Embed Size (px)
Citation preview
A BAC K I NJ U RYP R E V E N T I O N G U I D EF O R H E A L T H C A R E P R O V I D E R S

NO ONE IS REQUIRED TO USE THEINFORMATION IN THIS GUIDE
The guide is based on currently available information,but the study of how to prevent back injuries is a dynamic process and new information is constantlybeing developed. Ask your staff for their ideas and input.
Try some of the suggestions in this book to see if theywork for your organization. Cal/OSHA will periodically update the information to include the latest developments.
ACKNOWLEDGEMENTSWriters and Editors:
Mario Feletto, Cal/OSHA Consultation Service,Education and Training Unit, Sacramento, CAWalter Graze, Cal/OSHA Consultation Service,Headquarters, San Francisco, CA
The authors wish to thank the following persons and institutions for support and assistance in the research and development of this document.
Editorial Review:
Zin Cheung, Cal/OSHA Consultation Service,Education and Training Unit, Sacramento, CADr. John Howard, Chief, Division of OccupationalSafety and Health, California Department ofIndustrial Relations, San Francisco, CA
Layout and Design:
Ghedeon Bere, Office of State Printing,State of California
Draft Document Preparation:
Bernadine Osburn, Cal/OSHA Consultation Service,Education and Training Unit, Sacramento, CA
Photography
Emi Manning, UC Davis
Institutional Cooperators for OnsiteEvaluation and Research:
U.C. Davis Medical CenterHome Health Care Services Department
Catholic Health Care WestMercy General HospitalMercy American River HospitalMercy Care
Sutter Health CareSutter General Hospital
Eskaton Greenhaven Country PlaceEskaton Village
Peer Reviewers (alphabetical order bylast name):
Vicky Andreotti, U.C. Davis Medical Center,Sacramento, CAMichael L. Bradley, Sutter Community Hospital,Sacramento, CAWilliam Charney, San Francisco General Hospital,San Francisco, CADebbie Coughlin, Mercy Health Care,Sacramento, CADianne Factor, UCLA-LOSH, Los Angeles, CASue Glumac, OSHA Training Institute, San Diego, CADan Leiner, Cal/OSHA Consultation, Santa FeSprings, CAEd Mills, Cal/OSHA Consultation Service, Fresno, CABob Reeves, California Chamber of Commerce,Sacramento, CA
(Rev. 11/97)

This booklet is designed to provide general guidance for employers and employeesabout how to prevent back injury as a result of lifting and moving patients andresidents. It may be useful in settings such as hospitals, nursing homes, assisted-living facilities, board and care homes, and during the provision of home healthcare. Some of the benefits of back injury prevention include decreased injuries andcosts, as well as increased efficiency and employee morale. The practicalsuggestions in this guide are focused on orderlies, attendants, nurses, nursingassistants and others who actually lift and move patients and residents. Theinformation was developed with the help of individuals and institutions in thehealth care field who have found effective ways to prevent back injuries.
ABOUT THIS GUIDEABOUT THIS GUIDE
The guide discusses how to:
Understand the scope of the back injury problemAnalyze the workplace to find work activities, equipment and related factorswhich may contribute to the development of back injuriesIdentify and implement improvement optionsEvaluate the results
••
••
A. Do Lifting and Moving Patients or Residents Lead to Injury? 3
B. Lifting and Moving Patients and Residents 4
Physical Demands of Work 5
Equipment and Facilities 6
Work Practice and Administrative Issues 7
Personal Factors 7
C. Evaluating Work Activities 8
Performing Work Task Evaluations 8
Work Evaluation Tools 8
D. A Closer Look at Improvement Options 17
The Good News: Back Injury Prevention Success Stories 17
Identifying Solutions 18
1. Patient or Resident Assessment 19
2. Assist Equipment and Devices 20
3. Work Practices 22
4. Lift Team 25
5. Other Measures 26
Institutional Equipment and Facilities 26
Maintenance 27
Administrative Measures 27
Exercise 27
Safety Gear 28
E. Resource Information 29
Assist Equipment and Devices 29
Design of Institutional Equipment and Facilities 33
Proper Work Practices 35
Body Talk 39
F. References 41
CONTENTSCONTENTSCONTENTS

3
The Health Care Industry is facing a big chal-lenge. Nationally, total lost workday injury andillness incidence rates for Hospitals (4.1) aregreater than those for Private Industry (3.6).The rates for Home Health Care (5.0) andNursing and Personal Care Facilities (8.8) are
similar to or greater than more typically haz-ardous industries, such as Construction (4.9).(Note: Incident rates represent the number ofinjuries and illnesses per one hundred full-timeemployees.) Nursing aides, orderlies and atten-dants have a risk of lost workday injuries andillnesses about 3.5 times that of the average pri-vate industry worker. Their rate is similar tothat for construction laborers (Reuser, Report onthe American Workforce, Bureau of Labor Sta-tistics, 1994). Other health care providers are al-so getting hurt often. Why are their rates high?Two words—back injuries.
Nurses and other health care providers havesimilar percentages. These numbers may noteven tell the whole story. One study found thatonly one-third of nurses reported work-relatedback injuries. (The Magnitude of Low-BackProblems in Nursing, Owen, B., West. J. Nurs.
Res., Vol. 11, pp. 234-242 (April 1989)
Health care workers are hurting their backswhile lifting, transferring and otherwise movingpatients or residents. The costs are enormous.The direct costs in workers’ compensation, med-ical treatment and vocational rehabilitation arevery high. In California, back injuries accountfor the largest proportion of incurred losses inthe workers’ compensation system. Claims in-volving back strain can cost about $4,000. Theaverage back injury case costs $25,000. Moreserious cases requiring surgery can cost $85,000(State Compensation Insurance Fund). Basedon the average cost stated above, nationally, the approximately 67,000 back injuries amonghealth care workers could total $1.7 billion inworkers’ compensation.
Additionally, indirect costs such as lost produc-tion, retraining and sick or administrative timecan be at least four times the direct costs. Anindirect cost of particular concern is the disrup-tion of the professional integrity of services pro-vided. Injured health care workers cannot workup to their full potential or may even leave theprofession due to back injuries. Lastly, there isthe toll on their personal lives.
These increasing injury costs are occurring si-multaneously with a national push to reducehealth care spending. This pressure to functionin a more cost-conscious manner is leading toan emphasis on home health, reorganizationsand downsizing. These trends, along with thetraditional aspects of the health care workplace(e.g., emergency situations, long or rotatingshifts, night work, a high census, or caring forlarge numbers of acutely ill individuals), makeback injury prevention more difficult.
In spite of all of these challenges, many healthcare institutions have successfully preventedback injuries by using a combination of innova-tive approaches. There are solutions that work!A first step is to take a closer look at the typesof work activities which can contribute to backinjuries.
A DO LIFTING AND MOVING PATIENTS OR RESIDENTSLEAD TO INJURY?
Bure
au o
f Lab
or S
tatis
tics
(BLS
) (1
995)
Other
Back Injury
Other
Back Injury
ALL PRIVATE INDUSTRY
OCCUPATIONS
NURSING AIDES,ORDERLIES,
ATTENDANTS
26%46%
(BLS
, 199
3)
BACK INJURIES - AS A PERCENT OF TOTAL LOST WORKDAY CASES
0
2
4
6
8
10
Nursing Care
Home Health
Construction
Hospitals
Private Industry
LOST WORKDAY INCIDENCE RATES

WHAT CONTRIBUTES TO BACKINJURIES ?
Lifting or moving patients or residents requiresthe interaction of the health care worker, the in-dividual being moved, the equipment used andthe work environment. There are a great varietyof activities involved, including:
Manual liftingLaterally transferring between two horizontal surfacesAmbulatingRepositioning in bed or chairsManipulating extremitiesTransporting patients, residents and equipmentPerforming activities of daily livingStopping falls or transfers from the floor Assisting in surgery
When lifting or moving pa-tients or residents, there are anumber of factors which canlead to the development or ag-gravation of back injuries, in-cluding:
1. Physical demands of work2. Equipment and facilities3. Work practices or
administrative issues4. Personal factors
4
Caring for people often necessitates lifting orhelping them move. Since these work tasks in-volve sick or fragile human beings, they aremore complicated and risky than handling ma-terials in industrial settings. Compared to ob-jects manually lifted or moved in industrial set-tings, the body is heavier, more delicate andawkward to handle. Also, the center of gravityand the distance to the patient or resident canchange during the handling activity. This cansuddenly put the provider in an awkward pos-ture or position and require them to make moreforceful exertions (e.g., when stopping a fall).
In addition, patients and residents can havemedical, psychological or other conditions thatcan complicate lifting or moving them.
Lastly, health care workers mustoften engage in prescribed mobi-lizations where the goal ofstrengthening muscles and in-creasing skills means that thepatients or residents are “pushed”closer to the limits of their abili-ties. This increases the chancefor abrupt movements and falls.
LIFTING AND MOVING PATIENTS AND RESIDENTSB
Have IV ’s, monitoring devices,dressings or other complicatingfactorsNot be able to communicate well(e.g., disorientation or deafness)Be uncooperative or actively resist Have widely varied ranges ofmobilityBe subject to changes in conditiondue to fatigue or medication
They may:•
•
••
•
••
•••••••
Combative patient
Complicating factors

••
When assisting in surgery, providers:
Stand for long periods with a bentneck and back Hold manual retractors, patient’sextremities or heavy instrument setsfor prolonged periods
Repetition
Repetition means performing thesame motion over and over again. Ifrepetitive motions are frequent orsustained, they can contribute to fa-tigue and injuries. The number andlength of rest periods, the associatedforce, and unfamiliar work activitiescan all affect the impact of repetitionon the body. For example:
Repeated repositioning in bedNumerous transfers to and from beds,chairs or commodes without rest breaks
Bent back
5
The physical demands of work generally include forceful exertions,awkward position or postures,and repetition.
Forceful Exertions
Force is the amount of physical exer-tion or muscular effort expended.How much force is used and howlong it is sustained are important fac-tors contributing to injuries. Theseare influenced by the weight and con-dition of patients, residents or equip-ment. The type of grips, body pos-ture, and number of repetitions canalso affect the amount of force re-quired. Examples of excessive forceinclude:
Lifting or transferring heavy patientsUnexpected or abrupt forceful motionsStopping patient or resident falls orlifting them off the floor after a fall
Awkward Position orPosture
Repeated bending, twisting, reachingor holding prolonged fixed positionscan contribute to injuries of the neck,shoulder and back. Bending the backforward when lifting places greatloads on the muscles, discs and liga-ments of the lower back. One of themost damaging activities is to bend,reach out and lift, and then twistwhile raising the trunk. The liga-
ments of the back do not supporttwisting movements very well, espe-cially when the back is bent forward.As pressures on the discs in the lowerback increase, the center or nucleus ofthe disc is forced backwards. If thedisc bulges or ruptures, this can dam-age the surrounding nerves. Examplesof awkward posture are:
Bending, twisting or reaching when:
Attaching gait or transfer belts withhandles (e.g., the bed or chair is toolow or far away)Providing in-bed medical care (e.g.,the bed is too low and side rails areup)Washing patient’s legs and feet in ashower chair (e.g., the shower chair istoo low and access is limited) Dressing or undressing patients or res-idents Repositioning or turning patients inbed (e.g., the side rails are up, bed istoo low, and the provider reachesacross patient or resident)Performing stand-pivot transfers(e.g., the wheelchair is too far from thebed and the providers twist their bodies instead of moving their feet inthe direction of the transfer)
THE PHYSICALDEMANDS OF WORK
Extended reach
•• •
•
•
•
•
•
•
•
•
Bent back

