Embed Size (px)
Citation preview

1
Magnet Recognition ProgramClinical Excellence in Action
Magnet 102

Overview
• Explain importance of a strong, supportive Professional Practice Model (PPM)
• State role of Magnet Recognition Program as “evaluation” of PPM
• Describe the five Magnet Model components
• Share examples of evidence to illustrate Magnet Model components
• Outline components of Magnet Site Visit

Description of Magnet ®
• Promotes quality in a milieu that supports professional practice
• Identifies excellence in the delivery of nursing services to patients and families
• Provides a mechanism for the dissemination of “best practices” in nursing services
• Reflects the presence of both organizational, as well as nursing, excellence
• Demonstrates criteria-based evidence of a professional practice environment
© American Nurses Credentialing Center

Magnet Recognition
• Magnet Recognition is the highest recognition the American Nurses Credentialing Center grants to healthcare organizations for excellence in nursing practice.
• It is a hospital award.

TheJourney
MagnMagnetet
Qu
alit
y of
Lea
der
ship
Org
aniz
atio
nal
Str
uct
ure
Man
agem
ent
Sty
le
Per
son
nel
Pol
icie
s &
Pro
ced
ure
s
Pro
fess
ion
al M
odel
s of
Car
e Q
ual
ity
of C
are
Qu
alit
y Im
pro
vem
ent
Con
sult
atio
n &
Res
ourc
es
Au
ton
omy
Com
mu
nit
y &
th
e H
osp
ital
Nu
rses
as
Tea
cher
s
Imag
e of
Nu
rsin
g
Inte
rdis
cip
lin
ary
Rel
atio
nsh
ips
Pro
fess
ion
al D
evel
opm
ent
Grounded in Research

Magnet Designated Facility Information Update for January 2013
• The Commission on Magnet Recognition Program currently recognizes 395 healthcare organizations, as well as three in Australia, one in Singapore and one in Lebanon for their excellence in nursing service.
• Massachusetts General Hospital received Magnet designation in 2003 by the ANCC, the first in Massachusetts; Redesignated in 2008.

Benefits of Magnet Designation
For patients…• Multiple studies have shown that patient outcomes are more
favorable in Magnet hospitals. They experience fewer complications, lower mortality rates & higher patient satisfaction scores.
For nurses…• Professional nurses consider Magnet designation as the Gold
Standard when looking for a practice environment where autonomy, control over practice & professional development are emphasized.
For the hospital…• Magnet signifies high quality care to consumers. Many Magnet
hospitals advertise through media, newspaper announcements, billboards, radio & TV commercials. The improved attraction & retention of nurses results in significant cost savings. Of note, 8 of the top ten hospitals ranked by US News & World Report are Magnet Hospitals.

A New Model for
ANCC’s Magnet Recognition Program ®
EmpiricalOutcomes
StructuralEmpowerment
TransformationalLeadership
ExemplaryProfessional
Practice
New KnowledgeInnovations & Improvement
© American Nurses Credentialing Center

© American Nurses Credentialing Center
Theoretical Underpinning
Donabedian, 1966; 1990
Transformational Leadership
• Organizations can no longer just try to solve problems, fix broken systems, and empower staff – they must actually transform the organization to meet the future.
• This requires vision, influence, clinical knowledge, and strong expertise relating to professional nursing practice.
“It is relatively easy to lead people where they want to go; the transformational leader must lead people where they need to meet the demands of the future.” - ANCC

Transformational Leadership: In the Evidence...
• Alignment of Partners, MGH, Patient Care Services and Nursing’s strategic and quality plans
• How nurses at every level advocate for resources to support goals, e.g., new units (Bigelow 7 Short Stay, Blake 12 ICU); additional staff (Lunder 9 Oncology, MGH North Shore Surgical Center); and equipment (Dolphin mats to prevent pressure ulcers or Biopatch dressing to prevent central line infections)
• Patient Care Services’ Strategic Plan: key focus on patient experience, efficiency and effectiveness of care and ensuring staff have a strong voice in care delivery

