Embed Size (px)
Citation preview
This article was downloaded by: [University of Limerick]On: 28 April 2013, At: 14:01Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Child Neuropsychology: A Journal onNormal and Abnormal Development inChildhood and AdolescencePublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/ncny20
A comparison of working memoryprofiles in children with ADHD and DCDTracy Packiam Alloway aa Department of Psychology, University of Stirling, Stirling, UKVersion of record first published: 21 Mar 2011.
To cite this article: Tracy Packiam Alloway (2011): A comparison of working memory profilesin children with ADHD and DCD, Child Neuropsychology: A Journal on Normal and AbnormalDevelopment in Childhood and Adolescence, 17:5, 483-494
To link to this article: http://dx.doi.org/10.1080/09297049.2011.553590
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representationthat the contents will be complete or accurate or up to date. The accuracy of anyinstructions, formulae, and drug doses should be independently verified with primarysources. The publisher shall not be liable for any loss, actions, claims, proceedings,demand, or costs or damages whatsoever or howsoever caused arising directly orindirectly in connection with or arising out of the use of this material.
Child Neuropsychology, 2011, 17 (5), 483–494http://www.psypress.com/childneuropsychISSN: 0929-7049 print / 1744-4136 onlineDOI: 10.1080/09297049.2011.553590
A comparison of working memory profiles in children
with ADHD and DCD
Tracy Packiam Alloway
Department of Psychology, University of Stirling, Stirling, UK
The main objective of present study was to investigate whether the patterns of working memory per-formance differ as a function of attention and motor difficulties, and whether children with ADHDand DCD could be reliably discriminated on the basis of their memory deficits. A related aim was toinvestigate the link between their working memory profiles and academic attainment. Fifty childrenwith ADHD-Combined, 55 children with DCD, and an age-matched group of 50 typically developingchildren with average working memory were assessed on standardized measures of working mem-ory, IQ, and academic attainment (reading, spelling, comprehension, and math). The normal controlsperformed significantly better than both clinical groups on all working memory tests. Specific pat-terns emerged in the memory profile of the clinical groups: The children with DCD had a depressedperformance in all working memory tests, with particularly low scores in visuospatial memory tasks;children with ADHD performed within age-expected levels in short-term memory but had a pervasiveworking memory deficit that impacted both verbal and visuospatial domains. The clinical groups couldreliably be discriminated on the basis of their short-term memory scores. Their learning profiles weresimilar. It is possible that the working memory profiles of the children with ADHD and DCD are influ-enced by distinct underlying cognitive mechanisms, rather than a general neurodevelopmental delay.Despite these distinctive patterns of memory performance, both clinical groups performed similarlyon academic attainments, suggesting that memory may underlie learning difficulties, independent ofrelated clinical disorders.
Keywords: Working memory; Academic attainment; IQ; Developmental Coordination Disorder;Attention deficit-hyperactivity disorder.
Attention deficit/hyperactivity disorder (ADHD) and Developmental CoordinationDisorder (DCD) are common overlapping disorders. ADHD is characterized by difficul-ties with inhibiting behavior (Barkley, 1997) and delaying gratification (Sonuga-Barke,1994). While there are varying theories to explain underlying causes for the problems
This research was supported by a research grant awarded by the Economic and Social Research Councilof Great Britain. The author wishes to thank Kathryn Temple, Joni Holmes, and Kerry Hilton for assistance indata collection.
Address correspondence to Dr. Tracy Packiam Alloway, Department of Psychology, University of Stirling,Stirling, FK9 4LA, UK. E-mail: [email protected]
© 2011 Psychology Press, an imprint of the Taylor & Francis Group, an Informa business
Dow
nloa
ded
by [
Uni
vers
ity o
f L
imer
ick]
at 1
4:01
28
Apr
il 20
13
484 T. PACKIAM ALLOWAY
ADHD children demonstrate in various executive function tasks, there is a general con-sensus that they exhibit difficulty in controlling and inhibiting their behavior in a rangeof activities. DCD is a generalized problem that affects movement as well as perception(Visser, 2003). Observable behaviors in children with DCD include clumsiness, poor pos-ture, confusion about which hand to use, difficulties throwing or catching a ball, readingand writing difficulties, and an inability to hold a pen or pencil properly. The estimatedoverlap between ADHD and DCD is about 50% (Kaplan, Wilson, Dewey, & Crawford,1998; Pitcher, Piek, & Hay, 2003).
Studies that have examined comorbidity in individuals with ADHD and DCD havefocused on visual skills (Crawford & Dewey, 2008; Lewis, Vance, Maruff, Wilson, &Cairney, 2008) and executive function (Piek et al., 2004). In the present study, we extendedprevious research to focus on working memory performance. Working memory refers toour ability to mentally store and to manipulate information for a brief period. Accordingto one widely used model, working memory is a domain-general component responsiblefor the control of attention and processing that is involved in a range of regulatory func-tions, including the retrieval of information from long-term memory (Baddeley, 2000). Thismodel also includes two domain-specific stores responsible for the temporary storage ofverbal and visuospatial information and has been supported in studies of children (Alloway,Gathercole, & Pickering, 2006; Bayliss, Jarrold, Gunn, & Baddeley, 2003), adults (Kaneet al., 2004), and neuroimaging research (Jonides, Lacey, & Nee, 2005). In order to mea-sure short-term memory, the participant is required to recall sequences of material such asdigits or dot locations. Working memory tests require the individual to both process andstore increasing amounts of information.
