-
Dr. DATTEN BANGUN MSc,SpFKBagian Farmakologi dan
Terapeutik,Fakultas KedokteranUniversitas Sumatera UtaraDRUG
INTERACTIONS
-
CONCEPT :Drug interactions involve changes in the duration or
intensity of a drugs action caused by the presence of another
drug.
-
Drug interaction : desirable undesirable =adverse drug
interaction.
-
Defining a Drug InteractionA measurable modification (in
magnitude or duration) of the action of one drug by prior or
concomitant administration of another substance.Drug-drug (Rx, OTC,
herbal)Drug-food, drug-alcoholDrug-lab, drug-disease,
drug-chemicalWright 1992. Drug Interactions. In: Melmon and
Morrellis Clinical Pharmacology 1992
-
Mechanism of drug interactionPharmacokinetic
interactionsAbsorptionDistributionBiotransformation***ExcretionPharmacodynamic
interactionsReceptor interactionReceptor
sensitivityNeurotransmitter release/Drug transportationElectrolyte
balancePhysiological interactionsPharmaceutical interactions
-
Three Phases of Drug ActionI. PHARMACEUTICAL PHASE
II. PHARMACOKINETIC PHASE
III. PHARMACODYNAMIC PHASE
-
I. PHARMACEUTICAL PHASE
A solid drug (tablet) has to disintegrate before it can be
absorbed The process where a solid (tablet) goes into solution is
known as dissolution ALL drugs must be in solution to cross
biologic membranes
-
II. PHARMACOKINETIC PHASE What the body does to the drug- refers
to the study of how the body processes drugs .Movement of drugs
through the bodyIt includes the 4 basic components of : 1.
Absorption 2.Distribution3. Metabolism (Biotransformation) 4.
Excretion
-
III. PHARMACODYNAMIC PHASEWhat a drug does to the body- refers
to the study of the mechanism of drug action on living tissue.
Drugs may increase, decrease or replace enzymes, hormones or body
metabolic functions. Chemotherapeutic drugs alter an abnormal
parasite or growth on the body such as bacteria, viruses or
neoplastic tissue. examples: antibiotics and antineoplastic
drugs.
-
DRUG DRUG INTERACTION When one drug is administered, a response
occurs, if a second drug is given and response to other drug is
altered , a drug interactions is said to have occurred
This effect may be I.Desired or beneficial (efficacy without in
toxicity) e.g. Multi drug treatment of T.BAmoxicillin + clavulanic
acidL-Dopa + CarbidopaNaloxone to treat Morphine overdose*
-
DRUG DRUG INTERACTION II. Undesired or harmful (toxicity is with
in efficacy) Aspirin and Warfarin Propranolol + Salbutamol
Paracetamol + Alcohol Gentamycin + loop diuretics
*
-
DRUG INTERACTIONS
CLASSIFIED AS: ENHANCED EFFICACYA) USEFUL WITHOUT TOXICITY
TOXICITYB) HARMFUL EFFICACY
-
Drug-Drug interaction may alter drug effect byAdditive effect :
1 + 1 =2Synergistic effect : 1 +1 > 2Potentiation effect : 1 + 0
=2Antagonism : 1-1 = 0
-
Mechanism of drug interactionPharmacokinetic
interactionsAbsorptionDistributionBiotransformationExcretionPharmacodynamic
interactionsReceptor interactionReceptor
sensitivityNeurotransmitter release/Drug transportationElectrolyte
balancePhysiological interactions---- adrenalin in alergic
reactionPharmaceutical interactions
-
Risk Factors for Drug InteractionsHigh Risk PatientsElderly,
young, very sick, multiple diseaseMultiple drug therapyRenal, liver
impairmentHigh Risk DrugsNarrow therapeutic index drugsRecognised
enzyme inhibitors or inducers
-
Intravenous Nutrition CompatibilityContain many ingredientsAmino
acids, dextrose, lipids, electrolytes, vitamins and trace
elementsIssues of compatibility can be significant. Precipitates
can occur.Many patients receive medications simultaneously. Watch
for pH: change in color or clarity
-
Lipid CompatibilityMany institutions mix lipid in same container
with other ingredientsLipid is an oilinwater emulsionElectrolytes
destabilize the emulsionFat droplets aggregateClog blood vessels
form emboli
-
Intravenous CompatibilitypH - acid base interactions
Concentration - Vancomycin and ceftazidime.Crystal formation