Transformational Leadership: In the Evidence...
• Example of how Chief Nurse leads organizational-wide change, e.g., design and implementation of Innovation Unit
• How nurses lead during planned and unplanned change
•Planned: Innovation Units, Lunder Building
•Unplanned: Pediatric ICU evacuation
• How leaders value, encourage, recognize/reward and implement innovation: clinical recognition program, awards, Innovation Units
Transformational Leadership: In the Evidence...
• How nurse leaders use input from direct care nurses to improve the work environment and patient care Examples include: Staff Perceptions of the Professional Practice Environment Survey, PLEN Survey (educational learning needs assessment), Collaborative Governance Committees and Ambulatory Practice Committee
•Additional examples in the evidence included:
•Newborn Family Quiet Time
•Family presence during resuscitation in CICU
•lntracranial Neuroendovascular care redesign

Structural Empowerment• Solid structures and processes developed by leadership provide an environment where strong professional practice flourishes.
• It is an organization where the mission, vision and values come to life to achieve the outcomes important for the organization.
• Strong relationships and partnerships are developed with all kinds of community organizations to improve patient outcomes.
• This is accomplished through the organization’s strategic plan, structure, systems, policies and programs.
Structural Empowerment:In the Evidence…
• Structure and processes that support nurse involvement in organizational decision-making, e.g., Collaborative Governance, Innovation Unit Attending Nurse role, interdisciplinary post-op care processes team, Lunder Building planning teams
•Structure and processes that support nurse involvement in professional organizations and pursuit of formal education, continuing education and certification, e.g., tuition reimbursement, scholarships, flexible scheduling, paid time off, certification exam reimbursement, on-site certification exam preparation programs, Norman Knight Nursing Center, HealthStream on-line learning programs and simulation programs

Structural Empowerment:In the Evidence…
• Affiliations with schools of nursing, consortiums or community outreach programs, e.g., Institute for Patient Care, Dedicated Education Unit, Clinical Leadership Collaborative for Diversity in Nursing, ED and ICU Consortiums, MGH Center for Community Health, MGH/James P. Timilty Middle School Partnership, Bicentennial Scholars, International Twinning Programs (Huashan Hospital in Shanghai, King Edward VII Memorial Hospital in Bermuda)
•Community partnership to address healthcare needs, e.g., MGH Center for Community Health Improvement, Student Health Center at Chelsea High School, Boys and Girls & Boys Club of Boston, Charlestown Substance Abuse Coalition, Revere CARES
Structural Empowerment:In the Evidence…
• Recognition of Nursing
•Publications (Nursing at 200), featured in MGH publications (Hotline, Caring, MGH Magazine)
•Nurse Recognition Week
•Leadership positions in professional organizations (MARN, New England Regional Black Nurses Association)
•Grant funding (Ethics Residency and AgeWISE)
•Hosted national conference regarding professional practice
Exemplary Professional Practice
• This component entails a comprehensive understanding of the role of nursing; the application of that role with patients, families, communities and the interdisciplinary team; and the application of new knowledge and evidence.
• The goal is more than the establishment of strong professional practice; it is what that professional practice can achieve.
• Nurses are accountable for safe, ethical, evidence- based care.

Professional Practice Model
• Provides a comprehensive view of the components of professional practice and the contributions of all disciplines engaged in patient care. The model reflects an organizational commitment to teamwork in an effort to facilitate optimal patient care.
MGH Patient Care Services
• Creates a practice setting that best supports professional nursing practice and allows nurses to practice to their full potential.
American Association of Colleges of Nursing, 2010

Massachusetts General HospitalProfessional Practice Model
© MGH Patient Care Services 1996, 2006, 2012
Massachusetts General HospitalPatient Care Delivery Model
© MGH Patient Care Services 1996, 2006, 2012
Interdisciplinary, patient- and
family-focused care
A philosophy of relationship-based care guides our practice, emphasizing basic tenets of the caregiver’s relationship with:
• Self (self-awareness)• Team/Colleagues• Patient and Family
• Environment of Care

Exemplary Professional PracticeIn the Evidence…
• Evaluation of Professional Practice Environment
•Internal: Staff Perceptions Survey
•External: Magnet Recognition
•Promotion of patient and family involvement in plan of care
•Engagement of internal and external consultants to improve care in practice setting, e.g., Visiting Scholars, Clinical Nurse Specialists
•How staff participate in scheduling and staffing processes
•How nursing plays leadership role in interdisciplinary collaboration

