Embed Size (px)
Citation preview

8th Banff Conference on Allograft Pathology Edmonton, 15-21 July 2005
Proteinuria with
sirolimus therapy.
Christophe Legendre
Hôpital Necker, Université Paris V
Paris, France

Proteinuria with sirolimus therapy
1. Proteinuria and renal transplantation.
2. Proteinuria and sirolimus, the data:
- in patients converted from CsA,
- in de novo patients,
3. The mechanisms of increased proteinuria:
- CNI withdrawal,
- the role of sirolimus itself…

Proteinuria and renal transplantation
Fernandez- Fresnedo G et al, Nephrol Dial Transplant 2004
n = 3365

Fernandez- Fresnedo G et al, Nephrol Dial Transplant 2004

Proteinuria and renal transplantation
Halimi JM et al, Am J Transplant 2005 (in press)
484 patients, mean follow-up = 7.2 years

Proteinuria and renal TR
Halimi JM et al,
Am J Transplant 2005 (in press)
Proteinuria > 0.5 < 1g/d
Proteinuria < 0.5g/d
No proteinuria
Proteinuria and sirolimus, the data:
. Proteinuria was first reported in 2003 after renal allograft recipients were converted from a CNI-based regimen to a SRL-based regimen.
. 32 cases of proteinuria with a nephrotic syndrome in 18 cases out of 50 converted patients.
. Presence of focal segmental glomerular sclerosis in 4 cases.
Morelon E et al, Transplant Proc 2003

Proteinuria and sirolimus:conversion Csa-sirolimus.
Butani L, Transplantation 2004

Dittrich E et al, Transplant Int 2004
Proteinuria and sirolimus:conversion Csa-sirolimus.
. Report of 4 cases of heavy proteinuria, edema and decline of graft function after conversion.
. Withdrawal of SRL and reintroduction of CNI resulted in remission in 4 patients.
Letavernier E et al, Transplantation (In press)
0
500
1000
1500
2000
2500
3000
before(n=68)
M+3(n=56)
M+6(n=46)
M+12(n=41)
M+24(n=20)
pro
tein
uri
a (m
g/2
4h)
0
50
100
150
200
seru
m c
reat
inin
e (µ
mo
l/L
)
proteinuria (mg/24h)
serum creatinine (µmol/L)
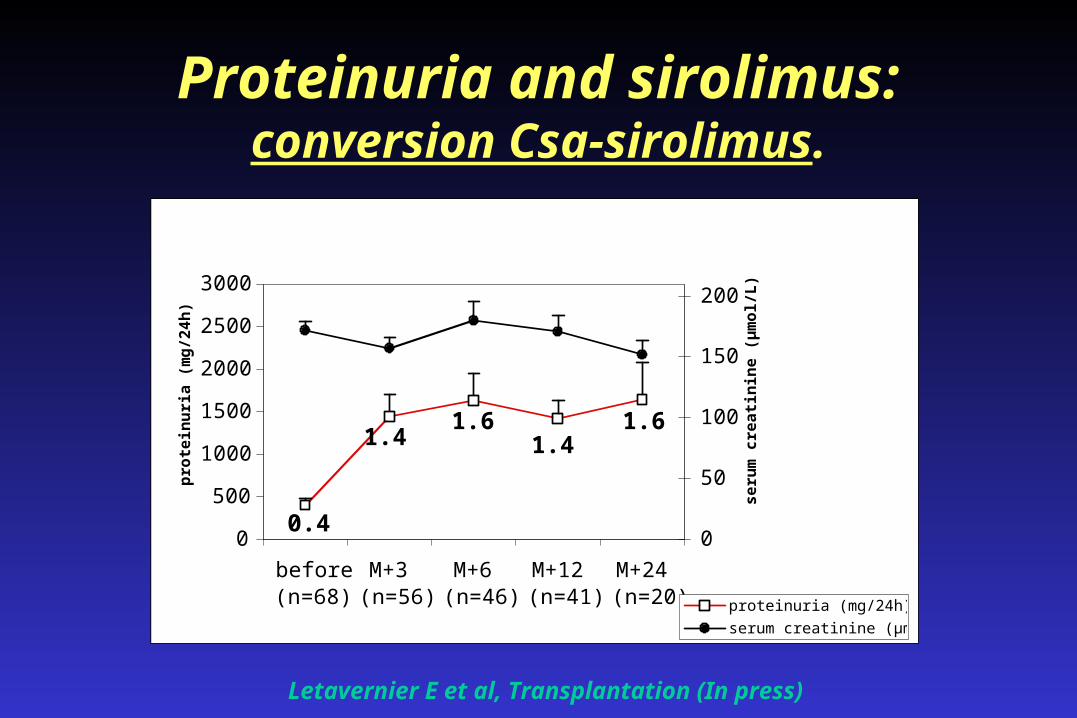
Proteinuria and sirolimus:conversion Csa-sirolimus.
0.4
1.41.6
1.41.6

Letavernier E et al, Transplantation (In press)
05
101520253035404550
% p
rote
inu
ria
ov
er
1 g
/24
h
before M+3 M+6 M+12 M+24
Proteinuria and sirolimus:conversion Csa-sirolimus.

