Embed Size (px)
Citation preview

'«rrTT-mwwWT'"'"•I"iLi>ay'V''-~-v-'.'iA*.
!•i|;.'.•i
f ••?*•.
I111
.•Jt
ri'ib
ti
CHAPTER
43COMPUTER ASSISTANCE IN
SPINE SURGERY
Jnnics Ziiclicriiiaii Richard Derby
COMPUTER TECIINOLOGYIN SPINE SURGERY
Along wiih our incrcnsing depth ofuiulcrstaiuling of disease processes andthe availability ofnew,and very sensitivediagnostic tests, the task of organizing,reporting, and recording pertinent in-furination for medical nianageinent andresearch on the spine is becoming increasingly complex. This complexity hasbeen .compounded by the increased de-iiiaiuls by the legal, industrial, and socialsystems for documentation. As is evidentfrom the diversity of opinions in thisbook innumerable fundamental questions regarding the nature and treatmentof back disease arc still unanswered. Thisis in part due to the time and difHcuIty-required for meaningful research. Therecent advantages in computer technology and reduced costs of hardware havemade it worthwhile to develop the following spine patient medical record system. This system incorporates reportgenerators, a comprehensive data basewith a function fuc research purposes,and a diagnostic program.
In the traditional oflTicc system, the
physician gathers information from thepatient and thin dictates that information, which is transcribed by a stenographer into a report form (Fig. 43-1).This system is somewhat redundant, in-cfllcicnt, and costly. Sorting through p.n-tients' past charts for research data isfurther time-consuming and often inac-turatc. It entails another step in organizing data once found in the charts. Computerizing thissystem greatly streamlinesthe process, resulting In reduced physician involvement and data recording andprocessing, which arc irrevelant tasks ofdrudgery not necessarily contributing tooptimal patient care. For example, applicationofthesystem foranew patientisasfollows.
Instead of spending 30 to 45 minutes •asking questions of a patient with complex problems for acomplete history, thephysician asks the patient to complete acomprehensive nudtlple-choice questionnaire (Fig. 43-2). This can be sent tonew patients before the olFice visit. Onseeing the patient, the physician may scanthe questionnaire and obtain more information or occasionally clarify ambigu-
ii

i
"'I TI' IVf^-1 f-f 1 V« ITf W] TT 1 TT T " ^ " " •' 1 iiV" yii<' )• I I -v iJI> ri] ••• I • ' '||'" •f",
c/WvHt.i:
492 Si»/iie Siiixciy; M Anfholosy'
30 inln.20 niln.
45 min. 5 nitn.
Jtr
M.O. jSecretary
Time
• SSinln.
: 45 inln.
Total : too mln.
r„.T.,.U.Io,»l sy«cm. Lcg.l.v hucicv, by ..by.icUn. Jic.Mio.. ofbh.o.ialfactors, tiaiisciiiiiioii of dictation, review of transcription.
ilics. The compltlc phy-sical exaniiiialioirform also produces imilliplc-clioicc answers .and is conipictcd by the physicianor assistant. The physician may then dictate a discussion based on the data obtained after reviewing any x-ray films orrecords (Fig. 43-3). This dictation then isadded to the computcr-gcneralcd narr.a-tivc history and physical examination.The latter usually comprises 90% ofthetext in that evaluation. Thus most ofthereport is produced by rapid entry ofniul-tiple-clioice responses by a data entryemployee into the computer (Fig. 43-4).The resultant text approaches the truenarrative report in its flow and in mostcases surpasses it in its completeness (Fig.43-5). . .
Since the history represents patient sdirect written responses, it is the mostvalid historical document. Complete records can be produced with physician timereduced by 80% and stenography expense reduced by 60%. In addition, the
hm
patient data is automatically filed according to the patient's demographic information and is instantaneously retrievable, as is all information relative to thepatient's progress (Fig. 43-6).