Exemplary Professional Practice In the Evidence…
• Interdisciplinary collaboration across multiple settings to ensure the continuum of care, e.g, case management, access nurse coordinators, clinical nursing supervisors, interdisciplinary rounds
• Annual performance appraisals include: self-evaluation, peer evaluation, manager evaluation and goal-setting
•Use of ANA Code of Ethics for Nurses to address complex ethical issues
•How nurses use resources to meet unique and individual needs of patients and families, e.g., consults, nurse orders, Blum Patient and Family Learning Center

Exemplary Professional Practice In the Evidence…
• Organizational structures and processes that are in place to identify and manage problems related to incompetent, unsafe or unprofessional conduct, e.g., Compliance Hotline, safety reporting system, MGH Workplace Violence initiative, MGH Credo and Boundary Statement
•Organization's workplace advocacy initiatives for caregiver stress, diversity, staff rights and confidentiality, e.g., Benson-Henry Institute for Mind Body Medicine, Employee Assistance Program, Office of Patient Advocacy, Policies on Staff Rights, Privacy Office, Diversity Steering Committee
•Structures and Processes to promote staff safety, e.g, Be Well, Work Well Program, Occupational Health, Quality Initiatives, Infection Control

New Knowledge, Innovation & Improvements
• This is the nursing research component of Magnet.
• Healthcare organizations, which earn the Magnet designation, must show they are open to, and even developing new models of care, applying existing evidence, building new evidence, and making visible contributions to the science of nursing.

New Knowledge, Innovation & Improvements
In the Evidence…
• Consistent involvement of nursing in Institutional Review Board
•Structure and processes to develop, expand and/or advance nursing research, e.g., Yvonne L. Munn Center for Nursing Research, Research and Evidence Based Practice Committee, Munn awards, Post-doctoral Fellowships, Nursing Research EXPO

New Knowledge, Innovation & Improvements
In the Evidence…
•Structures and processes to:
•Evaluate nursing care
•Translate new knowledge into nursing practice
•Participate in Innovation
•Involvement in evaluation and allocation of technology and information systems to support practice
•Participation in architecture and space design to support practice

Empirical Quality Results
The question the ANCC poses to organizations seeking Magnet status is not “What do you do?” or “How do you do it?” but rather a focus on “What difference have you made?” A shift from structure and process to outcomes.
• Healthcare organizations are expected to become pioneers of the future and to demonstrate solutions to numerous problems inherent in the health care systems today.
• Outcomes need to be categorized in terms of clinical outcomes related to nursing; workforce outcomes; patient outcomes; and organizational outcomes.
Key indicators that paint a picture of the organization.

Quality: Indicator Definitions
• Nursing-sensitive indicator“Measures and indicators that reflect the
impact of nursing care on outcomes.”
(ANA 2004)
• Clinically-relevant indicator
Indicators for specialty areas and ambulatory nursing practices that may not have a national benchmark but are clinically relevant

What We Measure• Pressure Ulcers• Falls• Physical Restraints• Pediatric Peripheral Infiltrations• Central Line Blood Stream Infections• Catheter-Associated Urinary Tract
Infections• Ventilator-Associated Pneumonia• Time in Therapeutic Range • Completion of INRs in 28 days• Administration of Prophylactic
Antibiotics before Surgical Incision• Universal Protocol• Administration of Prophylactic
Antibiotic before Cardiovascular Electronic Device Implementation
• DVT Prophylaxis +/- 24 hours before Surgery
• Administration of Prophylactic Antibiotics before Cesarean Section
• Administration of Appropriate DVT Prophylaxis before Cesarean Section
• Human Papillomavirus Vaccine
• Influenza Vaccine with Asthma • Diabetes Self Management • Informed Consent• Completion of RN Machine Safety
Check Prior to Initiation of Dialysis• Pre-operative Fall Risk Assessment• Successful First Attempts at
Peripheral Intravenous Insertions• Occlusion Rates in ICC Lines• Proportion of Infants in 22 to 29
Weeks Gestation Treated with Surfactant within 2 hours of birth
• Proportion of Infants in 22 to 29 Weeks Gestation Screened for Retinopathy of Prematurity (ROP)
• Managing Post-operative Care Correct Tray Set-up Protocol
• Vascular Access Time-Out • Door to IV rt-PA in 60 Minutes• Door to CT Scan (median time) • Acute Myocardial Infarction (AMI):
Primary PCI within 90 minutes of Arrival

