Embed Size (px)
Citation preview
4 2 0 A AASLD ABSTRACTS HEPATOLOGY October 2001
991
CURRENT HCV THERAPIES DO NOT MEET THE NEEDS OF THE M A - J O R I T Y OF US VETERANS. Ed Bini, New York Harbor VAMC, New York, NY; Norbert Brau, Bronx VAMC, Bronx, NY; Sam Ho, Minneapolis VAMC, Minneapolis, MN; David Johnson, Bay Pines VAMC, Bay Pines, FL; StephenJ Rossi, San Francisco VAMC, San Francisco, CA; LennoxJeffers, Miami VAMC, Miami, FL; Teresa Wright, San Francisco VAMC, San Francisco, CA
Introduction:Interferon based regimens remain the standard of care for treatment of chronic HCV infection. However, many patients are not treatment candidates due to contraindieations related and unrelated to interferon. The HCV-infected US Veteran pop- ulation has been reported to have a low percentage of acceptable treatment candidates. However, specific reasons why therapy is contraindicated in this population has not been examined in a multi-center, prospective fashion. Methods: Standardized information was collected in 5035 US Veterans at 25 VA medical centers from 9/99 to 12/00. All subjects were HCV antibody positive and under evaluation for interferon c¢2b plus ribavirin ther- apy. Treatment candidacy was determined by experienced GI or ID clinicians based on the established medical and psychosocial criteria outlined in the VA HCV Treatment Guide- lines. Information collected included determination of treatment candidacy, reasons for non-candidacy, patient decision regarding treatment, and patient reason for denying treat- ment. Results: Of the 5035 patients evaluated, 1866(37.1%) were candidates while 3169(62.9%) were not candidates for treatment. Table i summarizes the reasons for treat- ment non-eandidacy in 3002 patients where the specific parameters could be assessed. Patients with multiple reasons were included in each separate category. Of the 1866 patients who were treatment candidates, 1056 received treatment with interferon a2b plus rihavirin while 76 were treated with investigational agents. A total of 535 patients declined therapy despite being treatment candidates. The primary reasons were concerns over side-effects (24.7%) and deferring treatment until better therapies were available(24%). Conclusions: A large proportion of US Veterans being evaluated for HCV treatment have absolute cuntraindications to current therapies. In addition, a large percentage of veterans opted to defer treatment based on the high incidence of severe side-effects and the poor outcomes with the treatment currently available. The prevalence of specific medical con- ditions and social histories in this population clearly demonstrate the need for therapies with greater efficacy and fewer treatment limiting side-effects.