Ascorbic AcidPrecipitate formation Ca + PO4
-
PharmacokineticsMovement of drugs in the bodyFour
ProcessesAbsorptionDistributionMetabolismExcretion Drug
concentration at sites of action influenced by several factors,
such as:Route of administrationDoseCharacteristics of drug
molecules (e.g., lipid solubility)
-
II. Pharmacokinetic interactionsInteractions at the A D M E
levelAbsorption(impact on total absorption or
time-profile)Chemical/physico-chemical interaction (viz previous
slide)Drugs affecting GIT motility: Absorption is decreased by
laxatives (purgatives) increased passage through GIT (small
intestine) may affect absorption of drug with slow and/or low
absorptionSlowed absorption antimuscarinics may decrease the
emptying of stomach
-
Pharmacokinetic interactions1) Altered GIT absorption.Altered
pH, Altered bacterial flora, formation of drug chelates or
complexes, drug induced mucosal damage and altered GIT
motility.Altered pH; The non-ionized form of a drug is more lipid
soluble and more readily absorbed from GIT than the ionized form
does. -------Handerson-Hasselbalch Equation
-
Ex1., antiacids Decrease the pHDecrease the tablet dissolution
of Ketoconazole (acidic)Ex2., H2 antagonistspHTherefore, these
drugs must be separated by at least 2hours in the time of
administration of both .
-
b) Altered intestinal bacterial flora ;EX., In 10% 0f patients
receive digoxin..40% or more of the administered dose is
metabolized by the intestinal floraAntibiotics kill a large number
of the normal flora of the intestineIncrease digoxin conc. and
increase its toxicity
-
c) Complexation or chelation;EX1., Tetracycline interacts with
iron preparations orMilk (Ca2+ )Unabsorpable complexEx2., Antacid
(aluminum or magnesium) hydroxide Decrease absorption of
ciprofloxacin by 85% due to chelation
-
d) Drug-induced mucosal damage.Antineoplastic agents e.g.,
cyclophosphamide vincristineprocarbazine Inhibit absorption of
several drugseg., digoxine) Altered motilityMetoclopramide
(antiemitic)Increase absorption of cyclosporine due to the increase
of stomach emptying timeIncrease the toxicityof cyclosporine
-
DistributionDisplacement from tissue proteins: = quinidine may
displace digoxine (in addition to decease of its renal excretion)
-----digoxine intoxication
-
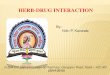
Protein BindingDrug DisplacementPlasmaTissueDrug Aprotein
boundDrug AfreeDrug AfreeDrug BDrugs A and B both bind to the same
plasma protein
-
Displaced protein bindingIt depends on the affinity of the drug
to plasma protein. The most likely bound drugs is capable to
displace others. The free drug is increased by displacement by
another drug with higher affinity. Phenytoin is a highly bound to
plasma protein (90%), Tolbutamide (96%), and warfarin (99%)Drugs
that displace these agents are
AspirinSulfonamidesphenylbutazone
-
II. Pharmacokinetic interactionsMetabolisms
(biotransformation)Impact on cytochrome P450There are different
isoforms of CYP450The most important are CYP450 3A4, 2D6 (the drugs
which are substrates can be found in tables)
-
Altered metabolismThe effect of one drug on the metabolism of
the other is well documented. The liver is the major site of drug
metabolism but other organs can also do e.g., WBC,skin,lung, and
GIT.CYP450 family is the major metabolizing enzyme in phase I
(oxidation process). Therefore, the effect of drugs on the rate of
metabolism of others can involve the following examples.
-
CYP 450 SystemDefinitionsSubstrate: Drug is metabolised by the
enzyme system
Inducer: Drug that will increase the synthesis of CYP450
enzymes
Inhibitor Drug that will decrease the metabolism of a
substrate
-
CYP450 NomenclatureCYP2D6FamilySub-FamilyIndividual Gene
-
Enzyme Induction Leads to production of more enzyme, usually
after 3-4 days of exposure to inducer-----drug metabolismMost CYPs
are inducible but not CYP2D6Time course of interaction depends on
half-life of inducer.