Equipment Design andMaintenance Issues
Holding, pushing or handling equip-ment can cause forceful exertions orawkward body postures. Some of theways equipment can cause problems include:
Jammed or worn wheels which make itharder to move and steerFaulty brakes which cause chairs or otherequipment to shift during transfersHard to reach controls or manual crankson beds, chairs, or equipment. These candiscourage providers from makingadjustments and cause them to assumeawkward postures or make forcefulexertionsHandles on beds, carts or otherequipment which are either the wrongsize or placed at an inappropriate height Missing attachable IV/Med poleswhich can lead to workers awkwardlypushing gurneys or wheelchairs with onehand and holding free-standing poleswith the other Older mechanical lift devices (forpatients or residents) which are hard tooperate, uncomfortable, unstable or evendangerousHigh or heavy medical, food or linencarts which require bending, reaching ortwisting to load or unload
•
•
•
•
•
•
•
6
Facilities Design andMaintenance Issues
Health care workers may beforced to assume awkwardpostures because rooms,bathrooms, hallways, andother spaces are small in size,crowded or have obstructions.These factors may alsoprevent getting help fromother employees or usingassist equipment. Poorlymaintained floors can causeslipping, tripping and abruptmovements when lifting ormoving patients, residents orequipment.
EQUIPMENT AND FACILITIES
Awkward, hard to crank
Hard to push and see over
Jammed wheel, faulty brakeHeavy cart, handles too high, hard to see over
High shower lip
Crowded room

7
These issues affect the equipment available to employees, the types of worktasks they perform and how these activities are accomplished. For example:
Lifting or moving patients or residents without help from assist equipment anddevices or other employeesPerforming unaccustomed physical work (e.g., a new hire, returning from a longabsence, or covering for absent employees)Using improper work practices (e.g., using poor body mechanics) Having ineffective equipment repair procedures (e.g., no standard repair tag) orlong repair turnaround timesNot storing, replacing or distributing equipment so that it is readily availableNot performing systematic patient or resident assessment Purchasing of equipment where selection is limited or there is no end-user review Training that is:a. limited only to proper body mechanics (e.g., does not include use of assist
equipment)b. not hands-on or reinforced on a systematic basis c. not demonstrated in a competency (Note: A competency is a testing or clinical evaluation where health care providersdemonstrate proficiency of the skills necessary for their particular job classification.)Poorly communicating job demands and expectations Not establishing physical job demands and essential job functions
WORK PRACTICE AND ADMINISTRATIVE ISSUES
PERSONAL FACTORS
•
•
••
••••
••
HOME AND RECREATIONAL ACTIVITIES
Our bodies do not stop functioning when we go home from work. Home andrecreational activities involving forceful exertions or awkward postures can alsolead to or aggravate back injuries. Some examples include sports and home re-pair work.
PHYSIOLOGICAL AND PSYCHOLOGICAL FACTORS
Physical fitness, weight, diet, exercise, personal habits and lifestyle may also af-fect the development of back injuries. Individuals who are not in good physi-cal condition tend to have more injuries. Excessive body weight can placeadded stress on the spine and is often associated with a higher rate of back in-juries. Previous trauma or certain medical conditions involving bones, joints,muscles, tendons, nerves and blood vessels (e.g., fractures, arthritis, history ofdisc problems or other back injuries) may predispose individuals to injuries.Psychological factors, such as stress, may influence the reporting of injuries,pain thresholds, and even the speed or degree of healing.
No help, bent back
Makeshift repair tag
The following sections are forthose who either will evaluate theworkplace or be responsible forselecting and trying out improve-ment options. Let us look at someuseful tools to gain insight intowhere potential problems in yourworkplace may lie.

8
PERFORMING WORK TASKEVALUATIONS
Gathering useful information is one way to startwhen addressing back injuries which arebrought to your attention. First, talk to the af-fected employees. What is the nature of theproblem and which specific work tasks are asso-ciated with it? Are the problems widespread,long-standing or severe? Is there a history ofsimilar complaints about a job classification,task, unit or floor? In the process of trying toreally understand the nature of the problem, usethe knowledge and expertise of individuals whocan help you (e.g., nursing personnel, superviso-ry staff, physical therapist, employee health,union representatives, maintenance or engineer-ing departments, etc.). Remember that you canaccomplish a great deal by:
Involving and communicating with employees Relying on the knowledge and skills you have in -house Using the simple tools given in this section
Besides talking to employees, you can determinethe types, numbers and severity of injuries andthe specific work tasks associated with them byanalyzing existing written records. This analysiscan help identify which work tasks are associat-ed with specific injuries. These records may in-clude:
OSHA Log 200, Employers’ and Doctors’ FirstReports of Occupational Injury and IllnessWorkers’ compensation claim recordsMedical or first aid records (while respecting con-fidential information)Workplace inspections, maintenance records, inci-dent or accident reports Employee reports or complaints
Based on the information you gather, you maydecide that the problems you are hearing aboutare connected to work activities. If this is the
case, you can take a closer look at work activitiesby performing a Work Task Evaluation. Worktask evaluations are simply a structured way oflooking at jobs, workstations, or equipment toidentify and analyze what aspects of the workmay be contributing to injuries. Work TaskEvaluations can also help clue you into what solutions may work.
WORK EVALUATIONTOOLS
You should have already identified where prob-lems are occurring. Pick a few areas that youthink may be the worst and can be easily ad-dressed. Involve the employees performing thework in evaluating the problems and coming upwith potential solutions. Use the following as-sessment tools to help you conduct your worktask evaluations:
Patient and Resident Handling ChecklistTask Analyzer Equipment ChecklistFacility Design ChecklistAdministrative Issues Checklist
There are instructions given for each of thetools.
EVALUATING WORK ACTIVITIESC
•• •••
••
•
•
••
•
•

9
1. Select the portion of the checklist which corresponds to the type of activitybeing evaluated:
TransfersAmbulating, Repositioning, ManipulatingTransporting or MovingMedically Related ActivitiesPerforming Activities of Daily Living
2. Fill out the checklist for each type of activity you wish to evaluate. Simplyplace a check mark (✓ ) in the rows and columns. Make additional copies of thechecklist when needed. Observers or employees performing the task can fill outthe checklist.
3. Make sure that typical work practices and equipment are used as you evaluatethe work. Watch individuals long enough to evaluate any changes in work activi-ties. Sample different employees performing the same jobs. Save your results forreview when you are considering improvement options.
After your evaluations, review your results and list the five activities you foundto be the most frequent and/or the hardest.
THE PATIENT AND RESIDENTHANDLING CHECKLIST
HOW TO USE YOUR CHECKLIST—AS EASY AS 1, 2, 3
•• •••
TOOL 1
1.
2.
3.
4.
5.

TOOL 1 — PATIENT AND RESIDENT HANDLING CHECKLISTTOOL 1 — PATIENT AND RESIDENT HANDLING CHECKLIST
(A) TRANSFERS
(1) BED TO AND FROM:
Chairs (e.g., regular/cardiac/geri/wheel/shower, etc.)
Gurneys
Floor
Other beds
Walker
Shower
Toilet/bedside commode
Bathtub
Other
(2) CHAIRS TO AND FROM:
Chairs (e.g., regular/cardiac/geri/wheel/shower, etc.)
Gurneys
Floor
Walker
Shower
Toilet
Bathtub
Other
(B) AMBULATING, REPOSITIONING, MANIPULATING
(1) Repositioning/Turning/Holding
Whole body (e.g., placing epidurals)
Extremities (e.g., exercising)
(2) Hand-cranking beds/equipment
(3) Assisting with ambulation
ACTIVITIES How often How hard Comments
Often Sometimes Hard Easy
10Make copies of all the pages with this symbol.
11
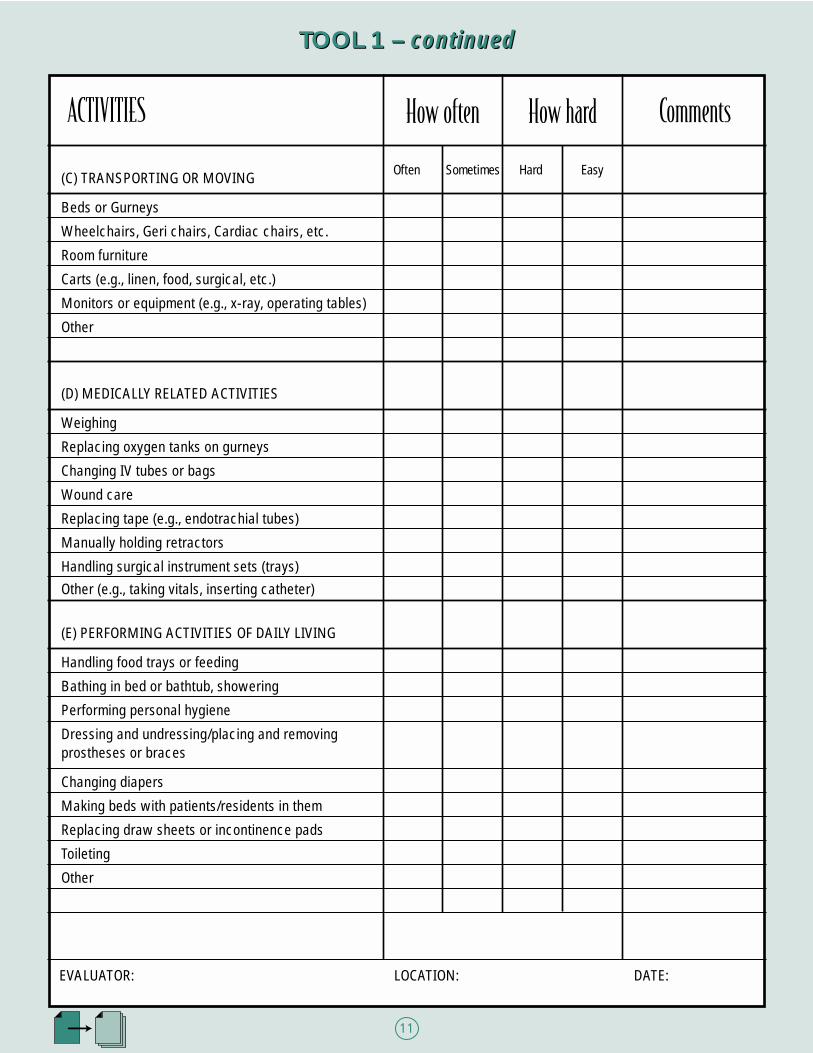
TOOL 1 – continued
(C) TRANSPORTING OR MOVING
Beds or Gurneys
Wheelchairs, Geri chairs, Cardiac chairs, etc.
Room furniture
Carts (e.g., linen, food, surgical, etc.)
Monitors or equipment (e.g., x-ray, operating tables)
Other
(D) MEDICALLY RELATED ACTIVITIES
Weighing
Replacing oxygen tanks on gurneys
Changing IV tubes or bags
Wound care
Replacing tape (e.g., endotrachial tubes)
Manually holding retractors
Handling surgical instrument sets (trays)Other (e.g., taking vitals, inserting catheter)
(E) PERFORMING ACTIVITIES OF DAILY LIVING
Handling food trays or feeding
Bathing in bed or bathtub, showering
Performing personal hygiene
Dressing and undressing/placing and removing prostheses or braces
Changing diapers
Making beds with patients/residents in them
Replacing draw sheets or incontinence pads
Toileting
Other
TOOL 1 – continued
Often Sometimes Hard Easy
ACTIVITIES How often How hard Comments
EVALUATOR: LOCATION: DATE:

12
THE WORK TASK ANALYZER
HOW TO USE YOUR TASK ANALYZER
TOOL 2
1. The purpose of Tool 2 is to evaluate in more detail the work tasks you have alreadyanalyzed with Tool 1—the Patient and Resident Handling Checklist. You may wantto do this if the problem is especially complicated, severe or widespread. A more in-depth analysis can also provide greater insights into the nature of the problem andpotential improvement options.
2. Analyze separately each of the tasks you previously evaluated using Tool 1— The Patient and Resident Handling Checklist. List one specific task in the space provided. For example:
Bed to gurney transferManipulating extremities for wound careMoving room furnitureBed to chair transfer
3. As you observe the task, simply place a check mark in the appropriate boxes andfill in your comments. Check as many boxes as may apply. Save your results for re-view when you are considering improvement options.
•• ••
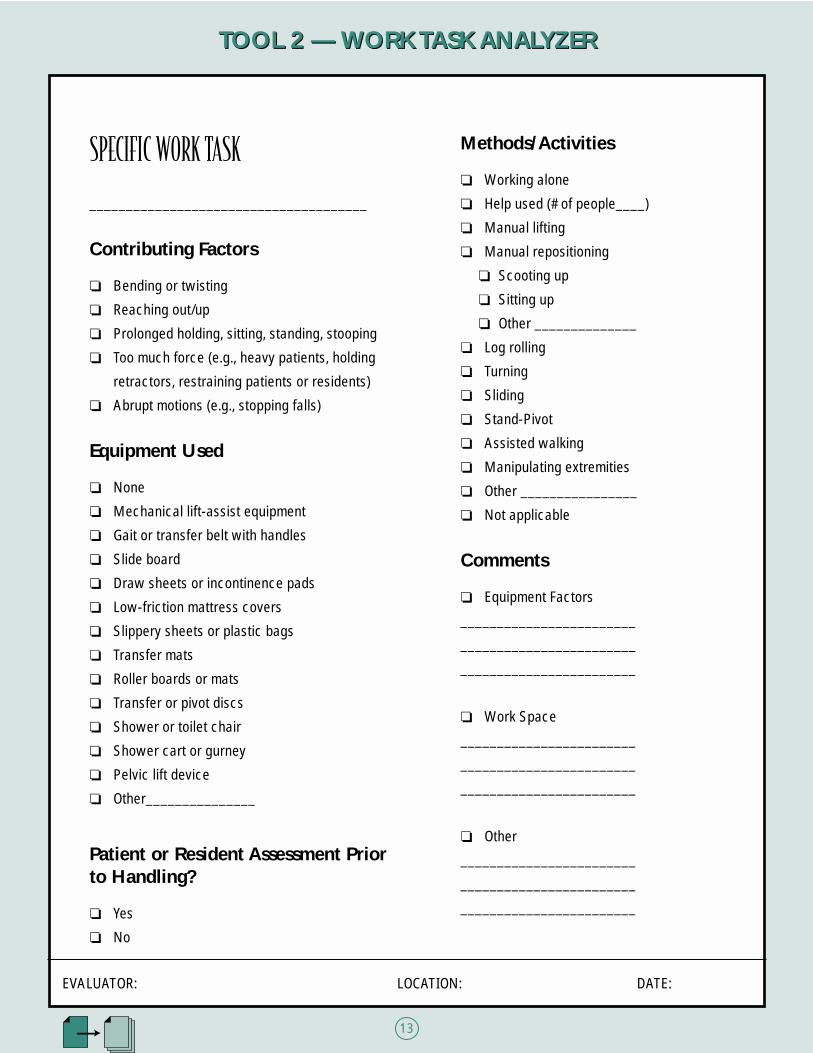
TOOL 2 — WORK TASK ANALYZERTOOL 2 — WORK TASK ANALYZER
13
SPECIFIC WORK TASK
______________________________________
Contributing Factors
❏ Bending or twisting
❏ Reaching out/up
❏ Prolonged holding, sitting, standing, stooping
❏ Too much force (e.g., heavy patients, holding
retractors, restraining patients or residents)
❏ Abrupt motions (e.g., stopping falls)
Equipment Used
❏ None
❏ Mechanical lift-assist equipment
❏ Gait or transfer belt with handles
❏ Slide board
❏ Draw sheets or incontinence pads
❏ Low-friction mattress covers
❏ Slippery sheets or plastic bags
❏ Transfer mats
❏ Roller boards or mats
❏ Transfer or pivot discs
❏ Shower or toilet chair
❏ Shower cart or gurney
❏ Pelvic lift device
❏ Other_______________
Patient or Resident Assessment Prior to Handling?
❏ Yes
❏ No
Methods/Activities
❏ Working alone
❏ Help used (# of people____)
❏ Manual lifting
❏ Manual repositioning
❏ Scooting up
❏ Sitting up
❏ Other ______________
❏ Log rolling
❏ Turning
❏ Sliding
❏ Stand-Pivot
❏ Assisted walking
❏ Manipulating extremities
❏ Other ________________
❏ Not applicable
Comments
❏ Equipment Factors
________________________
________________________
________________________
❏ Work Space
________________________
________________________
________________________
❏ Other
________________________
________________________
________________________
EVALUATOR: LOCATION: DATE:

1414
TOOL 3 — EQUIPMENT CHECKLIST
Place a check mark (✓ ) in the appropriate row or column to help identify problems with your equipment
Faulty brakes
Takes too long or hard to adjust
Casters/wheels do not roll easily
Too low/high
Too heavy/wide/big/unstable
Controls/handles in awkward position
Handles missing
Storage of items too low/high/awkward/far away/hard to find
Hard to steer
Design not appropriate for patient/resident condition
Armrests/foot pads not removable/adjustable
Items missing (e.g., slings, IV/Med poles)
Other
Faulty brakes
Takes too long or hard to adjust
Casters/wheels do not roll easily
Too low/high
Too heavy/wide/big
Controls/handles in awkward position
Handles missing
Storage of items too low/high/awkward/far away/hard to find
Hard to steer
Design not appropriate for patient/resident condition
Armrests/foot pads not removable/adjustable
Items missing (e.g., slings, IV/Med poles)
Other
BEDSFACTOR GURNEYS MEDICAL EQUIPMENT COMMENTSCARTS(or rails) (or rails) Medicine Surgery Food Laundry Monitor X-ray Other
LIFTDEVICES
FACTOR IV/MEDPOLES
CHAIRS OTHER COMMENTSGeri Cardiac Wheel Shower Toilet Other Equipment
EVALUATOR: LOCATION: DATE:
TOOL 3 — EQUIPMENT CHECKLIST

TOOL 4 — FACILITY DESIGN CHECKLISTTOOL 4 — FACILITY DESIGN CHECKLIST
1515
Place a check mark (✓ ) in space next to each item you feel may be a problem in your facility
FACTOR PROBLEM LOCATIONHigh threshold or obstructions in entry ways of bathrooms,showers, hallways, etc. prevent access for assist equipment
Steep ramp (greater than 10 degrees)
Small or cluttered rooms/bathrooms/hallways or other spaces
Door handles catch on beds/gurneys/etc.
Floors slippery/uneven/cluttered
Storage areas too high/low/awkward to reach
Bedside medical and electrical outlets too low/only on one side
Inadequate storage space
No grab rails by toilets or in bathtubs or showers
Toilet seats too low
Other
1
2
3
4
5
6
7
8
9
10
11
EVALUATOR: LOCATION: DATE:

TOOL 5 — ADMINISTRATIVE CHECKLISTTOOL 5 — ADMINISTRATIVE CHECKLIST
16
Based on observations in your facility, place a check mark (✓ ) in the NO column to help identify areas that may need a closer look
FACTOR NOYES COMMENTSSystematic patient or resident assessment
Formal policy or criteria for:
Getting help or using assist devices
Early reporting of problems
Guiding instead of stopping falls
Equipment maintenance:
Standardized tags
Short turnaround time
Effective tracking systems
Equipment purchasing/distribution:
Flexible contracts
Systematic end-user reviews
Sufficient quantities ordered
Adequate storage
Communication with employees by:
Meetings
Bulletin boards or memos
In-service or training sessions
Other means (please specify)
Job expectations clearly communicated
Training:
All employees trained
Hands-on practice
Opportunity for feedback
Content is comprehensive (e.g., equipment, policies, etc.)
Demonstrated in competency
Systematically reinforced
Other (please specify)
Where possible, physically hard work tasks distributed equallyamong employees or shifts
Where possible, scheduling avoids employees performingunaccustomed physical work
Other (e.g., effective early reporting)
1
2
3
4
5
6
7
8
9
10
EVALUATOR: LOCATION: DATE:

Here are just a few success stories showing how some institutions have been successful.
San Francisco General Hospital, California 275 bedsProblems: Many back injuries and high employee turnover due to lifting and moving of patients.Solutions: No lifting by nursing staff. Specially trained lifting team performs almost all patientlifting or moving of patients on the day shift. Policy of the lift team was to use mechanical lifting devices for all total body transfers.Results: In the first year of implementation, lost-time back injuries dropped from 16 to 1 andlost days from 215 to 6. By the second year, the nursing staff did not have one single back in-jury during the lift team’s shift. In the six years since the program began, workers’ compensa-tion costs dropped approximately 90%. The lift team’s cost was $70,000 per year.
Camden Nursing Home, Maine approx. 260 employees and 200 bedsProblems: High incidence of low-back pain and pulled muscles resulting from lifting or movingof residents.Solutions: Lift assist equipment required for all lifts (total cost of equipment was approximately$35,000); two employees required (using gait or transfer belt with handles) for all ambulationswhere residents are unstable; training from equipment manufacturers.Results: Workers’ compensation premium reduced from $750,000 to $184,000.
Kennebec Long-term Care, Maine approx. 250 employees and 300 bedsProblems: Low back strains, herniated discs, and shoulder strains from lifting, poor body me-chanics, resident falls and combative Alzheimer patients.Solutions: Employee committee (Certified Nursing Assistants) formed to evaluate mechanical liftassist equipment; systematic resident assessment instituted; use of gait belts required; full bodyand stand-assist lifts required for lifting or moving residents; comprehensive employee training;safety rewards and newsletters; modified duty programs instituted.Results: Workers’ compensation premiums dropped from $1.5 million in 1992 to $770,000 in1996. Number of lost work days dropped from 573 in 1991 to 12 in 1996.
17
Health care institutions which have been suc-cessful in preventing back injuries have em-ployed a multi-faceted approach involving:
Systematic patient or resident assessmentAssist equipment and devicesSafer work practicesLift teamsOther measures (e.g., proper equipment mainte-nance)
Comprehensive training
A CLOSER LOOK AT IMPROVEMENT OPTIONSD•• •••
•
THE GOOD NEWS: BACK INJURY PREVENTION SUCCESS STORIES
T
O
R
I
E
S
U C C E S SS

