, varying from 0 to 19 changes of placement. Amongst reasons for such changes are readmissions to Children’s Homes after the breakdown of a foster placement, boarding out in each of several short stay foster homes. and transfers from one residential establishment to another. On average these children had been placed in three different Children’s Homes (range l-8); and they had spent an average of 27.95 months (range 2-80 months) in their current placement. They had been in care for a mean of 58.62 months at the time of the first interview (range 6-154 months). Statistical analysis did not reveal any significant differences between treatment and con- trol groups in respect of the number of placement changes or any other indices of experience while in care.
The present sample of 39 enuretic children lived in 34 Children’s Homes, which ranged in size from small family units of four children to a large residential nursery where there were 53 children; the median number of children in a Home was 12. In the subjects’ bedrooms, the number of children varied from one up to nine children, with a median of four per room. Only one subject had a room of his own; this compared with 37.6% of children who had their own room in a study of treatment of children attending a local authority enuresis clinic (Morgan, 1973). The total number of adults (including both full- and part-time staff, domestic and ancillary workers) who were in regular contact with the children in each Home ranged from 4 to 36, with a median of 9. In sum, treatment was conducted in what is probably a fairly typical cross-section of residential Children’s Homes; and this study has evaluated “bell and pad” treatment when used under conditions that are in some respects very adverse, such as the number of children sharing a bedroom and the multiplicity of adult caretakers,
Twenty (51.4%) out of the 39 children maintained regular contact with their natural homes, and in a further 15 cases (38.5%) there was occasional contact with relatives; four children had no contact whatsoever with any relative.
RESULTS
Wetting frequencies in treatment and control groups
Inspection of Fig. 1 indicates a very considerable reduction in the mean wetting frequency in the treatment compared to the control group, as well as a massive reduction within the treatment group from their own baseline period.
C-7-4 = Control (N. 201 -= Treatment (N-19)
2 3 ii 5 6 7 8 9 10 11 12 13 Il. 15 16
Weeks
Fig. 1. Mean number of wet nights per week in treatment and control groups.

8 D. JEHC. R. T. T. MOKGAX R. K. TURNER and A. JONES
The mean frequencies of wetting in treatment and control groups were compared by a 2-way analysis of variance with repeat measures on one factor (Winer. 1962). Due to a loss of some of the control children from the study during the last four weeks of the comparative trial, the statistical analysis concerned only the first 12 weeks. The main effects of groups (F = 19.8807, @= 1,36, f< 0.001) and weeks (F = 7.3511. ~!f = 11,396, f < 0.001) were both significant. But. as the interaction term was also signifi- cant (F = 5.5851. df= 11.396, p < 0.001). subsequent analyses were made on each group separately. Mean bedwetting frequencies in the control group did not differ significantly over the 12-week period (F = 0.9678, df = 11,209, p > 0.05). On the other hand, a similar analysis of means in the treatment group indicated a highly significant treatment effect during the same 12-week period (F = 16.5068, df= 11,187, p < 0.001). The mean fre- quency of bedwetting in the first week of treatment differed significantly from all sub- sequent weeks, This is also very plain from Fig. 1 which shows that the marked drop in bedwetting frequency began from the first week onwards, indicating that the response to treatment was much earlier than in at least one previous report where there seemed to have been no significant treatment effect until after the first month (Turner et al., 1970).
The response of children to treatment was analysed further, using the Newman-Keuls procedure (Winer, 1962) for testing differences between all pairs of means (and including the four baseline weeks as well as the 12 weeks of treatment. There was a highly signifi- cant difference over this period (F = 21.6970, df = 15,255, p < 0.001) and baseline means were found to differ significantly from all subsequent means of the third week of treat- ment and onwards.
It is of interest that in the control group there was a tendency for the frequency of bedwetting to drop both during the first 2 weeks when a record was kept, and from the 13th week. These two trends both coincided with increased levels of therapist contact with the child during initial and final assessments. The importance in alarm treatment of non-specific factors such as attention from the therapist and an increased interest in the child is generally acknowledged, and perhaps one might expect their effects to be exaggerated when dealing with children who so rarely are visted by people from outside the Home.