Follow-up visits and their reports arcinamigcd similarly. Diagnostic test results such as EMG, CT scan, myclo-gram, MMFl, block injections, disco-grams, and operative reports are likewisereduced to computer-easy forms and entered under each patient's demographicfile. Narrative reports for each can be
' generated instantaneously if desired. Indexing allows one to scan all entrys for aparticular patient and review any particular entry in totality instantaneously. Thisis extremely useful in multidisciplinarycenters where network systems can allowcomplete access to any patient recorp invarious locations. Additionally, patientprogress and its relationship to therapeutic interventions can be graphically dein-oiistr.ated over time.
s

4» Hliich of the following activities change the nature of .your palm
5.
AggravatesPain
RelievesPain
1) Sitting
2) Standing •
. 3) Rising from sitting
, 4) Leaning forward(brushing teeth)
; 5) Walking
6) Lying on your side • .
71 Lying on your back
8) Lying on your stomach
9) Driving
10) Coughing/Sneez'ing.
11) Bending forward ^
Now go back and put an asterisk (*) next to the most aggravatingactivity and the most relieving activity.
Please answer the following questions using the following charti
! 1 • unable to tolerate• • 2 * several minutes only• ' ' 3 " about 10 minutes only
' ' , 4 " about 20 minutes only5 • about 1/2 hour only6 a about 1 hour
7 «• several hours• 8 indefinite period
1) Itow long can you sit?
2) How long can you stand?
3) How long can you walk?
Fig. 43-2 One page ofcomprehensive history questionnaire.
If

1
»r;jM » •• 'i'ln ' 'ii|iiM'."f M•.' ii!"a)'ii|v imi; i« t
I
Coiiipmer Assisfiiiice hi Sphic Surgery 495
SAN FHANCISCO ORTHOPAEDIC SURGEONS MEDICAL CROUP. INC.® 22J5 Hayes StreetSan Francisco, CA 91117
(415) 750-5556
January M, 1987
Dr. Donald Rcnson555 Calirornia SirccISao Francisco, CA 94102
RE: XXKXX xxxxx
Dear Dr. Denson:V6WI »«*••••*» ••
Th.ok r.. ».« «.« .0 " f" ""today. January 14, 1987. \
,„ESEHTCOknM,AmTS:
poUc '̂I-p...... .r -.kn... IP .1,. .1.1.. ppkic, .1.Crigiii knee and the riglil kip-
The pallcni describes her SJij'jlllermost of X' lilw;'modcralc ond can beimpossible a( lis worsi; severe, limillnB gculng out of bed. Ihc pain iscontrolled by niialBCsics at J«* If,cr gelling oiil of bed. il Is severe, limiiingmoderate and can be controlled by """[j" ' ,j|ng normal functions impossible. In theall activities, and by midday, it Is InU ' Impossible, and during the night, it «evening, the i>ain is intense, mak ng j, ,„„de worse by silling, leaning,moderate and can be controlled by »"? J"'®*- n.c |>ain is decreased by lying in awalking, driving. coughliiR ".® " . , ,„pjne position willi knees bent, lying In adecubitus position wllli legs curled up. lying in a supine p«prone position, standing and arising from sitting.
for symptomatic relief.
CoKCPIIy. IP .!'« "PklP. l'P°" '".p". »°p"
•»«four hours reclining on a couch.
• i a..t ii... rnllowina words 10 describe her paintMeCIII Pain Oncstloniialrci "-fcnjer; Troublesome; Radiating; Numb; andThrobbing; Sharp; Cramidng; Durning. Aching, Tend ,
"Cold.
(c) MKS 1986
Pig. 43-5 Typical first page of ccinputcr-gcncratcJ report.

rUE
SC
IlIi
'TlO
Nro
uT
UE
AiH
EN
T
Pati
en
tt
Dat
eo
fV
isit
:/
/
1.
2.
3.
4.