18
Once problem work activities havebeen identified and evaluated, how doyou decide which ones to address firstand what changes are appropriate?Review the information you havegathered up to this point to guideyour choices. Talk to the affected em-ployees to get their ideas on how toimprove their work activities. Coordi-nate the knowledge and expertise ofin-house staff to identify and try outsolutions. Depending on the natureand severity of the problems, it maybe useful to consult with:
Nursing Administration andSupervision Health and Safety CommitteesPurchasingMaintenanceQuality AssuranceHuman ResourcesUnion RepresentativesPhysical and Occupational TherapyEmployee HealthWorkers’ Compensation Risk ManagementFinance
Also, you can contact others in thehealth care industry, equipment ven-dors and private consultants.
SELECTING SPECIFIC IMPROVEMENT OPTIONS
Do you have the responsibility andauthority to implement any improve-ment measures? Securing manage-ment commitment will be essential tobring about positive change. Persuadethe decision makers in your organiza-tion by presenting the direct and in-direct costs of the problems andpointing out the injury reduction andcost-saving benefits. Keep in mindthat the benefits of improved employ-ee morale, patient comfort and betteremployee relations are not easily mea-sured.
First, recognize what is working welland try to key in on specific changesto make. Keep in mind that manyproblems once identified can besolved by quick fixes or simple, com-monsense improvements.Remember, start small and pick op-tions you can realistically put intoplace. As you progress, build on yourearly successes. Talk to the affectedemployees to get suggestions on howto modify improvements.
Some institutions have found the fol-lowing improvement options to be effective at reducing or preventingback injuries.
1.) Patient or Resident Assessment 2.) Assist Equipment and Devices3.)Proper Work Practices4.) Lift Teams5.) Other Measures
Institutional Equipment andFacilitiesMaintenanceAdministrative MeasuresExerciseSafety Gear
These suggestions are not the onlyones possible and may need to be al-tered to fit your particular situation.
In addition to workers’ compensation savings and reduced injuries, some institutions have experienced other significantbenefits from implementing an appropriate combination of improvement options. These include:
•• ••••
IDENTIFYING SOLUTIONS
•
• ••••••••••
Reduced absenteeism, turnover, and retrainingLower administrative costsMaximized efficiency and productivityImproved employee moraleImproved employee-management problem solvingIncreased patient or resident comfort
•
••••

Systematic patient or resident assess-ment, which is focused on the liftingor moving of the patient or resident,is essential to protect against injury.Unexpected movements, especiallyfalls, can hurt both the employee andthe patient or resident.
What information should theassessment include?
Many aspects of the patient’s or resi-dent’s condition can affect how theyare lifted or moved. In addition totheir weight, consider the following:
Medical Condition What could make them vulnerable to
further injury?
dizziness confusion deafnessmedicationmuscle spasmsrecent surgery sensitive skintotal hip replacement
Physical AbilityHow well can they sit up, stand up or
walk on their own? What is their endurance?
ambulatorystroke-weak on one sideweight-bearingupper-body strength
AcuityHow well do they follow
instructions?
general understandinglanguage problem
19
1.) Patient or Resident Assessment
•• ••••••
•• ••
••
BehaviorWhat might they do?
combativecooperative unpredictable
Use the assessment to decide the ap-propriate type of assist equipment ordevices, the techniques and numberof people needed and other relevantconsiderations. Always check thecondition of the patient or residenteach time before you begin and dur-ing the activity. Their medical condi-tion can change from day-to-day (forbetter or worse), during the day (fromfatigue, medication or other factors),and even during the activity.
How should the results of theassessment be communicatedto all who need to know?
Prior to lifting or moving patients orresidents, employees should be en-couraged to systematically review anyinformation relevant to the transferactivity. This information should bereadily available and clearly state theessential facts. Labels or signs cancommunicate the essential points in asimple manner. If there is a need topreserve confidentiality, you can usecolor-coded stickers that summarizeinformation. Another way to commu-nicate the information is to have briefdaily meetings. Finally, rememberthat patients’ or residents’ medicalconditions can change rapidly. As-sessments may need to be updatedand the new information sharedamong providers.
Independent
Minimum Assistance
Totally Dependent
•• •
Logos credit: Pg 42, Ref 4.

•••••
20
There are many types of equipmentand devices designed to make liftingor moving patients or residents easier.Remember, it is important to useproper work practices and body me-chanics in combination with equip-ment and devices. The following discussion categorizes assist equip-ment and devices by the type of workactivity in which they are used.
Lifting
Mechanical assist devices (e.g., lifts)help reduce injury by avoiding unnec-essary manual transfers, awkwardpostures, forceful exertions and repet-itive motions. Although these devicesmay appear to take longer to performthe lift or move, they may save stafftime by reducing the number of em-ployees needed on a given transfer.
Based on your evaluations, mechani-cal assist devices should be used forthe most potentially dangerous liftingor moving tasks.
Mechanical lifting devices eliminatethe need to manually lift or move pa-tients or residents:
To and from beds, chairs, gurneys, etc.Off of the floorTo a standing positionUp or over in bedDuring ambulationIn and out of vehiclesInto or out of bathtubs or showers
General categories of mechanical liftsinclude:
Total-body Stand-assistCompact (total-body or stand-assist)AmbulationBath/shower
Lifting devices have different fea-tures. When evaluating these deviceslook for those that:
Lift from floor up to the highest bedAllow the employee to operate theequipment in an upright, neutral pos-tureSteer and operate easilyAre stable and comfortable for thepatient or residentHave effective and easy to adjustbrakesFit easily into rooms, bathrooms, orsmall spacesCan go under beds and around equipmentHave slings which:- Attach with minimal lifting or
pulling - Come in a variety of sizes - Provide patient or resident comfort
(e.g., support the head, arms and legs)
Lift the heaviest, biggest, or smallestpatient or residentHave a bump sensor or emergency stopswitchDo not catch or pinch the body or thefeet Are easy to clean and maintainHave rechargeable batteries with suf-ficient capacity and fast chargingtimes
2.) Assist Equipment and Devices
•• •••••
Total-body lift
Stand-assist lift
Off the floor
••
••
•
•
•
•
•
•
•
••
Lifting device fits easily in bathroom
For more information on these de-vices and the proper work practices
associated with them, see pages 29-30 and 35-38.

21
Lateral Transfers (Sliding )
Lateral transfers or sliding can beused to move patients and residentsbetween two horizontal surfaces (e.g.,bed to gurney or bed to cardiac chair,etc.). Helpful equipment and devicesinclude slide boards, transfer mats,slippery sheets, draw sheets and in-continence pads. For more informa-tion on these and other devices andthe proper work practices associatedwith them, see pages 30 and 35-38.
Ambulating, Repositioning andManipulating
For help with these types of activities,use equipment and gait belts, transferbelts with handles, slippery sheets,plastic bags, draw sheets, inconti-nence pads, pivot discs, range of mo-tion machines, fixtures, etc. For moreinformation on these and other de-vices, as well as the proper work prac-tices associated with them, see pages30-31 and 35-38.
Performing Activities of DailyLiving
These activities include showering,bathing, toileting, dressing or un-dressing, and performing personal hygiene and related activities.Equipment and devices includeshower-toilet combination chairs, ex-tension hand tools, shower carts andgurneys, pelvic lift devices, etc. Formore information on these and otherdevices, as well as the proper workpractices associated with them, seepages 31-32 and 35-38.
Useful Tips
Health care workers should be en-couraged to use assist equipment anddevices when they are appropriate.To facilitate use, they should be:
Purchased in sufficient quantities Stored so they are visible and readilyavailableEvaluated and selected by the usersAccompanied by effective training Equipped with sufficient replacementaccessories (e.g., slings)Maintained in good working order
2.) Assist Equipment and Devices — continued
Draw sheet
Slide board
Transfer belt with handles
Shower-toilet chair with wheels
Slippery sheet with handles
••
•••
•

22
Health care providers can be injuredwhen manually lifting or moving pa-tients, residents or equipment. Man-ual handling can also be uncomfort-able for the patients or residents (e.g.,the under-the-axilla-lift). Consultinga physical therapist or reference textson proper body mechanics can alsohelp in evaluating lifting or othermanual activities. Whenever manualhandling of patients or residents isperformed, employees must be thor-oughly trained, including “hands-on”practice sessions under supervision.
Even when performed properly, man-ual lifting or moving of patients orresidents involving awkward positionand posture or forceful exertions (e.g.,lifting extremely heavy individuals)can still result in employee injury. Inthese situations, consideration shouldbe given to the use of mechanical lift-ing devices or other assist equipment.Prior to using mechanical lifting de-vices or other assist equipment, em-ployees need to be thoroughly trainedon how to use the equipment and onproper work practices.
The discussion which follows de-scribes the general principles of man-ually lifting and moving patients andresidents. See the Resources Infor-mation section on page 35-38 formore detailed information on the following:
Lifting and lateral transfersAmbulating, repositioning andmanipulatingTransporting patients, residents andequipmentPerforming activities of daily livingTransferring from the floorAssisting in surgery
3.) Proper Work Practices
••
•
•••
Assess the patient or resident before lifting or moving them
Eliminate or reduce manual lifting and moving of patients or residents
whenever possible. Use assist devices or equipment when available and ap-
propriate for the activity
Get patients or residents to help as much as possible by giving them clear,
simple instructions with adequate time for response
Know your own limits and do not exceed them
Get help whenever possible
Use teamwork. Try to choose team members who:
- are adequately trained, and;
- have a similar understanding of proper techniques and timing
Mentally plan and prepare (e.g., consider routes of travel and obstructions;
clear out paths)
Use (or modify) chairs, beds or other surfaces to keep work tasks, equipment
and supplies close and at the correct height (i.e., between the waist and
shoulders)
Make sure brakes hold properly and apply them firmly on beds, gurneys,
chairs, etc.
Use upright, neutral working postures and proper body mechanics
- Bend your legs, not your back. Use your legs to do the work
- When lifting or moving the patient or resident always face them
- Do not twist when turning. Pick up your feet and pivot your whole body
in the direction of the move
General Guidelines for Lifting and Moving Patients or Residents
••
•
••
•
•
•
•
The photos on the followingpage illustrate proper workpractices for some typical activities involving lifting andmoving patients and residents.

23
3.) Proper Work Practices — continued
Lateral transfer—working together, good posture (e.g.,straight back and minimal reach)
Performing an ADL—good posture (straight back, bent knees)
Repositioning—good body mechanics (e.g., straightback, patient close, bed at waist height)
Transporting patient—adequate helpTransfer from floor—using a slide board, enough help and a coordinated effort

24
Guiding and Slowing Falls
Reviewing patient or resident assess-ments and watching for signs ofweakness are effective ways of pre-venting falls. If falls do occur, no at-tempt should be made to stop themabruptly. Stopping falls is a sure wayto get hurt. The safest method in-volves guiding, slowing and loweringthe patient or resident to the floorwhile trying to maintain a neutralbody posture. Regulatory reportingrequirements may cause employees totry stopping a fall. Reporting of fallsshould not lead to fault-finding ornegative consequences.
Providing Home Health Care
This is a difficult situation for health care workers. Facilities and equipment are not under their control and they cannot get help from other employees. However, there are a few helpful strategies that can be followed:
Protect the patient
Protect your back, keep it straight
Using a gait belt Small lift for the home
Low chair, use good body mechanics
Low bed, crowded room
•• •••
Ask for help from the patient’s family or friendsProvide suggestions for the layout of bedrooms and other areasFollow correct body mechanicsMaintain clear spaces. Avoid trip or slip hazardsProvide suggestions for desirable equipment (e.g., gait belts, transfer devices appropriate for the home, shower-toilet chair combinations, extension hand tools for showering, adjustable beds, etc.). If medical supply companies do not stock these items, discuss other alternatives
3.) Proper Work Practices — continued