Letavernier E et al, Transplantation (In press)
0
500
1000
1500
2000
2500
3000
3500
CNI sirolimus CNI (2)
pro
tein
uri
a (m
g/2
4h)
0
50
100
150
200
seru
m c
reat
inin
e (µ
mo
l/L)
proteinuriaserum creatinine
Proteinuria and sirolimus:conversion Csa-sirolimus.
0.3
1.9
0.9

Patient Pathology % Alb
LOU… FSGS recurrence 93.3
LAB… FSGS recurrence 76.0
PID… Allograft nephropathy 96.8
HAO… Allograft nephropathy 83.6
RAM… Sirolimus 86.2
TRO… Sirolimus 75.8
Proteinuria and sirolimus:% of albumin (agarose gel with SDS).

Hadaya K et al, ATC 2004
Proteinuria and sirolimus:conversion Csa-sirolimus.
. Monocentric retrospective study (n=23).
. Conversion to SRL after a mean of 667 days.
. 16/23 patients discontinued SRL: 7 because of a nephrotic range proteinuria.
. Occurred 9 days after conversion.
. Association with history of acute rejection:
5/9 versus 1/13, p=0.02.
Dervaux T et al, ICTS 2004
Proteinuria and sirolimus:conversion Csa-sirolimus.
. Observational retrospective analysis in 30 liver and 29 kidney transplant recipients.
. Liver (n=30):
- 2 cases of proteinuria,
. Kidney (n=29):
- 14 patients with increasing proteinuria.

Proteinuria and sirolimus:conversion Csa-sirolimus.
. Increase in proteinuria in 40% kidney and heart transplant recipients (n=41). Lacha J et al, ATC 2005
. Increase in proteinuria in 61% of kidney transplant recipients (> 100% in 30% of cases). More prominent when Pu is low before switch (n=94). Ruiz C et al, ATC 2005
. Few data with Tac: 16% without Pu (Tac-SRL-Ste) versus 35% without Pu (SRL-Ste) (n=87). Morales JM et al,
ATC 2005

Proteinuria and sirolimus:conversion Csa-sirolimus.
. De novo proteinuria in 20% and increase in proteinuria in 28% of kidney transplant recipients (n=86). Birne R et al, ERA-EDTA 2005
. De novo proteinuria (> 0.5g/d) in 37% of kidney transplant recipients (> 2g/d in 12%). Bumbea V et al,
ERA-EDTA 2005

Proteinuria and sirolimus:conversion Csa-sirolimus.
. What are the predictors of a successful conversion from CNI to sirolimus?
- 59 patients studied,
- proteinuria below 0.8g/d is the only independent predictor for positive
outcome in a multivariate analysis.
Diekmann F et al, Am J Transplant 2004

Proteinuria and sirolimus:conversion Csa-sirolimus.
Diekmann F et al, Am J Transplant 2004

Proteinuria and sirolimus:conversion Csa-sirolimus.
The CONVERT Trial(n = 830)

Proteinuria and sirolimus:conversion Csa-sirolimus.

Proteinuria and sirolimus:de novo patients.

Proteinuria and sirolimus:de novo patients.
Flechner S et al, Am J Transplant 2004

Transplantation
Sirolimus (SRL)Load: 15mg x 2 days10mg / dayT0: 10-15ng/ml (HPLC)
Neoral (CsA)6-8 mg/kg/dT0: 150-250ng/ml W1-M375-150 ng/ml M3-M6
ATG: 5 days
+MMF: 2g/day
+STEROIDS
WITHDRAWN AT MONTH 6
Randomizationn=150
Group An=71
Group Bn=74
Lebranchu Y et al, ATC 2005
Proteinuria and sirolimus:de novo patients.

Lebranchu Y et al, ATC 2005
59
81
142
16
28
2 0 00
102030405060708090
<0.5g 0.5-1g 1-2g 2-5g >5g
SRL, n=49CsA, n=54
%
p<0,001
Mean: 0.64 vs 0.18 g/d for SRL vs CsA
Proteinuria at 12 months.

0,64
0,18
0,630,67
0,91
0,64
1,05
0,380,29
0,40,35
1,4
0
0,2
0,4
0,6
0,8
1
1,2
1,4
1,6
M1 M2 M3 M6 M9 M12
SRL groupCsA group
g/2
4 h
ou
rsProteinuria over 12 months.
Lebranchu Y et al, ATC 2005

Skhiri H et al, Transplant Int 2005
Proteinuria and sirolimus:conversion Csa-sirolimus.