Initial success and failure
Table 6 shows that all but one of the children in the treatment group ceased to wet the bed. In the one case of failure, the child absconded from his residential home within a few days of the start of treatment, and, in fact, it is arguable whether the “bell and pad” was ever used consistently even for this short period (there is no reason to believe that he absconded because of the start of the “bell and pad” treatment as he had previously been a persistent absconder). Since absconding might reasonably be expected to arise when working with children in residential establishments, it seems appropriate to regard the case as an instance of failure of treatment.
Frequencjs of relapse
There is no general agreement about what constitutes a relapse following treatment of enuresis, and the published research literature contains a very wide variety of differing definitions. Since any such definition is completely arbitrary, it seems more relevant in the present paper to describe cases as having relapsed only when this was sufficiently serious for further treatment to be requested by child care staff. However, comprehensive
Table 6. Number of children in the treatment group who achieved the criterion of initial success
Boys Girls Total
Success Fail Total 7 1 8
11 0 11 18 1 19

The treatment of nocturnal enuresis 9
information is available about intermittent and minor recurrences of the enuresis, and these data are also presented below. It is hoped that by describing the current state of all children as accurately and with as much detail as possible, readers can draw their own conclusions about the effectiveness of therapy taking into account not only cases of obvious relapse, but also instances where children had experienced occasional night wetting.
All the children have been followed up for at least 20 months, and in many cases for considerably longer. Within the first 6 months after discharge, three children had relapsed to the extent of requiring retreatment. These children relapsed 5, 8 and 24 weeks respectively after discharge. In one other case a relapse occurred 32 weeks after discharge. If we count as a relapse the case whose treatment could not be completed or followed up, then the total number of relapses was 4 (22.2%) out of 18 children at 6 months, and 5 (27.8%) out of 18 over the longer period of 20 months’ follow
up. Now that all the children have been followed up for at least 20 months, it is possible
to summarise what has happened to the 19 children who were allocated to the treatment group. The overall results are shown in Table 2. In one case treatment had to be stopped after only a few days, since the boy was persistently absconding and was sent to a Community School; thereafter therapy was impractical. This case is counted as the only total failure of treatment. The remaining 18 children (i.e. 95% of the total) achieved the criterion of two weeks’ continence, and all but one of these are now dry. The exception is a child whom it was not possible to monitor in the follow up, but who is now known to be still enuretic. Four other children did require a second or third course of treatment, but they are now substantially dry.
Occurrence of occasional wetting incidents amongst non-relapsed children
Five children were reported never to have wet the bed at all after discharge; treatment appears to have brought about a very marked change, since four of these children had previously been enuretic at least five times per week. In one case there was a very marked recurrence of enuresis within the first three months after discharge. This child was being considered for retreatment, but it was not possible to commence it because another child in the Home had begun to use the alarm; by the time this latter child became dry, there had been a natural remission of the enuresis in the relapsed child. In the remaining cases, isolated wetting incidents tended to occur about two or three times a month.
Precipitants for recurrence of enuresis
It would be wrong to assume that there is necessarily a causal relationship when the recurrence of enuresis follows some event which is presumed to be stressful for
Table 7. Summary of the results of treatment of nocturnal enuresis with long term follow up
Outcome
At conclusion of initial treatment: Dry Treatment discontinued (counted as
failure)
Total
On follow up after being dry initially: Still dry, without retreatment Now dry, after retreatment No information (counted as not dry-
later known to have relapsed
Total
Number (N = 19)
18
1
19
13 4
1
18
10 D. JEHU. R. T. T. MOKGAN. R. K. TURNER and A. JONES
the child. However, it is still very relevant to consider the available evidence regarding any possibly precipitant events that might be related to relapse. Taking first those children whose relapse was serious enough to merit consideration for retreatment, the analysis of case notes did reveal events which staff believed to have triggered a relapse in three out of the four cases.