25
Even with the availability of the appropriate assist equipment, injuries can still occur because ofa variety of factors, including:
Limited equipment usageNot asking for help from coworkersTraining that “doesn’t stick”Loss of patient or resident handling skills Employee turnoverInconsistent policies for lifting or moving patients or residentsOther factors (e.g., cramped rooms, bathrooms or facilities)
4.) Lift Team
How can these complex variables be ad-dressed in order to effectively reduce in-juries? Some institutions have chosen tocreate a special “lift team” dedicated toperforming the majority of the lifting ormoving of patient or residents. This canbe effective because it reduces the risksby relying on only a few thoroughlytrained employees. The team’s policy isto use assist equipment and not performmanual lifting or moving activities unlessnecessary. The lift team coordinates withthe nurses and other medical personnelresponsible for the patient or resident.The team performs both scheduled andunscheduled moves and is available bybeeper.
In one study, the response time from onelifting or moving activity to the next wasfive minutes. A two-person lift teamhandled the load for a hospital with acensus of 350 to 400 patients, of whom8% to 12% were handled from 9 AM to5 PM. [see The Lift Team: A MethodTo Reduce Lost Time Injury In Nurs-ing, Charney, W., Journal of the Ameri-can Association of Occupational Health
Nursing (AAOHN), May 1991, VOL.39, No. 5, and, for a more recent studyof ten hospitals and nursing homes, TheLift Team Method For Reducing BackInjury: A Ten Hospital Study, Charney,W., AAOHN, June 1997, VOL. 45,No. 6]
The lift team dramatically reduced backinjuries and their associated costs. Therewere also significant savings on adminis-trative and equipment costs. The studyfurther suggested that the use of the “liftteam” was beneficial to patients since itallowed them to be moved or transferredmore frequently in a safer, easier manner.
When considering the use of a lift team,keep in mind that:
It may be difficult to cover all lifting ormoving activities (e.g., dispersed facili-ties, medical emergencies or night orweekend shifts)There may be organizational constraints(e.g., no centralized staff that functionsacross departments, wards, or units)
•• •••••
•
•

26
Institutional Equipmentand Facilities
Well-designed and maintained insti-tutional equipment and facilities areimportant in reducing or preventingback injuries. Institutional equipmentshould be designed to allow the userto maintain neutral body postures andreduce forceful motions. For example:
Beds, wheelchairs, cardiac chairs andother equipment that are easy toadjust and moveEquipment with wheels that roll andsteer easily. These can decrease the forceand number of people needed For more detailed information on
beds, carts, chairs, gurneys and otherequipment, see the Resource Infor-mation section on page 33-34.
Facilities should be designed to alloweasy operation and movement ofequipment. During lifting or movingactivities, there should be enoughroom for staff to avoid awkward pos-tures and for other employees to help.For example:
Patient, resident, shower and bathrooms (and other areas) with adequatework space Low thresholds on entryways thatallow the use of equipment withwheels (e.g., rolling shower chairswhich eliminate an extra transfer)
For more detailed information onrooms, floors, hallways and otherareas see the Resource Informationsection on page 34.
5.) Other Measures
•
•
Attachable pole, 5th wheel, easy steering
Foot-operated bed control Enough space to work
Large shower room
Low threshold
Hand-held bed control
•
•
Handles allow neutral grip; cart not toobig or high
Adjustable or removable foot rests andarm pads

•
•
•
•
•
•
•
•
•
MaintenanceMaintenance personnel have an im-portant role to play in back injuryprevention programs. A regular pro-gram of maintenance can help ensuresufficient quantities of equipment inall units or floors and avoid shortagesand breakdowns.Systematic preventative maintenanceshould include:
Checking brakes for their ability tolock and holdOiling and adjusting mechanisms towork easily (e.g., to prevent stuckcranks or rails)Cleaning or replacing casters or wheelsso they roll easily and smoothlyReplacing and securing attachments(e.g., slings, bed controls, or foot-boards) Using standardized tags that have thename of the person reporting the prob-lem, their department, the date andthe problem description Instituting tracking systems to ensureprompt turnaround times Maintaining equipment instructionmanuals
Maintaining facilities properly can al-low easy equipment movement andreduce tripping or slipping.For example:
Keeping floors free of holes, clutter,broken tiles or slippery conditionsAdjusting doors to open easily
27
float pool may perform physical worktasks they are not accustomed to(e.g., lifting, pushing, being on one’sfeet all day, etc.). Performing unac-customed physical work can increasethe risk of back injuries. Where pos-sible, new or returning employeesshould be encouraged to increasegradually the pace or difficulty oftheir work activities.
Other Ideas
Other administrative measures to reduceor prevent back injuries can include:
Return-to-work and light-duty programsJob descriptions which establish theappropriate physical requirements Early reporting and treatment.Employees should be encouraged toreport physical problems or otherwork-related issues as early as possible.This is particularly important withback injuries which are less costly andserious at first, and more expensiveand severe in later stages
Exercise
A combination of the appropriateequipment, proper work practices andexercise programs can be effective atinjury prevention. Physically fit indi-
Administrative Measures
Equipment Purchase,Storage and Distribution
Some basic considerations include:Conducting a review that evaluates ifthe equipment is appropriate for thespecific lifting or moving activity.The review should involve onsite test-ing of a variety of equipment by theend usersOrdering a sufficient quantity ofequipment and attachments. This willallow the equipment to be readilyavailable at all the various locationswhere it is needed (e.g., enough lifts orIV/Med poles that are permanentlyattached to gurneys)Providing for the convenient storageof assist and institutional equipment.This can ensure that equipment is easyto find and, in turn, help encouragehealth care workers to use itUsing flexible purchasing proceduresthat allow for the evaluation and pur-chase of up-to-date equipment withthe most appropriate features
Remember that many equipment manufacturers or distributors are happyto provide samples of equipment forin-house demonstrations or evalua-tions.
Work Coordinating Tips
Certain work tasks may be especiallyhard to perform. Try to:
Break up tasks with rest breaks orlighter workSchedule hard tasks for early in thework shiftShare tasks more equally among shiftsSpecify criteria for getting help
Employees who are new, returningafter long absences or members of a
•
•
•
•
•
•
•
•
•
••
5.) Other Measures
Replacing wheels

•
•
•••
•
•
28
viduals tend to have fewer and lesssevere injuries.They also recoverfaster if they are hurt. Other potentialbenefits from long-term, sensible ex-ercise programs include:
Increased balance, coordination,strength and flexibilityWeight reductionReduced fatigue, stress and tension
Employers should encourage employ-ees to:
Warm up and stretch before engagingin work activities Participate in long-term, sensibleexercise programs involving aerobicconditioning and other appropriateactivities
Remember to consult with a physi-cian or physical therapist about whichaerobic, strength and flexibility exer-cises are right for the employee. Thisis especially important for those indi-viduals who have pre-existing injuriesor medical conditions.
Safety GearSafety gear includes items worn orattached to the body. Some consider-ations when selecting safety gear arediscussed below.
Footwear
The appropriate footwear can providegood traction to help prevent slips orfalls and cushioning when standing orwalking for long periods on hard sur-faces.
Back Belts
Back belts may help maintain theproper curvature of the spine duringlifting or physical exertion by apply-ing intra-abdominal compression onthe lumbar section of the spine.However, the use of back belts in pre-venting injuries remains a question
that requires further analysis. Studieshave not produced a conclusive bodyof evidence supporting the effective-ness of back belts as an injury reduc-tion tool (see Workplace Use of BackBelts, Review and Recommendations,NIOSH Back Belt Working Group,May 1994). One recent study con-ducted in an industrial setting sug-gests that back belts when accompa-nied by other measures may reducelow back injuries (see Reduction ofAcute Low Back Injuries by Use ofBack Supports, Kraus, et al., Interna-tional Journal of Occupational andEnvironmental Health, Volume 2,Oct.-Dec. 1996). Currently, there areno studies that address the effective-ness of back belts as an injury preven-tion tool in health care. Some con-cerns related to the use of back beltsare that they:
Provide a false sense of security andlead employees to lift loads beyondtheir capabilities Are used in lieu of other more provenoptionsMight not be worn properlyMay lead to decreased abdominalmuscle strength with prolonged use
TRYING OUT IMPROVEMENTOPTIONS
To effectively implement the improve-ment options selected, it is helpful toset a schedule, provide training and getfeedback on how changes are working.
Training
Effective training is an importantpart of trying to reduce or prevent in-juries. You have gathered a lot ofgood information. Look back at yournotes. Review the Work EvaluationTools, the improvement options andthe information in this booklet. All ofthese sources provide good informa-tion on the nature and causes of backinjuries, as well as measures to help
reduce or prevent them. You can nowuse the information and experiencesyou have accumulated in combinationwith your in-house expertise to helpwith the training. Keep in mind thattraining is not effective at reducinginjuries unless it:
Includes classroom education andhands-on practiceAllows feedback Requires that employees demonstratethe skills learned in a competencyevaluationIs systematically reinforced by retraining
Some areas to consider in your train-ing program are:
Anatomy and physiology related toback injuriesProper work practices and adminis-trative measuresPatient or resident assessmentAssist equipment and devicesReporting of injuries, equipment andfacility problems
Finally, remember that for training tobe successful at reducing employeeinjuries, management must providefirm support and workers must prac-tice the skills on a daily basis duringwork activities.
Getting Feedback
Open lines of communication allowyou to find out if improvements areworking and to respond quickly to newproblems. It is important to track theprogress of any improvements you tryout. Look to see if injuries and symp-toms associated with problem work ac-tivities are decreasing over time. Arethe improvements reducing costs andworking from a productivity and orga-nizational standpoint? When evaluatingimprovements, talk to your employeesand ask what suggestions they mayhave to refine the changes. Rememberto give the changes time to work andallow employees to get used to them.
•
••
•
•
••
•
••
•

LIFTS
Total-Body
These devices are designed to lift or move indi-viduals who are totally dependent by supportingtheir entire body weight during the transfer.The best devices are battery-operated. Typically,they can lift an individual from the floor to thehighest bed or gurney. Some devices can liftindividuals up to 500 pounds or more. There isa large number of different types of lifts avail-able with a variety of features.
Stand-Assist
These lifts are for moving patients and residentsto and from chairs, toilets, beds or into and outof showers. Stand-assist type lifts are appropri-ate for patients or residents who are weight-bearing and have some upper-body strengthand control. The best devices are battery oper-ated.
Compact
These are a smaller version of a total-body orstand-assist lift. They are appropriate for use inthe provision of home care, where space or stor-age is limited, or in moving individuals into andout of cars (e.g., emergency rooms).
RESOURCE INFORMATIONE
29
This section is intended to provide supplemental information on improvement options. In-cluded are descriptions of a variety of assist equipment and devices, design considerations,and work practices which may be effective in reducing or preventing back injuries. The op-tions listed are only a sampling of those available and may or may not work for your partic-ular situation or problem. Consult equipment manufactures for details on specific products.
ASSIST EQUIPMENT AND DEVICESASSIST EQUIPMENT AND DEVICES

Ambulation Lifts
These lifts support a patient or resi-dent during ambulation. The individ-ual pushes the lift along as they walk.A strap in the back prevents themfrom falling backwards.
Bathtub and Shower Lifts
Designed for transfers directly fromthe bed or chair to a bathtub orshower, without removing the patientor resident from the lift. They can beportable or fixed devices which oper-ate by batteries or the power from thefacility. The patient or resident canstay on the lift during the bathing orshowering activity and any related ac-tivities. Other types include bathtubsthat have built-in lift devices to lowerthe patient or resident directly intothe tub.
LATERAL TRANSFERS (SLIDING)
Transfer Boards
A board between two horizontal sur-faces that the patient or residentslides across. They may be unstablewhen transferring to or from surfacesof unequal height. They may be un-comfortable for very large patients.
Draw Sheets orIncontinence Pads
Commonly used to slide patients orresidents between horizontal surfaces,or for repositioning in beds or chairs.To ensure an adequate grip, theprovider should roll up the edges.This will also reduce forceful exer-tions and awkward upper body pos-tures. The sheets or pads should beused in combination with friction-re-ducing devices such as slide boards,slippery sheets, plastic bags, or low-friction mattress covers.
Gurneys with TransferDevices
Height-adjustable gurneys with built-in slide boards or mechanical means(e.g., hand or motorized crank) tolaterally move patients.
Cots
Strong fabric cots with handles toimprove the grip. They can be used
in combination with friction-reducingdevices such as slide boards or slip-pery sheets.
Slide Boards (SmoothMovers or Plastic TransferBoard)
A large plastic board which reducesfriction. Some slide boards havehand-holds. The patient or resident isslid or rolled onto the board and theboard is then pushed or pulled to ac-complish the transfer.In another common practice, theboard goes under the patient or resi-dent who is pulled over the board byuse of a draw sheet or incontinencepad.
Roller Boards or Mats
Boards or mats with vinyl coveringsand rollers. They are placed betweenthe transfer points. The patient orresident is placed on the board or matand rolled to the new position.
Slippery Sheets, Low-Friction Mattress Covers orPlastic Bags
Can be used under draw sheets or in-continence pads to reduce friction onlateral transfers. Slippery sheets orplastic bags can also be used in lieu ofdraw sheets or incontinence pads.
30

Transfer Mats
Two low-friction mats which areplaced under and strapped onto thepatient or resident (i.e., one under thehead, one under the hips). The matsare then pulled to accomplish thetransfer.
Transfer Slings
Slings with cut-outs or rings forhandholds. The slings are tucked se-curely around the patient or residentand help move them between varioussurfaces. When using these slings, re-member they may dig into or slip offthe patient or resident.
AMBULATIONS,REPOSITIONS,MANIPULATIONS
Fixtures and Stands
Devices which hold arms, legs and ex-tremities when providing medical care,assisting with surgical procedures, orperforming related services.
Gait Belts
Simple canvas belts, without handles,which are traditionally used to sup-port patients or residents during am-bulation. They may also be used to situp, reposition, or gradually lower in-dividuals to the floor during a fall.
The belts are fastened securelyaround the patient’s or resident’swaist and the care provider grips thebelt. When attaching, removing orusing gait belts you should avoidbending, twisting or reaching. Pre-cautions to consider when using gaitbelts include that they:
Can slide up causing scrapes, skintears, and rib injuriesAre not suitable for ambulations ofheavy or non-weight-bearing patientsor residentsCan, if set too tight, cause the careproviders’ knuckles to dig into thepatient or resident Have certain limitations for their use(e.g., recent abdominal or backsurgery, abdominal aneurysm, etc.)Should be used so that there is layer ofclothing between the skin and the belt
Transfer Belts with Handles
A wider version of a gait belt withbuckles. They have padded handleson each side that are easier to gripand allow better control in case of afall. The same considerations andprecautions apply as for gait belts (seeabove).
Hand Blocks
Blocks that enable the patient or resi-dent to raise themselves up and repo-sition in a bed.
Lift Chairs
Chairs equipped with a lift that slow-ly raises upward and tilts forward.This helps the patient or residentstand up.
Lift Cushions
A spring action lift cushion whichraises patients or residents up.
Pivot Discs
Discs which resemble a Lazy Susan.They are placed on the floor and usedto rotate the patient or resident 90degrees to a bed or a chair. Whenused properly, they can help providersperform transfers without twisting.
Push-up Bars
A bar on the bedside. It allows pa-tient or residents to reposition them-selves.
Range of Motion Machines
Machines which automatically moveor manipulate arms, legs or extremi-ties.
Trapeze Bar
A bar suspended from an overheadframe. The patient or resident graspsthe bar and assists in repositioning inbed.
ACTIVITIES OF DAILYLIVING
Hand Tools for Showering,Bathing and Cleaning
These include long-handled exten-sion tools on hand-held showerheads, wash or scrub brushes andother items. These tools can reducethe amount of bending, reaching andtwisting required when washing thelegs, feet and trunk of patients or residents.
31
•
•
•
•
•
Transfer belt with handles
Gait belt
32
Shower-Toileting Chairs
These are shower chairs which havewheels and are high enough to fitover the toilet. These save unneces-sary transfer to and from wheelchairs,toilets, portable commodes, or toilet-ing chairs. Use these in lieu of lowtoilet or shower chairs which do nothave wheels. The heavier metal onestend to be more stable. On all shower-toileting chairs, make sure thebrakes hold tightly.
Shower Carts or Gurneys
Gurneys or carts with waterprooftops so that patients or residents canthen be undressed, showered, driedand dressed on the cart or gurney.
Ramp or Bed Scales
Eliminate unnecessary transfers byweighing patients or residents inwheelchairs or in bed. Built-in bedscales will increase the weight of thebed and may prevent it from loweringto appropriate work heights.
Bath Boards
Boards leveled between the showerseat or bathtub. The patient or resi-dent slides or is assisted from a chairor wheelchair into the bathtub orshower. To reduce friction, make surethere is either clothing or other mate-rial between the person’s skin and theboard. These boards are appropriatefor non or partially weight-bearingindividuals with upper body strengthand control.
Pelvic Lift Devices (HipLifters)
Inflatable lifts that are positioned un-der the hips. They inflate like a pillowand lift the hips so a special bed pancan be readily inserted and removed.These devices may eliminate the needfor an additional transfer for toileting.
Height-Adjustable Bathtubs
Bathtubs with lifting and loweringmechanisms. Ambulatory patientsand residents can more easily climbinto a low bathtub. Nonambulatoryindividuals can be lowered in by a lift.The bathtub can be raised to waistheight to eliminate bending andreaching. Raising the bathtub will al-so reduce bending and reaching whencleaning the tub after the bath.
Toilet Seat Risers
Plastic seats on top of the toilet thatdecrease the distance and amount ofeffort required to lower or raise patients or residents.
Work Practice Guidelines for usingthe above-mentioned equipment anddevices are discussed on pages 35-58.

33
EQUIPMENT
BedsAdjustability• Easily adjustable (e.g., rails lower
or raise easily, short cycle time)• Height ranges that allow upright
working postures, use of lifts, andfacilitate patient or resident mobility
• Brakes, controls and handholdspositioned to allow upright workingpostures (i.e., easy to reach withoutbending or twisting)
Size and weight• Able to fit into rooms, down hall-
ways or other spaces• Easy to move (e.g., not excessively
heavy, large or bulky)Brakes which hold Foot boards which attach securely
Carts (e.g., laundry, food,medicine, crash, case, etc.)
Can move easilyNot too high or wide to see overor aroundHandles at approximately waistheight Storage or retrieval of items doesnot require bending too low,reaching too high or far
Shower/Toilet ChairCombinations
Have wheels which roll easily andsmoothlyHigh enough to fit over toilet
Brakes, which lock and hold effec-tively, on at least two wheelsRemovable commode bucket fortoiletingComfortable commode seatSafety beltAdjustable or removable arm andfootrestsHeavy enough to be stable
Room or Hallway Furniture
Light enough to move easilyHave wheels or casters which rolleasily and have good brakesNot too big or bulky (e.g., doesnot limit access for assist equip-ment and devices, staff or otheritems)
Cardiac or Geri Chairs
Easy to adjust, move and steerCoverings not too slippery (e.g.,requiring continued patient or resi-dent repositioning)
Gurneys
Easy to steer (e.g., by fifth wheelor other means)Easy to adjust (e.g., can easily raiseor lower entire gurney or side rails)Controls and handholds allow up-right, neutral working posture(e.g., easy to reach without bend-ing or reaching)Have IV/Med poles permanentlyattachedHave multiple attachment pointsfor IV/Med poles
IV/Med Poles (withwheels)
Base should be wide enough to en-sure stability without hitting thefeet of staff, patients or residentsWheels or casters roll easily
Medical Equipment (X-ray,monitors, microscopes, etc.)
Can be easily moved manually orself-propelled if very heavyNot too high or wide to see overor aroundHandles at waist height and posi-tioned to allow neutral posture
Wheelchairs
Stable (i.e., do not tip backwards)Footpads and armrests are remov-able and easily adjustable
The following information suggests some desirable design characteristics for equipment and facilities. For exact designspecifications or product line availability, consult with equipment suppliers or manufacturers.
DESIGN OF INSTITUTIONALEQUIPMENT AND FACILITIESDESIGN OF INSTITUTIONALEQUIPMENT AND FACILITIES
✖
✖
✖ ✖
✖ ✖
✖
✖
✖
✖
✖
✖
✖✖✖
✖
✖ ✖
✖
✖
✖
✖
✖
✖
✖ ✖
✖
✖
✖
✖
✖
✖ ✖
34
FACILITIES
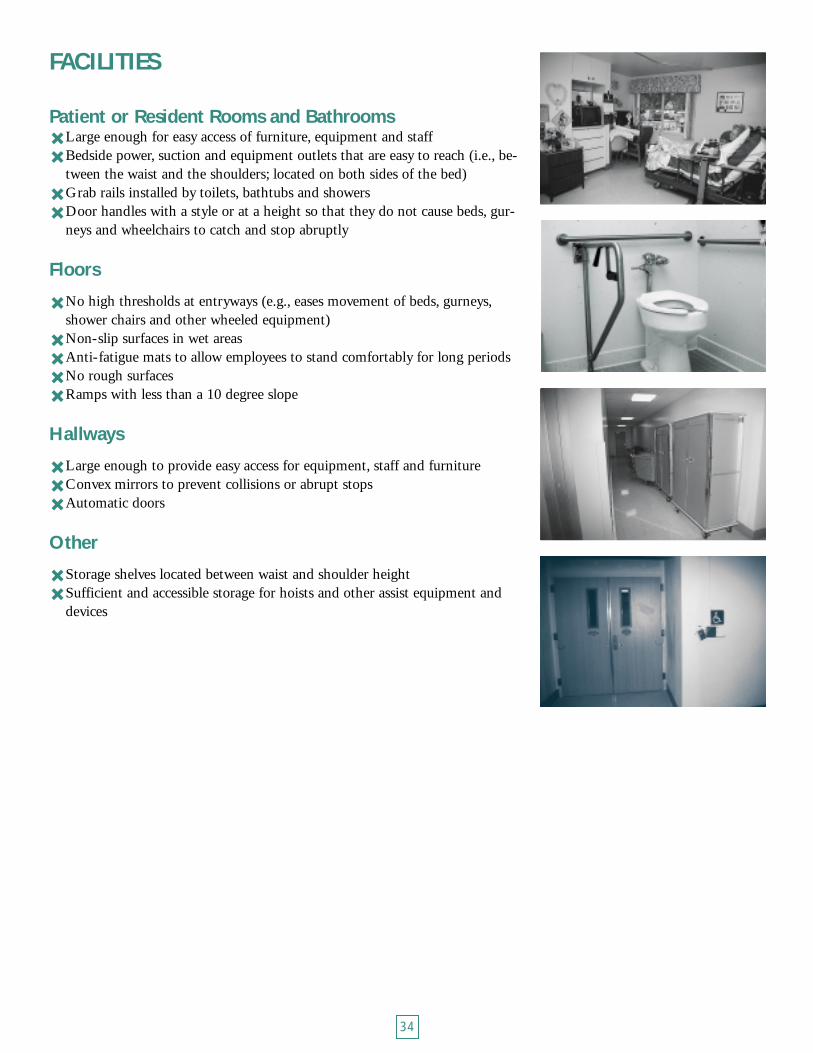
Patient or Resident Rooms and BathroomsLarge enough for easy access of furniture, equipment and staff Bedside power, suction and equipment outlets that are easy to reach (i.e., be-tween the waist and the shoulders; located on both sides of the bed)Grab rails installed by toilets, bathtubs and showersDoor handles with a style or at a height so that they do not cause beds, gur-neys and wheelchairs to catch and stop abruptly
Floors
No high thresholds at entryways (e.g., eases movement of beds, gurneys,shower chairs and other wheeled equipment)Non-slip surfaces in wet areasAnti-fatigue mats to allow employees to stand comfortably for long periodsNo rough surfaces Ramps with less than a 10 degree slope
Hallways
Large enough to provide easy access for equipment, staff and furnitureConvex mirrors to prevent collisions or abrupt stopsAutomatic doors
Other
Storage shelves located between waist and shoulder height Sufficient and accessible storage for hoists and other assist equipment and devices
✖ ✖
✖ ✖
✖
✖ ✖ ✖ ✖
✖ ✖ ✖
✖ ✖

35
In general, eliminate lifting and moving patients or residents manually wheneverpossible by using assist equipment and devices. Get help from other staff. Tell pa-tient or resident what they can do to help you. Give them clear, simple instructionswith adequate time for response.
GUIDELINES FOR MANUAL LIFTING AND LATERAL TRANSFERS
Lifting
Use upright, neutral working pos-tures and proper body mechanics•Bend your legs, not your back. Use your legs to do the work•When lifting or moving people always face them•Do not twist when turning. Pick up your feet and pivot your whole body in the direction of the move
Try to keep the person you are mov-ing, equipment and supplies close tothe body. Keep handholds betweenyour waist and shoulders
Move the person towards you, notaway from you
Use slides and lateral transfers insteadof manual lifting
Use a wide, balanced stance with onefoot slightly ahead of the other
Lower the person slowly by bendingyour legs, not your back. Return toan erect position as soon as possible
Use smooth movements and do notjerk. When lifting with others, coor-dinate lifts by counting down andsynchronizing the lift
PROPER WORK PRACTICESPROPER WORK PRACTICES
Lateral Transfers
Position surfaces (e.g., bed and gur-ney, bed and cardiac chair) as closeas possible to each other. Surfacesshould be at approximately waistheight, with the receiving surfaceslightly lower to take advantage ofgravity
Lower the rails on both surfaces(e.g., beds and gurneys)
Use draw sheets or incontinencepads in combination with friction-reducing devices (e.g., slide boards,slippery sheets, plastic bags, low-friction mattress covers, etc.)
Get a good hand-hold by rolling updraw sheets and incontenence padsor use other assist equipment such asslippery sheets with handles
Kneel on the bed or gurney to avoidextended reaches and bending of theback
Have team members on both sidesof the bed or other surfaces. Countdown and synchronize the lift. Usea smooth, coordinated push-pullmotion. Do not reach across the per-son you are moving
✖
✖
✖
✖
✖
✖
✖
✖
✖
✖
✖
✖
✖
Make copies of all the pages with this symbol.

36
GUIDELINES FOR AMBULATING, REPOSITIONING AND MANIPULATING
Using Gait or Transfer Beltswith Handles
Keep the individual as close as possibleAvoid bending, reaching or twistingyour back when:• attaching or removing belts (e.g., raise
or lower beds, bend at the knees) • lowering the individual down• assisting with ambulationPivot with your feet to turn Use a gentle rocking motion to takeadvantage of momentum
Performing Stand-Pivot TypeTransfers
Used for transferring from bed to chair,etc., or to help an individual get upfrom a sitting position.
Use transfer discs or other assistswhen available. If using a gait ortransfer belt with handles, follow theabove guidelines.Keep feet at least a shoulder widthapart If the patient or resident is on a bed,lower the bed so that they can placetheir feet on the floor to standPlace the receiving surface (e.g.,wheelchairs) on the individual’sstrong side (e.g., for stroke or hemi-paralysis conditions) so they canhelp in the transfer
Get the person closer to the edge ofbed or chair and ask them to leanforward as they stand (if medicallyappropriate)Block the individual’s weak leg withyour legs or knees (this may placeyour leg in an awkward, unstable po-sition; an alternative is to use atransfer belt with handles and strad-dle your legs around the weak leg ofthe patient or resident) Bend your legs, not your backPivot with your feet to turn Use a gentle, rocking motion to takeadvantage of momentum
Lifting or Moving Tasks withthe Patient or Resident inBed
Some common methods include scoot-ing up or repositioning individuals us-ing draw sheets and incontinence padsin combination with a log roll or othertechniques.
Adjust beds, gurneys or other sur-faces to waist height and as close toyou as possible Lower the rails on the bed, gurney,etc., and work on the side where theindividual is closestPlace equipment or items close toyou and at waist heightGet help and use teamwork
✖
✖
✖✖
✖
✖
✖
✖
✖
✖
✖ ✖✖
✖
✖
✖
✖
These work tasks are usually performed in or around beds, gurneys, chairs, toilets,showers and bathtubs. Equipment commonly used includes gait or transfer beltswith handles (for better grips and stability), pivot discs, draw sheets and inconti-nence pads.

37
GUIDELINES FOR TRANSPORTING PATIENTS,RESIDENTS AND EQUIPMENT
It is often necessary to transport people in gurneys, wheelchairs, or beds or handlevarious types of carts, monitors, instrument sets and other medical equipment.
Decrease the load or weight of carts, instrument trays, etc.Store items and equipment between waist and shoulder heightUse sliding motions or lateral transfers instead of lifting Push don’t pull. Keep loads close to your body. Use an upright, neutral postureand push with your whole body, not just your armsMove down the center of corridors to prevent collisionsWatch out for door handles and high thresholds which can cause abrupt stops
GUIDELINES FOR PERFORMING ACTIVITIES OF DAILY LIVING
Cramped showers, bathrooms or other facilities in combination with poor workpractices may cause providers to assume awkward positions or postures or useforceful exertions when performing ADLs.
Use upright, neutral working postures and proper body mechanics. Bend yourlegs, not your backEliminate bending, twisting and long reaches by:
• Using long-handled extension tools (e.g., hand-held shower heads, wash and scrub brushes)
• Wheeling people out of showers or bathrooms and turning them around to wash hard-to-reach places
Use shower-toilet chairs which are high enough to fit over toilets. This elimi-nates additional transfers to and from wheelchairs, toilets, etc.
Use shower carts or gurneys, bath boards, pelvic lift devices, bathtub andshower lifts and other helpful equipment
When providing in-bed medical care or other services, follow the guidelines listed previously.
✖ ✖ ✖ ✖
✖ ✖
✖
✖
✖
✖

38
GUIDELINES FOR TRANSFERRING FROM THE FLOOR
GUIDELINES FOR ASSISTING IN SURGERY
When it is medically appropriate, use a mechanical assist device to lift peoplefrom the floor. If assist devices are not readily available or appropriate, you mayhave to perform a manual lift. When placing slings, blankets, draw sheets or cotsunder the person:
Position at least two providers on each side of the person. Get additional helpfor large patients or residentsBend at your knees, not your back. Do not twistRoll the person onto their side without reaching across themIf using hoists, lower the hoist enough to attach slings without strain
If manually lifting, kneel on one knee, grasp the blanket, draw sheet or cot.Count down and synchronize the lift. Perform a smooth lift with your legs as youstand up. Do not bend your back.
✖
✖ ✖ ✖
Use retractor rings instead of prolonged manual holding of retractorsPosition operating tables or other surfaces at waist heightStand on lifts or stools to reduce reachingFrequently shift position or stretch during long operationsAvoid prolonged or repeated bending of the neck or the waistStand with one foot on a lift and frequently alternate feet to reduce pressure onthe backReduce the number of instrument sets (trays) on a case cartStore instrument sets (trays) in racks between the waist and shoulders Use stands or fixtures to hold extremitiesGet help from coworkers as needed to:
• Position legs or extremities in stirrups• Move heavy carts, microscopes, monitors, alternate operating tables, equipment or
fixtures
✖ ✖ ✖ ✖ ✖ ✖
✖ ✖ ✖✖

39
HOW WE ARE PUTTOGETHER
Back, neck, and shoulder injuries arethe most frequent and costly type ofinjuries among health care workers.Some basic information on the struc-ture and function of the body canhelp provide an understanding onhow these injuries occur and how wecan prevent them.
The Neck
The first seven vertebrae are calledcervical vertebrae and form the neck.Areas of the spine such as the neck,where flexible and inflexible sectionsjoin, are particularly susceptible tostrains, sprains and injuries.
The Shoulder
The shoulder is an example of a balland socket joint where the ball of onebone fits into a hollow crevice of an-other. The shoulder joint allowsmovement and rotation of the armsinward, outward, forward or back-ward. There are several different ten-dons attached to bones in the shoul-der. Bursae reduce friction and cush-ion the tendons as they slide backand forth.
The Back
Spinal Column
The spine is a column of approxi-mately 30 bones called vertebraewhich run from the neck to the tail-bone. These vertebrae are stacked ontop of one another in an S-shapedcolumn and form spinal joints whichmove independently. In the healthy
spine there are three natural curves: aforward curve in the neck, a back-ward curve in the chest area, and an-other forward curve in the lowerback. The back’s three natural curvesare correctly aligned when ears,shoulders and hips are in a straightline. At the end of the spine, the ver-tebrae are fused together to form thesacrum and the tailbone.
The lower back or lumbar area is theworkhorse of the back. It carriesmost of the weight and load of thebody. Aligning and supporting thelumbar curve properly helps preventinjury to vertebrae, discs and otherparts of the spine.
The spine also has various types ofassociated soft tissues like the spinalcord, nerves, discs, ligaments, musclesand blood vessels.
Discs
Discs are soft, shock-absorbing cush-ions located between vertebrae. Theyallow vertebral joints to movesmoothly and absorb shock as youmove. Each disc has a spongy center(i.e., the nucleus pulposus) and toughouter rings (i.e., the annulus fibrosis).
Muscles and Ligaments Affecting the Back
The vertebrae are connected by acomplex system of ligaments which“knit” them together. Strong flexiblemuscles maintain the three naturalspinal curves and help in movement.The most important muscles whichaffect the spine are the stomach, hipflexors, hamstrings, buttock and backmuscles.
Spinal Cord and Nerves
The spinal cord is a delicate cylinderof nerve fibers running the length ofthe spine inside a hollow tunnelformed by the vertebrae. Spinalnerves branch off of the spinal cordand exit through openings betweenvertebrae. These nerves then travel toall parts of the body.
Tendons
Tendons are tough, connective tissuethat attach muscles to bones. Theyhelp move the hands, arms, legs andother body parts by acting as “pulleys.”
Bursae
Bursae are small sacs filled with fluid.They serve as soft slippery cushionsbetween bony projections and mus-cle-tendon units.
TYPES OF INJURIES
Muscle Pain, Sprains andStrains
Pain in the muscles is extremely com-mon. When muscles contract repeti-tively without sufficient rest they canbecome sore and painful. This canhappen without movement (e.g., whenholding objects or fixed body pos-tures) or when we move repetitively.A sprain is damage to ligament fiberscaused by moving or twisting a jointbeyond its normal range. A strainoccurs when a muscle or a muscle-tendon unit is overused.
Bursitis
Bursitis is an irritation and inflamma-tion of bursae in the shoulders andother areas caused by their rubbingon adjacent tendons.
BODY TALKBODY TALK
40
Tendinitis andTenosynovitis
When a tendon is overused, it canbecome inflamed and irritated caus-ing tendinitis. When the tendonsheath is also involved, the conditionis called tenosynovitis.
Neck Tension Syndrome
The joint where the last neck vertebrameets the first mid-back vertebra is amajor site of acute back pain, muscletension and other injuries. Commonsymptoms include: muscle tightness,soreness, restricted movement,headaches, numbness and tingling inthe hands, wrists, arms or the upperback.
Shoulder Tendinitis,Bursitis and Impingement
Shoulder tendinitis is common inpeople who lift continuously or whowork at levels above their shoulder.Several different tendons attach tobones in the shoulder region and pro-duce different types of tendinitis, in-cluding rotator cuff and bicipital ten-dinitis. Shoulder bursitis inhibits thefree movement of the tendons in thecrowded shoulder girdle and limitsthe mobility of the shoulder. Shoul-der impingement occurs when en-larged or inflamed bursae or tendonsget caught between structures in theshoulder.
Degenerated, Bulging orRuptured (Herniated) Discs
Over time, discs wear out or degener-ate from natural aging. The discs dryout and become stiffer and less elas-tic. The outer fibrous rings can crackand the disc narrows. They become
less able to handle loads put on them.If the inner jelly-like center bulgesinto the outer rings ( i.e., the annu-lus), it may compress nearby nerves orblood vessels. If the inner jelly-likecenter breaks through the outer rings,the condition is called a ruptured(herniated) disc. The discs in thelower back are more susceptible todamage than other discs because theybear most of the load in lifting, bend-ing and twisting.
Sciatica
Sciatica occurs when bulging or rup-tured discs constrict the sciatic nerveor nearby blood vessels causing painto be felt (i.e., referred) down thehips, buttocks or legs.
Wear and Tear Arthritis(Degenerative orOsteoarthritis)
Degenerative or “osteo” (bone) arthri-tis simply means the wearing out ofjoints, vertebrae, discs, facets or otherstructures over time. Osteoarthritis isassociated with loads put on the spineover long time periods. As the discsdry out and narrow, they lose theirshock-absorbing ability. The verte-brae become closer together, irritatedand may produce bony outgrowths.
Facet Joint Syndrome
The facets interlock with the verte-brae above and below to form jointsin the spine. The facets can becomemisaligned from bending, lifting andtwisting while working.
“Slipped” Vertebrae(Spondylolisthesis)
Vertebrae in the lower back arepushed forward so they don’t line upwith other vertebrae. This conditiondisrupts the proper natural curves ofthe spine and causes joints, ligamentsand muscles to be overburdened.
Spinal Canal Narrowing(Spinal Stenosis)
Narrowing (i.e., stenosis) in the spinecan occur in the canal that the spinalcord runs through (or in the gap atthe sides of vertebrae where nervesexit).
Vertebrae Fractures
Events like slips, trips, and falls cangenerate severe forces on the spineand cause compression fractures ofthe vertebrae.

The following publications provided usefulbackground information in the development ofthis booklet. Readers may find additional in-formation on back injury prevention in healthcare by reviewing any of the following publica-tions.
ARTICLES
The Lift Team Method For Reducing BackInjury: A Ten Hospital Study, Charney, W.,Journal of the American Association of Occu-pational Health Nursing, June 1997, Vol. 45,No. 6
Identifying Risk Factors for Work RelatedMusculoskeletal Disorders in Nursing Homes,Orr, G. (OSHA Directorate of TechnicalSupport), Nursing Homes Safety and HealthTraining Course, OSHA Office of Trainingand Education, USDL ( July 1996)
Back Breaks, Romano, M., ContemporaryLong Term Care, pp. 45-51 (February 1996)
Reduction of Acute Low Back Injuries By Useof Back Supports, Kraus, J. F., Brown, K.A.,McArtheur, D.L., Peek-ASA, C., Samaniego,L., Kraus, C., and Zhou, L., InternationalJournal of Occupational and EnvironmentalHealth, Vol. 2, pp. 263-273 (Oct.-Dec. 1996)
The Epidemiology of Back Injuries in Nursesat a Large Canadian Tertiary Care Hospital:Implications for Prevention, Yassi, A.,Khokhar, J., Tate, R., Cooper, J. , Sow, C., Val-lentyne, S., Occupational Medicine, Volume45, No. 4, pp. 215-220 (1995)
Workplace Use of Back Belts, Review andRecommendations, Lemen, R.A., NIOSHBack Belts Working Group, U.S. Departmentof Health and Human Services, Public HealthService, Centers for Disease Control and Pre-vention, National Institute for OccupationalSafety and Health ( July 1994)
Report on the American Workforce, Bureauof Labor Statistics, 1994
Lifting Team Design, A Method to ReduceLost-time Back Injury in Nursing, Study inFour Acute Care Hospitals, Charney, W., Pa-per to The American Public Health Associa-tion Conference (October 1993)
Low Back Injuries Among Home HealthAides Compared with Hospital NursingAides, Myers, A., Jensen, R. C., Nestor, D.,Rattiner, I. J., Home Health Care ServicesQuarterly, Vol. 14 (February/March 1993)
Back Stress Isn’t Part of the Job, Owen, B.,Garg, A., American Journal of Nursing, pp.48-51 (February 1993)
Ergonomic Workplace Assessment in aHealth Care Context, McAtamney, L., Cor-lett, E.N., Ergonomics, Vol. 35, No. 9, pp.965-978 (1992)
Reducing Back Stress to Nursing Personnel:An Ergonomic Intervention in a NursingHome, Garg, A., Owen, B., Ergonomics, Vol.35, pp. 1353-1375 (1992)
An Ergonomic Evaluation of Nursing Assis-tants’ Job in a Nursing Home, Owen, B.,Garg, A., Carlson B., Ergonomics, Vol. 35,No. 1, pp. 979-995 (1992)
Four Methods for Identification of MostBack-Stressing Tasks Performed by NursingAssistants in Nursing Homes, Owen, B. D.,Garg, A., Jensen, R.C., International Journalof Industrial Ergonomics, Vol. 9, pp. 213-220( January 1992)
The Lift Team: A Method To Reduce LostTime Injury In Nursing, Charney, W., Journalof the American Association of OccupationalHealth Nursing, May 1991
REFERENCE READINGSF
41
1)
2 )
3)
4)
5)
6)
7)
8)
9)
10)
11)
12)
13)
14)
15)

42
Reducing Risk for Back Pain in Nursing Personnel,Owen, B., Garg, A., Journal of the American Associ-ation of Occupational Health Nursing, Vol. 39, pp.24-33 ( January 1991)
Patients Lifts, in Health Devices, Emergency CareResearch Institute, Vol. 19 No.3 (March 1990)
Nursing Home Aides Experience Increase in SeriousInjuries, Personick, M. E., Monthly Labor Review(February 1990)
Back Injuries Among Nursing Personnel Related toExposure, Jensen, R.C., Applied Occupational andEnvironmental Hygiene, Vol. 5, pp. 38-45 ( January1990)
The Magnitude of Low-Back Problems in Nursing,Owen, B., West. J. Nurs. Res., Vol. 11, pp. 234-242(April 1989)
Back Injury Control Programs for Nursing Staff,Jensen, R., Paper presented at 1989 International In-dustrial Engineering Conference and Societies’ Man-ufacturing and Productivity Symposium Proceedings
Hospital Bed Design and Operation—Effect on Inci-dence of Low Back Injury among Nursing Personnel,Nestor, D., Trends in Ergonomics—Human FactorsV, Hazadeh, F., (editor), Elsivier Science Publishers,B. V. (North-Holland) (1988)
The Use of Assistance While Lifting, Vojtecky, M.A., Harber, P., Sayre, J. W., Billet, E., and Shimozaki,S., Journal of Safety Research, Vol. 18, pp. 49-56(1987)
The Handling of Patients in Geriatric Wards, Takala,E. P., Kukkonen, R., Applied Ergonomics, Vol. 18.1,pp. 17-22 (March 1987)
Back Injury: A Preventable Occupational Hazard,Marchette, L., Marchette, B., Orthopedic Nursing,Vol. 4, No. 6 (November/December 1985)
BACK INJURY PREVENTIONGUIDES
Nursing Homes Safety and Health Training Course,OSHA Office of Training and Education, USDL( July 1996)
Back Injury Prevention Through Ergonomics: A Cur-riculum for Nurses, University of Oregon Labor Edu-cation and Research Center (in cooperation with theOregon Federation of Nurses and Health Profession-als under a grant from the Oregon OccupationalSafety and Health Division) (December 1995)
Back Facts: A Training Workbook To Prevent BackInjuries In Nursing Homes, SEIU Education andSupport Fund (under a grant from OSHA)
A Musculoskeletal Injury Prevention Process, New-foundland Hospital and Nursing Home Association,Department of Employment and Labour Relations,Newfoundland and Labrador Nurses’ Union, Canadi-an Union of Public Employees, and NewfoundlandAssociation of Public Employees (1991)
16)
17)
18)
19)
20)
21)
22)
23)
24)
25)
1)
2)
3)
4)

WE WANT TO HEAR FROM YOU
Topic YES NO COMMENTS
1. Are the descriptions of back injury risk factors accurate?
2. Are the work task evaluation tools useful?
3. Do the potential improvement options seem practical?
4. Will the guide’s information help convince your decisionmakers (e.g., administrators) to try out some improvements?
5. Overall, do you believe that the guide can help reduceback injuries?
ADDITIONAL COMMENTS (PLEASE WRITE IN)
1. Please describe briefly what your organization plans to do or has done as a result of this guide (e.g., designated individuals or a group to plan and decide the strategy on improvement options; looked at injury statistics; added up direct and indirect costs; performed work task evaluation(s); bought liftequipment; trained staff, etc.)
2. What specific comments or suggestions do you have to improve this guide? For example:• What else can be done to further persuade management to implement appropriate solutions?
Please be specific.• Are you aware of any other improvement options?• Are there any other important issues we did not address?
3. Do you have any other comments? (when referring to specific text or sections please indicate page numbers)
4. Are there any back injury success stories that you would like to share with us? If you provide yourname and phone number we can more easily get the full story.
**We value and welcome your comments on the back injury prevention guide. Cal OSHA wants to providethe best service possible to employers and employees in California. Please fax this form to the Educationand Training Unit of the Cal/OSHA Consultation Service at (916) 574-2532 or mail to: 2211 ParkTowne Circle #4, Sacramento, CA 95825. We thank you for your important participation!*


Cal/OSHA Consultation Programs
Northern California2424 Arden Way, Suite 410Sacramento, CA 95825(916) 263-0704
San Francisco Bay Area1515 Clay Street, Suite 1103Oakland, CA 94612(510) 622-2891
Los Angeles10350 Heritage Park Drive, Suite 201Santa Fe Springs, CA 90670(562) 944-9366
San Diego7575 Metropolitan DriveSuite 204San Diego, CA 92123(619) 767-2060
Central Valley1901 North Gateway Blvd., Suite 102Fresno, CA 93272(559) 454-1295
San Bernardino/Orange464 West 4th Street, Suite 339San Bernardino, CA 92401(909) 383-4567
San Fernando Valley6150 Van Nuys Blvd., Suite 307Van Nuys, CA 91401(818) 901-5754
10 ETU April 01
Toll-free number: 1-800-963-9424 • Internet: www.dir.ca.gov
Your call will in no way trigger an inspection byCal/OSHA enforcement.
• Voluntary Protection ProgramSan Francisco, CA 94142(415) 703-5272
• Education UnitSacramento, CA 95825(916) 574-2528
On-site Assistannce Program
Area Offices





























