Embed Size (px)
Citation preview

1Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
The impact of vaccination on the epidemiology of infectious diseases
(lecture 1)Roy Anderson
Department of Infectious Disease EpidemiologyFaculty of Medicine,
Imperial College London
New Delhi, India - September 19th 2011

2Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Contents-Lecture 1
• History.• Basic epidemiological principles.• Criteria for eradication.• Heterogeneities.• Impact of mass vaccination on
epidemiological pattern.• Conclusions.
Epidemiccurves

3Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Vaccines as a fraction of total pharmaceutical sales in total – worldwide in 2006
Total sales - $ 380 billion

4Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Geographical distribution of vaccine market share April 2011

5Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Vaccine Trails - Stages
• Pre-clinical 2 years• Phase 1 10-1000• Phase 2 100-1000• Phase 3 10,000-70,000• Phase 4 100,000-1,000,000
Stage Number of people in trial
Time from proof of concept to market – of the order of 10 years or longer

6Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Measles – England & Wales

7Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Pertussis notifications – England & Wales

8Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Emergence of P3 strains of Bordetella pertussis

9Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Sero-surveillance – mumps - Netherlands

10Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Hib (Haemophilus influenzae type b) Vaccination – England & Wales

11Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Pneumococcal disease age distribution - Netherlands

12Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Basic epidemiological principles

13Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Stochasticity & persistence
Disease extinction likely by chance when number of infectives falls to very low numbers.
- so extinction more frequent as population size decreases and cycle amplitudes increase.

14Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
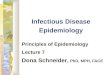
Critical community sizeMinimum population size at which measles fadeouts (proportion of weeks with no cases) become rare.
TRUE

15Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Seasonality in transmission of measles – school holidays
0
20
40
60
1 11 21 31 41 51
RCGP Model
Week
Inc
ide
nc
e
Confidencebar

16Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
HIV-1 prevalence in Nairobi, Kenya 1981-1999 – stratified by risk group
Year
% in
fected w
ith H
IV-
1
Sex workersMen with GUDPregnant women
Sex workersMen with GUDPregnant women
Pregnant womenPregnant women
Men with GUDMen with GUD
Sex workersSex workers

17Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Daniel Bernoulli - 1700 to 1782
D. Bernoulli (1760)used a simple mathematical
model to evaluate the effectiveness of variolation to
protect against smallpox.
Daniel Bernoulli was one of a number of early mathematicians
who turned their skills to probability problems raised by gamblers - perhaps at the card
tables in Monte Carlo (e.g. C. Huyghens 1657).

18Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Basic principles in Infectious Disease Epidemiology
• The key determinant of incidence and prevalence of infection is the basic reproductive number Ro.
• Ro measures the average number of secondary cases generated by one primary case in a susceptible population
• Many factors determine its magnitude, including those that influence the typical course of infection in the patient and those that determine transmission between people.

19Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Basic Reproductive number, Ro
Chains of transmission between hosts
Generation 1 2 3 4 5 6 7 8
Number Infected
R11 2 2 3 4 6 7
1 1.5 1.33 1.5 1.16
R0 Basic reproduction numberaverage no. of secondary cases generated by 1 primary case in a susceptible population
Rt Effective reproduction number number of infections caused by each new case occurring at time, t
• The key determinant of incidence and prevalence of infection is the basic reproductive number Ro.
• Many factors determine its magnitude, including those that influence the typical course of infection in the patient and those that determine transmission between people.

20Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
The epidemic curveR
ate
of
new
in
fect
ion
s
establishment exponentialgrowth
Time
exhau
stion
of
suscep
tibles
endemicity
Equilibrium, or recurrent epidemics
y e
(R0 -1
)/TG t
Random (stochastic)effects

21Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Typical course of infection within the host
Estimation of average latent & infectious periods plus distributions

22Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Viral load over course of infection as a function of patient age (influenza A - viral titre AUC versus age)
100
200
300
400
500
600
700
800
900
Vir
al t
itre
AU
C(l
og
10 T
CID
50
h/m
L)
0 10 20 30 40 50 60 70 800
Age (years)90 100
Line of regression
95% confidence limits for mean predicted value
Osterhaus, Oxford, Jackson, & Ward (2001)

23Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
The typical course of infection
0
10
20
30
40
50
60
70
80
90
100
Days post onset of clinical symptoms
Per
cen
tag
e o
f sa
mp
les
po
siti
ve
Naso pharangeal aspirate Stool Urine
1
10
100
1000
10000
1 2 3 4 5 6 7 8 9
days post viral inoculation
viral t
iter (l
og 10
)0
5
10
15
sympto
m sco
re
Viral load
Symptom score
Influenza ASARS CoV
* Hayden et al. (1998) J. Clin Invest 101 p643Experimental human influenza A/Texas/36/91 (H1N1) intranasal inoculation 105 dose Peiris et al (2003)

24Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Basic principles in Infectious Disease Epidemiology
• The magnitude of Ro varies according to location and population - it is strongly influenced by birth rate, population density and behavioural factors.
• The magnitude of Ro can be ascertained by cross sectional serological surveys.

25Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
What is Herd Immunity?
• The impact of the fraction immune in the community on the per capita rate of transmission of an infectious agent.
• The level of herd immunity can be measured by reference to the magnitude of reduction in the value of Ro.

26Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
How can the degree of herd immunity and the magnitude of Ro be assessed?
• Cross-sectional and longitudinal serological surveys.
• Serum and saliva (viral infections).• Activated T cells (bacteria and protozoa)?• Quantitative assays.

27Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Scientific methods in the study of herd immunity
• Immunological and Disease Surveillance methods provide the empirical base for analysis and interpretation.
• Mathematical & statistical methods play an important role in the analysis of infectious disease transmission and control.
• They help to define both what needs to be measured, and how best to measure define epidemiological quantities.

28Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Age in Years
Prop
ortion S
eropositive
0 2.5 5 7.5 10 12.5 15 17.5 20
1
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0
Maternal Antibodies Antibodies from Infection
Age-specific serology
Used to calculate the average age at infection, A, the average
duration of maternal antibody protection, M, and the degree
of herd immunity
Used to calculate the average age at infection, A, the average
duration of maternal antibody protection, M, and the degree
of herd immunity

29Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Serological profile - Varicella virus
(Schneweis et al, 1985 - Germany)

30Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Force or rate of infection λ and the average age of infection A – estimation from serology (1)
If the proportion seropositive at age a is p(a), then the average force or rate of infection λ over the interval 0 to a years of age is given by:
λ(a)=p(a)/[L(1-e(-a/L))]; eq(1)
where L is life expectancy. Other relationships of importance are:
A≈1/λ; eq(2)
R0≈L/A; eq(3)and pc=(1-1/R0)=(1-A/L). eq(4)
Here R0 is the basic reproductive number (average number of secondary cases generated by one primary case, and pc is the critical fraction to be vaccinated to block transmission.

31Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Force or rate of infection λ and the average age of infection A – estimation from serology (2)
A simple worked example is as follows. Consider measles where 70% of children are seropositive at age 3 years (p(3)=0.7), and life expectancy is 60 years. Using the equations in the previous slide:
from eqn(1) λ = 0.2392 yr-1;
the average age at infection, A = 4.18 years;
R0 = 14.35; and
pc = 0.93, or 93% coverage.
In reality many complications slightly alter these values. One important example is maternal antibodies which have a half life of 6 months in well nourished mothers who breast feed. This value (0.5 yrs) should be subtracted from a in the calculation of λ – which gives a required coverage of 94.2% (see Anderson & May (1991) for fuller discussion)

32Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
The calculation of the magnitude of Ro
A series of simple relationships exist between keyepidemiological, demographic and vaccination programme related parameters.
The magnitude of Ro and the average at infection prior to mass vaccination, A, plus life expectancy in the population are related as follows
)/()( MAALRo )/()( MAALRo Here, M is the average duration of maternal antibody protection (6 months) and L is life expectancy

33Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Force or rate of infection λ and the average age of infection A – estimation from serology (3)
Some examples of studies from which the data employed in the previous calculations can be derived. Serology for Rubella virus in the UK (see
Anderson & May (1991))
Decay in maternal antibodies Longitudinal and cross-sectional serological surveys

34Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
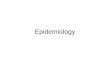
Mumps Virus - Age-specific change in the per capita rate of infection (Anderson & May 1983)
0.5-2 3-5 6-8 9-14 15+0
0.5
1
1.5
2
2.5
Age in years
Fo
rce o
f infe
ction
/ann
um

35Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Human Parvovirus B19 serology – force of
infection (FOI) by ageMossong et al (2008) Parvovirus B19 infection in five European countries: seroepidemiology, force of infection and maternal risk of infection. Epidemiol. Infect. (2008), 136, 1059–1068
Belgium
England
Finland
Poland
Italy Age (years)
Forc
e of
Infe
ction
(FO
I)
% S
erop
ositi
ve

36Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Parameters – Who mixes with Whom• Wallinga J, Teunis P, Kretzschmar M. (2006) Using data on social contacts
to estimate age-specific transmission parameters for respiratory-spread infectious agents. American Journal of Epidemiology 164, 936–944.
• Beutels P, et al. (2006) Social mixing patterns for transmission models of close contact infections : exploring self-evaluation and diary-based data collection through a web-based interface. Epidemiology and Infection. 134, 1158–1166.
• Edmunds WJ, O’Callaghan CJ, Nokes DJ. (1997) Who mixes with whom? A method to determine the contact patterns of adults that may lead to the spread of airborne infections. Proceedings of the Royal Society of London, Series B: Biological Sciences 264, 949–957.
• Farrington CP. (1990) Modelling forces of infection for measles, mumps and rubella. Statistics in Medicine 9, 953–967.

37Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Average age, A, at infection prior to immunisation
Infection Average age at infection, A
Location/time period
Measles virus 5-6 years
2-3 years
USA 1955-58
Bangkok, Thailand 1967
Rubella virus 9-10 years Sweden 1965
Varicella virus 6-8 years USA 1921-28
Polio virus 12-17 years USA 1920-60
Mumps virus 7-8 years England & Wales 1975
Smallpox virus 10-15years Bangladesh 1940

38Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Estimates of the basic reproductive number, Ro
Infection Location Time period Ro
Measles England
Canada
1947-50
1912-13
13-15
11-13
Varicella USA 1943 7-8
Mumps Netherlands 1970-80 11-14
Rubella West Germany 1970-79 6-7
Polio USA 1955 5-6
HIV-1 Nairobi, Kenya
(sex workers)
1981-85 11-12
Smallpox Bangladesh 1940 4-6
Influenza A (H1N1)
England 2010 1-1.5

39Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Estimation of R0 from past influenza A epidemics

40Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
SARS - distribution of R
0
5
10
15
20
25
30
Number
0 2 4 6 8 10 12
Number of secondary cases
Super spreadingevents (person,place & setting)
Rapid SARS Virus Spread in Flats 7 and 8, Block E
Amoy Garden, Hong Kong. 1st March 2003 –
292 people infected by one index case

41Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
The generation of secondary cases with vaccination
Generation 1 2 3 4 5 6 7 8
Number Infected
R11 2 2 3 4 5 11 2 1 1.5 1.33 1.25 0.2
Vaccinatedindividuals

42Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Basic principles in Infectious Disease Epidemiology
The magnitude of pc , the fraction of each birth cohort that must be immunised to block transmission is given bythe following simple expression:,
/]/[][ bLALpc /]/[][ bLALpc
The parameter b is the average age at first vaccination,L is life expectancy (related to the net birth rate), and A is the average age at infection prior to mass immunisation. Vaccine efficacy = ε, ranging from 0-1.

43Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Vaccine efficacy
MEASLES 90%-95%
MUMPS 72%-88%
RUBELLA 95%-98%
(Christensen & Bottiger,1991; Clarkson & Fine,1987; Ramsey et. al.,1994)

44Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
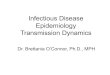
Mass vaccinationAnderson, et al (1998) Lancet 350:1466-1470
0.95
0.96
0.97
0.98
0.99
1
Average age at Vaccination V (years)
Fra
ctio
n f
va
ccin
ate
d
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5
Fraction that must be vaccinated toblock transmission (A=5 years)
Vaccine efficacy changes with age due to presence of maternal antibodies
Maximumvaccine
efficacy Q
Q=1.0
Q=0.98
Q=0.97

45Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Age at vaccination - good and bad patterns
0
20
40
60
80
% I
mm
un
ized
0- 1- 2- 3- 4- 5- 6- 7- 8- 9- 10-
Age group in years
Good pattern - clusteredaround the optimal age
Poor pattern - spreadto the right side ofthe optimal age

46Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
1) Increase in average age at infection
2) Increase in the inter-epidemic period
3) Toughs in susceptibility in the herd immunity profile
4) Changes in the age distribution of infection and serious disease
5) Non-linear relationship between the incidence of infection and disease and vaccine uptake
Predictions based on mathematical models of transmission and the
impact of mass vaccination

47Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Average age of infection - the impact of vaccination
0
10
20
30
40
50
60
0 0.2 0.4 0.6 0.8
Proportion of cohort immunised at age 2 years
Av
era
ge
ag
e a
t in
fec
tio
n (
yrs
)
Average age of infectionprior to vaccination set at 5 years.
Average age of vaccination setat 2 years.

48Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Vaccination - and the age distribution of infection

49Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Impact of vaccination on serology

50Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Herd immunity profile - across age classes and through time
(Anderson and May, 1982; Science 215:1053-60).
Measles - serology post the introduction of a cohort based vaccination programme

51Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
<1m
1-m
6-m
1-
2-
4-
6-
8-
10-
12-
14-
16-
20-
25-
30-
40-
>600
0.2
0.4
0.6
0.8
1
19791981
19831985
19871989
1991
Age
Fra
ction
sero
po
sitive
<1m
1-m
6-m
1-
2-
4-
6-
8-
10-
12-
14-
16-
20-
25-
30-
40-
>600
0.2
0.4
0.6
0.8
1
19791981
19831985
19871989
1991
Age
Fra
ction
sero
po
sitive
Female Male
Age stratified & longitudinal serologyfor Rubella antibodies. Finland 1979-91
(Ukkonen et al, 1995)

52Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
0
0.5
1
1.5
2
2.5
0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Proportion Vaccinated
Ra
tio
of
ca
se
s a
fte
r/b
efo
reMass vaccination can increase the incidence
of serious disease if the likelihood rises with age per case of infection
(Anderson & May, 1983; J. Hygiene 90:259-325)
The case of rubella and congenital rubella syndrome

53Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Percentage gain from the indirect effects of herd immunity
0
20
40
60
80
100
0.75 0.85 0.95
Proportion of cohort vaccinated
% g
ain
fro
m i
nd
ire
ct e
ffe
cts
Critical vaccinationcoverage to block
transmission, pc

54Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Ferguson et al, 2006 – Nature - on line
April 27th 2006
Individual based stochastic simulation model with three scales of mixing – extensive
sensitivity analysis and analysisof past influenza epidemics
200 days compressedinto a few seconds

55Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Conclusions• Eradication difficult when Ro large and population density plus net
birth rate high.• Heterogeneity in population density and vaccine coverage important.• Carrier state important as are reservoir hosts (if involved).• Mathematical & computational methods permit analytical &
simulation studies of potential impact of different strategies.• Cost benefit studies need to take account of indirect effects of mass
vaccination on transmission.• Vaccine coverage must be maintained at high levels to avoid the
immigration of infectives stimulating epidemics in susceptible pockets.• Imperfect vaccines – phase IV monitoring of vital importance.• Multi- strain systems – more research required – will new strains
replace those targeted by a multi-valent vaccine?

56Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
The End

57Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
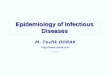
Mass vaccination programmes for infections where the incidence of serious disease rises with age at
infection (e.g. Rubella)Rubella. The equilibrium ration of rubella cases in pregnant women in the age range 16-40 years after vaccination of a proportion p)the horizontal axis). At age V years divided by cases before vaccination. The fertility function used to derive this graph is displayed below. The vaccination policy adopted is for vaccination of boys and girls around one year of age (V=1).
A is the average age of infection in years for
rubella prior to immunisation.

58Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Rubella vaccination programmes in the UK – change in policy (Anderson & May, 1983)
The ratio of cases of infection in 16-40 year old women after vaccination divided by before for tow different policies – vaccinated boys and girls at 2 years of age, and vaccinating girls only at 12 years of age. The dark shaded regions denote where a policy could make matters worse. In the UK with coverage above 80% no problem arises

59Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Spatial de-correlation inducedby vaccination - measles
Viewing de-correlation
Epidemics initially highly synchronised before vaccination, then increasingly de-correlated post-vaccination.
Spatial
location
Den
sity of cases

60Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
• High performance, object-oriented code. Intended to be scaleable to allow 000s of model simulations of 60 million population to be performed.
• Computationally intensive (>5GB memory use for 60 million).
• Three levels of population structure:
• Flexible modelling of disease biology (arbitrary distributions, number of disease stages), and interventions (ring vaccination, mass vaccination, quarantine, anti-viral treatment, movement constraints).
Model design for individual based stochastic simulations
Household Network(disease specific)
Distance
Pro
ba
bili
ty
Spatial

61Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Spatial kernels – mobile phone data – frequency versus – distanced moved per defined time unit
1
10
100
1000
10000
100000
1000 10000 100000 1000000
Sum over daily legs
Legs
Daily Extent
Distance metres
Nu
mb
er of
peo
ple

62Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Data needs: detailed population data: Landscan (Oakridge Natl. Lab.)
Need both population data (density, age, household)and mixing/travel data.
Population density – based on satellite imagery

63Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
HIV-1 vaccines• At present, there are many ongoing HIV-1 vaccine trials and
several pending for 2006, involving different vaccines (of which some are DNA-based, some use recombinant viral vectors, 4 are protein subunits and 3 are lipopeptide-based).
• Most are in Phase I, with VaxGen’s two trials (in North America and Thailand) the only Phase III studies completed. Both Phase III trials were completed in 2003, with efficacy data revealing no difference in infection in treated and untreated arms.
• The majority use clade B strains, but a few candidates (especially among the newer ones in the pipeline) are based on clades A, C, D and E (http://www.iavi.org).

64Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Eradication criterion – protective vaccines
]/1][/11[ 0 VLR
pc
pc is the critical fraction of each cohort immunised, R0 is the basic reproductive number, L is life expectancy, V is the duration of vaccine protection and ε is
vaccine efficacy

65Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Imperfect vaccines• Vaccinated individuals acquire infection but
show slower progression to AIDS.• Slower progression is linked to lower viral
loads – especially in the primary HIV-1 infection phase.
• Lower viral load is linked to lowered infectiousness to susceptible sexual partners.
• Vaccination may be linked to increased risk behaviours.

66Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
]/1[
]/1][/11[
00
0
RR
VLRp
vc
Eradication criterion – imperfect vaccines
pc is the critical fraction of each cohort immunised, R0 is the basic reproductive
number for unvaccinateds, R0v is the reproductive numbers for vaccinateds,
L is life expectancy, V is the duration of vaccine protection and ε is
vaccine efficacy

67Department of Infectious Disease Epidemiology, Faculty of Medicine, Imperial College London
Illustrative schematic diagram, in two dimensions, of a multidimensional parameter space denoting the six possible equilibrium states that can exist for different
epidemiological and vaccine property related parameter combinations (Anderson & Hanson, 2005, JID).
No vaccination & endemic persistence of HIV-1 infection
(Ro>1, p=0)
No vaccination & endemic persistence of HIV-1 infection
(Ro>1, p=0)
No persistence of HIV-1 infection
(Ro<1)
No persistence of HIV-1 infection
(Ro<1)
Vaccination & eradication of HIV-1 infection
(yv*=0)
Vaccination & eradication of HIV-1 infection
(yv*=0)
Vaccination & perverse outcome of increased HIV-1 infection& decreased population size
(yv*>y*, Nv*<N*)
Vaccination & perverse outcome of increased HIV-1 infection& decreased population size
(yv*>y*, Nv*<N*)
Vaccination & good outcome
of increased HIV-1 infection
but increased population size
(yv*>y*, Nv*>N*)
Vaccination & good outcome
of increased HIV-1 infection
but increased population size
(yv*>y*, Nv*>N*) Vaccination & good outcome of decreased HIV-1 infection& increased population size
(yv*<y*, Nv*>N*)
Vaccination & good outcome of decreased HIV-1 infection& increased population size
(yv*<y*, Nv*>N*)