While working memory can be reliably tested from as young as four years ofage (Alloway, Gathercole, Willis, & Adams, 2004), performance on working memorytasks is subject to large degrees of individual variation (Alloway & Gathercole, 2006).Individual differences in working memory capacity have important consequences forchildren’s ability to acquire knowledge and new skills (see Cowan & Alloway, 2008,for a review). In typically developing children, scores on working memory tasks pre-dict reading achievement independently of measures of phonological skills (Swanson &Beebe-Frankenberger, 2004). Working memory is also linked to math outcomes: Lowworking memory scores are closely related to poor performance on arithmetic word prob-lems (Swanson & Sachse-Lee, 2001) and poor computational skills (Bull & Scerif, 2001;Geary, Hoard, & Hamson, 1999). A recent large-scale screening of students with work-ing memory deficits identified that the majority of them also performed poorly in readingand math assessments, independent of their IQ (Alloway, Gathercole, Kirkwood, & Elliott,2009).
The aim of the present study was to investigate whether children with ADHD andthose with DCD differ in the severity and nature of their working memory deficits bycomparing them with each other. Working memory impairments have been implicated inboth groups. For example, there is a pattern of deficits in individuals with ADHD thatindicates an impairment in working memory (van Mourik, Oosterlaan, & Sergeant, 2005;Willcutt, Pennington, Olson, Chhabildas, & Hulslander, 2005), particularly in visuospa-tial tasks (Martinussen, Hayden, Hogg-Johnson, & Tannock, 2005). Children with DCDalso appear to have a specific deficit in visuospatial memory not found in children withgeneral learning difficulties (Alloway & Temple, 2007) or specific language impairments(Alloway & Archibald, 2008). But are their working memory deficits more striking thanthose with ADHD?
Dow
nloa
ded
by [
Uni
vers
ity o
f L
imer
ick]
at 1
4:01
28
Apr
il 20
13

WORKING MEMORY IN ADHD AND DCD 485
One possibility is that some individuals have a generalized heterogeneous neurode-velopmental condition when the early development of the brain is disrupted (Kaplan et al.,1998). This condition, known as Atypical Brain Development (ABD), is likely to resultin an overlap of working memory profiles between students with ADHD and those withDCD. However, common behavioral features such as motor impairments may not be drivenby a common neurological etiology (Cruddance & Riddell, 2006; Lewis et al., 2008). Forexample, although disruption to the neurocognitive networks that drive motor planningand coordination might explain deficits in those with DCD, impairments in attention andexecutive function might underlie motor problems in those with ADHD (see Piek, Dyck,Francis, & Conwell, 2007). This differentiation in neurobiological mechanisms may alsoresult in different patterns of memory skills and academic attainments. The present studycompared children with either attentional or movement difficulties only to address thisissue (though see the “Discussion” for future research).
METHOD
Participants
The participating schools represent a range of demographic backgrounds, indexed bythe national average of eligibility for free school meals, a poverty (income) index used inthe United Kingdom. Three groups of children participated in the study (N = 155) and wereall attending mainstream schools. All were native English speakers, and none had hearingimpairments. Parental consent was obtained for each child participating in the study.
The ADHD group comprised 50 children (43 boys; mean age = 9.75 years, SD = 12months) with a combination of hyperactive-impulsive and inattentive behavior (ADHD-Combined). Diagnosis of ADHD subtype was confirmed by a comprehensive clinicaldiagnostic assessment by pediatric psychiatrists and community pediatricians. The assess-ments were based on clinical assessments during interview sessions using the Diagnosticand Statistical Manual of Mental Disorders, fourth edition (DSM-IV) criteria (AmericanPsychiatric Association [APA], 1994), scores in the deficit range on the ContinuousPerformance Test (Conners, 2004). The study only included children who score in thenormal range on the Developmental, Diagnostic and Dimensional Interview (3di), a com-puterized assessment for Autistic Spectrum Disorders (Skuse et al., 2004). No participantshad received a clinical diagnosis of comorbid motor difficulties. All children were receivingstimulants for ADHD (e.g., methylphenidate). To ensure assessments were uninfluenced bymedication (Mehta, Goodyear, & Sahakian, 2004), participants ceased taking their medi-cation 24 hours prior to testing. The greater number of boys than girls in the ADHD groupreflects the higher rate of clinical diagnosis among boys (Gershon, 2002).
The DCD group consisted of 55 children (44 boys, mean age = 8.8 years, SD = 19months) attending mainstream schools. They were referred by either a pediatrician or anoccupational therapist who had identified them as experiencing motor difficulties usingthe Diagnostic and Statistical Manual for Mental Disorders, text revision (DSM-IV-TR,American Psychiatric Association, 2000) criteria and standardized motor assessments suchas the Movement Assessment Battery for Children (M-ABC; Henderson & Sugden, 1992).None of these children had received a clinical diagnosis of behavioral or attentional prob-lems. The gender distribution corresponds with reports of more males than females beingaffected (Mandich & Polatajko, 2003).