TIt
EA
lllE
NT
S
Rest
Uod
yB
iccb
aiii
csH
ack
scli
oo
i
Cli
lro
(>ra
cto
r
riiy
sicn
lT
liero
py5
.1Ik
jbll
lzatl
oii
5.2
Fle
xio
n5
.3E
xte
nsi
on
5.4
Sta
bil
izati
on
5.5
So
ftti
ssu
em
ob
iliz
ati
on
5.6
Tro
ctl
on
-
5.7
Pelv
ictr
acti
on
5.8
Ura
vlt
ytr
octl
on
.5
.9A
uto
tracti
on
5.1
0Ii
i|ia
tien
tsp
ine
relin
b5
.11
Ou
tpat
ien
tsp
ine
rcli
ab5
.12
Oth
er:
Mo
dali
ties
6.1
Ice
*6
.2
6.3
6.4
6.5
6.6
6.7
Heat
Ult
raso
un
d
bia
tlie
rniy
Sp
ray
&str
etc
hT
EN
Su
nit
Acu
pu
nct
ure
Hed
lest
ion
s7
.1A
iitl
infl
amm
ntor
y:.
7.2
Mu
scle
rela
xan
t:.
7.3
An
tid
epre
ssai
itI.
7.4
Ana
lges
ic|.
7.5
Oth
eri.
0R11
I0P
AE
U1C
SUPP
OR
T
1.
Co
rset
2.D
ody
Jack
et
3.
Lu
mb
arcu
shio
n4
.E
rgon
omlc
ch
air
5.
Ilo
rac
tracti
on
6.S
tati
on
ary
bic
ycl
e7
.H
ome
gym
8.
Nei
gh
bo
rho
od
gym
9.H
ome
exer
cise
prog
ram
10
.Sw
imm
ing
11
.O
ther:
OL
OC
KS
1.
Cau
dal
ep
idu
ral
2.
Lu
mb
arep
idu
ral
3.
Th
ora
cic
ep
idu
ral
4.
Sele
cti
ve
nerv
ero
ot
5.
Facet
blo
ck
.6.
Fac
etrh
lzot
omy
7.C
ost
ov
erte
bra
lJo
int
8.
Ind
well
ing
blo
ck9
.H
oo
kb
lock
10
.S
ym
path
eti
cb
lock
SURG
ERY
(an
dL
evel
)
Instr
um
en
tati
on
1.1
1.2
1.3
1.4
1.5
1.6
Liii
|ue
rod
sI
Harr
ing
ton
:K
no
dt
:
Ste
ffe
:
Ed
ward
s:.
Wir
es
:.
Fu
sio
n
2.1
Fu
sio
n:
2.2
Po
ste
rio
rla
teral
:2
.3A
nte
rio
rIn
terb
od
y:
2.4
Po
ster
ior
Inte
rbo
dy
:
Dla
cect
om
y3
.1M
icro
-;
3.2
Sta
nd
ard
i3
.3F
rag
men
tre
mo
val
:
Deco
mp
ress
ion
4.1
Ccii
tro
iI
4.2
Su
bart
lcu
lar:
4.3
Fo
ram
inal
:
'Ch
ecn
on
ucl
eoly
sis
5.1
Ch
ero
on
ucl
eoly
sis:
Hard
ware
Rem
ov
al
6.1
Rem
ov
al
of
rod
s6
.2R
emov
alo
fp
late
s6
.3R
emov
alof
bone
plug
Su
rgic
al
Rep
air
7.1
Pscu
dart
liro
sls
7.2
Rep
air
du
ral
leak
Pig.
-13-6
Di.<s
|>o5id
oiifo
rmis
com
plete
don
allp.
itleii
tvisi
tsan
dof
ten
obvi
atest
hene
edfo
ran
ypl
iysl
clan
dict
atio
n.