-
EX1., Enzyme inductionA drug may induce the enzyme that is
responsible for the metabolism of another drug or even itself e.g.,
Carbamazepine (antiepileptic drug ) increases its own
Metabolism------ tolerancePhenytoin increases hepatic metabolism of
theophyllineLeading to decrease its level Reduces its actionand
Vice versaN.B enzyme induction involves protein synthesis
.Therefore, it needs time up to 3 weeks to reach a maximal
effect
-
Induction: So whats the big deal?Increased P450 activity can
increase metabolism of substrates and lead to decreased levels and
effects of substratesClinical concern Subtherapeutic levels can
lead to decreased/lack of efficacy, e.g. with ARVs decreased levels
can lead to viral resistance!Ex:Phenobarbitone increase the
metabolism of estrogen-(active substance in oral
contraceptive)-----its blood level decreases---- spotting or even
pregnant
-
Enzyme InductionRifampicin has short half-life and induction
apparent with 24 hours
Phenobarbitone has longer half life so time to complete
induction takes longerCarbamazepineCigarette smoke
-
EX2., Enzyme inhibition;It is the decrease of the rate of
metabolism of a drug by another one.This will lead to the increase
of the concentration of the target drug and leading to the increase
of its toxicity .Inhibition of the enzyme may be due to the
competitionon its binding sites , so the onset of action is short
may be within 24h. N.B; When an enzyme inducer (e.g.carbamazepine)
is administered with an inhibitor (verapamil) The effect of the
inhibitor will be predominant
-
Enzyme InhibitionOften rapid, reversible and relatively short
acting. E.g. erythromycin and cyclosporin NB erythromycin is a
substrate and an inhibitor of CYP 3A4
May be prolonged due to long half- life of drug. E.g. amiodarone
and S-Warfarin NB amiodarone is an inhibitor of CYP2C9 but not a
substrate for this CYP
-
Inhibition: So whats the big deal?Inhibition decreases P450
activity, which can decrease metabolism/clearance of substrates and
lead to increased levels and effects of substratesClinical
concern-- Increased effects can mean increased risk of
toxicities!
-
II. Pharmacokinetic interactionsExcretion : mainly
renalInhibition of tubular secretion Uricosuric drug probenecid
decrease tubular secretion of some drugs, e.g. Penicilins,
-Decreases tubular secretion of methotrexate.Thiazide diuretics
cause relative Na+ depletion and thereby they indirectly increase
Li+ reabsorbtion Decreased renal clearence of Li+ = CNS
toxicity
-
Excretion mainly renalInhibition of tubular reabsorbtion:
Decreased reabsorption of sulfonamides during concomitant
administration of acidic drugs (e.g. Vitamin C) and aspirin in
particular
-
Excretion Interaction
Change in renal blood flow Methotrexate and NSAIDs
NSAIDS can decrease renal blood flow by inhibition of renal
prostaglandins. Reduced clearance of MTX and active (toxic)
metabolite
-
* Passive tubular reabsorption;Excretion and reabsorption of
drugs occur in the tubules By passive diffusion which is regulated
by concentration and lipid solubility.N.B., Ionized drugs are
reabsorbed lower than non-ionized ones Ex1., Sod.bicarb. Increases
lithium clearance and decreases its actionIncreases excretion of
jengkolic acidEx2., Antacids Increases salicylates clearance and
decreases its action
-
III. PHARMACODYNAMIC PHASEWhat a drug does to the body- refers
to the study of the mechanism of drug action on living tissue.
Drugs may increase, decrease or replace enzymes, hormones or body
metabolic functions. Chemotherapeutic drugs alter an abnormal
parasite or growth on the body such as bacteria, viruses or
neoplastic tissue. examples: antibiotics and antineoplastic
drugs.
-
THEORY OF DRUG-RECEPTOR INTERACTIONS
The majority of drugs are believed to exert their effects by
combining with a specialized area on the cell or within the cell
called receptors. Drug + Receptor Drug receptor (binding) =
ResponseA drug receptor may be on the cell surface or within the
cell Receptors come in many shapes that are specific for particular
drugs.The greater the degree of specificity and selectivity for
receptors, the fewer undesirable side effects and the greater drug
efficacy.