Dow
nloa
ded
by [
Uni
vers
ity o
f L
imer
ick]
at 1
4:01
28
Apr
il 20
13

486 T. PACKIAM ALLOWAY
As the main aim of the present study was to compare working memory profiles ofstudents with ADHD and those with DCD, a typically developing comparison group com-prised of students with working memory scores in the average range. They were selectedfrom a sample of approximately 1000 children, aged 8–11 years, who were screened ontwo tests of verbal working memory (listening recall and backwards digit recall subtestsof the Automated Working Memory Assessment [AWMA]; Alloway, 2007a). The nor-mal controls (NC) consisted of 50 children (30 boys, mean age = 9. 91 years, SD = 12months), with standard scores in the normal range (> 90 on both tests). The comparisongroup was also administered with the Conners’ Teacher Rating Scale– Revised (CTRS),which is designed to identify attentional failures and ADHD on the basis of classroombehaviors. T-scores (with a population mean of 50 and SD of 10) were within the averagerange for the ADHD Index (AWMA = 48). The comparison group was recruited from thesame schools as those children with ADHD and DCD.
Tasks and Procedure
Each child was tested individually in a quiet area of the school for two sessionslasting up to 40 minutes. Measures of memory and learning were administered in a fixedsequence designed to vary task demands across successive tests.
Working Memory. All 12 tests from the Automated Working MemoryAssessment (AWMA; Alloway, 2007a), a computer-based standardized battery that pro-vides multiple assessments of verbal and visuospatial short-term memory and of verbaland visuospatial working memory. Test reliability is reported in Alloway et al. (2006)and test validity is reported in Alloway, Gathercole, Kirkwood, and Elliott (2008). Therewere three measures of verbal short-term memory where the individual had to immedi-ately recall a sequence of information: digit recall, word recall, and nonword recall. Therewere three verbal working memory measures: listening recall, backward digit recall, andcounting recall. In the listening recall task, the child is presented with a series of spokensentences, has to verify the sentence by stating “true” or “false” and has to recall the finalword for each sentence in sequence. In the backwards digit recall task, the child is requiredto recall a sequence of spoken digits in the reverse order. In the counting recall task, thechild had to count the number of circles in an array and then recall the tallies of circles.For digit recall, word recall, nonword recall, listening recall, counting recall, and backwarddigit recall, test-retest reliabilities are .89, .88, .69, .88, .83, and .86, respectively.
Three measures of visuospatial short-term memory were administered. In the dotmatrix task, the child is shown the position of a red dot in a series of four by four matricesand has to recall this position by tapping the squares on the computer screen. In the mazesmemory task, the child is shown a maze with a red path drawn through it for three seconds.The child then has to trace in the same path on a blank maze presented on the computerscreen. In the block recall task, the child views a video of a series of blocks being tappedand reproduces the sequence in the correct order by tapping on a picture of the blocks.Three measures of visuospatial working memory were administered. In the odd-one-outtask, the child views three shapes, each in a box presented in a row, and identifies the odd-one-out shape. At the end of each trial, the child recalls the location of each odd-one-outshape, in the correct order, by tapping the correct box on the screen. In the Mr. X task,the child is presented with a picture of two Mr. X figures. The child identifies whether the
Dow
nloa
ded
by [
Uni
vers
ity o
f L
imer
ick]
at 1
4:01
28
Apr
il 20
13

WORKING MEMORY IN ADHD AND DCD 487
Mr. X with the blue hat is holding the ball in the same hand as the Mr. X with the yellowhat. The Mr. X with the blue hat may also be rotated. At the end of each trial, the child hasto recall the location of each ball in the blue Mr. X’s hand in sequence, by pointing to apicture with six compass points. In the spatial recall task, the child views a picture of twoarbitrary shapes where the shape on the right has a red dot on it and identifies whether theshape on the right is the same or opposite of the shape on the left. The shape with the red dotmay also be rotated. At the end of each trial, the child has to recall the location of each reddot on the shape in sequence, by pointing to a picture with three compass points. Test-retestreliabilities are .85, .86, .90, 88, .84, and .79 for dot matrix, mazes memory, block recall,odd-one-out, Mr. X, and spatial recall, respectively. Standard scores (M = 100; SD = 15)for individual tests and composite scores for each memory component were generatedautomatically by the AWMA for each child on the basis of their age. Composite short-termmemory and working memory scores were also calculated from the respective verbal andvisuospatial composite standard scores.
Learning. Two measures of academic attainment were administered. The WechslerObjective Reading Dimensions (WORD; Wechsler, 1993) consists of tests of basic read-ing, spelling, and reading comprehension. The Wechsler Objective Numerical Dimensions(WOND; Wechsler, 1996) assesses mathematical reasoning and number operations.
IQ. The vocabulary and block design subtests of the Wechsler Abbreviated Scalesof Intelligence (WASI; Wechsler, 1999) were used to yield verbal and performance IQscores. Raw scores were converted into standard scores, with a mean of 100 and a standarddeviation of 15.