One girl relapsed after an upsetting visit by a putative father; also there were serious staff difficulties in the Home. some of which concerned her directly. Another girl relapsed at the time of a move from one Home to another, and when there were family difficulties. Staff reported that the wetting recurred after she had been told that she was to change placement, and apparently disruptions occurred also at her natural home following the remarriage of her father. The boy who relapsed after 32 weeks of continence was said to have been very upset by a visit from his mother when the latter was drunk and abusive. Also, an attempt to establish suitable conditions for the boy’s return home “on trial” had been unsuccessful. In the one remaining case there seems to have been no significant event at all.
Rather less information is available about coincidentally stressful events among those children who experienced occasional wet beds. One child experienced briefly a slight reversal when the central heating was turned off and she was also said to wet on occasions during cold weather. A girl wet the bed for two nights at the time of a change of houseparents and when she also started at a new school.
It is perhaps of relevance that many of the remaining children had experiences that might have been stressful, without any relapse or even minor wetting incidents at all. For instance, two children had appeared in court over quite serious offences; one child had been transferred to a foster home, and another had just started at a new school and gone through the process of adjusting to being home on trial. Similarly, one other boy had started at a new school.
Other indices of outcome
During the initial assessment the housemothers and class teachers were asked to make ratings on 5-point scales of (i) each subject’s ability to mix with other children, and (ii) his degree of behaviour disturbance compared to other children in the Home or class. In addition. the housemothers were asked to describe the child on a set of 54 bipolar adjectival scales (Becker. 1960) which provide five factors which seemed to describe parent/child relationships: (i) hostility/withdrawal; (ii) relaxed disposition; (iii) lack of aggression; (iv) submissiveness. and (v) conduct problems. These 54 scales comprised a derivative of Becker’s scales (Patterson and Fagot, 1967) and a further seven scales with high loadings on a general evaluative factor (Osgood et al., 1957). To obtain some assessment of child’s self concept, the Coopersmith Self Esteem Inven- tory (Coopersmith, 1967) was administered: on a pre-recorded tape because of the read- ing difficulties exhibited by many of the children.
All these measures were repeated at the conclusion of treatment, but on none of them was any significant difference found either between the first and second adminis- trations, or between the treatment and control groups.
Duration of treatment
A recent review of the literature suggests that the duration of an average “bell and pad” treatment lasts from 8 and 10 weeks (Turner, 1973). There was a considerable range in the duration of treatment in the present study; at one extreme one child was dry to the criterion of 14 nights within 5 weeks, while at the other extreme therapy lasted for 28 weeks. The mean time for treatment (including the overlearning period) was 11.9 weeks, which is markedly shorter than that reported by Young and Morgan (1972b) in another study of alarm treatment with overlearning; but similar to that reported by Taylor and Turner (1975) who used the same approach in an outpatient setting. The present results are consistent with several earlier findings which indicated
The treatment of nocturnal enuresis 11
that the duration of treatment is unrelated to the age or sex of the children (Turner et al., 1970; Morgan and Young, 1972; Taylor and Turner, 1975).
Practical dificulties
There were four cases in which overlearning was either not attempted, or had to be abandoned. In one case, the child was discharged home to her mother as soon as she had been dry for 14 nights and before the child could start on overlearning. In a second case, the child was transferred to another Children’s Home where further treatment was impractical. Overlearning had to be abandoned in two other cases after a massive deterioration in wetting which did not improve with time.
One other practical difficulty was that of false alarms when the equipment was trig- gered by sweat. In three cases these alarms occurred very frequently, and in ten further instances they were occasional. Certainly, the problem of false alarms made the super- vision of treatment much more difficult for residential child care staff. It is of interest that there were few reports of difficulty in arousing children.
INDEPENDENT EVALUATION
Attribution of change
In each case the staff member most closely involved in the treatment of the child rated the extent to which the introduction of this form of treatment was considered to have brought about the reduction in wetting frequency, as distinct from the influence of other factors at the time.