Falls:Trends

HAPU:Trends

Restraints: Trends

CLABSI: Trends

• HCAHPS is an acronym for “Hospital Consumer Assessment of Healthcare Providers & Systems”
• Random sampling of adult inpatient discharges
• Excludes psychiatry, rehabilitation, and pediatric discharges
• Separate survey is done for inpatient pediatrics
• MGH administers through vendor (QDM) by phone
Patient Satisfaction: HCAHPS Survey Basics

• ED and Pediatrics: specialized surveys administered by QDM• Radiation Oncology and Infusion center: Press Ganey• Outpatient: CG-CAHPS “Clinician and Group Consumer Assessment of
Healthcare Providers & Systems” Survey • currently voluntary but CMS moving towards making it publicly reported• MGH is exploring ways of incorporating nursing specific questions into this survey.
• All of these surveys measure patients’ perceptions of “how often” they felt they received high quality clinical and customer service
Other Patient Experience Surveys

Nurse Listening – Indicator ResultsDuring this hospital stay how often did nurses listen carefully to you?
Adult Inpatient HCAHPS Item Level Top-Box ScoresNurses Listen vs. QDM 50th Percentile
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Quarter
To
p-B
ox
%
Nurses Listen 76.5% 75.6% 76.3% 74.9% 77.6% 77.2% 76.7% 77.9%
QDM 50th %ile 74.3% 74.3% 74.3% 74.3% 74.3% 74.3% 74.3% 74.3%
Oct - Dec 2010
Jan - Mar 2011
Apr-Jun 2011
Jul - Sep 2011
Oct - Dec 2011
Jan - Mar 2012
Apr - Jun 2012
Jul - Sep 2012
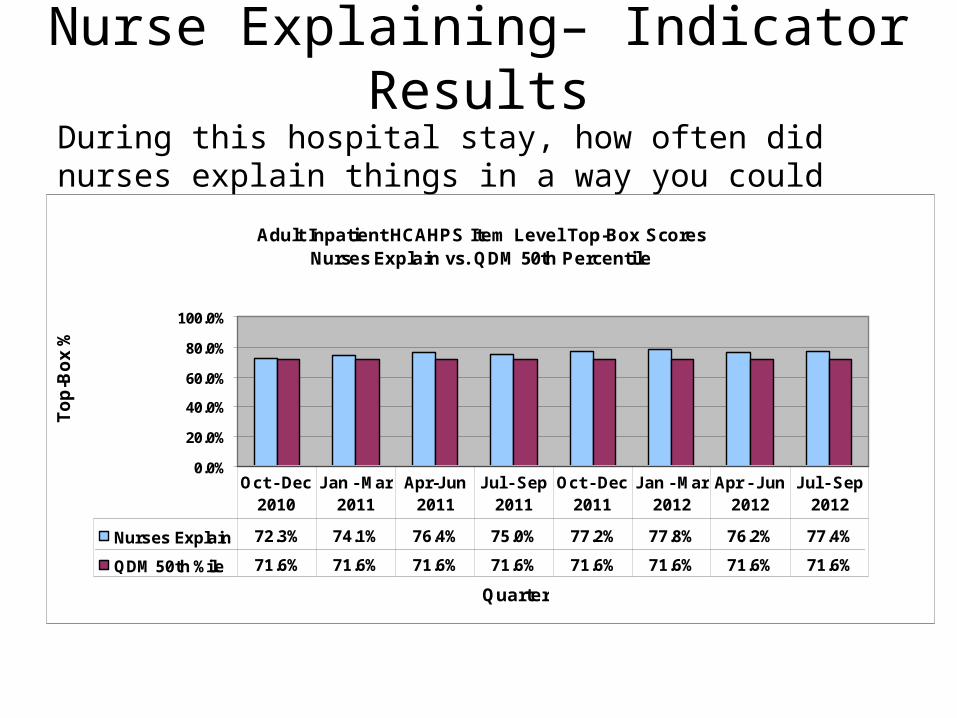
Nurse Explaining– Indicator ResultsDuring this hospital stay, how often did nurses explain things in a way you could understand?
Adult Inpatient HCAHPS Item Level Top-Box ScoresNurses Explain vs. QDM 50th Percentile
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Quarter
To
p-B
ox
%
Nurses Explain 72.3% 74.1% 76.4% 75.0% 77.2% 77.8% 76.2% 77.4%
QDM 50th %ile 71.6% 71.6% 71.6% 71.6% 71.6% 71.6% 71.6% 71.6%
Oct - Dec 2010
Jan - Mar 2011
Apr-Jun 2011
Jul - Sep 2011
Oct - Dec 2011
Jan - Mar 2012
Apr - Jun 2012
Jul - Sep 2012

Nurse Courtesy and Respect During this hospital stay, how often did nurses treat you with courtesy and respect?
Adult Inpatient HCAHPS Item Level Top-Box ScoresNurses Respect vs. QDM 50th Percentile
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Quarter
To
p-B
ox
%
Nurses Respect 87.2% 86.7% 85.6% 86.2% 87.1% 87.0% 87.2% 89.0%
QDM 50th %ile 84.7% 84.7% 84.7% 84.7% 84.7% 84.7% 84.7% 84.7%
Oct - Dec 2010
Jan - Mar 2011
Apr-Jun 2011
Jul - Sep 2011
Oct - Dec 2011
Jan - Mar 2012
Apr - Jun 2012
Jul - Sep 2012

Response to Pain– Indicator Results
During this hospital stay, how often did the hospital staff do everything they could to help you with your pain? Adult Inpatient HCAHPS Item Level Top-Box Scores
Help with Pain vs. QDM 50th Percentile
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Quarter
To
p-B
ox
%
Help with Pain 78.5% 78.2% 77.1% 78.6% 78.5% 79.9% 79.1% 79.3%
QDM 50th %ile 77.2% 77.2% 77.2% 77.2% 77.2% 77.2% 77.2% 77.2%
Oct - Dec 2010
Jan - Mar 2011
Apr-Jun 2011
Jul - Sep 2011
Oct - Dec 2011
Jan - Mar 2012
Apr - Jun 2012
Jul - Sep 2012

Nurse Satisfaction Surveys
• Staff Perceptions of Professional Practice Environment Survey– Measures: autonomy, control over practice, clinician-physician
relationships, communication, teamwork, conflict management, internal work motivation, cultural sensitivity
• NDNQI Nurse Survey with Practice Environment Scale Subscales)– Nurse Participation in Hospital Affairs– Nursing Foundations for Quality of Care– Nurse Manager Ability, Leadership, and Support of Nurses– Staffing and Resource Adequacy– Collegial Nurse-Physician Relations
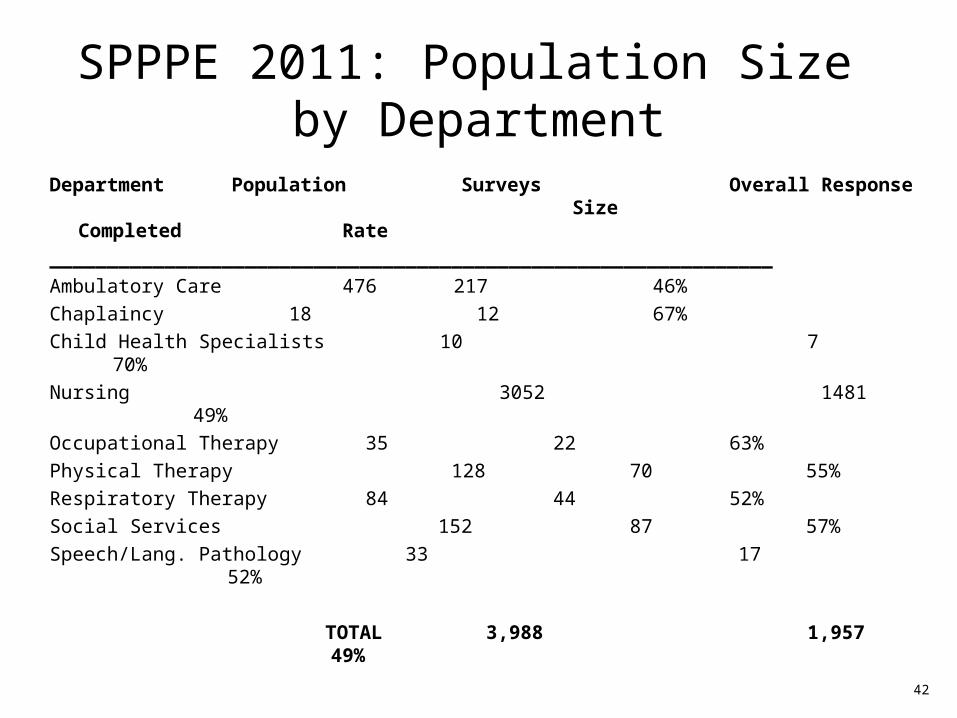
SPPPE 2011: Population Size by Department
Department Population Surveys Overall Response Size Completed Rate
_______________________________________________________________
Ambulatory Care 476 217 46%
Chaplaincy 18 12 67%
Child Health Specialists 10 7 70%
Nursing 3052 1481 49%
Occupational Therapy 35 22 63%
Physical Therapy 128 70 55%
Respiratory Therapy 84 44 52%
Social Services 152 87 57%
Speech/Lang. Pathology 33 17 52%
TOTAL 3,988 1,957 49%42

43
PCS Mean Scores on 8 Professional Practice Environment
Characteristics
Characteristic
2008 Mean
Scores N = 1,941
2010 Mean
Scores N = 1,664
2011 Mean
Scores N = 1,957
A utonom y/Leadersh ip 3.0 3.0 2.8
C lin ic ian /M D R ela tionsh ips 3.0 2.9 2.9
C ontro l O ver P ractice 2.9 2.9 3.0
C om m unica tion 3.1 3.0 3.0
Team w ork 2.9 2.8 2.9
C onflic t M anagem ent 2.7 2.6 2.7
In terna l W ork M otiva tion 3.4 3.4 3.4
C ultu ra l S ensitiv ity 3.2 3.2 3.2

44
2011 SPPPE: Overall Work Satisfaction
2008 2010 2011
N** Satisfied* N** Satisfied
* N**
Satisfied*
Total Patient Care Services
1934 85% 1638 87% 1919 86%
Ambulatory Care = = = = 214 85%
Chaplaincy 13 92% 13 92% 12 67%
Child Health Specialists
= = = = 7 100%
Nursing 1675 85% 1383 86% 1454 84
Occupational Therapy
26 100% 21 100% 22 86%
Physical Therapy 83 96% 85 94% 70 93%
Respiratory Therapy
58 95% 54 85% 44 93%
Social Services 59 66% 59 66% 80 81%
Speech/Language Pathology
20 100% 22 96% 16 94%
* Includes satisfied and very satisfied; ** N changed due to missing data
= not measured

NDNQI Nurse Survey – Nursing Participation in Hospital Affairs
Best Practices: Transformative Leadership, Collaborative Governance Committees, Clinical Recognition Programs, Access to CNO, Input into selection process for hiring new staff at all levels, Care Redesign Teams
Strategies for Improvement: Committee participation, Clinical Recognition Program
Massachusetts General Hospital - June 2012 SurveyNurse Satisfaction - Practice Environment Scale of the Nursing Work Index (PES-NWI)
NDNQI Database - Academic Medical Centers Benchmark
2.93 2.87
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
Mea
n S
core
MGH Mean NDNQI Academic Medical Center Mean
MGH Mean 2.93
NDNQI Academic MedicalCenter Mean
2.87
Nursing Participation in Hospital Affairs

Massachusetts General Hospital - June 2012 SurveyNurse Satisfaction - Practice Environment Scale of the Nursing Work Index (PES-NWI)
NDNQI Database - Academic Medical Centers Benchmark
3.12 3.09
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
Mea
n S
core
MGH Mean NDNQI Academic Medical Center Mean
MGH Mean 3.12
NDNQI Academic MedicalCenter Mean
3.09
Nursing Foundations for Quality of Care
NDNQI Nurse Survey – Nursing Foundations for Quality of Care
Best Practices: Continuing Education; MGH Mission, Credo, Boundaries; Nursing Sensitive Indicators; Unit-based Clinical Nurse Specialists; Learning bundles; Culture of Safety Survey; Excellence Every Day Portal; Toolkits; ethics resources
Strategies for Improvement: Monitoring of resources; sharing best practices
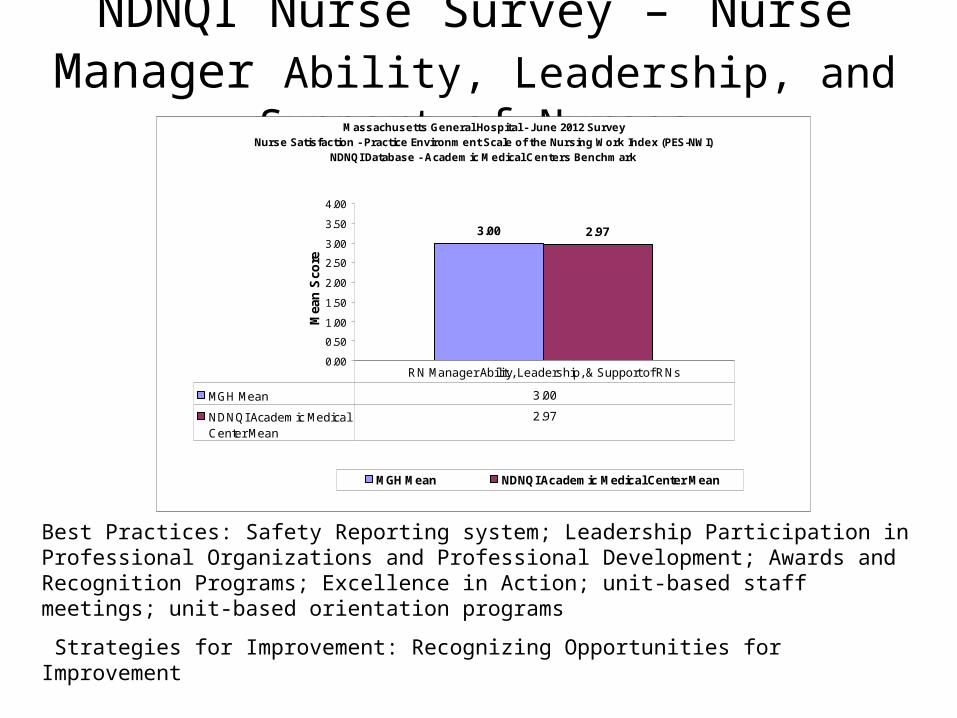
NDNQI Nurse Survey – Nurse Manager Ability, Leadership, and Support of Nurses
Best Practices: Safety Reporting system; Leadership Participation in Professional Organizations and Professional Development; Awards and Recognition Programs; Excellence in Action; unit-based staff meetings; unit-based orientation programs
Strategies for Improvement: Recognizing Opportunities for Improvement
Massachusetts General Hospital - June 2012 SurveyNurse Satisfaction - Practice Environment Scale of the Nursing Work Index (PES-NWI)
NDNQI Database - Academic Medical Centers Benchmark
3.00 2.97
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
Mea
n S
core
MGH Mean NDNQI Academic Medical Center Mean
MGH Mean 3.00
NDNQI Academic MedicalCenter Mean
2.97
RN Manager Ability, Leadership, & Support of RNs

NDNQI Nurse Survey – Staffing and Resource Adequacy
Massachusetts General Hospital - June 2012 SurveyNurse Satisfaction - Practice Environment Scale of the Nursing Work Index (PES-NWI)
NDNQI Database - Academic Medical Centers Benchmark
2.92 2.79
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
Mea
n S
core
MGH Mean NDNQI Academic Medical Center Mean
MGH Mean 2.92
NDNQI Academic MedicalCenter Mean
2.79
Staffing and Resource Adequacy
Best Practices: Quadramed workload activity measurement system; Exempt status; self-scheduling; budget
Strategies for Improvement: Leave of absence, capacity management

NDNQI Nurse Survey – Collegial Nurse-Physician Relations
Massachusetts General Hospital - June 2012 SurveyNurse Satisfaction - Practice Environment Scale of the Nursing Work Index (PES-NWI)
NDNQI Database - Academic Medical Centers Benchmark
3.09 3.07
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
Mean
Sco
re
MGH Mean NDNQI Academic Medical Center Mean
MGH Mean 3.09
NDNQI Academic MedicalCenter Mean
3.07
Collegial RN-MD Relations
Best Practices: Conflict resolution courses; nurse practitioner expansion; interdisciplinary rounds; care redesign teams; attending nurse role; safety reports
Strategies for Improvement: Monitoring impact of care redesign initiatives; care providers; roll-out of Attending Nurse role; addressing disruptive behavior

April 2010 – October 2012 Evidence collection and writing
October 1, 2012 Submitted evidence to ANCC
October 1, 2012 – Prepare for site visit Site visit 2013
March 4-7, 2013 Site Visit
Approx. 2 months post site visit Magnet Commission Vote
Magnet Re-designation Timeline

Purpose of Site Visit
• A site visit occurs if the scores for the sources of evidence fall within a range of excellence.
• The purpose of the site visit is to verify, clarify, and amplify the content of the written documentation and evaluate the organizational setting in which nursing is practiced.

Site Visit – March 4-7, 2013Appraisal Team• Mary G. Nash, PhD, FAAN, FACHE - Team Leader
Chief Nursing Officer and Associate Vice President for Health Sciences, Ohio State University Health System, Columbus, OH
• Carol “Sue” Johnson, PhD, RN, NE-BC – Team Member
Director, Nursing Clinical Excellence & Research, Parkview Health, Fort Wayne, IN
• Linda C. Lewis, RN, MSA, NEA-BC, FACHE – Team Member
Chief Nursing Officer and Vice President for Patient Care Services, Forsyth Medical Center, Winston-Salem, NC
• Linda Lawson, MS, RN, NEA-BC – Team Member
Chief Nursing Officer, Sierra Medical Center, El Paso, TX

Staff and Public Notices: Before 1/23/13
Staff Notices:- All-user message
- Mailing to MGH employees not on e-mail - Have 24/7 access to Magnet evidence (Magnet Portal Page: http://www.mghpcs.org/magnet or in Nursing Supervisor Office on Bigelow 1406D, phone 617-726- 6718, pager 617-726-2000 #2-5101
Public Notices: - Hospital signage (English & Spanish) - Newspaper ads: Boston Metro, Beacon Hill Times, Charlestown Patriot, Revere Journal, Chelsea Record, Waltham News Tribune, Danvers Herald, El Mundo Boston
Other: - MGH website - Caring Headlines, Fruit Street Physician, Hotline

Site Visit – Agenda• Visits to patient care settings (units, clinics, health centers) • Numerous meetings with MGH Staff Nurses
• Breakfast and luncheon meetings (randomly-selected nurses)• Health Centers nurses
• Nursing and Organizational meetings:• Hospital Senior Leadership plus representatives from MGH Board of
Trustees• Nursing Executive Leadership• Nursing Directors• Physicians• Collaborative Governance committees (Ethics, Research/EBP, Informatics,
all CG committees in aggregate)• Champions (e.g. Magnet, Pain, etc.) • Ancillary and Support Service Departments (Departments that support
nursing care delivery)• Additional meetings: Interdisciplinary Committees, Community, Schools of
Nursing, Human Resources, Nursing Education, Patient Satisfaction, Staff Satisfaction, Peer Review and Clinical Advancement)
• Document review: performance evaluations for all levels of nurses, IRB minutes, staff and patient complaints, requested information about selected sources of evidence
Champions
• Staff nurse representatives from each practice area along with all members of the Hospital community
• Role: To influenceTo communicate To educate
• Operationalized through Collaborative Governance structure and key linkages with off-site locations

Communications & Education Plan
Each week, 1 topic is covered by the 5 strategies below, and repeated as time allows• Magnet Monday → electronic and web portal• Weekly Luncheon → content is covered “live” in Lunder
234 allowing for Q&A and other dialogue• Tool Box → material is provided to the ND/CNS/CG
Champion to use (posted on portal page)• Leadership → materials are reviewed with the ND and
CNS groups by a member of the subcommittee • Unit-Based → tool box contents are covered at the local
level

Characteristics of Magnet Hospitals Include:
• Concern for patients and families is our #1 priority
• Nurses identify the hospital as a supportive place to work
• Nursing leadership is visible and accessible
• Autonomous and empowered clinicians
• Delivery of high quality nursing care as rated by patients and staff
• Strong and collegial nurse-physician relationships, teamwork and communication
• Delivery of interdisciplinary patient- and family-centered care



![PIANO CONCERTO IN F 2nd Movement for Clarinets · 102 102 102 102 102 102 102 102 102 102 102 10 44 [Title]](https://img.dokumen.tips/doc/110x75/5e3946b540eed0696e2e90d2/piano-concerto-in-f-2nd-movement-for-clarinets-102-102-102-102-102-102-102-102-102.jpg)








![UNIVERSIDADE DE SÃO PAULO ESCOLA DE ENFERMAGEM …...Parisi TCH. Magnet Recognition Program: revisão integrativa de literatura. [dissertação]. São Paulo: Escola de Enfermagem,](https://img.dokumen.tips/doc/110x75/5f92827a3289e04a0d2c50d2/universidade-de-sfo-paulo-escola-de-enfermagem-parisi-tch-magnet-recognition.jpg)

