-
Pharmacodynamic interactionsReceptor
interactionCompetitiveNon-competitiveSensitivity of receptorNumber
of receptorAffinity of receptorAlter neurotransmitter release /drug
transportationAlter water/electrolyte balance
-
Pharmacodynamic interactionsReceptor
interactionCompetitiveNon-competitiveSensitivity of receptorNumber
of receptorAffinity of receptorAlter neurotransmitter release /drug
transportationAlter water/electrolyte balance
-
Pharmacodynamic Interaction
Drug A alters the effect of Drug B without a change in
concentration of Drug B
-
Pharmacodynamic interactions;It means alteration of the dug
action without change in its serum concentration by pharmacokinetic
factors.EX., Propranolol + verapamil Synergistic or additive
effect
-
Pharmacodynamic InteractionsBenzodiazepines(and antihistamines,
anticonvulsants, barbiturates)AlcoholCNS depressantCNS
depressantAdditive CNS depressionRespiratory depression,
hypotension, coma
-
Pharmacodynamic interactionsOften take a 2 - agonist
(salbutimol) to induce broncodilationOften take blockers
(propanolol) to reduce heart, rate force of contraction
AsthmaticsHypertensionDiminished effect of 2 - agonist
-
Pharmacodynamic
interactionsAntidepressantsSympathomimeticsMonoamine Oxidase
Inhibitors (MAOIs) Inhibit breakdown ofNoradrenaline
DopamineDecongestants (pseudoephidrine)Asthma (salbutimol)Foods
rich in tyramine Beer, Hot Dogs, Wine, BeansMAOIs enhance effects
of these drugs (pseudoephidrine and salbutimol)And enhance the
action of tyramine
-
Pharmacodynamic InteractionsNSAIDsAntihypertensivesFor
inflammation/ headache.Most block Prostaglandin synthesis.
PGE2 and PGI2 cause renal arteriolar dilation1 Antagonist 1
AntagonistAngiotensin Converting Enzyme (ACE)
InhibitorsDiuretics
Loss of ability to dilate renal arterioles (via PGE2 and PG2)
can lead to hypertensive crisis in people taking
antihypertensives
-
PHARMACODYNAMIC INTERACTIONS:
BY ALTERING DRUG RECEPTOR SITES OR BY SECONDARY PHARMACOLOGICAL
MECHANISMS
MAY BE SYNERGISTIC.
-
SYNERGISTIC PHARMACODYNAMIC DRUG INTERACTIONS
DRUG
INTERACTS WITH
RESULTS IN
TUBOCURARINE
AMINOGLYCOSIDES
QUINIDINE
PROCAINE
PROLONGED
PARALYSIS
ORAL
HYPOGLYCAEMICS
SALICYLATES
PROPRANOLOL
EXCESSIVE
HYPOGLYCAEMIA
DIGITALIS
PROPRANOLOL
GUANETHIDINE
VERAPAMIL
BRADYCARDIA
ANTIHYPERTENSIVES
DIURETICS
ENHANCED
HYPOTENSION
-
DRUG INTERACTIONS MAY BE ANTAGONISTIC
PRIMARY DRUG
INTERACTS WITH
RESULTING IN
SALBUTAMOL
-PROPRANOLOL
ANTIAGONISM OF
BRONCHODILATION
ANTIHYPER-
TENSIVES
-NSAIDS
ANTAGONISM OF
HYPOTENSIVE
EFFECT (Na+ -
RETENTION)
- SELECTIVE COX 2
INHIBITORS
NO SIGNIFICANT EFFECTS ON Na
SULPHONAMIDES
-L. ANAETHETICS
-(PABA)
ANTAGONISM OF
ANTIMICROBIAL
EFFECTS
WARFARIN
OESTROGENS
WARFARIN EFFECT
ANTAGONIZED BY
INCREASED
CLOTTING FACTOR
SYNTHESIS
OPIOIDS
NALOXONE
ANTAGONISM
-
Pharmacodynamic Drug Interactions in Palliative
CareAnticholinergic effectsConstipationLowered seizure threshold
Serotonin syndromeCNS depressionQTc prolongation
-
Food-Drug Interactions
-
Definition of TermsDrug-nutrient interaction: the result of the
action between a drug and a nutrient that would not happen with the
nutrient or the drug alone
Food-drug interaction: a broad term that includes drug-nutrient
interactions and the effect of a medication on nutritional
status
-
Food-Drug InteractionFor example, a drug that causes chronic
nausea or mouth pain may result in poor intake and weight loss
-
Therapeutic ImportanceTherapeutically important interactions are
those that:Alter the intended response to the medicationCause drug
toxicityAlter normal nutritional status
-
Patients at Risk for Food-Nutrient InteractionsPatient with
chronic diseaseElderlyFetusInfantPregnant womanMalnourished
patientAllergies or intolerances
-
Food and Drug-Related Risk FactorsSpecial dietsNutritional
supplementsTube feedingHerbal or phytonutrient productsAlcohol
intakePolypharmacyDrugs of abuseNon-nutrients in foodsExcipients in
drugs or food
-