Table 1 Extrahepatic Medical Condition 909 (302~0) Treatment Non-reaponde¢ 732 (24,3%) Active Substance Abuse 525 (17,5%) Psychiatric Condition 488 (163%) Thrornbocytopenia (<85K) 281 (9.7%) Decompensated Uver Disease 274 (9.1%) Renal Dysfunction (Cr >1.5) 172 (5.7%) Neutropenia (<t500) 160 (3,3%) HBsAg (+) 93 (3.1%) Other 251 (8.4%)
992
IS ANTI-HCV THERAPY USEFUL FOR PREVENTING LIVER-RELATED DEATH IN PATIENTS WITH HCV CIRRHOSIS ? RESULT OF A RETRO- SPECTIVE COHORT STUDY IN 445 PATIENTS. Vincent Di Martino, Lucas Cavallaro, Marie-H~l~ne Tainturier,Joel Ezenfis, Vlad Ratziu, Yves Benhamou, Thierry Poynsrd, Muhivirc Group, GH Piti4-Salpetri~re, Paris France
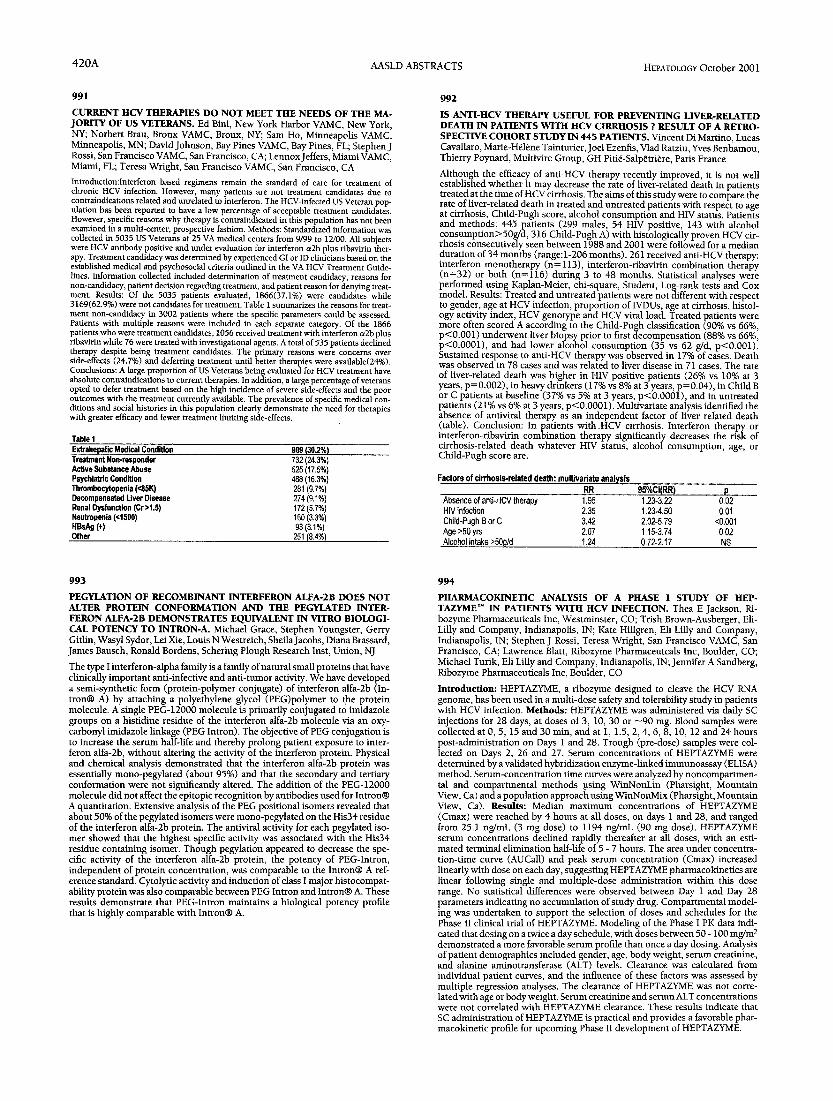
Although the efficacy of anti-HCV therapy recently improved, it is not well established whether it may decrease the rate of fiver-related death in patients treated at the time of HCV cirrhosis. The aims of this study were to compare the rate of liver-related death in treated and untreated patients with respect to age at cirrhosis, Child-Pugh score, alcohol consumption and HIV status. Patients and methods: 445 patients (299 males, 54 HIV positive, 143 with alcohol consumption>50g/d, 316 Child-Pugh A) with histologically proven HCV cir- rhosis consecutively seen between 1988 and 2001 were followed for a median duration of 34 months (range:l-206 months). 261 received anti-HCV therapy: interferon monotherapy (n= 113), interferon-ribavirin combination therapy (n=32) or both (n=116) during 3 to 48 months. Statistical analyses were performed using Kaplan-Meier, chi-square, Student, Log-rank tests and Cox model. Results: Treated and untreated patients were not different with respect to gender, age at HCV infection, proportion of IVDUs, age at cirrhosis, histol- ogy activity index, HCV genotype and HCV viral load. Treated patients were more often scored A according to the Child-Pugh classification (90% vs 66%, p<0.001) underwent liver biopsy prior to first decompensation (88% vs 66% p<0.0001), and had lower alcohol consumption (35 vs 62 g/d, p<0.001)i Sustained response to anti-HCV therapy was observed in 17% of cases. Death was observed in 78 cases and was related to liver disease in 71 cases. The rate of liver-related death was higher in HIV positive patients (26% vs 10% at 3 years, p=0.002), in heavy drinkers (17% vs 8% at 3 years, p=0.04), in Child B or C patients at baseline (37% vs 5% at 3 years, p<0.0001), and in untreated patients (21% vs 6% at 3 years, p<0.0001). Muhivariate analysis identified the absence of antiviral therapy as an independent factor of liver related death (table). Conclnsion: In patients with HCV cirrhosis, Interferon therapy or interferon-ribavirin combination therapy significantly decreases the risk of cirrhosis-related death whatever HIV status, alcohol consumption, age, or Child-Pugh score are.