}.'i

1. rsyclmlug leal2. Hill till iscipliiiary3. X-riiy4. EKG
St Done scnn6. Nyelogruin7. Hill
FUimiEll DIAGNOSTIC STUDIfcS
8. Dlscogroin9. CT Bcnn
10. Thcrinogciini11. llrcvlCfll
12. Done tienal Comecry13. Oclier:
CURRENT DIAGNOSIS
Aiunilnfl tear
SegmcnCal liisCoblllCyPitccc iircliropathyDniging disc syndromeSprninMgnfflcnC dysfiinccloiillernliiled niiclens pnlposusllernJnted nucleus pulposus w/radiculopotliySpinal stenosisSpinal utenosls w/rodlculopaCliy •Spondy 1o 1ys Js—ociiCeSpondylol Iscliesls—unstolileSpondylolIscliesls w/radlculopaCliyIntcrnnl disc dlsrupclonKractnre
Infect Ion
NcopliismFuncClonnl
Hetaliol Ic
Sysletnlc arthritisFulled surgery .Foatopcrat Ive—Eorly
. postoperative—hateOsteoporosisOther —
Cervical Thoracic l.umhnr
1.
2.
3.
4.
5.6.
7.8.
9.10.
11.
12.
13.
14.
15.
16.17.
18.
19.
20.
21.
22.
23.24.25.
Overo11 Response1 " Excellent
2 • Good
3 - Fair4 • Poor
5 " Worse
EVALUATION
Physical Exaininatlon1 - Ves
• 2 - Ho
' 3 •• No change
ENVIRONMENTAL FACTORS
Expected RTU dateLimitations
UW: FT PT No. of hrs.
Perm. & stationary:Disability rating :Next appointment t.
No repetitive bending, stooping, or pushingNo lifting more than -poundsNo sitting more than. -hoursNo standing more than ,hoursHo driving more than hoursVes 2 " NoD c D E F G II Totally disabled
> / . . Ready for .voc. rehab.: —
COMPUTER INSTRUCTIONS
1, Is this: II &P Follow-up • 2. Dictation? Yes3, Copies i Insurance——Referring HD——Attorney—4, Special Instructional
No Tnpe no, t..Chart-—
Fig. 43-6, coiuM
Pt..
I t-.
ii
i
a
sii
^198 Sifine Surj^eiy: An Anthology
Aquery program enables any variableor variables to be retrieved and analyzedwith casefor clinical research. Study flagsmay be placed on those entries that are.involved inprospective studies, allowingfor rapid retrieval and organization. Astatistical program that rnns all commonly used statistical tests is used to assess the population distribution significance levels. '
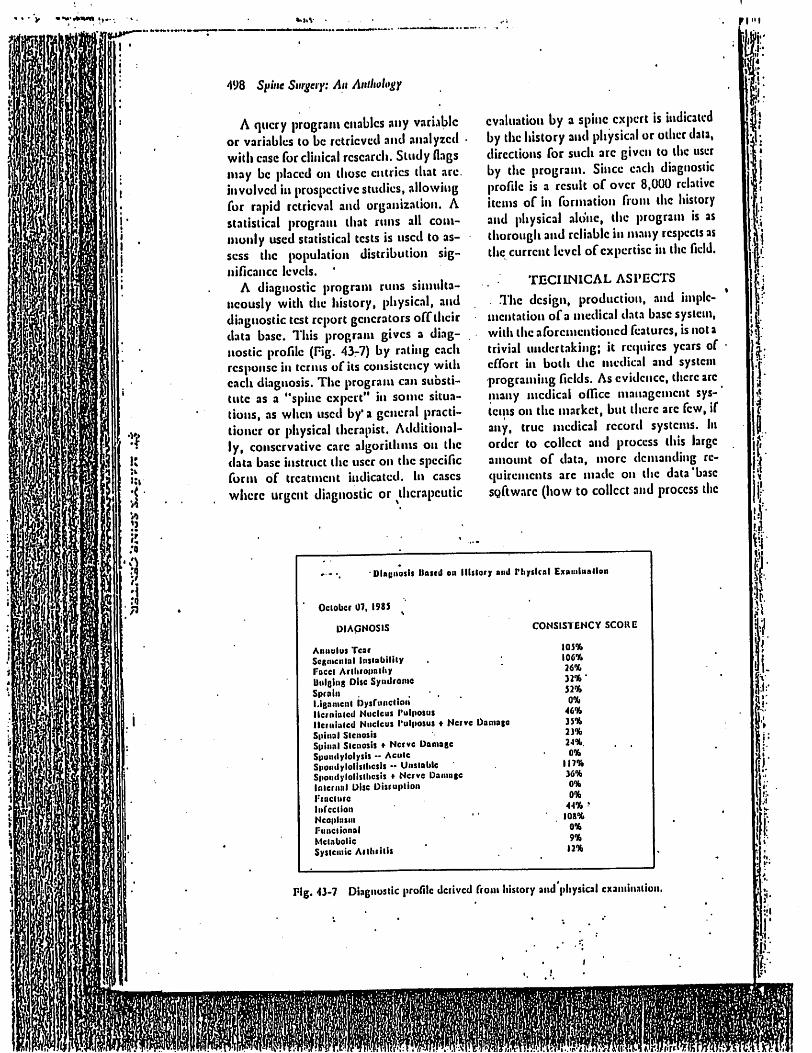
A diagnostic program runs simultaneously with the history, physical, anddiagnostic test report generators offtheirdata base. This program gives a diagnostic profile (Pig. 43r7) by rating eachresponse in terms of its consistency witheach diagnosis. The program can suosti-tute as a "spine expert" in some situations, as when used by'a general practitioner or physical therapist. Additionally, conservative care algorithms on thedata base instruct the user on the specificform of treatment indicated. In caseswhere urgent diagnostic or therapeutic