Food/Nutrient Effects on DrugsAbsorptionPresence of food and
nutrients in intestinal tract may affect absorption of
drugAntiosteoporosis drugs Fosamax or Actonel: absorption
negligible if given with food; 60% with coffee or orange juice
-
Food/Nutrient Effects on DrugsAbsorptionAbsorption of iron from
supplements 50% when taken with foodBest absorbed when taken with 8
oz of water on empty stomachFood may GI upsetIf take with food,
avoid bran, eggs, fiber supplements, tea, coffee, dairy products,
calcium supplements
-
Grapefruit Inhibits Metabolism of Many DrugsInactivates
metabolizing intestinal enzyme resulting in enhanced activity and
possible toxicityEffect persists for 72 hours so it is not helpful
to separate the drug and the grapefruitMany hospitals and health
care centers have taken grapefruit products off the menu
entirely
-
Drugs known to interact with grapefruit juiceAnti-hypertensives
(filodipine, nifedipine, nimodipine, nicardipine,
isradipine)Immunosuppressants (cyclosporine,
tacrolimus)Antihistamines (astemizole)Protease inhibitors
(saquinavir)Lipid-Lowering Drugs (atorvastatin, lovastatin,
simvastatin)Anti-anxiety, anti-depressants (buspirone, diazepam,
midazolam, triazolam, zaleplon, carbamazepine, clomipramine,
trazodone
-
Food/Nutrient Effects on Drug Action: CaffeineIncreases adverse
effects of stimulants such as amphetamines, methylphenidate,
theophylline, causing nervousness, tremor, insomniaCounters the
antianxiety effect of tranquilizers
-
Food/Nutrient Effects on Drug Action: AlcoholIn combination with
some drugs will produce additive toxicityWith CNS-suppressant drugs
may produce excessive drowsiness, incoordinationActs as gastric
irritant; in combination with other irritants such as NSAIDs may
increase chance of GI bleed
-
Food/Nutrient Effects on Drug Action: AlcoholShould not be
combined with other hepatotoxic drugs such as acetominophen,
amiodarone, methotrexateCan inhibit gluconeogenesis when consumed
in a fasting state; can prolong hypoglycemic episode caused by
insulin or other diabetes meds
-
Food Drug Effect
Foods Omeprazole in Action (Full stomach) lansoprazole
Itraconazloe in Bioavailability
Cran berry Warfarin in Bleeding Juice
Vitamin C Basic drugs e.g Pseudoephedrine Excretion
Tetracyclines Absorption
-
SummaryEverything interactsFood shares same ADME as do
drugsQuestion all conclusive studiesWhen in doubt, do more
research
-
*****A drug has go from its entry point to the tissues where it
has to react Where it enters the body ..IM, PO etc to where it has
to reactFor the drug to work, it must penetrate the cell
Biotransport refers to the movement of drugs across biologic
membranes Cell structure and molecular size of drugs effect the
movement across the cell membrane.
*All drugs must be in solution to cross biologic membranesThis
is the only way for a drug to reach its site of action
**Pharmacodynamic drugs are capable of changing the normal
physiologic function of the body. examples: slowing the heart rate,
increasing urinary output. Drugs can only alter an existing
function, they cannot create new responses.Drugs exert multiple
effects on the body.Drugs act on a biochemical level to alter the
normal physiologic function of the organism****Pharmacodynamic
drugs are capable of changing the normal physiologic function of
the body. examples: slowing the heart rate, increasing urinary
output. Drugs can only alter an existing function, they cannot
create new responses.Drugs exert multiple effects on the body.Drugs
act on a biochemical level to alter the normal physiologic function
of the organism*Receptors may be a portion of cell membrane, a
transport protein, a structural protein, an enzyme that is
inhibited by drugs, or the nucleic acid of a cell. Receptors come
in many shapes that are specific for particular drugs Receptors
dont exist in the body merely to bind drugs rather, their normal
function is to bind endogenous molecules such as hormones,
neurotransmitters etc.************