RESULTS
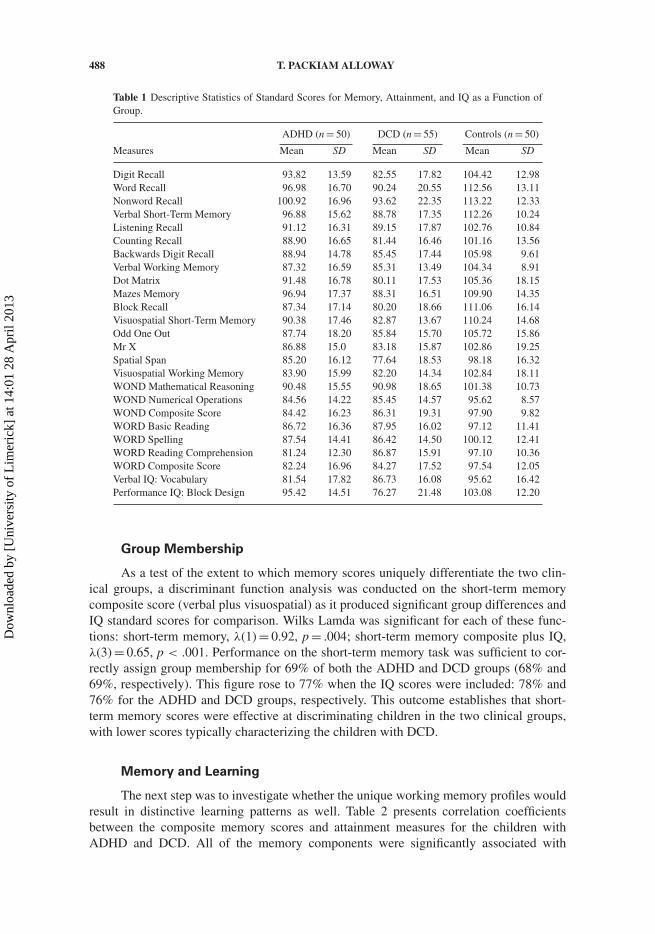
Descriptive statistics for the cognitive measures as a function of group are shownin Table 1. The following patterns emerged: Children with DCD had a depressed perfor-mance in all memory tests, with particularly low scores in the visuospatial memory tasks;children with ADHD performed within age-expected levels in short-term memory but hada pervasive working memory deficit that impacted both verbal and visuospatial domains. Inorder to compare the specificity of deficits between the groups, a series of MANOVAs wereperformed. The first MANOVA was performed on the memory composite standard scores.The overall group term was significant, (F = 15.08, p < .001, η2
p = .29). Post hoc pair-wise comparisons found significant differences between the following groups (p < .05,Bonferroni adjustment for multiple comparisons). In verbal and visuospatial short-termmemory (STM), the NC group performed better than both clinical groups and the ADHDgroup performed better than the DCD groups. In verbal and visuospatial working mem-ory (WM), the NC group performed better than both clinical groups. This pattern remainsthe same for both verbal and visuospatial STM and WM even when IQ is entered as acovariate.
The MANOVA performed on the IQ standard scores also revealed significant groupdifferences, (F = 23.17, p < .001, η2
p = .24). Post hoc pairwise comparisons found signifi-cant differences between the following groups (p < .05, Bonferroni adjustment for multiplecomparisons). In verbal IQ, the NC group performed better than both clinical groups; inperformance IQ, the NC group performed better than the DCD group only.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
imer
ick]
at 1
4:01
28
Apr
il 20
13
488 T. PACKIAM ALLOWAY
Table 1 Descriptive Statistics of Standard Scores for Memory, Attainment, and IQ as a Function ofGroup.
ADHD (n = 50) DCD (n = 55) Controls (n = 50)
Measures Mean SD Mean SD Mean SD
Digit Recall 93.82 13.59 82.55 17.82 104.42 12.98Word Recall 96.98 16.70 90.24 20.55 112.56 13.11Nonword Recall 100.92 16.96 93.62 22.35 113.22 12.33Verbal Short-Term Memory 96.88 15.62 88.78 17.35 112.26 10.24Listening Recall 91.12 16.31 89.15 17.87 102.76 10.84Counting Recall 88.90 16.65 81.44 16.46 101.16 13.56Backwards Digit Recall 88.94 14.78 85.45 17.44 105.98 9.61Verbal Working Memory 87.32 16.59 85.31 13.49 104.34 8.91Dot Matrix 91.48 16.78 80.11 17.53 105.36 18.15Mazes Memory 96.94 17.37 88.31 16.51 109.90 14.35Block Recall 87.34 17.14 80.20 18.66 111.06 16.14Visuospatial Short-Term Memory 90.38 17.46 82.87 13.67 110.24 14.68Odd One Out 87.74 18.20 85.84 15.70 105.72 15.86Mr X 86.88 15.0 83.18 15.87 102.86 19.25Spatial Span 85.20 16.12 77.64 18.53 98.18 16.32Visuospatial Working Memory 83.90 15.99 82.20 14.34 102.84 18.11WOND Mathematical Reasoning 90.48 15.55 90.98 18.65 101.38 10.73WOND Numerical Operations 84.56 14.22 85.45 14.57 95.62 8.57WOND Composite Score 84.42 16.23 86.31 19.31 97.90 9.82WORD Basic Reading 86.72 16.36 87.95 16.02 97.12 11.41WORD Spelling 87.54 14.41 86.42 14.50 100.12 12.41WORD Reading Comprehension 81.24 12.30 86.87 15.91 97.10 10.36WORD Composite Score 82.24 16.96 84.27 17.52 97.54 12.05Verbal IQ: Vocabulary 81.54 17.82 86.73 16.08 95.62 16.42Performance IQ: Block Design 95.42 14.51 76.27 21.48 103.08 12.20
Group Membership
As a test of the extent to which memory scores uniquely differentiate the two clin-ical groups, a discriminant function analysis was conducted on the short-term memorycomposite score (verbal plus visuospatial) as it produced significant group differences andIQ standard scores for comparison. Wilks Lamda was significant for each of these func-tions: short-term memory, λ(1) = 0.92, p = .004; short-term memory composite plus IQ,λ(3) = 0.65, p < .001. Performance on the short-term memory task was sufficient to cor-rectly assign group membership for 69% of both the ADHD and DCD groups (68% and69%, respectively). This figure rose to 77% when the IQ scores were included: 78% and76% for the ADHD and DCD groups, respectively. This outcome establishes that short-term memory scores were effective at discriminating children in the two clinical groups,with lower scores typically characterizing the children with DCD.