evaluation by a spine expert is indicatedby the history and physical or other data,directions for such are given to the userby the program. Since each diagnosticprofile is a result of over 8,000 relativeitems of in formation from the historyand physical alone, the program is asthorough and reliable in m.any respects asthe current level ofexpertise in the field.
TECHNICAL ASPECTS
. The design, production, and implementation of a medical data b.iscsystem,with the aforementioned features, is not atrivial undertaking; it requires years ofeffort in both the medieal and systemprograming fields. As evidence, there aremany medical olfice management systems on the market, bnt there arc few, ifany, true medical record systems. Inorder to collect and process this largeamount of data, more demanding requirements arc made on the data basesgftwarc (how to collect and process the
'DUgiiosIt liaitd ON nitlory aii«l riiysical E.xanilnollon
Oclobcr 07, I98S ^
DIAQNOSIS
Aniiului Tear
Scftiiicnial liisiabililyFocci ArlliiotinlltyUuleing DiscSyiidronieSprniiil.ignmcnl l)ysritncllonllcrninlcd Nucleus rulposusllciiiinlcd Nucleus I'uiposus « Nerve DamageSpinal SlenosisSpinal Slenosis ♦ Nerve DamageSpundylolysis -- AculcSpondylolislliesis - UnslnbleSpondyiolislliesis + Nerve DaiiingeInlernal Disc DisruplionFracture
InreclionNeoplasmFiineiionalMetabolicSystemic Arthritis
CONSISTENCY SCORE
105%
106%26%
32%"52%0%
46%
35%25%
2-I*. . .0%
117%36%
0%
0%41% •
108%
0%
9%12%
Pig. 43-7 Diagnostic profile derived frotii lilstory and piiysicai cxantlnation
ri "t
te
•I
•f
II
".c
.c
he
date), (he loading of the data base (what10collect), and the hartlware with whichto collect ami store this iiirorinatioii. Inaddition, both hardware and softwarecoinpatability nuist exist with currentaccelerating technology so that morecomplex use and interfaces can be easilyaccomplished." 'All data basesystems collect and storeinformation on secondary devices suchashard- and soft-sectored disks and tapebackups. More than just a filing system,however, the system has a central program code (driver or core), which interacts with modules ofspecially formattedinformation which the driver uses (in thesamewaya computer languageinterpretssourceor pseudocompiled code) to do itsvarious tasks. 7*hesc modules arc defined
by the system's data definition, screen,'report, and (|uery languages.