As far as 12 of the 18 children were concerned, the staff considered the reduction to be due mainly or entirely to the treatment provided. In the remaining six children, staff felt that a significant contribution came from other beneficial influences in the child’s life at the time of treatment. No staff member considered that the treatment was ever merely coincidental or secondary to other influences, and more than half the respondents thought the improvement to be due entirely to the “bell and pad” treatment.
General behauiour change
The staff interviewed considered that out of the 18 children, there were six who showed very substantial improvements in their general behaviour which were associated with treatment, while only slighter improvements were reported in another seven children.
These findings suggest that a significant number of the children showed substantial or partial improvements in other behaviour, indicating increased well-being and greater confidence in social relationships. Other children were less changed, and it is not clear whether this was related to less motivation toward success in the treatment or reflected less successful results or frequency of relapses in enuresis. There appears to be no evi- dence of symptom substitution as indicated by any deterioration in other behaviour.
Disruption in Homes
Although a form of treatment may be successful in the results it achieves for the person for whom it is provided, these may be outweighed by its adverse consequences for others. A significant feature of the “bell and pad” treatment is that the buzzer emits a loud, continuous buzzing noise at the moment the pad becomes moist, perhaps more often then once a night. particularly at the beginning stage of treatment. Not only may staff be woken, and indeed this may be necessary if the child needs help in getting up at night, but many children in Children’s Homes share bedrooms with other children. who may also be woken and disturbed by the noise. For these reasons the treatment could have an adverse influence on the life of the Home. The staff members interviewed were asked to recall the period when treatment was in progress and to describe the extent of any disruption.

12 D. JEHL. R. T. T. MORGAN, R. K. TURNER and A. JONES
It is clear that every Home suffered some disruption through introducing the treat- ment, but this was considered to be either hardly discernible or only occasional in 15 of the 18 cases, and as significant in the three remaining cases. In almost all the Homes, only the staff on duty and the child being treated were affected at all.
Thus, in the great majority of cases there was no significant disruption to the life of the Home, beyond some broken nights for the care staff who, without exception, considered this to be a worthwhile sacrifice. Children sharing bedrooms with those being treated quite quickly adjusted, literally ‘turning over’ once the initial impact of the noise was adjusted to. Many of the older children conducted their own treatment, and some younger ones were ‘taken over’ by older, helpful children.
Attitudes of staf to treatment
Many staff had been open minded towards “bell and pad” treatment often because they had no prior knowledge of it, and their attitudes could be said not to have changed. Some had been sceptical at first, but changed their attitude to one of respect for its effectiveness in helping the child. A few retained reservations, some because they felt that enuresis should be cured by a climate of care in its own time, rather than through the introduction of a specific technique: others because they were not convinced that cure was entirely due to the treatment or that it would work with a large range of age groups, or would be inappropriate for a sensitive child who might be upset at attention being drawn to an embarrassing difficulty. At least 13 of the 18 staff interviewed were sufficiently impressed by the value of treatment to consider using it in similar cases in future.
Attitudes of children to treatment
Only eleven children could be interviewed personally, and five of these were either pleased or very happy to use the alarm, while two had no particular feelings and were embarrassed or unhappy about doing so.
The responses suggest that for the large majority of the children there were no particu- larly negative reactions experienced as a result of the introduction of the treatment. For some there was a gain, however transient, in kudos, either from the “bell and pad” apparatus itself, or from association with the therapist. There are, however, strong indications of unhappy feelings about the bedwetting itself, however much the staff accepted it. More than half the children interviewed personally felt able to declare that for them the treatment had been “worthwhile” and they felt able to recommend it to others.
General comments
Enuresis is identified as a problem when a child is unable to control his urine at night beyond the age when most children can do so. There seem to be various reasons for concern. Adults feel that bedwetting may reflect a physical disability or indicate that the child is emotionally upset. Less rationally, perhaps, they fear that if control is not achieved at the usual age it may never be achieved, and many will have vague knowledge of people being enuretic until adulthood. Moreover, bladder control is a function that natural parents are expected to help their children to achieve by a norma- tive age. If they fail, it may well be felt to reflect adversely on their capacity as parents.
The attitudes among residential care staff seem somewhat different. Not being the natural parents they are not assumed by others to be in any way responsible for the child’s failure to achieve bladder control, nor, from the evidence gained during the evaluation, did they appear to assume this responsibility themselves. It was accepted that some children ‘bed wet’ and that it is due to insecurity from the disruption in their lives and was not likely to disappear until the child settled and became more secure. All the staff interviewed expressed an ideological belief that the enuresis had to be ‘accepted’, this being closely associated with acceptance of the child. In contrast, other forms of behaviour of an unpleasant nature, were not necessarily accepted in

The treatment of nocturnal enuresis 13
this way, perhaps because they were perceived as being something over which the child had voluntary control. On the other hand, acceptance is not as easy in practice as it appears to be from a more abstract vantage point. Almost without exception the interviewer sensed ambivalence from staff towards enuresis, and some were more open in their negative feelings than others. There is nothing pleasant about urine soaked sheets and pyjamas, even if there are readily available replacements and washing machines. In addition, bedwetting is behaviour associated with very young children. and it becomes more incongruous the older the child becomes. Children who are capable in other ways surely ought to be capable of controlling their bladder at night. despite evidence to the contrary. Staff acceptance seemed most stretched in relation to children who appeared indifferent to their bedwetting, and its consequence or efforts to reduce it. Some children were described as ‘lazy’ or ‘unconcerned and uncaring’, and even the most accepting staff clearly found enuresis a nuisance which they hoped would clear up. Only the very young and the most self-conscious, sensitive and upset children gained undiluted sympathy from staff.
The children themselves demonstrated mixed reactions to their enuresis. Some seemed indi~erent in their own feelings towards it, and also indi~erent to the attitudes of the care staff. Initially it seemed possible that this was a response to the acceptance overtly expressed in the staff culture, but it seems clear that staff did convey that bedwetting was a nuisance, and urine control a desirable state to achieve, even if they made efforts not to transfer their ambivalent feelings to the child as a person.
DISCUSSION
Eficacy of treatment
One way of evaluating the treatment provided is to examine the final outcome among those children who received it. All but two of these 19 children are known to be dry at the present time, although there is occasional wetting by two of the otherwise dry children. This high success rate is indicative of the very considerable effectiveness of this approach to the treatment of nocturnal enuresis.
Another way to assess the results is to compare the outcome at the conclusion of treatment in the treated children, whith their pre-treatment baseline, and with the out- come among the control children. There was no significant change in frequency of wetting in the control group over a 3- to 4-month period. In contrast, the treated group showed a significant reduction both in relation to their own baseline and when compared to the control children. This suggests that the beneficial results of therapy are not entirely explicable in terms of non-specific factors such as the enhanced attention given to the treated children, for the controls received this as well. In making this point we are not denying the importance of such factors, only suggesting that they cannot entirely account for the therapeutic results.
The “bell and pad” method of treatment is probably the single most effective form of treatment for this particular problem, and the results in the present study are as good as those obtained when it has been used with children in their own homes (Morgan and Young, 1972). There is, therefore, no evidence to support the widespread belief that it cannot be applied in residential Children’s Homes, or indeed in other institutional settings.
It is also important to assess outcome by taking into account the opinions of residen- tial staff who, after all, have to carry the main burden of therapy. On the basis of the evaluation by the independent assessor, these staff members considered the outcome to have been successful in the majority of cases, and two-thirds of the staff regarded the improvement as due mainly or entirely to the treatment provided.
It must be emphasised. however, that the treatment of any particular behaviour prob- lem is not an alternative to a more comprehensive programme of social work help for a child and his family. Most of the children achieved continence after “bell and

14 D. JEHL. R. 7. T. MORGAN, R. K. TURNER and A. Jams
pad” treatment, but it is not surprising that some continued to show many of the psychological and social problems which have been so well documented in studies of deprived children in care. The independent assessor explored the opinion of staff con- cerning any wider changes in the children’s behaviour. There seemed to be some diversity of opinion: certainly there was no evidence of any deterioration; and in one-third of the cases, the staff said that there had been striking improvements in behaviour, as well as apparent improvement in the self esteem of the child. In another third, the staff were of the opinion that no significant changes had occurred. and the children seemed to be substantially the same. As the independent assessor observed, control of the enuresis was felt to be a desirable social achievement, but it did not seem to have any more generalised implications for the child’s functioning. This conclusion accords with the general absence of change along dimensions other than enuresis as measured on a variety of psychometric instruments in the study.
Feusihilif~ of treatn?mt in Chikfren’s Homes
In contrast to research findings indicating a high rate of dropout with children in their own homes (Young and Morgan, 1972a), there was only one instance in this study where treatment had to be discontinued once it had begun, even though most children shared their bedrooms. Furthermore, the results of the independent assessment suggest very strongly that therapy did not present major difficulties; every Home suffered some disruption to residential staff whose nights were disturbed, but they all considered that the treatment had been worthwhile for the sake of the child. Certainly, the treatment seemed to have been acceptable to the children; perhaps, it offered them a chance to alleviate a problem which sometimes led to teasing. The question of the practicality of treatment can also be answered by considering whether staff would wish to apply this method of treatment for other children. Again, the results of the independent enquiry suggest that more than two-thirds of the staff were impressed sufficiently to consider using it in other cases. In summary, the treatment was practical and seemed to be acceptable to residential staff.
Viability of treut~ent in Social Sercices
There is ample evidence that enuresis is a very common problem amongst children in residential institutions. and in many cases it may continue into late adolescence or even into adulthood in some 3”, of the general population (Turner and Taylor. 1974). There is, therefore, a strong case for doing something about the problem. The present research has shown that an effective remedy is readily available and that it can be applied by residential staff without undue disruption of the life of the Home. It remains to consider how therapy should be offered within the setting of a social services department.
Clearly, any such treatment facility should be only one aspect of a behaviourally oriented support service to help residential staff in the management of children with difficult behaviour problems. As far as enuresis specifically is concerned, it is necessary for each child to be screened for possible organic pathology, and our experience in the present study indicated that this can be done very satisfactorily by the child’s general practitioner. It would, however, be necessary to ensure adequate screening for possible urinary infection, preferably by a local pathology laboratory. The psychological assess- ment of the child and the supervision of his behavioural treatment by the resident staff would need to be undertaken by a therapist who is trained in these procedures.
It must be emphasised again that the specific treatment of a particular problem is not an alternative to a more comprehensive programme of social work help for a child and his family. Without this, he may become dry but still retain many of the other psychological and social problems that are common among children in care. Conversely, a very satisfactory general programme of help may well not resolve particular difficulties such as bedwetting, which requires the inclusion of specific treatment procedures within the overall intervention.

The treatment of nocturnal enuresis 15
Implications of the research for behauiour therapy
This research trial has shown that a widely used form of behavioural treatment can be applied in a setting where it has not previously been evaluated. It is also appropriate to observe that although there is a huge literature concerning behaviour therapy for childhood disorders, there are still few studies where outcome has been assessed in properly controlled trials. The present paper confirms three earlier studies which have demonstrated a definite treatment effect (Werry and Cohrssen, 196.5; De Leon and Man- dell, 1966; Baker, 1969) and it contradicts one study (Turner et al., 1970) which failed to show any significant difference between treatment and control groups over the rela- tively brief period of one month.
The results also confirm earlier research findings that the relapse rate can be lowered significantly by modifying treatment to include an overlearning period of extra fluid intake (Young and Morgan, 1972b; Young and Morgan, 1972~; Taylor and Turner, 1975). The possible relationship between relapse and apparent stress raises several issues of considerable interest. Traditionally, behaviourists have argued that enuresis, like other behaviour disorders, is not necessarily indicative of any generalised emotional distur- bance. Certainly, the results of careful epidemiological surveys of children in the general population suggest strongly that it would be wrong to assume that all enuretics necess- arily have other behaviour problems (Rutter et al., 1970). However, it is equally plain that in about one-fifth of cases enuretic children do have other behaviour problems and that the existence of enuresis and other problems is most marked in girls (Rutter et al., 1973). Also, there is evidence to suggest that as a group, enuretic children are more likely to have experienced some environmental stress during the period when children are normally acquiring continence (Douglas, 1973). It is of interest, therefore, that in the present case series the recurrence of enuresis often coincided with potentially stressful events and that, at least in this very small sample, girls predominated amongst the children who relapsed. One possible explanation of this observation is that enuresis might arise in two ways; it might be a developmental disorder, in which there is a learning deficiency so that the child has not acquired bladder control. In these cases, like other developmental disorders, there is no greater chance of other behaviour prob- lems occurring. Other cases of enuresis might arise from stressful experiences that disrupt the learning of continence, and also cause additional behaviour problems. In yet other cases there might be some combination of deficient and disrupted learning. At this stage, a possible explanation along these lines is almost entirely speculative.
Acknowledgenlents-The Child Treatment Research Unit is financed by the Department of Health and Social Security, and by the City of Birmingham Social Services Committee who also provided facilities for this study. The investigators gratefully acknowledge their support while accepting entire responsibility for the contents of this report which do not necessarily represent the views of the sponsoring bodies. We also wish to acknowledge the secretarial and organisationa! help of June Carroll in preparing this research report.
REFERENCES
BAKER B. L. (1969) Symptom treatment and symptom substitution in enuresis. J. abnorm. Psychol. 74, 42-49. BECKER W. C. (1960) The relationship of factors in parental ratings of self and each other to the behaviour
of kindergarten children as rated by mothers, fathers and teachers. J. consulr. Psychol. 24, 507-527. BRIMER M. A. and DUNN L. M. (19621 Mtrtwd,fhr the Em&h Picture Vkubulary Test. Educational Evaluation
Enterprises. Bristol. COLLINS R. W. (1973) importance of bladder-cue buzzer contingency in the conditioning treatment for enuresis.
J. ahnornr. Psychol. 82. 299-308. COPPERSMITH S. (1967) The Anteccder~ts of’ S~~f~Esrwm Freeman. San Francisco. DAVIDKIN J. R. and DOUGLASS E. (1950) Nocturnal enuresis: a special approach to treatment. Er. med. J.
1. 13451347. DE LEON G. and MANDELL W. (1966) A comparison of conditioning and psychotherapy in the treatment
of functional enuresis. J. c/in. Pswhol. 12. 326-330. DOUGLAS J. W. B. (1970) Broken familes and child behaviour. J. R. Cd. Phncians. Lntrd. 4, 203-206. D~IAXAS J. W. B. (1973) Early dtsturbing events and later enuresis. In 1. KOLVIN. R. C. MACKEITH and
S. R. MEADOW (Eds.) BIaddrr Cortrrof anti Enuresis. Heinemann, London. FINLAY W. W., BESSERMANN R. L.. BENNETT L. F.. CLAPP R. K. and FINLAY P. M. (1973) The effect of
continuous, intermittent and “placebo” reinforcement on the effectiveness of the conditioning treatment for enuresis noctuma. B&r. Res. and Thrrap!* 11. 289-297.

16 D. JEHU. R. T. T. MORGAN. R. K. TURNER and A. JONES
KEMPE C. H. and HELFER R. E. (1972) Helping the Bnrrered Child and His Family. Lippincott. Oxford. MANN RUTH W., TAYLOR P. D. and TURNER R. K. (1975) Treatment of nocturnal enuresis by bell and
pad in general practice. reverb Visiror 48, 4O+i. MCCONAGHY N. (1969) A controlled trial of imipramine. amphetamine, bell and pad conditioninp and random
awakening in the treatment of nocturnal enuresis. iMed. J. Austr. 2, 237-239. Ministry of Health (1968) Enuresis alarms--a performance specification. MoH, London. Reprinted in Bladder
Control and Enurrsis. (Eds I. KOLVIN, R. C. MACKEITH.~~~ S. R. MEADOW). Heinemann. London. MORGAN R. T. T. (1973) Success and failure in the condirionina rrearment of childhood enuresis. PhD Thesis.
University of Leicester. MORGAN R. T. T. (1975) Enuresis and the enuresis alarm: u cfiniral manual j&r rhe rrearmenr q’ nocflirnal
enuresis. Child Treatment Research Unit. School of Social Work. Universitv of Leicester. MORGAN R. T. T. and YOL’NG G. C. (1972) The conditioning treatment of childhood enuresis. Br. J. XX.
Wk 2. 503-509. MOWRER 0. H. and MOWRER W. M. (1938) Enuresis-A method for its study and treatment. .4m. J. Orrho-
psychiarry 8. 436459.
NEALE M. (1966) Neule Analysis of Reading Ability: manual of directions and norms (2nd edn). Macmillan, London.
OSGOOD C. E.. Suer G. J. and TA~~~~BAU~~ P. H. (1957) The ~~easurenze~f qf .~eu~z~ng. Illinois University Press, Urbana.
PATTERWN G. R. and FAGOT B. I. (1967) Selective responsiveness to social reinforcers and deviant behaviour in children. Ps,rcliol. Rec. 17, 2699278.
RUTTER M. (1973) Indications for research: III. In Bladder Conrrol and Enuresis. (Eds I. KOLVIX. R. C. MAC- KEITH and S. R. MEADOW). Heinemann, London.
RUTTER M.. TIZARD J. and WHITMORE K. (1970) Educarion, Health and Behatliour. Longmans, London. RC’T~ER M., YULE W. and GRAHAM P. (1973) Enuresis and behavioural deviance. In Bladder ConrroI and
Enuresis. (Eds 1. KOLVIN, R. C. MA~KEITH and S. R. MEADOW). Heinemann. London. SACKS S., DE LEON G. and BLACKMAN S. (1974) Psychoiopical changes associated with conditioning functional
enuresis. J. clin. Psychoi. 3, 271-277. STEIN Z. A. and SUSSER M. (1967). The social dimensions of a symptom: a socio-medical study of enuresis.
Socia/ Sci. Med. 1, 183-201. TAYLOR P. D. and TURNER R. K. (1975) A clinical trial of continuous. intermittent and overlearning ‘bell
and pad’ treatment for nocturnal enuresis. Behac. Res. and Therapy 13, 281-293. TURNER R. K. (1973) Conditioning treatment of nocturnal enuresis: present status. In Bladder fonrrol and
Enuresis. (Eds I. KOLVIN. R. C. MACKEITH and S. R. MEA~MW). Heinemann, London. TURNER R. K. and TAYLOR f. D. (1974) Conditioning treatment of nocturnal enuresis: preliminary findinps.
Behar. Res. and Therapy 12. 41-52. TURNER R. K.. YOUNG G. C. and RA~HMAN S. (1970) Treatment of nocturnal enuresis by conditioning tech-
niques. Be/tar. Rrs. a7d Therapy 8. 367-381.
WERRY J. S. and COHRSSEN J. (1965) Enuresis: an etiological and therapeutic study. J. Pediar. 67, 423431. WINER B. (1962) Sratistical Methods in Experimenral Design. McGraw-Hill, New York. YOUNG G. C. and MORGAP~ R. T. T. (1972a) Childhood enuresis: termination of treatment by patients. Coni-
munirx Med. 129, 247-250.
YOUNG G. C. and MORGAN R. T. T. (1972b) Overlearnme in the conditioning treatment of enuresis. Behat-. Res. and Therapy 10, 147-151.
YOUNG G. C. and MORGAN R. T. T. (1972~) Overlearning in the conditioning treatment of enuresis-a long term follow up study. Behar. Rex and Therapy 10, 419-420.
YOUNG G. C. and MORGAN R. T. T. (1972d) Reasons for appointment failure among enuretic patients. Conr- munit.r Med. 129, 23-25.
YULE W. and RAYNES N. V. (1977). Behavioural characteristics of children in residential care in relation to indices of separation. f. c/i&i Ps~cliof. Ps~ciiiat. 13. 249-258.