Factors of cirrhosis.related death: multivariate analysis RR 95%CI(RR) p
Absence of anti-HCV therapy 1.95 1.23-3.22 0,02 HIV infection 2.35 1,23-4.50 0,01 Child-Pugh B or C 3.42 2,02-5,79 <0.001 Age >50 yrs 2.07 1.15-3,74 0,02 Alcohol intake >500/(1 1.24 0,72-2.17 NS
993
PEGYLATION OF RECOMBINANT INTERFERON ALFA-2B DOES NOT ALTER PROTEIN CONFORMATION AND THE PEGYLATED INTER- FERON ALFA-2B DEMONSTRATES EQUIVALENT IN VITRO BIOLOGI- CAL POTENCY TO INTRON-A. Michael Grace, Stephen Youngster, Gerry Gitlin, Wasyl Sydor, Lei Xie, Louis N Westreich, SheilaJacobs, Diana Brassard, James Bausch, Ronald Bordens, Schering Plough Research Inst, Union, NJ
The type I interferon-alpha family is a family of natural small proteins that have clinically important anti-infective and anti-tumor activity. We have developed a semi-synthetic form (protein-polymer conjugate) of interferon alfa-2b fin- tron® A) by attaching a polyethylene glycol (PEG)polymer to the protein molecule. A single PEG-12000 molecule is primarily conjugated to imidazole groups on a histidine residue of the interferon alfa-2b molecule via an oxy- carbonyl imidazole linkage (PEG Intron). The objective of PEG conjugation is to increase the serum half-fife and thereby prolong patient exposure to inter- feron alfa-2b, without altering the activity of the interferon protein. Physical and chemical analysis demonstrated that the interferon alfa-2b protein was essentially mono-pegylated (about 95%) and that the secondary and tertiary conformation were not significantly altered. The addition of the PEG-12000 molecule did not affect the epitopic recognition by antibodies used for Intron@ A quantitation. Extensive analysis of the PEG positional isomers revealed that about 50% of the pegylated isomers were mono-pegylated on the His34 residue of the interferon alfa-2b protein. The antivira] activity for each pegylated iso- mer showed that the highest specific activity was associated with the His34 residue containing isomer. Though pegyfation appeared to decrease the spe- cific activity of the interferon alfa-2b protein, the potency of PEG-Intron, independent of protein concentration, was comparable to the Intron@ A ref- erence standard. Cytolytic activity and induction of class I major histocompat- ability protein was also comparable between PEG Intron and Intron® A. These results demonstrate that PEG-Intron maintains a biological potency profile that is highly comparable with Intron@ A.
994
PHARMACOKINETIC ANALYSIS OF A PHASE I STUDY OF HEP- TAZYME T M IN PATIENTS WITH HCV INFECTION. Thea E Jackson, Ri- bozyme Pharmaceuticals Inc, Westminster, CO; Trish Brown-Ausberger, Eli- Lflly and Company, Indianapolis, IN; Kate Hfllgren, Eli Lilly and Company, Indianapolis, IN; Stephen J Rossi, Teresa Wright, San Francisco VAMC, San Francisco, CA; Lawrence Blatt, Ribozyme Pharmaceutcals Inc, Boulder, CO; Michael Turik, Eli Lilly and Company, Indianapolis, IN; Jennifer A Sandberg, Ribozyme Pharmaceuticals Inc, Boulder, CO
Introduction: HEPTAZYME, a ribozyme designed to cleave the HCV RNA genome, has been used in a multi-dose safety and tolerability study in patients with HCV infection. Methods: HEPTAZYME was administered via daily SC injections for 28 days, at doses of 3, 10, 30 or ~90 rag. Blood samples were collected at 0, 5, 15 and 30 min, and at 1, 1.5, 2, 4, 6, 8, 10, 12 and 24 hours post-administration on Days 1 and 28. Trough (pre-dose) samples were col- lected on Days 2, 26 and 27. Serum concentrations of HEPTAZYME were determined by a validated hybridization enzyme-linked immunoassay (ELISA) method. Serum-concentration time curves were analyzed by noncompartmen- tal and compartmental methods using WinNonLin (Pharsight, Mountain View, Ca) and a population approach using WinNonMix (Pharsight, Mountain View, Ca). Results: Median maximum concentrations of HEPTAZYME (Cmax) were reached by 4 hours at all doses, on days 1 and 28, and ranged from 25.1 ng/mL (3 mg dose) to 1194 ng/mL (90 mg dose). HEPTAZYME serum concentrations declined rapidly thereafter at all doses, with an esti- mated terminal elimination half-life of 5 - 7 hours. The area under concentra- tion-time curve (AUCall) and peak serum concentration (Cmax) increased linearly with dose on each day, suggesting HEPTAZYME pharmacokinetics are linear following single and multiple-dose administration within this dose range. No statistical differences were observed between Day 1 and Day 28 parameters indicating no accumulation of study drug. Compartmental model- ing was undertaken to support the selection of doses and schedules for the Phase II clinical trial of HEPTAZYME. Modeling of the Phase I PK data indi- cated that dosing on a twice a day schedule, with doses between 50 - 100 mg/m 2 demonstrated a more favorable serum profile than once a day dosing. Analysis of patient demographics included gender, age, body weight, serum creatinine, and alanine aminotransferase (ALT) levels. Clearance was calculated from individual patient curves, and the influence of these factors was assessed by multiple regression analyses. The clearance of HEPTAZYME was not corre- lated with age or body weight. Serum creatinine and serum ALT concentrations were not correlated with HEPTAZYME clearance. These results indicate that SC administration of HEPTAZYME is practical and provides a favorable phar- macokinetic profile for upcoming Phase II development of HEPTAZYME.




![Integrating the Healthcare Enterprise€¦ · Document Source Document ConsumerOn Entry [ITI Document Registry Document Repository Provide&Register Document Set – b [ITI-41] →](https://img.dokumen.tips/doc/110x75/5f08a1eb7e708231d422f7c5/integrating-the-healthcare-enterprise-document-source-document-consumeron-entry.jpg)
