Traditionally, data base systems havebeen cither relational, hierarchical, ornetwork in design. Most data bases arccurrently used for business applicationsand use a relational typeof iipdel with a.very limited'data definition language.These are unsuitable for the collection of
a full medical-records system, Medicalinformation ishighlystructured and possesses attributes ofall three designs. Theimplementation ofa system without thisstructure (the DUasc approach) can and isbeing done, but it will fall far short ofphysician expectations.
Before any ofthe data can be collected,it must be described to the data base via
the data definition language. The powerof thismodule,and in particular itsabilityto structure the data, sets the stage for allthe requirements to follow. Medical data .have a hierarchical-network structure
with multiple levels of repeating groups,thus the data definition must likewise
(iicilitate this organization. Purther, in.addition to the usual data element attributes, that is, character, number, date,there must be strong support for kcyed-
•••I '''SK*''" '•'V'"' •'.••»
Ci)iii]uiier Assisltmce in Spine Surgery 499
type data. The amount of informationand the time required to collect it absolutely require that most data collected onany individual patient are only a pointeror key to information described in thedata definition file.
Im.agine, for example, the problem ofhow to describe to the data base the loca
tion and characterofa patient's pain pattern. As seen in Pig. 4378, the logicalstructure isa repeating group ofhierarchical data elements that includes at the
highest level the body location. Relatedto body location is body symmetry, andrelated to body symmetry is a repeatinggroup of a pain type associated with thatrepeat of body location. These data ele
ments, in turn, point to their respectivekeyed answers, which, again can have ahierardiical format with pointers (network structure). All that is stored in thepatient's data file .arc. the key locations ofthe answers.
In addition to structuring the datawithin the patient record, the data definition module, controlled by the centralprogram core, must incorporate a secondary file storage scheme that allowspatients to own many repeating groupsof records (most likely in different files)based on several indexes. The most com
monly used and reliable is the "BalancedTree Indexing method" using either a Index Sequential Access Method (ISAM) orVariable Sequential Access Method(VSAM). This relational method ties allrecords together via cominun data elements present in each record (the patientname).
The screen design language with-which the screens are created and with
which the data arc primarily collectedmust be fast. With the volume ofdata that
must be collected it is too ntlich to expectthedataentry person to accept a mediocreperformance. Key choices must be displayed instantaneously. Windowing,color, and all the amenities of the ncy/
m

f: I ai
m
54^.
500 Spine Snrscry: An Ainlioio^y
IG. Use the body diagrams below to Indicate the location of any ofthe aenaationa listed. Mark the areas on the drawings with thesymbol that best describes the sensation that you feel.
Z - = = NumbnessO O o o pins and needles .X X X X Uurning pain/ / / / / Stabbing pain
' aAAAA Aching pain
FRONT BACK
PAIN DRAWIUG - Section HeaderBODV REGION - Keyed answer repeats' 15 times ....
SYHMCTRY - One keyed answer for each ••Body Region selectionSENSATION - Three keyed answers for each ••Symmetry" selection
Fig. 43-8 A, Scclorcd pain diagram. D, Ucpcaling iiiciarcliic dala elements.
PI
i••
ii
gciu
be s
ntis'
aiul
A

gciicraiion ofconiputcr tccluiology mustbe stniulard. If any of these features arcmissing, the data base isalready outdaicdand probably of marginal quality.