Memory and Learning
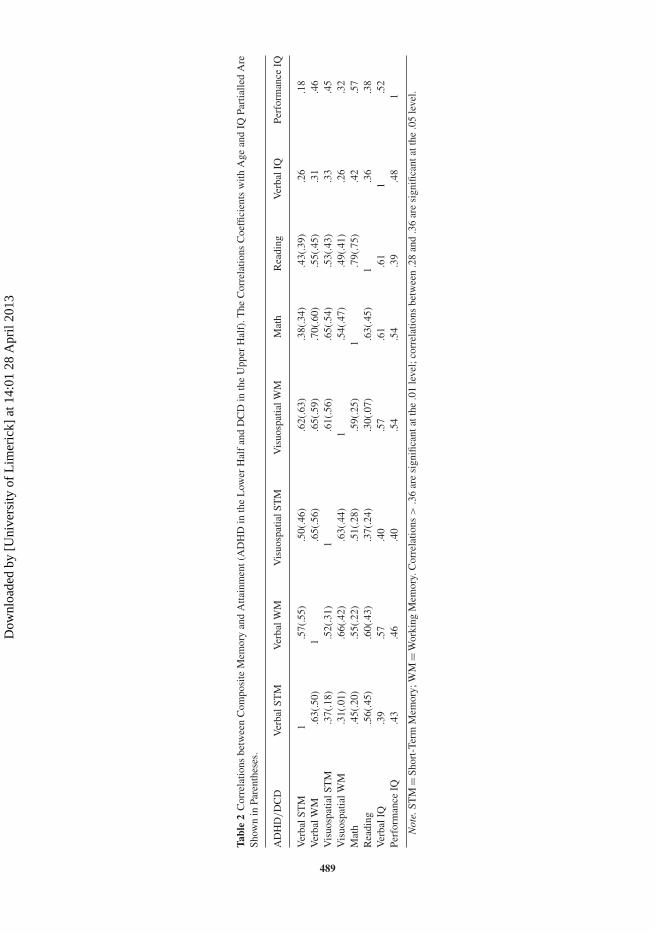
The next step was to investigate whether the unique working memory profiles wouldresult in distinctive learning patterns as well. Table 2 presents correlation coefficientsbetween the composite memory scores and attainment measures for the children withADHD and DCD. All of the memory components were significantly associated with
Dow
nloa
ded
by [
Uni
vers
ity o
f L
imer
ick]
at 1
4:01
28
Apr
il 20
13
Tabl
e2
Cor
rela
tions
betw
een
Com
posi
teM
emor
yan
dA
ttain
men
t(A
DH
Din
the
Low
erH
alf
and
DC
Din
the
Upp
erH
alf)
.The
Cor
rela
tions
Coe
ffici
ents
with
Age
and
IQPa
rtia
lled
Are
Show
nin
Pare
nthe
ses.
AD
HD
/D
CD
Ver
balS
TM
Ver
balW
MV
isuo
spat
ialS
TM
Vis
uosp
atia
lWM
Mat
hR
eadi
ngV
erba
lIQ
Perf
orm
ance
IQ
Ver
balS
TM
1.5
7(.5
5).5
0(.4
6).6
2(.6
3).3
8(.3
4).4
3(.3
9).2
6.1
8V
erba
lWM
.63(
.50)
1.6
5(.5
6).6
5(.5
9).7
0(.6
0).5
5(.4
5).3
1.4
6V
isuo
spat
ialS
TM
.37(
.18)
.52(
.31)
1.6
1(.5
6).6
5(.5
4).5
3(.4
3).3
3.4
5V
isuo
spat
ialW
M.3
1(.0
1).6
6(.4
2).6
3(.4
4)1
.54(
.47)
.49(
.41)
.26
.32
Mat
h.4
5(.2
0).5
5(.2
2).5
1(.2
8).5
9(.2
5)1
.79(
.75)
.42
.57
Rea
ding
.56(
.45)
.60(
.43)
.37(
.24)
.30(
.07)
.63(
.45)
1.3
6.3
8V
erba
lIQ
.39
.57
.40
.57
.61
.61
1.5
2Pe
rfor
man
ceIQ
.43
.46
.40
.54
.54
.39
.48
1
Not
e.ST
M=
Shor
t-Te
rmM
emor
y;W
M=
Wor
king
Mem
ory.
Cor
rela
tions
>.3
6ar
esi
gnifi
cant
atth
e.0
1le
vel;
corr
elat
ions
betw
een
.28
and
.36
are
sign
ifica
ntat
the
.05
leve
l.
489
Dow
nloa
ded
by [
Uni
vers
ity o
f L
imer
ick]
at 1
4:01
28
Apr
il 20
13

490 T. PACKIAM ALLOWAY
academic attainments in both clinical groups. For the ADHD group, rs ranged from .30to .60. For the DCD group, the magnitude of the correlations between the memory com-ponents and learning were ranged from .38 to .70. Partial correlations (with age and IQscores) partialled out are also shown in Table 2. The relationship between working mem-ory scores and attainment seems to be moderated to a greater extent in students with ADHDthan those with DCD.
DISCUSSION
The main objective of present study was to investigate whether the patterns of mem-ory performance differ as a function of attention and motor difficulties, and whetherchildren with ADHD and DCD could be reliably discriminated on the basis of theirmemory deficits. Of additional interest was the link between their memory profiles andacademic attainment. There were subtle differences in memory performance across theclinical groups. Children with ADHD exhibited deficits in both verbal and visuospatialworking memory measures whereas the DCD group had across-the-board deficits in bothverbal and visuospatial short-term and working memory. An important question is whethertheir respective core deficits contribute to their memory profile, or whether their memoryperformance represents an additional impairment.
The children with ADHD performed worse than the normal controls on all memorymeasures. There are several strands of evidence to suggest that this pattern of workingmemory impairments in children with ADHD could be the result of their core deficit,rather than represent a distinct impairment. First, according to one widely cited model toaccount for ADHD their working memory problems are a consequence of behavioral inhi-bition problems (Barkley, 1997; also Pennington & Ozonoff, 1996). Their primary deficit ininhibitory control results in secondary impairments in a range of executive function skills,including working memory. This pattern is evidenced in the present study, extending pre-vious research to a UK-based sample, and also supports this model as generalizable acrossdifferent countries. The second evidence arises from the view that information in spatialworking memory is subject to greater decay due to deficiencies in neural circuits involv-ing the frontal lobes and subcortical structures (Sergeant, 2000; Sonuga-Barke, 2003). Thepresent data indicated that the children with ADHD could not be distinguished from thosewith DCD in their working memory profile that are typically characterized by visuospatialmemory deficits (e.g., Alloway & Archibald, 2008; Alloway & Temple, 2007). The finalpiece of evidence comes from research on stimulant medication, such as methylphenidate,which suggests that when inhibitory control is improved, working memory improves aswell (e.g., Mehta et al., 2004). Taken together with the present findings, it seems likelythat working memory deficits in children with ADHD could be resultant from their coredeficit.
The children with DCD struggled in all memory tests compared to the normal con-trols, and in the short-term memory ones compared to those with ADHD. Was theirmemory profile driven by their motor impairments? A recent intervention study pro-vides some insight into this issue (Alloway & Warner, 2008). A group of children withmotor difficulties participated in an exercise-based intervention targeted to improve motorcoordination. Posttraining assessment indicated an improvement in visuospatial workingmemory tasks, but not verbal working memory ones. It is possible that the process-ing component of the task is associated with movement planning (e.g., shape rotation,
Dow
nloa
ded
by [
Uni
vers
ity o
f L
imer
ick]
at 1
4:01
28
Apr
il 20
13

WORKING MEMORY IN ADHD AND DCD 491
visual encoding) and was enhanced by movement training. It may be that children withDCD are characterized by two dimensions: one relating to movement control that affectscognitive tasks with a motor component, including working memory and IQ tasks (seeAlloway, 2007b, for further discussion); and another dimension relating to difficulties inprocessing and storing information as evidenced by deficits in both verbal and visuospatialdomains.
The comparison of two clinical groups who do not overlap in their symptoms offersa novel opportunity to understand how their respective impairments impact memory func-tioning. There are clear group differences with respect to short-term memory performance.The lack of significant difference in working memory performance between the two clini-cal groups does not necessarily mean that the etiology of the working memory deficits is thesame in the two disorders. It is possible that in those with ADHD, abnormalities in atten-tional functions that characterize the disorder may also interfere with working memoryability. In children with DCD, disruptions to neural mechanisms underlying motor planningmay also disrupt working memory performance. Thus, disruption to different underlyingcognitive mechanisms could result in a similar working memory profile as evidenced inthe present study.
It is difficult to speculate what patterns of working memory performance might beevidenced in those with comorbid disorders. There is a growing consensus that a gen-eral neurodevelopmental delay or the Atypical Brain Development account (ABD; Kaplanet al., 1998) cannot account for the fact that certain disorders have a greater tendency toco-occur with specific disorders (see Piek et al., 2004). For example, those with ADHDare more likely to also be diagnosed with Oppositional Defiant Disorder (ODD) even with-out comorbid motor problems (DCD), and those with DCD tend to also be diagnosed withAsperger’s syndrome if they also have comorbid ADHD (Kadesjö & Gillberg, 1999). Thesepatterns of specific co-occurrence provide evidence against a diffuse neurodevelopmentallag. It also seems unlikely that the ABD view could provide a satisfactory account for thedifferences in working memory profiles across various clinical groups.
A related issue is how children with ADHD and those with DCD overlapped in theirlearning outcomes in the present study. In both groups, working memory was significantlyassociated with standardized measures of reading, spelling, comprehension, and math. Oneexplanation can be drawn from a recent investigation of students identified on the basis of aworking memory deficit, rather than a learning disorder (Alloway et al., 2009). There werestrong links between working memory skills and learning outcomes, independent of IQ,suggesting that working memory may underlie learning difficulties, independent of coredeficits linked with various clinical disorders.
One limitation to the present study relates to the attention profile of students withDCD. Although none of the students in that group had received a diagnosis of ADHD, itis possible that this problem might have been undiagnosed at the time of data collection.Future research would benefit from including measures of attentional control to rule outthe possibility of behavioral problems.
In summary, children with ADHD and DCD can be characterized by unique short-term memory profiles, while their similar learning profiles are thought to reflect thecontribution of working memory to successful learning. Further research on those withcomorbid disorders, such as those with ADHD and Oppositional Defiant Disorder (ODD)or DCD, ADHD, and Asperger’s syndrome, can further clarify the impact of comorbidityin cognitive skills, such as working memory.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
imer
ick]
at 1
4:01
28
Apr
il 20
13

492 T. PACKIAM ALLOWAY
Key Points
1. The estimated overlap between ADHD and DCD is about 50%.2. An important question is whether their respective core deficits contribute to their work-
ing memory profile, or whether their working memory performance represents anadditional impairment.
3. Children with ADHD and DCD can be characterized by unique short-term memoryprofiles, with those with ADHD achieving higher scores.
4. They have similar learning profiles that are thought to reflect the contribution of workingmemory to successful learning.
5. Clinicians can provide guidance on early screening of working memory in these groups,as well as recommendations to boost working memory functioning in order to supportlearning.
Original manuscript received February 12, 2010Revised manuscript accepted December 24, 2010
First published online March 18, 2011
REFERENCES
Alloway, T. P. (2007a). Automated Working Memory Assessment. London, UK: PsychologicalCorporation.
Alloway, T. P. (2007b). Working memory, reading and mathematical skills in children withDevelopmental Coordination Disorder. Journal of Experimental Child Psychology, 96, 20–36.
Alloway, T. P., & Archibald, L. M. (2008). A comparison of working memory and learning in chil-dren with Developmental Coordination Disorder and specific language impairment. Journal ofLearning Disabilities, 41, 251–262.
Alloway, T. P., & Gathercole, S. E. (2006). How does working memory work in the classroom?Educational Research and Reviews, 1, 134–139.
Alloway, T. P., Gathercole, S. E, Kirkwood, H. J., & Elliott, J. E. (2008). Evaluating the validity ofthe Automated Working Memory Assessment. Educational Psychology, 7, 725–734.
Alloway, T. P., Gathercole, S. E, Kirkwood, H. J., & Elliott, J. E. (2009). The cognitive andbehavioural characteristics of children with low working memory. Child Development, 80,606–621.
Alloway, T. P., Gathercole, S. E., & Pickering, S. J. (2006). Verbal and visuo-spatial short-term andworking memory in children: Are they separable? Child Development, 77, 1698–1716.
Alloway, T. P., Gathercole, S. E., Willis, C., & Adams, A. M. (2004). A structural analysis of work-ing memory and related cognitive skills in early childhood. Journal of Experimental ChildPsychology, 87, 85–106.
Alloway, T. P., & Temple, K. J. (2007). A comparison of working memory profiles and learning inchildren with Developmental Coordination Disorder and moderate learning difficulties. AppliedCognitive Psychology, 21, 473–487.
Alloway, T. P., & Warner, C. (2008).The effect of task-specific training on learning and memoryin children with Developmental Coordination Disorder. Perceptual and Motor Skills, 107,273–280.
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders(4th ed.). Washington, DC: Author.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders(Revised 4th ed.). Washington, DC: Author.
Baddeley, A. D. (2000). The episodic buffer: A new component of working memory? Trends inCognitive Sciences, 4, 417–423.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
imer
ick]
at 1
4:01
28
Apr
il 20
13

WORKING MEMORY IN ADHD AND DCD 493
Barkley, R. A. (1997). Behavioural inhibition, sustained attention and executive functions:Constructing a unifying theory of ADHD. Psychological Bulletin, 121, 65–94.
Bayliss, D. M., Jarrold, C., Gunn, D. M., & Baddeley, A. D. (2003). The complexities of complexspan: Explaining individual differences in working memory in children and adults. Journal ofExperimental Psychology: General, 132, 71–92.
Bull, R., & Scerif, G. (2001). Executive functioning as a predictor of children’s mathematics ability:Shifting, inhibition and working memory. Developmental Neuropsychology, 19, 273–293.
Conners, K. (2004). Continuous Performance Test. Multi-Health Systems. Toronto, Canada.Cowan, N., & Alloway, T. P. (2008). The development of working memory. In N. Cowan (Ed.),
Development of Memory in Childhood (2nd ed., pp. 303–342). Hove, England: PsychologyPress.
Crawford, S., & Dewey, D. (2008). Co-occurring disorders: A possible key to visual perceptualdeficits in children with developmental coordination disorder? Human Movement Science, 27,154–169.
Cruddance, S. A., & Riddell, P. M. (2006). Attention processes in children with movementdifficulties, reading difficulties and both. Journal of Abnormal Child Psychology, 34, 672–680.
Geary, D. C., Hoard, M. K., & Hamson, C. O. (1999). Numerical and arithmetical cognition: Patternsof functions and deficits in children at risk for a mathematical disability. Journal of ExperimentalChild Psychology, 74, 213–239.
Gershon, J. (2002). A meta-analytic review of gender differences in ADHD. Journal of AttentionalDisorders, 5, 143–154.
Henderson, S. E., & Sugden, D. A. (1992). Movement Assessment Battery for Children. London, UK:Pearson Assessment.
Jonides, J., Lacey, S. C., & Nee, D. E. (2005). Processes of working memory in mind and brain.Current Directions in Psychological Science, 14, 2–5.
Kadesjö, B., & Gillberg, C. (1999). Developmental coordination disorder in Swedish 7-year-olds.Journal of the American Academy of Child and Adolescent Psychiatry, 38, 820–828.
Kane, M. J., Hambrick, D. Z., Tuholski, S. W., Wilhelm, O., Payne, T. W., & Engle, R. W. (2004).The generality of working memory capacity: A latent variable approach to verbal and visuo-spatial memory span and reasoning. Journal of Experimental Psychology: General, 133,189–217.
Kaplan, B. J., Wilson, B. N., Dewey, D. M., & Crawford, S. G. (1998). DCD may not be a discretedisorder. Human Movement Science, 17, 471–490.
Lewis, M., Vance, A., Maruff, P., Wilson, P., & Cairney, S. (2008). Differences in motor imagerybetween children with Developmental Coordination Disorder with and without the combinedtype of ADHD. Developmental Medicine & Child Neurology, 50, 608–612.
Mandich, A., & Polatajko, H. J. (2003). Developmental coordination disorder: Mechanisms,measurement and management. Human Movement Science, 22, 407–411.
Martinussen, R., Hayden, J., Hogg-Johnson, S., & Tannock, R. (2005). A meta-analysis of work-ing memory impairments in children attention-deficit/hyperactivity disorder. Journal of theAmerican Academy of Child and Adolescent Psychiatry, 44, 377–384.
Mehta, M. A., Goodyear, I. M., & Sahakian, B. J. (2004). Methylphenidate improves working mem-ory function and set-shifting AD/HD: Relationships to baseline memory capacity. Journal ofChild Psychology and Psychiatry, 45, 293–305.
Pennington, B. F., & Ozonoff, S. (1996). Executive functions and developmental psychopathology.Journal of Child Psychology and Psychiatry, 37, 51–87.
Piek, J. P., Dyck, M., Nieman, A., Anderson, M., Hay, D., Smith, L. et al. (2004). The relation-ship between motor coordination, executive functioning and attention in school aged children.Archives of Clinical Neuropsychology, 19, 1063–1076.
Piek, J. P., Dyck, M. J., Francis, M., & Conwell, A. (2007). Working memory, processing speed andset-shifting in children with DCD and ADHD. Developmental Medicine & Child Neurology, 49,678–683.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
imer
ick]
at 1
4:01
28
Apr
il 20
13

494 T. PACKIAM ALLOWAY
Pitcher, T. M., Piek, J. P., & Hay, D. A. (2003). Fine and gross motor ability in boys with AttentionDeficit Hyperactivity Disorder. Developmental Medicine & Child Neurology, 45, 525–535.
Sergeant, J. (2000). The cognitive-energetic model: An empirical approach to attention-deficithyperactivity disorder. Neuroscience and Biobehavioural Reviews, 24, 7–12.
Skuse, D., Warrington, R., Bishop, D. V. M., Chowdury, U., Mandy, W., & Place, M. (2004). TheDevelopmental, Diagnostic and Dimensional Interview (3di): A novel computerised assessmentfor Autistic Spectrum Disorders. Journal of the American Academy of Child and AdolescentPsychiatry, 43, 548–558.
Sonuga-Barke, E. J. S. (1994). Annotation: On dysfunction and function in psychological theories ofchildhood disorder. Journal of Child Psychology & Psychiatry, 35, 801–815.
Sonuga-Barke, E. J. S. (2003). The dual pathway model of AD/HD: An elaboration of neuro-developmental characteristics. Neuroscience and Biobehavioral Reviews, 27, 593–604.
Swanson, H. L., & Beebe-Frankenberger, M. (2004). The relationship between working memory andmathematical problem solving in children at risk and not at risk for math disabilities. Journal ofEducation Psychology, 96, 471–491.
Swanson, H. L., & Sachse-Lee, C. (2001). Mathematical problem solving and working memory inchildren with learning disabilities: Both executive and phonological processes are important.Journal of Experimental Child Psychology, 79, 294–321.
van Mourik, R., Oosterlaan, J., & Sergeant, J. A. (2005). The Stroop revisited: A meta-analysis ofinterference control in AD/HD. Journal of Child Psychology and Psychiatry, 46, 150–165.
Visser, J. (2003).Developmental coordination disorder: A review of research on subtypes andcomorbidities. Human Movement Science, 22, 479–493.
Wechsler, D. (1993). Wechsler Objective Reading Dimensions (WORD). London, UK: PsychologicalCorporation.
Wechsler, D. (1996). Wechsler Objective Number Dimensions (WOND). London, UK: PsychologicalCorporation.
Wechsler, D. (1999). Wechsler Abbreviated Scale of Intelligence (WASI). London, UK:Psychological Corporation.
Willcutt, E. G., Pennington, B. F., Olson, R. K., Chhabildas, N., & Hulslander, J. (2005).Neuropsychological analyses of comorbidity between reading disability and attention deficithyperactivity disorder: In search of the common deficit. Developmental Neuropsychology, 27,35–78.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
imer
ick]
at 1
4:01
28
Apr
il 20
13





