Mechanism of proteinuria:CNI withdrawal.
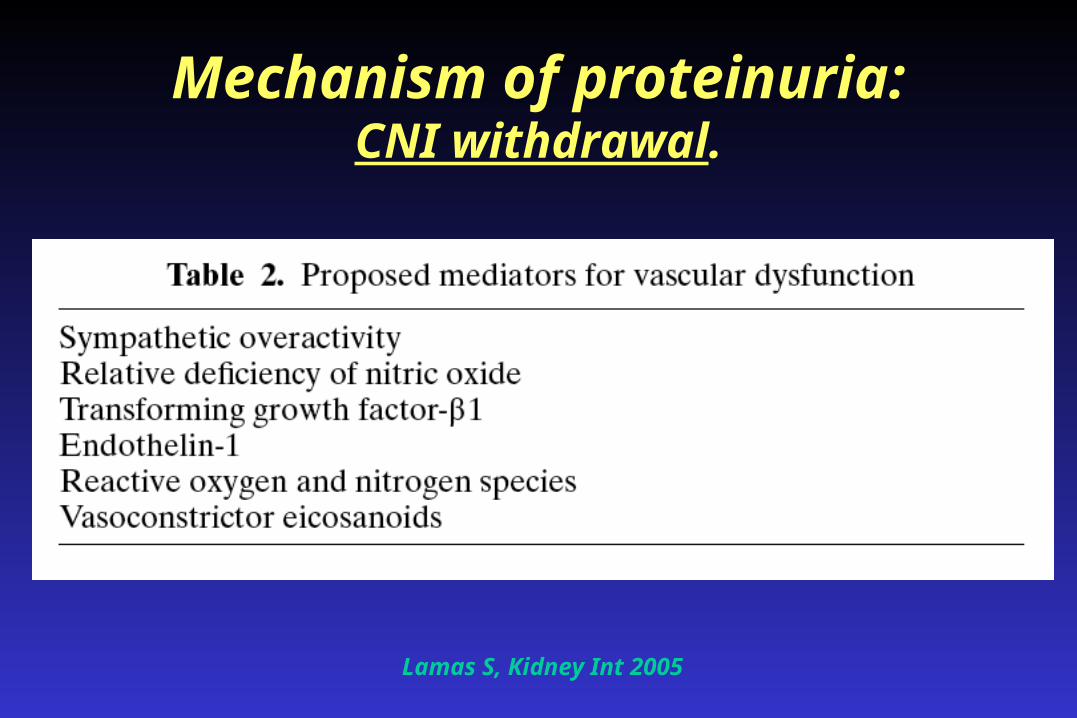
Mechanism of proteinuria:CNI withdrawal.
Lamas S, Kidney Int 2005

. In heart transplant recipients, progressive withdrawal of CsA leads to an increase of proteinuria:
- 162 ± 70µg/min (0.23g/d) at baseline
- 546 ± 300µg/min (0.79g/d) at 48 months.
Myers B et al, Kidney Int 1988
Mechanism of proteinuria:CNI withdrawal.

Mechanism of proteinuria:conversion CNI-MMF.
. Very few data on proteinuria after conversion from CsA to MMF in kidney transplant recipients!

Mechanism of proteinuria:conversion CNI-MMF.
. In unstable patients:
- Weir M et al, Kidney Int 2001 ………… No data
- Dudley C et al, Transplantation 2005 …. No data
- Ducloux D et al, Transplant Int 2002:
- 31 patients with chronic allograft dysfunction,
- Pu = 0.70 ± 0.6 g/d before switch,
- Pu = 1.79 ± 1.1g/d at end of follow-up (p=0.04).

Mechanism of proteinuria:conversion CNI-MMF.
Houdé I et al, Transplantation 2000

Mechanism of proteinuria:conversion CNI-MMF.
. In stable patients:
- Abramowicz D et al, Transplantation 2002 ………… No data
- Pascual M et al, Transplantation 2003 …………….. No data
- Thervet E et al, Clin Transplantation 2000:
- 28 patients on CsA-Aza-ste,
- 40 weeks of follow-up,
- Pu at baseline = 0.1 g/d,
- Pu at end of follow-up = 0.2 g/d.

Mechanism of proteinuria:conversion CNI-MMF.
. In stable patients:
- Smak Gregoor PJ et al, JASN 2002:
- patients on CsA-MMF-Ste,
- at 6 months post-RT, withdrawal of CsA or ste,
- proteinuria > 0.5 g/d:
- at baseline:18% (CsA-), 16% (ste-), 15% (control),
- at end of FU: 18%, 20%, 12% (ns).

Mechanism of proteinuria:the role of sirolimus.
. Acute nephrotoxicity in non-transplant patients with a chronic glomerulopathy. Fervenza PM et al, NDT 2004
. Proinflammatory effects of RAD in an experimental model of mesangial proliferative glomerulonephritis. Daniel C et al, Exp Nephrol 2000
. Rapamycin ameliorates proteinuria-associated tubulo-interstitial inflammation and fibrosis in experimental membranous nephropathy. Bonegio RGB et al, JASN 2005

Mechanism of proteinuria:no specific pathological aspect!

Summary
1. Proteinuria is a prognostic marker in renal transplantation.
2. Proteinuria appears or increases in transplant patients converted from CNI to SRL but we do not know yet precisely:
- in which patients,- what are the prognostic consequences,- the response to (which!) therapy.
3. The exact mechanism is unknown but the hemodynamic effect of CNI withdrawal is likely to be essential.

Thanks for your attention!
8th Banff Conference on Allograft Pathology Edmonton, 15-21 July 2005





