Ailata base is only as good as the quality and quantity of reports it is able toproduce. In .order to produce narrativereports there must be a very extensiveand specially designed report languagethat allows the gathering, testing, trahs-forinntion, checking, and formating ofkeyed information into anarrative reportthat approaches the quality of the physician-dictated report. In addition to usualprograming constructs such as multiplelevels of if-ihen-eisc statements, printercommands, and page formating, thereshould bespecial constructs to haitdle repealing groups, virtual access and testingofanydataelements in thedata b.isc, iindspecializedtests to deal with work substitution, to mention only a few.
finally, the query module must allowon-screen keyed access to any portion ofthe data definition hierarchy networkstructure with the ability to define multiple "and/or" conditions for gatheringand display of patient information. Themodule should format outputs that canbe used with graphic software.
Just as saws, hammers, ami {umber donot equal a house, the data-base softwaretoolsand computers do not equal a medical records system. However, given theproper tools, theJob can begin. TheJobentails deciding what to collect, organizing and structuring the data (data domain), and the building (loading) of thedata base itself.
Domain is an important key word.The domain must be limited and wellilefined. Trying to collect all possible occurrences andsituationsofa patientmedical chart is best avoided. I'his is not tosay that a near complete record is notdesired or cannot be achieved. A standard, however, must bein the particularmedical domain (for example, back care)
Ctinipiiler Assisltuice in Spine Snr^ciy 501
such that the information to be collected'and the keys to be stored arc agreed on
, and accepted by the m.aJority of physicians inthe ficjd. Given the disagreementamong most physician experts, this istlif-ficidt at best. The more practical approach would be a center devoted to thedomain that would set a dc facto standard, which could later be changed andImproved as the input of other users ofthe system are accumulated.
The smallest obstacle to overcome isthe hardware requirement. Thenew generation of microcomputer technologyh.as far outpaced llie available software.Stor.agc requirements will be large. Anactivepatientwith multiple visits andextensive testing and treatment records willrequire approximately 20 to 30 thousandb^ytes ofsecondary storage, withanaverage patient requirement of 15 to 20 thousand bytes. T'his translates toa ISO-megabyte disk for a practice of 10,000. Thisstoragecapacity is already available for avery reasonable price, and costs are rapidlydecreasing while storage capacities areincreasing. Laser technology, whichstores gigabytes of information, will beavailable in the near future.
Although it is a common buzzword,compatibility in both hardware and soft- "ware is of vital importance. It does nottake much computer knowledge to seethe direction development is t.nking:
1. Ihmiwnre coinpatihitily, 1UM isusingthe Intel's lAPX family of microprocessors.
2. Soflwnre conipnlibililY. C or Pascallanguages are by Hir thefavorite andmost common language currentlyused for system development.
3. OpcitUinj^ jyr/t'»i.'Thc MSDOS byMicrosoft or possibly a UNIX environment is available (UNIX,however, is not very user friendly).
We arecurrently using adevelopmental system by Medical Knowledge Systems of San Prancisco, California. The
Pit

!"
502 Spine Surgery: An Anthology
data-base system embodies most ofthercqiilremeiiis oiitliiicci above. I'lic loaii-ing lias been acontinuous and evolvingprocess; at the time ofthis writing, we arccollecting a full history and pliysicalexamination, follow-up visits, and miiiorproccdur.iI data. Over 50% ofour physician dictation time is done by the system.Our hardware consists of an IDM ATwith a 52-mcgabytc hard disk and 3.5-nnllion byte memory, .in enhanced colordisplay monitor, and an IIP laser jetpnntcr.
In conclusion, 1believe that the computer will phy an important role in theorganization of spine surgery programsby allowing spine surgery research toanswer the many unsolved problems amicontroversies presented throughout thisbook. The gradual acceptance ofastandardized method of evaluation andtreatment along with the general acceptance ofcomputer-aided dictations m.'jyencourage more software companies todevelop such systems.
n: